
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Neurol. , 24 January 2024
Sec. Dementia and Neurodegenerative Diseases
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1341661
 Jochum J. van’t Hooft1,2,3†
Jochum J. van’t Hooft1,2,3† Elia Benhamou1†
Elia Benhamou1† Claudia Albero Herreros1
Claudia Albero Herreros1 Jessica Jiang1†
Jessica Jiang1† Benjamin Levett1Lucy B. Core1Mai-Carmen Requena-Komuro1†
Benjamin Levett1Lucy B. Core1Mai-Carmen Requena-Komuro1† Chris J. D. Hardy1†Betty M. Tijms2,3†
Chris J. D. Hardy1†Betty M. Tijms2,3† Yolande A. L. Pijnenburg2,3†
Yolande A. L. Pijnenburg2,3† Jason D. Warren1*†
Jason D. Warren1*†Objectives: On phenotypic and neuroanatomical grounds, music exposure might potentially affect the clinical expression of behavioural variant frontotemporal dementia (bvFTD). However, this has not been clarified.
Methods: 14 consecutive patients with bvFTD fulfilling consensus diagnostic criteria were recruited via a specialist cognitive clinic. Earlier life musical experience, current musical listening habits and general socio-emotional behaviours were scored using a bespoke semi-quantitative musical survey and standardised functional scales, completed with the assistance of patients’ primary caregivers. Associations of musical scores with behavioural scales were assessed using a linear regression model adjusted for age, sex, educational attainment and level of executive and general cognitive impairment.
Results: Greater earlier life musical experience was associated with significantly lower Cambridge Behavioural Inventory (Revised) scores (β ± SE = −17.2 ± 5.2; p = 0.01) and higher Modified Interpersonal Reactivity Index (MIRI) perspective-taking scores (β ± SE = 2.8 ± 1.1; p = 0.03), after adjusting for general cognitive ability. Number of hours each week currently spent listening to music was associated with higher MIRI empathic concern (β ± SE = 0.7 ± 0.21; p = 0.015) and MIRI total scores (β ± SE = 1.1 ± 0.34; p = 0.014).
Discussion: Musical experience in earlier life and potentially ongoing regular music listening may ameliorate socio-emotional functioning in bvFTD. Future work in larger cohorts is required to substantiate the robustness of this association, establish its mechanism and evaluate its clinical potential.
While it is well established that musical expertise can shape brain structure and function (1, 2), the potential of music to modify the clinical expression of neurodegenerative brain pathologies has been largely unexplored. Limited evidence suggests that training on a musical instrument may benefit cognitive task performance in domains such as executive function and verbal memory, and may enhance the task-related functional connectivity of neural networks (3–5). Moreover, musicians may have a reduced incidence of dementia (6, 7). However, the mechanism of any protective effect and its disease specificity have not been clarified.
On neurobiological as well as clinical grounds, this issue may be particularly pertinent in the behavioural variant of frontotemporal dementia (bvFTD). This syndrome typically presents with impaired social and emotional awareness, empathy and perspective taking, accompanied by diverse abnormal behaviours including disinhibition, impulsivity, tactlessness, mental rigidity, obsessionality, perseveration and inertia (8). Music processing and social cognition engage common neural mechanisms, and these same mechanisms are targeted early and relatively selectively in bvFTD (9, 10). Long-term musical exposure is associated both with enhanced emotion recognition (11) and increased connectivity and functional integration in the salience network (1), a core target of the pathological process in bvFTD. This is in line with other work suggesting that certain occupational and lifestyle exposures may attenuate the phenotypic impact of bvFTD (12). Further, developmental amusia (‘tone deafness’) is associated with deficits of social signal processing in otherwise cognitively normal adults (13). Taken together, such evidence suggests that musical experience might modulate vulnerability to the clinical expression of bvFTD, putatively via effects on neural network resilience and reserve (12, 14).
Here we addressed whether past musical experience, current musical listening habits and/or musical perceptual skills affect the phenotypic expression of bvFTD. We studied a well-characterised bvFTD cohort, assessing patients musically using a customised caregiver survey and cognitive tests. Based on available evidence (1, 2, 9, 10, 12), we hypothesised that cumulative past musical experience would modulate behavioural symptoms of socio-emotional dysfunction in patients with bvFTD, independently of effects on general executive and other cognitive abilities.
Fourteen consecutive patients with bvFTD were recruited via a national tertiary referral centre in London, United Kingdom. All fulfilled consensus diagnostic criteria for bvFTD (8), supported by a comprehensive clinical, neuropsychological and behavioural assessment (Table 1) and brain MRI showing a compatible profile of atrophy. Exclusion criteria comprised inability to understand English or give informed consent, or neurological or psychiatric comorbidities. To interpret the clinical and musical profile of the bvFTD cohort, patients were referenced to a historical cohort of 29 demographically similar, healthy older British adults (details in Table 1), who had been assessed on the same musical, behavioural and neuropsychological measures. No patient had a disease-causing genetic mutation. None was known to have had premorbid developmental amusia.
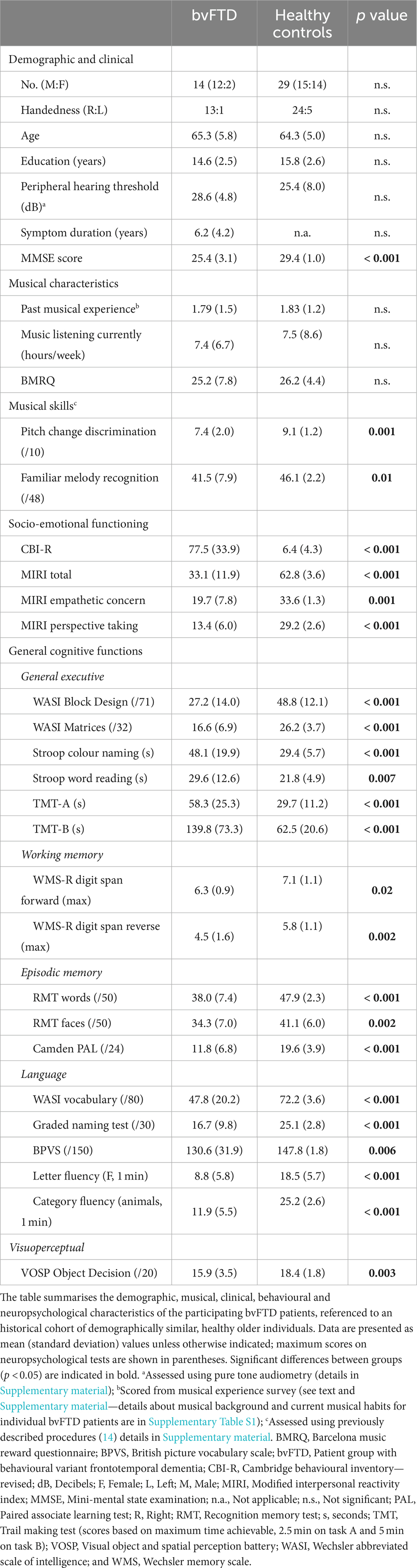
Table 1. Characteristics of the bvFTD group relative to healthy older individuals.
The study was approved by UCL/UCLH Joint Research Ethics Committee, and all patients gave informed consent to participate, in line with Declaration of Helsinki guidelines.
Patients’ past musical experience and current musical listening habits were assessed using a structured survey (see details in Supplementary material). Past experience of playing an instrument or singing was scored on a five-point scale, ranging from 0 (no past experience) to 4 (United Kingdom grade 7 or 8 qualification on an instrument or for singing). The estimated average number of hours the patient currently spent listening to music each week was also recorded. In addition, we administered the Barcelona Music Reward Questionnaire (BMRQ) (15), an index of pleasure in music. Musical survey information was gathered from and/or endorsed by each patient’s long-term primary caregiver.
To determine patients’ current musical skills, we administered tests assessing discrimination of pitch change direction and familiar melody recognition, using previously described procedures (14) (details in Supplementary material).
Behavioural changes and socio-emotional cognition were assessed using standardised informant-based questionnaires. Patients’ primary caregivers completed the Cambridge Behavioural Inventory (Revised) (CBI-R) (16), an index of general neurobehavioural and psychiatric symptoms; and the Modified Interpersonal Reactivity Index (MIRI) (17), an index of empathy and perspective taking. Whereas higher CBI-R score reflects more behavioural impairment, higher MIRI score reflects better socio-emotional functioning.
Statistical analyses were performed in R (v4.1.0). Demographic and clinical characteristics were investigated using T-tests and chi-squared tests where appropriate. Associations of past musical experience (survey scores), current music listening (hours spent listening to music each week), and musical test (pitch discrimination, melody recognition) scores with demographic and socio-emotional behavioural measures (separately for each of the subscales of the MIRI) were assessed within the bvFTD group using linear regressions. The analyses were repeated in the healthy control group to investigate the robustness of the associations. In the regression model, we adjusted for age, sex, years of formal education and measures of overall cognitive functioning (Mini-Mental State Examination score) and general executive function (WASI Block Design score). We also assessed the associations of patients’ musical experience with each of the neuropsychological tests (as a control for nonspecific disease effects). Results were plotted using lines of best fit based on Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC). A threshold p < 0.05 was accepted as the criterion for statistical significance in all analyses.
Demographic, musical, clinical, neuropsychological and behavioural characteristics of the bvFTD group are summarised in Table 1 (referenced to an historical cohort of healthy older individuals). Patients exhibited typical clinical and neuropsychological profiles of bvFTD.
Information about musical background and current musical listening habits for individual bvFTD patients are presented in Supplementary Table S1. While most patients had received at least some musical training, individual patients ranged widely in past musical experience: one had been a professional musician and four had never played an instrument. Caregiver survey responses further indicated considerable variation of current music listening within the bvFTD group, including patients who had developed musicophilia and music aversion as part of their illness. Overall, however, the patient group had similar musical characteristics to the historical healthy control cohort (Table 1). Patients as a group performed significantly worse than healthy controls on tests assessing current musical (pitch discrimination and melody recognition) skills.
Correlations of past musical experience with other cognitive and behavioural measures in the bvFTD group are presented in Figure 1 and Table 2. Within the bvFTD group, a higher past musical experience score was associated with significantly lower CBI-R score (β ± SE = −17.2 ± 5.2; 95% CI [−5.2, −29.3]; BIC/AIC = 134/129; R2 = 0.79; p = 0.01) and higher MIRI perspective-taking subscore (β ± SE = 2.8 ± 1.1; 95% CI [0.3, 5.3]; BIC/AIC = 90/85; R2 = 0.71; p = 0.03). Greater past musical experience was also significantly associated with higher number of hours currently spent listening to music each week (β ± SE = 4.02 ± 1.55; 95% CI [0.5, 7.6]; BIC/AIC = 100/95; R2 = 0.52; p = 0.03), and with better performance on the pitch discrimination test (β ± SE = 1.2 ± 0.27; 95% CI [0.6, 1.9]; BIC/AIC = 51/47; R2 = 0.82; p = 0.0019). Past musical experience was not associated with performance on general neuropsychological tests (all p > 0.05). In particular, there was no association with performance on standard tests of executive function (Table 2). When repeating regression analyses in the normal older control group, no significant associations were found (all p > 0.05, Supplementary Table S2).
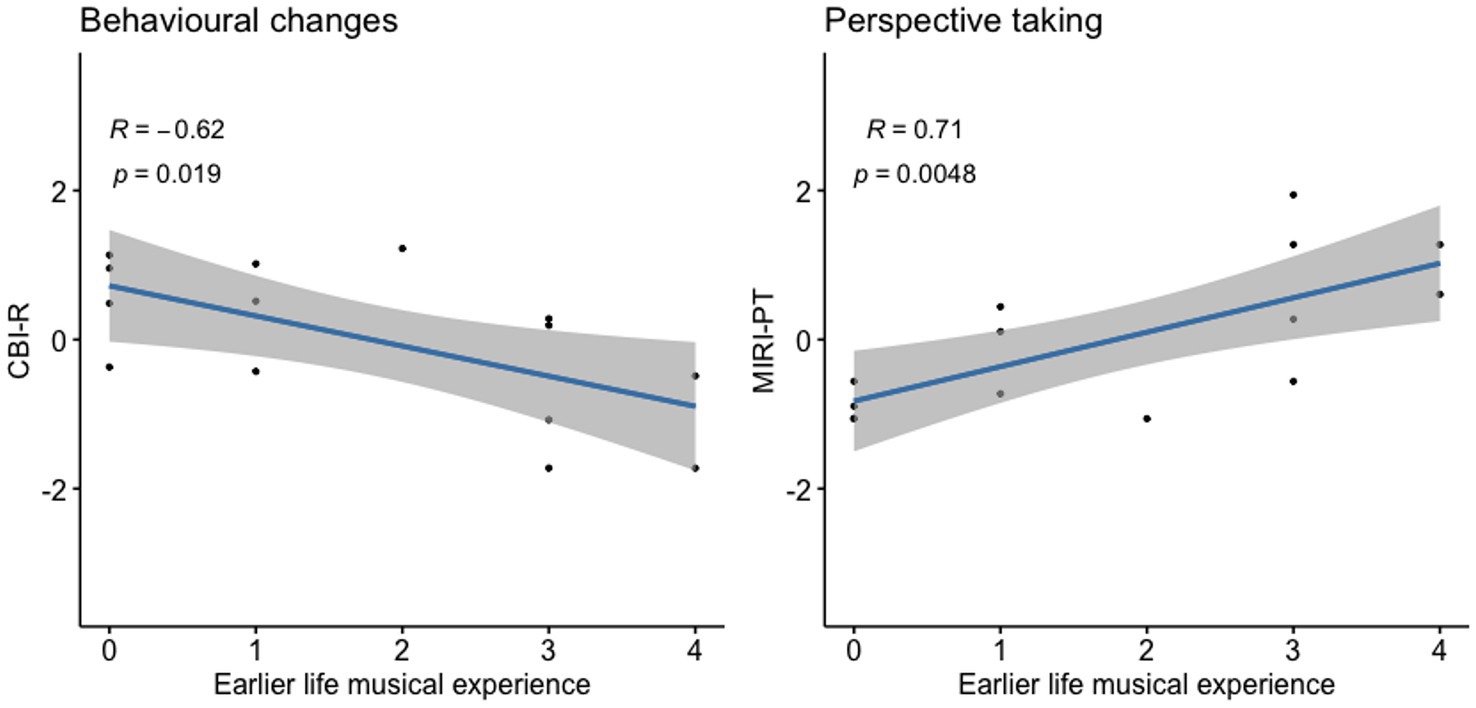
Figure 1. Association of past musical experience with socio-emotional functioning in bvFTD. Scores of individual bvFTD patients on standard measures of daily life socio-emotional functioning vs. their scores on our earlier life musical experience survey (graded between 0 and 4; see text and Supplementary material) are plotted, with lines of best fit and 95% confidence envelopes. CBI-R and MIRI-PT scores are z-transformed; Pearson correlations with corresponding p values are indicated on the plots. bvFTD, Patient group with behavioural variant frontotemporal dementia; CBI-R, Cambridge behavioural inventory—revised; and MIRI-PT, modified interpersonal reactivity index—perspective taking.
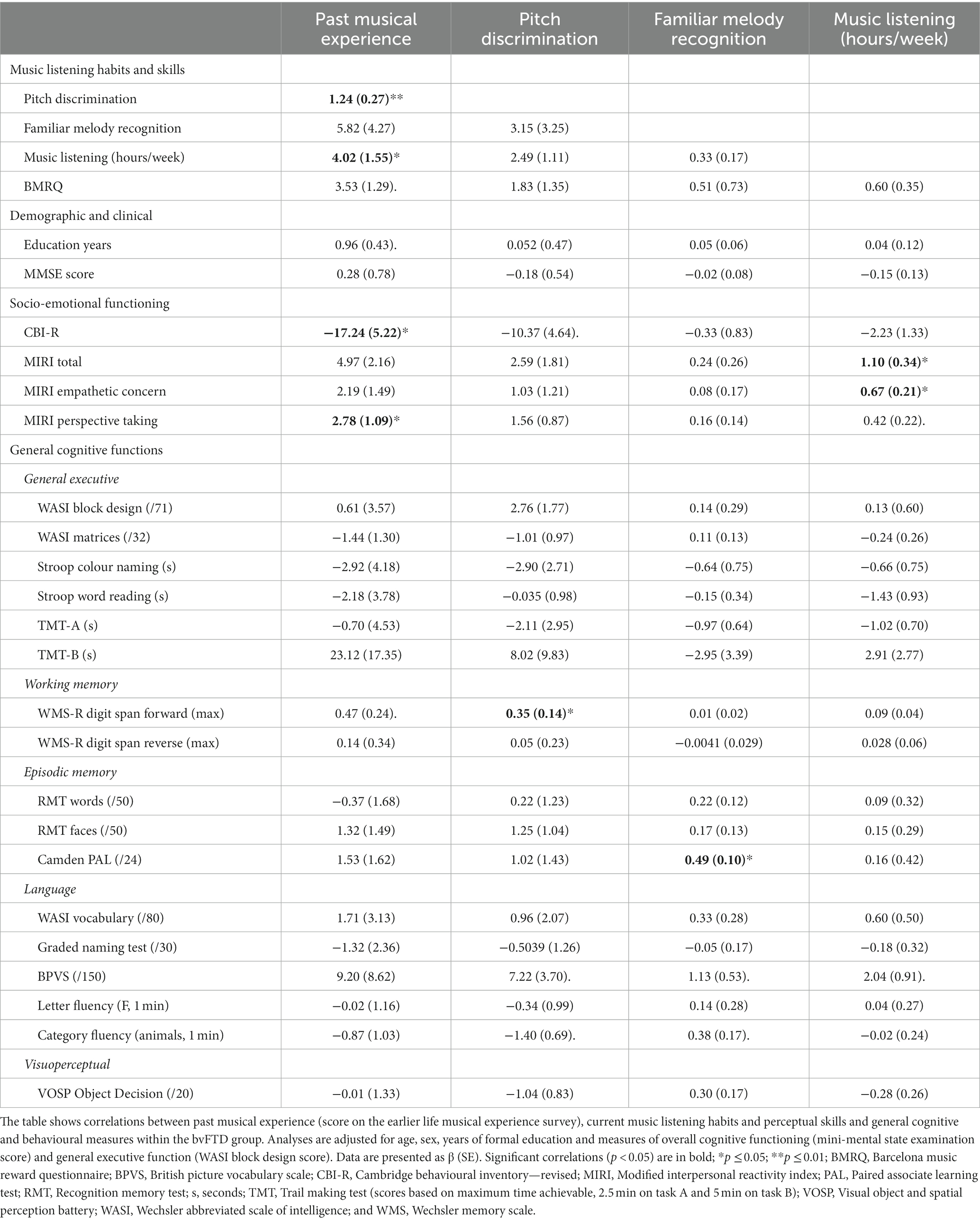
Table 2. Associations of past musical experience and current musical listening habits and skills with socio-emotional and neuropsychological measures in bvFTD.
Current music listening (higher number of hours per week) was significantly associated with higher MIRI empathic concern (β ± SE = 0.7 ± 0.21; BIC/AIC = 92/87; 95% CI [0.2, 1.2]; R2 = 0.84; p = 0.015) and MIRI total scores (β ± SE = 1.1 ± 0.34; 95% CI [0.3, 1.9]; BIC/AIC 105/100; R2 = 0.81; p = 0.014; Figure 2) but not with performance on general neuropsychological tests (all p > 0.05). Scores on tests assessing musical skills (pitch discrimination, melody recognition) were not significantly associated with CBI-R or MIRI scores in the bvFTD cohort (all p > 0.05). Pitch discrimination scores were significantly associated with a standard measure of auditory working memory, digit span forward (β ± SE = 0.35 ± 0.14; 95% CI [0.01, 0.7]; BIC/AIC = 44/38; R2 = 0.61; p = 0.045), while melody recognition performance was significantly associated only with a measure of episodic memory, paired associate learning (β ± SE = 0.49 ± 0.10; 95% CI [0.05, 0.9]; BIC/AIC = 37/36; R2 = 0.98; p = 0.042). When repeating regression analyses in the normal older control group, no significant associations were found (all p > 0.05, Supplementary Table S2).
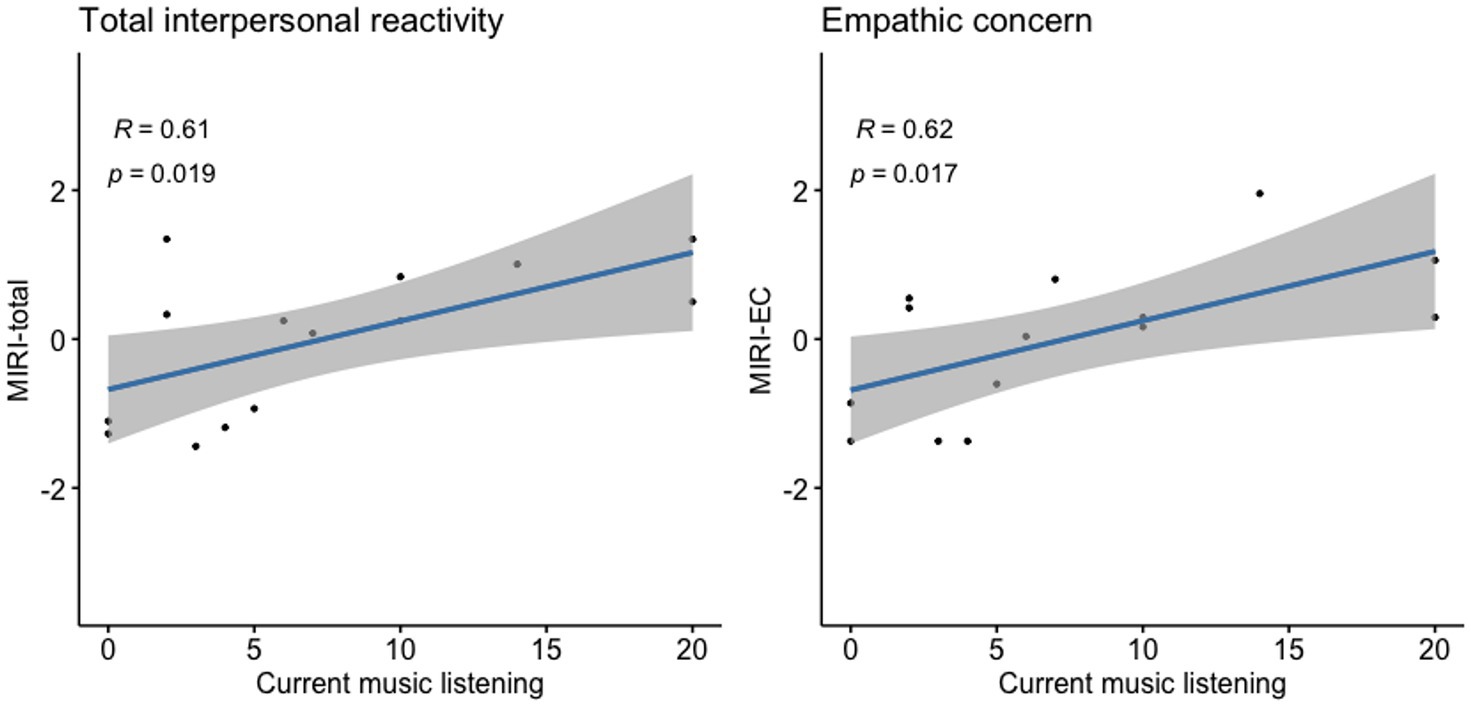
Figure 2. Association of current music listening with socio-emotional functioning in bvFTD. Scores of individual bvFTD patients on standard measures of daily life socio-emotional functioning versus their scores on our earlier life musical experience survey (graded between 0 and 4; see text and Supplementary material) are plotted, with lines of best fit and 95% confidence envelopes. MIRI-total and MIRI-EC scores are z-transformed; Pearson correlations with corresponding p values are indicated on the plots. bvFTD, Patient group with behavioural variant frontotemporal dementia; MIRI-EC, Modified interpersonal reactivity index—empathic concern; and MIRI-total, Modified interpersonal reactivity index—total score.
In this preliminary study, we have shown that greater earlier life musical experience and current regular listening to music (but not musical processing skills) correlate with lower levels of socio-emotional behavioural disturbance in a group of patients with bvFTD, after taking potentially confounding demographic, clinical and cognitive variables into account. This effect was not found in other, extra-musical cognitive domains, suggesting it may be specific for socio-emotional function, and in particular ‘theory of mind’ or awareness of others’ mental states (the MIRI domains of perspective-taking and empathic concern). We speculate that earlier life musical experience may be protective in bvFTD, perhaps by promoting resilience in brain circuits mediating behavioural regulation and theory of mind (1, 13): both key elements of interpersonal conduct in daily life.
These findings corroborate emerging evidence that musical training and other specific competencies in earlier life may influence the phenotypic expression of dementia (7, 12) and further align with previous work suggesting that music plays a role in building social cognitive skills during brain development (13). Further, we found that more regular current music listening was associated with higher empathic concern and overall interpersonal reactivity. These findings underline the potential value of continuing music listening to enhance socio-emotional engagement in dementia (18). Future studies should additionally investigate the effects of continued musical performance, engaging in inter-personal musical activities and active music-based interventions on socio-emotional functioning in bvFTD, and extend the investigation both in healthy older individuals and in patients with different dementia syndromes. It should be noted, however, that current music listening was here also positively correlated with past musical experience, raising the possibility that earlier life musical training primes later life listening habits, and thereby drives any ongoing beneficial effect from music listening. On the other hand, socio-emotional functioning did not correlate with level of musical perceptual skill. The interplay of these factors is not resolved by the current study. When repeating the regression analyses in the healthy older control group we found no associations of musical experience with socio-emotional functioning. This might reflect the limited range and sensitivity of socio-emotional measures in cognitively healthy people, and replication in larger cohorts are required for robust associations.
There are several important caveats on the interpretation of our findings. This is a small patient sample, and musical characteristics were assessed in part from potentially biassed or inaccurate caregiver reports. Furthermore, other non-musical factors (e.g., ethnic, cultural and linguistic) may influence behavioural outcomes in bvFTD (19), and were not accounted for here. Our results await prospective replication in larger, more diverse cohorts, with more detailed analysis of potentially relevant (or confounding) musical as well as demographic and clinical variables. There is a need to disambiguate the effects of past musical experience from current musical listening habits, particularly in planning musical interventions for people with established dementia. Notwithstanding the small cohort size, it is noteworthy that the inverse associations here between past musical experience, current music listening and socio-emotional dysfunction in bvFTD were robust to adjustments for potentially confounding executive and general cognitive factors. Moreover, none of the general cognitive measures sampled showed a significant association with past musical exposure or current music listening (Table 2). Earlier life musical exposure is, however, likely to correlate with a range of other non-musical characteristics and exposures that remain to be defined; nor is musical training (the main proxy for musical experience here) a prerequisite for musicality. More fundamentally, association does not establish causation: people with innately more resilient behavioural regulation and social cognition circuitry might be more likely to learn a musical instrument, or continue listening regularly to music. The socio-emotional benefits of musical training remain poorly understood, and causal relations could be further investigated with alternative indices of musicality and prospective longitudinal studies (11, 20).
Acknowledging these caveats, we hope that our findings will motivate further studies of musicality as a possible modulatory factor in FTD and other dementias—to clarify the nature of the modulatory effect, to establish its neural basis using functional and connectivity-based neuroimaging, and to explore its clinical potential. Analogous with the proposed link between developmental language disorders and primary progressive aphasia (21), one might ask whether the common complaint of developmental amusia (13) confers an increased vulnerability to FTD—and whether cumulative past musical engagement and indeed, continuing regular music listening or music-based behavioural interventions might ameliorate the impact of the disease.
The data analysed in this study are subject to the following licences/restrictions: we used patient datasets of the Dementia Research Centre. Requests to access these datasets should be directed to JW, amFzb24ud2FycmVuQHVjbC5hYy51aw==.
The study was approved by UCL/UCLH Joint Research Ethics Committee, reference number 06N032. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JH: Conceptualization, Formal Analysis, Investigation, Software, Visualization, Writing – original draft, Writing – review & editing. EB: Data curation, Writing – review & editing. CA: Data curation, Writing – review & editing. JJ: Data curation, Writing – review & editing. BL: Writing – review & editing. LC: Writing – review & editing. M-CR-K: Data curation, Writing – review & editing. CH: Writing – review & editing. BT: Writing – review & editing. YP: Writing – review & editing. JW: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The Dementia Research Centre is supported by Alzheimer’s Research United Kingdom, Brain Research UK, and the Wolfson Foundation. This work was supported by the Alzheimer’s Society, Alzheimer’s Research UK, the National Institute for Health Research University College London Hospitals Biomedical Research Centre, and the Royal National Institute for Deaf People. JH was supported by the Dutch Alzheimer’s association and the Dutch Alzheimer rally. EB was supported by a Brain Research UK PhD Studentship. JJ was supported by the National Brain Appeal (Frontotemporal Dementia Research PhD Studentship in Memory of David Blechner). M-CR-K was supported by a Wellcome Trust 4-year PhD Studentship in Neuroscience (102129/B/13/Z). CH has been supported by an RNID–Dunhill Medical Trust Pauline Ashley Fellowship (PA23_Hardy) and a Wellcome Institutional Strategic Support Fund (204841/Z/16/Z). JW receives grant support from Alzheimer’s Research UK, the Alzheimer’s Society, the Royal National Institute for Deaf People and the National Institute for Health and Care Research and UCL Music Futures.
We thank all participants and caregivers for their involvement.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1341661/full#supplementary-material
1. Luo, C, Tu, S, Peng, Y, Gao, S, Li, J, Dong, L, et al. Long-term effects of musical training and functional plasticity in salience system. Neural Plast. (2014) 2014:180138. doi: 10.1155/2014/180138
2. Penhune, VB. Understanding sensitive period effects in musical training. Curr Top Behav Neurosci. (2022) 53:167–88. doi: 10.1007/7854_2021_250
3. Guo, X, Yamashita, M, Suzuki, M, Ohsawa, C, Asano, K, Abe, N, et al. Musical instrument training program improves verbal memory and neural efficiency in novice older adults. Hum Brain Mapp. (2021) 42:1359–75. doi: 10.1002/hbm.25298
4. Wang, X, Soshi, T, Yamashita, M, Kakihara, M, Tsutsumi, T, Iwasaki, S, et al. Effects of a 10-week musical instrument training on cognitive function in healthy older adults: implications for desirable tests and period of training. Front Aging Neurosci. (2023) 15:1180259. doi: 10.3389/fnagi.2023.1180259
5. Yamashita, M, Ohsawa, C, Suzuki, M, Guo, X, Sadakata, M, Otsuka, Y, et al. Neural advantages of older musicians involve the cerebellum: implications for healthy aging through lifelong musical instrument training. Front Hum Neurosci. (2021) 15:784026. doi: 10.3389/fnhum.2021.784026
6. Verghese, J, Lipton, RB, Katz, MJ, Hall, CB, Derby, CA, Kuslansky, G, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med. (2003) 348:2508–16. doi: 10.1056/NEJMoa022252
7. Walsh, S, Causer, R, and Brayne, C. Does playing a musical instrument reduce the incidence of cognitive impairment and dementia? A systematic review and meta-analysis. Aging Ment Health. (2021) 25:593–601. doi: 10.1080/13607863.2019.1699019
8. Rascovsky, K, Hodges, JR, Knopman, D, Mendez, MF, Kramer, JH, Neuhaus, J, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain. (2011) 134:2456–77. doi: 10.1093/brain/awr179
9. Clark, CN, Downey, LE, and Warren, JD. Brain disorders and the biological role of music. Soc Cogn Affect Neurosci. (2015) 10:444–52. doi: 10.1093/scan/nsu079
10. Van’t Hooft, JJ, Pijnenburg, YAL, Sikkes, SAM, Scheltens, P, Spikman, JM, Jaschke, AC, et al. Frontotemporal dementia, music perception and social cognition share neurobiological circuits: a meta-analysis. Brain Cogn. (2021) 148:105660. doi: 10.1016/j.bandc.2020.105660
11. Correia, AI, Castro, SL, Macgregor, C, Müllensiefen, D, Schellenberg, EG, Lima, CF, et al. Enhanced recognition of vocal emotions in individuals with naturally good musical abilities. Emotion (2022) 22:894–906. doi: 10.1037/emo0000770
12. Dodich, A, Carli, G, Cerami, C, Iannaccone, S, Magnani, G, and Perani, D. Social and cognitive control skills in long-life occupation activities modulate the brain reserve in the behavioural variant of frontotemporal dementia. Cortex. (2018) 99:311–8. doi: 10.1016/j.cortex.2017.12.006
13. Lima, CF, Brancatisano, O, Fancourt, A, Müllensiefen, D, Scott, SK, Warren, JD, et al. Impaired socio-emotional processing in a developmental music disorder. Sci Rep. (2016) 6:34911. doi: 10.1038/srep34911
14. Benhamou, E, Zhao, S, Sivasathiaseelan, H, Johnson, JCS, Requena-Komuro, MC, Bond, RL, et al. Decoding expectation and surprise in dementia: the paradigm of music. Brain Commun. (2021) 3:fcab173. doi: 10.1093/braincomms/fcab173
15. Mas-Herrero, E, Marco-Pallares, J, Lorenzo-Seva, U, Zatorre, RJ, and Rodriguez-Fornells, A. Individual differences in music reward experiences. Music Percep Interdiscip J. (2012) 31:118–38.
16. Wear, HJ, Wedderburn, CJ, Mioshi, E, Williams-Gray, CH, Mason, SL, Barker, RA, et al. The Cambridge Behavioural inventory revised. Dement Neuropsychol. (2008) 2:102–7. doi: 10.1590/S1980-57642009DN20200005
17. Foster, PH, Russell, LL, Peakman, G, Convery, RS, Bouzigues, A, Greaves, CV, et al. Examining empathy deficits across familial forms of frontotemporal dementia within the GENFI cohort. Cortex. (2022) 150:12–28. doi: 10.1016/j.cortex.2022.01.012
18. Van Der Steen, JT, Smaling, HJA, Van Der Wouden, JC, Bruinsma, MS, Scholten, RJPM, and Vink, AC. Music-based therapeutic interventions for people with dementia. Cochrane Database Syst Rev. (2018) 2018:CD003477. doi: 10.1002/14651858.CD003477.pub4
19. Skeggs, A, Wei, G, Landin-Romero, R, Hodges, JR, Piguet, O, and Kumfor, F. The influence of culture and cognitive reserve on the clinical presentation of behavioural-variant frontotemporal dementia. J Neurol. (2023) 270:3192–203. doi: 10.1007/s00415-023-11638-w
20. Schellenberg, EG, and Lima, CF. Music training and nonmusical abilities. Annu Rev Psychol. (2023). doi: 10.1146/annurev-psych-032323-051354
Keywords: musical training, musician, music, frontotemporal dementia, social cognition, behaviour
Citation: van’t Hooft JJ, Benhamou E, Albero Herreros C, Jiang J, Levett B, Core LB, Requena-Komuro M-C, Hardy CJD, Tijms BM, Pijnenburg YAL and Warren JD (2024) Musical experience influences socio-emotional functioning in behavioural variant frontotemporal dementia. Front. Neurol. 15:1341661. doi: 10.3389/fneur.2024.1341661
Edited by:
Görsev Yener, İzmir University of Economics, TürkiyeReviewed by:
Zara Thompson, The University of Melbourne, AustraliaCopyright © 2024 van’t Hooft, Benhamou, Albero Herreros, Jiang, Levett, Core, Requena-Komuro, Hardy, Tijms, Pijnenburg and Warren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jason D. Warren, amFzb24ud2FycmVuQHVjbC5hYy51aw==
†ORCID: Jochum J. van’t Hooft, https://orcid.org/0000-0001-6917-5173
Elia Benhamou, https://orcid.org/0000-0003-0194-7995
Jessica Jiang, https://orcid.org/0000-0002-7074-3032
Mai-Carmen Requena-Komuro, https://orcid.org/0000-0002-5624-0527
Chris J. D. Hardy, https://orcid.org/0000-0002-4900-6492
Betty M. Tijms, https://orcid.org/0000-0002-2612-1797
Yolande A. L. Pijnenburg, https://orcid.org/0000-0003-2464-1905
Jason D. Warren, https://orcid.org/0000-0002-5405-0826
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.