
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 02 November 2023
Sec. Neurorehabilitation
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1270296
 Gabriella Paparella1*
Gabriella Paparella1* Cristina Stragà1Marinela Vavla2
Cristina Stragà1Marinela Vavla2 Nicola Pesenti3Vasco Merotto1Gian A. Martorel1
Nicola Pesenti3Vasco Merotto1Gian A. Martorel1 Sara Zalunardo1Maria Armellin1Jimmy Comiotto4
Sara Zalunardo1Maria Armellin1Jimmy Comiotto4 Andrea Martinuzzi1
Andrea Martinuzzi1Introduction: The relevance of rehabilitation in progressive neurological disorders, such as Friedreich’s Ataxia (FRDA), has yet to be convincingly proven. FRDA is characterized by ataxia, loss of gait, scoliosis, cardiomyopathy, dysarthria and dysphagia, with reduced life expectancy. The disease onset is usually in adolescence, leading to progressive disability. Omaveloxolone has been recently approved as the first pharmacological treatment for FRDA in adults and adolescents aged 16 years and older. Regarding non-pharmacological therapies, neurorehabilitation is a valuable aid in addressing the symptoms and in maintaining the residual functioning. We performed a prospective observational cohort study to evaluate the efficacy of inpatient rehabilitation (IR) for people with FRDA.
Methods: A total of 42 individuals (29 adults and 13 children) with FRDA were recruited. There were 27 ambulant and 15 non-ambulant participants. The patients underwent IR of 3 and 4 weeks in children and adults, respectively. The IR treatment was designed to be applied within a multidisciplinary setting, so FRDA patients underwent, in addition to physiotherapy, also occupational therapy, practical manual activities and psychological support aiming to enhance transferable skills useful in the activities of daily living. The primary outcome was the Scale for the Assessment and Rating of Ataxia (SARA). Other measures were: Friedreich Ataxia Rating Scale (FARS) and Nine Hole Peg Test (NHPT). Furthermore, we used the 6 Minute Walk Test (6MWT), the Timed Up and Go (TUG) and the Berg Balance Scale (BBS) only on ambulant subjects. Outcomes were evaluated at baseline and at the end of the treatment.
Results: We report that the IR significantly improves motor performance and ataxia symptoms in patients with FRDA. Our study shows significant functional improvement in all the outcome measures used, except for NHPT bilaterally. FARS and SARA scores post-IR are significatively reduced when compared (p < 0.001).
Discussion: We demonstrate that IR programs in FRDA can provide a meaningful clinical improvement in terms of outcome measures. These findings could be useful when approaching progressive neurological disorders.
Friedreich’s ataxia (FRDA) is an autosomal recessive neurodegenerative disorder. It is caused by an intronic GAA triplet repeat expansion in the FXN gene on chromosome 9 (1). Frataxin is a mitochondrial protein involved in iron homeostasis. The decreased frataxin production determines increased mitochondrial iron and free radicals leading to cellular damage and death, mostly in cardiac muscle, pancreatic islet cells and the nervous system (2). The age of onset is typically within the first two decades of life and individuals are wheelchair-bound 10–15 years after disease onset (3). FRDA is characterized by a progressive gait and limb ataxia, dysarthria, upper (UL) and lower limb (LL) areflexia, decreased vibration sense and LL muscular weakness. There are also non neurological signs such as scoliosis, pes cavus, hypertrophic cardiomyopathy and diabetes mellitus. Often, scoliosis and pes cavus can anticipate the neurological signs (3, 4). Age of onset, progression and severity are not uniformly distributed across patients, but variably correlate with the short allele expansion size (3, 5, 6). Treatment options are currently very limited for FRDA patients. In early 2023 Omaveloxolone has been approved as the first and only pharmacological treatment for FRDA in adults and adolescents aged 16 years and older. It is capable of improving modified Friedreich Ataxia Rating Scale (mFARS) score after chronic treatment (7–9).
Movement in humans is based on the continuous interaction between the individual, the task and the environment (10). The motor skills learning is more concentrated on achieving goals rather than acquiring specific movements. Therefore, the acquisition and adaptation of motor skills involves processes associated with practice and experience. The cerebellum, involved in the interface between the sensorimotor and cognitive control domains, has a direct role in the coordination, shape and fine control of movement and cognitive functions (11). It integrates sensory inputs, mainly visual, proprioceptive and vestibular, with voluntary motor action in order to ensure timing, duration and amplitude of the muscle activity (12). The cerebellum also plays a fundamental role in internal models for the adaptation of the motor gesture during a task (feed-forward control) and motor-learning (11–13). Accordingly, individuals with cerebellar ataxia present impairments in motor learning regarding both simple and complex motor skills, which can limit functional recovery. For this reason, physiotherapy treatment in patients with degenerative ataxia has long been the subject of discussion (12, 13).
Neurorehabilitation is recognized as one of the most useful non-pharmacological therapies to clinically improve cerebellar disorders involving balance, gait ataxia, UL and LL incoordination and postural sway (14–20). The majority of studies have been carried out with patients with spinocerebellar ataxia, and very few have been performed in the FRDA population. These studies present a significant heterogeneity with respect to characteristics of the participants, outcome measures, the training type, intensity and duration of rehabilitation and the settings of interventions.
Milne et al. (21) performed an interesting systematic review of rehabilitation interventions for subjects with degenerative genetic ataxia. Out of a total of 292 subjects involved, only 67 were affected by FRDA. Seven types of intervention were proposed in the examined studies: coordination and balance training, multifaceted inpatient rehabilitation, a cycling regime, balance training, treadmill training, occupational therapy and inspiratory muscle training. Several settings were contemplated: inpatient, outpatient and home-based.
Only few studies have considered a multidisciplinary inpatient approach (16, 20, 22). Among them, the work of Miyay et al. (22) that described in detail the combined treatment of occupational therapy and physiotherapy, even if on patients not FRDA, is very interesting.
Milne et al. (21) state that “coordination and balance training and multifaceted inpatient rehabilitation demonstrated the greatest percentage change in the SARA, while multifaceted inpatient rehabilitation appeared to have the greatest impact on function.” Additionally, “preliminary findings suggest that multifaceted programs incorporating more than one focus, such as coordination and balance training or multidisciplinary inpatient programs, may have greater effect than singularly focused therapies such as balance training or occupational therapy alone.”
Considering intensity, some authors have pointed out that the effectiveness of interventions is also correlated with the intensity of exercise (15, 17). Regarding the duration, improvements in ataxia apparently require a minimum of 4 weeks (21).
The majority of multidisciplinary work involved only patients aged 15 years or older. A systematic review by Hartley et al. (23) concluded that the studies analyzed show promising results but no definitive conclusions could be drawn on the effectiveness of exercise and physical therapy in children.
The published literature so far provides detailed protocols related to the physiotherapy program only (19, 24). These protocols focus not only on balance and coordination, but also on muscle strengthening and proprioception. In light of the previous studies, we hypothesized that multidisciplinary intensive IR could be beneficial to FRDA, and perhaps modify disease progression. Such setting would allow also for minimizing possible environmental confounders and thus it was deemed as the most appropriate for a prospective study.
According to the International Classification of Functioning, Disability and Health (ICF) (25), health is the product of the interaction of the contextual factors with the individual functioning and disability is defined as a negative interaction among these factors. Thus, following the bio-psychosocial model of the ICF it is possible to obtain the information on health starting from the evaluation of body functions and structures, activities and participation, but necessarily considering how the contextual factors modulate the individual functioning in the various situations of life. The activities are the execution of a task or set of actions by an individual and participation is the involvement in a life situation. The importance of the role of occupations and the close relationship between the person, activity and the environment emerge (26). Our goal is not only to work on function, but also on activity and participation optimizing in the same time the contextual factors.
Therefore, we designed an experiment aiming to assess, by means of standardized ataxia outcome measures, the efficacy of neurorehabilitation as IR in FRDA, in patients with different age range and disease severity. The second aim was to create and test a specific IR protocol tailored to the specific needs and functional disabilities in FRDA.
This was a prospective observational cohort study, as classified by the Institutional Review Board (IRB). The study scheme is presented in Figure 1.

Figure 1. Study scheme. IR, inpatient rehabilitation.
A total of 42 individuals with FRDA were recruited at the “Eugenio Medea” Scientific Institute in Pieve di Soligo and Conegliano (Treviso, Italy) to take part in this study. All participants and their parents/legal tutors were informed regarding the experimental nature of the study and signed the informed consent in accordance with the Declaration of Helsinki (World Medical Association, 1964). The study was reviewed and approved by the competent Ethics Committee (Prot. No 051/11-CE).
The inclusion criteria were: genetic diagnosis of FRDA with GAA trinucleotide expansion or gene mutation, willingness to participate in the study. Exclusion criteria included contemporary participation in other clinical trials or introduction of new disease modifying treatments; any other form of physiotherapy external to the study protocol, any acute condition or orthopedic injury that could eventually limit the ability to fully participate in the intensive therapy schedule.
The patients underwent an IR protocol created at the study center ad hoc for FRDA patients, considering their main needs and disability impairments as identified by the appropriate ICF categories and qualifiers (Table 1).
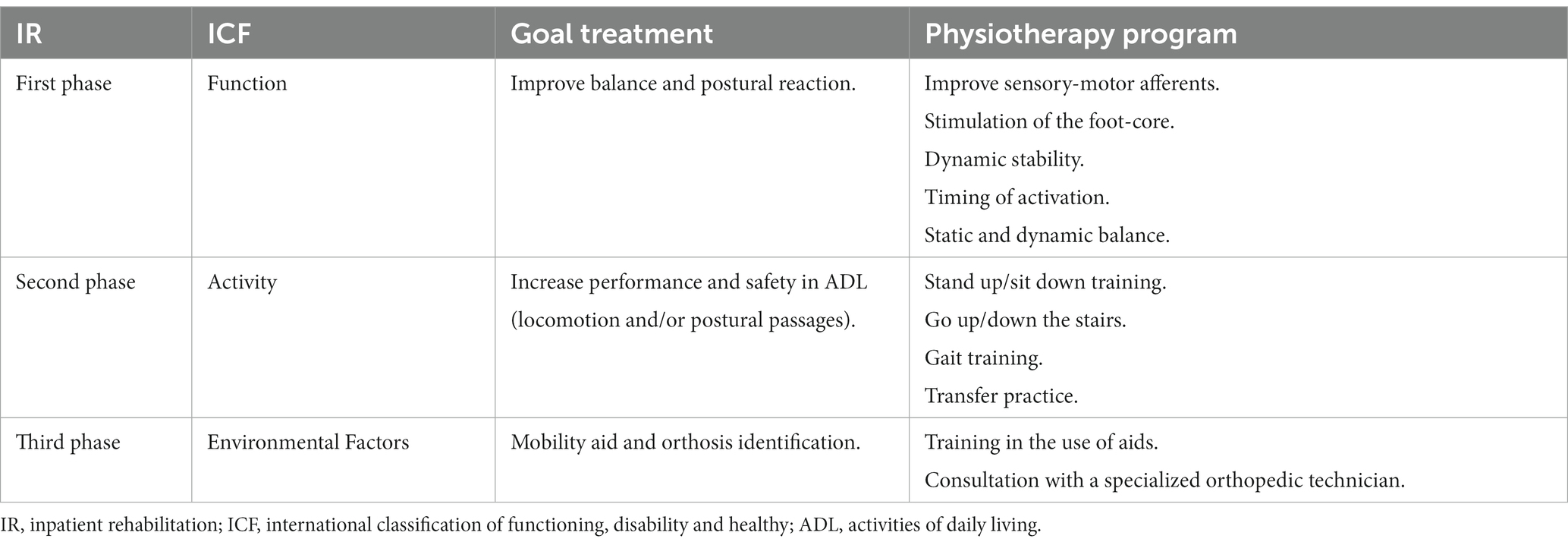
Table 1. Summary of the IR study protocol.
The FRDA program, based in an individualized IR ward, consisted of a multidisciplinary management (physiotherapy, occupational therapy, practical manual activities, psychological support, speech therapy, clinical psychology). Our goal was to focus not only on function but also on activity and participation by modulating environmental factors.
The IR duration was set to be of 3 and 4 weeks in children and adults, respectively. Literature shows that a period of intensive rehabilitation of at least 4 weeks can improve the function in FRDA (21). Therefore, we chose a 4 weeks duration IR for the adults and 3 weeks duration IR for the children cohort. The latter group duration was tailored in relation to their maximal compliance abilities. All patients received 11 weekly physiotherapy sessions of 45 min each (2 daily sessions from Monday to Friday and 1 session on Saturday morning).
The focus of the physiotherapy program was to improve physical abilities, in particular trunk stability and postural control with activation of deep trunk musculature. This was performed conveying the correct sensitive information, performing the accurate stimulation of the anticipatory postural adjustments (APAs) that would eventually lead to a reduction of the synergism and compensations of postural muscles, and furthermore an adequate orientation of proximal segments and finally distal coordination.
The physiotherapy program was goal-related and specifically designed in accordance with the level of clinical severity. The cohort was divided into two groups: ambulant and non-ambulant. Based on the staging of the Friedreich’s Ataxia Rating Scale (FARS), ambulant patients were considered to be those able to walk, even with any type of aid (FARS stage ≤4.0). Non-ambulant patients were the ones confined to wheelchairs (27). The former underwent program oriented to improve balance and gait pattern, subsequently preventing falls and inactivity. The latter underwent program oriented to trunk control, ULs motility and training of safer and more functional transfer techniques.
Physiotherapy was designed to be applied within a multidisciplinary setting. Therefore, FRDA patients also underwent occupational therapy, practical manual activities and psychological support aiming to enhance transferable skills useful in the activities of daily living (ADLs). In particular, occupational therapy and practical manual activities were useful to strengthen and maintain the skills acquired in the physiotherapy setting.
Patients performed 4 occupational therapy sessions of 45 min each per week. Occupational therapy goals are highly individualized and are set to help individuals improve their ability to perform daily activities and enhance their quality of life. The occupational therapy program empathized coordinative task of the upper limbs and trunk and dual-motor task such as handling objects while standing and walking.
Adult subjects also performed practical manual activities (6/week of 45 min each). The activity consists in carrying out laboratory activities (e.g., construction of wooden products, drawings, mosaic compositions, weaving of wicker baskets). Such activities can be carried out sitting or standing, depending on the severity of the patient. For the children, these activities were integrated into occupational therapy.
All patients received psychological support (3/week of 45 min each) for disease acceptance and elaboration of their experience, for coping strategy and acceptance of adaptations and aids identified by the physiotherapist and occupational therapist.
Moreover, in the first week of hospitalization, all patients underwent neuropsychological assessment and speech therapy in 5 and 3 sessions (45 min each) respectively. The speech therapist evaluated swallowing and language.
The detailed protocol of interventions is illustrated in Table 2.
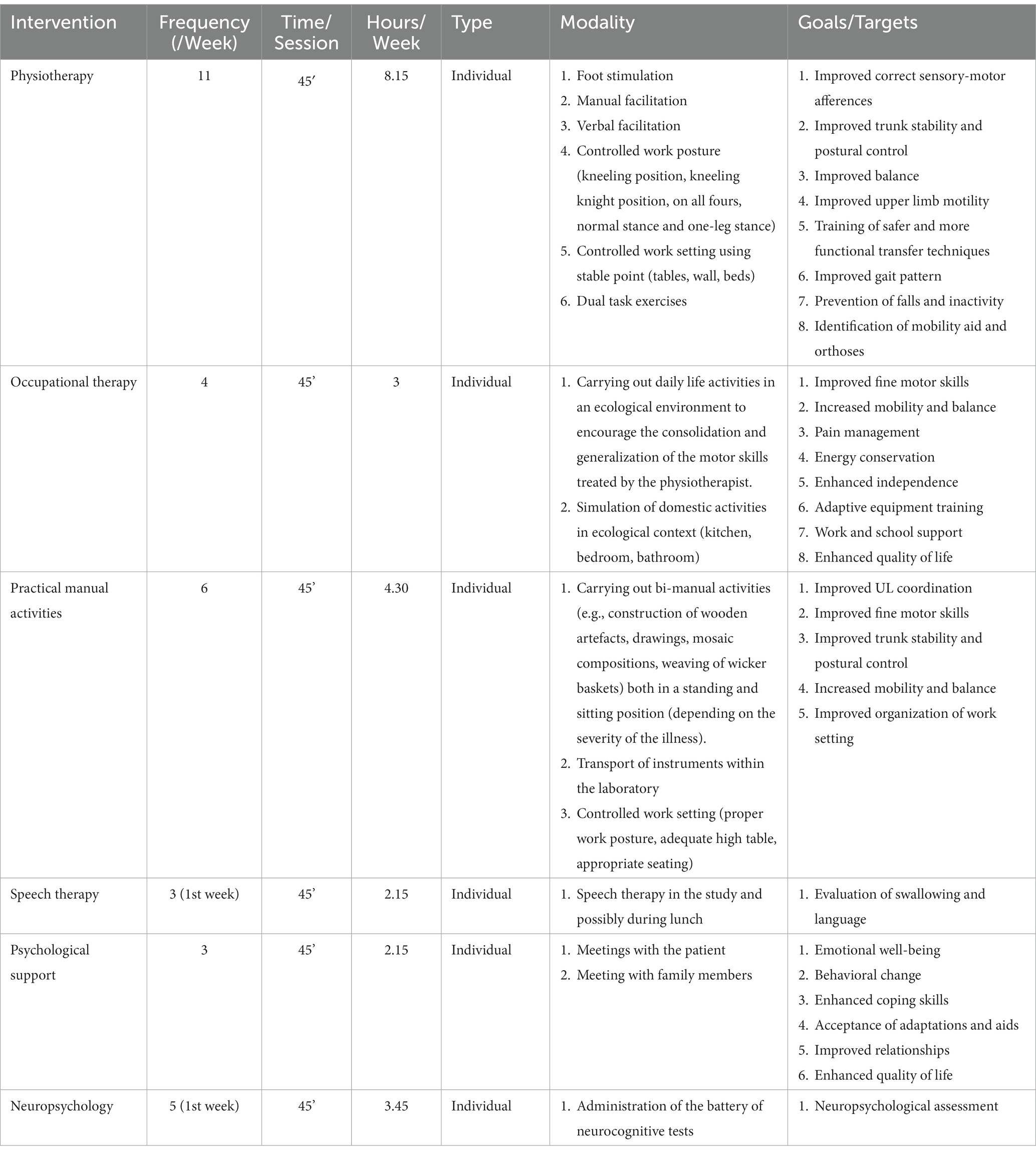
Table 2. Detailed protocol of interventions.
Patients were clinically assessed according to a specific clinical protocol administered by trained and expert physiotherapists. The assessing physiotherapists were not directly involved in the treatment sessions. The assessments were taken at the same time of the day for both pre-IR and post-IR assessment.
The primary outcome was the Scale for the Assessment and Rating of Ataxia (SARA) (28) that is based on a semi-quantitative clinical assessment of cerebellar ataxia (spinocerebellar, Friedreich’s and sporadic ataxia) on an impairment level. SARA has 8 items (gait, stance, sitting, speech, finger-chase, nose-finger, fast alternating movements, heel-shin). It has a maximum score of 40 (severe ataxia) and a minimum of 0 (no ataxia).
Other measures included were the Friedreich Ataxia Rating Scale (FARS) (27) that is a disease-specific outcome measures comprising a functional ataxia staging score, activities of daily living (ADL) subscale, a neurological exam (bulbar, upper limb coordination, lower limb coordination, peripheral nervous system and upright stability) and instrumental tests such as Nine Hole Peg Test (NHPT) (29) to assess hand dexterity bilaterally. NHPT is the most commonly used tool for assessing manual dexterity. It consists of a plastic console with a round dish for the pegs at one end and a nine-hole peg-board at the opposite end. Subject must take pegs from a container, one by one, and insert them into the holes in the board, as quickly as possible. Then the patient has to remove the pegs from the holes, one by one, and put them back in the container. The total time to complete the activity is recorded. Both the dominant and non-dominant hand are tested twice. The Friedreich Ataxia Rating Scale neurologic examination (nFARS) consists of 5 subscales directed to bulbar function (maximum of 11 points), upper limb coordination (maximum of 36 points), lower limb coordination (maximum of 16 points), peripheral nervous system (maximum of 26 points), and upright stability (US; maximum of 28 points). The neurological exam has a maximum score of 117 (severe ataxia). The staging systems used in ataxia are mainly based on walking disability. The score ranges between 0 (normal) to 6 (confined to wheelchair or bed with total dependency for all activities of daily living. Total disability).
Furthermore, only on ambulant subjects, we used the 6 Minute Walk Test (6MWT) (30, 31) to measure the ambulation skills and the Timed Up and Go test (TUG) (32) that assesses mobility, balance, walking ability, and fall risk. The equilibrium was assessed by the Berg Balance Scale (BBS) (33) (range 0–56), a 14-item validated scale that assesses balance abilities during sitting, standing and positional changes (scores of ≤43.5 suggest risk of falls).
Patient characteristics were summarized using descriptive statistics. Mean (SD), median (IQr) were used for continuous variables with normal and non-normal distribution, respectively. Absolute frequency (Percentage) for categorical variables.
To evaluate the intervention effect pre-post we used paired T-test or Wilcoxon signed rank test based on the normality of the distribution. Comparison between the extent of improvement for the outcome measures between different groups (ambulant vs. non-ambulant subjects and adults vs. children), independent t-test or Mann–Whitney U test were used.
Spearman’s correlation coefficient was used to study the correlation between disease duration or the number of triplets and the extent of improvement.
All tests were two-tailed and p < 0.05 was considered significant. All statistical analyses were performed using R version 4.0.1 (R Foundation for Statistical Computing, Austria) (34).
According to defined inclusion criteria we recruited 42 patients, 29 adults and 13 children (age range 8–11 years N = 2; age range 12–17 years N = 11), with an age of 20.7 ± 8.6 (mean ± SD) years and disease duration of 8.9 ± 4.7 years. Patients declared an age at onset of about 11.7 ± 7.7 years. There were 29 females (69%). Thirty-nine of the patients’ cohort were homozygous for the GAA repeat expansion (93%). Three participants had a heterozygous GAA expansion (two presented a 460 GAA repeat expansion on one allele and a nonsense point mutation on the other; one carried a 666 GAA repeat expansion on one allele and a nonsense point mutation on the other). The mean GAA repeat expansion in the short-allele (GAA1) was 701.1 ± 136.8 (range 383–956), while the long allele (GAA2) counted for 911.8 ± 197.5 (range 460–1,436). The mean SARA score was 17.4 ± 7.8 (range 6.0–32.5), therefore patients of variable severity were included. Twenty-seven patients (64%) were able to walk with or without walking aids on a level surface. In particular: 18 of them walk independently (8 adults and 10 children), 5 with a walker, 2 with support (wall or person), 1 with a cane and 1 with crutches.
The demographic and clinical data of patients are presented in Table 3.

Table 3. Demographic and clinical data of patients included in this study.
All patients underwent IR, completing the proposed treatment and no adverse event was reported by any of the participants. All patients were evaluated according to the clinical protocol. Non-ambulant patients were not subjected to the following tests: 6MWT, BBS, TUG. Only three patients did not perform the BBS and one the TUG scale as these scales were initially optional.
Assessments were carried out at the beginning of the IR (pre) and at the end (post). Table 4 presents evolutions of the scales administered to the entire cohort of patients. All patients benefited from rehabilitation treatment in all measured scales. We observed a significant reduction in SARA scale (from 17.4 to 16.1, average reduction of 1.3, p < 0.001). Similar significant variations were found also in total FARS scale (average reduction of 4.3, p < 0.001) and in all its subscales (average reduction FARS LL of 1.1, p < 0.001; FARS UL: 2.1, p < 0.001; FARS US: 1.1, p < 0.001), as shown in Figure 2. In NHPT there was a reduction in the task execution time but the change was not statistically significant in either the dominant hand or the non-dominant one (see Figure 3).

Table 4. Comparison of the scales administered to the entire cohort of patients pre vs. post IR.
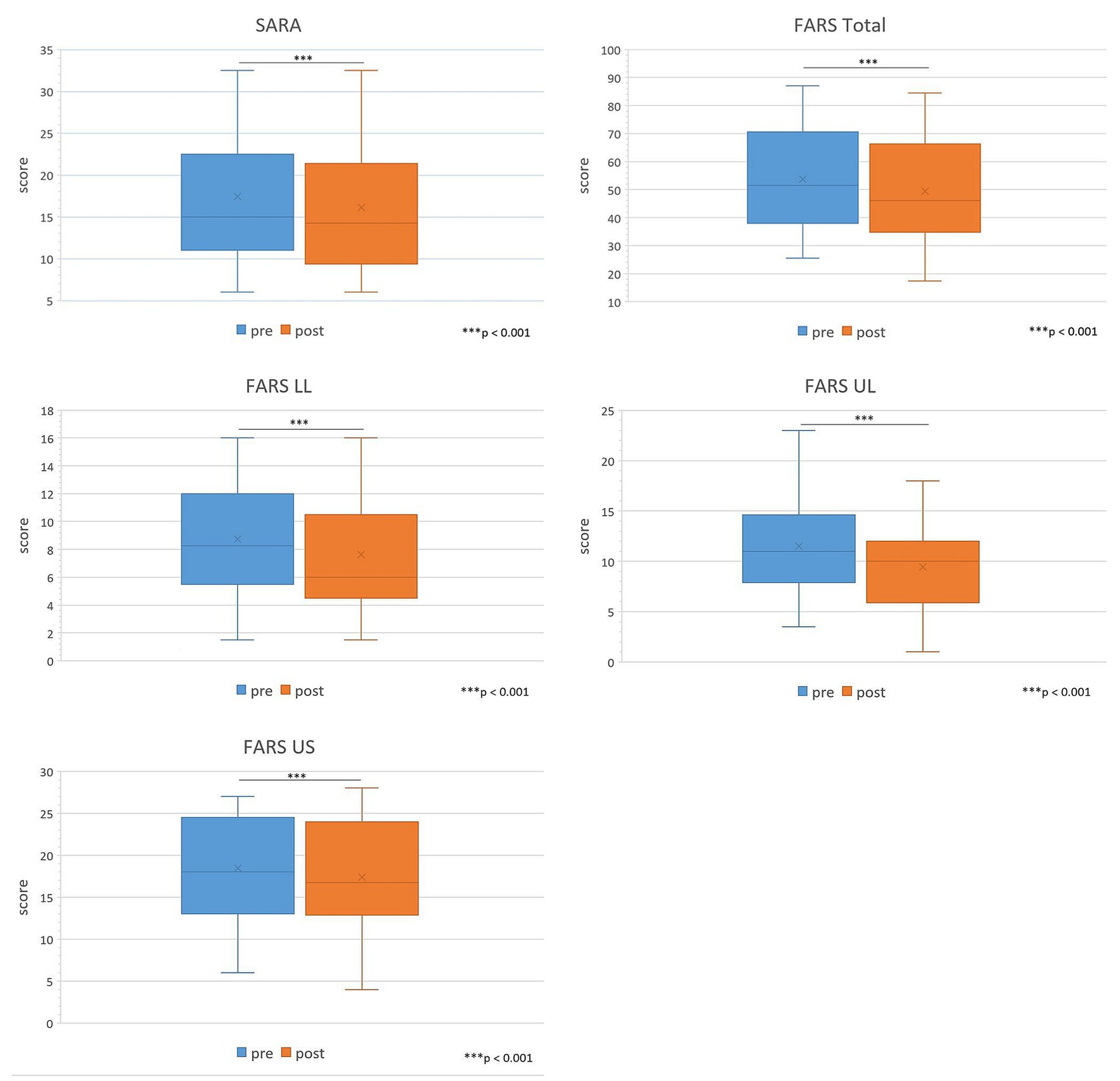
Figure 2. Comparison of SARA, FARS Total, FARS LL, FARS UL and FARS US administered to the entire cohort of patients pre vs. post IR. LL, lower limb; UL, upper limb; US, upright stability. Sig: *** <0.001.
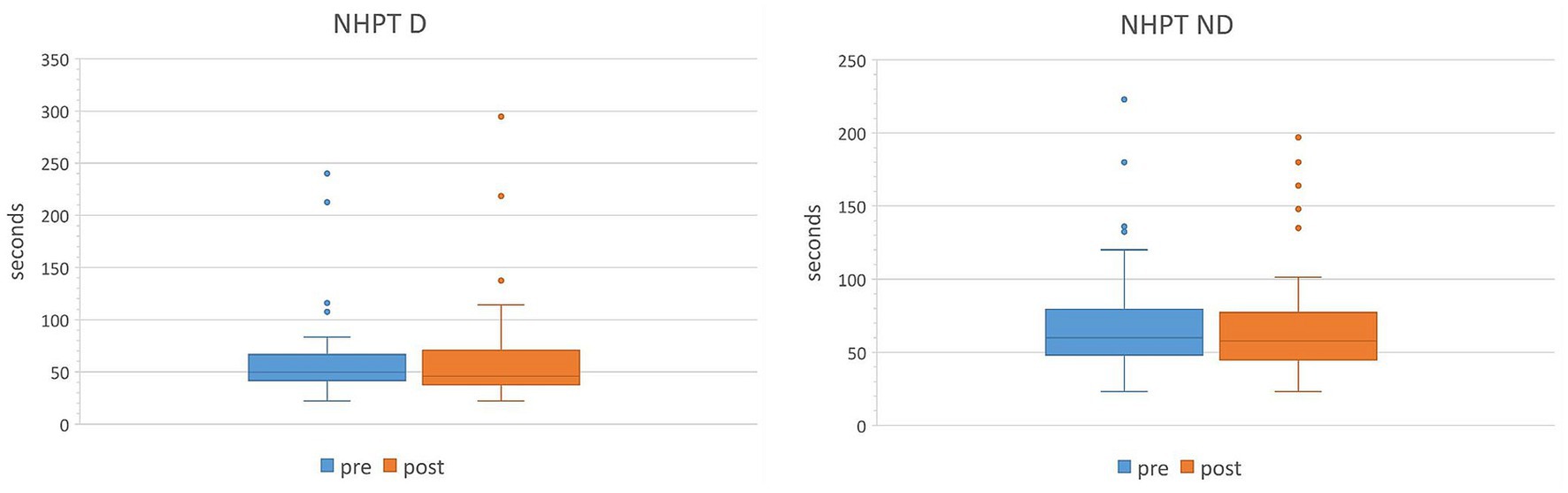
Figure 3. Comparison of NHPT in dominant and non-dominant hand administered to the entire cohort of patients pre vs. post IR. D, dominant hand; ND, non-dominant hand.
We then divided the cohort into ambulant (n = 27) and non-ambulant (n = 15) patients (Table 5). In both groups there was a significant improvement in the SARA, FARS Total and its subscales.
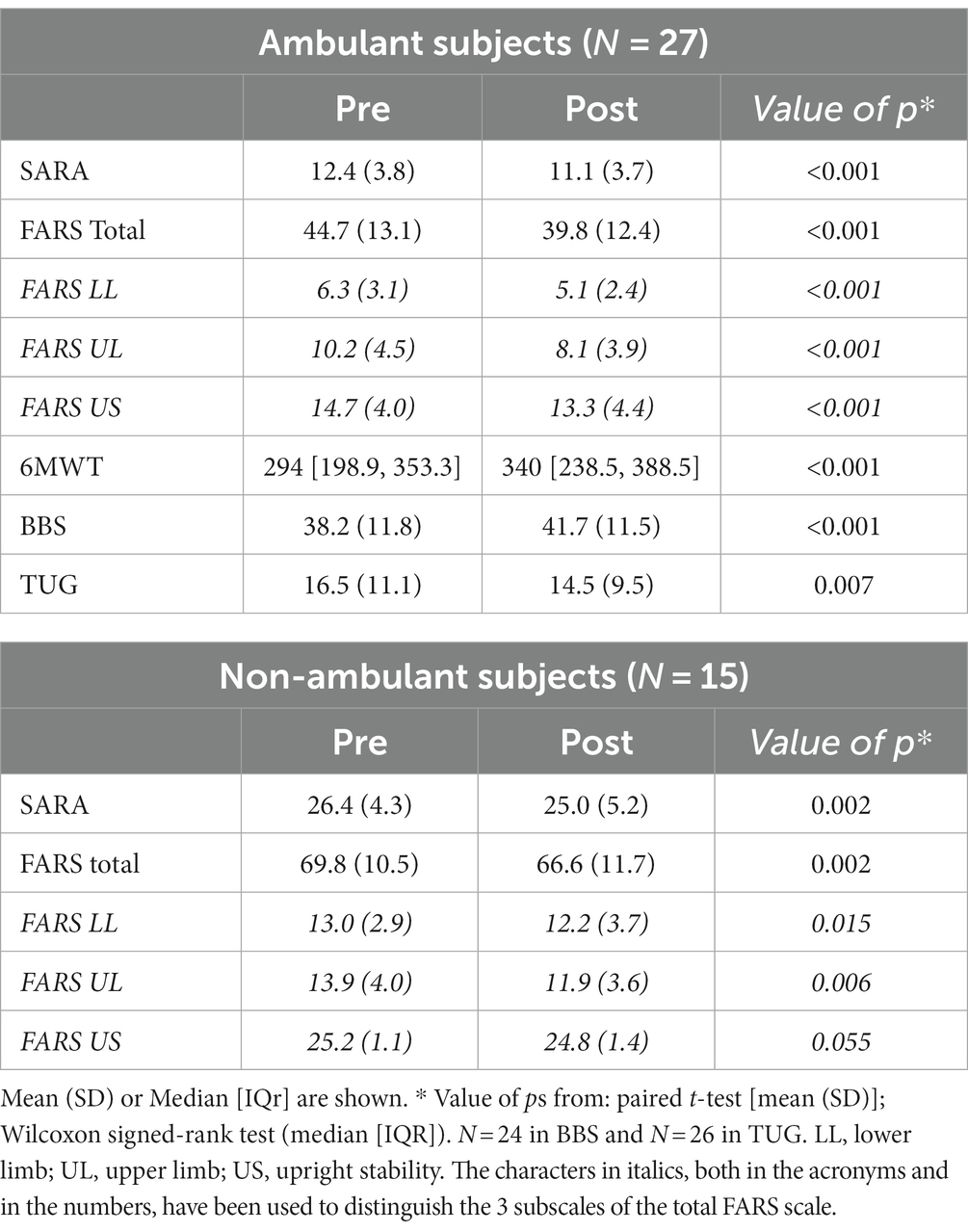
Table 5. Comparison of the scales pre vs. post IR in ambulant and non-ambulant subjects.
We then compared the extent of improvement between the two groups: ambulant vs. non-ambulant (Supplementary Table S1). No significant differences emerged, except for FARS US (average reduction of 1.4 in ambulant vs. 0.3 in non-ambulant subjects, p = 0.008, independent t-test).
Regarding the assessments performed only on ambulant patients (see Figure 4), in the 6MWT there was a significant variation in terms of increase in meters walked after IR (average increase of 24.5 meters, p < 0.001), in the BBS a significant increase in the score (from 38.2 to 41.7, p < 0.001) and in the TUG a significant decrease in time spent to perform the task (average reduction of 2 s, p = 0.007).
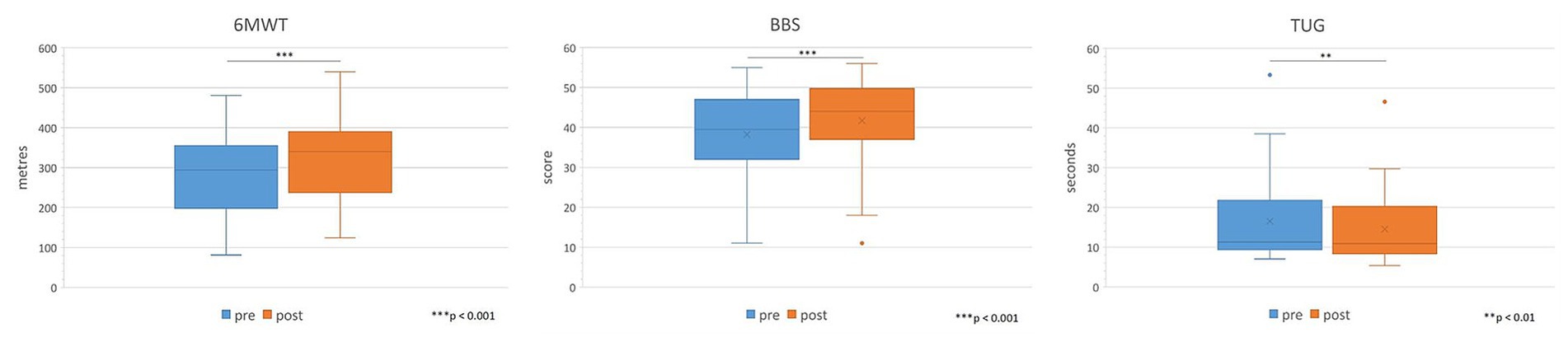
Figure 4. Comparison of 6MWT, BBS, and TUG administered only to ambulant patients pre vs. post IR. Sig: *** <0.001, ** <0.01.
The total cohort was then divided into adults (n = 29) and children (n = 13). In both groups taken separately the results already seen above were confirmed (Table 6). Regarding NHPT, in both groups there was a reduction in the task execution time but not statistically significant in either the dominant hand or the non-dominant hand.
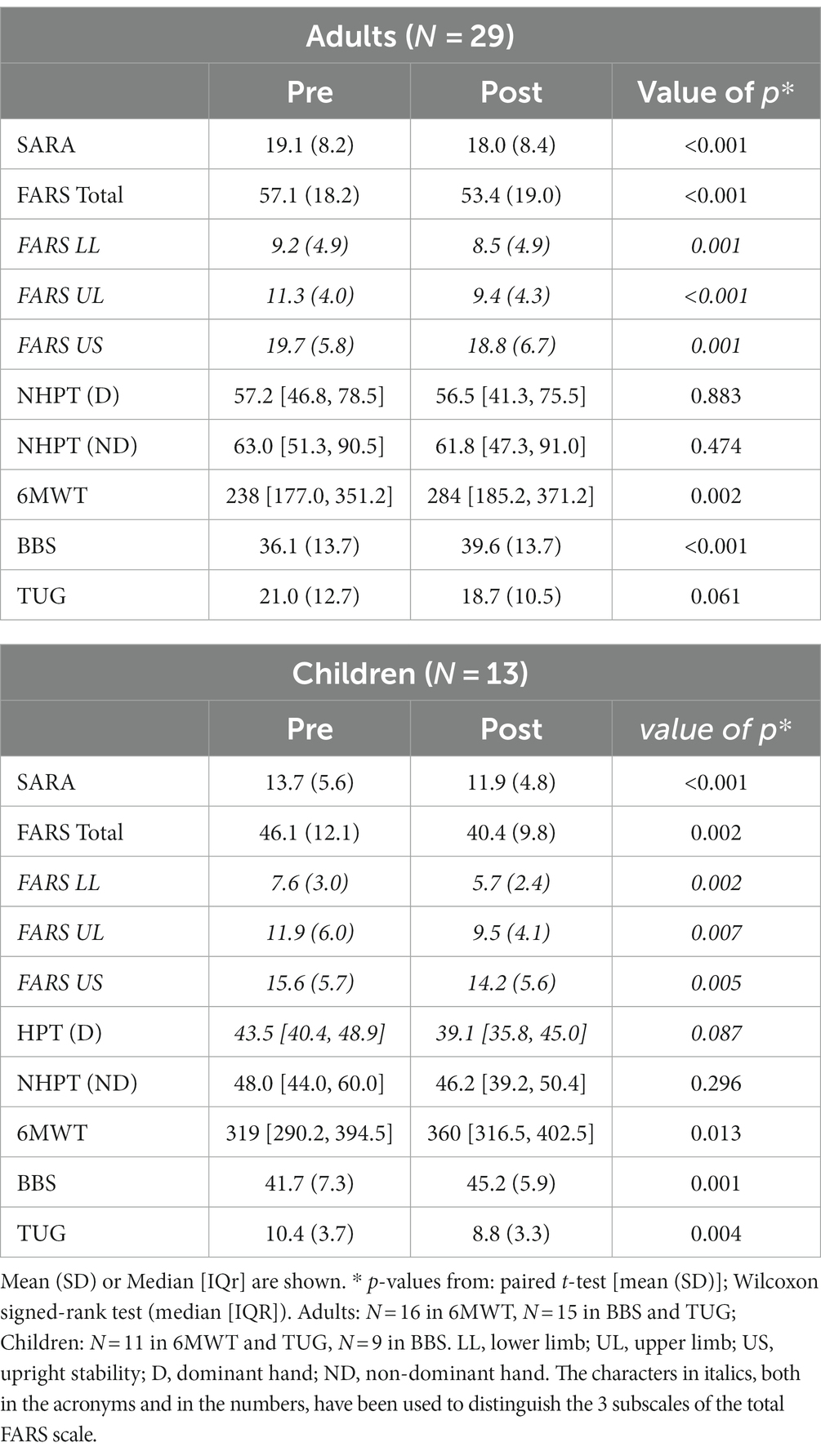
Table 6. Comparison of the scales pre vs. post IR in adults and children.
The comparison between the two groups (adults vs. children) in terms of extent of improvement (Supplementary Table S2) showed no statistically significant difference, except for FARS LL (average reduction of 0.7 in adults vs. 1.9 in children, p = 0.012, independent t-test).
We also assessed the correlation between the extent of improvement and the number of GAA1 triplets repeats and disease duration, respectively. This analysis was performed by considering the whole population and for individual subpopulations of adult/children, ambulant/non-ambulant. No significant results were found.
The aim of this study was to evaluate the efficacy of neurorehabilitation intended as IR in FRDA, in patients with different age range and disease severity, by using standardized ataxia outcome measures. The second aim was to validate an IR protocol tailored to the specific needs and functional disabilities in FRDA, that takes into account not only functions but also the domains of activity and participation as defined by the ICF.
The size of our participants’ sample, albeit not large, is still comparatively one of the most numerous in the literature on FRDA cohorts, since most studies involved small cohorts of non-homogeneous ataxias.
Although there are clinical outcomes validated for FRDA, such as FARS, mFARS and SARA (35), in the literature there is a heterogeneity of indicators, with consequent difficulty in comparing the results of the various studies.
This study is the first to involve a cohort of individuals with FRDA of a wide range of ages and severity, applying a unique assessment protocol. This made it possible to compare the effectiveness of the rehabilitation process between groups of different ages (children and adults) and of different severity (ambulant and non-ambulant subjects).
We show that an inpatient intensive rehabilitation significantly improves motor performance and ataxia symptoms in people with FRDA. Our study shows significant functional improvement in all the outcome measures used, except NHPT bilaterally, even if there was an average reduction of the task execution time. In children, however, the reduction is more marked than in adults, but it must be considered that there is a great variability and a low number of subjects.
The results show a significant reduction in ataxia symptoms measured with the SARA scale. These results are in agreement with several previous studies which have used the same outcome measure to assess efficacy of rehabilitation (14, 15, 17, 18). In our study we had an average improvement of 1.3 points on the SARA scale. This improvement is significant, given that 1 SARA point would be the expected disease progression in 1 year (36). When considered separately, the disease progression is twice as faster in ambulatory FRDA patients compared to non-ambulatory ones (37) and progresses more in early onset patients compared to typical or late onset (35). If these data of natural history are projected on our results that show comparable improvement in all cohorts irrespective of ambulatory status or age of onset, the difference in observed versus expected outcome would highlight a much greater impact of IR on ambulatory and early onset subjects. This observation is not unexpected, since the functioning reserves should be comparably greater in these patients.
In the works of Ilg et al. (14) and Schatton et al. (17) there was reported a variation of the SARA score of 2.5 and 5.2, respectively. However, their cohorts involved patients with different cerebellar ataxia, including FRDA patients. As the same authors underline, patients with afferent ataxia, such as FRDA, show minor improvements compared to subjects with cerebellar ataxia.
In our work we recorded an improvement in UL coordination, with a reduction in the NHPT task execution time but the change was not statistically significant in either the dominant hand or the non-dominant hand. Leonardi et al. (18) has reported a NHPT improvement in the dominant hand in their cohort. Nevertheless, Leonardi’s work has involved a small number of adult ambulant patients with ataxias of various origins and a short disease duration when compared to our cohort.
Disease progression in subjects with FRDA is measures using rating scales, such as SARA and FARS. They represent a valid tool for monitoring the progress of the disease although they depend greatly on axial functions, balance and gait (35% in SARA and 34% mFARS). This varies the sensitivity of the scales to the progression of symptoms in different disease phases. In the ambulatory phase, the worsening is correlated primarily with the mFARS US score and then with the items relating to the LL score (35). The study by Reetz et al. (37) shows that, after the loss of walking, the SARA items relating to the functions of the trunk and lower limbs are affected by the ceiling effect with reduced ability to highlight disease progression. Our study considers ambulatory and non-ambulatory patients. With the same scales used, despite the reduced sensitivity of the SARA and FARS scales in non-ambulatory subjects, we show that subjects with advanced pathology (non-ambulant subjects) also benefit from the rehabilitation program, as already highlighted by Schatton et al. (17) and Milne et al. (19). In the work of Miyai et al. (22), there was greater improvement in mildly affected subjects and this could be due to the fact that they recruited adult ambulatory patients with spinocerebellar ataxia and idiopathic cerebellar ataxia. This result is not confirmed by our study. In the comparison between the two groups (ambulant and non-ambulant), a statistically significant difference was found only in FARS US in the ambulant patients. This datum is an expected result as the items concerning the FARS US reflect the ability to maintain an upright position, balance in tandem and walking. These items are not applicable in the majority of non-ambulant patients.
Although the literature does not confirm the validity of rehabilitation in children (23), our study shows that even in the early stages of the disease we can document benefits. We obtained a significant improvement in LL coordination in children but no changes in walking outcomes of a similar magnitude. Coordination of the LL is a function, while walking represents an activity. Walking is influenced by several factors. In addition to the coordination of the LL, the postural stability of the trunk, weakness and proprioception of the LL are affected. Therefore, improving coordination alone does not automatically change walking.
By comparing adults with children, we demonstrate that the improvement in FARS LL subscale is more significant in children that underwent rehabilitation versus the adults. Observing the entry SARA scores, children involved in the study presented a mild condition and only two patients were non-ambulant. The initial stage of the disease is characterized by a weakness of the muscles for the pelvic stabilization, in particular the gluteus medium and gluteus maximus which, as the disease progresses, involves a greater number of muscles of the lower limbs (38–40). Therefore, in adult patients there is greater impairment of the lower limbs both in terms of weakness, proprioception and coordination. This could explain the difference between the two groups.
In this study we demonstrated the effectiveness of intensive rehabilitation in FRDA individuals with different age range and disease severity. Nevertheless, there are still many questions to address. What is the rationale for an optimal rehabilitation in the context of a progressive neurodegenerative condition? Which is the most efficient frequency and duration of the training sessions? When is the best timing to start with physiotherapy? Which training methods and mechanisms are most useful? How should we adapt the training program to the different stages of the disease and ages at onset?
Our work has confirmed that rehabilitative training leads to improved motor performance. The lack of a control group does not allow us to draw absolute conclusions, both in terms of intensity and in terms of setting.
A multidisciplinary management including occupational therapy (22) is considered appropriate in order to integrate the rehabilitation program into daily practice. Inclusion of occupational therapy in the program was a good motivational support and resulted in improvements in selected areas of activity hardly captured by the reported scales. The experience of the direct transferability of the selected motor improvements in changes in the way tasks of the daily life are carried out results in a strong positive feedback for patients and caregivers.
Our experience shows that also psychological support is a fundamental element in the rehabilitation process. Each patient presents a cognitive-behavioral modality when facing the disease. Each individual has a specific and unique “coping style.” Psychological support represents a moment of listening and elaboration of the experience related to the disease. The psychologist helps to accept the disease and at the same time adhere to the rehabilitation program including the adoption of prescribed aids.
In our study, we expected children to respond and perform better than adults. On the contrary no difference could be demonstrated between the two groups. This could be due to a lack of motivation for intensive and continuous physiotherapy in children. Moreover, by analyzing the age of onset of subjects, most children have an early onset, while in adults the majority have a typical onset, causing a different disease progression. It is also true that the cohort of children is smaller and includes children over 8 years of age, so it does not allow us to generalize the results to the entire pediatric population and does not allow us to draw solid conclusions.
On the assumption that there is little motivation of the children to traditional rehabilitation, it is considered useful to introduce a type of training based on whole body-controlled video games (“exergames”) to maximize engagement in the proposed programs. Even though we have only anecdotical experience of such approach, we believe that this technology supported training may represent a valid alternative to the classic rehabilitation program especially for children to improve, through the playful aspect, the motivation and adherence to the protocol.
Our protocol includes a series of exercises designed to promote muscle strengthening and sensory stimulation. Patients with FRDA already present, in the initial stages, weakness of the muscles of the lower limbs, in particular of the pelvis stabilizers, and weakness of the muscles of the trunk, in particular of the abdominal ones. Proprioceptive sensory loss is an important component of FRDA. Sensory stimulation through active and passive mobilization of the foot/ankle (19) or through electrical stimulation (18) determines changes in the clinical picture.
According to Donchin et al. (41), there are different learning mechanisms based on the stage of the disease. We thus should plan a differentiated rehabilitation path between adult and children and in different disease stages.
A major limitation of this study is the absence of a control group.
Although the number of participants in the study is relevant considering that FRDA is a rare disease, the cohort was too small to be stratified according to expansion size and disease duration. This did not allow to identify biological predictors of the rehabilitation program effectiveness.
Another limitation is the lack of follow up and evaluation of the retention time and long-term effects.
Therefore, it is essential that future studies include larger cohorts of participants and a randomized controlled design. A multi-center design, albeit more difficult to manage and prone to inter-center comparability problems, could provide critical information on protocol transferability and generalizability of the results.
The findings of this study indicate that inpatient multi-disciplinary rehabilitation determines significant improvements in motor performance and ataxic symptoms in people with FRDA with different age range and disease severity.
The rehabilitation approach must not only focus on a single function but on multiple functions and also on activity and participation optimizing in the same time the contextual factors.
Further studies with more numerous cohorts and randomized controlled design would be appropriate to verify the intensity, type and duration of rehabilitation, taking into account the characteristics of individual patients in terms of disease stage and age at onset.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Ethics Committee of IRCCS E.Medea. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
GP: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. CS: Data curation, Writing – original draft, Writing – review & editing. MV: Conceptualization, Writing – review & editing. NP: Formal analysis, Writing – review & editing. VM: Investigation, Writing – review & editing. GM: Investigation, Writing – review & editing. SZ: Investigation, Writing – review & editing. MA: Investigation, Writing – review & editing. JC: Investigation, Writing – review & editing. AM: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by the Italian Ministry of Health, grant number RC 2022–23. MV received funds from the Association “Ogni Giorno per Emma.”
The help of patients’ associations in directing the patients to our institution is gratefully acknowledged. The authors would also like to thank all the participants who gave their time for this study.
NP collaborates with Revelo Datalabs Srl.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1270296/full#supplementary-material
1. Campuzano, V, Montermini, L, Moltò, MD, Pianese, L, Cossée, M, Cavalcanti, F, et al. Friedreich's ataxia: autosomal recessive disease caused by an intronic GAA triplet repeat expansion. Science. (1996) 271:1423–7. doi: 10.1126/science.271.5254.1423
2. Maring, JR, and Croarkin, E. Presentation and progression of Friedreich ataxia and implications for physical therapist examination. Phys Ther. (2007) 87:1687–96. doi: 10.2522/ptj.20060232
3. Parkinson, MH, Boesch, S, Nachbauer, W, Mariotti, C, and Giunti, P. Clinical features of Friedreich's ataxia: classical and atypical phenotypes. J Neurochem. (2013) 126:103–17. doi: 10.1111/jnc.12317
4. Schulz, JB, Boesch, S, Bürk, K, Dürr, A, Giunti, P, Mariotti, C, et al. Diagnosis and treatment of Friedreich ataxia: a European perspective. Nat Rev Neurol. (2009) 5:222–34. doi: 10.1038/nrneurol.2009.26
5. Dürr, A, Cossee, M, Agid, Y, Campuzano, V, Mignard, C, Penet, C, et al. Clinical and genetic abnormalities in patients with Friedreich's ataxia. N Engl J Med. (1996) 335:1169–75. doi: 10.1056/NEJM199610173351601
6. Schöls, L, Amoiridis, G, Przuntek, H, Frank, G, Epplen, JT, Epplen, C, et al. Revision of the phenotype according to molecular genetics. Brain. (1997) 120:2131–40. doi: 10.1093/brain/120.12.2131
7. Lynch, DR, Farmer, J, Hauser, L, Blair, IA, Wang, QQ, Mesaros, C, et al. Safety, pharmacodynamics, and potential benefit of omaveloxolone in Friedreich ataxia. Ann Clin Transl Neurol. (2018) 6:15–26. doi: 10.1002/acn3.660
8. Lynch, DR, Chin, MP, Delatycki, MB, Subramony, SH, Corti, M, Hoyle, JC, et al. Safety and efficacy of Omaveloxolone in Friedreich Ataxia (MOXIe study). Ann Neurol. (2021) 89:212–25. doi: 10.1002/ana.25934
9. Subramony, SH, and Lynch, DL. A milestone in the treatment of ataxias: approval of Omaveloxolone for Friedreich Ataxia. Cerebellum. (2023). doi: 10.1007/s12311-023-01568-8
10. Shumway-Cook, A, and Woollacott, MH. Motor control: Translating research into clinical practice. 5th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins (2016).
11. Koziol, LF, Budding, D, Andreasen, N, D'Arrigo, S, Bulgheroni, S, Imamizu, H, et al. Consensus paper: the cerebellum's role in movement and cognition. Cerebellum. (2014) 13:151–77. doi: 10.1007/s12311-013-0511-x
12. Matilla-Dueñas, A, Serrano, C, Ivánovic, Y, Alvarez, R, Latorre, P, and Genís, D. Novel therapeutic challenges in cerebellar diseases In: M Manto, JD Schmahmann, F Rossi, DL Gruol, and N Koibuchi, editors. Handbook of the cerebellum and cerebellar disorders. Dordrecht: Springer (2013). 2370–94.
13. Marsden, J, and Harris, C. Cerebellar ataxia: pathophysiology and rehabilitation. Clin Rehabil. (2011) 25:195–216. doi: 10.1177/0269215510382495
14. Ilg, W, Synofzik, M, Brötz, D, Burkard, S, Giese, MA, and Schöls, L. Intensive coordinative training improves motor performance in degenerative cerebellar disease. Neurology. (2009) 73:1823–30. doi: 10.1212/WNL.0b013e3181c33adf
15. Ilg, W, Schatton, C, Schicks, J, Giese, MA, Schöls, L, and Synofzik, M. Video game-based coordinative training improves ataxia in children with degenerative ataxia. Neurology. (2012) 79:2056–60. doi: 10.1212/WNL.0b013e3182749e67
16. Milne, SC, Campagna, EJ, Corben, LA, Delatycki, MB, Teo, K, Churchyard, AJ, et al. Retrospective study of the effects of inpatient rehabilitation on improving and maintaining functional independence in people with Friedreich ataxia. Arch Phys Med Rehabil. (2012) 93:1860–3. doi: 10.1016/j.apmr.2012.03.026
17. Schatton, C, Synofzik, M, Fleszar, Z, Giese, MA, Schöls, L, and Ilg, W. Individualized exergame training improves postural control in advanced degenerative spinocerebellar ataxia: a rater-blinded, intra-individually controlled trial. Parkinsonism Relat Disord. (2017) 39:80–4. doi: 10.1016/j.parkreldis.2017.03.016
18. Leonardi, L, Aceto, MG, Marcotulli, C, Arcuria, G, Serrao, M, Pierelli, F, et al. A wearable proprioceptive stabilizer for rehabilitation of limb and gait ataxia in hereditary cerebellar ataxias: a pilot open-labeled study. Neurol Sci. (2017) 38:459–63. doi: 10.1007/s10072-016-2800-x
19. Milne, SC, Corben, LA, Roberts, M, Murphy, A, Tai, G, Georgiou-Karistianis, N, et al. Can rehabilitation improve the health and well-being in Friedreich's ataxia: a randomized controlled trial? Clin Rehabil. (2018) 32:630–43. doi: 10.1177/0269215517736903
20. Doğan-Aslan, M, Büyükvural-Şen, S, Nakipoğlu-Yüzer, GF, and Özgirgin, N. Demographic and clinical features and rehabilitation outcomes of patients with Friedreich ataxia: a retrospective study. Turk J Phys Med Rehabil. (2018) 64:230–8. doi: 10.5606/tftrd.2018.2213
21. Milne, SC, Corben, LA, Georgiou-Karistianis, N, Delatycki, MB, and Yiu, EM. Rehabilitation for individuals with genetic degenerative Ataxia: a systematic review. Neurorehabil Neural Repair. (2017) 31:609–22. doi: 10.1177/1545968317712469
22. Miyai, I, Ito, M, Hattori, N, Mihara, M, Hatakenaka, M, Yagura, H, et al. Cerebellar ataxia rehabilitation trial in degenerative cerebellar diseases. Neurorehabil Neural Repair. (2012) 26:515–22. doi: 10.1177/1545968311425918
23. Hartley, H, Cassidy, E, Bunn, L, Kumar, R, Pizer, B, Lane, S, et al. Exercise and physical therapy interventions for children with Ataxia: a systematic review. Cerebellum. (2019) 18:951–68. doi: 10.1007/s12311-019-01063-z
24. Milne, SC, Corben, LA, Roberts, M, Szmulewicz, D, Burns, J, Grobler, AC, et al. Rehabilitation for ataxia study: protocol for a randomised controlled trial of an outpatient and supported home-based physiotherapy programme for people with hereditary cerebellar ataxia. BMJ Open. (2020) 10:e040230. doi: 10.1136/bmjopen-2020-040230
25. International Classification of Functioning. Disability and health: ICF. Geneva, Switzerland: World Health Organization (2001).
26. Haglund, L, and Henriksson, C. Concepts in occupational therapy in relation to the ICF. Occup Ther Int. (2003) 10:253–68. doi: 10.1002/oti.189
27. Lynch, DR, Farmer, JM, Tsou, AY, Perlman, S, Subramony, SH, Gomez, CM, et al. Measuring Friedreich ataxia: complementary features of examination and performance measures. Neurology. (2006) 66:1711–6. doi: 10.1212/01.wnl.0000218155.46739.90
28. Schmitz-Hübsch, T, du Montcel, ST, Baliko, L, Berciano, J, Boesch, S, Depondt, C, et al. Scale for the assessment and rating of ataxia: development of a new clinical scale. Neurology. (2006) 66:1717–20. doi: 10.1212/01.wnl.0000219042.60538.92
29. Mathiowetz, V, Weber, K, Kashman, N, and Volland, G. Adult norms for the nine hole peg test of finger dexterity. Occup Therapy J Res. (1985) 5:24–38. doi: 10.1177/153944928500500102
30. Guyatt, GH, Sullivan, MJ, Thompson, PJ, Fallen, EL, Pugsley, SO, Taylor, DW, et al. The 6-minute walk: a new measure of exercise capacity in patients with chronic heart failure. Can Med Assoc J. (1985) 132:919–23.
32. Podsiadlo, D, and Richardson, S. The timed "up & go": a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. (1991) 39:142–8. doi: 10.1111/j.1532-5415.1991.tb01616.x
33. Berg, K, Wood-Dauphinee, S, and Williams, JI. The balance scale: reliability assessment with elderly residents and patients with an acute stroke. Scand J Rehabil Med. (1995) 27:27–36.
34. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2022).
35. Rummey, C, Corben, LA, Delatycki, M, Wilmot, G, Subramony, SH, Corti, M, et al. Natural history of Friedreich's Ataxia: heterogeneity of neurological progression and consequences for clinical trial design. Neurology. (2022) 99:e1499–510. doi: 10.1212/WNL.0000000000200913
36. Marelli, C, Figoni, J, Charles, P, Anheim, M, Tchikviladze, M, Vincitorio, CM, et al. Annual change in Friedreich's ataxia evaluated by the scale for the assessment and rating of Ataxia (SARA) is independent of disease severity. Mov Disord. (2012) 27:135–9. doi: 10.1002/mds.23879
37. Reetz, K, Dogan, I, Hilgers, RD, Giunti, P, Parkinson, MH, Mariotti, C, et al. EFACTS study group. Progression characteristics of the European Friedreich's Ataxia consortium for translational studies (EFACTS): a 4-year cohort study. Lancet Neurol. (2021) 20:362–72. doi: 10.1016/S1474-4422(21)00027-2
38. Beauchamp, M, Labelle, H, Duhaime, M, and Joncas, J. Natural history of muscle weakness in Friedreich's Ataxia and its relation to loss of ambulation. Clin Orthop Relat Res. (1995) 311:270–5.
39. Sival, DA, Pouwels, ME, Van Brederode, A, Maurits, NM, Verschuuren-Bemelmans, CC, Brunt, ER, et al. In children with Friedreich ataxia, muscle and ataxia parameters are associated. Dev Med Child Neurol. (2011) 53:529–34. doi: 10.1111/j.1469-8749.2011.03931.x
40. Corben, LA, Collins, V, Milne, S, Farmer, J, Musheno, A, Lynch, D, et al. Clinical management guidelines writing group. Clinical management guidelines for Friedreich ataxia: best practice in rare diseases. Orphanet J Rare Dis. (2022) 17:415. doi: 10.1186/s13023-022-02568-3
Keywords: Friedreich ataxia, inpatients, rehabilitation, treatment outcome, children, adults
Citation: Paparella G, Stragà C, Vavla M, Pesenti N, Merotto V, Martorel GA, Zalunardo S, Armellin M, Comiotto J and Martinuzzi A (2023) Effectiveness of rehabilitation intervention in persons with Friedreich ataxia. Front. Neurol. 14:1270296. doi: 10.3389/fneur.2023.1270296
Edited by:
Kevin J. O’Donovan, United States Military Academy, United StatesReviewed by:
Louise A. Corben, Royal Children's Hospital, AustraliaCopyright © 2023 Paparella, Stragà, Vavla, Pesenti, Merotto, Martorel, Zalunardo, Armellin, Comiotto and Martinuzzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gabriella Paparella, Z2FicmllbGxhLnBhcGFyZWxsYUBsYW5vc3RyYWZhbWlnbGlhLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.