
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 08 March 2024
Sec. Headache and Neurogenic Pain
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1355877
 Pablo Irimia1*
Pablo Irimia1* Sonia Santos-Lasaosa2
Sonia Santos-Lasaosa2 Patricia Pozo-Rosich3,4Rogelio Leira5Julio Pascual6
Patricia Pozo-Rosich3,4Rogelio Leira5Julio Pascual6 José Miguel Láinez7
José Miguel Láinez7Eptinezumab, a monoclonal antibody that targets calcitonin gene-related peptide (CGRP), was recently approved in Europe for the prophylactic treatment of migraine in adults who have at least four migraine days a month. Eptinezumab is administered by intravenous infusion every 12 weeks. During recent months, a considerable amount of evidence from eptinezumab trials has been published. The aim of this review is to describe the existing evidence on the tolerability, safety and efficacy of eptinezumab in patients with migraine. Data from randomized (PROMISE-1, PROMISE-2, RELIEF and DELIVER) and open-label (PREVAIL) phase 3 clinical trials have demonstrated the favorable effect of eptinezumab in migraine symptoms from first day of treatment. These studies showed that eptinezumab results in an overall reduction in mean monthly migraine days (MMDs), increases in the ≥50% and ≥ 75% migraine responder rates (MRRs) and improvements in patient-reported outcome measures in both patients with episodic migraine (EM) and with chronic migraine (CM), including patients who failed previous preventive treatments. The RELIEF trial also showed that eptinezumab, within 2 h of administration, reduced headache pain, migraine-associated symptoms and acute medication use when administered during a migraine attack. Eptinezumab benefits manifested as early as day 1 after dosing and with the subsequent doses lasted up to at least 2 years. Treatment-emergent adverse events reported by ≥2% of patients included upper respiratory tract infection and fatigue. Current evidence demonstrates that eptinezumab has a potent, fast-acting, sustained migraine preventive effect in patients with EM and CM. Eptinezumab has also shown to be well tolerated, supporting its use in the treatment of patients with migraine and inclusion in the current migraine therapeutic options.
Migraine is a chronic neurological disorder that affects approximately 15% of the world’s population, with certain European countries presenting the highest prevalence rates (1, 2). Patients with migraine suffer recurring attacks of headache and other symptoms (including nausea, vomiting, phonophobia and photophobia) lasting approximately 4 to 72 h (3). Migraine impairs the physical, psychological and social well-being of patients, both during attacks and on migraine-free days (‘interictal’), and substantially reduces their ability to work or go to school and their health-related quality of life (HRQoL) (4–6). The burden of migraine is not only placed on patients and their families but also on society at large.
The International Classification of Headache Disorders 3 (ICHD-3) criteria defines chronic migraine (CM) as ≥15 days with migraine per month [d/mo] where at least 8 of those have migraine features for at least 3 months (7, 8). Both episodic migraine (EM) and CM can be treated using acute and/or preventive therapies. Drugs targeting the calcitonin gene-related peptide (CGRP), a peptide involved in migraine pain generation that is released by the trigemino-vascular system during migraine attacks, have emerged during the last decade. These anti-CGRP agents have demonstrated benefits for the preventive treatment of EM and CM (9–12) and a more favorable benefit–risk ratio than established treatments (13). Eptinezumab is a potent monoclonal antibody targeting the circulating CGRP, administered by intravenous (IV) infusion (14). Eptinezumab has shown to be effective and safe during the clinical development program, leading to the approval, in February 2020 in the United States and in January 2022 in Europe, of the 100 mg and 300 mg doses for the prophylactic treatment of migraine in adults with at least 4 migraine days per month (15, 16).
During recent months, a large number of results from post-hoc analyses of data from eptinezumab pivotal trials (17, 18) has been published (19–30), together with primary and post-hoc results from the DELIVER trial (31–34). Also, numerous clinical trials on eptinezumab are currently being conducted (35–42). This article provides an updated narrative review of eptinezumab evidence in EM and CM and a summary of the ongoing trials. To this end, a systematic search for articles, abstracts, and poster presentations, published prior to 12th May 2023 was conducted on PubMed (U.S. National Library of Medicine), using the terms ‘eptinezumab’ and ‘ALD403’. We filtered by article type (clinical trials, randomized clinical trials and meta-analysis were included; books and documents, reviews and systematic reviews were excluded), and a total of 48 articles emerged (35 publications of results from clinical trials, including post-hoc analysis, and 13 meta-analysis). Ongoing studies were searched on clinicaltrials.gov (U.S. National Library of Medicine) using the term ‘eptinezumab’; the search resulted in 109 ongoing studies. Further publications were revised and included to provide context.
In this narrative review, we provide results of the efficacy and safety of the doses of eptinezumab that have been tested, with a special focus on the 100-mg dose, since it is the dose recommended by the health authorities. Results for the primary endpoint and key secondary endpoints of each study are presented. This review aims to build upon existing reviews of eptinezumab (43–45) by providing updated information from recently published studies and offering a detailed description of ongoing research.
Eptinezumab is the only antibody targeting the CGRP pathway with an intravenous route of administration. Pharmacokinetic analyses (46) showed that the maximum concentration (Cmax) was immediate (i.e., 30 min after the start of a 30-min administration), which might provide an explanation for the fast onset of eptinezumab effect (46, 47), and contrasts with longer median values (4–14 days) of subcutaneous (SC) anti-CGRP (48–50). The eptinezumab elimination half-life of 27 days and the low exposure metrics required to achieve 90% of the maximal efficacy (EC90) supports its administration every 12 weeks. Its clearance (0.15 L/day) and volume of distribution (3.64 L) were consistent with other monoclonal antibodies. Age, sex, race, immunogenicity and concomitant preventive treatments only caused small changes in pharmacokinetics, and dose adjustments are not required.
In terms of route of administration, IV infusions have shown higher Cmax than SC and intramuscular administrations (47). The rapid attainment of high plasma concentrations with the IV administration together with the good tolerability (even when co-administered with SC sumatriptan) and low immunogenicity, supported the administration of eptinezumab as IV infusions (47).
The immediate, effective and sustained effect of eptinezumab can be explained by its structure and binding properties. The attributes of the fragment antigen-binding (Fab) region and the conformational changes that occur upon eptinezumab binding to CGRP create a ‘latch-and lock’ mechanism. This mechanism hampers its dissociation (51), increases the specificity and durability of its effect, and probably underlie the sustained migraine preventive effect.
The efficacy and safety of eptinezumab in the prevention of migraine was evaluated in five large-scale phase 3 clinical trials: four randomized clinical trials (PROMISE-1, PROMISE-2, RELIEF, and DELIVER) and one open-label trial (PREVAIL). In this section, efficacy findings from these clinical trials and subsequent post-hoc analysis from these studies have been summarized. We report findings of studies including patients with EM only, followed by studies including patients only with CM, and then including both. Figure 1 displays the primary and key secondary efficacy endpoints of the phase 3 trials. Tolerability and safety data are reported in the next section of this article (see Tolerability and safety).
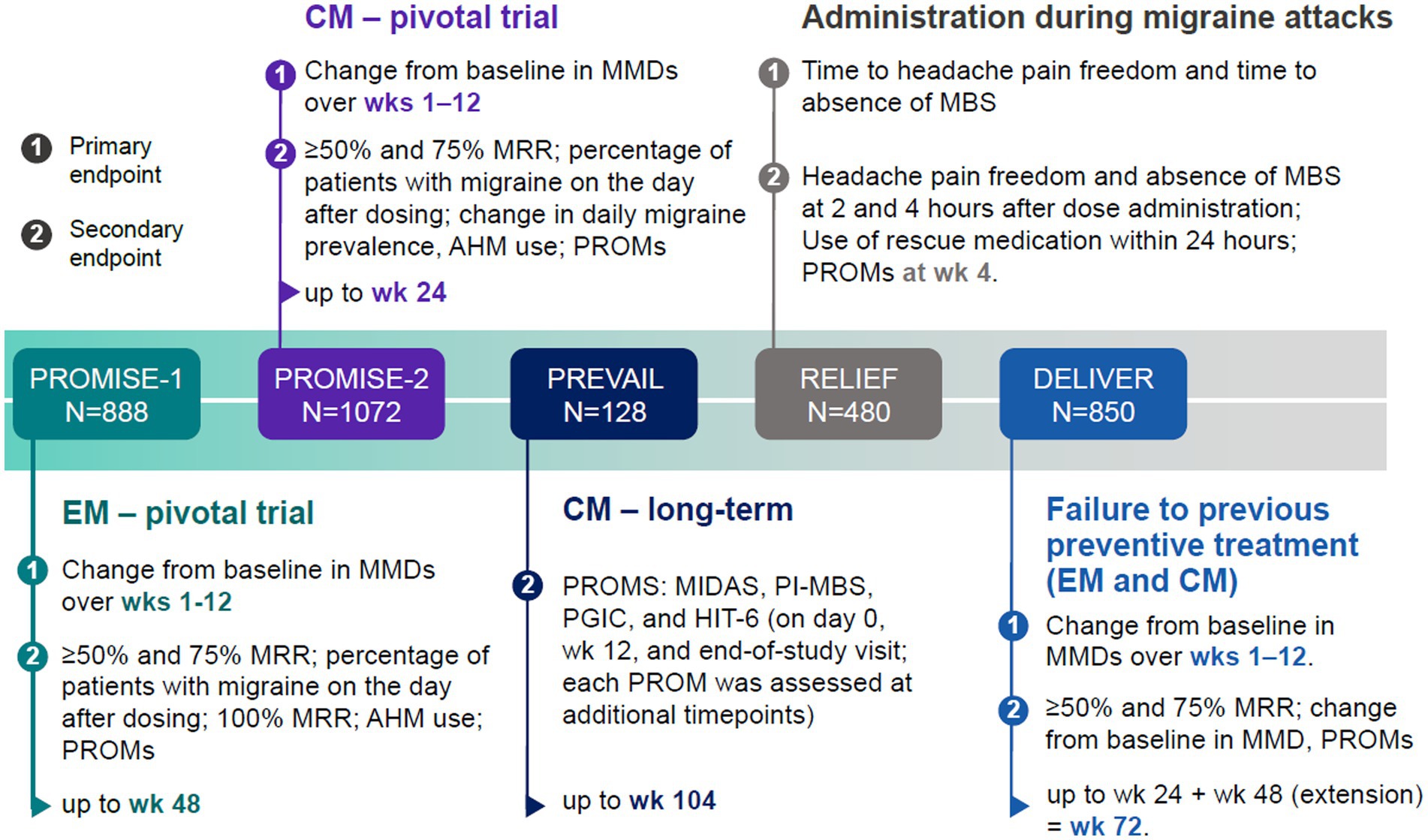
Figure 1. Primary and key secondary efficacy endpoints in eptinezumab phase 3 clinical trials. Primary (1) and main secondary (2) efficacy endpoints in eptinezumab clinical trials included (i) change from baseline in monthly migraine days (MMDs), (ii) ≥50% or ≥ 75% migraine responder rate (MRR), defined as the proportion of patients who achieved a ≥ 50% or ≥ 75% reduction in average MMDs at a specific week from their baseline, (iii) percentage of patients with a migraine on the day after dosing, and (iv) patient-reported outcome measures (PROMs) on disability, function, and health-related quality of life (HRQoL), among others. The number of migraine days was recorded using an electronic diary (eDiary). In the RELIEF trial, patients experiencing migraine on 4–15 days per month in the 3 months prior to screening were included. AHM, acute headache medication; CM, chronic migraine; EM, episodic migraine; MBS, most bothersome symptoms.
PROMISE-1 was a phase 3, multicenter, randomized, double-blind, placebo-controlled, parallel-group trial (18). Adults (n = 888) with EM were randomly assigned in a 1:1:1:1 ratio to receive eptinezumab 30, 100, 300 mg, or placebo for up to 48 weeks (four doses in total). Acute headache medication (AHM) was limited to ≤14 d/mo, and preventive treatment was not allowed, except for menstrual migraines. Mean monthly migraine days (MMDs) were significantly reduced from baseline (≈8.6) over weeks 1–12 compared to placebo in the 100 mg (−3.9; p = 0.0182) and 300 mg groups (−4.3; p = 0.0001). Efficacy was maintained up to week 48 (year 1), with a significant reduction in the MMDs after the second (weeks 13–24), third (weeks 25–36), and fourth (weeks 37–48) infusions (52). Overall, the percentage of patients with a ≥ 50% or ≥ 75% reduction in MMDs up to week 48 was higher with eptinezumab than with placebo. Eptinezumab-treated patients were more likely to achieve ≥50% and ≥ 75% migraine response during weeks 1–48 than placebo, except for the ≥75% migraine responder rate (MRR) which was similar (≈39%) for the 100 mg and placebo groups for weeks 37–48. Results of MMDs and MRRs from the PROMISE studies for the 100 mg dose are shown in Table 1.
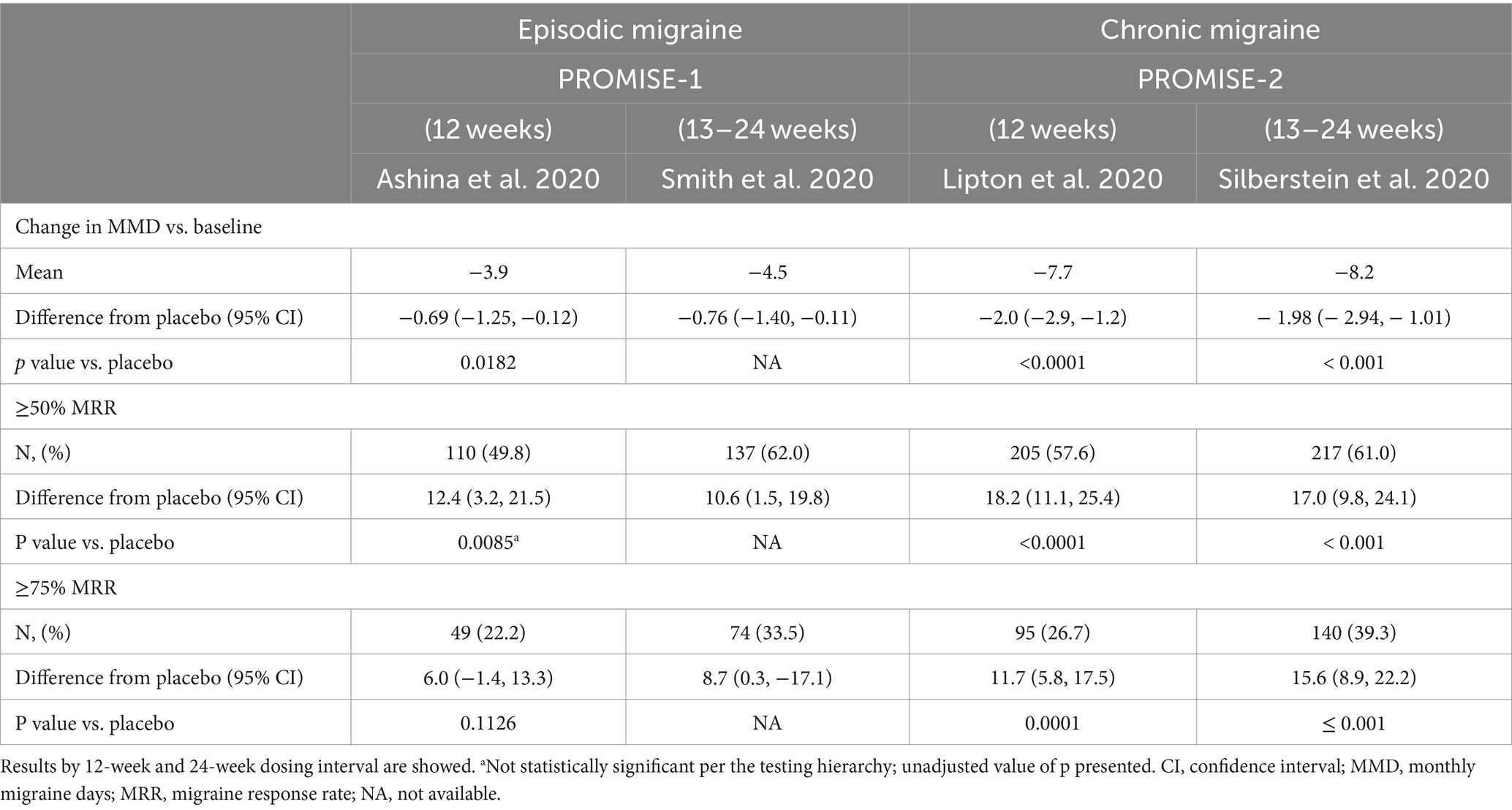
Table 1. Summary of efficacy results of eptinezumab 100 mg from the phase III PROMISE-1 and -2 trials.
The migraine preventive effect of eptinezumab in patients with EM was observed on the first day after the infusion (18, 53). The average percentage of patients with a migraine on any given day at baseline (30.7%) was significantly reduced on day 1 with the 100-mg dose (14.8%; p = 0.0312) and the 300-mg dose (13.9%, p = 0.0159) compared with placebo (22.5%), entailing a > 50% reduction compared to baseline. The mean number of MMDs on day 1 was −4.5 with 100 mg (p = 0.021) and − 4.7 (p = 0.010) with the 300 mg (53). However, it should be acknowledged that the specific assumptions made by the researchers for evaluating this endpoint represent a limitation. The study normalized measures to a 28-day month to facilitate comparison with MMDs, based on the assumption of a consistent migraine rate over this period, which may not be entirely acceptable in clinical practice.
Eptinezumab also reduced AHM use from weeks 1–4 up to week 24, especially in patients with higher baseline use, and improved HRQoL in three domains of the Short-Form Health Survey (SF-36; bodily pain, physical role-functioning, and social role-functioning) after 1 year (52).
PROMISE-2 was a phase 3, multicenter, randomized, double-blind, placebo-controlled, parallel-group trial (17). Adults with CM (n = 1,072) were randomly assigned in a 1:1:1 ratio to receive eptinezumab 100, 300 mg, or placebo every 12 weeks for up to 24 weeks (two infusions in total). Use of barbiturates or prescription opioids were allowed ≤4 d/mo if use was stable for ≥2 months. Other AHM such as triptans, nonsteroidal anti-inflammatory drugs, and simple analgesics were not restricted. The reduction in MMDs from weeks 1–12 was statistically significant for eptinezumab doses of 100 (−7.7; p < 0.0001) and 300 mg (−8.2; p < 0.0001) compared to placebo (−5.6). Patients receiving eptinezumab were more likely than the placebo group to achieve ≥50% and ≥ 75% migraine response during weeks 1–12 (see Table 1).
As observed in patients with EM (18), eptinezumab also had a migraine-preventive effect on day one after dosing in patients with CM (17). The average percentage of patients with a migraine on any given day at baseline (58%) was significantly reduced on the first day after administering 100 mg (−50.3%; p < 0.0001) and 300 mg (−51.6%; p < 0.0001) of eptinezumab, but not placebo (−21.7%). Patients using eptinezumab vs. placebo reported greater improvements in the ability to function (measured by the 6-item Headache Impact Test; HIT-6) and higher reductions in AHM use from baseline to week 12 (17).
Results through 24 weeks of treatment showed that the reductions in MMDs observed with the first dose (17) continued to improve after the second dose (−8.2 days with 100 mg and − 8.8 with 300 mg, vs. −6.2 with placebo, p < 0.0001) (54). The ≥50% and ≥ 75% MRRs also increased after the second dose (54). The percentage of patients with no migraine for a 4-week interval (from week 13 to 24) was higher in the eptinezumab groups (100 mg: 17.8%; 300 mg: 20.8%) than in the placebo group (9.3%). Both doses further reduced AHM days from baseline to up to week 24 (difference from placebo: − 1.1 days with 100 mg; −1.7 days with 300 mg).
Health authorities have suggested including the assessment of most bothersome symptoms (MBS) as an endpoint in clinical trials evaluating migraine treatment (55). In line with this recommendation and considering that MBS vary from person to person, individual MBS were secondarily assessed in the PROMISE-2 study (56). Patients were asked to self-report their MBS in an open-ended question (patient-identified MBS, PI-MBS) at screening and to rate the overall change in their severity during subsequent visits. At week 4, a higher percentage of eptinezumab-treated patients reported much or very much improvement in their PI-MBS (100 mg, 45%; 300 mg, 57%) compared to placebo (29%). Improvements in PI-MBS continued at week 12 (100 mg, 53%; 300 mg, 61%; placebo, 34%), and were sustained up to week 32. A post-hoc analysis showed that improvements in PI-MBS correlated with changes in MMDs and other patient-reported outcome measures (PROMs), such as HIT-6, Patient Global Impression of Change [PGIC], SF-36, and EuroQol-5-dimension visual analog scale (EQ-5D-5L VAS) at week 12 (20). PI-MBS improvement predicted better outcomes across all PROMs in addition to change in the MMDs (p < 0.003) (20). PI-MBS, thus, appear to be a clinically useful patient-centered measure for evaluating the effect of preventive treatments in those aspects more disturbing to each individual.
Several post-hoc analyses of data from clinical trials further exhibited eptinezumab efficacy in alleviating CM (Table 2). Buse et al. (19) assessed the consistency and predictive ability of migraine response during month 1 on later response, by using data from the PROMISE-2 study. During month 1, more eptinezumab-treated than placebo-treated patients were ≥ 75% MRR (100 mg, 30.9%; 300 mg, 36.9%; placebo, 15.6%) and had improvements in the PGIC scores (100 mg, 46%; 300 mg, 58.7%; placebo 32.4%). Among ≥75% migraine responders at month 1, the ≥75% MRR for the five subsequent months was higher in the eptinezumab groups (100 mg, 41.8%; 300 mg, 46.5%) than in the placebo group (36.8%). PGIC scores at month 1 predicted scores at month 6, with more than 80% of the patients who obtained very much improved rates at month 1 obtaining very much improved or much improved scores at month 6 (100 mg, 82.9%, 300 mg, 86.4%; placebo, 81.5%). Overall, patients who benefited from eptinezumab the first month had consistent benefits during the following months, suggesting that early response can predict sustained response.
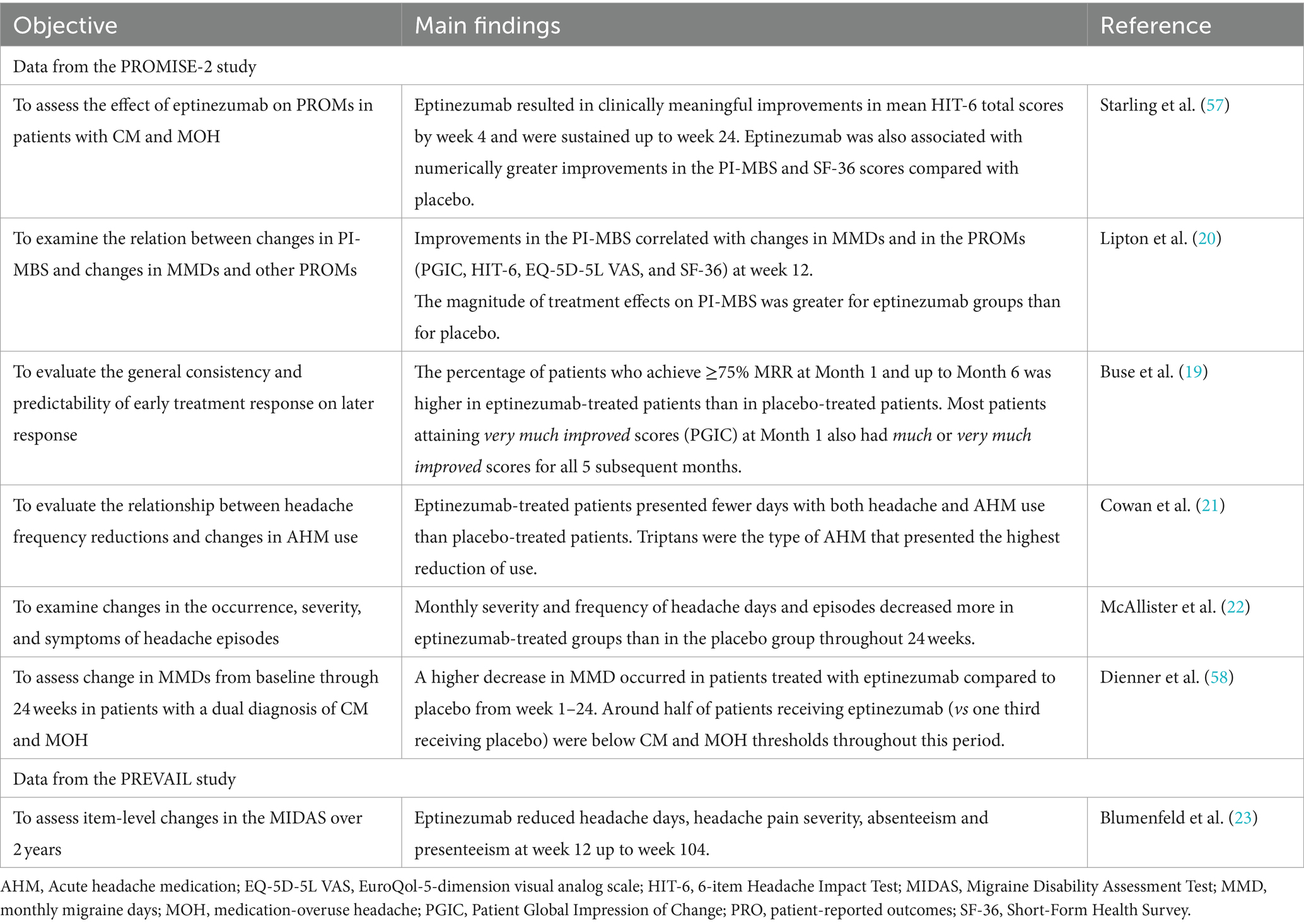
Table 2. Post-hoc analysis of clinical trials in CM.
Forty percent (n = 431) of patients in the PROMISE-2 study had medication-overuse headache (MOH), a secondary headache resulting from the overuse of analgesics or other medication to alleviate acute migraine attacks. Subgroup analyses in these patients with dual diagnosis of CM and MOH were conducted (57–59). Greater mean changes from baseline in MMDs were observed for eptinezumab 300 mg during week 1 through 12, compared with placebo (p < 0.0001) and the changes were sustained up to week 24 (58). Approximately half and one-third of eptinezumab-treated patients experienced ≥50% and ≥ 75% migraine response, respectively, as early as weeks 1 and up to week 24, compared with one-third and one-sixth of placebo patients, respectively. Fewer patients had a migraine on day 1 in eptinezumab groups (27.8%, 100 mg; 30.1%, 300 mg), than in the placebo group (45.5%). Slightly more than half of patients (51.1%, 100 mg; 54.4%, 300 mg) receiving eptinezumab were below the diagnostic thresholds for CM for 24 weeks, compared with one third (32.4%) of patients receiving placebo. Similar percentages were observed on the use of AHM below the diagnostic thresholds for MOH (50.5%, 100 mg; 49.5%, 300 mg; 27.1%, placebo), suggesting resolution of both diagnoses in half of the treated patients. Over 24 weeks, monthly AHM use almost halved. Eptinezumab also numerically increased the percentage of patients who were below ICHD-3 diagnostic thresholds for CM and MOH (59). These results suggest that patients with CM and MOH could have their MOH managed with eptinezumab, without requiring withdrawal from pharmacological treatment.
The association between reductions in headache frequency and changes in AHM use was specifically tested in another subanalysis (21). Three subgroups of CM patients were considered: total population, patients with MOH, and patients with MOH who were ≥ 50% responders during treatment (weeks 1–24). In the three subgroups, the proportion of days with both headache and AHM use decreased more in eptinezumab-treated patients compared to placebo-treated patients (total population: 25.1% vs. 17.0%; MOH subgroup: 29.2% vs. 18.4%; MOH with ≥50% response subgroup: 38.3% vs. 31.5%). Triptans were the type of AHM that presented the highest reduction of use during treatment.
McAllister et al. showed that eptinezumab not only steadily decreased migraine and headache frequency, but also severity, with the remaining headache episodes being less severe (post-hoc analysis of the PROMISE-2) (22). This reduction in headache frequency and severity was maintained up to week 104 by post-hoc analysis of another phase 3 trial (see Safety section for a full description of the PREVAIL study); these analysis also revealed that absenteeism and presenteeism decreased during this two-year period as well (23).
The efficacy of eptinezumab treatment separately observed in either EM or CM was further confirmed with a broader spectrum of migraine patients (Figure 2). Here, we report the main results of post-hoc analyses of pooled data of the PROMISE-1 and -2 studies and findings from the RELIEF and DELIVER trials.
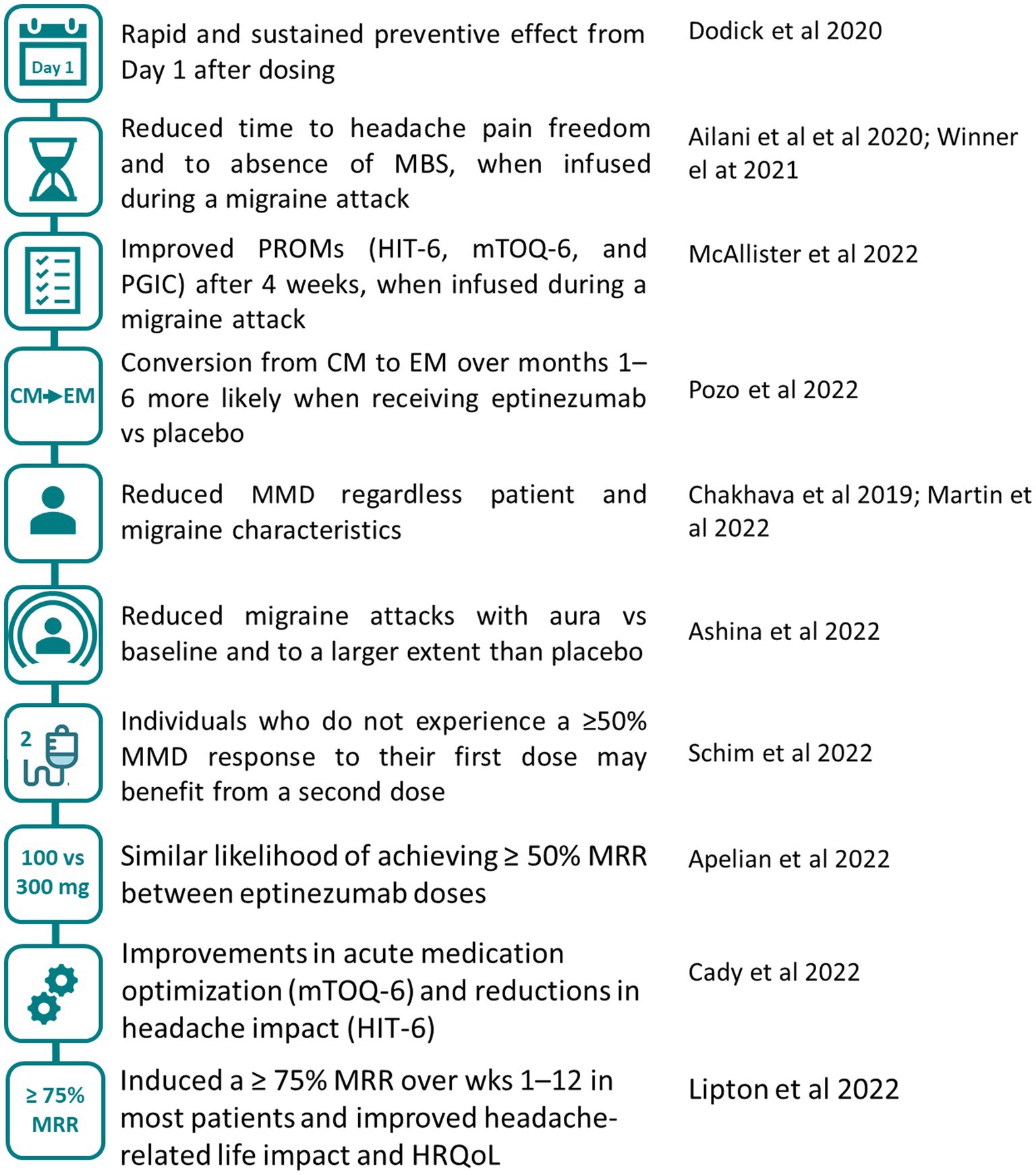
Figure 2. Effect of eptinezumab on migraine (EM and CM). Main conclusions regarding eptinezumab efficacy from post-hoc analysis that pooled patients from the pivotal trials (26–30, 53, 60, 61) and from studies that included patients with migraine 4–15 d/mo (24, 25, 62, 63). HIT-6, 6-item Headache Impact Test; HRQoL, health-related quality of life; MMD, monthly migraine days; MRR, migraine response rate; mTOQ-6, 6-item migraine Treatment Optimization Questionnaire; PGIC, Patient Global Impression of Change; PROMs, patient-reported outcome measures.
The efficacy of eptinezumab on the first day following infusion observed on EM (18, 64) or CM (17, 65) separately was further confirmed when data from these trials was pooled and analyzed together (53). Moreover, the value attributed by patients to the reduction in the likelihood of migraine on day 1 after infusion was tested by an online survey in patients with EM or CM (n = 101). Patients considered the time to effect onset to be at least as important as a clinically relevant reduction in migraine days during the first month of treatment (66). Another online survey (n = 604) also showed that patients deemed speed of onset, together with mode of administration and durability of preventive effect, as the treatment attributes with the highest relative importance (67). Early onset and sustained efficacy of eptinezumab could potentially increase treatment adherence, since one of the main reasons for treatment discontinuation is perceived lack of efficacy (68).
Considering the rapid effect of eptinezumab and its relevance to patients, the efficacy of eptinezumab was evaluated in patients who were having a migraine attack in the RELIEF study, a phase 3, multicenter, parallel-group, double-blind, randomized, placebo-controlled trial (62, 63). The study included 480 patients eligible for preventive migraine treatment (experiencing migraine 4–15 d/mo) who were treated either with 100 mg of eptinezumab or placebo within 1 to 6 h of the migraine attack onset. Participants were not allowed to use rescue medication 24 h prior to or 2 h following the infusion. Eptinezumab obtained better results for time to headache pain freedom (median hours, 4 eptinezumab vs. 9 placebo; p < 0.001) and time to absence of MBS (2 eptinezumab vs. 3 placebo; p < 0.001) (63). As early as 1 h after the start of the infusion, more eptinezumab-treated patients than placebo-treated achieved headache pain freedom, headache pain relief, and absence of MBS (p < 0.05), which lasted through hour 48 (62). After 2 h, almost one-fourth of patients (23.5%) treated with eptinezumab achieved headache pain freedom (62). Median time to next migraine was also significantly longer with eptinezumab (10 days) than with placebo (5 days; p < 0.001) (63). Fewer patients used AHM within 24 and 48 h in the eptinezumab than in the placebo group (p < 0.001) (63). Patients eligible for preventive migraine treatment, therefore, could benefit from receiving eptinezumab during an active migraine attack, due to the rapid resolution of migraine symptoms and the reduction of AHM use.
Eptinezumab treatment initiated during a migraine attack also resulted in greater improvements on PROM scores compared to placebo, such as in HIT-6 (p < 0.0001), 6-item migraine Treatment Optimization Questionnaire (mTOQ-6; p < 0.01), and PGIC (much or very much improved: 59.3% eptinezumab vs. 25.9% placebo) after 4 weeks (24). The improvements in PROM scores were more pronounced in patients with headache pain freedom 2 h after the infusion (24) and in those with poor acute treatment optimization prior to eptinezumab (25).These findings suggest that at least some of the benefits reported by patients after 4 weeks of the initial dose might be related to the fast onset of eptinezumab effect.
Diagnostic migraine classification, based on the number of headache days, continues to play a major role in determining access to preventive treatment. Pozo-Rosich et al. conducted a post-hoc analysis of data from the PROMISE studies considering four classification categories of monthly headache days (MHDs: ≥ 15, CM; 10–14, high-frequency EM; 4–9, low frequency EM; and ≤ 3) (26). The analysis showed that eptinezumab reduced headache frequency over months 1–6. Patients treated with eptinezumab improved their diagnostic classification, as they were more likely than placebo-treated patients to experience a shift of one or more headache day categories, achieving a reduction of at least one MHD over 6 months. More than half of CM patients were classified as EM the first month after eptinezumab infusion (58.7%, 100 mg; 61.7%, 300 mg), whereas less than half of placebo patients (45.6%) were. Similarly, a higher percentage of patients in the eptinezumab than in the placebo group converted from CM to EM in the following 6 months and were also more likely to fall below the threshold for initiating preventive treatment (≤ 4 MHDs).
Importantly, eptinezumab efficacy was independent of patient and disease characteristics at baseline, as demonstrated by several post-hoc analyses of the PROMISE studies. Efficacy was observed regardless of the race/ethnicity, demographics, migraine features, and concomitant medication use (28, 60, 69, 70). The efficacy of eptinezumab demonstrated no dose-dependent effect within the range of 100 to 300 mg. Apelian et al. (27) reported that the likelihood of achieving ≥50% MRR was similar across patients with either the 100-mg or 300-mg eptinezumab dose. The odds ratio, however, indicated that 300 mg had slightly higher efficacy than 100 mg in certain subgroups (such as patients with EM and obesity; and patients with CM and: < 15 MMDs at baseline, mobility problems on the EQ-5D-5L in CM, or a score > 45 on the SF-36 vitality), but these numerically higher improvements for the 300-mg dose were not statistically significant. These results were aligned with a meta-analysis of four randomized controlled trials (n = 2,739) that found no statistically significant differences between the two doses in ≥50% MRR, MMDs, and patients with migraine 1 day after the infusion.
Around half of the patients in the PROMISE trials had a self-reported history of experiencing aura. Ashina et al. (29) assessed the efficacy of eptinezumab in this subgroup. This analysis confirmed that eptinezumab decreased MMDs in patients with aura and EM (−4.0, 100 mg; −4.2, 300 mg; −3.1–7.1) or CM (−7.1, 100 mg; −7.6, 300 mg; 6.0, placebo), similar to results in the global study population. Eptinezumab reduced, to a greater extent than placebo, the percentage of migraine attacks with aura relative to baseline, suggesting a potential effect on lessening aura frequency beyond migraine frequency. The reduction of migraine attacks with aura may be important because migraine with aura is associated with an increased risk of cerebrovascular and cardiovascular disease (71, 72).
In the pivotal trials, the effect of eptinezumab in patients with failure with previous preventive treatment remained unexplored, despite patients being refractory to several preventive treatments are common. To evaluate eptinezumab in patients with failure with prior treatments, Ashina et al. conducted the DELIVER study, a phase 3b, multicenter, randomized, double-blind, placebo-controlled trial (31). Patients with EM (54%; high-frequency EM, 41%) or CM (46%) and two-to-four previous preventive treatment failures were included and were randomly assigned to eptinezumab 100, 300 mg, or placebo (1:1:1). The most common previous preventive medication failures were amitriptyline and topiramate. The reduction in mean MMDs from baseline to weeks 1–12 was −4·8 with 100 mg, −5·3 with 300 mg, and − 2·1 with placebo (p < 0·0001), and the effect was sustained or further improved over weeks 13–24 (−5.4 with 100 mg, −6.1 with 300 mg, and − 2.4 with placebo). The ≥50% MRR was also greater (p < 0.0001) for eptinezumab (42% with 100 mg; 49% with 300 mg) than placebo (13%) over weeks 1–12 and the effect further improved after the second infusion (52% with 100 mg; 59% with 300 mg; and 24% with placebo). The ≥75% MRR followed a similar trend over this period (weeks 1–12: 16% with 100 mg, 19% with 300 mg, 2% with placebo; weeks 13–24: 21% with 100 mg, 28% with 300 mg, 7% with placebo; p < 0.0001). Even in these patients with failure with prior treatments, total scores in the HIT-6 had higher improvements with eptinezumab compared with placebo by week 12, and fewer severe migraine attacks, MHDs and episodes, and monthly acute medication days (12–4 weeks).
Analysis of subpopulations considering sex, age, disease classification, MOH diagnosis, or number of prior preventive treatment failures, confirmed a significantly greater efficacy of eptinezumab than placebo for reducing MMDs across most subgroups (32, 33), demonstrating its efficacy regardless patient’s characteristics. Moreover, eptinezumab significantly improved more than placebo patients’ overall health, headache-related quality of life, absenteeism, presenteeism, work productivity loss, and activity impairment (32, 34).
Results from the DELIVER study consolidated the fast and sustained efficacy of eptinezumab observed in prior studies. However, findings from the DELIVER study are worth discussing here. On one hand, the placebo effect in the DELIVER study was numerically lower than in the PROMISE studies, which might reflect lower expectations among patients with failure of previous preventive treatments compared with those without prior failure. The efficacy observed with eptinezumab, despite the low expectations for these patients, highlights its superiority vs. placebo. On the other hand, slightly lower ≥50% and ≥ 75% MRR were registered in the DELIVER than in the PROMISE studies, probably due to a more difficult-to-treat migraine in patients included in former than in the latter. Yet, a higher proportion of patients with unsuccessful prior preventive therapies and treated with eptinezumab had higher ≥50% MRR than when treated with other SC anti-CGRP (73). The DELIVER study had a dose-blinded extension (48 weeks) which demonstrated long-term effectiveness and safety and tolerability of eptinezumab for up to 18 month in patients with migraine and 2–4 prior preventive treatment failures (74).
One of the most recent post-hoc analyses of the PROMISE studies by Schim et al. showed that around one-third of patients with suboptimal response (<50% MMD reduction from baseline in MMDs over weeks 1–12) after the first dose, responded (≥ 50% MMD reduction) to the second dose (30). They identified potential first-infusion predictors of second-infusion response by using full logistic regression analysis. The analysis showed that percent change in MMDs across weeks 1–12 was a significant first-dose predictor of second-dose response in patients with EM and CM, and change in HIT-6 total score in CM. Even in patients who had no change in MMDs after their first infusion, the likelihood of having a ≥ 50% MMD increased after the second infusion. Schim et al. also included a table with the likelihood of response according to first-dose predictors (30), which could be helpful for making individualized treatment decisions in the clinical practice.
Several aspects of the efficacy results of the studies reported here deserve to be discussed. First, some of these findings have been obtained from post-hoc analysis, which entail methodological limitations, and should be replicated in studies specifically designed to test those endpoints. Second, a considerable placebo effect was observed across the efficacy endpoints, in line with findings of other anti-CGRP (75–77) and migraine treatments (78). As it is well known, the placebo effect could be due to several factors, including the clinical environment, interactions with healthcare professionals, patient expectations and beliefs, or the treatment administration route (79). Third, all data was obtained from clinical trials, which included strict screening criteria for patients and were conducted in a highly controlled clinical environment. Studies in the real-world setting are needed to confirm results from clinical trials in a more heterogeneous population in terms of demographics, socioeconomic factors, migraine characteristics, comorbidities, and concomitant medication use. Also, the efficacy of eptinezumab in patients with previous treatment failure to an anti-CGRP has not been examined since these patients were excluded from the DELIVER study. The efficacy of eptinezumab in this population, as well as in combination with other prevention and nonpharmacological therapies, should be explored.
The tolerability and safety of eptinezumab was also evaluated in the above-mentioned clinical trials (17, 18, 23, 31, 52, 54, 62–65, 80), which showed that eptinezumab was well tolerated and had a favorable safety profile in patients with EM and CM. Treatment-emergent adverse events (TEAE) were similar across doses and treatment groups and did not increase with continuous dosing. These results were further confirmed in two meta-analyses (81, 82). One of these meta-analyses included patients who received at least 1 dose of eptinezumab (n = 2076) or placebo (n = 791) in five eptinezumab trials (NCT01772524, NCT02275117, PROMISE-1, PROMISE-2, and PREVAIL). The study showed that the proportion of patients who had at least one TEAE was consistent across active and placebo groups (54.0%, 30 mg; 52.2%, 100 mg; 56.7%, 300 mg; and 52.3%, placebo) and no dose-related trends were observed (Table 3) (81). The most frequent study-drug-related TEAE was fatigue (eptinezumab, 2.0% vs. placebo, 0.9%) (81). Among study-drug-related TEAEs, six events reported by four patients (eptinezumab, n = 3; placebo, n = 1) were considered severe. No life-threatening (grade 4) or fatal (grade 5) TEAEs occurred (81). The other meta-analysis that pooled 2,739 participants from four of the eptinezumab trials (NCT01772524, NCT02275117, PROMISE-1, PROMISE-2) confirmed that TEAEs were not statistically different between the eptinezumab and placebo group (82).
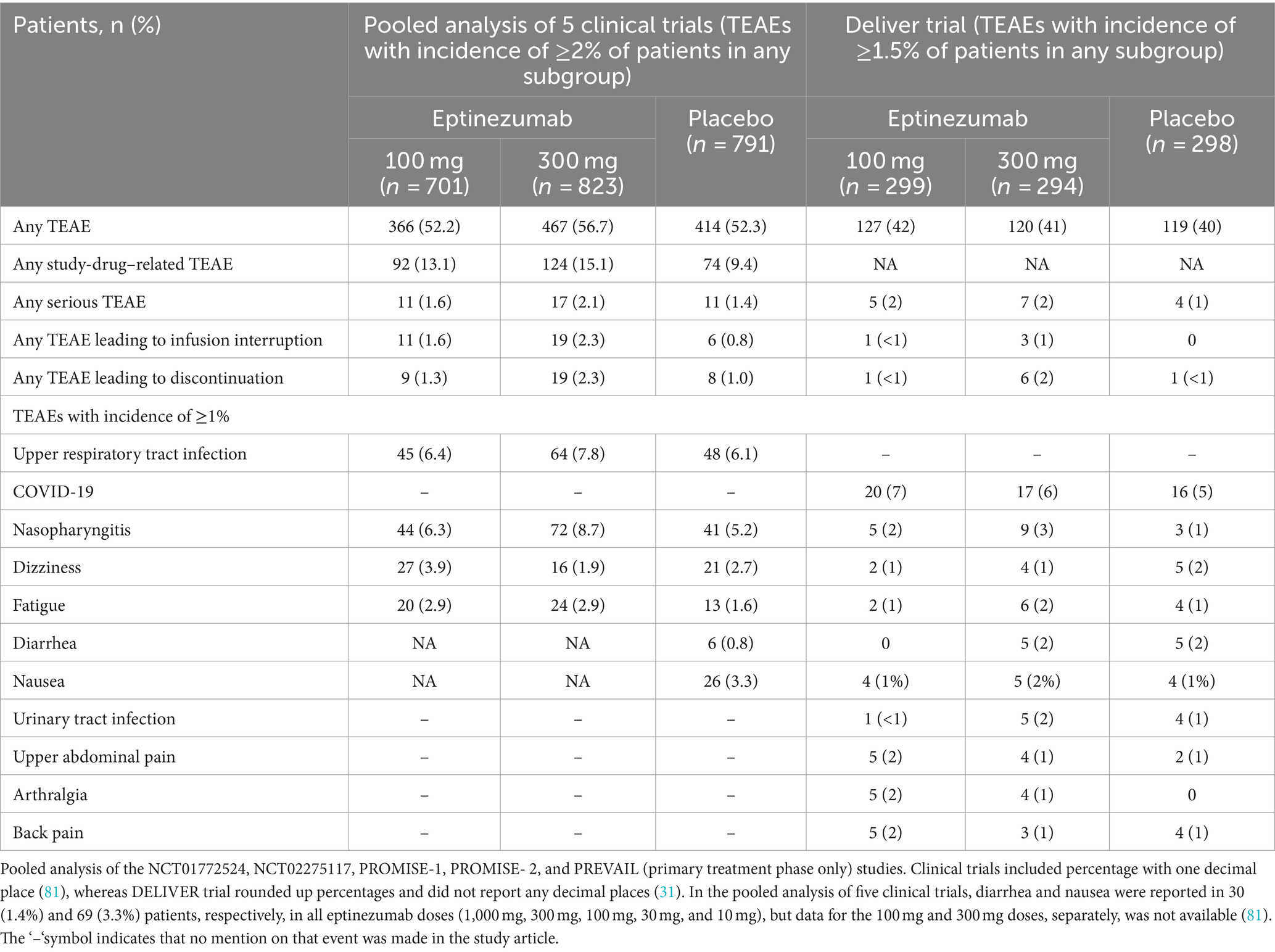
Table 3. Summary of TEAEs.
Up to 1 year, a lower proportion of patients reported at least one TEAE in the second and subsequent dosing intervals than in the first dosing interval across all treatment groups, and no serious tolerability issues were identified with continued dosing (52). The PREVAIL study, an open-label phase 3 trial, assessed long-term safety and immunogenicity of eptinezumab 300 mg, a dose that is three times higher than the recommended dose according to the Summary of Product Characteristics (SmPC), for up to eight doses in patients with CM and a follow-up of 104 weeks (80). During the study, 91 out of 128 patients experienced at least one TEAE, most of them during the first treatment phase. Thirteen patients had severe TEAEs, which were unrelated to eptinezumab. Eighteen patients had at least one study-drug-related TEAE, with hypersensitivity and fatigue being the most common. Only one serious TEAE was considered related to eptinezumab (anaphylactic reaction, grade 2; however, due to the patient’s medical history and reaction during the TEAE, the investigators concluded that this event could be more accurately described as an allergic reaction).
Importantly, eptinezumab has been shown to be safe and well tolerated regardless of patient characteristics (28, 31, 83). Two randomized, double-blind, placebo-controlled trials were conducted to examine the safety and metabolic effects of eptinezumab in patients without migraine who were overweight or obese (study 1; n = 24) and with type 1 diabetes (T1D; study 2; n = 21) (83). In the first study, 37.5% of eptinezumab-treated and 25.0% of placebo-treated patients reported a TEAE; only one TEAE (in the active group) was deemed drug-related. No difference between patients treated with eptinezumab and placebo emerged from baseline to day 7 in terms of basal metabolic rate. In the second study, 85.7% of eptinezumab-treated and 100% of placebo-treated patients reported a TEAE, which were drug-related in four patients (two in the active group, two in the placebo group). No significant difference in insulin sensitivity was detected between treatment groups. In both studies, all TEAEs were mild or moderate in severity and no TEAEs leading to discontinuation or serious events were reported.
Results from the DELIVER study also confirmed that TEAEs occurred with a similar incidence and seriousness in patients treated either with eptinezumab or placebo who had two-to-four previous preventive treatment failures (31). The most common TEAE was COVID-19 in all groups (Table 3).
Patients with migraine have an increased risk for cardiovascular events, which might be potentially exacerbated by anti-CGRP treatments that hamper vasodilation (84). The effect of eptinezumab on cardiovascular events and comorbidities was assessed by pooling safety data (n = 2,268) from four clinical trials on eptinezumab (85). The analysis showed that cardiovascular TEAEs considered treatment-related were rare (n = 27) and the incidence was similar in placebo (n = 6) and eptinezumab groups (100 mg, n = 8; 300 mg, n = 7; 1,000 mg, n = 6). Most cardiovascular TEAEs occurred in patients with ≥1 and ≥ 2 cardiovascular risk factors at baseline, and all events were mild or moderate in severity with none being serious or life-threatening. No relevant effect of eptinezumab or difference between treatment groups was observed on blood pressure, heart rate or concomitant cardiovascular medication use for up to 56 weeks. A total of 9 (1.3%) and 13 (1.9%) patients receiving the 100-mg and 300-mg dose and 8 (1.0%) patients in the placebo group discontinued study drug due to TEAEs.
The immunogenic profile of eptinezumab was also characterized by pooling data (n = 2076) from five clinical trials (NCT01772524, NCT02275117, PROMISE-1 and -2, and PREVAIL studies) (86). Immunogenicity was assessed in serum from all patients who received eptinezumab, and samples were collected on day 0 and regularly throughout each study at similar time points (2-week time point to evaluate early seroconversion, followed by sampling at 4-week intervals). Anti-drug antibody (ADAs) and neutralizing antibodies (Nabs) were found in 15.9 and 6.2% patients treated with eptinezumab, respectively. In all four trials, ADA/NAb development began around week 8, peaked at week 24 (second infusion), and steadily declined during the subsequent weeks, regardless of eptinezumab dose or number of doses. Even when ADA or NAb presented, eptinezumab maintained its efficacy and safety profile.
Collectively, results from pooled data from clinical trials has demonstrated that eptinezumab, in general, is well tolerated, and has a favorable long-term safety profile.
Eptinezumab has unique features that offers potential clinical benefits. It shows a fast onset of action and effectiveness in treating migraine attacks. Using eptinezumab during a migraine attack leads to significant improvements in pain freedom and the most bothersome symptoms within the first 2 h post-infusion (63). Moreover, the convenience of intravenous administration every 3 months distinguishes eptinezumab from other monthly subcutaneous CGRP mAbs. Existing literature suggests that individuals in need of rapid relief, those who prefer less frequent dosing, or those who have not responded adequately to other CGRP mAbs may benefit the most from eptinezumab. However, comprehensive comparative studies are necessary to establish specific patient profiles.
Nine clinical trials on eptinezumab are currently ongoing (35–42, 87). A brief description of each study is reported in Table 4. Most of the studies are randomized clinical trials in adults, with change in the number of MMDs at variable timepoints as the primary endpoint. The CHRONICLE trial is an open-label study evaluating primarily the safety of eptinezumab in patients with cluster headache.
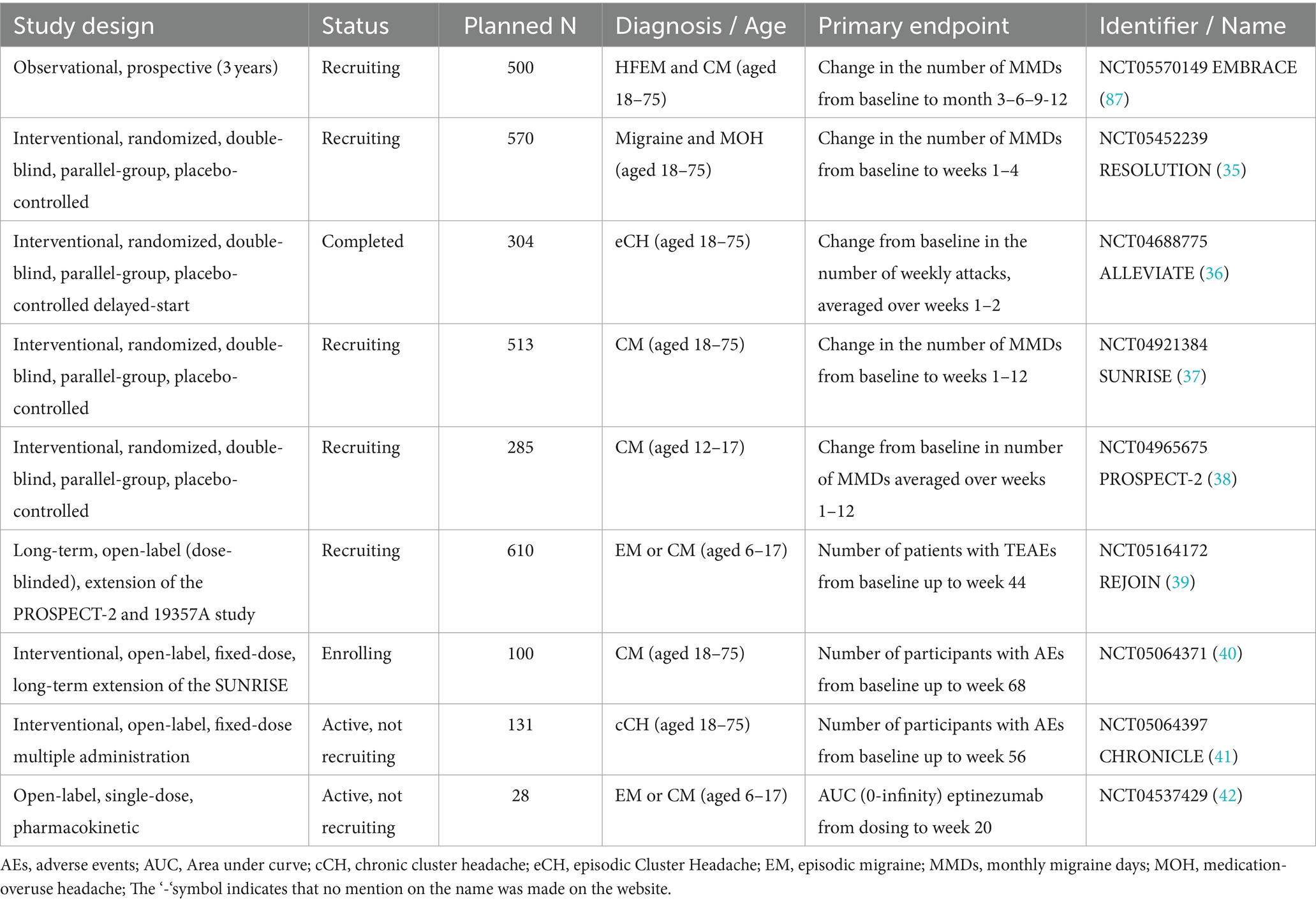
Table 4. Ongoing studies on eptinezumab registered on clinical trials.
Clinical trials on children and adolescents are also ongoing and will provide information on the pharmacokinetics, efficacy, and safety of eptinezumab on these populations, who are currently not allowed to be treated with eptinezumab according to the SmPC.
In terms of eptinezumab dosage optimization, further research is needed to discern specific patient profiles that would benefit from the 300 mg dose, particularly in cases where the recommended 100 mg dose results in a suboptimal response. Such studies are key for assisting neurologists in making informed dosing adjustments, particularly in light of the current absence of detailed guidance in the SmPC.
Collectively, data from clinical trials has demonstrated that eptinezumab is a potent, fast, effective and safe preventive treatment across migraine diagnoses, patient demographics and disease characteristics, and prior treatments. Eptinezumab benefits manifested as early as day 1 after dosing and lasted up to at least 2 years. The evidence reported by the studies supports that eptinezumab is effective as a preventive treatment and also demonstrates immediate efficacy in alleviating migraine pain and symptoms when administered during a migraine attack in candidates eligible for preventive treatment. Therefore, the data suggest that eptinezumab could serve as a quarterly preventive treatment option, offering potential additional benefits for active migraine attack when initiated during the attacks. The rapid onset and sustained efficacy of eptinezumab could potentially reduce migraine burden and give patients a sense of control. Real-world studies that assess the effectiveness and safety of eptinezumab in a diverse patient population, and in comparison with other CGRP mAbs, are needed. This research would increase our understanding of the role of eptinezumab in migraine management.
PI: Conceptualization, Funding acquisition, Validation, Writing –review & editing. SS-L: Validation, Writing –review & editing. PP-R: Validation, Writing –review & editing. RL: Validation, Writing –review & editing. JP: Validation, Writing –review & editing. JL: Conceptualization, Funding acquisition, Validation, Writing –review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Medical writing was funded by Lundbeck Spain in accordance with Good Publication Practice (GPP3) guidelines. Lundbeck Spain was not involved in the study design, collection, analysis, interpretation of data, or the decision to submit it for publication.
The authors thank Laura Prieto del Val of Evidenze Health España, S.L.U, for providing medical writing support (writing of the original draft, implementing changes in the manuscript after authors’ revisions, adapting the manuscript to journal requirements and submission to the journal), which was funded by Lundbeck Spain in accordance with Good Publication Practice (GPP3) guidelines.
PI received honoraria from Eli Lilly, Novartis, TEVA, Abbvie, Lündbeck and Chiesi for consultancy and educational activities. SS-L has received honoraria from Abbvie, Almirall, Amgen, Chiesi, Eisai, Grünenthal, Exeltis, Lilly, Lündbeck, Novartis, Pfizer and Teva. PP-R has received honoraria as a consultant and speaker, in the last 5 years, for: AbbVie, Amgen, Biohaven, Chiesi, Eli Lilly, Lundbeck, Medscape, Novartis, Pfizer and Teva. Her research group has received research grants from AbbVie, Novartis and Teva; and, has received funding for clinical trials from Alder, AbbVie, Amgen, Biohaven, Electrocore, Eli Lilly, Lundbeck, Novartis and Teva. She is the Honorary Secretary of the International Headache Society. She is in the editorial board of Revista de Neurologia, associate editor for Cephalalgia, Headache, The Journal of Headache and Pain, Neurologia, Frontiers of Neurology. She is a member of the Clinical Trials Guidelines Committee and Scientific Committee of the International Headache Society. She has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. She is the founder of www.midolordecabeza.org. She does not own stocks from any pharmaceutical company. JP received honoraria from Abbvie, Almirall, Eli Lilly, Lundbeck, Novartis and TEVA for consultancy and educational activities.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1355877/full#supplementary-material
1. GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2018) 17:954–76. doi: 10.1016/s1474-4422(18)30322-3
2. Safiri, S, Pourfathi, H, Eagan, A, Mansournia, MA, Khodayari, MT, Sullman, MJM, et al. Global, regional, and national burden of migraine in 204 countries and territories, 1990 to 2019. Pain. (2022) 163:e293–309. doi: 10.1097/j.pain.0000000000002275
3. Ferrari, MD, Goadsby, PJ, Burstein, R, Kurth, T, Ayata, C, Charles, A, et al. Migraine. Nat Rev Dis Primers. (2022) 8:2. doi: 10.1038/s41572-021-00328-4
4. Leonardi, M, and Raggi, A. A narrative review on the burden of migraine: when the burden is the impact on people’s life. J Headache Pain. (2019) 20:41. doi: 10.1186/s10194-019-0993-0
5. Doane, MJ, Gupta, S, Fang, J, Laflamme, AK, and Vo, P. The humanistic and economic burden of migraine in Europe: a cross-sectional survey in five countries. Neurol Ther. (2020) 9:535–49. doi: 10.1007/s40120-020-00196-2
6. Hubig, LT, Smith, T, Williams, E, Powell, L, Johnston, K, Harris, L, et al. Measuring interictal burden among people affected by migraine: a descriptive survey study. J Headache Pain. (2022) 23:97. doi: 10.1186/s10194-022-01467-z
7. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders. 3rd edn. Cephalalgia (2018); 38: 1–211. doi: 10.1177/0333102417738202
8. Goadsby, PJ, and Evers, S. International classification of headache disorders - ICHD-4alpha. Cephalalgia. (2020) 40:887–8. doi: 10.1177/0333102420919098
9. Eigenbrodt, AK, Ashina, H, Khan, S, Diener, HC, Mitsikostas, DD, Sinclair, AJ, et al. Diagnosis and management of migraine in ten steps. Nat Rev Neurol. (2021) 17:501–14. doi: 10.1038/s41582-021-00509-5
10. Edvinsson, L. Role of CGRP in migraine In: SD Brain and P Geppetti, editors. Calcitonin gene-related peptide (CGRP) mechanisms: Focus on migraine. Cham: Springer International Publishing (2019). 121–30.
11. Deng, H, Li, G-G, Nie, H, Feng, YY, Guo, GY, Guo, WL, et al. Efficacy and safety of calcitonin-gene-related peptide binding monoclonal antibodies for the preventive treatment of episodic migraine - an updated systematic review and meta-analysis. BMC Neurol. (2020) 20:57–7. doi: 10.1186/s12883-020-01633-3
13. Drellia, K, Kokoti, L, Deligianni, CI, Papadopoulos, D, and Mitsikostas, DD. Anti-CGRP monoclonal antibodies for migraine prevention: a systematic review and likelihood to help or harm analysis. Cephalalgia. (2021) 41:851–64. doi: 10.1177/0333102421989601
14. Garcia-Martinez, LF, Raport, CJ, Ojala, EW, Dutzar, B, Anderson, K, Stewart, E, et al. Pharmacologic characterization of ALD403, a potent neutralizing humanized monoclonal antibody against the calcitonin gene-related peptide. J Pharmacol Exp Ther. (2020) 374:93–103. doi: 10.1124/jpet.119.264671
15. European Medicines Agency. Summary of Product Characteristics: Eptinezumab (VYEPTI). Available at: https://www.ema.europa.eu/en/documents/product-information/vyepti-epar-product-information_en.pdf. (Accessed February 8, 2023).
16. Food and Drug Administration. VYEPTITM (eptinezumab-jjmr) injection for intravenous use. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/761119s000lbl.pdf. (Accessed January 24, 2024).
17. Lipton, RB, Goadsby, PJ, Smith, J, Schaeffler, BA, Biondi, DM, Hirman, J, et al. Efficacy and safety of eptinezumab in patients with chronic migraine: PROMISE-2. Neurology. (2020) 94:e1365–77. doi: 10.1212/wnl.0000000000009169
18. Ashina, M, Saper, J, Cady, R, Schaeffler, BA, Biondi, DM, Hirman, J, et al. Eptinezumab in episodic migraine: a randomized, double-blind, placebo-controlled study (PROMISE-1). Cephalalgia. (2020) 40:241–54. doi: 10.1177/0333102420905132
19. Buse, DC, Winner, PK, Charleston, L, Hirman, J, Cady, R, and Brevig, T. Early response to eptinezumab indicates high likelihood of continued response in patients with chronic migraine. J Headache Pain. (2022) 23:29. doi: 10.1186/s10194-022-01387-y
20. Lipton, RB, Goadsby, PJ, Dodick, DW, McGinley, JS, Houts, CR, Wirth, RJ, et al. Evaluating the clinical utility of the patient-identified most bothersome symptom measure from PROMISE-2 for research in migraine prevention. Headache. (2022) 62:690–9. doi: 10.1111/head.14295
21. Cowan, RP, Marmura, MJ, Diener, HC, Starling, AJ, Schim, J, Hirman, J, et al. Quantity changes in acute headache medication use among patients with chronic migraine treated with eptinezumab: subanalysis of the PROMISE-2 study. J Headache Pain. (2022) 23:115. doi: 10.1186/s10194-022-01482-0
22. McAllister, P, Kudrow, D, Cady, R, Hirman, J, and Ettrup, A. Reduction in migraine-associated burden after eptinezumab treatment in patients with chronic migraine. Cephalalgia. (2022) 42:1005–12. doi: 10.1177/03331024221089567
23. Blumenfeld, A, Ettrup, A, Hirman, J, Ebert, B, and Cady, R. Long-term reductions in disease impact in patients with chronic migraine following preventive treatment with eptinezumab. BMC Neurol. (2022) 22:251. doi: 10.1186/s12883-022-02774-3
24. McAllister, P, Winner, PK, Ailani, J, Buse, DC, Lipton, RB, Chakhava, G, et al. Eptinezumab treatment initiated during a migraine attack is associated with meaningful improvement in patient-reported outcome measures: secondary results from the randomized controlled RELIEF study. J Headache Pain. (2022) 23:22. doi: 10.1186/s10194-021-01376-7
25. Cady, R, Lipton, RB, Buse, DC, Josiassen, MK, Lindsten, A, and Ettrup, A. Optimization of acute medication use following eptinezumab initiation during a migraine attack: post hoc analysis of the RELIEF study. J Headache Pain. (2022) 23:91. doi: 10.1186/s10194-022-01463-3
26. Pozo-Rosich, P, Dodick, DW, Ettrup, A, Hirman, J, and Cady, R. Shift in diagnostic classification of migraine after initiation of preventive treatment with eptinezumab: post hoc analysis of the PROMISE studies. BMC Neurol. (2022) 22:394. doi: 10.1186/s12883-022-02914-9
27. Apelian, R, Boyle, L, Hirman, J, and Asher, D. Measuring dose-related efficacy of eptinezumab for migraine prevention: post hoc analysis of PROMISE-1 and PROMISE-2. J Headache Pain. (2022) 23:48. doi: 10.1186/s10194-022-01418-8
28. Martin, V, Nagy, AJ, Janelidze, M, Giorgadze, G, Hirman, J, Cady, R, et al. Impact of baseline characteristics on the efficacy and safety of Eptinezumab in patients with migraine: subgroup analyses of PROMISE-1 and PROMISE-2. Clin Ther. (2022) 44:389–402. doi: 10.1016/j.clinthera.2022.01.006
29. Ashina, M, McAllister, P, Cady, R, Hirman, J, and Ettrup, A. Efficacy and safety of eptinezumab in patients with migraine and self-reported aura: post hoc analysis of PROMISE-1 and PROMISE-2. Cephalalgia. (2022) 42:696–704. doi: 10.1177/03331024221077646
30. Schim, JD, Anderson, C, Brunner, E, Hirman, J, Ogbru, A, Cady, R, et al. Likelihood of response with subsequent dosing for patients with migraine and initial suboptimal response with eptinezumab: a post hoc analysis of two placebo-controlled randomized clinical trials. Headache. (2022) 62:558–65. doi: 10.1111/head.14302
31. Ashina, M, Lanteri-Minet, M, Pozo-Rosich, P, Ettrup, A, Christoffersen, CL, Josiassen, MK, et al. Safety and efficacy of eptinezumab for migraine prevention in patients with two-to-four previous preventive treatment failures (DELIVER): a multi-arm, randomised, double-blind, placebo-controlled, phase 3b trial. Lancet Neurol. (2022) 21:597–607. doi: 10.1016/s1474-4422(22)00185-5
32. Goadsby, PJ, Barbanti, P, Lambru, G, Ettrup, A, Christoffersen, CL, Josiassen, MK, et al. Eptinezumab improved patient-reported outcomes and quality of life in patients with migraine and prior preventive treatment failures. Eur J Neurol. (2023) 30:1089–98. doi: 10.1111/ene.15670
33. Ashina, M, Lanteri-Minet, M, Ettrup, A, Christoffersen, CL, Josiassen, MK, Phul, R, et al. Efficacy and safety of eptinezumab for migraine prevention in patients with prior preventive treatment failures: subgroup analysis of the randomized, placebo-controlled DELIVER study. Cephalalgia. (2023) 43:3331024231170807. doi: 10.1177/03331024231170807
34. Barbanti, P, Goadsby, PJ, Lambru, G, Ettrup, A, Christoffersen, CL, Josiassen, MK, et al. Effects of eptinezumab on self-reported work productivity in adults with migraine and prior preventive treatment failure in the randomized, double-blind, placebo-controlled DELIVER study. J Headache Pain. (2022) 23:153. doi: 10.1186/s10194-022-01521-w
35. H. Lundbeck A/S. A study of Eptinezumab in participants with migraine and medication overuse headache. Available at: https://clinicaltrials.gov/ct2/show/NCT05452239?recrs=a&cond=eptinezumab&draw=2&rank=1 (Accessed November 23, 2022).
36. H. Lundbeck A/S. Eptinezumab in participants with episodic cluster headache (ALLEVIATE). Available at: https://clinicaltrials.gov/ct2/show/NCT04688775?recrs=a&cond=eptinezumab&draw=2&rank=2 (Accessed November 23, 2022).
37. H. Lundbeck A/S. Eptinezumab as Preventive Treatment of Migraine in Adults With Migraine (Sunrise). Available at: https://clinicaltrials.gov/ct2/show/NCT04921384?recrs=a&cond=eptinezumab&draw=2&rank=3 (Accessed November 23, 2022).
38. H. Lundbeck A/S. A Study With Eptinezumab in Adolescents (12-17 Years) With Chronic Migraine (PROSPECT-2). Available at: https://clinicaltrials.gov/ct2/show/NCT04965675?recrs=a&cond=eptinezumab&draw=2&rank=6 (Accessed November 23, 2022).
39. H. Lundbeck A/S. A Study With Eptinezumab in Children and Adolescents (6 to 17 Years) With Chronic or Episodic Migraine. Available at: https://clinicaltrials.gov/ct2/show/NCT05164172?recrs=a&cond=eptinezumab&draw=2&rank=5 (Accessed November 23, 2022).
40. H. Lundbeck A/S. Long-Term Extension Study With Eptinezumab as Preventive Treatment in Participants With Migraine in Japan. Available at: https://clinicaltrials.gov/ct2/show/NCT05064371?recrs=df&cond=eptinezumab&draw=2&rank=1 (Accessed November 23, 2022).
41. H. Lundbeck A/S. A 1-year Trial to Inform About Long-term Exposure to Eptinezumab in Participants With Chronic Cluster Headache (cCH) (CHRONICLE). Available at: https://clinicaltrials.gov/ct2/show/NCT05064397?recrs=df&cond=eptinezumab&draw=2&rank=2 (Accessed November 23, 2022).
42. H. Lundbeck A/S. A Study in Children and Young People With Migraine to Learn What the Body Does to Eptinezumab. Available at: https://clinicaltrials.gov/ct2/show/NCT04537429?recrs=df&cond=eptinezumab&draw=2&rank=3 (Accessed November 23, 2022).
43. Datta, A, Maryala, S, and John, R. A review of Eptinezumab use in migraine. Cureus. (2021) 13:e18032. doi: 10.7759/cureus.18032
44. Siahaan, YMT, Hartoyo, V, and Hariyanto, TI. Efficacy and safety of eptinezumab as preventive treatment for episodic/chronic migraine: a systematic review and meta-analysis. Clin Exp Pharmacol Physiol. (2022) 49:1156–68. doi: 10.1111/1440-1681.13700
45. Villar-Martínez, MD, Moreno-Ajona, D, and Goadsby, PJ. Eptinezumab for the preventive treatment of migraine. Pain Manag. (2021) 11:113–21. doi: 10.2217/pmt-2020-0075
46. Baker, B, Schaeffler, B, Beliveau, M, Rubets, I, Pederson, S, Trinh, MM, et al. Population pharmacokinetic and exposure-response analysis of eptinezumab in the treatment of episodic and chronic migraine. Pharmacol Res Perspect. (2020) 8:e00567. doi: 10.1002/prp2.567
47. Morgan, KW, and Joyner, KR. Eptinezumab: a calcitonin gene-related peptide monoclonal antibody infusion for migraine prevention. SAGE Open Med. (2021) 9:20503121211050186. doi: 10.1177/20503121211050186
48. Cohen-Barak, O, Weiss, S, Rasamoelisolo, M, Faulhaber, N, Yeung, PP, Loupe, PS, et al. A phase 1 study to assess the pharmacokinetics, safety, and tolerability of fremanezumab doses (225 mg, 675 mg and 900 mg) in Japanese and Caucasian healthy subjects. Cephalalgia. (2018) 38:1960–71. doi: 10.1177/0333102418771376
49. Monteith, D, Collins, EC, Vandermeulen, C, van Hecken, A, Raddad, E, Scherer, JC, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of the CGRP binding monoclonal antibody LY2951742 (Galcanezumab) in healthy volunteers. Front Pharmacol. (2017) 8:740. doi: 10.3389/fphar.2017.00740
50. de Hoon, J, van Hecken, A, Vandermeulen, C, Yan, L, Smith, B, Chen, JS, et al. Phase I, randomized, double-blind, placebo-controlled, single-dose, and multiple-dose studies of Erenumab in healthy subjects and patients with migraine. Clin Pharmacol Ther. (2018) 103:815–25. doi: 10.1002/cpt.799
51. David, L, Scalley-Kim, M, Olland, A, White, A, and Misura, K. The eptinezumab: CGRP complex structure - the role of conformational changes in binding stabilization. Bioengineered. (2021) 12:11076–86. doi: 10.1080/21655979.2021.2006977
52. Smith, TR, Janelidze, M, Chakhava, G, Cady, R, Hirman, J, Allan, B, et al. Eptinezumab for the prevention of episodic migraine: sustained effect through 1 year of treatment in the PROMISE-1 study. Clin Ther. (2020) 42:2254–2265.e3. doi: 10.1016/j.clinthera.2020.11.007
53. Dodick, DW, Gottschalk, C, Cady, R, Hirman, J, Smith, J, and Snapinn, S. Eptinezumab demonstrated efficacy in sustained prevention of episodic and chronic migraine beginning on day 1 after dosing. Headache. (2020) 60:2220–31. doi: 10.1111/head.14007
54. Silberstein, S, Diamond, M, Hindiyeh, NA, Biondi, DM, Cady, R, Hirman, J, et al. Eptinezumab for the prevention of chronic migraine: efficacy and safety through 24 weeks of treatment in the phase 3 PROMISE-2 (prevention of migraine via intravenous ALD403 safety and efficacy-2) study. J Headache Pain. (2020) 21:120. doi: 10.1186/s10194-020-01186-3
55. Food and Drug Administration (FDA). Migraine: Developing drugs for acute treatment guidance for industry. (2018). Available at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/migraine-developing-drugs-acute-treatment.
56. Lipton, RB, Dodick, DW, Ailani, J, McGill, L, Hirman, J, and Cady, R. Patient-identified most bothersome symptom in preventive migraine treatment with eptinezumab: a novel patient-centered outcome. Headache. (2021) 61:766–76. doi: 10.1111/head.14120
57. Starling, AJ, Cowan, RP, Buse, DC, Diener, HC, Marmura, MJ, Hirman, J, et al. Eptinezumab improved patient-reported outcomes in patients with migraine and medication-overuse headache: subgroup analysis of the randomized PROMISE-2 trial. Headache. (2023) 63:264–74. doi: 10.1111/head.14434
58. Diener, HC, Marmura, MJ, Tepper, SJ, Cowan, R, Starling, AJ, Diamond, ML, et al. Efficacy, tolerability, and safety of eptinezumab in patients with a dual diagnosis of chronic migraine and medication-overuse headache: subgroup analysis of PROMISE-2. Headache. (2021) 61:125–36. doi: 10.1111/head.14036
59. Marmura, MJ, Diener, HC, Cowan, RP, Tepper, SJ, Diamond, ML, Starling, AJ, et al. Preventive migraine treatment with eptinezumab reduced acute headache medication and headache frequency to below diagnostic thresholds in patients with chronic migraine and medication-overuse headache. Headache. (2021) 61:1421–31. doi: 10.1111/head.14206
60. Chakhava, G, Cady, R, and Kassel, E. Consistent reductions in migraine frequency with eptinezumab treatment in patients with migraine stratified by disease characteristics: subgroup analysis of PROMISE-1 and PROMISE-2. J Headache Pain. (2019) 20:109. doi: 10.1186/s10194-019-1049-1
61. Lipton, RB, Charleston, L, Tassorelli, C, Brevig, T, Hirman, J, and Cady, R. Patient-reported outcomes, health-related quality of life, and acute medication use in patients with a ≥ 75% response to eptinezumab: subgroup pooled analysis of the PROMISE trials. J Headache Pain. (2022) 23:23. doi: 10.1186/s10194-022-01386-z
62. Ailani, J, McAllister, P, Winner, PK, Chakhava, G, Krog Josiassen, M, Lindsten, A, et al. Rapid resolution of migraine symptoms after initiating the preventive treatment eptinezumab during a migraine attack: results from the randomized RELIEF trial. BMC Neurol. (2022) 22:205. doi: 10.1186/s12883-022-02714-1
63. Winner, PK, McAllister, P, Chakhava, G, Ailani, J, Ettrup, A, Krog Josiassen, M, et al. Effects of intravenous Eptinezumab vs placebo on headache pain and Most bothersome symptom when initiated during a migraine attack: a randomized clinical trial. JAMA. (2021) 325:2348–56. doi: 10.1001/jama.2021.7665
64. Dodick, DW, Goadsby, PJ, Silberstein, SD, Lipton, RB, Olesen, J, Ashina, M, et al. Safety and efficacy of ALD403, an antibody to calcitonin gene-related peptide, for the prevention of frequent episodic migraine: a randomised, double-blind, placebo-controlled, exploratory phase 2 trial. Lancet Neurol. (2014) 13:1100–7. doi: 10.1016/s1474-4422(14)70209-1
65. Dodick, DW, Lipton, RB, Silberstein, S, Goadsby, PJ, Biondi, D, Hirman, J, et al. Eptinezumab for prevention of chronic migraine: a randomized phase 2b clinical trial. Cephalalgia. (2019) 39:1075–85. doi: 10.1177/0333102419858355
66. Ailani, J, Winner, P, Hartry, A, Brevig, T, Bøg, M, Lassen, AB, et al. Patient preference for early onset of efficacy of preventive migraine treatments. Headache. (2022) 62:374–82. doi: 10.1111/head.14255
67. Schwedt, T, Martin, A, Kymes, S, Talon, B, Lee, XY, Cady, R, et al. CO39 patient preferences for attributes of advanced migraine prevention medications: findings from a discrete choice experiment. Value Health. (2022) 25:S311. doi: 10.1016/j.jval.2022.04.137
68. Kawata, AK, Shah, N, Poon, JL, Shaffer, S, Sapra, S, Wilcox, TK, et al. Understanding the migraine treatment landscape prior to the introduction of calcitonin gene-related peptide inhibitors: results from the assessment of TolerabiliTy and effectiveness in MigrAINe patients using preventive treatment (ATTAIN) study. Headache. (2021) 61:438–54. doi: 10.1111/head.14053
69. Misura, K, Song, Y, and Madan, A. IHC 2019 abstracts. Cephalalgia. (2019) 39:1–337. doi: 10.1177/0333102419859835
70. Martin, V, Tassorelli, C, Ettrup, A, Hirman, J, and Cady, R. Eptinezumab for migraine prevention in patients 50 years or older. Acta Neurol Scand. (2022) 145:698–705. doi: 10.1111/ane.13603
71. Kurth, T, Rist, PM, Ridker, PM, Kotler, G, Bubes, V, and Buring, JE. Association of Migraine with Aura and Other Risk Factors with Incident Cardiovascular Disease in women. JAMA. (2020) 323:2281–9. doi: 10.1001/jama.2020.7172
72. Mahmoud, AN, Mentias, A, Elgendy, AY, Qazi, A, Barakat, AF, Saad, M, et al. Migraine and the risk of cardiovascular and cerebrovascular events: a meta-analysis of 16 cohort studies including 1 152 407 subjects. BMJ Open. (2018) 8:e020498. doi: 10.1136/bmjopen-2017-020498
73. Ornello, R, and Sacco, S. A new option for patients with treatment-resistant migraine. Lancet Neurol. (2022) 21:578–9. doi: 10.1016/s1474-4422(22)00222-8
74. Ashina, M, Tepper, S, Gendolla, A, Sperling, B, Ettrup, A, Josiassen, MK, et al. Long-term effectiveness of Eptinezumab in patients with migraine and prior preventive treatment failures: extension of a randomized controlled trial. J Headache Pain. (2023) 24:155. doi: 10.1186/s10194-023-01688-w
75. Dodick, DW, Ashina, M, Brandes, JL, Kudrow, D, Lanteri-Minet, M, Osipova, V, et al. ARISE: a phase 3 randomized trial of erenumab for episodic migraine. Cephalalgia. (2018) 38:1026–37. doi: 10.1177/0333102418759786
76. Detke, HC, Goadsby, PJ, Wang, S, Friedman, DI, Selzler, KJ, and Aurora, SK. Galcanezumab in chronic migraine: the randomized, double-blind, placebo-controlled REGAIN study. Neurology. (2018) 91:e2211–21. doi: 10.1212/wnl.0000000000006640
77. Dodick, DW, Silberstein, SD, Bigal, ME, Yeung, PP, Goadsby, PJ, Blankenbiller, T, et al. Effect of Fremanezumab compared with placebo for prevention of episodic migraine: a randomized clinical trial. JAMA. (2018) 319:1999–2008. doi: 10.1001/jama.2018.4853
78. Autret, A, Valade, D, and Debiais, S. Placebo and other psychological interactions in headache treatment. J Headache Pain. (2012) 13:191–8. doi: 10.1007/s10194-012-0422-0
79. Swerts, DB, Benedetti, F, and Peres, MFP. Different routes of administration in chronic migraine prevention lead to different placebo responses: a meta-analysis. Pain. (2022) 163:415–24. doi: 10.1097/j.pain.0000000000002365
80. Kudrow, D, Cady, RK, Allan, B, Pederson, SM, Hirman, J, Mehta, LR, et al. Long-term safety and tolerability of eptinezumab in patients with chronic migraine: a 2-year, open-label, phase 3 trial. BMC Neurol. (2021) 21:126. doi: 10.1186/s12883-021-02123-w
81. Smith, TR, Spierings, ELH, Cady, R, Hirman, J, Schaeffler, B, Shen, V, et al. Safety and tolerability of eptinezumab in patients with migraine: a pooled analysis of 5 clinical trials. J Headache Pain. (2021) 22:16. doi: 10.1186/s10194-021-01227-5
82. Yan, Z, Xue, T, Chen, S, Wu, X, Yang, X, Liu, G, et al. Different dosage regimens of Eptinezumab for the treatment of migraine: a meta-analysis from randomized controlled trials. J Headache Pain. (2021) 22:10. doi: 10.1186/s10194-021-01220-y
83. Baker, B, Schaeffler, B, Hirman, J, Hompesch, M, Pederson, S, and Smith, J. Tolerability of eptinezumab in overweight, obese or type 1 diabetes patients. Endocrinol Diabetes Metab. (2021) 4:e00217. doi: 10.1002/edm2.217
84. Rubio-Beltrán, E, and van den Brink, AM. Understanding CGRP and cardiovascular risk. Handb Exp Pharmacol. (2019) 255:131–40. doi: 10.1007/164_2019_204
85. Smith, TR, Spierings, ELH, Cady, R, Hirman, J, Ettrup, A, and Shen, V. Cardiovascular outcomes in adults with migraine treated with eptinezumab for migraine prevention: pooled data from four randomized, double-blind, placebo-controlled studies. J Headache Pain. (2021) 22:143. doi: 10.1186/s10194-021-01360-1
86. Pederson, S, Biondi, DM, Allan, B, Cady, R, Schaeffler, B, Baker, B, et al. Clinical immunogenicity evaluation of Eptinezumab, a therapeutic humanized monoclonal antibody targeting calcitonin gene-related peptide (CGRP) for the preventive treatment of migraine. Front Immunol. (2021) 12:765822. doi: 10.3389/fimmu.2021.765822
87. IRCCS San Raffaele Roma. EptinezuMaB in ReAl-world evidenCE: a 12 Week, Multicenter, Real Life, Cohort Study in Migraine (EMBRACE). Available at: https://clinicaltrials.gov/ct2/show/NCT05570149?recrs=b&cond=eptinezumab&draw=2&rank=1 (Accessed November 23, 2022).

Keywords: eptinezumab, clinical development, narrative review, chronic migraine, episodic migraine, preventive treatment, calcitonin gene-related peptide, fast onset of action
Citation: Irimia P, Santos-Lasaosa S, Pozo-Rosich P, Leira R, Pascual J and Láinez JM (2024) Eptinezumab for the preventive treatment of episodic and chronic migraine: a narrative review. Front. Neurol. 15:1355877. doi: 10.3389/fneur.2024.1355877
Edited by:
Willias Masocha, Kuwait University, KuwaitReviewed by:
Lars Neeb, Charité University Medicine Berlin, GermanyCopyright © 2024 Irimia, Santos-Lasaosa, Pozo-Rosich, Leira, Pascual and Láinez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo Irimia, cGlyaW1pYUB1bmF2LmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.