 Xuezheng Li1
Xuezheng Li1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol. , 06 December 2023
Sec. Experimental Therapeutics
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1270624
Introduction: Optimal treatment strategies for post-stroke dysphagia (PSD) remain to be explored. Electroacupuncture (EA) has attracted widespread attention due to its simplicity, cheapness, and safety. However, the efficacy of EA in the treatment of PSD lacks high-level evidence-based medical support. This study aimed to systematically evaluate the clinical value of EA in the treatment of PSD.
Methods: A total of seven databases were searched for relevant literature. All randomized controlled trials (RCTs) on EA alone or EA combined with other interventions for the treatment of PSD were assessed using the modified Jadad scale. The studies with a score of ≥4 were included. The quality of the included studies was then assessed using the Cochrane Collaboration’s tool. The meta-analysis was performed using Rev. Man 5.3 software.
Results: Twelve studies involving 1,358 patients were included in the meta-analysis. Meta-analysis results showed that the EA group was superior to the control group in terms of clinical response rate (OR = 2.63, 95% CI = 1.97 to 3.53) and videofluoroscopic swallowing study (VFSS) score (MD = 0.73, 95% CI = 0.29 to 1.16). There was no significant difference between the two groups in the standardized swallowing assessment (SSA) score (MD = -3.11, 95% CI = -6.45 to 0.23), Rosenbek penetration-aspiration scale (PAS) score (MD = -0.68, 95% CI = -2.78 to 1.41), Swallowing Quality of Life (SWAL-QOL) score (MD = 13.24, 95% CI = -7.74 to 34.21), or incidence of adverse events (OR = 1.58, 95% CI = 0.73 to 3.38).
Conclusion: This study shows that EA combined with conventional treatment or other interventions can significantly improve the clinical response rate and VFSS score in patients with PSD without increasing adverse reactions.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=396840.
Swallowing disorders are one of the common complications after stroke, with a prevalence of approximately 37 to 78% in stroke patients (1). Patients with swallowing disorders may suffer from slow food intake, choking on water, and dysphagia, which seriously affect their quality of life (1). Due to a decline in swallowing function, patients are more prone to developing aspiration pneumonia (OR = 4.08, 95% CI = 2.13–7.79) (2) and malnutrition (OR = 0.91, 95% CI = 0.83–0.99) (3) or even death (OR = 4.07, 95% CI = 2.17–7.63) (2). In addition, PSD has also brought a huge economic burden to patients, families, and society. In the United States, the mean hospital stay of patients with dysphagia is 3.8 days longer than that of patients without dysphagia, which will incur an extra mean hospitalization expense of USD 6,243 (4). Therefore, it is necessary to find an effective way to treat dysphagia.
Currently, there are many clinical methods to treat dysphagia, such as swallowing training (5), neuromuscular electrical stimulation (6), non-invasive transcranial direct current stimulation (7), and balloon dilation therapy (8). Although these treatments have been employed to treat dysphagia (9), the optimal treatment protocols for dysphagia remain to be explored (10). It is generally believed that dysphagia in stroke patients is induced by a focal lesion that interrupts the connection between the nucleus tractus solitarius (NTS) and nucleus ambiguus (NA) on the same side of the lesion (11). Studies have revealed that electroacupuncture (EA) is a potential intervention strategy for dysphagia, which can improve the swallowing function through the neural circuit of the “primary motor cortex (M1) - parabrachial nucleus (PBN) - NTS” (12). However, the application of EA in the treatment of poststroke dysphagia (PSD) is still controversial. Some studies have shown that acupuncture, including EA, helps patients recover from post-stroke sequelae, like dysphagia (13, 14). However, other studies have shown that acupuncture has no effect on the recovery of patients’ functions after stroke (15, 16). A previous meta-analysis (17) only included articles comparing the efficacy of EA combined with swallowing training and single swallowing training, and the authors pointed out that the quality of the included literature was relatively poor. Therefore, these findings are inconclusive. More clinical studies on EA for the treatment of PSD have emerged afterward and shown positive therapeutic outcomes.
Therefore, this study included randomized controlled trials (RCTs) on both EA alone and EA combined with conventional interventions. Relevant articles were screened for inclusion or exclusion using the modified Jadad scale. The aim of this study was to conduct a meta-analysis of RCTs on EA and EA combined with other interventions for the treatment of poststroke dysphagia (PSD), in order to provide higher quality evidence-based basis for the clinical rehabilitation of patients with PSD.
This systematic review protocol was registered on the PROSPERO registration platform (ID: CRD42023396840) on 17 February 2023 and was conducted according to the PRISMA statement (18).
A total of seven databases were searched, including four English databases: PubMed, Embase, the Web of Science, and Cochrane Library; and three Chinese databases: CNKI, Wanfang Data, and China Biology Medicine (CBM). All publications, regardless of country, language, or article type, were searched from the inception of databases to 1 February 2023. A comprehensive search was conducted with stroke, dysphagia, and EA as keywords. Chinese search terms included “stroke,” “apoplexy,” “cerebrovascular disease,” “cerebrovascular accident”; “swallowing,” “dysphagia,” “deglutition difficulty”; “EA,” and “EA therapy.” English search terms included: “stroke,” “acute cerebrovascular lesion,” “cerebrovascular accident,” “CVAs,” “dysphagia,” “deglutition difficulty “, “deglutition disorder,” “swallowing difficult,” “electroacupuncture,” “electro-acupuncture,” and “electronic acupuncture.” The search terms and search formulas were modified and refined according to the requirements of different databases to ensure that all databases were adequately searched. The detailed search strategy is provided in Supplementary File S1.
Firstly, all RCTs on EA for the treatment of PSD were searched, whereas non-randomized studies, observational studies, experimental animal studies, qualitative studies, case reports, empirical summaries, and correspondence were excluded. Secondly, the methodological quality of the literature was assessed using the modified Jadad scale and criteria (19). Based on the scale, the studies achieving a Jadad score of less than 4 were excluded, and all RCTs on EA for the treatment of PSD with a score of 4 or higher were included, which ensured the quality of articles included in this meta-analysis.
All patients met the clear clinical diagnostic criteria for PSD: (1) diagnosis of ischemic or hemorrhagic stroke by CT or MRI and (2) diagnosis of dysphagia by clinical bedside swallowing assessment, videofluoroscopic swallowing study (VFSS), or fiberoptic endoscopic evaluation of swallowing (FEES).
The experimental interventions of the studies included in this paper included EA alone or EA combined with other interventions such as medication, rehabilitation training, neuromuscular electrical stimulation, and ice stimulation. Except for EA, the rest of the interventions should remain the same between the experimental and control groups (except for conventional acupuncture, sham acupuncture, and other blinded strategies).
To evaluate the effect of treatment on PSD, we used the following outcomes as primary outcome indicators: (1) clinical response rate, (2) VFSS score, (3) standardized swallowing assessment (SSA) score, (4) Rosenbek penetration-aspiration scale (PAS) score, and (5) Swallowing Quality of Life (SWAL-QOL) score. Secondary outcome indicators were the number and severity of adverse events to evaluate the safety of treatment.
After the search was completed, the retrieved documents were imported into Endnote 20 software. After automatic duplicate removal, the titles and abstracts of the articles were read independently by two reviewers (Li Xuezheng and Guo Hua) to exclude studies that clearly did not meet the inclusion criteria. The full texts of the remaining studies were re-screened to judge whether the articles met the inclusion criteria. Two independent investigators extracted data from the included studies. The extracted data included general information, such as first author, year of publication, sample size, randomization method, and grouping; participant information, such as sex, age, and duration of disease; intervention information, such as the number of interventions, acupuncture points, and EA parameters; outcome indicator data; follow-up outcomes and duration; and adverse events. In case of disagreement, a third reviewer (Li Hao) was consulted for adjudication.
First, two reviewers (Li Xuezheng and Guo Hua) independently evaluated the methodological quality of the included literature using the modified Jadad scale and criteria (19). Studies achieving a score of 4 or higher were considered high-quality, while those scoring less than 4 were considered low-quality. In case of disagreement, the decision was referred to a third reviewer (Li Hao).
The risk of bias in the studies achieving a score of 4 or higher was then assessed using the Cochrane Collaboration’s tool (20). Items in the tool are divided into seven sectors: (A) Random sequence generation; (B) Allocation concealment; (C) Blinding of participants and personnel; (D) Blinding of outcome assessment; (E) Incomplete outcome data; (F) Selective reporting; and (G) Other bias. The risk of bias in the searched original articles was assessed, and the included studies were rated as having a “Low,” “High,” or “Unclear” risk of bias. Based on the above seven sectors of items, these articles were classified as “Yes” (low bias for A - E; high bias for F - G), “No” (high bias for A - E; low bias for F - G), and “Unclear” (lack of relevant information or presence of uncertain bias). Two reviewers (Li Xuezheng and Fu Xuefeng) independently conducted the assessment. In case of disagreement, a third reviewer (Lu Lijun) was consulted for adjudication.
Finally, the level of evidence for each outcome indicator was assessed independently by two investigators (Lijun Lu and Xuefeng Fu) using the Grade Pro tool from five aspects: “Risk of bias,” “Inconsistency,” “Indirectness,” “Imprecision,” and “Publication bias.” If there was a disagreement, it was resolved by the decision of the third reviewer (Xuezhen Li).
Statistical analysis of the included RCT studies was performed using Review Manager 5.3 software. Data included dichotomous and continuous variables. Odds ratios (ORs) with 95% confidence intervals (CIs) were used to represent dichotomous variables; while mean differences (MDs) with 95% CIs were used to represent continuous variables. Heterogeneity among studies was determined by the I2 test. If I2 < 50%, a fixed-effects model was used for data analysis; conversely, if I2 ≥ 50%, a random-effects model was adopted. A funnel plot was used to test publication bias.
The literature screening PRISMA flow chart is shown in Figure 1. Literature was carefully screened for eligibility according to the principles of Population, Intervention, Comparison, Outcomes, and Study (PICOS). The search in seven databases identified a total of 1,115 documents. After excluding 575 duplicates, 540 publications were left. After the initial screening of titles and abstracts, 344 articles were obtained, and 250 irrelevant articles were further excluded by reading the full text. Quality assessment was performed on the remaining 94 articles, and 82 low-quality articles (Jadad score < 4) were excluded. Finally, 12 high-quality eligible articles were included (14, 21–31).
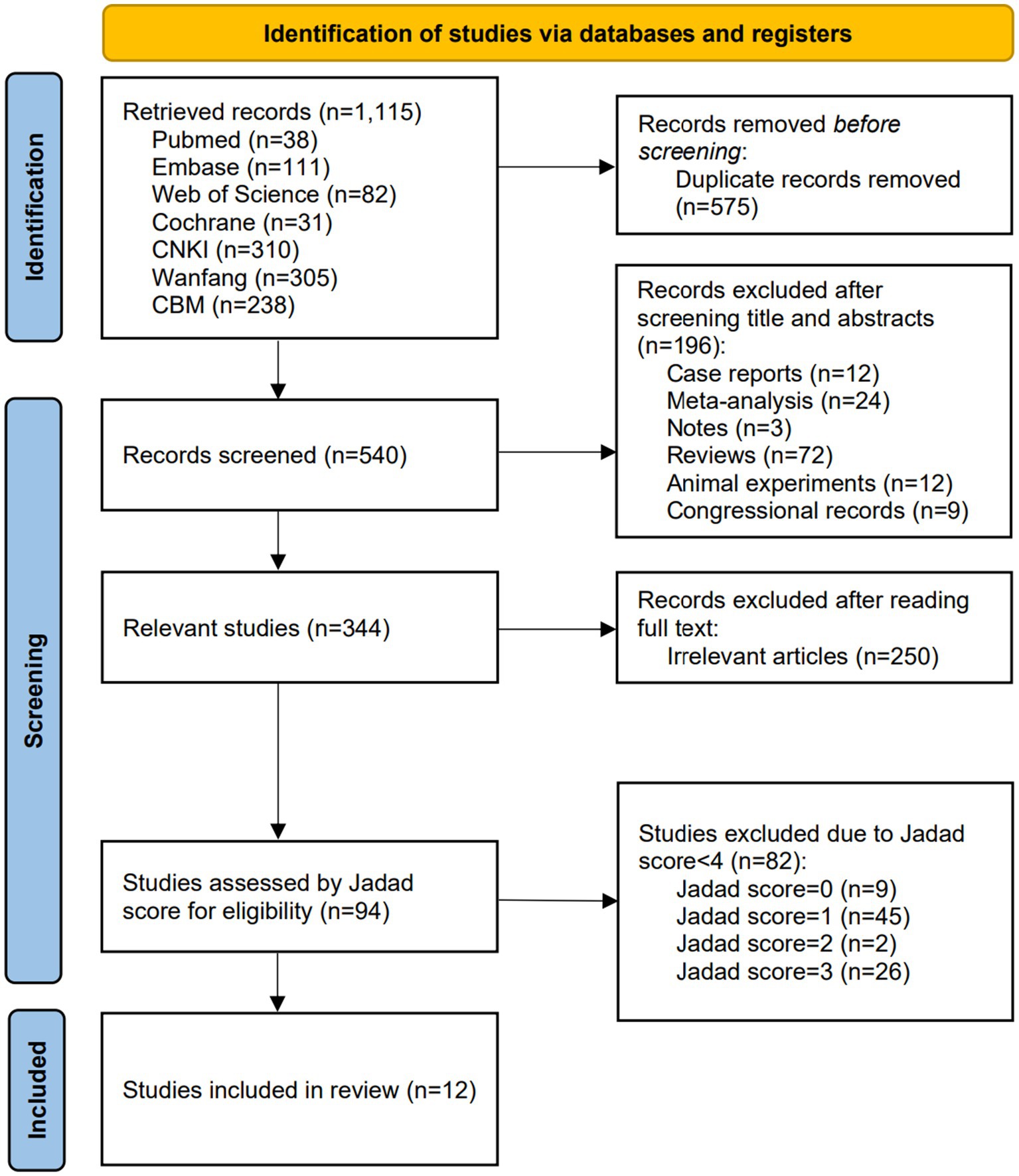
Figure 1. Flow diagram for the selection of the included studies.
The basic information of the included studies is shown in Table 1. A total of 12 articles were included, with all the studies conducted in China. They were published between 2011 and 2022, with two of them published in English and the remaining 10 in Chinese. The total number of eligible cases was 1,358, including 747 cases in the experimental group and 611 cases in the control group. In all of these trials, the frequency of EA interventions was at least five times per week and the duration was at least 2 weeks. Two articles (22, 28) included two pairs of trials, five (14, 23, 26, 28, 29) had subject dropout, and three (14, 28, 31) reported subject follow-up, with no follow-up lasting longer than 3 months. The articles reported the following outcome indicators: (1) 10 articles reported clinical response rate (14, 21–23, 25–29, 31); (2) two articles reported VFSS scores (14, 22); (3) five articles reported SSA scores (21, 27–29, 31); (4) three articles reported PAS scores (24, 27, 30); (5) three articles reported SWAL-QOL scores (28, 29, 31); and (6) seven articles mentioned adverse effects (14, 21–24, 28, 29).
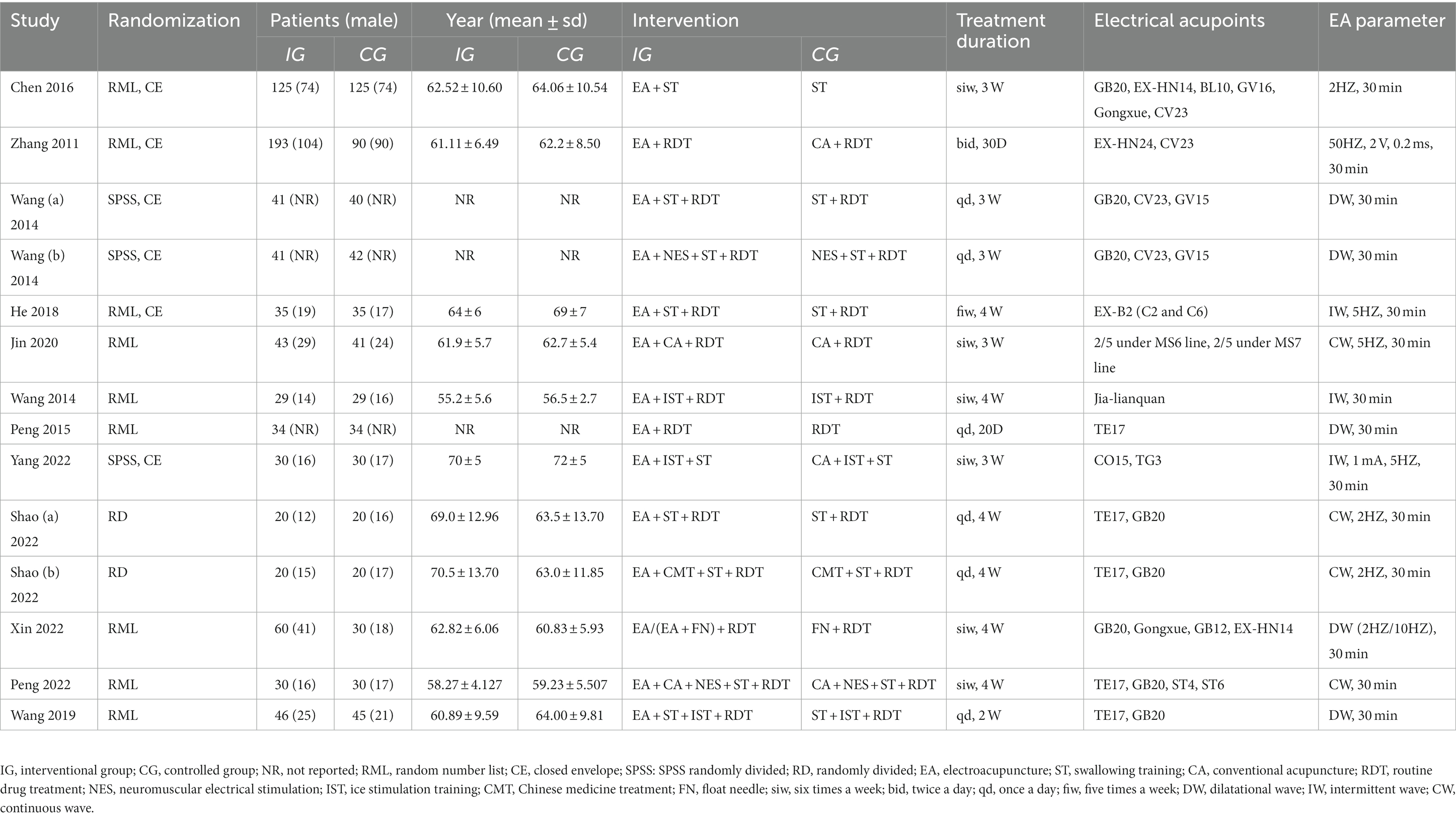
Table 1. Characteristics of the included studies.
The Jadad scores of the articles included in this study are shown in Table 2. All 12 included articles mentioned randomized grouping, and 11 of them mentioned random number tables or similar methods. Five articles described randomization concealment through computer control or in other specific ways such as the use of sealed envelopes. Six articles stated that the trials were blinded, with three of them describing specific measures. Nine articles did not have subject dropout or described the number and reasons for subject dropout after it occurred.
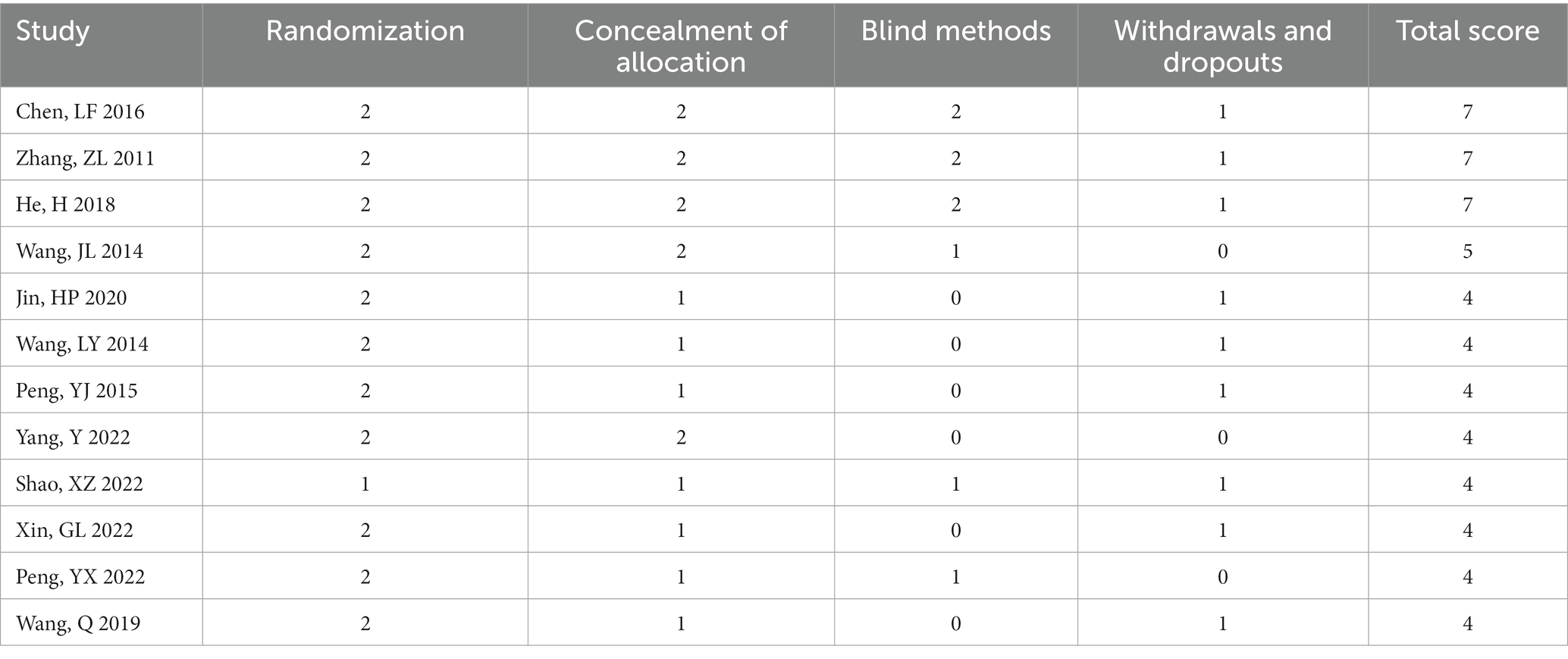
Table 2. Jadad scores of the included studies.
The quality evaluation of the 12 included articles is shown in Figure 2 and Figure 3. Based on the Cochrane Collaboration’s tool for assessing the risk of bias, it was found that the risk of bias (14, 21, 23) was relatively low in three studies and unclear in nine studies (22, 24–31). As shown in Figure 4, a funnel plot was used to reflect the publication bias. The symmetrical curve graph showed that the publication bias of these studies was relatively low.

Figure 2. Methodological quality summary: review authors’ judgments about each study’s methodological quality.
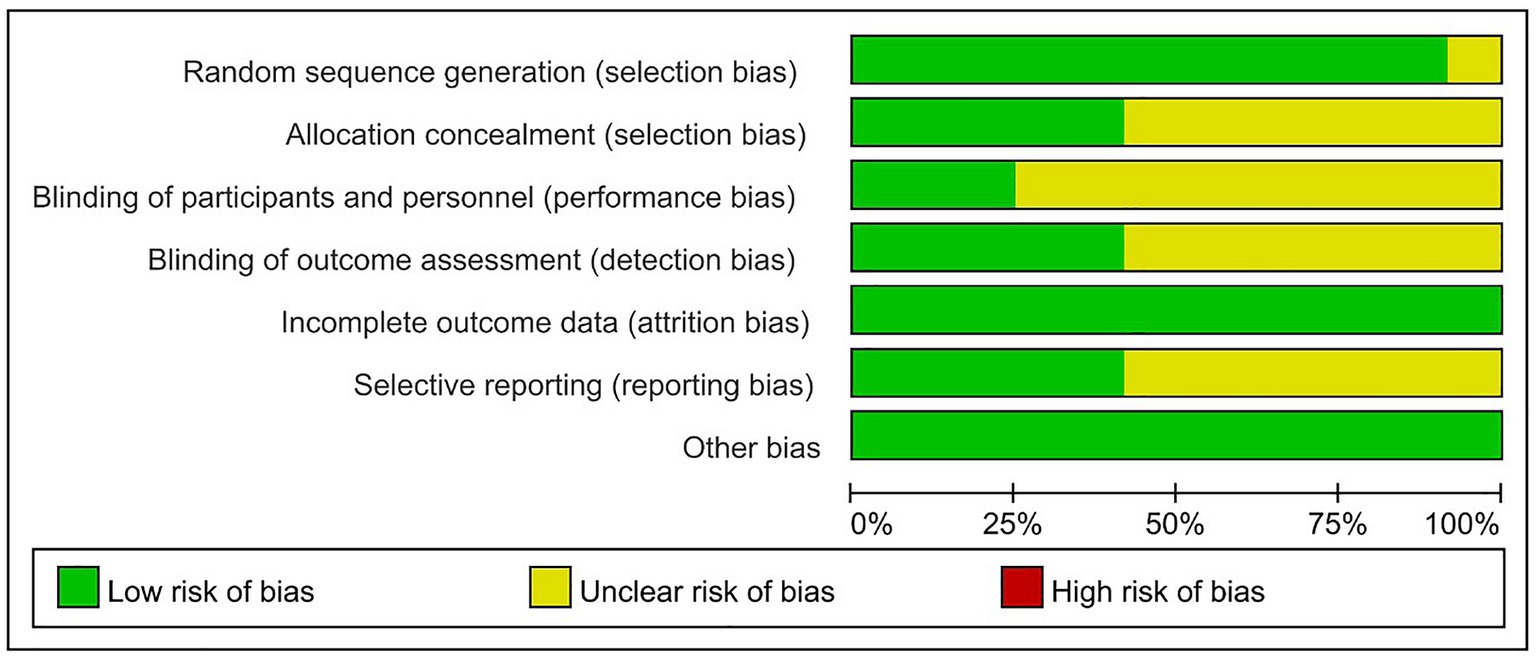
Figure 3. Methodological quality graph: review authors’ judgments about each study’s methodological quality.
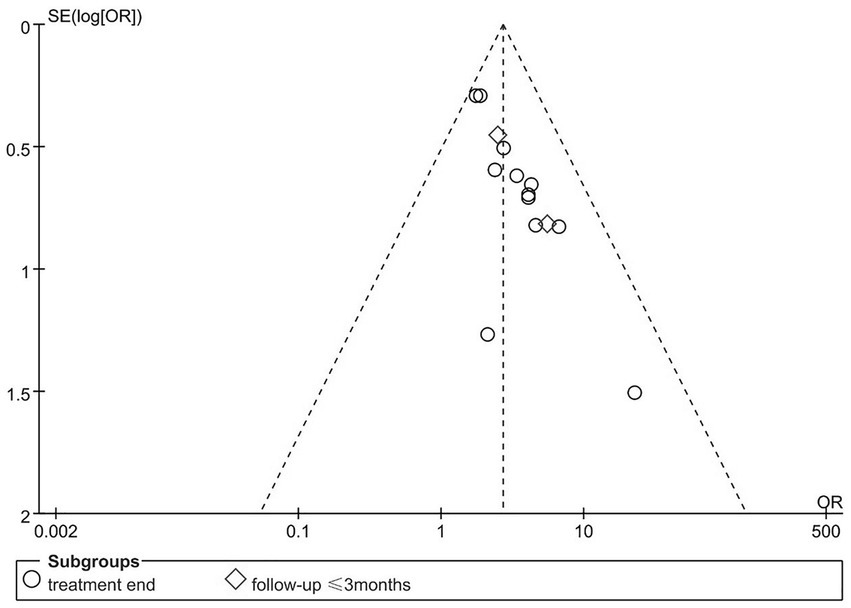
Figure 4. Publication bias of the involved studies.
Finally, the evidence level of all outcome indicators was evaluated using the Grade Pro tool. The results showed that the evidence level of all outcome indicators remained at moderate or higher, with six outcome indicators assessed as high evidence level. The evidence level of each outcome indicator is shown in Supplementary File S2.
The clinical response rate was reported in 10 articles with 12 pairs of trials, including 644 subjects in the experimental group and 507 in the control group. A meta-analysis of 12 RCTs was performed using a fixed-effects model, and the results are shown in Figure 5. The results showed that the EA group was significantly more effective than the control group in terms of response rate (OR = 2.63, 95% CI = 1.97 to 3.53, p < 0.00001). Among them, the clinical response rate was reflected in three studies according to changes in the VFSS score. A subgroup analysis was conducted, indicating that the efficacy of the EA group was significantly superior to that of the control group (OR = 2.16, 95% CI = 1.35 to 3.46, p = 0.001). In five studies, the clinical response rate was reflected according to changes in the water swallow test (WST) score, revealing that the EA group had significantly higher efficacy than the control group (OR = 2.72, 95% CI = 1.77 to 4.19, p < 0.00001).
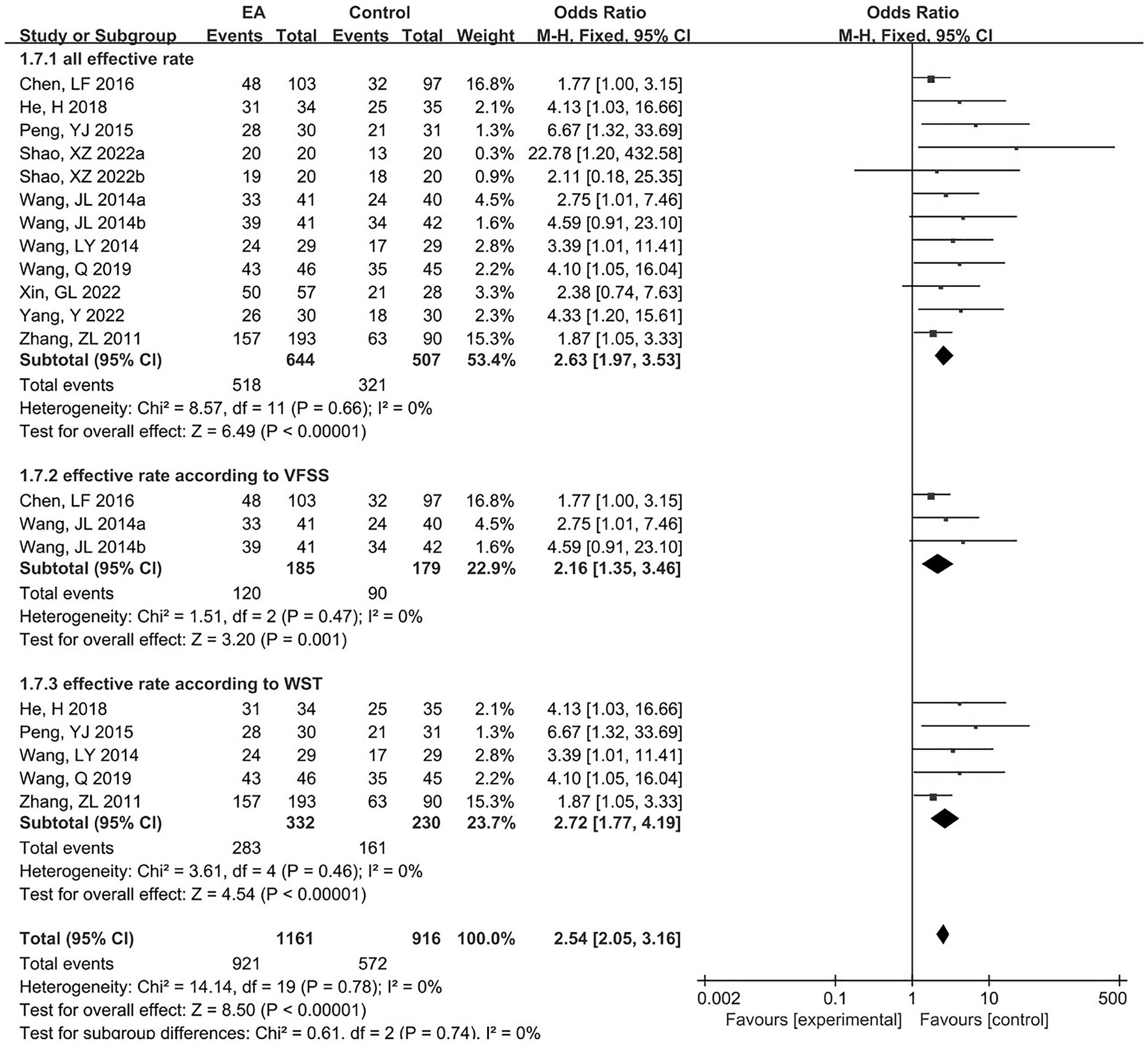
Figure 5. The forest plot of the effectiveness rate.
Two articles reported VFSS scores, including three pairs of trials, with 150 subjects in the experimental group and 147 in the control group. A meta-analysis of the three RCTs was performed using a fixed-effects model, and the results are shown in Figure 6. The results showed that the EA group showed more significant improvement in VFSS scores than the control group (MD = 0.73, 95% CI = 0.29 to 1.16, p = 0.001).

Figure 6. The forest plot for VFSS.
Five articles reported SSA scores, including six pairs of trials, with 365 subjects in the experimental group and 230 in the control group. A meta-analysis of the six RCTs was conducted using a fixed-effects model, and the results are shown in Figure 7. The results showed that there was no statistical difference in SSA scores, although there was an improvement in the EA group (MD = -3.11, 95% CI = -6.45 to 0.23, p = 0.07). In addition, two articles (totaling three sets of trials) reported follow-up results. Subgroup analysis was performed and showed no statistical difference in SSA scores (MD = -3.40, 95% CI = -7.59 to 0.79, p = 0.11), but the combined effect size was statistically different (MD = -3.22, 95% CI = -5.83 to −0.61, p = 0.02).
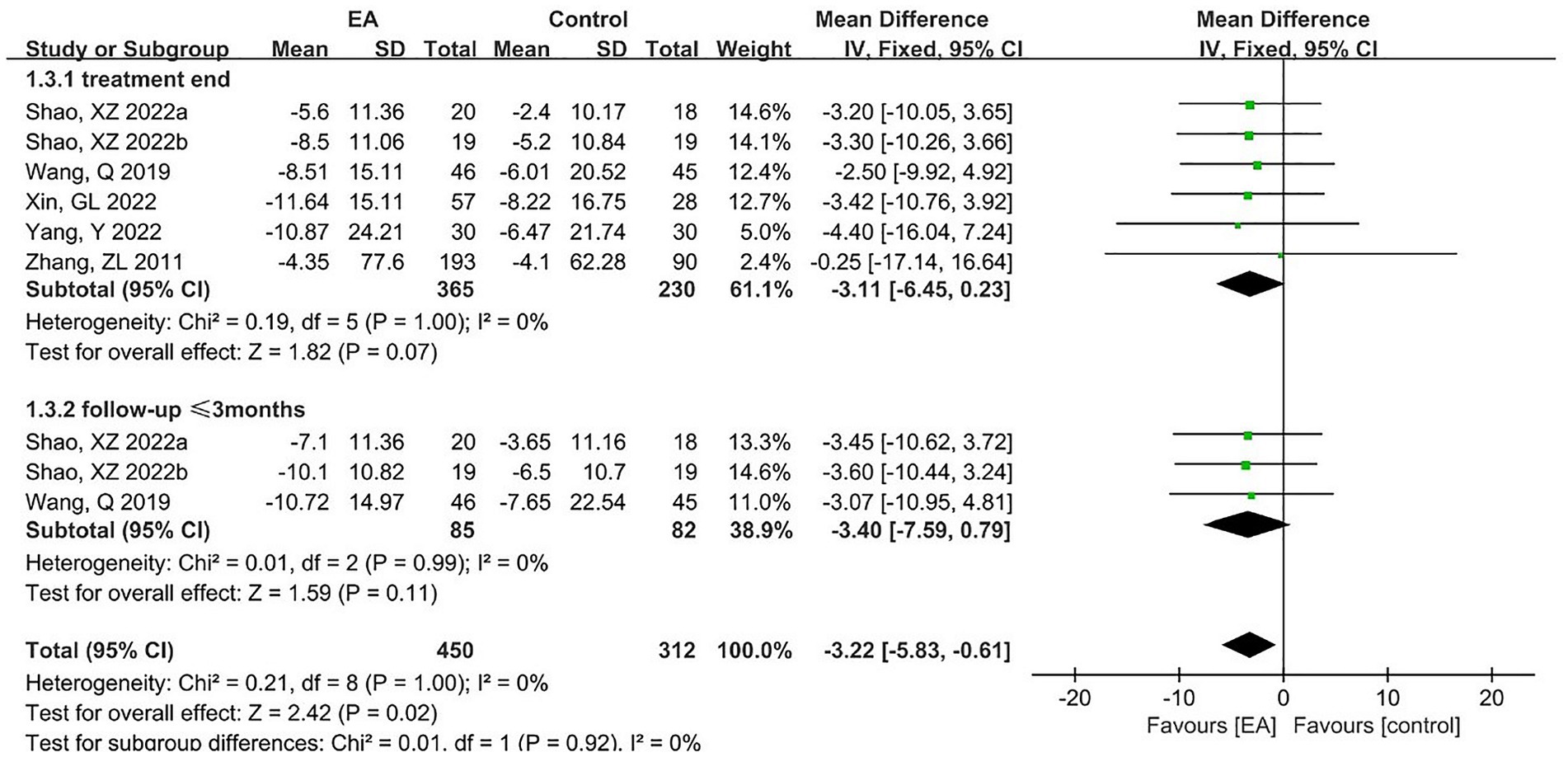
Figure 7. The forest plot for SSA.
Three articles reported PAS scores, with 103 subjects in the experimental group and 101 in the control group. A meta-analysis of the three RCTs was performed using a fixed-effects model, and the results are shown in Figure 8. The results showed that in terms of PAS scores, there was an improvement in the EA group but no statistical difference (MD = -0.68, 95% CI = -2.78 to 1.41, p = 0.52).

Figure 8. The forest plot for PAS.
Three articles reported SWAL-QOL scores, including four pairs of trials, with 142 subjects in the experimental group and 110 in the control group. A meta-analysis of four RCTs was performed using a fixed-effects model, and the results are shown in Figure 9. The results showed that in terms of SWAL-QOL scores, there was an improvement in the EA group but no statistical difference (MD = 13.24, 95% CI = -7.74 to 34.21, p = 0.22). In addition, two articles (totaling three pairs of trials) reported follow-up results. Subgroup analysis was performed and showed no statistical difference in SWAL-QOL scores (MD = 12.96, 95% CI = -19.58 to 45.50, p = 0.44).
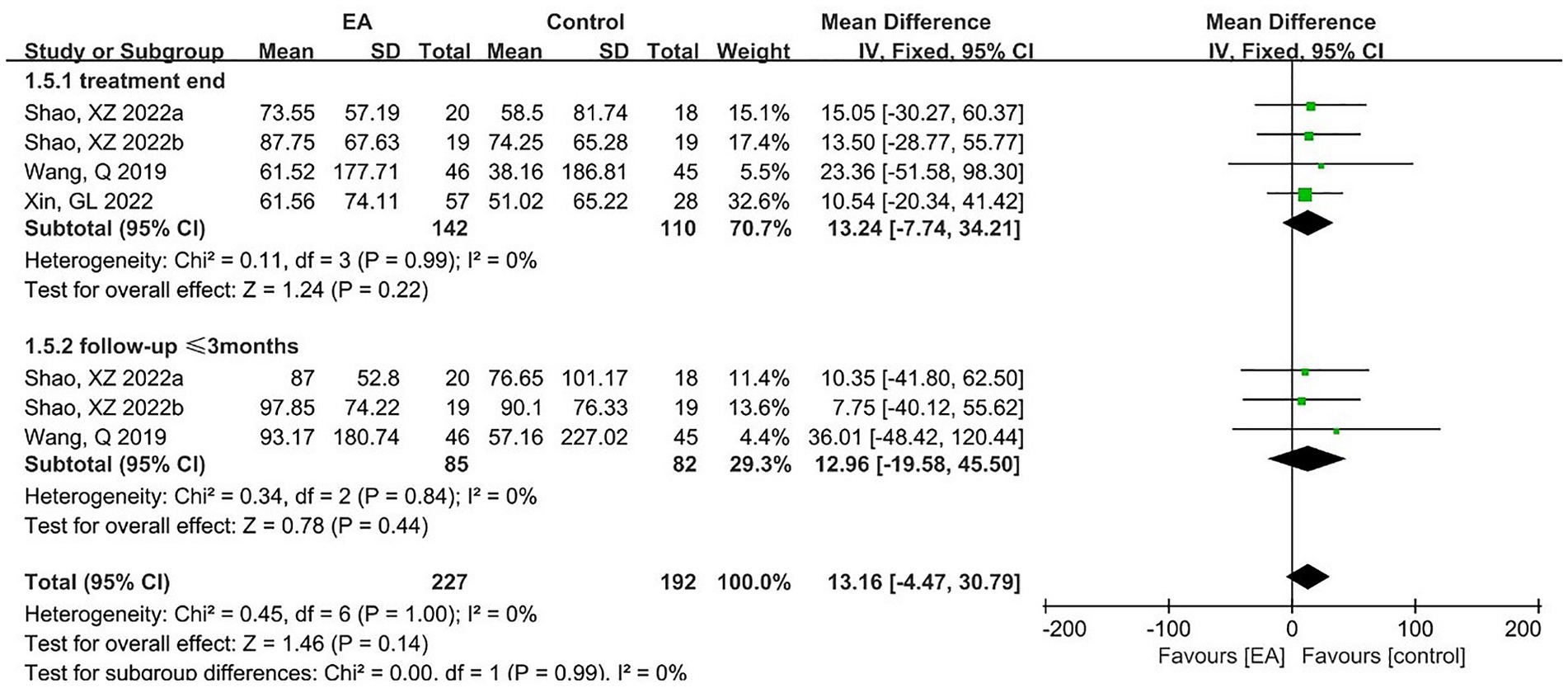
Figure 9. The forest plot for SWAL-QOL.
Adverse reactions were reported in seven articles, two of which were excluded because the specific number of subjects with adverse reactions was not described. The remaining five RCTs were subjected to meta-analysis, with 430 subjects in the experimental group and 291 in the control group. Adverse reactions included local numbness, subcutaneous hemorrhage, pain, and papular dermatitis. However, none of them were serious, and there were no life-threatening serious adverse events. A fixed-effects model was adopted for the meta-analysis, and the results of the meta-analysis are shown in Figure 10. The results showed no significant difference between the two groups in terms of adverse reactions, and EA did not increase the incidence of adverse reactions (OR = 1.58, 95% CI = 0.73 to 3.38, p = 0.24).
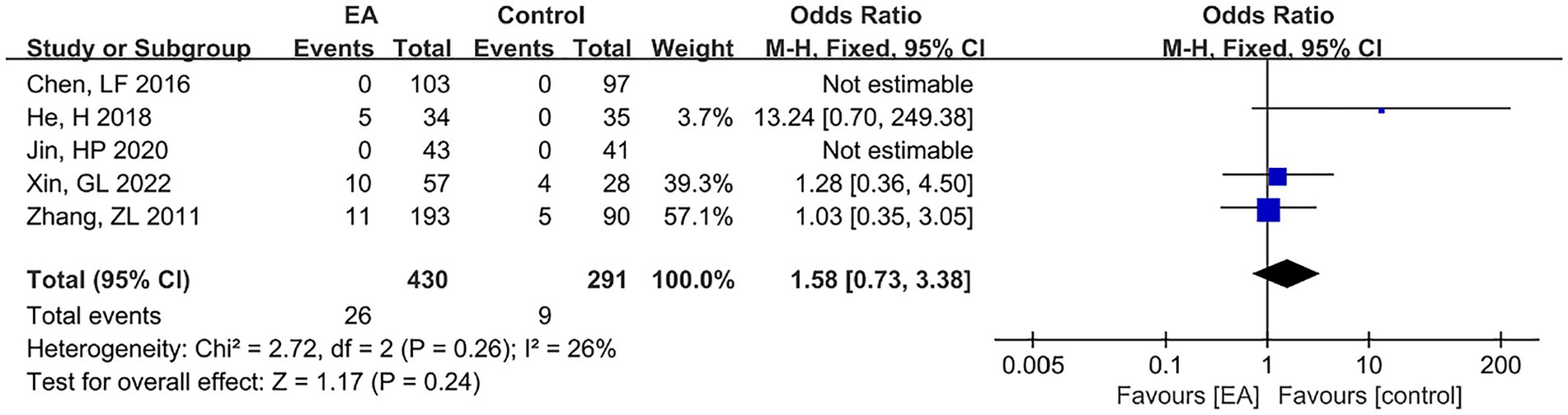
Figure 10. The forest plot for adverse events.
This meta-analysis included 12 RCTs involving 1,358 patients with PSD. The results showed that EA could benefit patients with PSD in terms of the clinical response rate and VFSS score after the exclusion of low-quality literature and the inclusion of the latest studies.
Two meta-analyses (17, 32) previously published on the similar topic were also searched. In the study conducted by Huang JK et al. (17), although beneficial results were concluded, the authors pointed out that the quality of the included articles was relatively low. Accordingly, such results were not conclusive enough. Another meta-analysis published in a Chinese journal was a similar case (32), in which all the 18 articles included had a high risk of bias. Furthermore, some results of the two meta-analyses were significantly heterogeneous, but the reasons for heterogeneity were not discussed in either of them. These meta-analyses only included the articles on the comparison between EA combined with swallowing training and swallowing training alone, and excluded the studies on EA combined with other treatments. There is no study assessing whether the addition of EA will still be conducive to the rehabilitation of dysphagia when multiple interventions are combined. In our study, therefore, the studies on EA alone and EA combined with other interventions were included, while low-quality RCTs were excluded using the modified Jadad scale, which made our results more reliable and convincing. The assessment of evidence level also confirmed our judgment. The evidence level was high for six outcome indicators in this study, proving that the overall quality of this paper is high.
Based on our study results, there was no significant difference between both groups in the SSA score, PAS score, SWAL-QOL score, and incidence of adverse events. In terms of the clinical response rate and VFSS score, the improvement of the EA group was significantly superior to that of the control group. Our findings in the clinical response rate were the same as those concluded from previous meta-analyses (17, 32). However, the clinical response rate was not assessed using a unified measurement tool in previous meta-analyses. In our study, a subgroup analysis was conducted according to different measurement tools. Among the included studies, the clinical response rate was weighed according to changes in the VFSS score in three studies, while it was weighed based on the WST score in five studies. The results of the subgroup analysis still revealed that EA benefited patients and had relatively low heterogeneity. Therefore, our study was more credible from the perspective of the clinical response rate. Moreover, VFSS is the “gold standard” for the evaluation of dysphagia (33, 34). Based on our study findings, both the clinical response rate obtained from VFSS and the VFSS score showed that EA improved PSD. The efficacy of EA based on VFSS has also been demonstrated in the study conducted by Zhang Shengyu et al. (35), which is consistent with our observations.
Notably, EA did not improve the SSA score, PAS score, or SWAL-QOL score, which was inconsistent with the results of the clinical response rate and VFSS score. This may be related to different acupoint selections. It was found that in studies where the VFSS score was involved, the acupoint of Lianquan (CV23) was selected in all trials. In studies where the SSA score was involved, CV23 was selected in only one trial (21). In studies where PAS and SWAL-QOL scores were involved, it was not selected in any trial. The study conducted by Yuan S et al. (36) showed that administering EA on CV23 could regulate the swallowing function through excitatory neurons in the paraventricular hypothalamus. By comparing the effects of administering EA on CV23 and Neiguan (PC6), Ye QP et al. found that administering EA on CV23 could regulate the swallowing function by activating swallowing-related interneurons in the ventrolateral medulla oblongata (37). In addition, in a recent study, Ye QP et al. also demonstrated through optogenetics and chemogenetics that the NTS is involved in the regulation of EA on CV23 for PSD, revealing the role of the M1-NTS pathway in EA on CV23 (38). The latest research shows that in addition to the central nervous system, EA on CV23 can also have an impact on the peripheral nervous system and the local swallowing muscles. The study conducted by Yuan S et al. (39) suggests that TRPV1 at the CV23 can regulate local blood perfusion, thereby promoting the recovery of swallowing function. In combination with our study results, we believe that this may suggest a certain value of administering EA on CV23 in the improvement of PSD.
Additionally, we also recognize that the studies on EA in modern medicine have been increasingly getting advanced with the progress of science and technology. A growing number of articles are emerging to study and demonstrate the efficacy of EA with the aid of advanced equipment and technology. Wu Wenbao et al. (40) combined cerebral diffusion tensor imaging (DTI) techniques and VFSS to explore the clinical significance of acupuncture intervention in PSD. They administered EA on the acupoints of Sishencong, Baihui, Temple, Fengchi, and Tongue Triple Acupuncture and found that the fractional anisotropy (FA) values in the infarcted areas of the cerebral hemispheres were improved significantly, and that FA values were positively correlated with the integrity of white matter fiber tracts (41), suggesting that EA on relevant acupoints may have restored cortical function. Zhu Runjia et al. (42) observed the clinical efficacy of EA in the treatment of ischemic stroke through transcranial Doppler (TCD), finding that EA stimulation could improve the intracranial vascular function of patients. The main action principle is to reduce vascular resistance by changing the elasticity and compliance of the corresponding blood vessel, so as to increase cerebral blood supply and promote rehabilitation after stroke, thus indirectly improving the swallowing function. Lan Chunwei et al. (43) observed the effect of EA on PSD through magnetic resonance spectroscopy (MRS) and surface electromyography (sEMG), finding that EA could decrease the contents of rNAA and Lac/Cr in the brain to reduce the mean amplitude of sEMG in the pharynx and shorten the swallowing time course. Their findings indicate that EA improves the swallowing function of patients with PSD by influencing brain metabolism and ameliorating the contraction of peripheral swallowing muscles. Most of the outcome indicators included in our study were scale scores. In fact, we also wanted to analyze the efficacy of EA in combination with microcosmic study data. However, it was a pity that among our included studies, EEG was performed in only one study to detect the degree of cerebral cortex inhibition (24); a transcranial magnetic stimulator was used in one study to detect the effect of EA on motor-evoked potential (MEP) (27), and sEMG was performed in one study to quantitatively assess swallowing muscle groups (29). In this context, we cannot provide further evidence to explore the efficacy of EA. More high-quality studies are desired to solve this problem in the future.
We also acknowledge that this systematic review has some limitations. Firstly, based on the Cochrane Collaboration’s tool for assessing the risk of bias, nine of our included studies (22, 24–31) had unclear risk of bias. For example, Shao XZ et al. (28) only expressed random allocation but did not describe the specific method for random allocation, which reduced the quality of this meta-analysis. Secondly, some outcome indicators were only involved in two to three studies. In this regard, the insufficient sample size was also one of our regrets. Finally, it was impossible to continue the efficacy analysis of EA from the perspective of new technology since there were few studies reporting microcosmic study data.
In spite of some limitations, the findings of this systematic review are still of great clinical and basic scientific significance. In combination with previous meta-analyses (17, 32), we are surer that EA is a safe and reliable treatment approach for patients with PSD. Although further studies are still required to demonstrate the efficacy of EA (acupoint selection in EA or with the aid of new technology), this paper still provides a new evidence-based basis for the clinical rehabilitation of patients with PSD and offers the orientation and theoretical support for future studies. Therefore, our study is indeed of great value.
In conclusion, EA is effective and safe in treating PSD. EA combined with conventional treatment or other interventions can significantly improve the clinical response rate and VFSS score in patients with PSD, without increasing the incidence of adverse reactions. There is no statistical difference between the two groups in terms of the improvement of SSA score, PAS score, and SWAL-QOL score. More high-quality RCT studies are still needed in the future to further explore the efficacy of EA in the treatment of PSD.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
XL: Formal analysis, Investigation, Writing – original draft, Writing – review & editing. HL: Formal analysis, Investigation, Writing – original draft. WY: Methodology, Writing – original draft. HG: Formal analysis, Investigation, Writing – review & editing. KG: Methodology, Writing – review & editing. LL: Writing – review & editing. XF: Writing – review & editing. ZH: Conceptualization, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by a project grant from the Guangzhou Municipal Science and Technology Bureau (No. 202201011729).
We thank all the investigators and supporters who participated in and supported this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1270624/full#supplementary-material
1. Martino, R, Foley, N, Bhogal, S, Diamant, N, Speechley, M, Teasell, R, et al. Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke. (2005) 12:2756–63. doi: 10.1161/01.STR.0000190056.76543.eb
2. Banda, KJ, Chu, H, Kang, XL, Liu, D, Pien, LC, and Jen, HJ. Prevalence of dysphagia and risk of pneumonia and mortality in acute stroke patients: a Meta-analysis. BMC Geriatr. (2022) 22:420. doi: 10.1186/s12877-022-02960-5
3. Tagliaferri, S, Lauretani, F, Pelá, G, Meschi, T, and Maggio, M. The risk of dysphagia is associated with malnutrition and poor functional outcomes in a large population of outpatient older individuals. Clin Nutr. (2019) 38:2684–9. doi: 10.1016/j.clnu.2018.11.022
4. Patel, DA, Krishnaswami, S, Steger, E, Conover, E, Vaezi, MF, Ciucci, MR, et al. Economic and survival burden of dysphagia among inpatients in the United States. Dis Esophagus. (2018) 31:1–7. doi: 10.1093/dote/dox131
5. Park, HS, Oh, DH, Yoon, T, and Park, JS. Effect of effortful swallowing training on tongue strength and oropharyngeal swallowing function in stroke patients with dysphagia: a double-blind, randomized controlled trial. Int J Lang Commun Disord. (2019) 54:479–84. doi: 10.1111/1460-6984.12453
6. Park, JS, Oh, DH, Hwang, NK, and Lee, JH. Effects of neuromuscular electrical stimulation combined with effortful swallowing on post-stroke oropharyngeal dysphagia: a randomised controlled trial. J Oral Rehabil. (2016) 43:426–34. doi: 10.1111/joor.12390
7. Mao, H, Lyu, Y, Li, Y, Gan, L, Ni, J, Liu, L, et al. Clinical study on swallowing function of brainstem stroke by Tdcs. Neurol Sci. (2022) 43:477–84. doi: 10.1007/s10072-021-05247-6
8. Hu, T, Cai, Y, Shen, Z, Chen, A, Wu, Y, Song, T, et al. A novel balloon catheter-based dilation intervention for patients with Cricopharyngeus achalasia after stroke: a randomized study. Dysphagia. (2022) 37:1414–22. doi: 10.1007/s00455-021-10400-6
9. Li, LX, Deng, K, and Qu, Y. Acupuncture treatment for post-stroke dysphagia: an update Meta-analysis of randomized controlled trials. Chin J Integr Med. (2018) 24:686–95. doi: 10.1007/s11655-018-3005-3
10. Cohen, DL, Roffe, C, Beavan, J, Blackett, B, Fairfield, CA, Hamdy, S, et al. Post-stroke dysphagia: a review and design considerations for future trials. Int J Stroke. (2016) 11:399–411. doi: 10.1177/1747493016639057
11. Panebianco, M, Marchese-Ragona, R, Masiero, S, and Restivo, DA. Dysphagia in neurological diseases: a literature review. Neurol Sci. (2020) 41:3067–73. doi: 10.1007/s10072-020-04495-2
12. Yao, L, Ye, Q, Liu, Y, Yao, S, Yuan, S, Xu, Q, et al. Electroacupuncture improves swallowing function in a post-stroke dysphagia mouse model by activating the motor cortex inputs to the nucleus Tractus Solitarii through the parabrachial nuclei. Nat Commun. (2023) 14:810. doi: 10.1038/s41467-023-36448-6
13. Vados, L, Ferreira, A, Zhao, S, Vercelino, R, and Wang, S. Effectiveness of acupuncture combined with rehabilitation for treatment of acute or subacute stroke: a systematic review. Acupunct Med. (2015) 33:180–7. doi: 10.1136/acupmed-2014-010705
14. Chen, L, Fang, J, Ma, R, Gu, X, Chen, L, Li, J, et al. Additional effects of acupuncture on early comprehensive rehabilitation in patients with mild to moderate acute ischemic stroke: a multicenter randomized controlled trial. BMC Complement Altern Med. (2016) 16:226. doi: 10.1186/s12906-016-1193-y
15. Kong, JC, Lee, MS, Shin, BC, Song, YS, and Ernst, E. Acupuncture for functional recovery after stroke: a systematic review of sham-controlled randomized clinical trials. Can Med Assoc J. (2010) 182:1723–9. doi: 10.1503/cmaj.091113
16. Bai, YL, Li, L, Hu, YS, Wu, Y, Xie, PJ, Wang, SW, et al. Prospective, randomized controlled trial of physiotherapy and acupuncture on motor function and daily activities in patients with ischemic stroke. J Altern Complement Med. (2013) 19:684–9. doi: 10.1089/acm.2012.0578
17. Huang, J, Shi, Y, Qin, X, Shen, M, Wu, M, and Huang, Y. Clinical effects and safety of electroacupuncture for the treatment of poststroke dysphagia: a comprehensive systematic review and meta-analysis. Evid Based Complement Alternat Med. (2020) 2020:1560978–9. doi: 10.1155/2020/1560978
18. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DG. Preferred reporting items for systematic reviews and Meta-analyses: the Prisma statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
19. Jadad, AR, Moore, RA, Carroll, D, Jenkinson, C, Reynolds, DJ, Gavaghan, DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. (1996) 17:1–12. doi: 10.1016/0197-2456(95)00134-4
20. Higgins, JP, Altman, DG, Gøtzsche, PC, Jüni, P, Moher, D, Oxman, AD, et al. The Cochrane collaboration's tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
21. Zhang, Z, Zhao, S, Chen, G, Ji, X, Xue, L, and Yang, Y. Treatment of dysphagia after apoplexy by deep-acupuncture Chonggu point: a randomized controlled study. Chin Acupunct Moxibust. (2011) 31:385–90. doi: 10.13703/j.0255-2930.2011.05.002
22. Wang, J, Ding, D, Tan, F, Wan, S, Wu, H, Huang, T, et al. Clinical study on the treatment of swallowing disorder in acute cerebral infarction by neuromuscular electrical stimulation combined with electroacupuncture. Chongq Med. (2014) 43:4071–3. doi: 10.3969/j.issn.1671-8348.2014.30.030
23. He, H, Zhang, W, Zhu, J, Peng, H, Wang, X, and Liao, X. Treatment of post-stroke dysphagia with electroacupuncture based on cervical pinch points. Shanghai J Acu-mox. (2018) 37:852–5. doi: 10.13460/j.issn.1005-0957.2018.08.0852
24. Jin, H, Li, X, Ye, Q, and Wang, Y. Effect of bilateral cephalometric electrical stimulation on swallowing chronological parameters and cortical excitability in patients with cortical post-stroke dysphagia. Acupunct Res. (2020) 45:473–9. doi: 10.13702/j.1000-0607.190697
25. Wang, L, and Huang, G. Efficacy of electroacupuncture combined with ice stimulation in the treatment of post-stroke dysphagia. J Tradit Chin Med. (2014) 36:57–8.
26. Peng, Y, Sun, J, Wang, H, Chen, L, and Sheng, C. Efficacy of electroacupuncture in the treatment of patients with post-stroke pseudobulbar palsy. World Chin Med. (2015) A02:2.
27. Yang, Y, and Jin, HP. Observations on Efficacy of Auricular Electrical Stimulation for Dysphagia After Cerebral Infarction and Its Effect on Motor Evoked Potential. Shanghai J Acu-mox. (2022) 41:760–764. doi: 10.13460/j.issn.1005-0957.2022.08.0760
28. Shao, X, Chen, B, Zhu, L, Zhu, L, Zheng, J, Pu, X, et al. The Effects of Adding Di-Tan Decoction (DTD) and/or Electroacupuncture (EA) to Standard Swallowing Rehabilitation Training (SRT) for Improving Poststroke Dysphagia (PSD): A Pilot, Single-Centred, Randomized Trial. Evid Based Complement Alternat Med. (2022) 2022:2011597. doi: 10.1155/2022/2011597
29. Xin, G, Wang, L, Li, J, Liang, B, Guo, X, Wang, Y, et al. Effect of floating acupuncture combined with electroacupuncture on swallowing function and surface myoelectricity in patients with post-stroke dysphagia. Chin Arch Tradit Chin Med. (2022) 40:36–40. doi: 10.13193/j.issn.1673-7717.2022.12.008
30. Peng, Y, Tang, M, Chen, T, Lu, X, and Huang, F. Effect of crossed electric item needling combined with swallowing training on swallowing function and pulmonary infection in post-stroke tracheotomy patients. J Guangzhou Univ Trad Chin Med. (2022) 39:83–7. doi: 10.13359/j.cnki.gzxbtcm.2022.01.015
31. Wang, Q, Man, B, and Xu, J. Treatment of post-ischemic stroke dysphagia with "Tong guan Li Qiao" acupuncture method. Jilin J Chin Med. (2019) 39:1469–72. doi: 10.13463/j.cnki.jlzyy.2019.11.020
32. Geng, J, Gao, Y, Cao, B, Zhao, Y, Liu, W, and Wang, J. Meta-analysis of the efficacy of electroacupuncture for post-stroke dysphagia Shaanxi. J Tradit Chin Med. (2021) 42:1814–8.
33. Langmore, SE. History of Fiberoptic Endoscopic Evaluation of Swallowing for Evaluation and Management of Pharyngeal Dysphagia: Changes over the Years. Dysphagia. (2017) 1:27–38. doi: 10.1007/s00455-016-9775-x
34. Allen, J, Blair, D, and Miles, A. Assessment of videofluoroscopic swallow study findings before and after cricopharyngeal myotomy. Head Neck. (2017) 9:1869–1875. doi: 10.1002/hed.24846
35. Zhang, S, Liu, S, Wu, W, Chen, Y, Liao, K, Xiang, Y, et al. Efficacy of Vitalstim Acupoint Electroacupuncture combined with rehabilitation training in the treatment of post-stroke swallowing disorder. Acupunct Res. (2017) 42:168–72. doi: 10.13702/j.1000-0607.2017.02.015
36. Yuan, S, Deng, B, Ye, Q, Wu, Z, Wu, J, Wang, L, et al. Excitatory neurons in paraventricular hypothalamus contributed to the mechanism underlying acupuncture regulating the swallowing function. Sci Rep. (2022) 12:5797. doi: 10.1038/s41598-022-09470-9
37. Ye, Q, Liu, C, Shi, J, You, H, Zhao, J, Liu, J, et al. Effect of electro-acupuncture on regulating the swallowing by activating the interneuron in ventrolateral medulla (Vlm). Brain Res Bull. (2019) 144:132–9. doi: 10.1016/j.brainresbull.2018.11.021
38. Ye, Q, Yuan, S, Yao, L, Dai, Y, Deng, B, Hu, J, et al. Participation of the nucleus Tractus Solitarius in the therapeutic effect of electroacupuncture on post-stroke dysphagia through the primary motor cortex. CNS Neurosci Ther. (2023). doi: 10.1111/cns.14442
39. Yuan, S, Qiu, B, Liang, Y, Deng, B, Xu, J, Tang, X, et al. Role of Trpv 1 in electroacupuncture-mediated signal to the primary sensory cortex during regulation of the swallowing function. CNS Neurosci Ther. (2023). doi: 10.1111/cns.14457
40. Wu, WB, Fan, DF, Que, BF, Lian, QQ, Zheng, C, Tang, LL, et al. Clinical effect of Liyan Tongqiao acupuncture in treatment of post-stroke dysphagia: an analysis based on diffusion tensor imaging. Zhen Ci Yan Jiu. (2020) 45:985–9. doi: 10.13702/j.1000-0607.200085
41. Mourão, LF, Friel, KM, Sheppard, JJ, Kuo, HC, Luchesi, KF, Gordon, AM, et al. The role of the Corpus callosum in pediatric dysphagia: preliminary findings from a diffusion tensor imaging study in children with unilateral spastic cerebral palsy. Dysphagia. (2017) 32:703–13. doi: 10.1007/s00455-017-9816-0
42. Zhu, R, Xu, M, Ge, L, Chen, C, Su, X, Zhang, L, et al. Clinical study of the effect of Electroacupuncture on rehabilitation and Tcd in convalescent stroke patients. Shanghai J Acu-mox. (2015) 34:389–92. doi: 10.13460/j.issn.1005-0957.2015.05.0389
43. Lan, C, Liu, T, Yuan, K, Li, J, Liu, S, and Wang, Q. Effect of Electroacupuncture on cerebral Neurometabolites of magnetic resonance spectroscopy and surface electromyography in patients with post-stroke dysphagia. Guid J Trad Chin Med Pharm. (2020) 26:97–101. doi: 10.13862/j.cnki.cn43-1446/r.2020.16.024
Keywords: stroke, dysphagia, electroacupuncture, meta-analysis, systematic review, randomized controlled trials
Citation: Li X, Lu L, Fu X, Li H, Yang W, Guo H, Guo K and Huang Z (2023) Systematic review and meta-analysis of the efficacy and safety of electroacupuncture for poststroke dysphagia. Front. Neurol. 14:1270624. doi: 10.3389/fneur.2023.1270624
Edited by:
Yang Ye, Peking University Third Hospital, ChinaReviewed by:
Mostafa Meshref, Al-Azhar University, EgyptCopyright © 2023 Li, Lu, Fu, Li, Yang, Guo, Guo and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhen Huang, mishz@126.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.