
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Neurol. , 14 December 2023
Sec. Multiple Sclerosis and Neuroimmunology
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1289810
This article is part of the Research Topic The diagnostic difficulties of immune-mediated neuropathies View all 9 articles
 Sara Mariotto1Piera de Gaspari2Dominik Jäger3Stefanie Hahn3Cindy Forni3Sandra Saschenbrecker3*Erik Lattwein3Alessandro Dinoto1Sergio Ferrari1
Sara Mariotto1Piera de Gaspari2Dominik Jäger3Stefanie Hahn3Cindy Forni3Sandra Saschenbrecker3*Erik Lattwein3Alessandro Dinoto1Sergio Ferrari1Peripheral neuropathy with antibodies to myelin-associated glycoprotein (MAG) is an autoimmune demyelinating disorder of the peripheral nervous system caused by pathogenic IgM recognizing the human natural killer-1 glycoepitope expressed on MAG. This study aimed to analyze the performance of a new indirect immunofluorescence cell-based assay (CBA, EUROIMMUN) for the detection of anti-MAG IgM. Antibody reactivity was determined in sera from 95 patients with clinical and neurophysiological evidence of anti-MAG-associated neuropathy and in control samples from 55 patients with other forms of peripheral neuropathy. Compared to the results of the gold standard method (ELISA, Bühlmann) and using samples at a dilution of 1:100, the CBA had a sensitivity of 98.9% and a specificity of 100% (PPV 100%, NPV 98.2%). In conclusion, the CBA allows the detection of antibodies to MAG using an easy and standardized technique, and it presents a sensitive and specific alternative to the more time-consuming ELISA. Larger studies are needed to address anti-MAG titer monitoring in parallel with clinical activity.
Myelin-associated glycoprotein (MAG) is a 100 kDa transmembrane glycoprotein expressed by Schwann cells and represents a target of monoclonal IgM autoantibodies (MAG-Abs). These antibodies recognize the human natural killer-1 (HNK-1) carbohydrate epitope, which is highly expressed on MAG. MAG-Abs are associated with a slowly progressive large-fiber distal symmetrical sensorimotor polyneuropathy with prominent sensory impairment, ataxia, and intention tremor (1–5). The pathogenic role of MAG-Abs has been confirmed by pathological studies on nerve biopsies, showing a relationship between the widening of myelin lamellae (with deposits of IgM M-protein and complement) and segmental demyelination (6–8). Antibodies to MAG can be detected in patient sera by enzyme-linked immunosorbent assay (ELISA) or Western blot using MAG or purified myelin (9–11). For both methods of MAG-Abs detection, a normal range should be defined, as low titers may be found in normal subjects (12). ELISA is often preferred to Western blot because it is more sensitive in detecting serum MAG-Abs, easier to use, and allows antibody titration, which is potentially useful for monitoring responses to therapies (13).
The aim of this study was to determine the clinical performance of a novel immunofluorescence fixed cell-based assay (CBA, EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany) in comparison with the gold-standard technique used to identify MAG-Abs (ELISA, Bühlmann, Schönenbuch, Switzerland).
Sera of consecutive MAG-Abs-positive subjects (n = 95) with a compatible clinical and electrophysiological phenotype diagnosed between August, 2018 and March, 2021 at the Neuropathology Laboratory, University of Verona, Italy were analyzed using the novel fixed CBA. A group of MAG-Abs-negative subjects with peripheral neuropathy of a different origin (n = 55) was also tested for comparison.
This assay (Bühlmann) employs a quantitative enzymatically amplified sandwich-type immunoassay technique. Plates precoated with highly purified MAG from human brain were used. Briefly, reconstituted calibrators and diluted patient sera were incubated for 2 h in wells, and MAG-Abs were bound by the immobilized human MAG. After washing steps, horseradish peroxidase-labeled antibodies to human IgM were added to the wells and incubated for 2 h. After washing steps, the substrate solution containing tetramethylbenzidine was added and incubated for 30 min. The proportion of MAG-Abs was revealed in a blue scale. The color development was stopped by adding H2SO4, which caused the blue solution to turn yellow. The intensity of the color absorbance was measured in a microplate reader at a wavelength of 450 nm. The absorbance measured was directly proportional to the concentration of MAG-Abs. The concentration of MAG-Abs in samples was calculated in comparison to the standard curve, plotted with human MAG-Abs calibrators, and expressed as Bühlmann titer units (BTU).
The EUROIMMUN Anti-MAG IgM CBA is a research-use-only indirect immunofluorescence test. Each test field on the slides contains two BIOCHIPs, one coated with recombinant HEK-293 cells expressing the MAG/HNK-1 antigen and the other coated with control-transfected HEK-293 cells. In brief, samples (diluted from 1:10 to 1:1,000,000) were incubated with the test substrates for 30 min at room temperature. After washing, the slides were incubated with fluorescein isothiocyanate (FITC)-labeled goat anti-human IgM (EUROIMMUN) for 30 min at room temperature. After washing and embedding, the slides were evaluated by fluorescence microscopy. Samples were classified as positive or negative based on the fluorescence intensity of the MAG/HNK-1-expressing cells in direct comparison with control-transfected cells and control samples. Endpoint titers refer to the highest dilution showing visible fluorescence.
Data are presented as median (range) and number (percentage), as appropriate. Sensitivity, specificity, positive predictive values (PPV) and negative predictive values (NPV) were calculated. Confidence intervals (95% CI) were calculated according to the Clopper-Pearson method. Sensitivity, specificity, PPV and NPV were calculated for the CBA at 1:10 and 1:100 dilution. Lastly, the correlation between titers obtained by ELISA and CBA was evaluated with a two-tailed Pearson’s correlation analysis.
We analyzed 95 patients (F = 32, median age 74 years, range 49–92) with clinical and neurophysiological signs compatible with anti-MAG-associated neuropathy confirmed using the recommended ELISA (>1,000 BTU). All were positive at a 1:10 titration using EUROIMMUN’s fixed CBA. When performing further titrations, 94/95 were also positive at a 1:100 dilution, 74 at 1:1,000, 60 at 1:10,000, 20 at 1:100,000, and 11 at 1:1,000,000 (Figure 1).
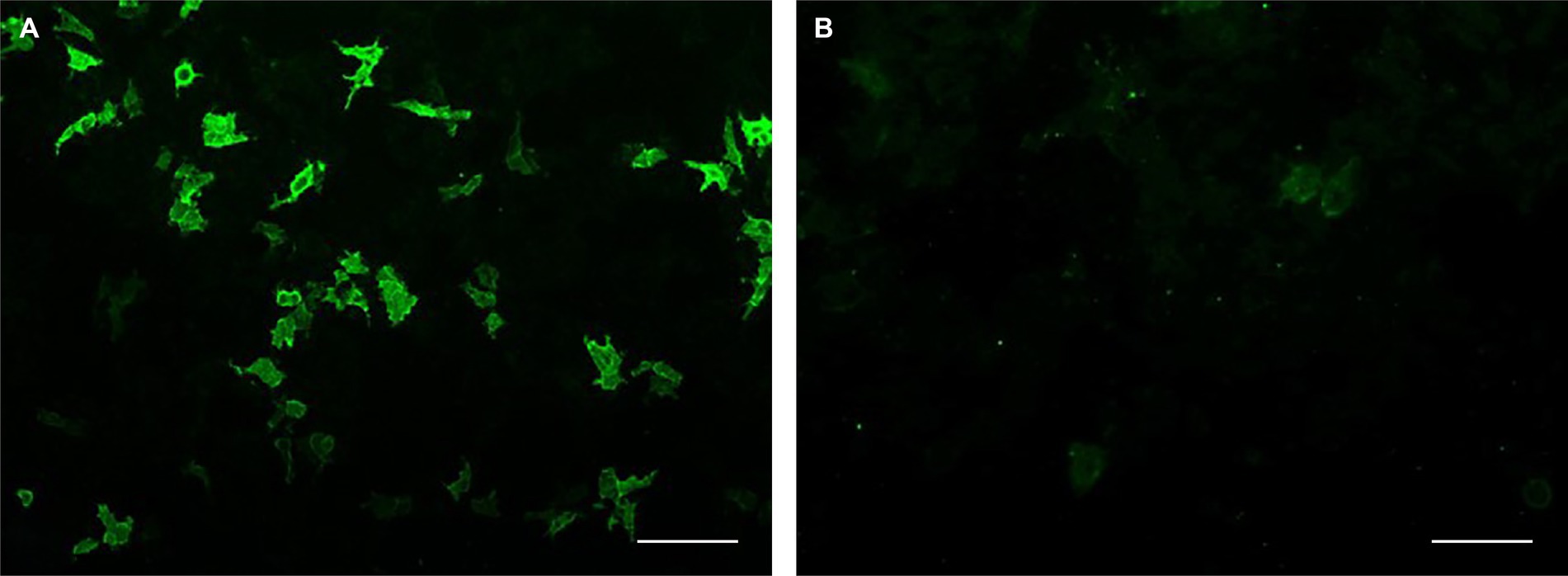
Figure 1. Recombinant cell-based indirect immunofluorescence assay. Serum from a patient with anti-MAG neuropathy was incubated with (A) HEK-293 cells expressing recombinant MAG/HNK-1 antigen and (B) control-transfected HEK-293 cells. Scale bar: 100 μm.
Among cases with “weak positivity” (n = 33) according to the standardized ELISA technique (1:1,000–1:10,000 BTU), 28 had a titer of ≤1:1,000 using the fixed CBA (1:10 n = 1, 1:100 n = 18, 1:1,000 n = 9). Among cases with “strong positivity” (n = 62) according to the standardized ELISA technique (≥1:10,000 BTU), 55 had a titer ≥1:10,000 using the fixed CBA (1:10,000 n = 38, 1:100,000 n = 7, 1:1,000,000 n = 10).
All patients with other forms of peripheral neuropathy, included as controls (n = 55, F = 18, median age 67 years, range 7–91), were negative by ELISA. Of these, 6 were positive by CBA at a 1:10 dilution and none was positive at 1:100 or further titrations.
When comparing results of the fixed CBA with those of the reference ELISA technique, we observed that at a 1:10 dilution, the CBA had 100% (CI 96.2–100%) sensitivity and 89.1% specificity (CI 77.8–95.9%, PPV 94.1%, NPV 100%), while at a 1:100 dilution, the sensitivity was 98.9% (CI 94.3–100%) and the specificity 100% (CI 93.5–100%, PPV 100%, NPV 98.2%). There was a trend toward correlation between the titer observed using the two techniques (p = 0.07).
We herein provide preliminary comparative data of MAG-Abs testing using the recommended ELISA technique and a novel ready-to-use fixed CBA. For the assessment of anti-MAG positivity, our results support the use of the novel CBA at a dilution of 1:100, which has the highest specificity (100%) and a very good sensitivity (98.9%). Compared to the other methods, this easy technique has many advantages, including [i] the expression of natively folded antigen in the membranes of the cell substrate enabling the detection of Abs binding to conformational epitopes, [ii] flexibility in assay design (BIOCHIP mosaics), and [iii] fluorescence stability, which allows multiple persons to analyze the slides and exchange images among centers. This standardized technique minimizes inter-assay variability and enables efficient preparation of large, standardized batches in a short time. In addition, it allows both identification and quantification (using further titrations) of specific antibodies.
Italian guidelines for MAG-Abs testing were recently developed through a consensus process that also reported indications and limits of anti-MAG testing, instructions for results interpretation, and an agreed-upon laboratory protocol (14). This consensus supports the use of ELISA as the most appropriate diagnostic technique, although the best cut-off of positivity is still an open question. In accordance with a previous study (13), sera with values between 1,000 and 10,000 BTU are interpreted as “weak positive” and are prone to diagnostic issues. Furthermore, a recent study identified a grey area between 1,500 and 7,000 BTU in which the differential diagnosis between chronic inflammatory demyelinating polyneuropathy (CIDP) and anti-MAG-associated neuropathy is challenging (15). In this scenario, CBA allows monitoring of MAG-Abs titer levels through further titrations, which is important for clinical correlations (16). In addition, fluorescent CBA is based on an easy and standardized technique, that is already used by many laboratories to identify antibodies to central nervous system antigens, such as antibodies to neuronal surface antigens in patients with autoimmune encephalitis or to aquaporin-4 in subjects with neuromyelitis optica spectrum disorders (17). Although qualitative concordance between CBA and ELISA results is promising, titers and BTUs are not perfectly comparable. Specific studies examining MAG-Abs titers in relation with clinical activity will clarify the suitability of this novel assay for disease monitoring.
In conclusion, the novel immunofluorescence CBA analyzed herein has a good sensitivity/specificity for the detection of MAG-Abs and retains several practical advantages. Larger studies designed with the aim of comparing and monitoring MAG-Abs titers in parallel with clinical activity are mandatory to confirm and expand our data.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval was not required for the studies involving humans because only leftover samples after completion of all diagnostic measures were included and patient data were processed anonymously. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements because only leftover samples after completion of all diagnostic measures were included and patient data were processed anonymously. All samples analyzed are part of Biob-Neu-DNA-2014.
SM: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. PG: Data curation, Investigation, Methodology, Writing – review & editing. DJ: Conceptualization, Supervision, Writing – review & editing. SH: Conceptualization, Methodology, Validation, Writing – review & editing. CF: Methodology, Validation, Writing – review & editing, Conceptualization. SS: Writing – review & editing. EL: Conceptualization, Methodology, Validation, Writing – review & editing. AD: Data curation, Formal analysis, Investigation, Writing – review & editing. SF: Conceptualization, Project administration, Supervision, Writing – review & editing.
This study was funded by EUROIMMUN Medizinische Labordiagnostika AG, in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
The authors would like to thank Daniela Alberti for her excellent technical assistance.
DJ, SH, CF, SS, and EL are employees of EUROIMMUN, a manufacturer of diagnostic reagents.
The authors declare that this study received funding from EUROIMMUN Medizinische Labordiagnostika AG. The funder had the following involvement in the study: study design, interpretation of data, and the decision to publish. The funder also covered the open access publication fees.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Latov, N, Braun, PE, Gross, RB, Sherman, WH, Penn, AS, and Chess, L. Plasma cell dyscrasia and peripheral neuropathy: identification of the myelin antigens that react with human paraproteins. Proc Natl Acad Sci U S A. (1981) 78:7139–42. doi: 10.1073/pnas.78.11.7139
2. Pedersen, SF, Pullman, SL, Latov, N, and Brannagan, TH III. Physiological tremor analysis of patients with anti-myelin-associated glycoprotein associated neuropathy and tremor. Muscle Nerve. (1997) 20:38–44. doi: 10.1002/(SICI)1097-4598(199701)20:1<38::AID-MUS5>3.0.CO;2-I
3. Bain, PG, Britton, TC, Jenkins, IH, Thompson, PD, Rothwell, JC, Thomas, PK, et al. Tremor associated with benign IgM paraproteinaemic neuropathy. Brain. (1996) 119:789–99. doi: 10.1093/brain/119.3.789
4. Yeung, KB, Thomas, PK, King, RH, Waddy, H, Will, RG, Hughes, RA, et al. The clinical spectrum of peripheral neuropathies associated with benign monoclonal IgM, IgG and IgA paraproteinaemia. Comparative clinical, immunological and nerve biopsy findings. J Neurol. (1991) 238:383–91. doi: 10.1007/BF00319857
5. Nobile-Orazio, E, Meucci, N, Baldini, L, Di, TA, and Scarlato, G. Long-term prognosis of neuropathy associated with anti-MAG IgM M-proteins and its relationship to immune therapies. Brain. (2000) 123:710–7. doi: 10.1093/brain/123.4.710
6. Kawagashira, Y, Koike, H, Tomita, M, Morozumi, S, Iijima, M, Nakamura, T, et al. Morphological progression of myelin abnormalities in IgM-monoclonal gammopathy of undetermined significance anti-myelin-associated glycoprotein neuropathy. J Neuropathol Exp Neurol. (2010) 69:1143–57. doi: 10.1097/NEN.0b013e3181fa44af
7. Gabriel, JM, Erne, B, Miescher, GC, Miller, SL, Vital, A, Vital, C, et al. Selective loss of myelin-associated glycoprotein from myelin correlates with anti-MAG antibody titre in demyelinating paraproteinaemic polyneuropathy. Brain. (1996) 119:775–87. doi: 10.1093/brain/119.3.775
8. Monaco, S, Bonetti, B, Ferrari, S, Moretto, G, Nardelli, E, Tedesco, F, et al. Complement-mediated demyelination in patients with IgM monoclonal gammopathy and polyneuropathy. N Engl J Med. (1990) 322:649–52. doi: 10.1056/NEJM199003083221002
9. Ilyas, AA, Quarles, RH, Dalakas, MC, and Brady, RO. Polyneuropathy with monoclonal gammopathy: glycolipids are frequently antigens for IgM paraproteins. Proc Natl Acad Sci U S A. (1985) 82:6697–700. doi: 10.1073/pnas.82.19.6697
10. Quarles, RH. Myelin-associated glycoprotein (MAG): past, present and beyond. J Neurochem. (2007) 100:1431–48. doi: 10.1111/j.1471-4159.2006.04319.x
11. Nobile-Orazio, E, Francomano, E, Daverio, R, Barbieri, S, Marmiroli, P, Manfredini, E, et al. Anti-myelin-associated glycoprotein IgM antibody titers in neuropathy associated with macroglobulinemia. Ann Neurol. (1989) 26:543–50. doi: 10.1002/ana.410260408
12. Nobile-Orazio, E, Vietorisz, T, Messito, MJ, Sherman, WH, and Latov, N. Anti-MAG IgM antibodies in patients with neuropathy and IgM M proteins: detection by ELISA. Neurology. (1983) 33:939–42. doi: 10.1212/wnl.33.7.939
13. Kuijf, ML, Eurelings, M, Tio-Gillen, AP, van Doorn, PA, van den Berg, LH, Hooijkaas, H, et al. Detection of anti-MAG antibodies in polyneuropathy associated with IgM monoclonal gammopathy. Neurology. (2009) 73:688–95. doi: 10.1212/WNL.0b013e3181b59a80
14. Franciotta, D, Gastaldi, M, Benedetti, L, Garnero, M, Biagioli, T, Brogi, M, et al. Diagnostics of anti-MAG antibody polyneuropathy. Neurol Sci. (2017) 38:249–52. doi: 10.1007/s10072-017-3024-4
15. Liberatore, G, Giannotta, C, Sajeev, BP, Morenghi, E, Terenghi, F, Gallia, F, et al. Sensitivity and specificity of a commercial ELISA test for anti-MAG antibodies in patients with neuropathy. J Neuroimmunol. (2020) 345:577288. doi: 10.1016/j.jneuroim.2020.577288
16. Nobile-Orazio, E, Giannotta, C, and Briani, C. Anti-ganglioside complex IgM antibodies in multifocal motor neuropathy and chronic immune-mediated neuropathies. J Neuroimmunol. (2010) 219:119–22. doi: 10.1016/j.jneuroim.2009.11.012
Keywords: cell-based assay, HNK-1, human natural killer-1, IgM autoantibodies, MAG, myelin-associated glycoprotein, neuropathy
Citation: Mariotto S, de Gaspari P, Jäger D, Hahn S, Forni C, Saschenbrecker S, Lattwein E, Dinoto A and Ferrari S (2023) A novel cell-based immunofluorescence assay for the detection of autoantibodies to myelin-associated glycoprotein. Front. Neurol. 14:1289810. doi: 10.3389/fneur.2023.1289810
Edited by:
Edyta Dziadkowiak, Wroclaw Medical University, PolandReviewed by:
Željka Vogrinc, University Hospital Centre Zagreb, CroatiaCopyright © 2023 Mariotto, de Gaspari, Jäger, Hahn, Forni, Saschenbrecker, Lattwein, Dinoto and Ferrari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sandra Saschenbrecker, s.saschenbrecker@euroimmun.de
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.