 Bo Sun
Bo Sun Yuchen Sun†
Yuchen Sun†
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol., 20 March 2024
Sec. Epilepsy
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1356715
Objective: This study aimed to explore the prevalence and risk factors of early postoperative seizures in patients with glioma through meta-analysis.
Methods: Case–control studies and cohort studies on the prevalence and risk factors of early postoperative seizures in glioma patients were retrieved from various databases including CNKI, Wanfang, VIP, PubMed, Embase, Cochrane Library, and Web of Science, and the retrieval deadline for the data was 1 April 2023. Stata15.0 was used to analyze the data.
Results: This review included 11 studies consisting of 488 patients with early postoperative seizures and 2,051 patients without early postoperative seizures. The research findings suggest that the prevalence of glioma is complicated by seizures (ES = 19%, 95% confidence interval [CI] [14%−25%]). The results also indicated a history of seizures (RR = 1.94, 95% CI [1.76, 2.14], P = 0.001), preoperative dyskinesia (RR = 3.13, 95% CI [1.20, 8.15], P = 0.02), frontal lobe tumor (RR = 1.45, 95% CI [1.16, 1.83], P = 0.001), pathological grade ≤2 (RR = 1.74, 95% CI [1.13, 2.67], P = 0.012), tumor≥ 3 cm (RR = 1.70, 95% CI [1.18, 2.45], P = 0.005), tumor resection (RR = 1.60, 95% CI [1.36, 1.88], P = 0.001), tumor edema ≥ 2 cm (RR = 1.77, 95% CI [1.40, 2.25], P = 0.001), and glioma cavity hemorrhage (RR=3.15, 95% CI [1.85, 5.37], P = 0.001). The multivariate analysis results showed that a history of seizures, dyskinesia, tumor ≥3 cm, peritumoral edema ≥2 cm, and glioma cavity hemorrhage were indicated as risk factors for glioma complicated with early postoperative seizures.
Significance: Based on the existing evidence, seizure history, dyskinesia, frontal lobe tumor, pathological grade ≤2, tumor ≥3 cm, partial tumor resection, edema around tumor ≥2 cm, and glioma cavity hemorrhage are indicated as risk factors for glioma complicated with early postoperative seizures.
Gliomas originate from the abnormal proliferation of glial cells in the brain (1, 2), and they are common primary central nervous system tumors (3), with a high mortality risk (4). The annual occurrence of gliomas is about 5–8 cases per 100,000 people, while the annual mortality rate is as high as 30,000, ranking third after pancreatic and lung cancers (5–7). In patients with gliomas, seizures are often the initial symptom and the reason for seeking medical attention. Glioma-related seizures are typical accompanying symptoms of gliomas, especially in low-grade gliomas (8, 9), where the main symptoms are sudden paroxysmal convulsions, foaming at the mouth, loss of consciousness, and convulsions of the limbs (10). The specific mechanisms underlying glioma-related seizures are not yet fully understood, and pathological changes and pathogenic mechanisms are diverse, likely resulting from the combined effects of multiple factors (11, 12). The abnormal expression of tumor-related genes is considered to be closely associated with the occurrence and development of seizures in brain tumors, especially gliomas (13). Although advances in surgery and chemoradiotherapy have improved the prognosis of glioma cases, the presence of seizures severely affects the quality of life for patients (14). Currently, the clinical efficacy of treating glioma-related seizures remains unsatisfactory because of an incomplete understanding of the pathophysiological, biochemical, molecular, and pharmacological mechanisms underlying its occurrence (15, 16). Giraldi et al. (17) found that there exist an obviously increased cumulative risk of new-onset seizures after craniotomy. Previous studies confirmed that seizures are a common complication of intracranial gliomas that can lead to disability or even death. Therefore, it is important to determine the relevant risk factors for early postoperative seizures in gliomas cases. However, the risk factors associated with gliomas remain controversial (18). Therefore, this study aimed to address these controversies through a meta-analysis investigating such risk factors. It is hoped that, by preventing and treating early postoperative seizures, the quality of life and outcomes of glioma patients can be improved.
This systematic review is conducted according to the preferred reporting items of the Protocol for Systematic Reviews and Meta-analyses (PRISMA-P) guidelines. The review will be conducted according to PRISMA criteria (19). The registration number is CRD42023415658.
We searched the CNKI, Wanfang, VIP, PubMed, Embase, Cochrane Library, Web of Science, and other databases to identify the risk factors of seizures in glioma cases. The search deadline for the data was 1 April 2023. Subjects and free words were used for retrieval: seizures, glioma, and risk factors. See Supplementary material 1 for specific retrieval strategies.
The study included adults who met the diagnostic criteria for glioma (including low- and high-grade gliomas) (20), and the exposure factor was early postoperative seizures (occurred within 7 days after surgery). The primary outcome was the prevalence of postoperative seizures, while the secondary outcome was risk factors for postoperative seizures. The eligible study designs included case–control and cohort studies.
The exclusion criteria encompassed meta-analyses, protocols, letters, repeatedly published articles, systematic reviews, failure to obtain full text, failure to obtain available data, and animal experiments.
Two independent evaluators performed the literature screening to extract data and directly screened the easily judged literature by reading the titles, abstracts, and the full text. Any disagreements were resolved by consulting relevant experts. The selection criteria were strictly followed during the screening process. They extracted the corresponding indicators from the studies and cross-checked the extracted data to ensure consistency. The primary collected data included the name of the first author, year of publication, country, study design, sample size, sex, and age.
The Newcastle-Ottawa Scale (NOS) (21) was utilized to assess the case–control studies, including the study population (4 points) and measurement of exposure factors or results (3 points). The total score of the scale is 9, with scores of ≤ 4, 5–6, and ≥7 indicating low, medium, high quality, respectively. If the two researchers disagree on the evaluation process, they will discuss the decision or seek input from a third party.
Stata 15.0 was used to statistically analyze the data. Risk values for each study were expressed as RR values, with corresponding 95% confidence intervals (CIs) calculated. The heterogeneity test (Q test) and I2 statistics were used to select the appropriate model for calculating the pooled RR. If I2 > 50%, the random-effects model was adopted; if I2 ≤ 50%, the fixed-effects model was applied. For I2 > 50%, we assessed the sensitivity of the literature using the leave-one-out method. Additionally, we assessed publication bias using the Egger test, with a significance level set at 0.05.
By searching the CNKI, Wanfang, VIP, PubMed, Embase, Cochrane Library, and Web of Science databases, 641 documents were initially obtained, 503 documents were retained after removing duplicate documents, 36 articles were preliminarily screened by reading the titles and abstracts, and 11 documents were included after reading the full text. Figure 1 shows the retrieval flowchart.
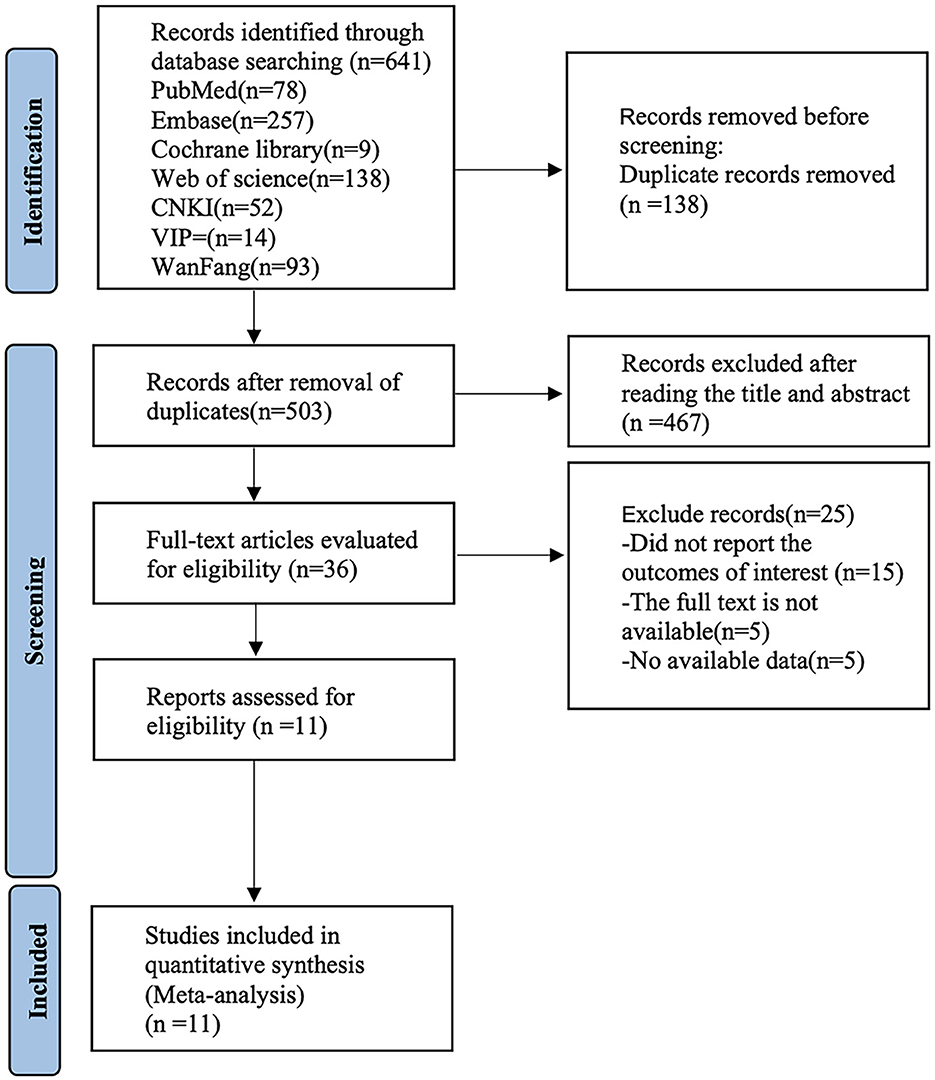
Figure 1. Flow chart of the literature search.
The 11 included (22–32) studies were case–control studies, involving 488 patients with early postoperative seizures and 2,051 patients without early postoperative seizures. The inclusion criteria specified that the age of patients ranged from 7 to 81 years. See Supplementary Table S1 for specific document characteristics. Eleven articles were evaluated using the NOS criteria: one (23) scored 6 points, indicating that the research quality was moderate. The remaining articles scored 7–8 points, and the overall quality of those articles was high. See Supplementary Table S2 for specific quality evaluations.
Eleven studies (22–32) have reported the prevalence of gliomas complicated by early postoperative seizures. The heterogeneity test (I2 = 92.3%, P = 0.001) was conducted based on the random-effects model. It was found that the prevalence of glioma is complicated by early postoperative seizures (ES = 19%, 95% CI [14%−25%]) because the heterogeneity of the indicators was large; therefore, sensitivity analysis was carried out to eliminate them one by one. The analysis results indicated that the sensitivity was low, and the analysis results were stable. The Egger test was performed on the index to evaluate publication bias (P = 0.026), and the prevalence was more likely to indicate publication bias (see Supplementary Figure 1).
Nine studies (22–30) mentioned a history of seizures (defined as tumor-related seizures before surgery) as a risk factor for seizures, and the heterogeneity test (I2 = 24.6%, P = 0.225) was conducted based on the fixed-effects model. The results suggested that a history of seizures was a risk factor for glioma complicated by seizures, and there exists an obvious difference (RR = 1.94, 95% CI [1.76, 2.14], P = 0.001) (see Figure 2 and Supplementary Table S3).
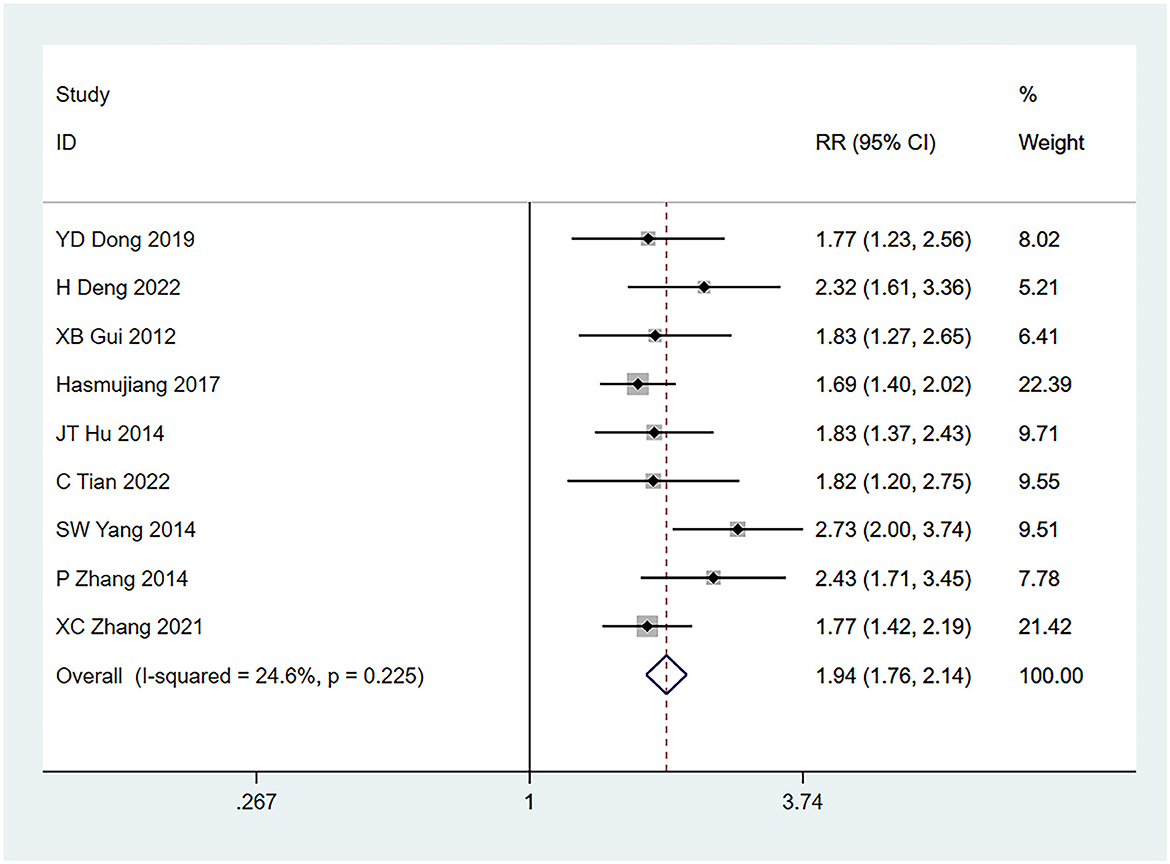
Figure 2. Forest plot of the meta-analysis of seizure history.
Preoperative dyskinesia (22, 25, 30) was mentioned as a risk factor in three studies, and the heterogeneity test (I2 = 89.2%, P = 0.001) was performed based on the random-effects model. It was found that preoperative dyskinesia was a risk factor for glioma complicated by seizures, and there exists an obvious difference (RR = 3.13, 95% CI [1.20, 8.15], P = 0.02) (see Figure 3 and Supplementary Table S3).
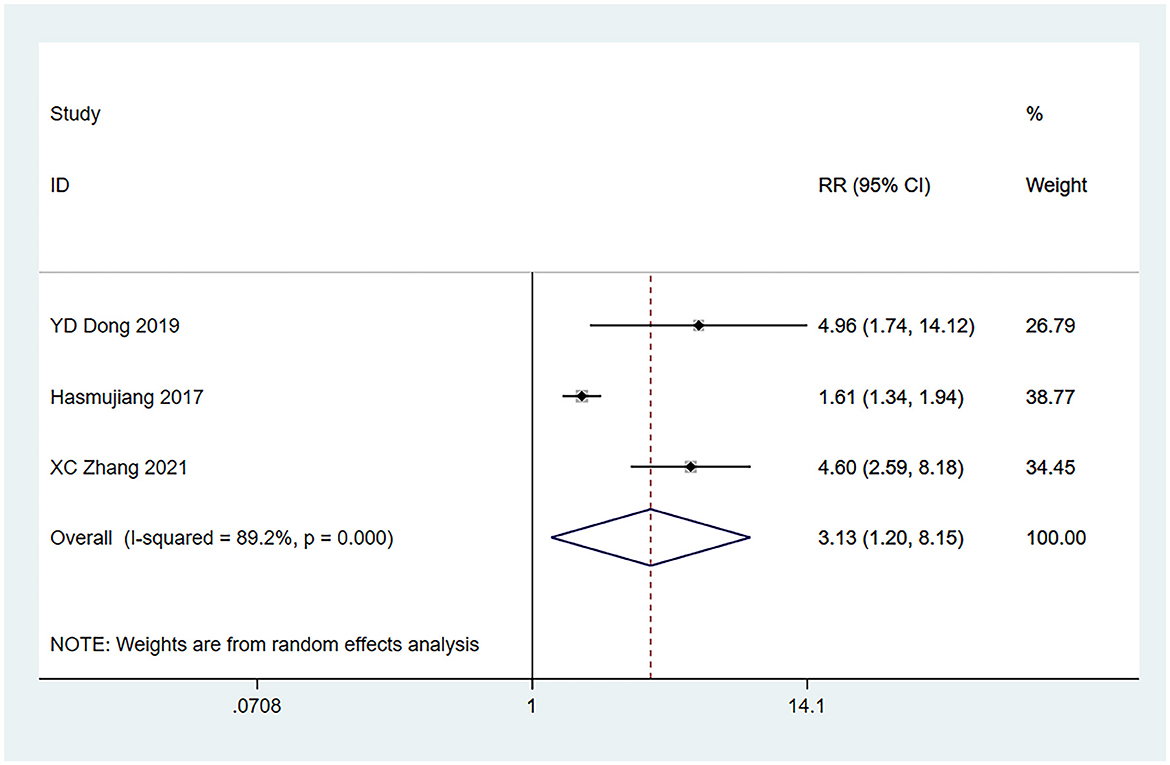
Figure 3. Forest plot of the meta-analysis of preoperative dyskinesia.
Nine studies (22–24, 26–31) identified frontal lobe tumor location as a risk factor for seizures, and the heterogeneity test (I2 = 75.6%, P = 0.001) was performed based on the random-effects model. It was found that frontal lobe tumors were risk factors for glioma complicated with seizures, and there exists an obvious difference (RR = 1.45, 95% CI [1.16, 1.83], P = 0.001), as shown in Figure 4 and Supplementary Table S3.
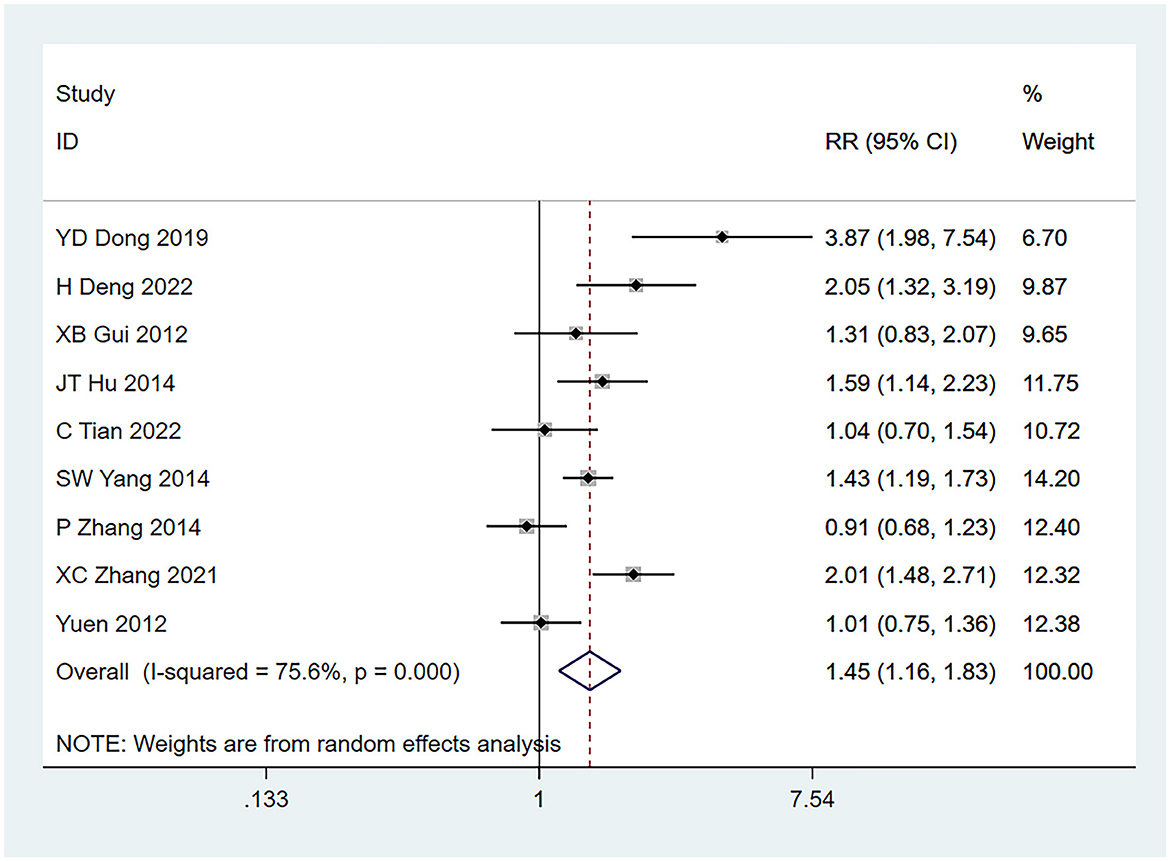
Figure 4. Forest plot of the meta-analysis of frontal lobe tumors.
Eight studies (22–24, 26–30) identified pathological grade ≤ 2 as a risk factor for seizures, and the heterogeneity test (I2 = 85.9%, P = 0.001) was performed based on the random-effects model. The results of the analysis reflected that pathological grade ≤ 2 was a risk factor for tumor-associated seizures and there exist an obvious difference (RR = 1.74, 95% CI [1.13, 2.67], P = 0.012) (see Figure 5 and Supplementary Table S3).
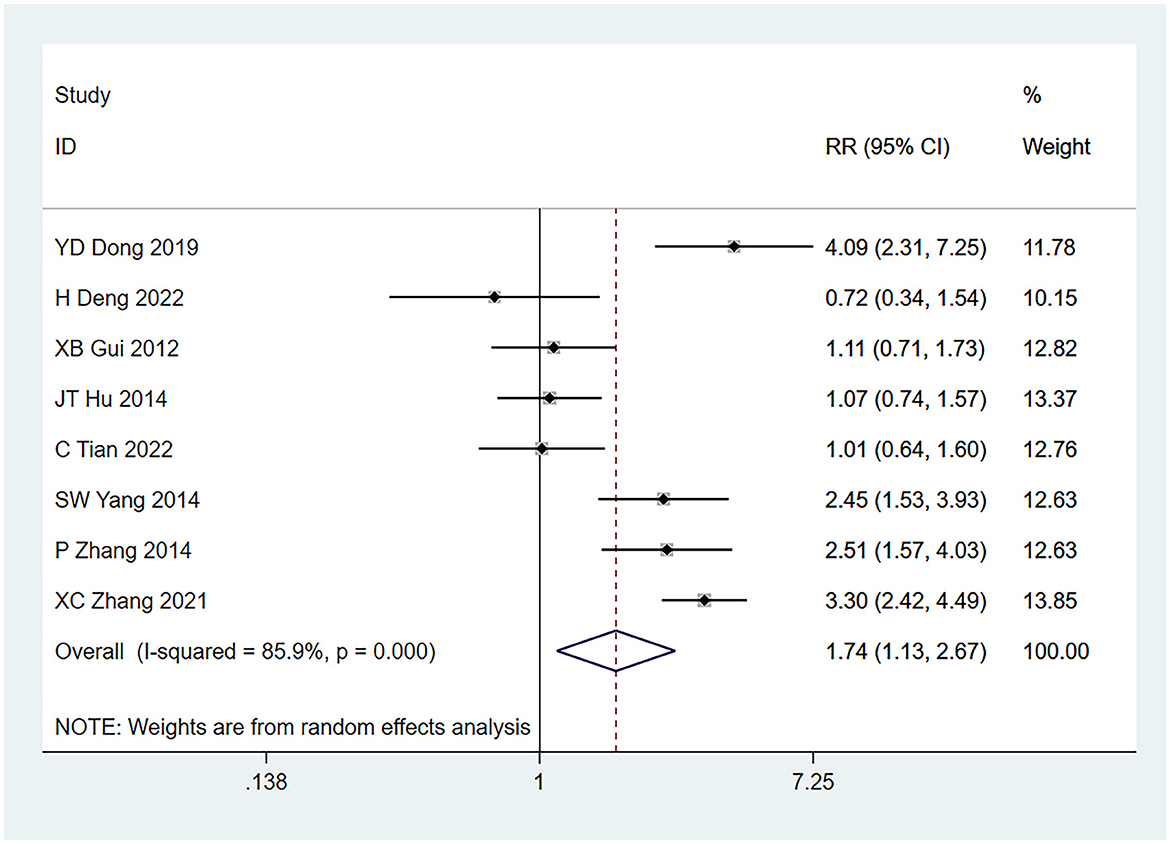
Figure 5. Forest plot of the meta-analysis of pathological grade <2.
Eight studies (22–24, 26–30) mentioned tumors ≥3 cm as a risk factor for seizures, and the heterogeneity test (I2 = 92.4%, P = 0.001) was performed based on the random-effects model. It was found that tumors ≥3 cm were considered a statistically significant risk factor for tumor-associated seizures (RR = 1.70, 95% CI [1.18, 2.45], P = 0.005) (see Figure 6 and Supplementary Table S3).
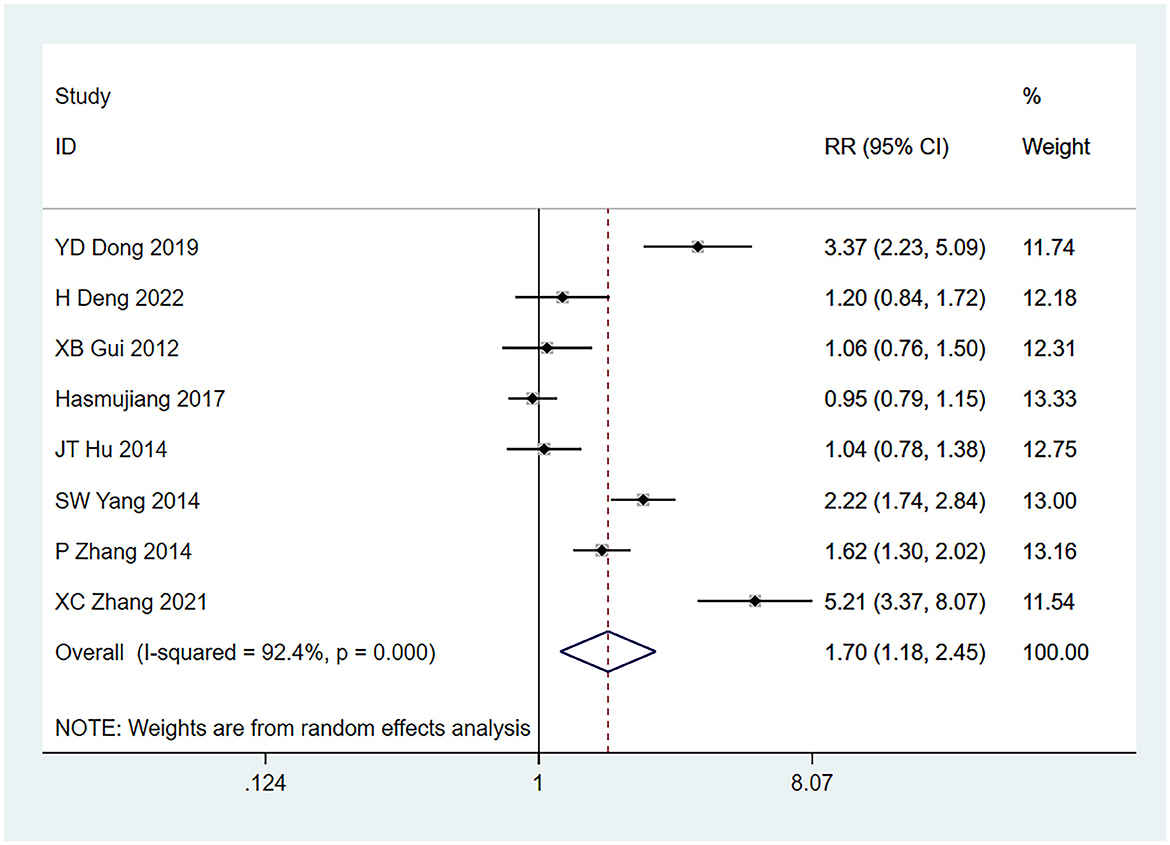
Figure 6. Forest plot of the meta-analysis of tumor >3 cm.
Seven studies (22–24, 26–29) mentioned partial tumor resection as a risk factor, and the heterogeneity test (I2 = 7.7%, P = 0.369) was performed based on the fixed-effects model. It was found that partial tumor resection was a statistically significant risk factor for tumor-associated seizures (RR = 1.60, 95% CI [1.36, 1.88], P = 0.001) (see Supplementary Table S3).
Six studies (22, 23, 25, 27–29) mentioned peritumor edema ≥2 cm as a risk factor for seizures, and the heterogeneity test (I2 = 63.7%, P = 0.017) was performed based on the random-effects model. As a result, peritumor edema ≥2 cm was found to be a statistically significant risk factor for tumor-associated seizures (RR = 1.77, 95% CI [1.40, 2.25], P = 0.001) (see Supplementary Table S3).
Six studies (22, 23, 25, 27–29) mentioned glioma cavity hemorrhage as a risk factor for seizures, and the heterogeneity test (I2 = 83.9%, P = 0.001) was conducted based on the random-effects model. It was found that glioma cavity hemorrhage was a risk factor for tumor-associated seizures, with obvious difference (RR = 3.15, 95% CI [1.85, 5.37], P = 0.001) (see Supplementary Table S3).
Differences in the correlations between male and female sex, circulatory disease, metabolic disease, blurred tumor boundaries, prophylactic medication, and glioma with seizures were not statistically significant (Supplementary Table S3).
The results of the multifactorial analysis mentioned in the research study were analyzed and combined. It was found that there exists an obvious difference in the correlation between frontal lobe tumors, partial tumor resection, prophylactic medication, and tumor-associated seizures. A history of seizures (ES = 2.54, 95% CI [1.24, 5.20], P = 0.011), motor impairment (ES = 2.53, 95% CI (1.83, 3.51), P = 0.001], tumor ≥3 cm (ES = 2.56, 95% CI [1.99, 3.31], P = 0.001), peritumor edema ≥2 cm (ES = 2.53, 95% CI [1.83, 3.51], P = 0.001), and glioma cavity hemorrhage (ES = 2.93, 95% CI (1.79, 4.81), P = 0.001) can be regarded as risk factors for tumor-associated seizures (see Supplementary Table S4).
The publication bias was assessed based on Egger's test for each risk factor. The p-values for each indicator, whether in univariate or multifactorial analysis, were >0.05, indicating no publication bias (see Supplementary Tables S3, S4).
Many recent reports have used the review and meta-analysis to report the prevalence of seizures in patients with glioma. However, Zhang et al. (33) focused their study on assessing the relationship between tumor location and preoperative seizures in patients with glioma, Shan et al. (34) studied the prognostic factors of postoperative glioma and Audrey et al. (35) focused on the incidence of seizures in different glioma types. To the best of our knowledge, this study is the first to explore the risk factors of gliomas complicated by early postoperative seizures using a meta-analysis, the inclusion criteria for the current study differed from those used in all of the previous studies. Through the analysis of single and multiple factors, this study found that a history of seizures is a key risk factor of glioma complicated by seizures, indicating that the risk of seizures in glioma cases with preoperative seizures increased significantly. This may be related to the instability of neuronal membrane potential, decrease in seizure threshold, and abnormal discharge in patients with seizures, which is caused by abnormal and excessive discharge of cortical neurons. Therefore, patients with preoperative seizures should actively use drugs to reduce its occurrence (36). The present study also found an obviously higher occurrence of seizures in patients with dyskinesia in cranial glioma. However, previous literature found that there was no strong correlation between early postoperative epilepsy and dyskinesia (37). This conclusion may be due to the limited number of preoperative dyskinesia cases included in the present research; however, this highlights the need for future studies to pay closer attention to this aspect. Patients with preoperative dyskinesia, which indicates that their neurological function has been damaged to some extent and that they are more prone to epilepsy due to their inability to perform movements, need to be given priority attention to prevent epilepsy. The occurrence of seizures is significantly higher in cases with peri-tumoral edema ≥2 cm. A possible reason for this is that peritumoral edema includes both vasogenic and cytotoxic brain edema. Vasogenic brain edema increases capillary permeability and broken blood–brain barrier, leading to an abnormal distribution of ions inside and outside the cells, which in turn stimulates nerves and triggers seizures (38). In addition, when astrocytes are involved in cytotoxic brain edema due to increased occupancy effects, their ability to take up glutamate is reduced, which in turn affects the stability of the nerve cell membrane, inducing neuroexcitability and ultimately leading to seizures (39). This study also found that intratumoral hemorrhage is an independent risk factor for gliomas complicated by seizures. Intratumoral hemorrhage can cause brain tissue hypoxia and energy metabolism disorders. Iron ions in the blood can catalyze the production of oxygen free radicals, form lipid peroxides, and cause neuronal necrosis, leading to seizures. Therefore, intratumoral hemorrhage is considered a cause of early seizures (40). It has been shown that the tumor pathological grade is usually negatively correlated with early postoperative seizure events, possibly because seizures are characterized by abnormal neuronal firing. As the pathological grade of the glioma increases, infiltrative growth tends to become more pronounced, and this infiltrative growth of tumor cells may destroy projection fibers and neurons, thereby inhibiting the spread of seizure firing (41). This is in line with the previous study, which indicated that a pathological grade of ≤ 2 is an independent risk factor for tumor-associated seizures. For cases with larger tumors, the tumor is more likely to compress adjacent normal brain tissues, causing ischemia and metabolic disorders in the brain. This compression can result in an imbalance of intra- and extra-cellular ion levels, increasing the risk of seizures, which further supports the findings of the present study, indicating that tumors ≥3 cm are an independent risk factor for tumor-associated seizures (42, 43). Telfeian et al. observed that the smaller the size of glioblastoma multiforme, the higher the risk of postoperative seizures. This could be because more brain tissue dissection may be required to reach smaller tumors, thus explaining the higher risk of seizures after surgery for smaller tumors (44). In patients with partially resected gliomas, the residual tumor may continue to invade brain tissues and stimulate the cerebral cortex, leading to abnormal cortical discharges and triggering seizures (45). Therefore, the patient's condition should be considered during clinical treatment, and the tumor should be removed as completely as possible. If complete removal of the tumor is not possible, early prevention and treatment of seizures should be actively pursued before and after surgery to decrease the risk of early postoperative seizures and improve prognosis.
The current study has the following limitations: First, the number of articles included in this review was small, and most of these articles were from China, which may be subject to selection bias. Second, the diagnostic criteria for glioma and seizures used in the included studies were not consistent, which may account for significant heterogeneity. Third, the analysis process of this study did not distinguish between odds ratio (OR), relative risk (RR), or hazard ratio (HR), and although the actual difference between the three is not significant, there is some difference in the risk assessments of the diseases they essentially measure, which may lead to some bias in the results.
Based on the available evidence, history of seizures, dyskinesia, frontal lobe tumors, pathological grade ≤ 2, tumor ≥3 cm, partial tumor resection, peritumor edema ≥2 cm, and glioma cavity hemorrhage are identified as risk factors for early postoperative seizures, and clinical practitioners can combine these indicators for early detection, diagnosis, and intervention in such kind of cases, thereby improving the quality of life of affected individuals.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
BS: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. YS: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. ZW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Writing – original draft. CZ: Investigation, Methodology, Software, Writing – original draft. LY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1356715/full#supplementary-material
Supplementary Material 1. Search history.
Supplementary Table S1. Literature characteristics.
Supplementary Table S2. NOS scores.
Supplementary Table S3. Single-factor meta-analysis.
Supplementary Table S4. Multi-factor meta-analysis.
Supplementary Figure S1. (A) Meta-analysis of the prevalence of glioma complicated with early postoperative seizures; (B) Sensitivity analysis of the prevalence of glioma with early postoperative seizures; (C) Egger's test of the prevalence of glioma complicated with early postoperative seizures.
1. Yan Y, Zeng S, Gong Z, Xu Z. Clinical implication of cellular vaccine in glioma: current advances and future prospects. J Exp Clin Cancer Res. (2020) 39:257. doi: 10.1186/s13046-020-01778-6
2. Lang F, Liu Y, Chou FJ, Yang C. Genotoxic therapy and resistance mechanism in gliomas. Pharmacol Ther. (2021) 228:107922. doi: 10.1016/j.pharmthera.2021.107922
3. Yang K, Wu Z, Zhang H, Zhang N, Wu W, Wang Z, et al. Glioma targeted therapy: insight into future of molecular approaches. Mol Cancer. (2022) 21:39. doi: 10.1186/s12943-022-01513-z
4. Norouzi M. Gold nanoparticles in glioma theranostics. Pharmacol Res. (2020) 156:104753. doi: 10.1016/j.phrs.2020.104753
5. Lin J, Bytnar JA, Theeler BJ, McGlynn KA, Shriver CD, Zhu K. Survival among patients with glioma in the US military health system: a comparison with patients in the Surveillance, Epidemiology, and End Results program. Cancer. (2020) 126:3053–60. doi: 10.1002/cncr.32884
6. Roux A, Boddaert N, Grill J, Castel D, Zanello M, Zah-Bi G, et al. High prevalence of developmental venous anomaly in diffuse intrinsic pontine gliomas: a pediatric control study. Neurosurgery. (2020) 86:517–23. doi: 10.1093/neuros/nyz298
7. Bello-Alvarez C, Camacho-Arroyo I. Impact of sex in the prevalence and progression of glioblastomas: the role of gonadal steroid hormones. Biol Sex Differ. (2021) 12:28. doi: 10.1186/s13293-021-00372-5
8. Berg-Beckhoff G, Schüz J, Blettner M, Münster E, Schlaefer K, Wahrendorf J, et al. History of allergic disease and seizures and risk of glioma and meningioma (INTERPHONE study group, Germany). Eur J Epidemiol. (2009) 24:433–40. doi: 10.1007/s10654-009-9355-6
9. Douw L, de Groot M, van Dellen E, Aronica E, Heimans JJ, Klein M, et al. Local MEG networks: the missing link between protein expression and seizures in glioma patients? Neuroimage. (2013) 75:195–203. doi: 10.1016/j.neuroimage.2013.02.067
10. Armstrong TS, Grant R, Gilbert MR, Lee JW, Norden AD. Seizures in glioma patients: mechanisms, management, and impact of anticonvulsant therapy. Neuro Oncol. (2016) 18:779–89. doi: 10.1093/neuonc/nov269
11. Yamagata A, Fukai S. Insights into the mechanisms of seizures from structural biology of LGI1-ADAM22. Cell Mol Life Sci. (2020) 77:267–74. doi: 10.1007/s00018-019-03269-0
12. Schlehofer B, Blettner M, Moissonnier M, Deltour I, Giles GG, Armstrong B, et al. Association of allergic diseases and seizures with risk of glioma, meningioma and acoustic neuroma: results from the INTERPHONE international case-control study. Eur J Epidemiol. (2022) 37:503–12. doi: 10.1007/s10654-022-00843-y
13. Fang S, Li L, Weng S, Guo Y, Fan X, Jiang T, et al. Altering patterns of sensorimotor network in patients with different pathological diagnoses and glioma-related seizures under the latest glioma classification of the central nervous system. CNS Neurosci Ther. (2023) 29:1368–78. doi: 10.1111/cns.14109
14. Avila EK, Chamberlain M, Schiff D, Reijneveld JC, Armstrong TS, Ruda R, et al. Seizure control as a new metric in assessing efficacy of tumor treatment in low-grade glioma trials. Neuro Oncol. (2017) 19:12–21. doi: 10.1093/neuonc/now190
15. de Bruijn M, van Sonderen A, van Coevorden-Hameete MH, Bastiaansen AEM, Schreurs MWJ, Rouhl RPW, et al. Evaluation of seizure treatment in anti-LGI1, anti-NMDAR, and anti-GABA(B) R encephalitis. Neurology. (2019) 92:e2185–96. doi: 10.1212/WNL.0000000000007475
16. van der Meer PB, Dirven L, Fiocco M, Vos MJ, Kouwenhoven MCM, van den Bent MJ, et al. First-line antiepileptic drug treatment in glioma patients with seizures: levetiracetam vs valproic acid. Epilepsia. (2021) 62:1119–29. doi: 10.1111/epi.16880
17. Giraldi L, Vinsløv Hansen J, Wohlfahrt J, Fugleholm K, Melbye M, Munch TN. Postoperative de novo seizures after craniotomy: a nationwide register-based cohort study. J Neurol Neurosurg Psychiatry. (2022) 93:436–44. doi: 10.1136/jnnp-2021-326968
18. Koekkoek JA, Dirven L, Taphoorn MJ. The withdrawal of antiepileptic drugs in patients with low-grade and anaplastic glioma. Expert Rev Neurother. (2017) 17:193–202. doi: 10.1080/14737175.2016.1219250
19. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. (2009) 6:e1000100. doi: 10.1371/journal.pmed.1000100
20. Jiang T, Nam DH, Ram Z, Poon WS, Wang J, Boldbaatar D, et al. Clinical practice guidelines for the management of adult diffuse gliomas. Cancer Lett. (2021) 499:60–72. doi: 10.1016/j.canlet.2020.10.050
21. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–5. doi: 10.1007/s10654-010-9491-z
22. Dong Y, Peng B, Luo D, Song Q. Risk factors for early epileptic seizures after brain glioma surgery. Chin J Microinv Neurosurg. (2019) 24: 204–7.
23. Deng H, Hu J, Liu J, Zhu W, Hu J. Risk factors for early postoperative seizures in patients with glioma. Med Equip. (2022) 35: 97–9.
24. Gui X, Fu X, Niu C, Qian R, Yao Y, Zhu S, et al. Risk factors of early epileptic seizure after supratentorial glioma surgery. J Stereot Funct Neurosurg. (2012) 25: 287–90.
25. Hasmujiang R, Yang X. Analysis of the status quo and risk factors of seizures in early stage after brain glioma surgery. Cancer Prog. (2017) 15: 947–9.
26. Hu J, Lv Y-X, Wang H, Tu H, Li X, Hu S, et al. Analysis of influencing factors of seizures after brain glioma surgery. Shaanxi Med J. (2014) 4:471–3.
27. Tian C, Wu R, Zhang X, Yu Y. Analysis of related influencing factors of epileptic seizure after craniocerebral glioma surgery. China Med J. (2022) 57: 1337–40.
28. Yang S, Xia L, Gao C, Xie Y, Wang A, Dong Developed. Analysis of risk factors for early epileptic seizure after brain glioma surgery. Chin J Appl Neurol Dis. (2015) 24:24–6.
29. Zhang P, Lu Y. Analysis of related factors of early epileptic seizure after brain glioma surgery. Chin J Appl Neurol Dis. (2014) 7:68–70.
30. Zhang X, Ma J, Zhu C, Yu Q, Chen K, Jiang J. Logistic regression analysis of risk factors associated with early epileptic seizure after brain glioma surgery. Cancer Prev Treatment. (2021) 34: 138–42.
31. Yuen TI, Morokoff AP, Bjorksten A, D'Abaco G, Paradiso L, Finch S, et al. Glutamate is associated with a higher risk of seizures in patients with gliomas. Neurology. (2012) 79:883–9. doi: 10.1212/WNL.0b013e318266fa89
32. Yu Z, Zhang N, Hameed NUF, Qiu T, Zhuang D, Lu J, et al. The analysis of risk factors and survival outcome for Chinese patients with seizures with high-grade glioma. World Neurosurg. (2019) 125:e947–57. doi: 10.1016/j.wneu.2019.01.213
33. Falco-Walter J. Seizures-definition, classification, pathophysiology, and epidemiology. Semin Neurol. (2020) 40:617–23. doi: 10.1055/s-0040-1718719
34. Specchio N, Wirrell EC, Scheffer IE, Nabbout R, Riney K, Samia P, et al. International league against seizures classification and definition of seizures syndromes with onset in childhood: position paper by the ilae task force on nosology and definitions. Epilepsia. (2022) 63:1398–442. doi: 10.1111/epi.17241
35. Reddy C, Saini AG. Metabolic seizures. Indian J Pediatr. (2021) 88:1025–32. doi: 10.1007/s12098-020-03510-w
36. Leone MA, Ivashynka AV, Tonini MC, Bogliun G, Montano V, Ravetti C, et al. Risk factors for a first epileptic seizure symptomatic of brain tumour or brain vascular malformation. A case control study. Swiss Med Wkly. (2011) 141:w13155. doi: 10.4414/smw.2011.13155
37. Fang S, Li Y, Wang Y, Zhang Z, Jiang T. Awake craniotomy for gliomas involving motor-related areas: classification and function recovery. J Neurooncol. (2020) 148:317–25. doi: 10.1007/s11060-020-03520-w
38. Gao A, Yang H, Wang Y, Zhao G, Wang C, Wang H, et al. Radiomics for the prediction of seizures in patients with frontal glioma. Front Oncol. (2021) 11:725926. doi: 10.3389/fonc.2021.725926
39. Mader MM, Deuter D, Sauvigny T, Borchert P, Faizy TD, Bester M, et al. Diffusion tensor imaging changes in patients with glioma-associated seizures. J Neurooncol. (2022) 160:311–20. doi: 10.1007/s11060-022-04139-9
40. Zhang R, Xu X, Zhou H, Yao D, Wei R, Muhammad S. Pediatric angiocentric glioma with acute intracerebral hemorrhage: a case report with 36 months follow-up. Surg Neurol Int. (2021) 12:499. doi: 10.25259/SNI_791_2021
41. Luyken C, Blümcke I, Fimmers R, Urbach H, Elger CE, Wiestler OD, et al. The spectrum of long-term seizures-associated tumors: long-term seizure and tumor outcome and neurosurgical aspects. Epilepsia. (2003) 44:822–30. doi: 10.1046/j.1528-1157.2003.56102.x
42. Slegers RJ, Blumcke I. Low-grade developmental and seizures associated brain tumors: a critical update 2020. Acta Neuropathol Commun. (2020) 8:27. doi: 10.1186/s40478-020-00904-x
43. Métais A, Appay R, Pagès M, Gallardo C, Silva K, Siegfried A, et al. Low-grade seizures-associated neuroepithelial tumours with a prominent oligodendroglioma-like component: the diagnostic challenges. Neuropathol Appl Neurobiol. (2022) 48:e12769. doi: 10.1111/nan.12769
44. Telfeian AE, Philips MF, Crino PB, Judy KD. Early postoperative seizures in patients undergoing craniotomy for glioblastoma multiforme. J Exp Clin Cancer Res. (2001) 20:5–10.
Keywords: glioma, seizures, risk factors, meta-analysis, systematic review
Citation: Sun B, Sun Y, Wang Z, Zhao C and Yang L (2024) Prevalence and risk factors of early postoperative seizures in patients with glioma: a systematic review and meta-analysis. Front. Neurol. 15:1356715. doi: 10.3389/fneur.2024.1356715
Received: 16 December 2023; Accepted: 05 March 2024;
Published: 20 March 2024.
Edited by:
Peter C. Reinacher, Freiburg University Medical Center, GermanyReviewed by:
Meihua Yang, Army Medical University, ChinaCopyright © 2024 Sun, Sun, Wang, Zhao and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liang Yang, am9qb183QDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.