
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 11 January 2024
Sec. Neuro-Oncology and Neurosurgical Oncology
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1317858
This article is part of the Research TopicSurgical Management of Spine and Spinal Cord MetastasisView all 6 articles
 Hwa Kyung Byun1
Hwa Kyung Byun1 Woong Sub Koom2*
Woong Sub Koom2* Se-Jun Park3Sang-Il Kim4Jin Ho Kim5Young-Hoon Kim4Bong-Soon Chang6
Se-Jun Park3Sang-Il Kim4Jin Ho Kim5Young-Hoon Kim4Bong-Soon Chang6 Yong Chan Ahn7* on behalf of Korean Society of Spine Tumor
Yong Chan Ahn7* on behalf of Korean Society of Spine TumorPurpose: To understand the current practice of radiation oncologists (ROs) and orthopedic surgeons (OSs) regarding spine metastasis.
Methods: In 2022, an internet-based survey was conducted for ROs and OSs who treat spinal metastasis in Korea. Respondents were asked to choose the treatment option for two clinical scenarios. Scenario 1 involved a case displaying symptoms of leg weakness due to spinal cord compression and Scenario 2 involved a case with back pain due to pathologic compression fracture. The survey also included a question that required respondents to rank the importance of 11 clinical factors that affect treatment decisions.
Results: Forty-nine ROs and 30 OSs responded to the survey. There were significant differences in treatment choices between two groups for both scenarios (P = 0.001). In Scenario 1, more OSs chose surgical resection than ROs (43.3% vs. 16.7%), while more ROs chose radiotherapy than OSs (83.3% vs. 53.3%). In Scenario 2, a similar proportion of OSs and ROs chose radiotherapy (OSs, 71.4% vs. ROs, 67.3%), while more OSs opted for prophylactic fixation after radiotherapy than ROs (95.0% vs. 42.4%). The top three factors influencing treatment decisions were general performance status, life expectancy, and spinal instability for both ROs and OSs. In both Scenarios 1 and 2, the treatment decisions of ROs changed significantly when clinical conditions related to these top three factors were altered.
Conclusion: Although ROs and OSs share the same factors influencing treatment decisions for spinal metastases, notable differences exist in their actual treatment preferences, with ROs preferring radiotherapy and OSs opting for surgical resection. Multidisciplinary discussions may be necessary to reduce the gap in decision-making.
The spine is one of the most common sites of cancer metastasis (1). Spine metastasis can cause symptoms such as pain, spinal cord compression, hypercalcemia, and pathologic fracture, which usually adversely impact the patients' health status and quality of life (2). The clinical situations in which spine metastasis occurs vary greatly from patient to patient, and frequently present with complex therapeutic challenges. The type of cancer, patient's condition, location of involved spine, severity of clinical symptoms metastasis can vary depending on the individual basis. Thus, treatment plans need to be carefully made taking the individual clinical situation of each patient into account.
For managing the spine metastasis patients, various options including analgesics, systemic chemotherapy, hormonal therapy, bisphosphonates, systemic radiopharmaceuticals, and local therapies such as surgery and radiation therapy (RT) are available, and interdisciplinary care among radiologists, medical oncologists, radiation oncologists (ROs), orthopedic surgeons (OSs), pain medicine specialists, and palliative care professionals is desirable (3). Among several options, local therapy is particularly important as it can lead to local tumor control, neural compression relief, and pain control. Surgery has the capability of stabilizing mechanical instability in addition. Thus, it is crucial to understand the current practice patterns by ROs and OSs, who are frequently engaged in the management of spine metastasis patients.
There were two survey studies, initiated by Korean ROs previously, on the practice patterns for spine metastasis, which were limited among ROs (4, 5). Considering that not only ROs but also OSs are main specialties of local therapy for patients with spine metastasis, it would be clinically meaningful to compare and analyze the opinions of two main specialists. We intended, through this study, to investigate the current practice patterns by ROs and OSs in managing the spine metastasis patients and identify the clinical factors influencing their clinical decision-making.
This study was initiated by the Korean Society of Spine Tumor, and the questionnaires were distributed among the members of three societies: the Korean Society of Spine Tumor; the Korean Society for Radiation Oncology; and the Korean Society of Spine Surgery, respectively. The survey was conducted as an online survey using the Google Forms from August until November 2022. A total of 79 specialists responded to the questionnaire, including 49 ROs and 30 OSs, all of whom were affiliated at the university hospitals or tertiary hospitals.
The questionnaires were developed by consensus among four ROs (HB, WK, JK, and YA) and two OSs (S-JP and S-IK). The survey consisted of three parts. The first was related to the general characteristics of the respondents. In the second part, two clinical scenarios were generated, on each of which, the respondents were asked to choose their preferred treatment option from a list of six: (1) surgical resection alone; (2) surgical resection plus postoperative RT; (3) RT alone; (4) RT plus prophylactic fixation; (5) non-surgical intervention; and (6) observation, respectively. The original clinical scenario 1 described a 55-year-old male patient with hepatocellular carcinoma who presented with a week-long history of leg weakness due to spinal cord compression with Bilsky grade 3 compression at the T7 level (Figures 1a, b) (6). Based on the imaging studies, this patient had a single spine metastasis, and the spinal instability neoplastic score (SINS) was 9, indicating a potentially unstable spine (7). The patient's Karnofsky performance status (KPS) before the onset of leg weakness was 70, with the expected survival time shorter than 6 months. There was no further plan of systemic treatment. The original clinical scenario 2 described a 60-year-old female patient with breast cancer who presented with severe back pain due to pathologic compression fracture at T10 level with spinal cord abutment (Figures 1c, d) (Bilsky grade 1c). The patient's SINS was 9, indicating a potential unstable spine. Multiple spine metastases were also present, and KPS was 90, with the expected survival time longer than 6 months. There was a further plan of systemic treatment. In addition to the original scenarios, the respondents were asked to choose their preferred treatment option assuming that some conditions were different from the original ones while all others were the same (i.e., differences in the involved spine level, life expectancy, SINS, KPS, plan of systemic therapy, etc…). The third part of the survey intended to identify the factors that influenced treatment decision and included 11 factors: patient's age; general performance status; life expectancy; expected complication by spine metastasis-directed treatment; patient's convenience by treatment; expected efficacy of treatment for metastasis; policy and situation of the respondent's institute or training habits; spinal instability; location of the tumor; number of spine metastases; and further systemic treatment plan, respectively. The respondents were asked to rank the factors in the order of importance. The detail of questionnaire is provided in Supplementary material.

Figure 1. (a, b) T2-weighted MR images demonstrate a spine metastasis in clinical scenario 1. Scenario 1 describes a 55-year-old male patient with hepatocellular carcinoma who presented with a week-long history of leg weakness due to spinal cord compression (Bilsky grade 3) at the T7 level. The patient had a single spinal metastasis, a SINS score of 9, a KPS score of 70, an expected survival time of <6 months, and no further plan for systemic treatment. (c, d) T2-weighted MR images demonstrate spine metastases in clinical scenario 2. Scenario 2 describes a 60-year-old female patient with breast cancer who presented with severe back pain due to a pathologic compression fracture at the T10 level with spinal cord abutment (Bilsky grade 1c). The patient had multiple spinal metastases, a SINS score of 9, a KPS score of 90, an expected survival time of more than 6 months, and a plan for further systemic treatment.
The collected answers for the second part by ROs and OSs were compared using the chi-square test. The McNemar's test was conducted to compare whether a significant difference occurred in the modified clinical scenarios, when compared with the original. The Bonferroni correction was applied to correct for multiple comparisons. A two-sided P-value <0.05 was considered significant. For the third part, the final ranking was determined by arranging the average value of each respondent's ranking for each clinical factor in order. All the statistical analyses were performed using the SPSS software version 25.0 (IBM Inc., Armonk, NY, USA).
Of the 79 respondents, 30 were OSs and 49 were ROs. The OSs were working in 26 different tertiary or university hospitals, with a median of one respondent per hospital (range, 1–2). The ROs were working in 33 different tertiary or university hospitals, with a median of one respondent per hospital (range, 1–8). Regarding the OSs, the median period of practicing as an orthopedic surgeon was 12 years [interquartile range (IQR), 7–17 years]. The majority (70.0%) reported that >200 spine surgeries were performed per year, and also the majority (66.7%) reported that ≤ 30 surgeries in relation with spine metastasis were performed per year at their departments, respectively (Table 1). Among the ROs, the median period of practicing as a radiation oncologist was 9 years (IQR, 5–17 years). The number of daily RT patients varied from ≤ 50 to >300, and the number of patients who received spine RT per year varied from ≤ 50 to >300 at their departments.
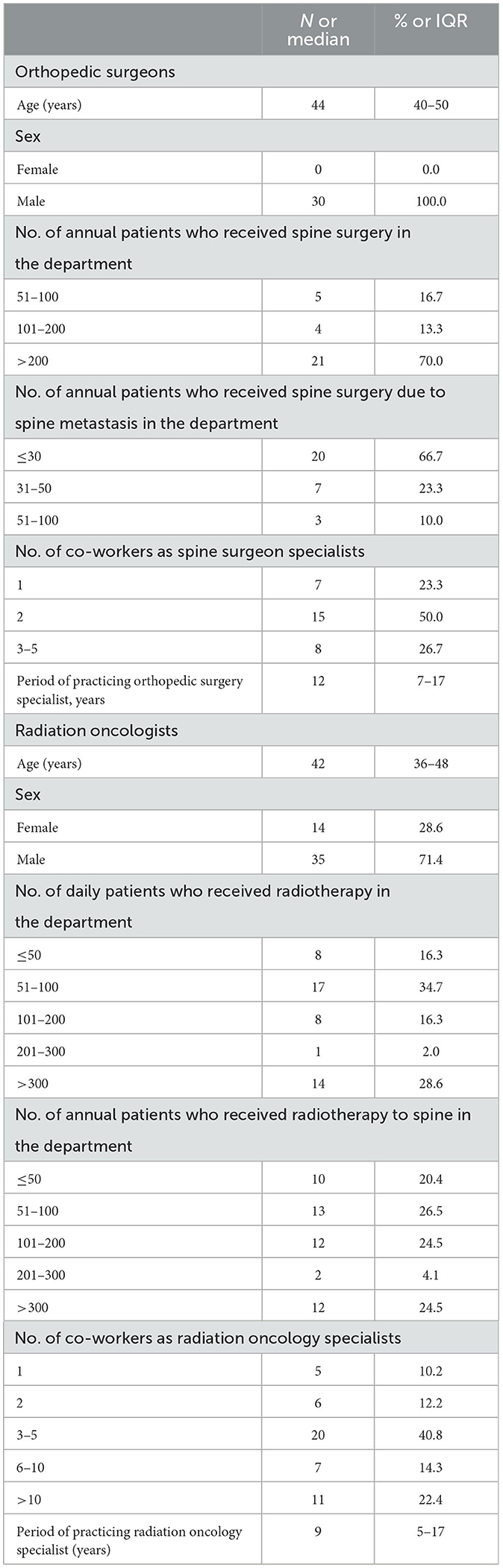
Table 1. Characteristics of respondents.
In scenario 1, which represented a case with cord compression symptoms, there was a significant difference in treatment choice between OSs and ROs (Figure 2, P < 0.001). The rate of choosing surgical resection (with or without postoperative RT) was significantly higher among OSs than ROs (43.3% vs. 16.7%, P = 0.010). Conversely, ROs more frequently preferred RT (with or without prophylactic fixation) than OSs (83.3% vs. 53.3%, P = 0.004). Among those who chose RT, the proportion of those who chose prophylactic fixation was higher among OSs (50.0% vs. 7.5%, P = 0.001).
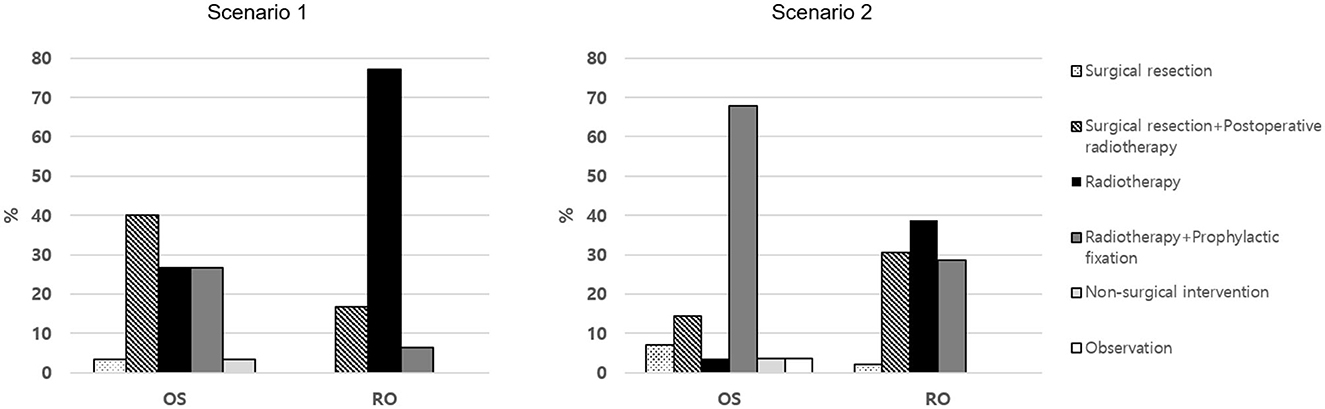
Figure 2. The choice of treatment methods for spine metastasis in clinical scenarios.
In scenario 2, which represented a case with pathologic compression fracture, there also was a significant difference in treatment choice between OSs and ROs (Figure 2, P < 0.001). RT (with or without prophylactic fixation) was the most frequently chosen treatment method by both OSs and ROs (71.4% vs. 67.3%, P = 0.710). Among those who chose RT, however, the proportion of OSs who opted for prophylactic fixation was significantly higher (95.0% vs. 42.4%, P < 0.001).
Table 2 summarized the patterns of answers by OSs and ROs on the scenarios 1 and 2. In scenario 1, OSs chose surgical resection in 43.3% of cases in the original scenario, and more frequently chose surgical resection under the condition that the expected survival was longer than 6 months (76.7%, P = 0.018), but their choices did not change on other modified conditions. Among ROs, 16.7% chose surgical resection in the original scenario, and more frequently chose surgical resection if the expected survival was longer than 6 months (51.0%, P < 0.001), if there was an unstable spine (49.0%, P < 0.001), if the KPS was 90 (44.9%, P = 0.009), and if symptom duration was 1 day (51.0%, P < 0.001), respectively.
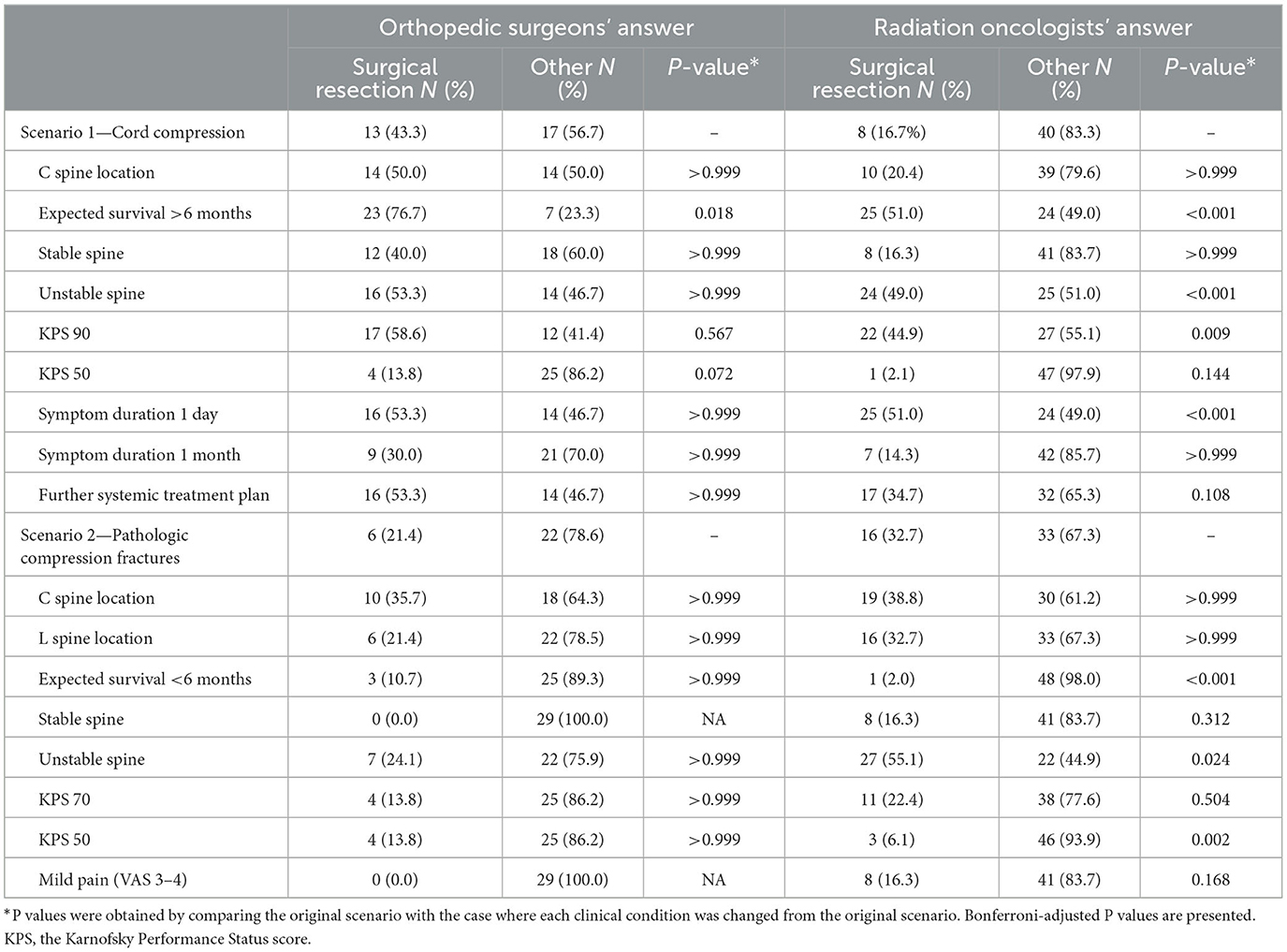
Table 2. Number of answers selecting surgical resection according to the clinical conditions.
In scenario 2, 21.4% of OSs chose surgical resection in the original scenario, and no one chose surgical resection if the spine was stable or if the patient had mild pain. Among ROs, 32.7% chose surgical resection in the original scenario, which was significantly less frequently chosen if the expected survival was shorter 6 months (2.0%, P < 0.001) or if the KPS score was 50 (6.1%, P = 0.002), respectively. On the other hand, ROs chose surgical resection more frequently if the spine was unstable (55.1%, P = 0.024).
In the third part, the factors influencing treatment decisions were ranked by the participating OSs and ROs (Table 3). The top three factors chosen by ROs were general performance status, followed by life expectancy, and spinal instability, respectively. Those chosen by OSs were life expectancy, followed by general performance status, and spinal instability, respectively. The top three factors were, more or less, very similar between specialties. Both groups also commonly considered the expectation of treatment efficacy for spine metastasis and the number of spine metastasis as an important factor, with five out of the top six factors being in common.
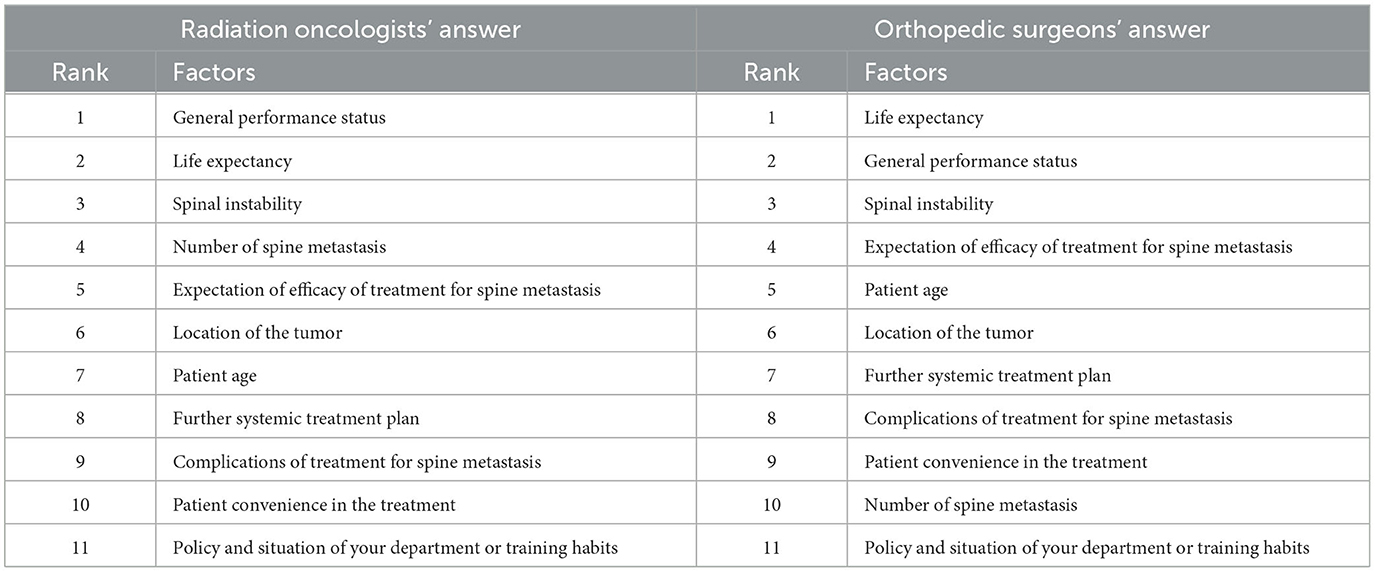
Table 3. Ranking of clinical factors influencing treatment decision-making for spine metastasis.
In this study, we aimed to investigate the current practice patterns of the Korean ROs and OSs with respect to the preferred management option for the spine metastasis patients and the factors influencing their treatment decisions. Our findings demonstrated significant differences between the two specialties, with ROs predominantly favoring RT while OSs preferring surgical resection, respectively. Despite this divergence in treatment preferences, the top three factors influencing the treatment decision (general performance status, life expectancy, and spinal instability) were in common among the two specialties. Notably, in both Scenarios 1 and 2, the treatment decisions of ROs showed significant differences when clinical conditions related to these top three factors were altered.
The results of this study highlight that there exists significant heterogeneity in the practice patterns across two different clinical backgrounds: OSs tend to favor surgical intervention; while ROs generally prefer RT, respectively. This could be attributed to the heterogeneous nature of bone metastasis and the availability of diverse treatment options. Numerous methods have been proposed to aid treatment decision-making for spine metastasis. The SINS aims to quantify the spinal instability and to assist in surgical decision-making (7). The modified Tokuhashi scoring system strives to predict prognosis in the patients with metastatic spinal disease using six factors: general condition; number of non-spinal bone metastasis; number of spinal metastasis; type of primary lesion; presence or absence of metastasis to major organs; and state of paralysis, respectively (8). The Tomita's scoring system is based on the type of primary tumor, presence and operability of visceral metastasis, and number of bony metastasis, respectively (9). In the guidelines for the diagnosis and treatment of bone metastasis published by Japanese medical groups, surgery and RT are suggested as local therapy options (10). However, this guideline offered limited details regarding the selection of specific local therapies in various clinical situations. No universal guideline, which considers all patient-, tumor-, and spine-related clinical elements, is available as of yet. In this context, examining the experts' clinical decision-making in the representative clinical scenarios through surveys, as in this study, could be beneficial and valid to understanding the current real-world practice patterns.
A randomized trial conducted by Patchell et al. (11) demonstrated that direct decompressive surgical resection followed by RT provided better outcomes in terms of preserving or improving ambulatory function, local control, and survival, when compared to RT alone. However, the application of surgery is not always available because of inherent risks of complications (12). Hence, it is crucial to make an appropriate selection of the patients who require surgery based on their clinical condition. In our study, we examined whether the changes in clinical conditions within the clinical scenarios influenced surgical decision-making. As a result, surgical treatment was preferred when the expected survival was longer, general performance status was better, spine was unstable, and symptom onset of spinal cord compression was recent, respectively. On the other hand, non-surgical treatment was more frequently favored when the expected survival was shorter, general performance status was poorer, spine was stable, and there was only mild pain, respectively. Additionally, the top three important clinical factors in treatment decisions were in common between ROs and OSs (life expectancy, general performance status, and spinal instability).
Our study could add to the existing literature, which were primarily focused on surveys of single specialties. Yu et al. (5) previously surveyed the practice patterns of Korean ROs in the context of spine metastasis. A multinational online survey study, encompassing three Asian countries (Korea, China, and Japan), showed diverse practice preferences in RT for spine metastasis in each nation (4). Spratt et al. (13) examined a real world practice pattern of the U.S. ROs in treating bone metastasis, showing diverse RT approaches. In contrast to the previous studies that solely investigated RT, our study assessed both RT and surgery as local therapies for spine metastasis. This multidisciplinary approach would offer a more comprehensive understanding of clinical practice patterns in this field.
The limited number of participating physicians in this survey represents a significant limitation of this study. However, this survey was sent to ROs and OSs nationwide, and most of the participants belonged to the tertiary or university hospitals in Korea and their main interest practice fields include spine tumor. Another limitation is the presentation of a limited number of scenarios. Nevertheless, within each scenario, variations in clinical conditions were introduced to facilitate the consideration of treatment decisions in a broader range of situations.
The discrepancy in treatment decision shown between ROs and OSs in our study calls for the need for multidisciplinary care. Harel and Angelov (14) suggested a treatment algorithm for the patients with spine metastasis incorporating RT, radiosurgery, systemic therapy, and surgery, emphasizing multidisciplinary integration. Barton et al. (15) interviewed a multidisciplinary cohort of physicians treating spine metastasis, in which, the respondents strongly emphasized the importance of multidisciplinary care and communication among multidisciplinary team members. To achieve a multidisciplinary approach, Kimura (16) suggested a cancer board focusing on the management of bone metastasis involving a team of doctors in oncology, palliative care, radiation oncology, orthopedics, nuclear medicine, radiology, and rehabilitation, respectively. In Korea, however, it is known that only a few hospitals operate regular multidisciplinary tumor boards specialized in bone metastasis. The shared-decision making through the specialized cancer board will contribute to improving the care quality, patient satisfaction level as well as the clinical outcomes. More active participation among the specialists who care for the spine tumor patients are highly encouraged.
Our study suggests that the actual decision-making processes differ significantly between ROs and OSs, although both parties take into account the factors in common in their treatment decision (general performance status, life expectancy, spinal instability, expectation of treatment, and number of spine metastasis). This implies that the same patient is more likely to receive RT if seen by ROs first, and more likely to undergo surgery if seen by Oss first, respectively. This discrepancy in treatment policy may cause confusion to the patients and may interfere with obtaining the optimal treatment outcomes. Our findings indicate that it is necessary to engage in multidisciplinary discussion and determine treatment plan based on the individual clinical situation in order to reduce the gap in treatment decision and to endorse higher clinical benefit to the patients.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
HB: Data curation, Formal analysis, Methodology, Writing—original draft. WK: Conceptualization, Data curation, Methodology, Writing—review & editing. S-JP: Data curation, Methodology, Writing—review & editing. S-IK: Data curation, Methodology, Writing—review & editing. JK: Data curation, Methodology, Writing—review & editing. Y-HK: Data curation, Writing—review & editing. B-SC: Data curation, Writing—review & editing. YA: Conceptualization, Data curation, Methodology, Writing—review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1317858/full#supplementary-material
1. Ortiz Gómez JA. The incidence of vertebral body metastases. Int Orthop. (1995) 19:309–11. doi: 10.1007/BF00181116
2. Selvaggi G, Scagliotti GV. Management of bone metastases in cancer: a review. Crit Rev Oncol Hematol. (2005) 56:365–78. doi: 10.1016/j.critrevonc.2005.03.011
3. Janjan N. Bone metastases: approaches to management. Semin Oncol. (2001) 28:28–34. doi: 10.1016/S0093-7754(01)90229-5
4. Yu JI, Park HC, Ahn YC, Gao XS, Wang JJ, Zeng ZC, et al. Spine metastasis practice patterns among korean, chinese, and japanese radiation oncologists: a multinational online survey study. J Radiat Res. (2017) 58:155–63. doi: 10.1093/jrr/rrw089
5. Yu JI, Park HC, Ahn YC, Chung Y, Koom WS, Song SY. Variation in practice patterns of Korean radiation oncologists for spine metastasis between 2009 and 2014. Cancer Res Treat. (2016) 48:1102–9. doi: 10.4143/crt.2015.207
6. Bilsky MH, Laufer I, Fourney DR, Groff M, Schmidt MH, Varga PP, et al. Reliability analysis of the epidural spinal cord compression scale. J Neurosurg Spine. (2010) 13:324–8. doi: 10.3171/2010.3.SPINE09459
7. Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine. (2010) 35:E1221–9. doi: 10.1097/BRS.0b013e3181e16ae2
8. Tokuhashi Y, Matsuzaki H, Oda H, Oshima M, Ryu J. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine. (2005) 30:2186–91. doi: 10.1097/01.brs.0000180401.06919.a5
9. Tomita K, Kawahara N, Kobayashi T, Yoshida A, Murakami H, Akamaru T. Surgical strategy for spinal metastases. Spine. (2001) 26:298–306. doi: 10.1097/00007632-200102010-00016
10. Shibata H, Kato S, Sekine I, Abe K, Araki N, Iguchi H, et al. Diagnosis and treatment of bone metastasis: comprehensive guideline of the Japanese Society of Medical Oncology, Japanese Orthopedic Association, Japanese Urological Association, and Japanese Society for Radiation Oncology. ESMO Open. (2016) 1:e000037. doi: 10.1136/esmoopen-2016-000037
11. Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. (2005) 366:643–8. doi: 10.1016/S0140-6736(05)66954-1
12. Smith JS, Saulle D, Chen CJ, Lenke LG, Polly DW Jr, Kasliwal MK, et al. Rates and causes of mortality associated with spine surgery based on 108,419 procedures: a review of the Scoliosis Research Society Morbidity and Mortality Database. Spine. (2012) 37:1975–82. doi: 10.1097/BRS.0b013e318257fada
13. Spratt DE, Mancini BR, Hayman JA, Boike T, Pierce LJ, Moran JM, et al. Contemporary statewide practice pattern assessment of the palliative treatment of bone metastasis. Int J Radiat Oncol Biol Phys. (2018) 101:462–7. doi: 10.1016/j.ijrobp.2018.02.037
14. Harel R, Angelov L. Spine metastases: current treatments and future directions. Eur J Cancer. (2010) 46:2696–707. doi: 10.1016/j.ejca.2010.04.025
15. Barton LB, Arant KR, Blucher JA, Sarno DL, Redmond KJ, Balboni TA, et al. Clinician experiences in treatment decision-making for patients with spinal metastases: a qualitative study. J Bone Joint Surg Am. (2021) 103:e1. doi: 10.2106/JBJS.20.00334
Keywords: spine metastasis, surgical resection, radiotherapy, survey, multidisciplinary discussion, pattern of care
Citation: Byun HK, Koom WS, Park S-J, Kim S-I, Kim JH, Kim Y-H, Chang B-S and Ahn YC (2024) Different decision-making in spine metastasis management among radiation oncologists and orthopedic surgeons: a Korean online survey study. Front. Neurol. 14:1317858. doi: 10.3389/fneur.2023.1317858
Received: 10 October 2023; Accepted: 27 December 2023;
Published: 11 January 2024.
Edited by:
Rouzbeh Motiei-Langroudi, University of Kentucky, United StatesReviewed by:
Hidefumi Aoyama, Hokkaido University, JapanCopyright © 2024 Byun, Koom, Park, Kim, Kim, Kim, Chang and Ahn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yong Chan Ahn, YWhueWNAc2trdS5lZHU=; Woong Sub Koom, bWRnb2xkQHl1aHMuYWM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.