 João Moura1,2*†
João Moura1,2*† Joana Fernandes1Maria João Lima3Ana Paula Sousa4
Joana Fernandes1Maria João Lima3Ana Paula Sousa4 Raquel Samões1,2,5
Raquel Samões1,2,5 Ana Martins Silva1,2,5
Ana Martins Silva1,2,5 Ernestina Santos1,2,5
Ernestina Santos1,2,5- 1Department of Neurology, Centro Hospitalar Universitário de Santo António, Porto, Portugal
- 2Unit of Multidisciplinary Research in Biomedicine (UMIB), Instituto de Ciências Biomédicas Abel Salazar (ICBAS), University of Porto, Porto, Portugal
- 3Department of Neurology, Unidade Local de Saúde de Matosinhos, Porto, Portugal
- 4Department of Neurophysiology, Hospital de Santo António, Centro Hospitalar Universitário Do Porto, Porto, Portugal
- 5Laboratory for Integrative and Translational Research in Population Health (ITR), Porto, Portugal
Introduction: Early-onset (EOMG) and late-onset (LOMG) are distinct groups of MG patients. It is unclear if treatment strategies and treatment-related adverse events may differ according to the age of MG onset.
Methods: This single-center retrospective study includes all MG patients followed at a tertiary center since 2007. We reviewed the electronic clinical records.
Results: In total, 212 patients were identified, 142 (67.0%) females, with a median disease duration of 10 years. The median age of symptom onset was 42.0 (26.0–64.5) years, with 130 (61.3%) EOMG cases and 82 (38.7%) LOMG. EOMG were more frequently female, had longer disease duration and often more generalized MG (p < 0.001). Comorbidities were significantly more frequent in LOMG (67.1%) compared to EOMG (53.1%) (p = 0.002). Steroid-related adverse effects motivating the switch to steroid-sparing agents (82.0%) were different between groups, with hypertension, hypercholesterolemia, diabetes mellitus and malignancies being more common in LOMG. At the same time, osteoporosis and dyspepsia were more frequent in EOMG (p < 0.001). The most common first-line choice was azathioprine (45.8%), and rituximab was used in 4 patients (1.9%).
Conclusion: Our study shows that treatment modalities are similar between EOMG and LOMG, while steroid-related adverse events appear to be distinct.
Introduction
Myasthenia gravis (MG) is a chronic autoimmune neuromuscular disease characterized by ocular and generalized muscle weakness. This disorder has a heterogeneous pathogenesis and variable phenotype associated with distinct disease subtypes (1, 2). When considering the age of onset, patients <50 years are considered early-onset MG (EOMG), while patients with disease onset above 50 years belong to the late-onset MG group (LOMG).
Classically, treatment response is considered satisfactory in MG. The approval of novel immunosuppressive drugs to treat MG cases offers the opportunity to tailor the treatment to each patient. Baseline comorbidities and treatment-related side effects are essential aspects to consider in this process (3). Some studies suggest that EOMG and LOMG may differ in these characteristics (4, 5). However, it is still unclear if treatment-related adverse events are associated with the age of MG onset.
This study aims to describe a MG cohort and evaluate comorbidities, treatment strategies and treatment-related adverse events between EOMG and LOMG.
Methods
We retrospectively analyzed the medical records of MG patients from an institutional database that contains all MG cases followed in the Centro Hospitalar Universitario de Santo António Neuroimmunology Outpatient Clinic. This database is updated annually since 2007. MG was diagnosed by practicing neurologists specialized in neuroimmunology (ES, AMS, APS, and RS) based on a combination of clinical features, neurophysiological studies, antibody testing and response to pyridostigmine (2). Patients aged <50 years were classified as EOMG, while patients ≥50 years were considered LOMG (1).
We collected information concerning sex, age of onset and age at diagnosis. We extracted data on the prevalence of different comorbidities using what was defined in previous studies. Comorbidities were classified as treatment-related if they appeared after the initiation of a specific treatment and if the neurologist considered the comorbidity an effect of treatment, according to the medical records. The baseline Myasthenia Gravis Foundation of America (MGFA) score and the occurrence of myasthenic crisis or hospital admission due to MG during the disease course were retrospectively collected. Data on the use of anticholinesterases (and maximum dose), steroids (and maximum dose), and other immunosuppressors used during the disease course was additionally detailed.
Qualitative variables were studied using absolute and relative frequencies. The median and interquartile range (p25–p75) (IQR) were calculated for quantitative variables. An X2 was used to compare categorical variables, while a Mann–Whitney U test was used for continuous variables. Statistical analysis was performed in SPSS Statistics version 29. A p-value < 0.05 was considered statistically significant.
This study was approved by Centro Hospitalar Universitário de Santo António Ethical Committee. Informed consent was waived due to the retrospective nature of the study.
Results
In total, 212 patients were identified, 103 (79.2%) female. The median disease duration was ten years, and the median follow-up time was 8 years. The median age of symptom onset was 42.0 (26.0–64.5) years, with 130 (61.3%) EOMG cases and 82 (38.7%) LOMG. Table 1 summarizes the characteristics of the cohort. Overall, EOMG were more frequently female and had longer disease duration. MG phenotypes were significantly different between groups, with EOMG patients having significantly more generalized MG (80.0% vs. 56.1%) and LOMG patients having more ocular MG (43.9% vs. 20.0%) (p < 0.001). Figure 1 shows the distribution of baseline MGFA scores concerning the age of onset.
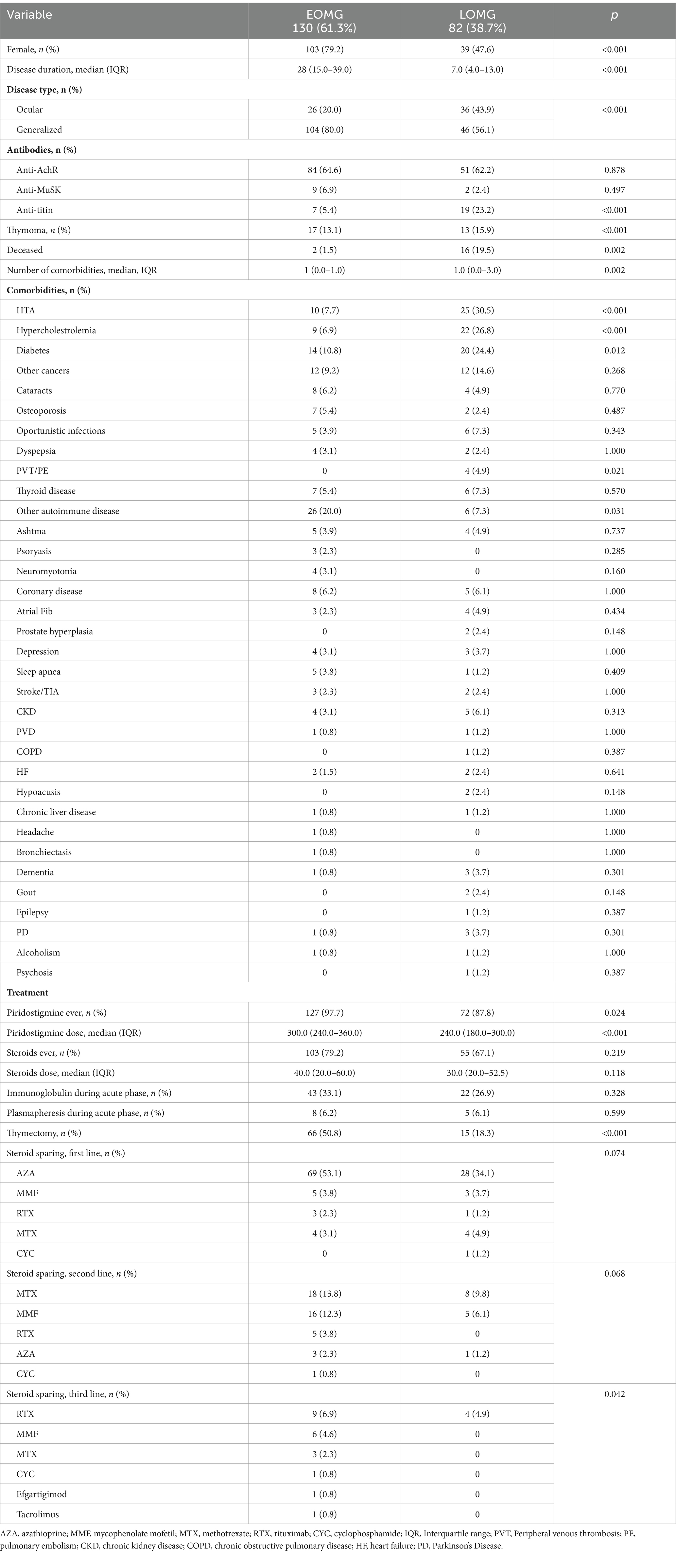
Table 1. Characterization of the MG cohort according to age of onset.
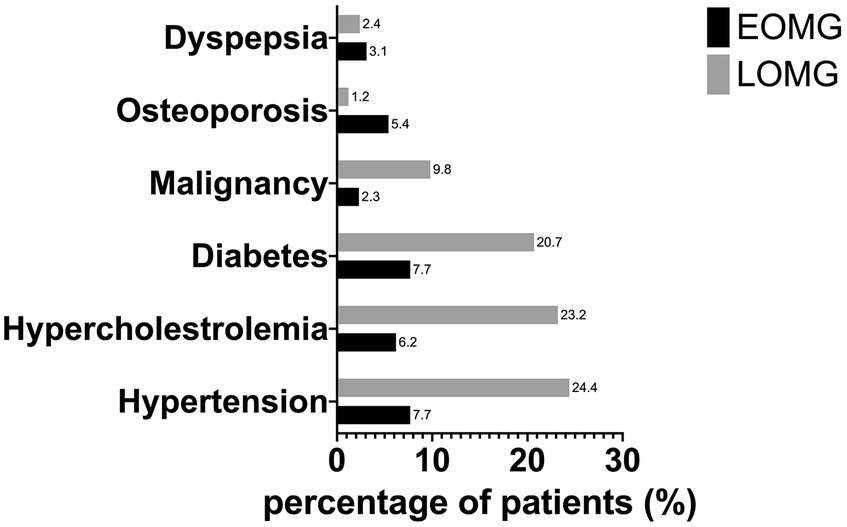
Figure 1. Distribution of MGFA scores according to the age of onset.
At least one comorbidity was present in 124 patients (58.5%), with a median of 1.0 (0.0–2.0) comorbidity per patient. Comorbidities were significantly more frequent in LOMG (67.1%) compared to EOMG (53.1%) (p = 0.002). In particular, arterial hypertension, dyslipidemia, diabetes mellitus and venous thromboembolism were significantly more associated with LOMG, as shown in Table 1. Patients with and without thymomas had a similar number of comorbidities (p = 0.582).
Fifty patients (23.6%) had at least one myasthenic crisis requiring acute treatment throughout the disease course. There was no difference concerning age of onset (26.1% EOMG vs. 19.5% LOMG, p = 0.320). In total, 41 (19.3%) patients required hospital admission due to MG exacerbations, 20 EOMG (16.1%) and 21 LOMG (25.6%) (p = 0.335). Regarding the treatment regimens, pyridostigmine was offered to 93.9% of patients, with significantly more EOMG patients receiving treatment (p = 0.024). The median highest dose of anticholinesterase was 300.0 (240.0–360.0), which was higher in EOMG compared to LOMG (300.0 versus 240.0, p < 0.001). Acute treatment modalities comprised human immunoglobulin (30.7%) and plasmapheresis (6.1%). Steroids were used in 74.5% of patients, with 15.6% requiring prednisolone as part of maintenance treatment. Treatment-related side effects were the most common reason for choosing a steroid-sparing agent (82.0%). From these, hypertension, hypercholesterolemia, diabetes mellitus and malignancies were more common in LOMG, while osteoporosis and dyspepsia were more frequent in EOMG (p < 0.001) (Figure 2).
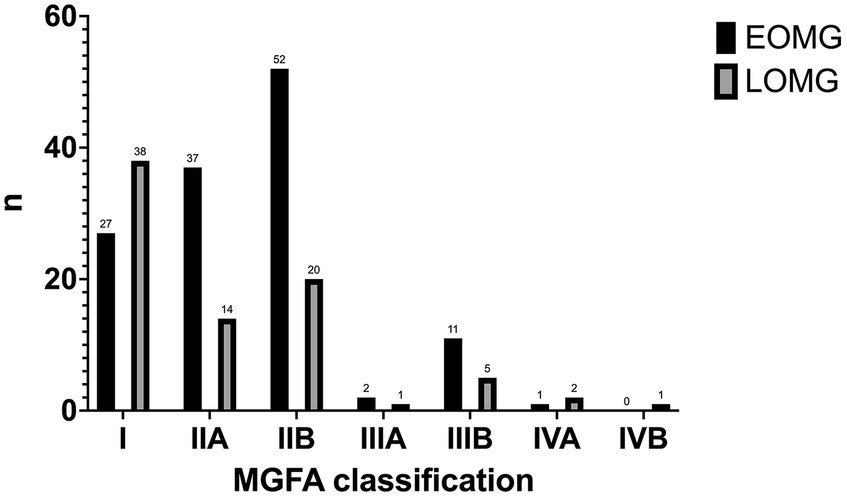
Figure 2. Adverse effects associated with steroids in EOMG and LOMG.
Most patients were switched to steroid-sparing agents, with the most common first-line choice being azathioprine (45.8%). Rituximab was used as a first-line option in 4 patients (1.9%): 2 anti-MuSK-associated MG cases, 1 with comorbid autoimmune disease and 1 EOMG case with an aggressive course. There was no significant difference between EOMG and LOMG regarding first-line options. Second-line immunotherapy was required in 26.9%, mainly for improving disease control (85.8%). Treatment-related adverse events motivating a therapy switch to second-line agents (3.8%) included hepatitis (2.4%), repeated infections (0.9%) and pancytopenia (0.5%). The most common second and third-line agents were methotrexate (12.3%) and rituximab (6.1%), respectively. Tocilizumab (0.5%) and efgartigimod (0.5%) were only used as third-line alternatives in EOMG cases. Thymectomy was performed in 81 (38.2%) patients, more frequently in EOMG (81.5%) than LOMG (18.5%). The median time to thymectomy was 1.0 (1.0–3.0) years. Thymoma was identified in 30 (14.2%), most commonly of type 2B (53.3%), while hyperplasia was present in the remaining patients. Although more thymomas being identified in EOMG (56.7% vs. 43.3%), this difference was not statistically significant.
Discussion
This study underscores the importance of considering the age of MG onset and comorbidities in treatment selection.
Overall, our MG cohort follows what is described in the literature for EOMG concerning female predominance and tendency toward generalized disease (1, 6). Thymomas were more frequently found in LOMG cases (p < 0.001), which is consistent with the literature (7). However, patients proposed for thymectomy were already the ones with an increased probability of having a thymoma based on imaging studies, which could introduce bias.
In our cohort, most MG patients had at least one comorbidity (approximately 59%), these being more frequent in LOMG cases. LOMG had significantly more comorbidities, particularly comorbidities associated with increased cardiovascular risk (arterial hypertension, dyslipidemia, and diabetes mellitus), consistent with previous reports (4). However, we could not exclude that these resulted from older age and not disease type. A previous study compared age-and sex-matched groups of EOMG and LOMG and found no significant differences, consistent with comorbidities probably resulting from the cumulative effect of increased aged than with MG type (5). Some conditions like dyslipidemia and hypertension may be particularly bothersome in MG since some treatment options (statins and beta-blockers) might worsen MG symptoms (8).
Steroid-related adverse effects motivating treatment change were frequent, consistent with the general recommendations for corticotherapy. However, the profile of side effects differs between LOMG and EOMG. Steroid-treated LOMG more frequently developed malignancies and the same comorbidities that were already more frequent in this subgroup (arterial hypertension, hypercholesterolemia, diabetes mellitus). This effect might be explained by age, as previously addressed. In the EOMG group, osteoporosis and dyspepsia were more frequent. Steroid-induced osteoporosis mainly affects individuals 20–45 years, consistent with our findings (9, 10). This probably results from the cumulative effect of corticotherapy for several years, since the mean dose was not significantly different between groups.
Immunosuppression is generally associated with favorable outcomes in MG, irrespective of the age of onset (11). In most cases from our study, steroid sparing agents were introduced first, and the dose of steroids progressively tapered while a steroid-sparing agent was introduced. The choice of steroid-sparing agents followed what is recommended in the literature, with the most frequent options being azathioprine, mycophenolate mofetil and methotrexate (1, 8, 12). MMF has been suggested as an alternative first-line steroid-sparing agent, due to its favorable profile (13). The results from our practice, with AZA as the commonest option, are in line with recently published guidelines (14). Anti-CD20 antibody therapy (rituximab) was generally reserved to more severe or refractory cases. These findings are consistent with other studies showing that the therapeutic management does not seem to differ between EOMG and LOMG, despite the latter having more comorbidities (11, 15). Rituximab has also been shown to be a safe and effective treatment in late-onset cases of aggressive generalized MG (16). Regarding other monoclonal antibodies, eculizumab and tocilizumab were used in 1 EOMG patient each, which is statistically non-significant. Both treatments have been shown to be safe and effective in patients with later age of onset (17, 18). Overall, there was a tendency toward late-onset forms requiring fewer drugs and thus being less frequently treatment-refractory, confirming findings from a recent study (6).
This study has several limitations that must be addressed. First, its retrospective design based on clinical records with a relatively small sample size. Second, we opted to use the age of 50 as a cut-off to define EOMG and LOMG, but there are other cut-off values proposed in the literature (19). Moreover, we have not considered the subgroup of very-late onset forms that is increasingly recognized (20). We have not specifically addressed the efficacy of different treatment modalities based on the MGFA score, as the purpose of this study was to specifically study treatment modalities and respective side effects in EOMG and LOMG. In the future, doing a longitudinal study with this purpose would be interesting.
MG is a complex neuroimmunological disorder whose treatment implicates taking into account patient comorbidities and strategies to avoid treatment-related adverse events. The growing subgroup of LOMG poses further challenges to neurologists handling this disorder. Our study describes the similarities in treatment modalities between EOMG and LOMG and the differences in steroid-related adverse events between each group.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comissão de ética do Centro Hospitalar Universitário de Santo António. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation because the retrospective study was based on information from clinical records.
Author contributions
JM: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. JF: Conceptualization, Formal analysis, Methodology, Writing – original draft. ML: Conceptualization, Formal analysis, Methodology, Writing – original draft. AS: Writing – review & editing. RS: Writing – review & editing. AM: Writing – review & editing. ES: Conceptualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gilhus, EN, and Verschuuren, JJ. Myasthenia gravis: subgroup classification and therapeutic strategies. Lancet Neurol. (2015) 14:1023–36. doi: 10.1016/S1474-4422(15)00145-3
2. Vincent, A, Palace, J, and Hilton-Jones, D. Myasthenia gravis. Lancet. (2001) 357:2122–8. doi: 10.1016/S0140-6736(00)05186-2
3. Narayanaswami, P, Sanders, BD, Wolfe, G, Benatar, M, Cea, G, Evoli, A, et al. International consensus guidance for management of myasthenia gravis. Neurology. (2021) 96:114–22. doi: 10.1212/WNL.0000000000011124
4. Misra, KU, Kalita, J, Singh, KV, and Kumar, S. A study of comorbidities in myasthenia gravis. Acta Neurol Belg. (2020) 120:59–64. doi: 10.1007/s13760-019-01102-w
5. Klimiec-Moskal, E, Quirke, M, and Leite, IM. Comorbidities in older patients with myasthenia gravis — Comparison between early-and late-onset disease. Acta Neurol Scand. (2022) 145:371–4. doi: 10.1111/ane.13549
6. Cortés-Vicente, E, Álvarez-Velasco, R, Segovia, S, Paradas, C, Casasnovas, C, Guerrero-Sola, A, et al. Clinical and therapeutic features of myasthenia gravis in adults based on age at onset. Neurology. (2020) 94:e1171–80. doi: 10.1212/WNL.0000000000008903
7. Mao, Z-F, Mo, X-A, Qin, C, Lai, Y-R, and Hackett, LM. Incidence of thymoma in myasthenia gravis: a systematic review. J Clin Neurol. (2012) 8:161–9. doi: 10.3988/jcn.2012.8.3.161
8. Sanders, BD, Wolfe, IG, Benatar, M, Evoli, A, Gilhus, NE, Illa, I, et al. International consensus guidance for management of myasthenia gravis. Neurology. (2016) 87:419–25. doi: 10.1212/WNL.0000000000002790
9. Khosla, S, Lufkin, EG, Hodgson, SF, Fitzpatrick, LA, and Melton, LJ. Epidemiology and clinical features of osteoporosis in young individuals. Bone. (1994) 15:551–5. doi: 10.1016/8756-3282(94)90280-1
10. Mazziotti, G, Angeli, A, Bilezikian, PJ, Canalis, E, and Giustina, A. Glucocorticoid-induced osteoporosis: an update. Trends Endocrinol Metab. (2006) 17:144–9. doi: 10.1016/j.tem.2006.03.009
11. Yildiz Celik, S, Durmus, H, Yilmaz, V, Saruhan Direskeneli, G, Gulsen Parman, Y, Serdaroglu Oflazer, P, et al. Late-onset generalized myasthenia gravis: clinical features, treatment, and outcome. Acta Neurol Belg. (2020) 120:133–40. doi: 10.1007/s13760-019-01252-x
12. Lascano, MA, and Lalive, HP. Update in immunosuppressive therapy of myasthenia gravis. Autoimmun Rev. (2021) 20:102712. doi: 10.1016/j.autrev.2020.102712
13. Hanisch, F, Wendt, M, and Zierz, S. Mycophenolate mofetil as second line immunosuppressant in myasthenia gravis - a long-term prospective open-label study. Eur J Med Res. (2009) 14:364–6. doi: 10.1186/2047-783X-14-8-364
14. Wiendl, H, Abicht, A, Chan, A, Della Marina, A, Hagenacker, T, Hekmat, K, et al. Guideline for the management of myasthenic syndromes. Ther Adv Neurol Disord. (2023) 16:17562864231213240. doi: 10.1177/17562864231213240
15. Pasqualin, F, Guidoni, VS, Ermani, M, Pegoraro, E, and Bonifati, MD. Outcome measures and treatment effectiveness in late onset myasthenia gravis. Neurol Res Pract. (2020) 2:2. doi: 10.1186/s42466-020-00091-z
16. Monte, ME, Giménez, GF, Morán, DAJ, and Andres, LMJ. Rituximab para el tratamiento de la miastenia grave generalizada: experiencia en la práctica clínica. Rev Neurol. (2021) 73:416–20. doi: 10.33588/rn.7312.2021166
17. Howard, FJ, Bril, V, Vu, T, Karam, C, Peric, S, Margania, T, et al. Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): a multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. (2021) 20:526–36. doi: 10.1016/S1474-4422(21)00159-9
18. Jia, D, Zhang, F, Li, H, Shen, Y, Jin, Z, Shi, FD, et al. Responsiveness to tocilizumab in anti-acetylcholine receptor-positive generalized myasthenia gravis. Aging Dis. (2023):01. doi: 10.14336/AD.2023.0528
19. Hellmann, AM, Mosberg-Galili, R, and Steiner, I. Myasthenia gravis in the elderly. J Neurol Sci. (2013) 325:1–5. doi: 10.1016/j.jns.2012.10.028
Keywords: myasthenia gravis, late-onset, comorbidities, steroid-sparing, immunosuppression
Citation: Moura J, Fernandes J, Lima MJ, Sousa AP, Samões R, Martins Silva A and Santos E (2024) Treatment strategies and treatment-related adverse events in MG according to the age of onset. Front. Neurol. 15:1277420. doi: 10.3389/fneur.2024.1277420
Edited by:
German Moris, SESPA, SpainReviewed by:
Michelangelo Maestri, University of Pisa, ItalyMarc De Baets, Maastricht University, Netherlands
Copyright © 2024 Moura, Fernandes, Lima, Sousa, Samões, Martins Silva and Santos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: João Moura, bW91cmEubmV1cm9AY2hwb3J0by5taW4tc2F1ZGUucHQ=
†ORCID: João Moura, http://orcid.org/0000-0002-4212-906X