
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol., 15 September 2023
Sec. Neurorehabilitation
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1234205
This article is part of the Research TopicReviews in NeurorehabilitationView all 17 articles
 Teresa Paolucci1
Teresa Paolucci1 Francesco Agostini2
Francesco Agostini2 Elena Mussomeli2
Elena Mussomeli2 Sara Cazzolla2Marco Conti2
Sara Cazzolla2Marco Conti2 Francescapia Sarno1
Francescapia Sarno1 Andrea Bernetti2
Andrea Bernetti2 Marco Paoloni2
Marco Paoloni2 Massimiliano Mangone2*
Massimiliano Mangone2*Background: Stroke is a main cause of disability worldwide and its neuro-rehabilitative management is not limited to the acute phase but requires continuity in the rehabilitation approach especially in the chronic phase. The aim of this scoping review was to highlight the different treatment opportunities available in neurorehabilitation, effective for patients with chronic stroke sequelae, not only in terms of maintaining motor function but also improving it.
Methods: The literature search was conducted using the following databases: MEDLINE (PubMed), PEDro, Scopus, Web of Science (WOS), Cochrane from 2012 to February 2023. We selected Randomized Clinical Trials in English dealing with neurorehabilitation strategies in chronic hemiplegic patients after stroke focusing on motor function, muscular strength, gait, postural balance, spasticity, and quality of life.
Results: According to the inclusion criteria, 47 articles were selected for our review. All of them were analyzed following the primary outcome and the rehabilitation technique used. Despite the different protocols used within the same technique and despite the chronicity of the disease, all studies report an improvement after the rehabilitation treatment of motor function and quality of life.
Conclusion: The literature analyzed invites us to reflect respect to neurorehabilitation approach to the patient with chronic stroke sequelae often considered to have as its objective the maintenance of the present motor function and contain disability: instead, the review reports how, even in chronicity, the patient always reports margins of statistically and clinically significant improvement. The chronic stroke rehabilitation over 6 months has been proved effective in obtaining recovery in different settings.
Stroke is one of the leading causes of death worldwide (1, 2) and it often leads to severe neurologically based disability in adults (3). Its consequences can affect cognitive, psychological, social and physical integrity: the assessment should consider the patient comprehensively in order to allow the best possible return to everyday life. Motor impairment is the most frequently recorded disability after a stroke episode (4), for this reason patient’s rehabilitation is essential to achieve a good recovery (5). In agreement with the literature, chronic stroke phase begins 6 months after the acute event: it is considered that the best recovery plateau is reached at this point, in fact there is much evidence in favor of the improvements achieved in the acute and subacute phases. It is estimated that 80% of stroke patients achieve their maximum recovery within the first 3 months, reaching 95 and 100%, respectively, after the first semester and 1 year (6, 7). One of the causes might be the tendency to give more importance to the reacquisition of walking than to the fine motor skills, for instance it is estimated that upper limb motor impairment persists in 55–75% of chronic stroke patients (8, 9). However, stroke patients often need a longer period of rehabilitation, after the first phase that is provided in a hospitalization context, whereas the patient needs to experiment and integrate the motor and cognitive skills re-acquired after the stroke in his/her social context, both family and work. As a matter of fact, an important unresolved point concerns the timing of the stroke rehabilitation: it is common practice to limit the intensive treatment to the first 3 months after the acute event and consider the subsequent rehabilitation proposals as maintaining the present functional conditions and prevent secondary complications. However, several studies offer evidence in support of a rehabilitation continuity in chronic hemiplegic patients (10–12) aimed at ensuring the achievement of further objectives in the long term, as well as maintaining the already achieved results in day hospital or rehabilitative outpatient setting. For example, it is essential to avoid the risk of falling in stroke patients, and therefore improve stability and balance (13, 14) even some time after the onset of symptoms. Neuronal plasticity plays an important role in motor recovery, as well as the equilibrium between excitatory and inhibitory signals in the brain pathways (15, 16).
Various processes such as restitution, substitution and compensation can explain how it is possible to notice some improvements in the recovery of the upper limbs even years after the acute event (17–20). Restitution means a reacquisition of the lost abilities; substitution refers to the replacement of the motor paths while motor compensation requires the adaptation of other motor elements (21). As an actual fact, international guidelines recommend a rehabilitation program continuation after discharge from the post-acute care center (22–24), lasting at least a few weeks up to months as required by residual impairment.
Different neurorehabilitation techniques are followed in chronic post-stroke patient, such as traditional physiotherapy, mirror therapy, Neuromuscular Electrical Stimulation (NMES), orthoses and robotic, virtual reality (VR). From the literature, it is often clear how neuro-rehabilitative exercise is often associated with innovative techniques such as VR or robotic training for gait recovery and it is not possible to indicate which technique or protocol is better than the other: there is a great heterogeneity in the protocols and setting (outpatient, at home, remotely in tele-rehabilitation).
At present time, an ideal neurorehabilitation approach among all the various therapy possibilities has not been established. The clinical and research question should be: “What is the best neuro-rehabilitative approach for patient with chronic stroke?” evaluating the resources of the social and family context too (presence or not of the care giver, accessibility to care).
Considering these premises, the following review lends itself to identify Randomized Controlled Trials (RCT) suggesting the possibility of achieving goals in rehabilitative interventions starting 6 months or more after the acute event, particularly regarding residual motor deficits.
Because the neuro-rehabilitative approach beyond the acute stroke event may not only have as its objective the maintenance of the motor function but the improvement of the function in social life.
The aim of this scoping review was to highlight the different treatment opportunities available in neurorehabilitation, effective for patients with chronic stroke sequelae, not only in terms of maintaining motor function but also improving it.
The Preferred Reporting Items for Systematic Reviews extension for Scoping Reviews (PRISMAScR) checklist was followed for writing this scoping review (25, 26).
All randomized controlled trials published from 2012 to January 2023 written in English and specifically dealing with the topic of “rehabilitation strategies in chronic hemiplegic patient after stroke” were considered as eligible if they reflected the following PCC framework: (i) Population: males and females with diagnosis of chronic stroke (≥ 6 months), age > 18 years old. (ii) Concept: rehabilitative techniques specifically addressed to treat motor impairment in chronic stroke patients according to International Guidelines (23). (iii) Context: sequelae, such as motor function, muscular strength, gait, postural balance, spasticity and quality of life, secondary to a chronic stroke.
We excluded pilot studies, studies without full-text available, without specified acute post-event period (6 months), with a PEDRO score under 5, (27) involving less than or equal to 10 patients, non-inferiority studies and studies which were not focused on the outcomes measures we meant to analyze.
A literature search was conducted (December 2022–January 2023) using the following databases: MEDLINE (PubMed), PEDro, Scopus, Web of Science (WOS), Cochrane. Keywords used were “chronic stroke AND rehabilitation, chronic stroke AND physiotherapy, chronic stroke AND recovery, chronic stroke AND exercise.” Searches were supplemented by hand searching of additional articles meeting eligibility criteria that were cited in reference lists.
All articles identified in the research were imported into Microsoft Excel. Two independent reviewers searched databases by using the same method to guarantee suitable cross-checking of the results. The authors evaluated the studies collected by the searches based on the inclusion and exclusion criteria established and selected them according with eligibility criteria. The authors independently checked the titles, abstracts, and full text of suitable studies.
Data extracted from selected studies were: Authors and date of study, type of interventions, outcomes, population, who delivered the intervention; study design and authors conclusions. All data required to answer the study questions were published in the articles. Any disagreements regarding the data collection were solved by discussion until consensus.
As shown in the study flow chart (Figure 1) the literature search identified 883 records. After removing duplicates, the research resulted in 478 records. A total of 99 records were screened based on their titles and abstracts. Then 39 were discarded following application of the inclusion and exclusion criteria. Finally, 47 were considered relevant for qualitative analysis.
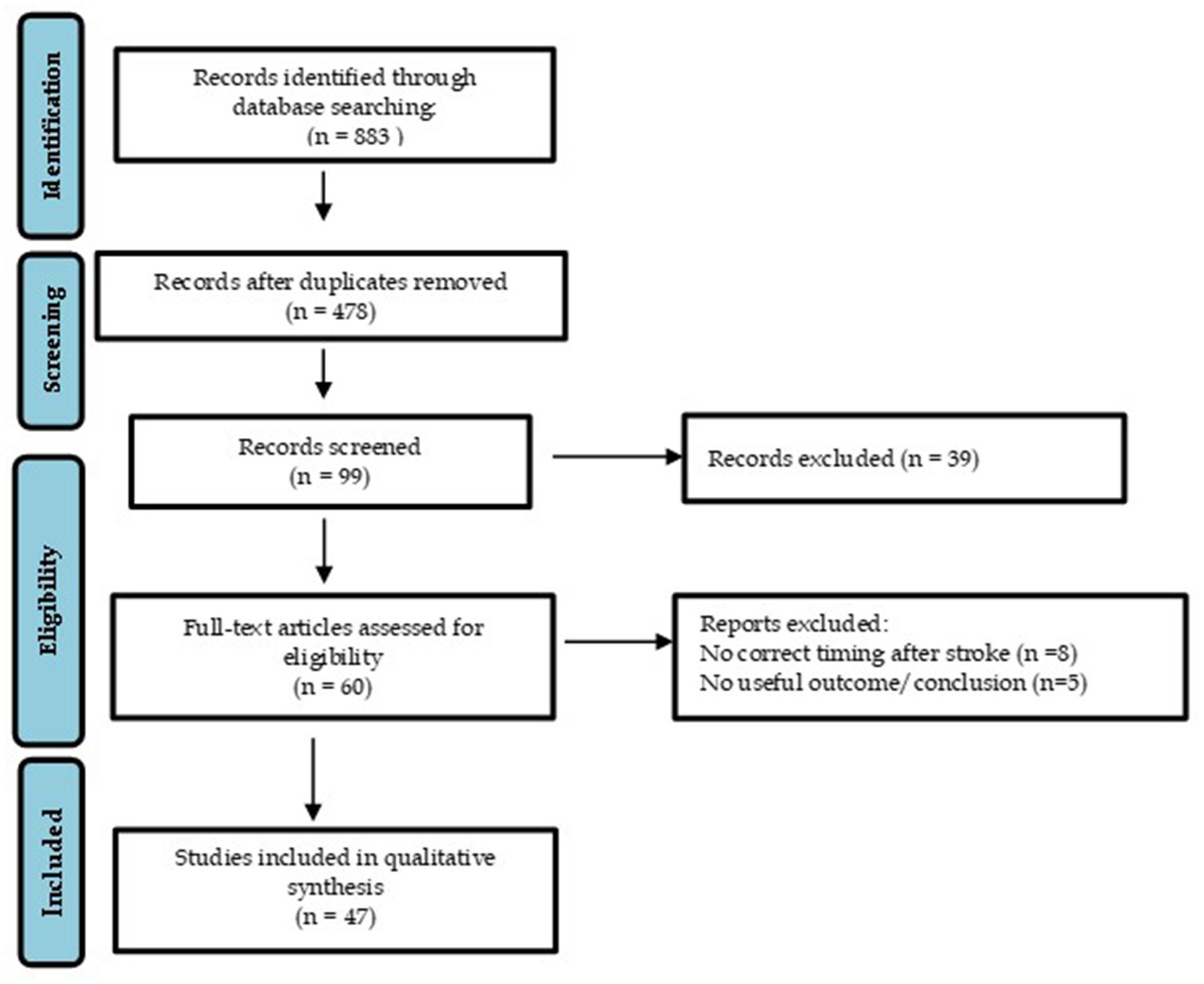
Figure 1. Flow chart.
Characteristics of included studies are summarized in Table 1.

Table 1. General characteristics of included studies.
The included studies were heterogeneous because they have treated different rehabilitative techniques. Following our inclusion criteria, in our research we focused on various domains such as function, balance, walking abilities, spasticity and quality of life. Later we decided to analyze these RCTs dividing them in three different groups based on the principal aim: lower limb, upper limb and other outcomes; then we settled the studies in subgroups by the used rehabilitative technique. The mean and standard deviation values of the studies Pedro Score were, respectively, 6.68 and 1.04.
In Calabrò et al. work, the protocol with Ekso, an exoskeleton, showed a significant improvement at 10 Meter Walking Test (10MWT), Cortico-Spinal Excitability (CSE) and Sensory-Motor Integration (SMI) in the affected side, overall gait quality, hip and knee muscle activation and Frontoparietal Effective Connectivity (FPEC) (28). Similar results in walking speed were seen in Kooncumchoo et al. study where they compared an innovative end effector robot (I-Walk) to overground gait training (29). Instead, Wu et al. analyzed if there were differences between a robotic resistance training and a robotic assistance training. The results were similar except for better improvements in 6 Meter Walking Test (6MWT) and Berg Balance Scale (BBS) in the assistance training (30).
Lee et al. investigated how afferent electrical stimulation associated with mirror therapy could modify various outcomes in chronic stroke patients’ life. After 4 weeks, important differences were found in Berg Balance Scale (BBS), gait velocity, step length and stride length (31). In Arya et al. work, an activity-based mirror therapy was compared to a conventional one; after 3 months of intervention, there were statistically significant improvements in Fugl Meyer Lower Extremity (FMA-LE), Rivermead Visual Gait Assessment (RVGA) and Brunnstrom recovery stages (BRS-LE). No meaningful one was found at 10MWT (32). In Son et al. study, the experimental group performed a self-observation training associated with exercise therapy with significant ameliorations in muscle activity of the rectus femoris, biceps femoris, tibialis anterior and gastrocnemius and an improvement in 10MWT and Timed Up and Go (TUG) (33). The intervention group in Bang et al. paper watched a video of treadmill walking actions taken at various speeds before the training itself with significant progress in TUG, 10MWT, 6MWT and in maximal flexed knee ankle in the swing phase during walking (34).
Cho et al. investigate how motor imagery training with gait training, compared to classic gait training, could modify balance and gait abilities. After intervention there were significant improvements in FRT (Functional Reach Test), TUG (Timed Up-and-Go) and 10MWT (35). Dickstein et al. used a motor imagery technique with motor and motivational contents performed in the participants’ home with a significant amelioration concerning In-home walking (36).
In et al. investigated the effects of virtual reality reflection therapy (an enhanced version of the mirror therapy concept) on chronic stroke patients. After 4 weeks of program, there were significant improvements in the experimental group in BBS, Functional Reach Test (FRT), TUG, postural sway and 10MWT (37). In Kayabinar et al. study, virtual reality augmented robot-assisted gait training was compared to conventional robot-assisted gait training; after 4 weeks of intervention, there were ameliorations in motor task and cognitive task added to 10MWT in cognitive dual-task, although there was no statistically significant difference with the control group. FGA, RMI, BBS, and Functional Independence Measure (FIM) total scores improved in both groups but with no differences (38). In Llorens et al. study, a virtual reality-based stepping training was used in the intervention group to see any improvement in balance. After 20 sessions, there were significant changes in BBS, 10MWT and in Brunel Balance Assessment (BBA) (39).
Alwhaibi et al. evaluated the effects of somatosensory rehabilitation on neural and functional recovery of Lower Extremity. After treatment, there was a significant improvement in FIM but no significant changes were found in QEEG scores (40).
In Yang et al. study, Neuro-Muscular Electrical Stimulation (NMES) on anterior tibialis muscle or medial gastrocnemius muscle was compared to range of motion and stretching exercises in patients with inadequate ankle control. After 7 weeks of training, the NMES-TA group showed significant improvements in dynamic spasticity, spatial asymmetry, ankle plantarflexion during push off and muscle strength of ankle dorsiflexors (41). In Bethoux et al. work, the aim was to compare the effects of peroneal nerve Functional Electrical Stimulation (FES) to Ankle-Foot Orthosis (AFO). After 6 months of intervention the results were that FES stimulation is equivalent to AFO with no significant differences between groups (42). Beaulieu et al. used Repetitive Peripheral Magnetic Stimulation (RPMS) on paretic tibialis anterior muscle with a significant increase in ankle dorsiflexion mobility and maximal isometric strength and a decrease in resistance to plantar flexor stretch (43).
In Lee et al. study, a local vibration stimulus training program was applied to see the effects on postural sway and gait with significant results, after 6 weeks, in postural sway distance with eyes-open and closed, in postural sway velocity with eyes-open and closed and in gait speed, cadence, step length and single limb support time (44).
Park et al. associated a two-channel TENS, placed on the affected lower extremity on lateral and medial quadriceps muscle and gastrocnemius muscle, with an exercise program. After 6 weeks there were significant improvements in spasticity, static balance parameters, dynamic balance, gait speed and cadence, step and stride length on the paretic side (45). Lim et al. investigated the effects of a home- based rehabilitation program on postural balance, walking and quality of life with ameliorations in postural balance, comfortable speed, and fast speed walking but with no significant differences with the control group (46). Hornby et al., with their study, underlined how a high-intensity training can bring significant improvements in stepping amount and rate, with additional gains in spatiotemporal symmetry and balance confidence (47).
Globas et al. measured how high-intensity aerobic treadmill training influenced gait performances with a significant progress of peak exercise capacity and 6MWT in the intervention group, maintained also at 1-year follow up with a little decrease of walking capacities (48). In Chen I et al. work, a turning-based treadmill was compared to a normal treadmill, and after 4 weeks of training they noticed significant improvements on turning speed, straight-walking performance, strength of hip muscles and ankle dorsiflexors and balance control, maintained also at the 1-month follow up (49). In Choi et al. study, whole-body vibration was combined with treadmill training with significant changes in walking performances, gait parameters and 6MWT compared to control group (50). Cho et al. matched treadmill training with a real-world video recording; after 6 weeks there were significant improvements in dynamic balance and gait parameters (51). On the other hand, Hwang D. et al. used tilt sensor functional electrical stimulation on common peroneal nerve in treadmill training with significant ameliorations in TUG, BBS, 10MWT and anterior tibialis muscle architecture in the intervention group (52).
An et al. investigated how a talocrural mobilization with movements can influence ankle strength, dorsiflexion passive range of motion and weight-bearing ability on the paretic limb: they showed significant ameliorations compared to the control group after 5 weeks of intervention (53). In Park et al. work, the intervention group experienced a four-week training of self-ankle mobilization with movement, and it was compared to a calf muscle stretching group; significant changes were found in gait parameters and fall risk (54). On the other hand, Liao W. et al. put in evidence how lateral wedge soles and visual biofeedback balance training group can improve balance Computerized Adaptive Test (CAT) and TUG test (55).
Cho et al. used an upper limb exoskeleton machine with two different protocols: the robot-assisted as needed protocol was significantly more effective than the robot-assisted with guidance force protocol in FMA and Action Research Arm Test (ARAT) (56). Cordo et al. analyze if there are significant differences between the use of EMG biofeedback and torque biofeedback in robot-assisted movement associated with muscle vibration in severe hand impairment following stroke but the results showed no meaningful distinction between them (57). Hung et al. investigate if a hybrid approach (arm training + robot therapy) could bring changes in motor function. They divided their patients in three groups: unilateral hybrid RT, bilateral hybrid RT and robot assisted therapy. The results favored Bilateral Hybrid Therapy (BHT) over Unilateral Hybrid Therapy (UHT) on the FMA total score and distal score. RT group showed significant improvements in the mobility domain of Nottingham Extended Activities of Daily Living (NEADL) (58). Lin et al. investigated the effects of a computer-aided bilateral isometric handgrip on paretic hand and arm motor control in chronic stroke patients. After 4 weeks of interventions, there were significant improvements in the FMA-UE, BI (Barthel Index), Wolf Motor Function Test (WMFT) and Modified Ashworth Scale (MAS) (59).
In Choi et al. work, mirror therapy was associated with a Gesture Recognition device (GR group) and compared with a second group with conventional Mirror Therapy (MR group) and a third group with sham therapy (CG). There were significant changes in upper extremity function, depression, and quality of life in the GR group and improvements in neck discomfort in MR and CG group (60). Lee et al. investigated the effects of afferent electrical stimulation associated with mirror therapy in stroke patients’ life: there was an increase in muscle strength measured with a handheld dynamometer (31). In Colomer et al. study, mirror therapy was applied to chronic stroke patients with severely impaired upper limb function. After 8 weeks, the experimental group showed significant improvements in tactile sensation compared to the control group but a similar increase in FMA and ability subscales in WMFT (61). Cho et al. associated mirror therapy with transcranial Direct Current Stimulation (tDCS). This innovative technique showed significant improvements compared to control group in the Box and Block Test (BBT) and grip strength (62).
In Hernandez et al. work, a virtual reality- based rehabilitation was compared to an evidence-based home exercise program in influencing upper extremity function; no significant differences were found between groups (63).
De Diego et al. compared a sensory stimulation and functional activity training with a control group who went under a standard rehabilitation program. After 8 weeks there were significant improvements in the experimental group especially in the sensory tests (64).
Lee et al. decided to investigate the effects of combining robot-assisted therapy with neuromuscular electrical stimulation; after 4 weeks of intervention there were significant changes in wrist flexors MAS score, WFMT quality of movement and the hand function domain of Stroke Impact Scale (SIS) (65). Knutson et al. compared Contralaterally Controlled Functional Electrical Stimulation (CCFES) to cyclic NeuroMuscular Electrical Stimulation (cNMES) with a significant improvement at the BBT in the CCFES group (66).
Tavernese et al. used segmental muscle vibration over biceps brachii and flexor carpi ulnaris muscles of the paretic side with a significant improvement in the normalized jerk, an indicator of smoothness of the movement, in mean linear velocity, in mean angular velocity at shoulder, in distance to target at the end of movement and movement duration (67). On the other hand, Costantino C. et al. analyzed the short-term effect of local muscle vibration treatment on upper limb obtaining significant results, after 4 weeks, in grip muscle strength, pain and quality of life and decrease of spasticity (68).
Karthikbabu et al. compared plinth and Swiss ball-based trunk exercise regimes with a standard physiotherapy; after 6 weeks there were significant changes in Trunk Impairment Scale (TIS), BBA, Tinetti scale, gait speed, SIS and community reintegration but they were retained during the 3–12 months follow up (69). In Lee et al. work, there was a comparison of the effects of a Conventional Core Stabilization (CCS) and a Dynamic Neuromuscular Stabilization (DNS) on Anticipatory Postural Adjustment (APA), time, balance performance and fear of falls in chronic stroke patients. After the intervention the APA times changed significantly in the DNS group; the BBS, TIS and Falls Efficacy Scale (FES) scores improved in both groups but with a time stability only in the DNS group (70). Lee et al. investigated the effect on trunk control and dynamic balance ability in the sitting position of a dual motor task training program. After 6 weeks, the experimental group showed significant improvements in trunk control ability and dynamic balance in sitting position (71).
Park et al. investigated the effects of a Land-based and Aquatic Trunk Exercise program (LATE) in chronic stroke patients; after 4 weeks of intervention there were clinically significant improvements in Korean-TIS, 3-level Postural Assessment Scale for Stroke (PASS 3-L), BBS 3-Level and Modified-BI scores and Functional Reach Test (FRT) distance (72). In Perez-de la Cruz work, the program of Ai Chi aquatic therapy showed that there were significant ameliorations in post treatment pain and resilience; also, they found changes in the SF-36 test except for general health, vitality, and social functions (73). Also, Ku et al. studied the effects of Ai Chi therapy but under a different point of view, focusing on the significant changes seen in Limits of Stability (LOS) test (anteroposterior axis), BBS and FMA (74).
In this systematic review, we conducted the research including randomized controlled trials (RCT) published over the last 10 years with the purpose of identifying all the effective rehabilitation treatments and setting in chronic stroke patients. We also wondered about the possibilities of improvements and the future perspectives for both patients and research. In fact, the mechanism on which recovery can occur even more than 6 months after the acute event has not been fully clarified yet, therefore it cannot be assumed that any therapeutic option will be successful. Insights of this kind could make a significant contribution to the knowledge of this chronic neurological issue and above all to what a patient can probably expect from the course of his disease.
Several authors decided to explore the rehabilitative perspective of robotic technology, obtaining most of the results. In Calabrò et al. and Kooncumchoo et al. studies, two types of gait training machines (Ekso in the first one and I-Walk in the second one) were tested: in both studies there was a significant improvement in 10MWT/speed but only in the first one there were positive changes in gait quality. Even if the I-Walk machine did not show massive advantages compared to conventional therapy, it sufficiently facilitates locomotor function with the setting of task-specific training and an adequate number of repetitions with an appropriate gait pattern (50 step/min). In this way, the patient learns to control new movements with normal biomechanics and to use less energy when performing tasks. In contrast, the repetitions in the conventional PT group were possibly inadequate to control precise movement but the sensory stimulation by the physical therapist provided a more effective patient response and range of motion (28, 29).
Both in Wu et al. and Cho et al. studies, the robotic assistance protocol showed to be superior or not inferior to other protocols. In Wu et al. work, the resistance protocol did not overcome the assistance training protocol in improving endurance, balance, and balance confidence in individuals poststroke. A possible reason is that the motor memory and the acquired cognitive strategies, resulted from the resistance force applied to lower limbs, may be less retained and transferred to overground walking. Certainly, a force perturbation and a controlled assistance load to the paretic leg during treadmill training may be used as an adjuvant tool to improve locomotor functions in poststroke patients, even for subjects of a high functional level (30, 56).
Hung et al. decided to investigate if robot-assisted therapy could bring more improvements either if associated with unilateral or bilateral arm training. In the end. BHT was more effective for improving upper extremity motor function probably because the patients were more likely to use their affected Upper Extremity (UE) with the assistance of the unaffected UE and practiced more in dexterity tasks compared with those in the UHT group. At the same time, UHT is useful in term of enhancing UE motor abilities and physical- related Quality of Life but the results were not maintained at long term. Instead, the robot training group showed higher improvements in functional ambulation (58). On the other hand, Cordò et al. studied an existing protocol using robot-assisted movement combined with local vibration therapy; they wanted to assess if EMG biofeedback or torque biofeedback could improve the recovery of the severe hand impairment. The results were overlapping in both cases (57). Upper Limb function was also used as an outcome in Lin et al. article: the intervention group reached optimal changes in FMA, BI, WMFT and MAS by using a computer-aided bilateral isometric handgrip (59).
A hybrid approach was used by Lee et al. combining robot-assisted therapy with Neuromuscular Electrical Stimulation to implement the functions of the upper limb, in particular of the hand (65). They achieved good results as well as Yang et al. that used NMES on anterior tibialis muscle and medial gastrocnemius muscle (41). Knutson et al. demonstrated the predominant effects of CCFES on cNMES in achieving a finer hand dexterity (66). On the contrary, intervention superiority was not obtained in the study conducted by Bethoux et al. as they used FES on common peroneal nerve com-pared to Ankle Foot Orthosis (42). Beaulieu et al. showed how also RPSM is an effective tool for ameliorations in stroke patients with a paretic tibialis anterior muscle and with spastic plantar flexor muscles (43).
A great technologic resource for recovery in chronic stroke patients is the use of virtual reality of different types (immersive or exergames) in lower limb and balance function. The protocols used by the authors are different, some using Exergame with physical exercise that integrates motion-tracking technology that enables interaction with the game and real-time feedback of user’s performance or immersive VR with deep mental involvement in something action. In the context of virtual reality, and in a technical acceptance of the term, immersion is achieved by removing as many real-world sensations as possible and substituting these with the sensations corresponding to the virtual reality experience, but the patient must have good confidence with the technology and bring back an adequate cognitive reserve, that’s why an adequate MMSE is always required.
Supporting evidence can be found in Kayabinar et al. and in Llorens et al. studies where they both used Virtual Reality combined with robotic technology or with stepping training.
In Kayabinar et al. work, VR was added as support in robot-assisted gait training under the form of an exergame: the experimental group was tasked to walk in a forest environment with many trees, without hitting them and trying to collect the coins that appeared on the screen. The patients determined their direction during the game by transferring weight to their extremities on the device. The protocol lasted 6 weeks, two session/week, for a total of 12 sessions (38).
On the other hand, Llorens et al. associated immersive VR with stepping training to create a protocol of 20 one-hour rehabilitation sessions, 5 days a week for 4 weeks. The experimental group underwent 30 min of conventional therapy and 30 min of training with the virtual rehabilitation system in that order. In this group, the exercises of conventional therapy were administered consecutively in single 5-min repetitions and the training with the virtual rehabilitation system consisted of three 6-min repetitions with one and a half minute breaks between them. The exercise immersed the participants in a 3D virtual environment with their feet represented by two shoes that mimicked their movement in the real world (39).
Also, the combination of immersive VR with MT showed to be an excellent therapeutic choice as confirmed by In et al. where visual illusion was used to help the patient in the recovery of the Lower Limb Function (37).
Instead, as regards the Upper Limb Function (ULF), VR has not proved to be superior compared to home exercises programs as seen in Hernandez et al. (63).
Following the discovery of the mirror neuron system, it has been years since mirror therapy has been used as a fundamental tool for recovery in stroke patients. Therefore, in our research it is not surprising the great number of articles regarding new upgrades of this technique: for example, Arya et al. showed how an activity-based mirror therapy was more effective than the conventional one (32).
Assuming the positive effects of MT, some authors have combined it with other rehabilitation technologies such as afferent electrical stimulation (31) and TDCS (Transcranial Direct Current Stimulation). Minimum collateral effects were found in the second work: a patient dropped out the study for the appearance of a headache (62). The pairing of tDCS with MT may influence restoration of daily function and movement efficiency of the paretic hand in chronic stroke patients. Sequentially applying tDCS prior to MT seems to be advantageous for enhancing daily function and hand movement control and may be considered as a potentially useful strategy in future clinical application. Both these hybrid techniques have reported good results especially regarding muscle strength.
Choi et al. have implemented mirror therapy with a gesture recognition device obtaining significant changes in motor function but also in quality of life and depression (60). A limit of this technique was found by Colomer et al. and relates to the severity of the upper limb impairment: patients with severely impaired UE function, treated with MT, showed some improvements in tactile sensation similarly to the control group in FMA and ability subscales (61).
However, authors agree in suggesting MT even in completely plegic stroke survivors, as it uses visual stimuli for producing a desired response in the affected limb to have effects not just on motor impairments but also on sensations, visuospatial neglect, and pain after stroke. Also, MT is an easy and low-cost method.
Son et al. demonstrated how self-observation training (a specific protocol based on eliciting mirror neuron system) associated with exercise therapy can improve muscle activity of the most important muscles involved in gait (33). Also, a video of treadmill walking action taken at various speeds can be an optimal instrument for the recovery of gait functions as demonstrated by Bang et al. (34). Cho et al. used an innovative program based on motor imagery training where patients were asked to conceive motor patterns associated with gait; there were improvements in many outcomes such as gait abilities and balance (35). The same technique was used by Dickstein et al. but it was performed in a household setting with optimal results (36). Somatosensory training was treated by Alwhaibi et al. and De Diego et al. with the purpose of acquiring some latent function, as actually noticed in the results obtained in the FIM score and in the sensory tests (40, 64). In our research, a technique that obtained excel-lent achievements both in postural sway and in upper limb function was the local vibration stimulus training program (44, 68).
More in detail, Tavernese et al. demonstrated how the segmental muscle vibration can improve, at least in a short-term period, upper limb motor performances of reaching movement (67).
Physical exercise is the basis of rehabilitation treatment after a stroke episode, we therefore tried to define what features it should have to be effective in the chronic stroke patient. For example, high-intensity exercise appears to be effective in gaining gait abilities (stepping amount and rate) and spatiotemporal symmetry as showed by Hornby et al. (47). Its positive influence can also be enhanced by the combination with TENS, placed on the affected lower extremity, as seen in Park et al. work with a reduction of spasticity and an improvement in balance and gait (45).
As a matter of fact, lack of trunk control is usually a critical problem in chronic stroke patient, for this reason plenty of studies are introducing specific new protocols about it.
Karthikbabu et al. tried to demonstrate the efficacy of a plinth and Swiss ball-based trunk exercise regime, but the initial good results were not maintained over the time (12 months follow up) (69). Instead, in the research of Lee et al. the beneficial effects reached with a dual motor task training program were sustained (71). Lee et al. decided to focus on anticipatory postural adjustments (APA) with two different strategies. The one with better results was dynamic neuromuscular stabilization (DNS) with achievements maintained over the time (70). Treadmill Training is another classic fundamental tool that can be used in chronic stroke patient for recovery in gait performance and balance skills as seen in Globas et al. paper where patients improved their walking capacities after a treadmill training (48). In our research we found four studies that tried to ameliorate this technique. Chen I. et al. demonstrated that turning-based treadmill is more effective than the normal one in walking performance (49). This outcome was also studied and improved in Choi et al. work and in Cho et al. work where the treadmill training was associated with a whole-body vibration in the first one and with real-world video recording in the second one (50, 51). Treadmill training was also matched with tilt sensor functional electrical stimulation on common peroneal nerve demonstrating to be a valid instrument in balance, gait and muscle architecture (42).
Aquatic programs in chronic stroke patients seem to be well accepted and performed, presuming an adequate cardiovascular and cognitive condition. Park et al. supplemented a land-based trunk exercise program with an aquatic one in patients with significant improvements in balance, independence, and quality of life (72).
A well specified protocol is Ai Chi which consists of Tai Chi principles applied in water. This form of aquatic exercise involves a total of 19 standardized movement patterns that focus on coordination of body movements with breathing and specific patterns. This practice is safe, standardized, does not require specific equipment, it can be taught in a group setting and allows participants to continue their own. It has been proven to be a valid therapeutic option in improving balance, motor function and in reducing post treatment pain (73, 74).
In our research we found out that other different approaches have been applied to these patients, such as different types of mobilizations (talocrural and self-ankle) as used in An et al. and Park et al. works, which demonstrated how balance and gait parameters can be restored by using them (52, 53).
Instead, Liao et al. established how both lateral wedge soles and visual biofeedback balance training can reinforce balance abilities (55).
Some of the selected studies have shown that chronic stroke patients’ rehabilitation can also be performed in a home environment, with or without the presence of the physical therapist, taking for granted an adequate cognitive condition and ability to understand the instructions: in this way the management of the patient after discharging gets simpler (36, 46, 54, 63, 64).
Moreover, a home-based setting allows greater patient compliance. Home rehabilitation makes it possible to contain the high costs of inpatient rehabilitation programs and improve the continuity of care while patients are transferred to home. Moreover, the possibility of treatment at home allows to reduce the economic costs and makes life easier for the patient and the caregiver and is a valid tool during periods of pandemic such as covid.
After discharge from in-hospital rehabilitation, chronic post-stroke patients should have the opportunity to continue the rehabilitation through structured programs to maintain the benefits acquired during intensive rehabilitation treatment.
The present study represents an overview, through scoping review, of the main rehabilitation techniques commonly used in patients with disabilities secondary to chronic stroke. No comparisons were made between the different neurorehabilitation techniques or the waiting list or with placebo. This comparison will be the subject of future studies.
Our study provides an overview of the main rehabilitation techniques used in patients with chronic stroke sequelae with different levels of efficacy. For a long time, it was believed that the window of opportunity within which to provide stroke rehabilitation was limited to the first 3–6 months after the acute event. As a result, too often, rehabilitation resources for managing chronic stroke have not been adequate. But when does one reach a phase of stabilized outcomes and is it therefore correct to speak of chronicity? Although the definition of acute phase and chronic phase in terms of recovery is still debated, there are different evidence in support of a rehabilitation continuity in the chronic hemiplegic patient aimed at guaranteeing further results also in the long term. Considering these considerations, our data suggest that a prosecution of the rehabilitation is possible even after the first 6 months, not only as a maintenance treatment but also aimed to acquire or recover some loss functions. Furthermore, we have noticed how a rehabilitation protocol can be ap-plied in an outpatient setting but also at home, and this could increase patient compliance including caregiver support. The reading of this evidence is intricate by methodological factors such as the variety of used scales and outcomes, follow up timing, range and characteristics of the population studied. Nonetheless other studies are needed to establish shared neuro- rehabilitative protocols with respect to the different characteristics of the patients in the chronic post-stroke phase.
TP, EM, SC, and FS: conceptualization. TP, EM, and SC: methodology. EM and SC: investigation and formal analysis. EM, SC, and MM: data curation. TP, FS, EM, and SC: writing—original draft and preparation. TP, EM, SC, MC, MM, and MP: writing—review and editing. TP, MM, MP, FA, and AB: visualization. TP, MM, and MP: supervision. All authors read and approved the final version of the Manuscript.
The authors thank Pierluigi Zoccolotti, Department of Psychology, Sapienza University of Rome (Italy) for the suggestions and indications in the interpretation of the results and their discussion.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Winstein, CJ, Stein, J, Arena, R, Bates, B, Cherney, LR, Cramer, SC, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2016) 47:e98–e169. doi: 10.1161/STR.0000000000000098
2. Feigin, VL, Brainin, M, Norrving, B, Martins, S, Sacco, RL, Hacke, W, et al. World stroke organization (WSO): global stroke fact sheet 2022. Int J Stroke. (2022) 17:18–29. doi: 10.1177/17474930211065917
3. Thrift, AG, Thayabaranathan, T, Howard, G, Howard, VJ, Rothwell, PM, Feigin, VL, et al. Global stroke statistics. Int J Stroke. (2017) 12:13–32. doi: 10.1177/1747493016676285
4. Langhorne, P, Coupar, F, and Pollock, A. Motor recovery after stroke: a systematic review. Lancet Neurol. (2009) 8:741–54. doi: 10.1016/S1474-4422(09)70150-4
5. Gittler, M, and Davis, AM. Guidelines for adult stroke rehabilitation and recovery. JAMA. (2018) 319:820–1. doi: 10.1001/jama.2017.22036
6. Yagura, H, Miyai, I, Seike, Y, Suzuki, T, and Yanagihara, T. Benefit of inpatient multidisciplinary rehabilitation up to 1 year after stroke. Arch Phys Med Rehabil. (2003) 84:1687–91. doi: 10.1053/S0003-9993(03)00286-7
7. Miyai, I, Suzuki, T, Kii, K, Kang, J, and Kajiura, I. Functional outcome of multidisciplinary rehabilitation in chronic stroke. Neurorehabil Neural Repair. (1998) 12:95–9.
8. Coscia, M, Wessel, MJ, Chaudary, U, Millán, J, Micera, S, Guggisberg, A, et al. Neurotechnology-aided interventions for upper limb motor rehabilitation in severe chronic stroke. Brain. (2019) 142:2182–97. doi: 10.1093/brain/awz181
9. Lawrence, ES, Coshall, C, Dundas, R, Stewart, J, Rudd, AG, Howard, R, et al. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke. (2001) 32:1279–84. doi: 10.1161/01.STR.32.6.1279
10. Page, SJ, Gater, DR, and Bach-Y-Rita, P. Reconsidering the motor recovery plateau in stroke rehabilitation. Arch Phys Med Rehabil. (2004) 85:1377–81. doi: 10.1016/j.apmr.2003.12.031
11. Smith, G V, Silver, KHC, Goldberg, AP, and Macko, RF. Task-oriented exercise improves hamstring strength and spastic reflexes in chronic stroke patients. (1999). Available at: http://www.strokeaha.org
12. Whitall, J, Waller, SMC, Silver, KHC, and Macko, RF. Repetitive bilateral arm training with rhythmic auditory cueing improves motor function in chronic hemiparetic stroke. Stroke. (2000) 31:2390–5. doi: 10.1161/01.STR.31.10.2390
13. Cakar, E, Durmus, O, Tekin, L, Dincer, U, and Kiralp, MZ. The ankle-foot orthosis improves balance and reduces fall risk of chronic spastic hemiparetic patients. Eur J Phys Rehabil Med. (2010) 46:363–8.
14. Januário, F, Campos, I, and Amaral, C. Rehabilitation of postural stability in ataxic/hemiplegic patients after stroke. Disabil Rehabil. (2010) 32:1775–9. doi: 10.3109/09638281003734433
15. Michielsen, ME, Selles, RW, Van Der Geest, JN, Eckhardt, M, Yavuzer, G, Stam, HJ, et al. Motor recovery and cortical reorganization after mirror therapy in chronic stroke patients: a phase II randomized controlled trial. Neurorehabil Neural Repair. (2011) 25:223–33. doi: 10.1177/1545968310385127
16. Ehrensberger, M, Simpson, D, Broderick, P, Blake, C, Horgan, F, Hickey, P, et al. Unilateral strength training and Mirror therapy in patients with chronic stroke: a pilot randomized trial. Am J Phys Med Rehabil. (2019) 98:657–65. doi: 10.1097/PHM.0000000000001162
17. Pollock, A, Farmer, SE, Brady, MC, Langhorne, P, Mead, GE, Mehrholz, J, et al. Interventions for improving upper limb function after stroke. Cochrane Database Syst Rev. (2014) 2014:CD010820. doi: 10.1002/14651858.CD010820.pub2
18. Pekna, M, Pekny, M, and Nilsson, M. Modulation of neural plasticity as a basis for stroke rehabilitation. Stroke. (2012) 43:2819–28. doi: 10.1161/STROKEAHA.112.654228
19. Bonita, R, and Beaglehole, R. Recovery of motor function after stroke. Stroke (1988);19:1497–1500. doi: 10.1161/01.STR.19.12.1497 1524-4628.
20. Barnes, M, Dobkin, B, and Bogousslavsky, J. Recovery after stroke Cambridge University Press (2005).
21. Levin, MF, Kleim, JA, and Wolf, SL. What do motor recovery and compensationg mean in patients following stroke? Neurorehabil Neural Repair. (2009) 23:313–9. doi: 10.1177/1545968308328727
22. Stroke Prevention and Educational Awareness Diffusion. Ictus cerebrale: Linee guida italiane di prevenzione e trattamento (2016).
23. Management Stroke Rehabilitation Working Group. VA/Dod clinical practice guideline for the management of stroke rehabilitation The Management of Stroke Rehabilitation Working Group. Available at: http://www.healthquality.va.govor http://www.qmo.amedd.army.mil.
24. Teasell, R, Foley Msc, N, Mbbs, NH, Salter Msc, K, Cotoi Msc, A, and Richardson, M. Evidence-based review of stroke rehabilitation. 17th ed Available at: www.ebrsr.com.
25. Peters, MDJ, Marnie, C, Tricco, AC, Pollock, D, Munn, Z, Alexander, L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. (2020) 18:2119–26. doi: 10.11124/JBIES-20-00167
26. Tricco, AC, Lillie, E, Zarin, W, O'Brien, KK, Colquhoun, H, Levac, D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
27. de Morton, NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. (2009) 55:129–33. doi: 10.1016/S0004-9514(09)70043-1
28. Calabrò, RS, Naro, A, Russo, M, Bramanti, P, Carioti, L, Balletta, T, et al. Shaping neuroplasticity by using powered exoskeletons in patients with stroke: a randomized clinical trial. J Neuroeng Rehabil. (2018) 15:35. doi: 10.1186/s12984-018-0377-8
29. Kooncumchoo, P, Namdaeng, P, Hanmanop, S, Rungroungdouyboon, B, Klarod, K, Kiatkulanusorn, S, et al. Gait improvement in chronic stroke survivors by using an innovative gait training machine: a randomized controlled trial. Int J Environ Res Public Health. (2022) 19:224. doi: 10.3390/ijerph19010224
30. Wu, M, Landry, JM, Kim, J, Schmit, BD, Yen, SC, and Macdonald, J. Robotic resistance/assistance training improves locomotor function in individuals poststroke: a randomized controlled study. Arch Phys Med Rehabil. (2014) 95:799–806. doi: 10.1016/j.apmr.2013.12.021
31. Lee, D, and Lee, G. Effect of afferent electrical stimulation with mirror therapy on motor function, balance, and gait in chronic stroke survivors: a randomized controlled trial. Eur J Phys Rehabil Med. (2019) 55:442–9. doi: 10.23736/S1973-9087.19.05334-6
32. Arya, KN, Pandian, S, and Kumar, V. Effect of activity-based mirror therapy on lower limb motor-recovery and gait in stroke: a randomised controlled trial. Neuropsychol Rehabil. (2019) 29:1193–210. doi: 10.1080/09602011.2017.1377087
33. Son, YL, and Kim, JW. The effects of mirror neuron system-based self-observation training on lower limb muscle activity and dynamic balance in patients with chronic stroke. J Phys Ther Sci. (2018) 30:1241–4. doi: 10.1589/jpts.30.1241
34. Bang, DH, Shin, WS, Kim, SY, and Choi, JD. The effects of action observational training on walking ability in chronic stroke patients: a double-blind randomized controlled trial. Clin Rehabil. (2013) 27:1118–25. doi: 10.1177/0269215513501528
35. Cho, HY, Kim, JS, and Lee, GC. Effects of motor imagery training on balance and gait abilities in post-stroke patients: a randomized controlled trial. Clin Rehabil. (2013) 27:675–80. doi: 10.1177/0269215512464702
36. Dickstein, R, Deutsch, JE, Yoeli, Y, Kafri, M, Falash, F, Dunsky, A, et al. Effects of integrated motor imagery practice on gait of individuals with chronic stroke: a half-crossover randomized study. Arch Phys Med Rehabil. (2013) 94:2119–25. doi: 10.1016/j.apmr.2013.06.031
37. In, T, Lee, K, and Song, C. Virtual reality reflection therapy improves balance and gait in patients with chronic stroke: randomized controlled trials. Med Sci Monit. (2016) 22:4046–53. doi: 10.12659/MSM.898157
38. Kayabinar, B, Alemdaroğlu-Gürbüz, İ, and Yilmaz, Ö. The effects of virtual reality augmented robot-assisted gait training on dual-task performance and functional measures in chronic stroke: a randomized controlled single-blind trial. Eur J Phys Rehabil Med. (2021) 57:227–37. doi: 10.23736/S1973-9087.21.06441-8
39. Lloréns, R, Gil-Gómez, JA, Alcañiz, M, Colomer, C, and Noé, E. Improvement in balance using a virtual reality-based stepping exercise: a randomized controlled trial involving individuals with chronic stroke. Clin Rehabil. (2015) 29:261–8. doi: 10.1177/0269215514543333
40. Alwhaibi, RM, Mahmoud, NF, Basheer, MA, Zakaria, HM, Elzanaty, MY, Ragab, WM, et al. Impact of somatosensory training on neural and functional recovery of lower extremity in patients with chronic stroke: a single blind controlled randomized trial. Int J Environ Res Public Health. (2021) 18:583:1–10. doi: 10.3390/ijerph18020583
41. Yang, YR, Mi, PL, Huang, SF, Chiu, SL, Liu, YC, and Wang, RY. Effects of neuromuscular electrical stimulation on gait performance in chronic stroke with inadequate ankle control - a randomized controlled trial. PLoS One. (2018) 13:e0208609. doi: 10.1371/journal.pone.0208609
42. Bethoux, F, Rogers, HL, Nolan, KJ, Abrams, GM, Annaswamy, TM, Brandstater, M, et al. The effects of peroneal nerve functional electrical stimulation versus ankle-foot orthosis in patients with chronic stroke: a randomized controlled trial. Neurorehabil Neural Repair. (2014) 28:688–97. doi: 10.1177/1545968314521007
43. Beaulieu, LD, Massé-Alarie, H, Brouwer, B, and Schneider, C. Noninvasive neurostimulation in chronic stroke: a double-blind randomized sham-controlled testing of clinical and corticomotor effects. Top Stroke Rehabil. (2015) 22:8–17. doi: 10.1179/1074935714Z.0000000032
44. Lee, SW, Cho, KH, and Lee, WH. Effect of a local vibration stimulus training programme on postural sway and gait in chronic stroke patients: a randomized controlled trial. Clin Rehabil. (2013) 27:921–31. doi: 10.1177/0269215513485100
45. Park, J, Seo, D, Choi, W, and Lee, S. The effects of exercise with TENS on spasticity, balance, and gait in patients with chronic stroke: a randomized controlled trial. Med Sci Monit. (2014) 20:1890–6. doi: 10.12659/MSM.890926
46. Lim, JH, Lee, HS, and Song, CS. Home-based rehabilitation programs on postural balance, walking, and quality of life in patients with stroke: a single-blind, randomized controlled trial. Medicine. (2021) 100:E27154. doi: 10.1097/MD.0000000000027154
47. Hornby, TG, Henderson, CE, Plawecki, A, Lucas, E, Lotter, J, Holthus, M, et al. Contributions of stepping intensity and variability to mobility in individuals poststroke. Stroke. (2019) 50:2492–9. doi: 10.1161/STROKEAHA.119.026254
48. Globas, C, Becker, C, Cerny, J, Lam, JM, Lindemann, U, Forrester, LW, et al. Chronic stroke survivors benefit from high-intensity aerobic treadmill exercise: a randomized control trial. Neurorehabil Neural Repair. (2012) 26:85–95. doi: 10.1177/1545968311418675
49. Chen, IH, Yang, YR, Chan, RC, and Wang, RY. Turning-based treadmill training improves turning performance and gait symmetry after stroke. Neurorehabil Neural Repair. (2014) 28:45–55. doi: 10.1177/1545968313497102
50. Choi, W, Han, D, Kim, J, and Lee, S. Whole-body vibration combined with treadmill training improves walking performance in post-stroke patients: a randomized controlled trial. Med Sci Monit. (2017) 23:4918–25. doi: 10.12659/MSM.904474
51. Cho, KH, and Lee, WH. Effect of treadmill training based real-world video recording on balance and gait in chronic stroke patients: a randomized controlled trial. Gait Posture. (2014) 39:523–8. doi: 10.1016/j.gaitpost.2013.09.003
52. Hwang, DY, Lee, HJ, Lee, GC, and Lee, SM. Treadmill training with tilt sensor functional electrical stimulation for improving balance, gait, and muscle architecture of tibialis anterior of survivors with chronic stroke: a randomized controlled trial. Technol Health Care. (2015) 23:443–52. doi: 10.3233/THC-150903
53. An, CM, and Jo, SO. Effects of talocrural mobilization with movement on ankle strength, mobility, and weight-bearing ability in hemiplegic patients with chronic stroke: a randomized controlled trial. J Stroke Cerebrovasc Dis. (2017) 26:169–76. doi: 10.1016/j.jstrokecerebrovasdis.2016.09.005
54. Park, D, Cynn, HS, Yi, C, Choi, WJ, Shim, JH, and Oh, DW. Four-week training involving self-ankle mobilization with movement versus calf muscle stretching in patients with chronic stroke: a randomized controlled study. Top Stroke Rehabil. (2020) 27:296–304. doi: 10.1080/10749357.2019.1690831
55. Liao, WC, Lai, CL, Hsu, PS, Chen, KC, and Wang, CH. Different weight shift trainings can improve the balance performance of patients with a chronic stroke: a randomized controlled trial. Medicine. (2018) 97:e13207. doi: 10.1097/MD.0000000000013207
56. Cho, KH, and Song, WK. Robot-assisted reach training with an active assistant protocol for long-term upper extremity impairment poststroke: a randomized controlled trial. Arch Phys Med Rehabil. (2019) 100:213–9. doi: 10.1016/j.apmr.2018.10.002
57. Cordo, P, Wolf, S, Lou, JS, Bogey, R, Stevenson, M, Hayes, J, et al. Treatment of severe hand impairment following stroke by combining assisted movement, muscle vibration, and biofeedback. J Neurol Phys Ther. (2013) 37:194–203. doi: 10.1097/NPT.0000000000000023
58. Hung, C-s, Lin, K-c, Chang, W-y, Huang, W-c, Chang, YJ, Chen, CL, et al. Unilateral vs bilateral hybrid approaches for upper limb rehabilitation in chronic stroke: a randomized controlled trial. Arch Phys Med Rehabil. (2019) 100:2225–32. doi: 10.1016/j.apmr.2019.06.021
59. Lin, CH, Chou, LW, Luo, HJ, Tsai, PY, Lieu, FK, Chiang, SL, et al. Effects of computer-aided interlimb force coupling training on paretic hand and arm motor control following chronic stroke: a randomized controlled trial. PLoS One. (2015) 10:e0131048. doi: 10.1371/journal.pone.0131048
60. Choi, HS, Shin, WS, and Bang, DH. Mirror therapy using gesture recognition for upper limb function, neck discomfort, and quality of life after chronic stroke: a single-blind randomized controlled trial. Med Sci Monit. (2019) 25:3271–8. doi: 10.12659/MSM.914095
61. Colomer, C, Noè, E, and Llorens, R. Mirror therapy in chronic stroke survivors with severely impaired upper limb function: a randomized controlled trial. Eur J Phys Rehabil Med. (2016) 52:271–8.
62. Cho, HS, and Cha, HG. Effect of mirror therapy with tDCS on functional recovery of the upper extremity of stroke patients. J Phys Ther Sci. (2015) 27:1045–7. doi: 10.1589/jpts.27.1045
63. Hernandez, A, and Bubyr, L. Virtual reality-based rehabilitation as a feasible and engaging tool for the management of chronic poststroke upper-extremity function recovery: randomized controlled trial. JMIR Serious Games. (2022) 1:e37506. doi: 10.2196/preprints.37506
64. De Diego, C, Puig, S, and Navarro, X. A sensorimotor stimulation program for rehabilitation of chronic stroke patients. Restor Neurol Neurosci. (2013) 31:361–71. doi: 10.3233/RNN-120250
65. Lee, YY, Lin, KC, Cheng, HJ, Wu, CY, Hsieh, YW, and Chen, CK. Effects of combining robot-assisted therapy with neuromuscular electrical stimulation on motor impairment, motor and daily function, and quality of life in patients with chronic stroke: a double-blinded randomized controlled trial. J Neuroeng Rehabil. (2015) 12:96. doi: 10.1186/s12984-015-0088-3
66. Knutson, JS, Gunzler, DD, Wilson, RD, and Chae, J. Contralaterally controlled functional electrical stimulation improves hand dexterity in chronic hemiparesis: a randomized trial. Stroke. (2016) 47:2596–602. doi: 10.1161/STROKEAHA.116.013791
67. Tavernese, E, Paoloni, M, Mangone, M, Mandic, V, Sale, P, Franceschini, M, et al. Segmental muscle vibration improves reaching movement in patients with chronic stroke. A randomized controlled trial. Neurorehabilitation. (2013) 32:591–9. doi: 10.3233/NRE-130881
68. Costantino, C, Galuppo, L, and Romiti, D. Short-term effect of local muscle vibration treatment versus sham therapy on upper limb in chronic post-stroke patients: a randomized controlled trial. Eur J Phys Rehabil Med. (2017) 53:32–40. doi: 10.23736/S1973-9087.16.04211-8
69. Karthikbabu, S, Chakrapani, M, Ganesan, S, Ellajosyula, R, and Solomon, JM. Efficacy of trunk regimes on balance, mobility, physical function, and community reintegration in chronic stroke: a parallel-group randomized trial. J Stroke Cerebrovasc Dis. (2018) 27:1003–11. doi: 10.1016/j.jstrokecerebrovasdis.2017.11.003
70. Lee, NG, You, J, Yi, CH, Jeon, HS, Choi, BS, Lee, DR, et al. Best Core stabilization for anticipatory postural adjustment and falls in hemiparetic stroke. Arch Phys Med Rehabil. (2018) 99:2168–74. doi: 10.1016/j.apmr.2018.01.027
71. Lee, Y, Lee, J, Shin, S, and Lee, S. The effect of dual motor task training while sitting on trunk control ability and balance of patients with chronic stroke. J Phys Ther Sci. (2012) 24:345–9. doi: 10.1589/jpts.24.345
72. Park, HK, Lee, HJ, Lee, SJ, and Lee, WH. Land-based and aquatic trunk exercise program improve trunk control, balance and activities of daily living ability in stroke: a randomized CLINICAL trial. Eur J Phys Rehabil Med. (2019) 55:687–94. doi: 10.23736/S1973-9087.18.05369-8
73. Pérez-De la Cruz, S. Influence of an aquatic therapy program on perceived pain, stress, and quality of life in chronic stroke patients: a randomized trial. Int J Environ Res Public Health. (2020) 17:1–12. doi: 10.3390/ijerph17134796
Keywords: chronic stroke, motor impairment, stroke sequelae, rehabilitation, hemiplegic patient, recovery
Citation: Paolucci T, Agostini F, Mussomeli E, Cazzolla S, Conti M, Sarno F, Bernetti A, Paoloni M and Mangone M (2023) A rehabilitative approach beyond the acute stroke event: a scoping review about functional recovery perspectives in the chronic hemiplegic patient. Front. Neurol. 14:1234205. doi: 10.3389/fneur.2023.1234205
Edited by:
Dmitrii Kaplun, Saint Petersburg State Electrotechnical University, RussiaReviewed by:
Damiana Scuteri, University of Calabria, ItalyCopyright © 2023 Paolucci, Agostini, Mussomeli, Cazzolla, Conti, Sarno, Bernetti, Paoloni and Mangone. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Massimiliano Mangone, bWFzc2ltaWxpYW5vLm1hbmdvbmVAdW5pcm9tYTEuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.