
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 11 July 2023
Sec. Dementia and Neurodegenerative Diseases
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1198869
 Francisco Lopera1*†
Francisco Lopera1*† Nilton Custodio2†
Nilton Custodio2† Mariana Rico-Restrepo3
Mariana Rico-Restrepo3 Ricardo F. Allegri4
Ricardo F. Allegri4 José Domingo Barrientos5Estuardo Garcia Batres6
José Domingo Barrientos5Estuardo Garcia Batres6 Ismael L. Calandri4Cristian Calero Moscoso7
Ismael L. Calandri4Cristian Calero Moscoso7 Paulo Caramelli8
Paulo Caramelli8 Juan Carlos Duran Quiroz9
Juan Carlos Duran Quiroz9 Angela Marie Jansen10
Angela Marie Jansen10 Alberto José Mimenza Alvarado11
Alberto José Mimenza Alvarado11 Ricardo Nitrini12
Ricardo Nitrini12 Jose F. Parodi13Claudia Ramos14
Jose F. Parodi13Claudia Ramos14 Andrea Slachevsky15
Andrea Slachevsky15 Sonia María Dozzi Brucki12
Sonia María Dozzi Brucki12Alzheimer’s disease (AD) represents a substantial burden to patients, their caregivers, health systems, and society in Latin America and the Caribbean (LAC). This impact is exacerbated by limited access to diagnosis, specialized care, and therapies for AD within and among nations. The region has varied geographic, ethnic, cultural, and economic conditions, which create unique challenges to AD diagnosis and management. To address these issues, the Americas Health Foundation convened a panel of eight neurologists, geriatricians, and psychiatrists from Argentina, Brazil, Colombia, Ecuador, Guatemala, Mexico, and Peru who are experts in AD for a three-day virtual meeting to discuss best practices for AD diagnosis and treatment in LAC and create a manuscript offering recommendations to address identified barriers. In LAC, several barriers hamper diagnosing and treating people with dementia. These barriers include access to healthcare, fragmented healthcare systems, limited research funding, unstandardized diagnosis and treatment, genetic heterogeneity, and varying social determinants of health. Additional training for physicians and other healthcare workers at the primary care level, region-specific or adequately adapted cognitive tests, increased public healthcare insurance coverage of testing and treatment, and dedicated search strategies to detect populations with gene variants associated with AD are among the recommendations to improve the landscape of AD.
Dementia represents a substantial public health challenge in Latin America and the Caribbean (LAC). The demographic structure of LAC has rapidly evolved in recent decades to resemble that of high-income countries (1), with a prevalence of dementia in LAC ranging from 7.1 to 11.5% in individuals over 65 years of age, exceeding that of Europe and the United States. The number of people with dementia in LAC is expected to rise from 7.8 million in 2013 to more than 27 million by 2050, owing to demographic and health changes (2). The widespread idea that dementia and Alzheimer’s disease (AD) are problems in high-income countries must be changed.
AD is the most common cause of dementia in LAC, accounting for 50–84% of cases (3, 4). An aging population and low socioeconomic and educational levels (especially illiteracy) contribute to an increasing prevalence (1, 5). Despite global advancements in fighting dementia, substantial barriers to managing AD persist in LAC. Despite the considerable burden of disease that dementia represents, only Chile, Costa Rica, Cuba, Mexico, and Puerto Rico have national dementia plans; they are insufficiently funded. Argentina discontinued its dementia program (6). The absence of these programs is often due to economic and political instability. Although an exact figure is unavailable, many people living with AD in the region lack access to diagnosis and basic support for their disease. Furthermore, a lack of clinical practice guidelines or recommendations on AD diagnosis and treatment hinders early detection and results in unstandardized management. This review aims to provide multidisciplinary expert recommendations for managing AD in LAC.
Americas Health Foundation (AHF) assembled a multidisciplinary panel of eight neurologists, geriatricians, and psychiatrists who are experts in AD from Argentina, Brazil, Colombia, Ecuador, Guatemala, Mexico, and Peru. On September 27, 29, and 30, 2022, they had virtual meetings to develop recommendations for overcoming AD diagnosis and treatment obstacles in LAC. AHF used PubMed, MEDLINE, and EMBASE to identify AD scientists and clinicians from LAC. Augmenting this search, AHF contacted LAC’s medical community thought leaders to confirm that the list accurately represented the required specialties. All the experts who attended the meeting are named authors of this manuscript.
AHF researched AD in PubMed, MEDLINE, and EMBASE. “Treatment,” “management,” “diagnosis,” “quality of life,” and “patient journey” in combination with “Latin America,” and “Alzheimer’s disease” were searched with dates ranging from 01/01/2016 to 06/10/2022. The articles identified were in English, Portuguese, and Spanish. Articles from LAC were prioritized.
Based on the literature search, AHF developed specific questions to address barriers limiting access to AD diagnosis and treatment in LAC and assigned one to each panel member. A written response to each question was drafted by individual panel members based on the literature review and personal expertise. The entire panel reviewed and edited each narrative during the three-day conference through numerous rounds of discussion until a total agreement was reached. An AHF staff member moderated the discussion. When the panel disagreed, additional discussions were held until everyone agreed on the paper’s content. After the conference, seven neurologists, geriatricians, and psychiatrists who are experts in AD from Argentina, Bolivia, Brazil, Chile, Colombia, and Peru reviewed and edited the document. Their contributions were discussed and incorporated. All authors reviewed and approved the final manuscript. The recommendations are based on the evidence gathered and expert opinion and were approved by all authors.
Eight population studies conducted in Brazil, Chile, Cuba, Peru, and Venezuela showed a dementia prevalence of 7.1% that doubles every 5 years from 65 years onward (3). The dementia incidence rate was 13.8 per 1,000 people/year for individuals over 65, while that of AD was 7.7 (7). In a systematic review of 17 LAC countries, all-cause dementia prevalence was 10.66%. A higher prevalence was observed among women (8.97%) and rural residents (8.68%). Those with no formal education had more than double the frequency (21.37%) compared to at least 1 year of education (9.88%) (8).
Mortality from dementia increased by 148% between 1990 and 2016. In 2016, dementia was the fifth most common cause of death worldwide, responsible for 2.4 million deaths. Dementia accounted for 4.4% of all deaths and 8.6% of deaths among those over 70, making dementia the second leading cause of mortality in this age group (9). Of 17.4 million people in Chile, there were 3,852 dementia deaths in 2012 (including 1,585 Alzheimer’s deaths) (10). Dementia caused 28.8 million disability-adjusted life years (DALYs) worldwide. It represented 1.2% of DALYs across all ages and 6.3% in those over 70 (11). A study in Chile based on the Chilean national health survey found that dementia had a high impact at the population level in terms of Quality-Adjusted Life Years (QALY) lost and at the individual level in terms of loss of Health-State Utilities (HSU), outnumbering other diseases (12).
In LAC, the fight against dementia faces pressing challenges, including healthcare access barriers, fragmented healthcare systems, limited research funding, unstandardized diagnosis and treatment, genetic heterogeneity, and varying social determinants of health (5, 11). Additionally, dementia is not a priority for most LAC countries, despite its considerable disease burden (2). Only Chile, Costa Rica, Cuba, Mexico, and Puerto Rico have national dementia plans, but insufficient funding often limits them. Other important barriers are insufficient training in dementia for health professionals and ageism or myths about aging. Four main challenge areas were highlighted at the World Congress of Neurology in Santiago, Chile, in 2015: timely diagnosis, therapeutic approaches and participation in clinical trials, treatment and post-diagnostic support, and research collaboration (6).
There is growing evidence that healthcare-related disparities have a greater impact on populations with low educational and socioeconomic levels, commonly found in LAC. There are often misdiagnoses (13) and delays in referrals to dementia specialists (2). Evidence suggests that racial and ethnic minority groups within LAC are less likely to receive treatment and more likely to discontinue anti-dementia medications (2). Due to fragmentation in healthcare systems, a lack of continuity of care, and access to specialists, patients often remain on antipsychotic medication, even once behavioral symptoms have resolved (14). However, more studies on treatment trends in LAC are necessary. The direct and indirect costs related to AD care are generally borne by the patient’s families, with variations between and within countries and depending on health insurance and socioeconomic level (15, 16).
Certain risk factors for dementia can potentially be modifiable throughout life. These include low education (8%), hypertension (2%), hearing loss (8%), obesity (1%), smoking (5%), alcoholism (1%), cranial trauma (3%), depression (4%), physical inactivity (3%), social isolation (2%), diabetes (1%) and air pollution (2%). Compared to Europe and North America, the population attributable fraction for modifiable risk factors for dementia is higher due to a greater prevalence of cardiovascular risk factors (17, 18). Of note, these are not risk factors specific for AD but for neurodegeneration and dementia syndrome. In LAC, controlling these factors could prevent up to 40–56% of dementia cases (17, 19, 20).
Research on AD in LAC has grown recently but is still limited, mainly due to restricted funding. In 2013, there were 715 AD clinical trials globally, and only 34 were in South America (21). By 2020, only 6% of active trials included LAC countries, mainly Argentina, Brazil, Chile, Colombia, and Mexico (6). LatAm-FINGERS, the dementia prevention lifestyle-change trial for dementia prevention, has been operating since 2021. This is the only dementia trial designed in Latin America and brings together 12 countries in the region (Argentina, Brazil, Bolivia, Chile, Colombia, Costa Rica, Ecuador, Mexico, Peru, Puerto Rico, Dominican Republic, and Uruguay) (22). Scarce regional data impacts understanding pharmacokinetics, pharmacodynamics, and genetic influences and hinders public policy development. Favorable regulatory environments for clinical trials, clinical trial unit infrastructure, and increased funding mechanisms must be developed to increase LAC participation in AD research.
LAC countries have different cultural, linguistic, and ideological nuances determining AD detection, management, and prognosis. The main obstacles to early AD detection in LAC are misconceptions surrounding memory impairment, training at the primary care level, and specialist availability (23).
AD diagnosis in LAC is primarily based on clinical information and cognitive tests. Biomarkers and imaging are limited to a few centers, and genetic screening is rare (9). When applied effectively, clinical criteria (24, 25) when used effectively, may offer up to 90% diagnostic accuracy. Some countries have recommendations and guidelines for dementia diagnosis and management (Argentina (26), Brazil (27), Chile (28, 29), Colombia (30), Mexico (31), Peru) (23, 32, 33).
According to DSM-5, dementia includes memory loss, cognitive decline, and impairment of functionality. Consequently, these must be evidenced in clinical practice using brief cognitive tests (BCTs) and questionnaires about activities of daily living (ADL). Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Addenbrooke’s cognitive examination (ACE III), and Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) are the most widely used instruments across LAC (8). Evidence shows sociodemographic variables, including age, sex, education, literacy, and language impact BCT performance (32). The high prevalence of lower educational achievement and socioeconomic disparities in LAC (34) and the fact that the performance of illiterate individuals on neuropsychological tests often resembles that of literate individuals with dementia may contribute to misdiagnosis (8, 35, 36). Thus, as a minimum, countries should have cognitive tests validated for their local context. The Rowland Universal Dementia Assessment Scale (RUDAS) (35) and Brief Cognitive Screening Battery (BCSB) (36, 37) could better adapt to the conditions of LAC populations. The Pfeffer Functional Activities Questionnaire (PFAQ) and the Technology-Activities of Daily Living Questionnaire (T-ADLQ) are recommended to evaluate ADL (38).
Many communities in LAC only have access to primary care. Opportunities for diagnosis may be missed because primary care providers (PCPs) often fail to screen older adults for AD due to insufficient time and training. Early symptoms of dementia, such as memory impairment, may not be apparent during a routine office visit unless they are directly assessed (39). Thus, it is crucial to increase LAC PCPs’ awareness of their role in AD early detection and training on the appropriate application of cognitive assessment tools. To this end, recommendations are proposed for evaluating memory complaints at the primary care level in LAC (See Figure 1).
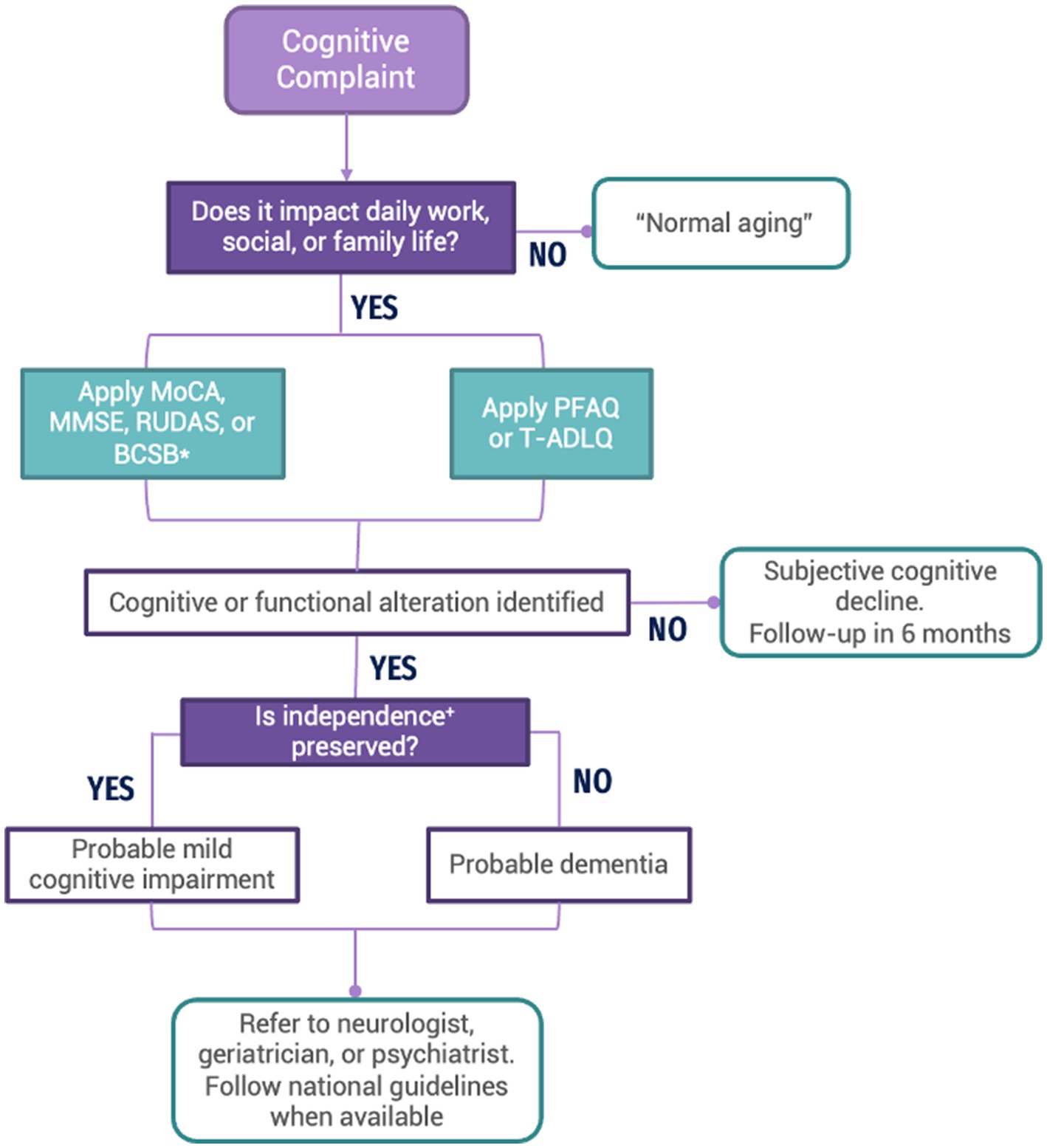
Figure 1. Flow chart depicting the recommended process to assess patients with cognitive complaints at the primary care level in LAC. MoCA, Montreal Cognitive Assessment; MMSE, Mini-Mental State Examination; RUDAS, Rowland Universal Dementia Assessment Scale; BCSB, Brief Cognitive Screening Battery; PFAQ, Pfeffer Functional Activities Questionnaire; T-DALQ, Technology-Activities of Daily Living Questionnaire. *Adjusted for patient’s age, literacy, and educational levels. +Independence is understood as the ability or aptitude to make informed and responsible decisions in ADL (managing financial affairs, fulfilling a desired task, driving a vehicle, administering medications, or living independently) (40).
1. A complete anamnesis and physical exam should be conducted. The presence of an accompanying family member or caregiver is necessary. A structured interview should identify whether the cognitive complaint affects the patient’s daily work, social or family life. If the answer is yes, the evaluation should be continued. Notably, questions about behavioral or emotional symptoms should be asked.
2. Conduct a cognitive evaluation using MoCA, MMSE, RUDAS, or BCSB (41) with the appropriate adjustments based on the patient’s age, education, and literacy level.
3. Conduct a functional evaluation using the PFAQ or T-ADLQ: Technology–Activities of Daily Living Questionnaire’.
4. If an impairment is identified in cognitive or functional assessments, refer to a specialist (neurologist, geriatrician, or psychiatrist) for continued evaluation and care or follow the national guideline for dementia.
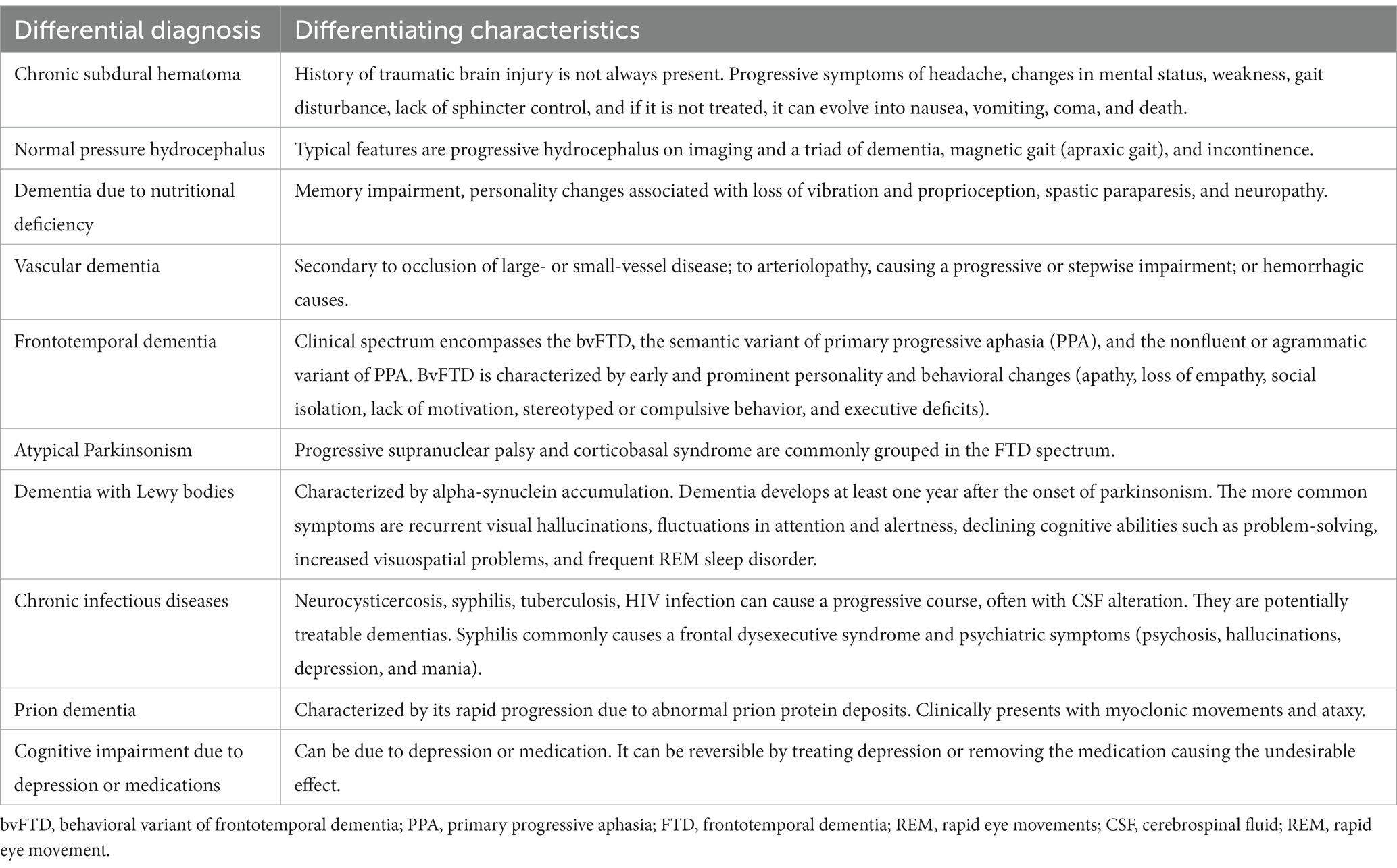
1. Conduct a complete physical examination and a direct interview to understand the patient’s context and support network, comorbidities, current medication, and the level of impact of symptoms on the patient’s life. The presence of a family member or caregiver is necessary. Consider differential diagnosis (Table 1).
2. Order a formal neuropsychological evaluation (if available), particularly if symptoms are mild [e.g., mild cognitive impairment (MCI)] or in cases where the differential diagnosis is challenging (e.g., non-amnestic/atypical presentations of AD).
3. Order additional testing. These may include imaging studies. The neuroimage of choice in patients with dementia is magnetic resonance imaging (MRI). In cases where it is unavailable or contraindicated, a computerized tomography (CT) can be performed (suggested neuroimaging can be found in Table 2). Laboratory tests: thyroid profile, lipid profile, vitamin B12, folic acid, venereal disease research laboratory test (VDRL), blood glucose, renal function, complete blood count with sedimentation rate, and electrolytes must also be ordered to rule out reversible causes of cognitive impairment or clinical comorbidities that may impair cognitive functioning.
4. Make treatment and follow-up decisions based on evaluation findings.
5. Order biomarkers, when available, for patients with symptom onset below 65 years of age or MCI or atypical AD clinical presentations.
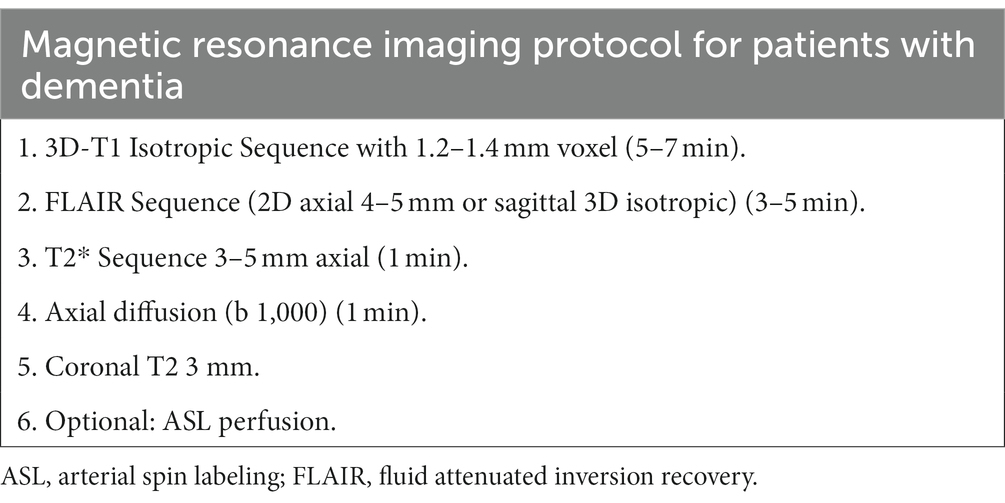
Table 2. Magnetic resonance imaging protocol for patients with dementia (45).
Given that the pathophysiological processes of AD are a continuum that begins years before the first symptoms appear, the US National Institute on Aging and the Alzheimer’s Association proposed two AD diagnostic categories based on their stage of progression: preclinical or asymptomatic (biological definition of AD); and clinical or symptomatic (clinical definition of AD). Of note, preclinical diagnosis is currently recommended only in research contexts. The clinical stage can, in turn, be divided into two subcategories: MCI; and dementia in mild, moderate, and severe stages. AD can be monitored throughout this continuum using biomarkers or direct and indirect indicators of neuropathological changes in the brain, as well as clinical signs and symptoms (46). In LAC, monitoring with biomarkers and indicators of neuropathological changes in the brain is currently applied primarily in research contexts.
The preclinical stage can also be subdivided into stages. This has been done with the genetic form of AD caused by the Paisa mutation (E280A in PS1). This mutation affects 25 multigenerational families in Mendelian inheritance, representing the largest group in the world, consisting of more than 6,000 inheritors and 1,200 carriers. The time between birth and 24 years of age is Phase 0, when abnormally high levels of pTau217 and neurofilament light chain (NfL) are detected in plasma and low levels of Aß42 -amyloid in cerebrospinal fluid (CSF). Phase 1 lasts from 24 to 28 years when amyloid-positive cells begin to appear on the positron emission tomography (PET)-amyloid image. Phase 2 is from 28 to 32 years of age when a significant reduction in memory scores on the 10-word CERAD list is detected in asymptomatic people without memory problems. In stage 3, from 32 to 38 years of age, positive signs of tauopathy appear in the PET-tau image, and subjective memory loss occurs without impact. Finally, in Phase 4, from 38 to 44 years of age, when memory complaints with impact and MCI appear (47, 48). The most used staging scales for AD in LAC are the Global Deterioration Scale (GDS) and Clinical Dementia Rating Scale (CDR); GDS offers significant advantages by more clearly defining the MCI stage, in addition to having validation studies in LAC (46). The correlation of AD clinical stages with the GDS and CDR is shown in Figure 2 (1, 49, 50).
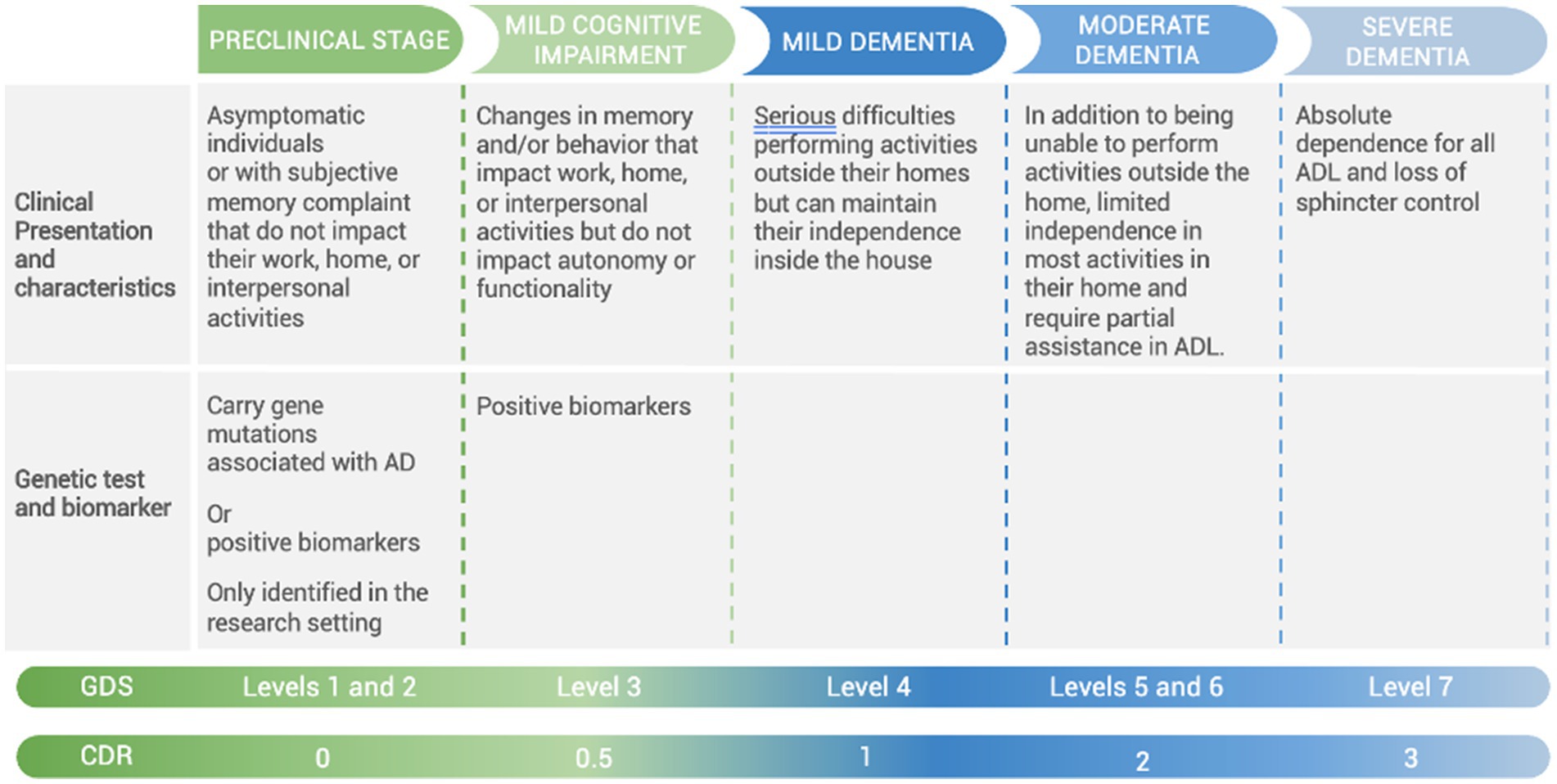
Figure 2. Correlation of AD clinical stages with Global Deterioration Scale (GDS) and Clinical Dementia Rating Scale (CDR). ADL, activities of daily living; AD, Alzheimer’s disease.
After a patient receives a diagnosis, the pathway to receive treatment and support varies among countries and depends widely on what type of healthcare insurance the patient has. Non-pharmacological management encompasses a wide range of non-invasive, safe approaches and techniques that, when used in a standardized and guided manner, can improve cognitive function, neuropsychiatric symptoms, and independence in patients with AD, as well as their caregivers’ quality of life (QoL). These interventions do not influence the underlying pathophysiological mechanisms; they focus on maintaining the patient’s functionality for as long as possible as the disease progresses (51). A scoping review was conducted of non-pharmacologic interventions for caregivers of people living with dementia in LAC (52), but there are scarce publications about non-pharmacological strategies aimed at the patient residing in any LAC country (53). Three months of multimodal training contributed to mobility and executive function in elderly individuals with mild cognitive impairment but not in those with Alzheimer’s disease; additionally, in Massachusetts, an intervention (Virtual mentalizing imagery therapy) has been adapted for Hispanic participants living in Boston (54).
Multiple studies confirm the positive effect of exercise programs in reducing the progression of dependence in patients with AD (55–57). In animal models, exercise therapy improved cognitive performance mechanisms, such as increasing growth factors (58), alleviating oxidative stress (59), decreasing antibody concentrations (60). Early intervention in the 3xTg-AD mice with an amyloid β-antibody fragment ameliorates the first hallmarks of Alzheimer’s disease (60), and inhibits tau phosphorylation from slowing the progression of dementia (60). Treadmill exercise promotes E3 ubiquitin ligase to remove amyloid β and P-tau and improve cognitive ability in APP/PS1 transgenic mice (61), but the applicability in humans may have some variability in cognitive improvement due to the differences in exercise modality, intensity, frequency, and duration of study design; so, future research on the process of exercise therapy for cognitive improvement needs to describe more specific exercise modalities and find more accurate ways to mitigate the process of dementia (62).
On the other hand, concerning rehabilitation goals and collaborative goal-setting in patients with mild-to-moderate dementia was feasible, especially when patients were supported by a structured approach, which yielded a more holistic view of potential rehabilitation goals and needs from the patients’ perspective. Mobility-related functions were stated as the most critical rehabilitation goals, followed by functions related to psychological well-being, and self-reported functional problems showed a significant relationship with objective clinical assessments indicating a sustained insight into acute functional deficits in patients with mild-to-moderate dementia (63). Cognitive stimulation involves themed activities and is typically implemented twice weekly. Several studies report improved general cognitive functioning in patients with mild-to-moderate dementia (7, 64). Current evidence suggests that it can be delivered face-to-face or online (65, 66). Integrating exercise, proper nutrition, and cognitive and social interventions may significantly mitigate cognitive decline in people with dementia. In fact, the benefits of non-pharmacological interventions provide the basis for future pharmacological interventions (67).
All guidelines agree that the first-line treatment for behavioral and psychological symptoms should be non-pharmacological management. Interventions range from tailored activity programs to sensorial, psychological, and behavioral approaches, including environmental redesign, validation, reminiscence, and light therapy (7, 68). A first-line pharmacological approach should only be used if neuropsychiatric symptoms cause a high risk of harm (6).
Other types of non-pharmacological therapy, such as occupational therapy, including activity simplification, adaptive aids, problem-solving strategies, skill training, and caregiver education, have shown slight improvements in patient and caregiver QoL (69). Complementary therapies such as transcranial magnetic stimulation, alternative medicine, music, art, aroma, and massage therapy require further study to determine their benefit (7). Preliminary studies on communication technology therapies, such as home automation, virtual reality, video games, and telemedicine, show promising results that have yet to be confirmed (7).
Pharmacological therapy for AD currently consists of symptomatic treatments that seek to lessen the impact of cognitive symptoms, alleviate behavioral and psychological symptoms, and preserve functionality. There is great heterogeneity in the availability of anti-dementia treatments in LAC. In some countries, they are available through private or public healthcare; in others, they entail out-of-pocket costs for patients and their caregivers (1) (Table 3).
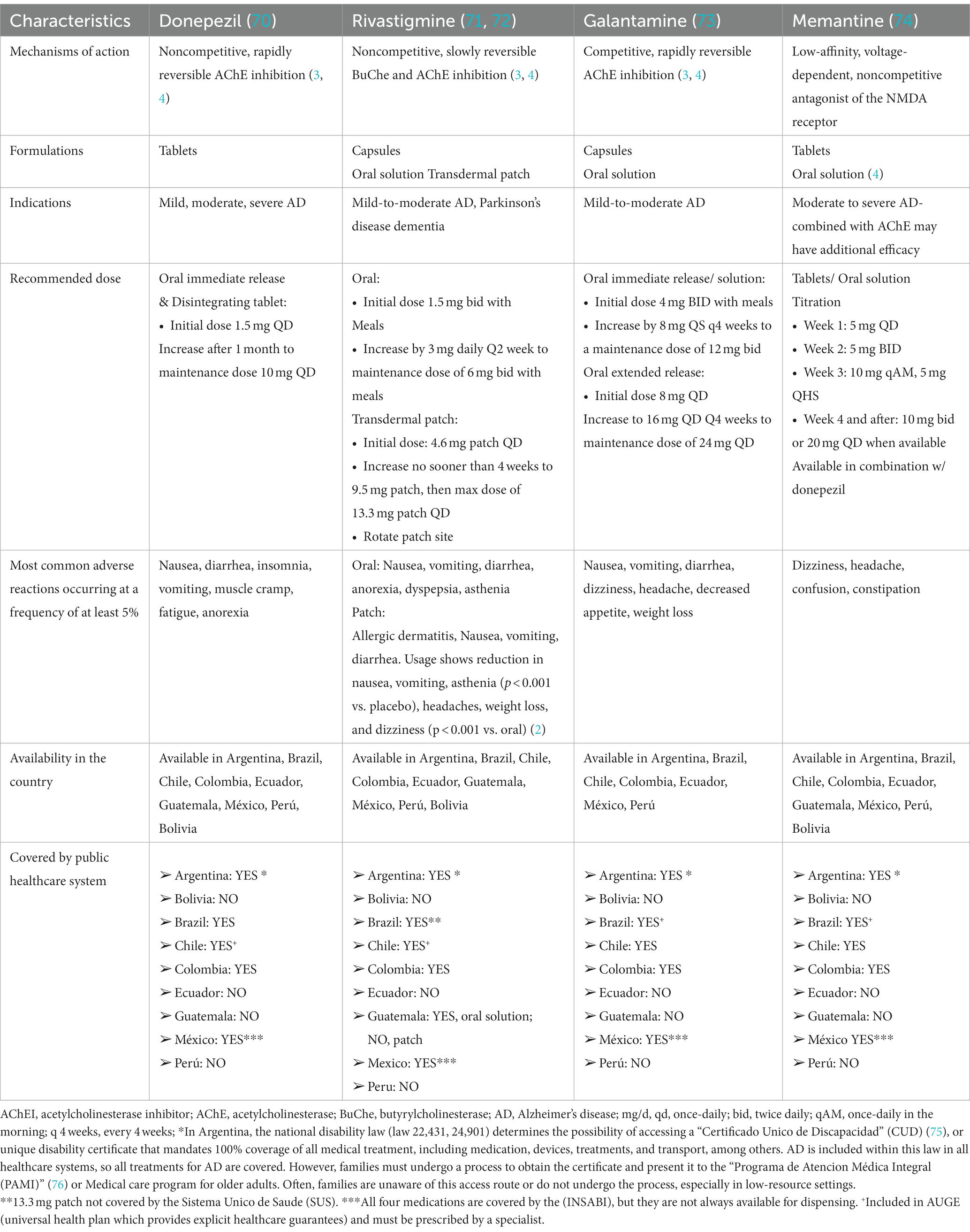
Table 3. Characteristics and access of cognitive-enhancing medications approved for AD.
Of the four FDA-approved drugs for AD treatment, three are acetylcholinesterase inhibitors (AChEIs) (donepezil, galantamine, rivastigmine) (2) and one, memantine (3), is an N-methyl-D-aspartate (NMDA) receptor antagonist. In some LAC countries, molecules approved for commercial use are often prescribed as adjuvants in AD treatment. These include Ginkgo biloba, cerebrolysin, nimodipine, and citicoline. All of them lack scientific evidence for their use in AD.
Rivastigmine patches have additional benefits, including simple administration, once-daily application, caregiver empowerment, prevention of accidental overdose, small and discrete size, comfort, and immediate removal in an emergency (77). From the pharmacological point of view, patches allow sustained plasma levels, reduce adverse events, and allow easier access to the optimal dose. Moreover, they avoid the digestive tract, making them independent of food intake and preventing first-pass loss (77, 78).
To improve treatment adherence, patients and caregivers should be counseled on realistic treatment outcomes and expectations of stabilizing cognitive symptoms and improving QoL rather than achieving noticeable improvements.
What “matters to the person” is one of the factors that should guide the care and design of health services in the 21st century (79–81). That means person center care versus disease center care. Early detection of cognitive impairment and AD can take several paths in LAC. The Pan American Health Organization has defined healthy aging as the process of greater functional ability that allows living with well-being. The functional ability (“to be and do what one considers valuable”) comprises the intrinsic capacity (sum of physical and mental capabilities), the environment, and the interaction between the two. The intrinsic capacity has several components or domains (cognitive, psychological, sensory, mobility, and vitality). Persons are integral beings, and the alteration in one of the domains of intrinsic capacity can be a warning sign of a latent or potential cognitive alteration (82). Bidirectional associations of the cognitive domain with mobility (83) (cognitive motor syndrome (84), cognitive frailty) (85), sensory (visual (86) and hearing (87)), psychological (88), and vitality (89)(metabolism and nutrition) have been demonstrated. Likewise, the manifestations in different domains worsen the prognosis of active life and well-being (90). Detecting changes in any of these domains can help detect early and manage cognitive alterations that could materialize in AD or its risk factors (91). At the same time, managing alterations in domains other than cognitive can optimize cognitive performance and facilitate care (92, 93). One of the justifications for the early diagnosis of AD is that the person can decide on treatment options at all stages of the disease (94).
Although AChEI are not approved for MCI in LAC, they are commonly prescribed for this indication, according to this panel’s experience. Some evidence exists of slight cognitive benefits and delays in conversion to dementia using donepezil in people with MCI (95, 96). This panel recommends initiating therapy with AChEI if there is amyloidosis in CSF or brain imaging or if there is a high suspicion of MCI due to AD because the patient meets one or more of the following criteria: (1) specific alteration of episodic memory; (2) reduced hippocampal volume; (3) has a proven causative genetic factor. Of note, memantine is often inadequately initiated at diagnosis, even if the patient has MCI or mild dementia. This is an erroneous practice, which should be avoided as memantine is not indicated in these cases (See Figure 3).
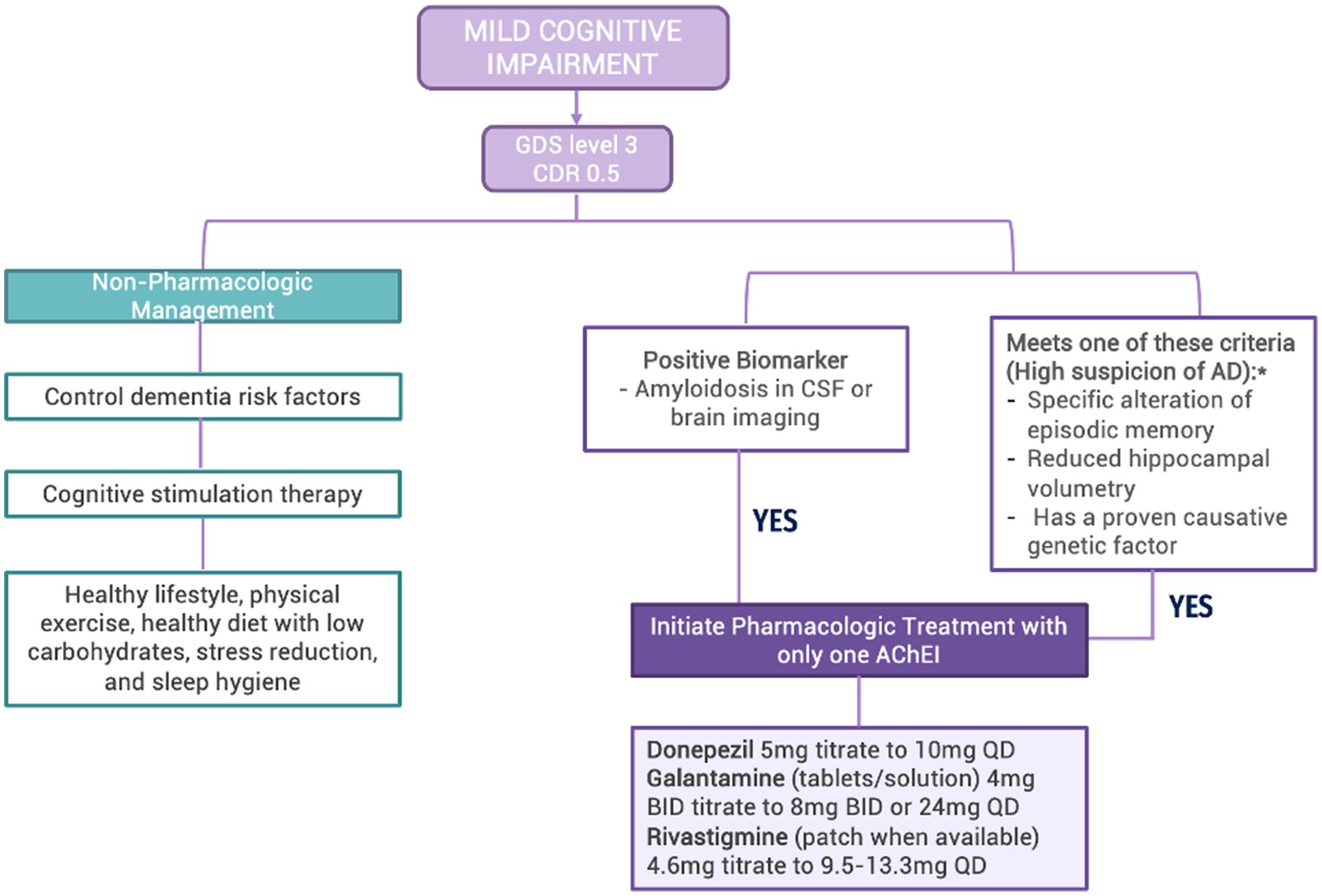
Figure 3. Algorithm for the management of mild cognitive impairment in LAC Legend: GDS: Global Deterioration Scale; CDR: Clinical Dementia Rating Scale; CSF: cerebrospinal fluid; AD: Alzheimer’s Disease; AChEI: acetylcholinesterase inhibitors *Although AChEI is not currently approved for the indication of MCI, this expert panel recommends its use in the specified situation.
For this group, treatment and management based on the following principles are required (See Figure 4):
1. Non-pharmacological interventions (97–99): A healthy lifestyle with physical exercise, a healthy diet with low carbohydrates, stress reduction, and sleep hygiene; control of dementia risk factors; cognitive stimulation therapy; and environmental redesign.
2. Pharmacologic therapy (100): Using one AChEI that increases the level of acetylcholine; if deterioration continues, measured by a drop >2 points on the MMSE in <6 months, a different AChEI should be initiated. If deterioration continues, memantine should be added to the treatment regimen.
3. Participation in pharmacological and non-pharmacological tertiary prevention studies, pending the commercial availability of these treatments, or palliative studies, depending on disease progression.
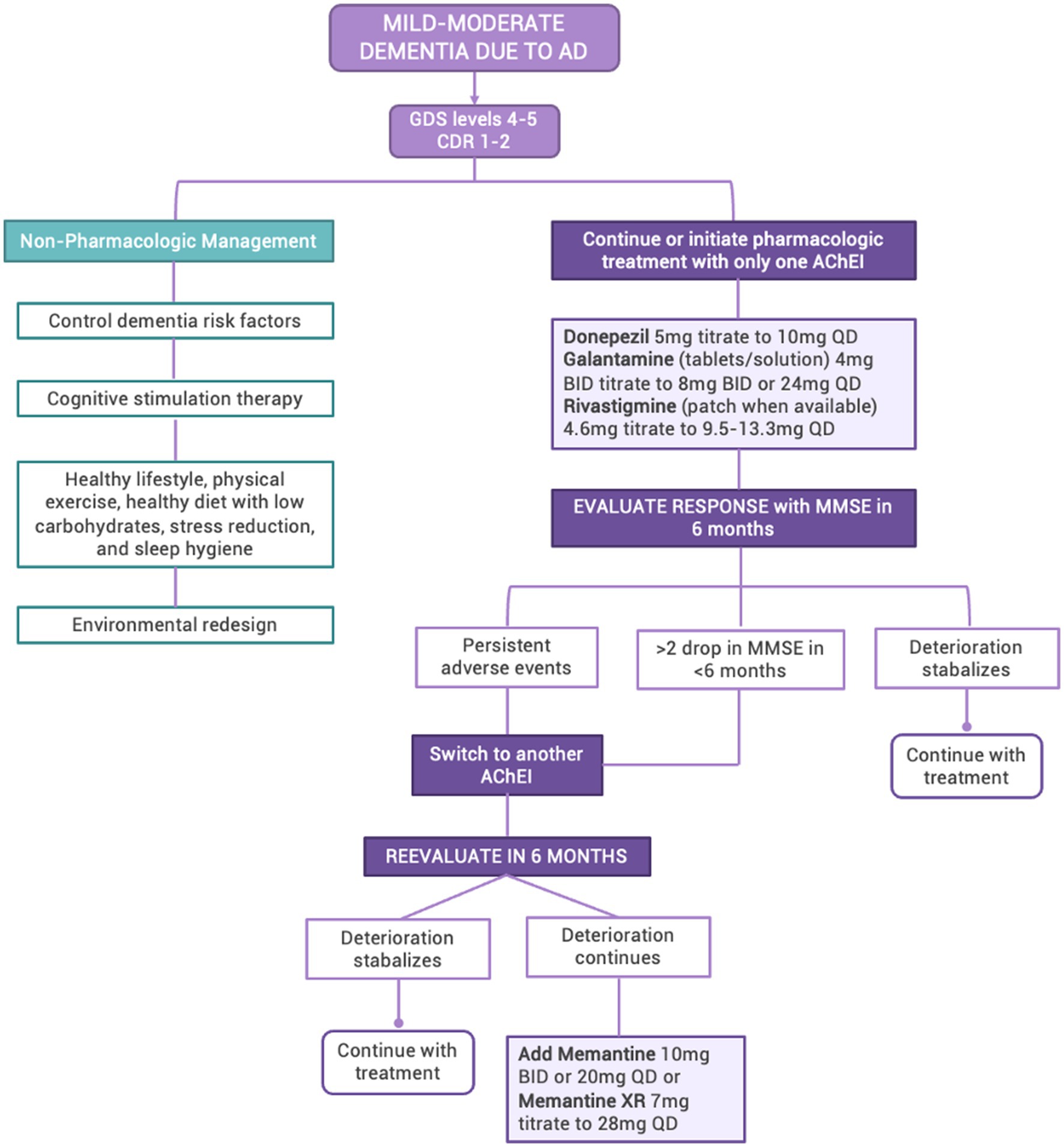
Figure 4. Algorithm for the management of mild–moderate dementia due to AD in LAC GDS, Global Deterioration Scale; CDR, Clinical Dementia Rating Scale; AD, Alzheimer’s Disease; AChEI, acetylcholinesterase inhibitors; MMSE, Mini-Mental State Evaluation.
Severe behavioral and psychological symptoms are hallmarks of this stage, and many patients require long-term institutional care (101, 102, 103). In LAC, most caregivers of patients with AD are women, frequently wives or daughters, that co-reside with the patient and do not receive financial compensation (104, 105). Severe AD results in a higher burden for caregivers, associated with higher levels of behavioral disturbances in patients (5).
This group requires treatment and management based on the following principles (See Figure 5) and guidelines (Table 4).
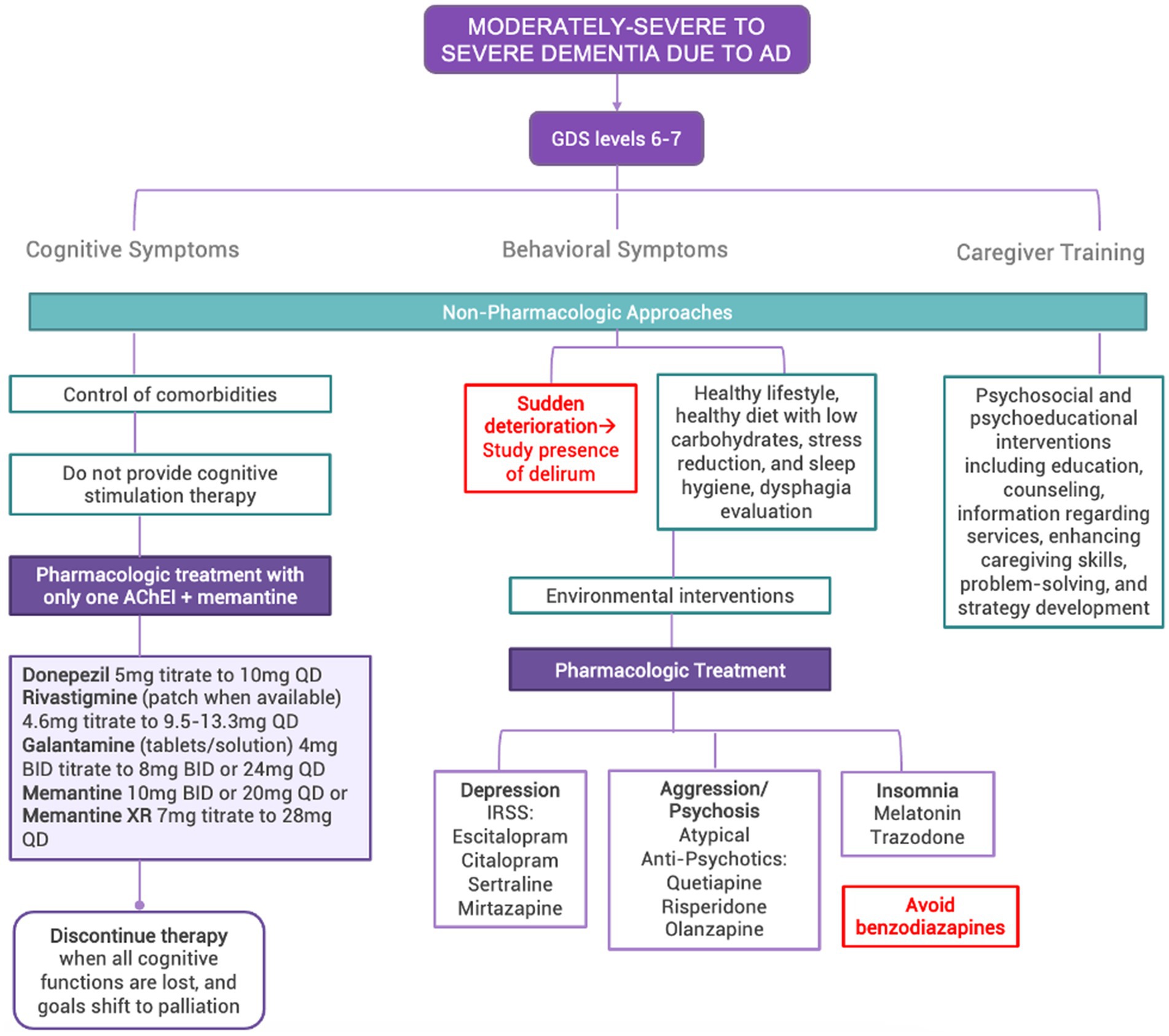
Figure 5. Algorithm for the management of moderately-severe to severe dementia due to AD in LAC. GDS, Global Deterioration Scale; CDR, Clinical Dementia Rating Scale; AD, Alzheimer’s Disease; AChEI, acetylcholinesterase inhibitors.
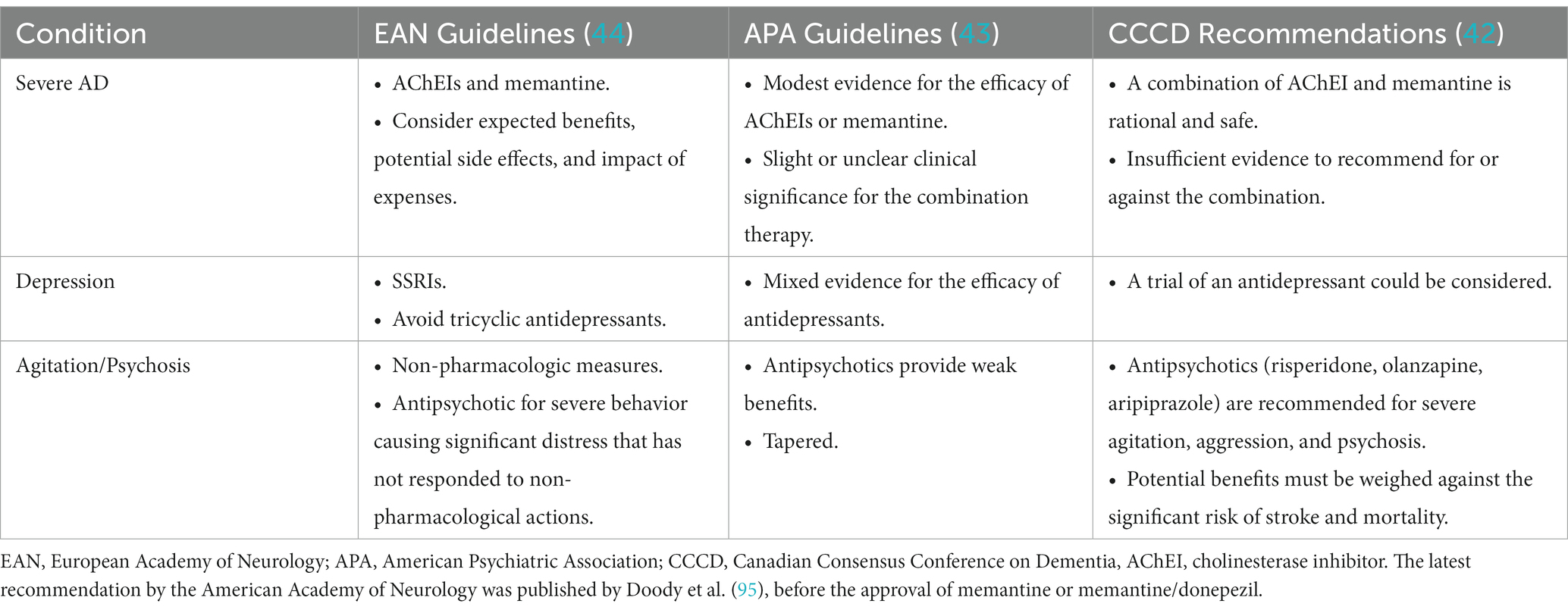
Table 4. Summary of clinical practice guideline recommendations for the treatment of severe AD.
Enteral nutrition (nasogastric tubes and percutaneous endoscopic gastrostomy) and hydration should be considered medical treatments rather than basic care and, therefore, should only be used if there is a realistic probability of improving or maintaining the patient’s condition and QoL. Enteral nutrition should not be initiated when no functional patient benefits are expected. Especially in patients where death is imminent (e.g., within the next 4 weeks or in advanced dementia), the patient’s comfort is the highest priority (106).
Cognitive stimulation is ineffective at this stage (29). Activities should be restricted when patients can no longer participate safely and productively (107). Non-pharmacologic approaches should be considered in treating behavioral symptoms before pharmacologic ones (108, 109). Specific behavioral management can help reduce depression, aggression, incontinence (24), and insomnia (110).
AChEI, combined with memantine, can be prescribed to these patients (101, 111–113). Several considerations must be made when deciding whether to continue treatment with the aforementioned depending on the clinician’s judgment. Because many LAC families must incur out-of-pocket expenses to acquire these therapies, physicians must evaluate the cost–benefit of using these medications related to the coverage of other needs in patients with severe AD (114, 115). Comorbidities must also be considered. Additionally, these treatments should not be initiated at a severe AD stage if the patient has not received them previously. Expected benefits include modest improvements or a slower decline in cognition function and behavior in severe AD (6, 116). The addition of memantine to AChEI significantly delayed nursing home admissions (117). Discontinuation of AChEI may worsen cognitive, neuropsychiatric, or functional status (118). Treatment should be continued until clinical benefit can no longer be demonstrated. Patients who are bedridden, noncommunicative, and can no longer perform basic daily activities can generally be safely withdrawn from medications. Medications should not be suspended simply because the patient has been admitted to a long-term care facility (1).
Severe behavioral and psychological symptoms (agitation, aggression, and psychosis) are the hallmark of severe dementia (5). However, the onset of delirium caused by infection, pain, other medical conditions, side effects from medication, and psychosocial or environmental factors must be considered in patients with a sudden worsening of behaviors (119, 120). Atypical antipsychotics and antidepressants may be initiated at the lowest doses, titrated slowly, and fully monitored (1) due to the anti-muscarinic adverse effects of these drugs (20). Attempts to taper or withdraw should be made (1) if there is no clinically significant response after 4 weeks (121) or (2) after 4 months of behavior stability (34). Risperidone, olanzapine, and quetiapine can be used for severe agitation, aggression, and psychosis. The potential benefit of all antipsychotic agents must be weighed against the potential risks, such as cerebrovascular events and death (122, 123). The mortality rate varies between first and second generation (haloperidol 20%, olanzapine 13%, risperidone 13%, quetiapine 9%) (34). Selective serotonin reuptake inhibitors can be used to treat severe depression (122). Benzodiazepines should be avoided or used in emergencies only for brief periods due to potential or paradoxical adverse events (falls, excessive sedation, worsening cognition) (20). Periodic medication review and de-prescribing opportunities guided by function and active life expectancy should be frequent practices in people with AD, especially those with multimorbidity (109, 124, 125).
Psychosocial and psychoeducational interventions for caregivers of people with AD should be provided (42). These can include education, counseling, information regarding services, enhancing caregiving skills, problem-solving, and strategy development. Some evidence-based health promotion programs can help care for persons with chronic diseases and caregivers’ self-care and self-efficacy (126).
Physical environment interventions are beneficial. These include more visible toilets, outdoor areas with therapeutic design features, high light levels, moderate stimulation, and reduction of overstimulation when bathing (127). Most patients with severe dementia require institutional care; however (7, 8), families often decide to keep the patient at home in LAC (17, 21). This may result from caregivers’ guilt or, more frequently, a lack of coverage by the healthcare system and the family’s inability to cover these expenses (17). In the terminal phase of dementia, palliative care may be helpful (38).
Disease-modifying AD treatments are currently being studied. More than 800 medications have been evaluated in clinical trials in recent years with negative results. This failure is mainly because they have been tested in the dementia stage, where the brain has suffered substantial damage, and it may be too late to obtain positive results. Recently, the strategy has begun to change, seeking to prevent or to clinical progression rather than cure the disease. LAC must prepare for the imminent paradigm shift for AD management from reactive treatment to prevention/disease modification.
Delaying the onset of AD symptoms by 5 years would reduce the prevalence and costs of the disease by 50% (128). Tertiary prevention consists of treating symptomatic people with MCI to avoid progression into dementia. Secondary prevention consists of treating asymptomatic people with neuropathological alterations of AD to prevent progression to MCI and, ultimately, to dementia. Primary prevention consists of treating asymptomatic people without neuropathological disease changes to avoid or delay it. In tertiary prevention, various anti-amyloid agents have been unsuccessful at slowing cognitive decline despite demonstrating biological improvement (129). Some anti-amyloid agents are evaluated in secondary prevention research, while primary prevention studies are planned for clinical trials. Lecanemab was associated with less cognitive and functional decline than placebo at 18 months in patients with MCI and mild dementia due to AD but was related to adverse events (130). Of note, the clinical significance of this change has been questioned (130). The drug has been recently approved for clinical use by the United States Food and Drug Administration and raises expectations for treating AD in its early stages. However, its prescription should still be limited to tertiary care centers, and its effect to be proven in clinical practice. The United States Food and Drug Administration has also approved Aducanumab. It has demonstrated biological but not clinical efficacy (131).
New alternatives with anti-tau, anti-inflammatory medicines, and combined treatments are also under development. However, in current clinical practice, only symptomatic treatment can be offered to patients with dementia, and tertiary prevention treatments to patients with MCI to prevent progression to dementia. Additionally, current research indicates that an anti-amyloid alone will not be enough to treat or prevent Alzheimer’s.
An understanding of AD genetics is necessary to understand potential future treatment targets. In this sense, there are two main variants of AD: familial AD, which has an autosomal dominant inheritance pattern and manifests early, before the age of 65, and sporadic AD, which is polygenic with a complex pattern of inheritance of susceptibility genes and is characterized by its late onset, after age 65.
Approximately 1–2% of AD cases are familial with Mendelian inheritance. The genes involved in the autosomal dominant familial pattern are known as causative genes because the carriers of some of these gene mutations have a 100% risk of developing the disease, given that these mutations have 100% penetrance. In the sporadic form, many susceptibility genes exist, which do not cause the disease but contribute to its risk. Systematic meta-analysis suggests that at least 20 loci have modest but significant effects on AD risk. The presence of APOE allele e4 is the most significant genetic risk factor in sporadic AD. Carriers of the e4 allele have a three to tenfold increased chance of developing AD. Other relevant susceptibility genes are clusterin (CLU), also known as APOJ, PICALM, TOMM40, CR1, and LRP1 (132).
Autosomal dominant forms of AD are most frequently caused by mutations in the PS1 gene (133). Through monitoring the population with the Paisa mutation (E280A in PS1) in Colombia, it has been possible to describe the pre-dementia stages of AD and its ages of onset. Moreover, it enabled the identification of a woman who carried both a causative mutation for AD and a protective mutation, delaying the onset of the disease for almost three decades. This patient, as a carrier of mutation E280A in PS1, would typically be condemned to the onset of symptoms of memory loss at the age of 44; however, she was homozygote for the Christchurch mutation (R136S) in APOE3, which caused the onset of MCI to be delayed to age 72. She had massive amyloidosis, low levels of tauopathy, and mild neurodegeneration. The effect of the protector mutation in weakening the ApoE-HSPG bond and reducing the dissemination of the tau protein could have therapeutic potential (9, 134).
We characterized the world’s second case with ascertained extreme resilience to autosomal dominant Alzheimer’s disease (ADAD). It was a man that remained cognitively intact until 70 years of age despite carrying a PSEN1-E280A mutation. Like the APOECh carrier, he had an extremely elevated amyloid plaque burden and limited entorhinal tau tangle burden. He did not carry the APOECh variant but was heterozygous for a rare variant in RELN (H3447R, termed Reelin-COLBOS). RELN-COLBOS is a gain-of-function variant that reduced human Tau phosphorylation in a knockin mouse. This genetic variant in a case protected from ADAD suggests a role for RELN signaling in resilience to dementia (135).
Box 1. The three types of genetic biomarkers related to AD.
Causation Biomarkers: Mutations in PPA, PS1, and PS2 that cause familial AD with early-onset before age 65, with an autosomal dominant Mendelian inheritance pattern.
Susceptibility Biomarkers: A range of genes or genetic variants confer susceptibility but do not cause the disease. The most important of these include the e4 variant of APOE and TREM2.
Protective Genetic Biomarkers: Genes or variants that have a protective effect, preventing or delaying disease onset. Includes the e2 variant of APOE (136), mutation A673T in PPA (137), the Christchurch mutation (R136S) in ApoE3 (138), the V236E variant in 22 APOE 3, and the R251G variant in APOE 4 (139). Reelin-Colbos mutation (H3447R) (135).
Summarizes causation, susceptibility, and protective biomarkers.
The AT (N) research framework recognizes three general groups of biological markers of AD based on the nature of the pathological process measured by each of them: A–amyloid, T–tauopathy, and N–neurodegeneration (1).
Box 2. The three general groups of biological markers for AD.
Biomarkers of cerebral amyloidosis (A): Amyloid-PET is a direct imaging biomarker of the presence of amyloid in the cerebral parenchyma, while the level of Aß-42 or the Aß-42/Aß-40 ratio in CSF is an indirect biochemical marker of the presence of Aß-42 deposits in the brain.
Biomarkers of cerebral tauopathy (T): Direct imaging method is PET-tau, which is a direct imaging biomarker of the presence of tauopathy in the brain. An indirect method is the level of phosphorylated tau (p-TAU) in the CSF. Plasma levels of p-tau217 and p-tau181 appear to have a promising future as low-cost and easy-to-access biochemical markers of tauopathy associated with AD (140).
Biomarkers of neurodegeneration (N): Brain MRI–direct imaging indicator of the degree of neurodegeneration and cerebral atrophy, measurable by cortical and hippocampal volumetry. PET with fluorodeoxyglucose (FDG) is a direct imaging biomarker of cerebral metabolism and an indirect, non-specific marker of neurodegeneration.
The exact alteration times of the different biomarkers in sporadic Alzheimer’s are not known, but in the autosomal dominant familial form with the E280A mutation in PS1 it has been discovered that carriers of the Paisa mutation show high levels of biomarkers such as ß42 in cerebrospinal fluid, NFL and phTAU in plasma at 24, 20 years before the first symptoms of Mild Cognitive Impairment. Additionally, neuroimaging studies have revealed that these individuals showed PET-amyloid positivity at 28 and pTAU positivity 10 years later at 38. Biomarkers of amyloidosis do not correlate well with alterations in cognition, but Imaging biomarkers of tauopathy and neurodegeneration correlate well with the onset of subjective memory complaints at 38 and later with mild cognitive impairment at 44 ad dementia at 49. Regarding cognitive markers, decreased performance in the word-list test of CERAD battery around 32 years is the earliest sign of cognitive decline. Currently, new research using digital neuropsychology tools aims to investigate the suitability of performance in spatial navigation tasks as cognitive markers since the preclinical stage of AD. This information is crucial for designing primary and secondary prevention clinical trials for Alzheimer’s.
To achieve a biological diagnosis of AD, it is necessary to demonstrate alterations in at least the biomarkers “A” and “T.” A person with abnormal changes in the biomarker “A” with normal “T” biomarkers cannot be diagnosed with AD but is said to have “pathological alterations of Alzheimer’s.” Nonetheless, “pathological alterations of Alzheimer’s” and “AD” represent phases on the same Alzheimer’s continuum. The “A” biological markers determine whether an individual is on the AD continuum. The “T” biological markers determine whether someone on the AD continuum has a neuropathological disease diagnosis. And the “N” biomarkers reflect the degree of atrophy from the clinical syndrome. Biomarkers and the ATN biological classification are primarily used to increase diagnostic accuracy (141). The AT(N) framework guides research on AD toward personalized medicine and allows for flexibility in the future regarding the addition of other biomarkers that may be discovered and validated.
LAC faces diverse challenges in the fight against AD. Regulatory entities and governments must encourage and facilitate global and regional AD research participation. Increased education and awareness efforts among the general population must be undertaken to dispel myths about memory loss. Creating public healthcare strategies to control modifiable risk factors for neurodegeneration and dementia syndrome in LAC could prevent up to 56% of dementia cases (19). Additionally, training at the primary care level is necessary to improve early AD detection and increase adequate referral situations. Because of the diverse populations in LAC, countries should have cognitive tests validated for their local context. A harmonized diagnostic approach using validated BCTs would increase early AD detection and provide the basis for research collaboration and standardized data generation throughout the region.
The financial burden of the direct and indirect costs related to AD care in LA are currently borne primarily by the families, exacerbated by minimal coverage of cognitive-enhancing medication through the public healthcare systems. Without access to improved treatments and preventive therapy, the adverse repercussions of AD will continue to impact LAC people, healthcare systems, and economies. Given that currently available biomarkers entail high costs and invasive procedures, there is an unmet need for peripheral biomarkers (plasma, saliva, tears, urine, fecal matter) for AD diagnosis that would provide a more accessible alternative to LAC economies and set the stage for prevention.
The high prevalence of genetic AD in Colombia and several other LAC countries suggests a similar situation throughout the region, necessitating dedicated search strategies for populations with genetic AD variants. Consequently, LAC has the potential to play an essential role in the future of primary and secondary prevention for AD.
We hope this document will be a tool to improve the expertise and professionalism of health professionals and thus optimize the individual care of people with AD and their families. And, importantly, it also equips professionals to be leaders in transforming health services in LAC countries (142, 143).
FL, NC, RA, JB, EG, CC, AM, and SB: writing—original draft, investigation, formal analysis, and validation. AJ: writing—review and editing, methodology, and project administration. MR-R: writing—review and editing, visualization, conceptualization, methodology, and project administration. IC, PC, JD, RN, JP, CR, and AS: writing—review and editing, visualization, formal analysis, and validation.
The organization and implementation of the consensus conference were carried out by the AHF, a 501(c)3 nonprofit organization dedicated to improving healthcare throughout the Latin American Region and was supported by an unrestricted grant from Adium. The funder had no influence on the design, implementation, and content of this manuscript.
The authors would like to thank Ms. Thais Vidal, BA, for her assistance in language-editing the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Parra, MA, Baez, S, Allegri, R, Nitrini, R, Lopera, F, Slachevsky, A, et al. Dementia in Latin America: assessing the present and envisioning the future. Neurology. (2018) 90:222–31. doi: 10.1212/WNL.0000000000004897
2. Custodio, N, Wheelock, A, Thumala, D, and Slachevsky, A. Dementia in Latin America: epidemiological evidence and implications for public policy. Front Aging Neurosci. (2017) 9:221. doi: 10.3389/fnagi.2017.00221
3. Nitrini, R, Bottino, CMC, Albala, C, Capuñay, NSC, Ketzoian, C, Rodriguez, JJL, et al. Prevalence of dementia in Latin America: a collaborative study of population-based cohorts. Int Psychogeriatr. (2009) 21:622–30. doi: 10.1017/S1041610209009430
4. Suemoto, CK, Ferretti-Rebustini, REL, Rodriguez, RD, Leite, REP, Soterio, L, Brucki, SMD, et al. Neuropathological diagnoses and clinical correlates in older adults in Brazil: a cross-sectional study. PLoS Med. (2017) 14:e1002267. doi: 10.1371/journal.pmed.1002267
5. Parra, MA, Orellana, P, Leon, T, Victoria, CG, Henriquez, F, Gomez, R, et al. Biomarkers for dementia in Latin American countries: gaps and opportunities. Alzheimers Dement. (2023) 19:721–35. doi: 10.1002/alz.12757
6. Lancet Neurology . A neurology revival in Latin America. Lancet Neurol. (2015) 14:1143. doi: 10.1016/S1474-4422(15)00307-5
7. Nitrini, R, Caramelli, P, Herrera, E, Bahia, VS, Caixeta, LF, Radanovic, M, et al. Incidence of dementia in a community-dwelling Brazilian population. Alzheimer Dis Assoc Disord. (2004) 18:241–6.
8. Ribeiro, F, Teixeira-Santos, AC, Caramelli, P, and Leist, AK. Prevalence of dementia in Latin America and Caribbean countries: systematic review and meta-analyses exploring age, sex, rurality, and education as possible determinants. Ageing Res Rev. (2022) 81:101703. doi: 10.1016/j.arr.2022.101703
9. Nichols, E, Szoeke, CEI, Vollset, SE, Abbasi, N, Abd-Allah, F, Abdela, J, et al. Global, regional, and national burden of Alzheimer's disease and other dementias, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:88–106. doi: 10.1016/S1474-4422(18)30403-4
10. Russ, TC, Murianni, L, Icaza, G, Slachevsky, A, and Starr, JM. Geographical variation in dementia mortality in Italy, New Zealand, and Chile: the impact of latitude, vitamin D, and air pollution. Dement Geriatr Cogn Disord. (2016) 42:31–41. doi: 10.1159/000447449
11. Parra, MA, Baez, S, Sedeño, L, Gonzalez Campo, C, Santamaría-García, H, Aprahamian, I, et al. Dementia in Latin America: paving the way toward a regional action plan. Alzheimers Dement. (2021) 17:295–313. doi: 10.1002/alz.12202
12. Zitko, P, Slachevsky, A, and Jimenez, D. The prevalence, associated factors, and the burden on health state utilities for dementia in Chile. Alzheimers Dement. (2020) 16:e042466. doi: 10.1002/alz.042466
13. Lang, L, Clifford, A, Wei, L, Zhang, D, Leung, D, Augustine, G, et al. Prevalence and determinants of undetected dementia in the community: a systematic literature review and a meta-analysis. BMJ Open. (2017) 7:e011146. doi: 10.1136/bmjopen-2016-011146
14. Filshtein, T, Beckett, LA, Godwind, H, Hinton, L, and Xiong, GL. Incident antipsychotic use in a diverse population with dementia. J Am Geriatr Soc. (2016) 64:e44:–e46. doi: 10.1111/jgs.14209
15. Alva-Dìaz, C, Malaga, M, Rodriguez-Calienes, A, Morán-Mariños, C, Velásquez-Rimachi, V, and Custodio, N. Costs related to frontotemporal dementia in Latin America: a scoping review of economic health studies. Front Neurol. (2021) 12:1273. doi: 10.3389/fneur.2021.684850
16. Hojman, D, Duarte, F, Ruiz-Tagle, J, Budnich, M, Delgado, C, and Slachevsky, A. The cost of dementia in an unequal country: the case of Chile. PLoS One. (2017) 12:e0172204. doi: 10.1371/journal.pone.0172204
17. Suemoto, CK, Mukadam, N, Brucki, SMD, Caramelli, P, Nitrini, R, Laks, J, et al. Risk factors for dementia in Brazil: differences by region and race. Alzheimers Dement. (2022) 19:1849–57. doi: 10.1002/alz.12820
18. Vergara, RC, Zitko, P, Slachevsky, A, San Martin, C, and Delgado, C. Population attributable fraction of modifiable risk factors for dementia in Chile. Alzheimers Dement (Amst). (2022) 14:e12273. doi: 10.1002/dad2.12273
19. Livingston, G, Huntley, J, Sommerlad, A, Ames, D, Ballard, C, Banerjee, S, et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet. (2020) 396:413–46. doi: 10.1016/S0140-6736(20)30367-6
20. Mukadam, N, Sommerlad, A, Huntley, J, and Livingston, G. Population attributable fractions for risk factors for dementia in low-income and middle-income countries: an analysis using cross-sectional survey data. Lancet Glob Health. (2019) 7:e596–603. doi: 10.1016/S2214-109X(19)30074-9
21. Allegri, RF, Bagnati, P, Brucki, S, and Nitrini, R. South America’s AD clinical trials experience: lessons learned from Argentina and Brazil In: M Bairu and MW Weiner, editors. Global clinical trials for Alzheimer's disease. San Diego: Academic Press (2014). 219–30.
22. Kivipelto, M, Mangialasche, F, Snyder, HM, Allegri, R, Andrieu, S, Arai, H, et al. World-wide FINGERS network: a global approach to risk reduction and prevention of dementia. Alzheimers Dement. (2020) 16:1078–94. doi: 10.1002/alz.12123
23. World Health Organization . Alzheimer’s disease international. Dementia: a public health priority. Geneva: World Health Organization (2012). 112 p.
24. Wahlund, LO . Magnetic resonance imaging and computed tomography in Alzheimer's disease. Acta Neurol Scand. (1996) 168:50–3. doi: 10.1111/j.1600-0404.1996.tb00373.x
25. Serrano, RA, and Lopez-Pousa, S. Enfermedad de Alzheimer y otras demencias. 3rd ed. Mexico: Editorial medica Panamericana (2007).
26. Allegri, RF, Arizaga, RL, Bavec, CV, Colli, LP, Demey, I, Fernández, MC, et al. Enfermedad de Alzheimer. Guía Práct Clín Neurol Argent. (2011) 3:120–37. doi: 10.1016/S1853-0028(11)70026-X
27. Brucki, SMD, Aprahamian, I, Borelli, WV, Da Silveira, VC, Ferretti, CEL, Smid, J, et al. Management in severe dementia: recommendations of the scientific Department of Cognitive Neurology and Aging of the Brazilian academy of neurology. Dement Neuropsychol. (2022) 16:101–20. doi: 10.1590/1980-5764-DN-2022-S107PT
28. Chile Ministry of Health . Problema de Salud AUGE N°85: Demencia tipo Alzheimer. Chile: Chile Ministry of Health (2023).
29. Behrens, MI, and Slachevsky, A. Guías clínicas de diagnóstico y tratamiento de las demencias. Rev Chil Neuropsiquiatr. (2007) 45:189–90.
30. Ministerio de Salud y Protección Social Instituto de Evaluación Tecnológica en Salud . Guía de Práctica Clínica para el diagnóstico y tratamiento del trastorno neurocognoscitivo mayor (Demencia) (Adopción). (2017) Available at: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/INEC/IETS/gpc-demencia-completa.pdf.
31. Instituto Mexicano del Seguro Social . Diagnostico y Tratamiento de la Enfermedad de Alzheimer: Evidencias y Recomendaciones (2017). Available at: https://www.imss.gob.mx/sites/all/statics/guiasclinicas/393GER.pdf. (Accessed February 22, 2023).
32. Prince, MJ, Comas-Herrera, A, Knapp, M, Guerchet, MM, and Karagiannidou, M. World Alzheimer report 2016-improving healthcare for people living with dementia: Coverage, quality and costs now and in the future. London: Alzheimer’s Disease International (2016).
33. Peru Minister of Health . DEMENCIA TIPO ALZHEIMER: Código CIE-10: F 00. Available at: http://diresacusco.gob.pe/salud_individual/servicios/Gu%C3%ADas%20de%20Pr%C3%A1ctica%20Cl%C3%ADnica%20MINSA/Propuestas%20previas%20de%20GPC/Gu%C3%ADas%20Pr%C3%A1cticas%20Cl%C3%ADnicas%20en%20Neurolog%C3%ADa/guia.Alzheimer.pdf. (Accessed February 22, 2023).
34. Custodio, N, Duque, L, Montesinos, R, Alva-Diaz, C, Mellado, M, and Slachevsky, A. Systematic review of the diagnostic validity of brief cognitive screenings for early dementia detection in Spanish-speaking adults in Latin America. Front Aging Neurosci. (2020) 12:12. doi: 10.3389/fnagi.2020.00270
35. Custodio, N, Montesinos, R, Lira, D, Herrera-Perez, E, Chavez, K, Reynoso-Guzman, W, et al. Validation of the RUDAS for the identification of dementia in illiterate and low-educated older adults in Lima, Peru. Front Neurol. (2020) 11:11. doi: 10.3389/fneur.2020.00374
36. Ortega, LV, Aprahamian, I, Martinelli, JE, Cecchini, MA, Cação, JC, and Yassuda, MS. Diagnostic accuracy of usual cognitive screening tests versus appropriate tests for lower education to identify Alzheimer disease. J Geriatr Psychiatry Neurol. (2020) 34:891988720958542:222–31. doi: 10.1177/0891988720958542
37. Peles, PRH, de Souza, SL, de Souza, LC, and Caramelli, P. Accuracy of the brief cognitive screening battery for diagnosing Alzheimer's disease defined by cerebrospinal fluid biomarkers and AT (N) classification: a case-control study. Arq Neuropsiquiatr. (2022) 80:23–9. doi: 10.1590/0004-282x-anp-2021-0012
38. Quiroga, P, Albala, C, and Klaasen, G. Validación de un test de tamizaje para el diagnóstico de demencia asociada a edad, en Chile. Rev Med Chil. (2004) 132:467–78. doi: 10.4067/S0034-98872004000400009
39. Bradford, A, Kunik, ME, Schulz, P, Williams, SP, and Singh, H. Missed and delayed diagnosis of dementia in primary care: prevalence and contributing factors. Alzheimer Dis Assoc Disord. (2009) 23:306–14. doi: 10.1097/WAD.0b013e3181a6bebc
40. Massa, A, and Choncho, A. Decision making and consents given by demented patients. Are they valid? Rev Méd Chile. (2017) 145:1312–8. doi: 10.4067/S0034-98872017001001312
41. Nitrini, R, Brucki, SMD, Yassuda, MS, Fichman, HC, and Caramelli, P. The figure memory test: diagnosis of memory impairment in populations with heterogeneous educational background. Dement Neuropsychol. (2021) 15:173–85. doi: 10.1590/1980-57642021dn15-020004
42. Kerwin, D, Abdelnour, C, Caramelli, P, Ogunniyi, A, Shi, J, Zetterberg, H, et al. Alzheimer's disease diagnosis and management: perspectives from around the world. Alzheimers Dement. (2022) 14:e12334. doi: 10.1002/dad2.12334
43. Rabins, PV, Rovner, BW, Rummans, T, Schneider, LS, and Tariot, PN. Guideline watch (October 2014): practice guideline for the treatment of patients with Alzheimer's disease and other dementias. Focus. (2017) 15:110–28. doi: 10.1176/appi.focus.15106
44. Hort, J, O’Brien, JT, Gainotti, G, Pirttila, T, Popescu, BO, Rektorova, I, et al. EFNS scientist panel on dementia. EFNS guidelines for the diagnosis and management of Alzheimer’s disease. Eur J Neurol. (2010) 17:1236–48. doi: 10.1111/j.1468-1331.2010.03040.x
45. Filippi, M, Agosta, F, Barkhof, F, Dubois, B, Fox, NC, Frisoni, GB, et al. EFNS task force: the use of neuroimaging in the diagnosis of dementia. Eur J Neurol. (2012) 19:e131-40–1487-501. doi: 10.1111/j.1468-1331.2012.03859.x
46. Jack, CR Jr, Bennett, DA, Blennow, K, Carrillo, MC, Dunn, B, Haeberlein, SB, et al. NIA-AA research framework: toward a biological definition of Alzheimer's disease. Alzheimers Dement. (2018) 14:535–62. doi: 10.1016/j.jalz.2018.02.018
47. Acosta-Baena, N, Sepulveda-Falla, D, Lopera-Gómez, CM, Jaramillo-Elorza, MC, Moreno, S, Aguirre-Acevedo, DC, et al. Pre-dementia clinical stages in presenilin 1 E280A familial early-onset Alzheimer's disease: a retrospective cohort study. Lancet Neurol. (2011) 10:213–20. doi: 10.1016/S1474-4422(10)70323-9
48. Aguirre-Acevedo, DC, Lopera, F, Henao, E, Tirado, V, Muñoz, C, Giraldo, M, et al. Cognitive decline in a Colombian kindred with autosomal dominant Alzheimer disease: a retrospective cohort study. JAMA Neurol. (2016) 73:431–8. doi: 10.1001/jamaneurol.2015.4851
49. López-Álvarez, J, and Agüera-Ortiz, LF. Nuevos criterios diagnósticos de la demencia y la enfermedad de Alzheimer: una visión desde la psicogeriatría. Psicogeriatría. (2015) 5:3–14.
50. Robert, P, Ferris, S, Gauthier, S, Ihl, R, Winblad, B, and Tennigkeit, F. Review of Alzheimer's disease scales: is there a need for a new multi-domain scale for therapy evaluation in medical practice? Alzheimers Res Ther. (2010) 2:24–13. doi: 10.1186/alzrt48
51. Zucchella, C, Sinforiani, E, Tamburin, S, Federico, A, Mantovani, E, Bernini, S, et al. The multidisciplinary approach to Alzheimer's disease and dementia. A narrative review of non-pharmacological treatment. Front Neurol. (2018) 9:1058. doi: 10.3389/fneur.2018.01058
52. Aravena, JM, Gajardo, J, Saguez, R, Hinton, L, and Gitlin, LN. Nonpharmacologic interventions for family caregivers of people living with dementia in Latin-America: a scoping review. Am J Geriatr Psychiatry. (2022) 30:859–77. doi: 10.1016/j.jagp.2021.10.013
53. De Oliveira, SF, Ferreira, JV, Plácido, J, Sant'Anna, P, Araújo, J, Marinho, V, et al. Three months of multimodal training contributes to mobility and executive function in elderly individuals with mild cognitive impairment, but not in those with Alzheimer's disease: a randomized controlled trial. Maturitas. (2019) 126:28–33. doi: 10.1016/j.maturitas.2019.04.217
54. Ramirez-Gomez, L, Johnson, JK, Ritchie, C, Meyer, AK, Tan, E, Madarasmi, S, et al. Virtual mentalizing imagery therapy for Spanish language Latino family dementia caregivers: a feasibility and acceptability study. Front Psychol. (2023) 14:961835. doi: 10.3389/fpsyg.2023.961835
55. Abraha, I, Rimland, JM, Trotta, FM, Dell'Aquila, G, Cruz-Jentoft, A, Petrovic, M, et al. Systematic review of systematic reviews of non-pharmacological interventions to treat behavioural disturbances in older patients with dementia. The SENATOR-OnTop series. BMJ Open. (2017) 7:e012759. doi: 10.1136/bmjopen-2016-012759
56. Krivanek, TJ, Gale, SA, McFeeley, BM, Nicastri, CM, and Daffner, KR. Promoting successful cognitive aging: a ten-year update. J Alzheimers Dis. (2021) 81:871–920. doi: 10.3233/JAD-201462
57. Lamb, SE, Sheehan, B, Atherton, N, Nichols, V, Collins, H, Mistry, D, et al. Dementia and physical activity (DAPA) trial of moderate to high intensity exercise training for people with dementia: randomised controlled trial. BMJ. (2018) 361:k1675. doi: 10.1136/bmj.k1675
58. Xue, B, Waseem, SMA, Zhu, Z, Alshahrani, MA, Nazam, N, Anjum, F, et al. Brain-derived neurotrophic factor: a connecting link between nutrition, lifestyle, and Alzheimer's disease. Front Neurosci. (2022) 16:925991. doi: 10.3389/fnins.2022.925991
59. Hu, S, Wan, X, Li, X, and Wang, X. Aerobic exercise alleviates pyroptosis-related diseases by regulating NLRP3 inflammasome. Front Physiol. (2022) 13:965366. doi: 10.3389/fphys.2022.965366
60. Giménez-Llort, L, Rivera-Hernández, G, Marin-Argany, M, Sánchez-Quesada, JL, and Villegas, S. Early intervention in the 3xTg-AD mice with an amyloid β-antibody fragment ameliorates first hallmarks of Alzheimer disease. MAbs. (2013) 5:665–864. doi: 10.4161/mabs.25424
61. Xu, L, Li, M, Wei, A, Yang, M, Li, C, Liu, R, et al. Treadmill exercise promotes E3 ubiquitin ligase to remove amyloid β and P-tau and improve cognitive ability in APP/PS1 transgenic mice. J Neuroinflammation. (2022) 19:243. doi: 10.1186/s12974-022-02607-7
62. Luo, G, Zhang, J, Song, Z, Wang, Y, Wang, X, Qu, H, et al. Effectiveness of non-pharmacological therapies on cognitive function in patients with dementia-a network meta-analysis of randomized controlled trials. Front Aging Neurosci. (2023) 15:1131744. doi: 10.3389/fnagi.2023.1131744
63. Dutzi, I, Schwenk, M, Kirchner, M, Bauer, JM, and Hauer, K. "what would you like to achieve?" goal-setting in patients with dementia in geriatric rehabilitation. BMC Geriatr. (2019) 19:280. doi: 10.1186/s12877-019-1296-7
64. Bahar-Fuchs, A, Martyr, A, Goh, AMY, Sabates, J, and Clare, L. Cognitive training for people with mild to moderate dementia. Cochrane Database Syst Rev. (2019):CD013069. doi: 10.1002/14651858.CD013069.pub2
65. Perkins, L, Fisher, E, Felstead, C, Rooney, C, Wong, GHY, Dai, R, et al. Delivering cognitive stimulation therapy (CST) virtually: developing and field-testing a new framework. Clin Interv Aging. (2022) 17:97–116. doi: 10.2147/CIA.S348906
66. Chen, X . Effectiveness of cognitive stimulation therapy (CST) on cognition, quality of life and neuropsychiatric symptoms for patients living with dementia: a meta-analysis. Geriatr Nurs. (2022) 47:201–10. doi: 10.1016/j.gerinurse.2022.07.012
67. Gubert, C, and Hannan, AJ. Exercise mimetics: harnessing the therapeutic effects of physical activity. Nat Rev Drug Discov. (2021) 20:862–79. doi: 10.1038/s41573-021-00217-1
68. Chalfont, G, Milligan, C, and Simpson, J. A mixed methods systematic review of multimodal non-pharmacological interventions to improve cognition for people with dementia. Dementia. (2020) 19:1086–130. doi: 10.1177/1471301218795289
69. Forbes, D, Forbes, SC, Blake, CM, Thiessen, EJ, and Forbes, S. Exercise programs for people with dementia. Cochrane Database Syst Rev. (2015) 2015:CD006489. doi: 10.1002/14651858.CD006489.pub4
72. Patch, E . Rivastigmine transdermal system [Package insert]. Basel, Switzerland: Novartis (2000).
75. Argentina government . How to obtain the single disability certivcate (CUD). Available at: https://www.argentina.gob.ar/servicio/como-obtener-el-certificado-unico-de-discapacidad-cud.
76. The National Institute of social Services for Retirees and Pensioners. Available at: https://www.pami.org.ar/tramite/medicamentos-discapacidad. (Accessed February 27, 2023).
77. Bernabei, R, and Martínez-Lage, P. Clinical benefits associated with a transdermal patch for dementia. Eur Neurol Rev. (2008) 3:10. doi: 10.17925/ENR.2008.03.01.10
78. Dhillon, S . Rivastigmine transdermal Patch. Drugs. (2011) 71:1209–31. doi: 10.2165/11206380-000000000-00000
79. Lundy, J, Hayden, D, Pyland, S, Berg-Weger, M, Malmstrom, TK, and Morley, JE. An age-friendly health system. J Am Geriatr Soc. (2021) 69:806–12. doi: 10.1111/jgs.16959
80. Improvement IfH . Age-friendly health systems: Guide to using the 4Ms in the Care of Older Adults 2020. Available at: https://www.ihi.org/Engage/Initiatives/Age-Friendly-Health-Systems/Documents/IHIAgeFriendlyHealthSystems_GuidetoUsing4MsCare.pdf. (Accessed February 22, 2023).
81. World Health Organization . Informe Mundial Sobre Envejecimiento y Salud. (2015). Available at: http://apps.who.int/iris/bitstream/10665/186471/1/WHO_FWC_ALC_15.01_spa.pdf.nih.gov/pubmed/15003161%5Cn.
82. Sandival Ampuero, G, Runzer-Colmenares, F, and Parodi, J. La valoración funcional como predictor de deterioro cognitivo: cohorte retrospectiva. Medwave. (2017) 17:e7099. doi: 10.5867/medwave.2017.09.7099
83. Parodi, J, Nieto-Gutierrez, W, Tellez, W, Ventocilla-Gonzales, I, Runzer-Colmenares, F, and Taype-Rondan, A. Gait speed and the appearance of neurocognitive disorders in older adults: results of a Peruvian cohort. Esp Geriatr Gerontol. (2018) 53:73–6. doi: 10.1016/j.regg.2017.08.001
84. Aguilar-Navarro, SG, Mimenza-Alvarado, AJ, Aguilar-Esquivel, JE, Yeverino-Castro, SG, Juárez-Cedillo, T, and Mejía-Arango, S. Motoric cognitive risk syndrome: prevalence and risk of cognitive impairment in a population studied in the Mexican health and aging study 2012-2015. J Nutr Health Aging. (2019) 23:227–31. doi: 10.1007/s12603-019-1160-7
85. Esteban-Cornejo, I, Cabanas-Sánchez, V, Higueras-Fresnillo, S, Ortega, FB, Kramer, AF, Rodriguez-Artalejo, F, et al. Cognitive frailty and mortality in a National Cohort of older adults: the role of physical activity. Mayo Clin Proc. (2019) 94:1180–9. doi: 10.1016/j.mayocp.2018.10.027
86. Varadaraj, V, Munoz, B, Deal, JA, An, Y, Albert, MS, Resnick, SM, et al. Association of Vision Impairment with Cognitive Decline across Multiple Domains in older adults. JAMA Netw Open. (2021) 4:e2117416. doi: 10.1001/jamanetworkopen.2021.17416
87. Wang, HF, Zhang, W, Rolls, ET, Li, Y, Wang, L, Ma, YH, et al. Hearing impairment is associated with cognitive decline, brain atrophy and tau pathology. EBioMedicine. (2022) 86:104336. doi: 10.1016/j.ebiom.2022.104336
88. Panza, F, Frisardi, V, Capurso, C, D'Introno, A, Colacicco, AM, Imbimbo, BP, et al. Late-life depression, mild cognitive impairment, and dementia: possible continuum? Am J Geriatr Psychiatry. (2010) 18:98–116. doi: 10.1097/JGP.0b013e3181b0fa13
89. Gutiérrez-Robledo, LM, García-Chanes, RE, and Pérez-Zepeda, MU. Allostatic load as a biological substrate to intrinsic capacity: a secondary analysis of CRELES. J Nutr Health Aging. (2019) 23:788–95. doi: 10.1007/s12603-019-1251-5
90. Pajuelo-Vasquez, R, Pajares-Ramirez, L, Gutierrez-Baca, W, Calderon-Ocon, V, Grande-Bernuy, M, Parodi, J, et al. Association between motoric cognitive risk syndrome and risk of mortality in older adults: results of a 5-year retrospective cohort. Ageing Int. (2022) 2022:9508. doi: 10.1007/s12126-022-09508-3
91. Yang, Q, Tian, C, Tseng, B, Zhang, B, Huang, S, Jin, S, et al. Gait change in dual task as a behavioral marker to detect mild cognitive impairment in elderly persons: a systematic review and Meta-analysis. Arch Phys Med Rehabil. (2020) 101:1813–21. doi: 10.1016/j.apmr.2020.05.020
92. Robledo, LMG, Cano-GutiéRrez, C, and Garcia, EV. Healthcare for older people in central and South America. Age Ageing. (2022) 51:afac017. doi: 10.1093/ageing/afac017
93. Hampel, H, Au, R, Mattke, S, van der Flier, WM, Aisen, P, Apostolova, L, et al. Designing the next-generation clinical care pathway for Alzheimer’s disease. Nat Aging. (2022) 2:692–703. doi: 10.1038/s43587-022-00269-x
94. Gillett, G . Advance decisions in dementia: when the past conflicts with the present. J Med Ethics. (2019) 45:204–8. doi: 10.1136/medethics-2018-104919
95. Doody, RS, Ferris, SH, Salloway, S, Sun, Y, Goldman, R, Watkins, WE, et al. Donepezil treatment of patients with MCI: a 48-week randomized, placebo-controlled trial. Neurology. (2009) 72:1555–61. doi: 10.1212/01.wnl.0000344650.95823.03
96. Petersen, RC, Thomas, RG, Grundman, M, Bennett, D, Doody, R, Ferris, S, et al. Vitamin E and donepezil for the treatment of mild cognitive impairment. N Engl J Med. (2005) 352:2379–88. doi: 10.1056/NEJMoa050151
97. Farina, N, Rusted, J, and Tabet, N. The effect of exercise interventions on cognitive outcome in Alzheimer's disease: a systematic review. Int Psychogeriatr. (2014) 26:9–18. doi: 10.1017/S1041610213001385
98. Larson, EB, Wang, L, Bowen, JD, McCormick, WC, Teri, L, Crane, P, et al. Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Ann Intern Med. (2006) 144:73–81. doi: 10.7326/0003-4819-144-2-200601170-00004
99. Hsu, WY, Ku, Y, Zanto, TP, and Gazzaley, A. Effects of noninvasive brain stimulation on cognitive function in healthy aging and Alzheimer's disease: a systematic review and meta-analysis. Neurobiol Aging. (2015) 36:2348–59. doi: 10.1016/j.neurobiolaging.2015.04.016
100. Birks, JS, and Harvey, RJ. Donepezil for dementia due to Alzheimer's disease. Cochrane Database Syst Rev. (2018) 6:Cd001190. doi: 10.1002/14651858.CD001190.pub3
101. Reisberg, B, Doody, R, Stöffler, A, Schmitt, F, Ferris, S, and Möbius, HJ. Memantine in moderate-to-severe Alzheimer's disease. N Engl J Med. (2003) 348:1333–41. doi: 10.1056/NEJMoa013128
102. Hébert, R, Dubois, M-F, Wolfson, C, Chambers, L, and Cohen, C. Factors associated with long-term institutionalization of older people with dementia: data from the Canadian study of health and aging. J Gerontol Ser A Biol Med Sci. (2001) 56:M693–9. doi: 10.1093/gerona/56.11.M693
103. Knopman, DS, Berg, JD, Thomas, R, Grundman, M, Thal, LJ, and Sano, M. Nursing home placement is related to dementia progression: experience from a clinical trial. Alzheimers Dis Coop Stud Neurol. (1999) 52:714–8. doi: 10.1212/WNL.52.4.714
104. Allegri, RF, Sarasola, D, Serrano, CM, Taragano, FE, Arizaga, RL, Butman, J, et al. Neuropsychiatric symptoms as a predictor of caregiver burden in Alzheimer’s disease. Neuropsychiatr Dis Treat. (2006) 2:105–10.
105. Group TDR . Care arrangements for people with dementia in developing countries. Int J Geriatr Psychiatry. (2004) 19:170–7. doi: 10.1002/gps.1046
106. Volkert, D, Beck, AM, Cederholm, T, Cruz-Jentoft, A, Hooper, L, Kiesswetter, E, et al. ESPEN practical guideline: clinical nutrition and hydration in geriatrics. Clin Nutr. (2022) 41:958–89. doi: 10.1016/j.clnu.2022.01.024
107. Arvanitakis, Z, Shah, RC, and Bennett, DA. Diagnosis and management of dementia. JAMA. (2019) 322:1589–99. doi: 10.1001/jama.2019.4782
108. Fazio, S, Pace, D, Maslow, K, Zimmerman, S, and Kallmyer, B. Alzheimer’s association dementia care practice recommendations. Oxford: Oxford University Press US, p. S1–S9. (2018).
109. Guidelines, N . Dementia: Assessment, management and support for people living with dementia and their carers. London: National Institute for Health and Care Excellence (NICE) (2018).
110. Ismail, Z, Black, SE, Camicioli, R, Chertkow, H, Herrmann, N, Laforce, R Jr, et al. Recommendations of the 5th Canadian consensus conference on the diagnosis and treatment of dementia. Alzheimers Dement. (2020) 16:1182–95. doi: 10.1002/alz.12105
111. Black, SE, Doody, R, Li, H, McRae, T, Jambor, KM, Xu, Y, et al. Donepezil preserves cognition and global function in patients with severe Alzheimer disease. Neurology. (2007) 69:459–69. doi: 10.1212/01.wnl.0000266627.96040.5a
112. Winblad, B, Kilander, L, Eriksson, S, Minthon, L, Båtsman, S, Wetterholm, AL, et al. Donepezil in patients with severe Alzheimer's disease: double-blind, parallel-group, placebo-controlled study. Lancet. (2006) 367:1057–65. doi: 10.1016/S0140-6736(06)68350-5
113. Winblad, B, and Poritis, N. Memantine in severe dementia: results of the 9M-best study (benefit and efficacy in severly demented patients during treatment with memantine). Int J Geriatr Psychiatry. (1999) 14:135–46. doi: 10.1002/(SICI)1099-1166(199902)14:2<135::AID-GPS906>3.0.CO;2-0
114. Allegri, RF, Butman, J, Arizaga, RL, Machnicki, G, Serrano, C, Taragano, FE, et al. Economic impact of dementia in developing countries: an evaluation of costs of Alzheimer-type dementia in Argentina. Int Psychogeriatr. (2007) 19:705–18. doi: 10.1017/S1041610206003784
115. Rojas, G, Bartoloni, L, Dillon, C, Serrano, CM, Iturry, M, and Allegri, RF. Clinical and economic characteristics associated with direct costs of Alzheimer's, frontotemporal and vascular dementia in Argentina. Int Psychogeriatr. (2011) 23:554–61. doi: 10.1017/S1041610210002012
116. McShane, R, Westby, MJ, Roberts, E, Minakaran, N, Schneider, L, Farrimond, LE, et al. Memantine for dementia. Cochrane Database Syst Rev. (2019) 3:CD003154. doi: 10.1002/14651858.CD003154.pub6
117. Lopez, OL, Becker, JT, Wahed, AS, Saxton, J, Sweet, RA, Wolk, DA, et al. Long-term effects of the concomitant use of memantine with cholinesterase inhibition in Alzheimer disease. J Neurol Neurosurg Psychiatry. (2009) 80:600–7. doi: 10.1136/jnnp.2008.158964
118. Parsons, C, Lim, WY, Loy, C, McGuinness, B, Passmore, P, Ward, SA, et al. Withdrawal or continuation of cholinesterase inhibitors or memantine or both, in people with dementia. Cochrane Database Syst Rev. (2021) 2:CD009081. doi: 10.1002/14651858.CD009081.pub2
119. NCCfMH . Dementia: A NICE-SCIE guideline on supporting people with dementia and their Cares in health and social care. Leicester (UK): British Psychological Society (UK) (2007).
120. Waldemar, G, Dubois, B, Emre, M, Georges, J, McKeith, IG, Rossor, M, et al. Recommendations for the diagnosis and management of Alzheimer's disease and other disorders associated with dementia: EFNS guideline. Eur J Neurol. (2007) 14:e1–e26. doi: 10.1111/j.1468-1331.2006.01605.x
121. Reus, VI, Fochtmann, LJ, Eyler, AE, Hilty, DM, Horvitz-Lennon, M, Jibson, MD, et al. The American Psychiatric Association practice guideline on the use of antipsychotics to treat agitation or psychosis in patients with dementia. Am J Psychiatr. (2016) 173:543–6. doi: 10.1176/appi.ajp.2015.173501
122. Herrmann, N, and Lanctôt, KL. Do atypical antipsychotics cause stroke? CNS Drugs. (2005) 19:91–103. doi: 10.2165/00023210-200519020-00001
123. Wooltorton, E . Risperidone (Risperdal): increased rate of cerebrovascular events in dementia trials. CMAJ. (2002) 167:1269–70.
124. Pazan, F, Petrovic, M, Cherubini, A, Onder, G, Cruz-Jentoft, AJ, Denkinger, M, et al. Current evidence on the impact of medication optimization or pharmacological interventions on frailty or aspects of frailty: a systematic review of randomized controlled trials. Eur J Clin Pharmacol. (2021) 77:1–12. doi: 10.1007/s00228-020-02951-8
125. Appleby, J . Improper use of prescription drugs cost $200 billion a year, report finds. Kaiser Heal News. (2013).
126. PAHO . Portfolio: Evidence-based programs for a person-centered, integrated Care for Older People at the primary healthcare level. Washington, DC: PAHO (2013).
128. Zissimopoulos, J, Crimmins, E, and St, CP. The value of delaying Alzheimer's disease onset. Forum Health Econ Policy. (2014) 18:25–39. doi: 10.1515/fhep-2014-0013
129. Joe, E, and Ringman, JM. Cognitive symptoms of Alzheimer's disease: clinical management and prevention. BMJ. (2019) 367:l6217. doi: 10.1136/bmj.l6217
130. van Dyck, CH, Swanson, CJ, Aisen, P, Bateman, RJ, Chen, C, Gee, M, et al. Lecanemab in early Alzheimer’s disease. N Engl J Med. (2022) 388:9–21. doi: 10.1056/NEJMoa2212948
131. Synnott, PG, Whittington, MD, Lin, GA, Rind, DM, and Pearson, SD. The effectiveness and value of aducanumab for Alzheimer’s disease. J Manag Care Spec Pharm. (2021) 27:1613–7. doi: 10.18553/jmcp.2021.27.11.1613
132. Kunkle, BA-O, Grenier-Boley, B, Sims, R, Bis, JC, Damotte, V, Naj, AC, et al. Genetic meta-analysis of diagnosed Alzheimer's disease identifies new risk loci and implicates Aβ, tau, immunity and lipid processing. Nat Genet. (2019) 51:414–30. doi: 10.1038/s41588-019-0358-2
133. Cacace, R, Sleegers, K, and Van Broeckhoven, C. Molecular genetics of early-onset Alzheimer's disease revisited. Alzheimers Dement. (2016) 12:733–48. doi: 10.1016/j.jalz.2016.01.012
134. Sepulveda-Falla, D, Sanchez, JS, Almeida, MC, Boassa, D, Acosta-Uribe, J, Vila-Castelar, C, et al. Distinct tau neuropathology and cellular profiles of an APOE3 Christchurch homozygote protected against autosomal dominant Alzheimer’s dementia. Acta Neuropathol. (2022) 144:589–601. doi: 10.1007/s00401-022-02467-8
135. Lopera, F, Marino, C, Chandrahas, AS, O’Hare, M, Villalba-Moreno, ND, Aguillon, D, et al. Resilience to autosomal dominant Alzheimer’s disease in a Reelin-COLBOS heterozygous man. Nat Med. (2023) 29:1243–52. doi: 10.1038/s41591-023-02318-3
136. Vélez, JI, Lopera, F, Sepulveda-Falla, D, Patel, HR, Johar, AS, Chuah, A, et al. APOE*E2 allele delays age of onset in PSEN1 E280A Alzheimer's disease. Mol Psychiatry. (2016) 21:916–24. doi: 10.1038/mp.2015.177
137. Jonsson, T, Atwal, JK, Steinberg, S, Snaedal, J, Jonsson, PV, Bjornsson, S, et al. A mutation in APP protects against Alzheimer's disease and age-related cognitive decline. Nature. (2012) 488:96–9. doi: 10.1038/nature11283
138. Arboleda-Velasquez, JA-O, Lopera, F, O'Hare, M, Delgado-Tirado, S, Marino, C, Chmielewska, N, et al. Resistance to autosomal dominant Alzheimer's disease in an APOE3 Christchurch homozygote: a case report. Nat Med. (2019) 25:1680–3. doi: 10.1038/s41591-019-0611-3
139. Le Guen, Y, Belloy, ME, Grenier-Boley, B, de Rojas, I, Castillo-Morales, A, Jansen, I, et al. Association of Rare APOE missense variants V236E and R251G with risk of Alzheimer disease. JAMA Neurol. (2022) 79:652–63. doi: 10.1001/jamaneurol.2022.1166
140. Palmqvist, S, Janelidze, S, Quiroz, YT, Zetterberg, H, Lopera, F, Stomrud, E, et al. Discriminative accuracy of plasma Phospho-tau217 for Alzheimer disease vs other neurodegenerative disorders. JAMA. (2020) 324:772–81. doi: 10.1001/jama.2020.12134
141. Allegri, RF, Chrem Méndez, P, Calandri, I, Cohen, G, Martín, ME, Russo, MJ, et al. Prognostic value of ATN Alzheimer biomarkers: 60-month follow-up results from the argentine Alzheimer's disease neuroimaging initiative. Alzheimers Dement (Amst). (2020) 12:e12026. doi: 10.1002/dad2.12026
142. Handley, M, Bunn, F, and Goodman, C. Interventions that support the creation of dementia friendly environments in health care: protocol for a realist review. Syst Rev. (2015) 4:180. doi: 10.1186/s13643-015-0168-2
Keywords: Alzheimer’s disease, Alzheimer’s disease treatment, Latin America, Latin American and Caribbean region, Alzheimer’s disease management, Alzheimer’s disease biomarkers, Alzheimer’s disease recommendations
Citation: Lopera F, Custodio N, Rico-Restrepo M, Allegri RF, Barrientos JD, Garcia Batres E, Calandri IL, Calero Moscoso C, Caramelli P, Duran Quiroz JC, Jansen AM, Mimenza Alvarado AJ, Nitrini R, Parodi JF, Ramos C, Slachevsky A and Brucki SMD (2023) A task force for diagnosis and treatment of people with Alzheimer’s disease in Latin America. Front. Neurol. 14:1198869. doi: 10.3389/fneur.2023.1198869
Edited by:
Serge Gauthier, McGill University, CanadaReviewed by:
Maria Del Carmen Silva-Lucero, National Autonomous University of Mexico, MexicoCopyright © 2023 Lopera, Custodio, Rico-Restrepo, Allegri, Barrientos, Garcia Batres, Calandri, Calero Moscoso, Caramelli, Duran Quiroz, Jansen, Mimenza Alvarado, Nitrini, Parodi, Ramos, Slachevsky and Brucki. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francisco Lopera, ZnJhbmNpc2NvLmxvcGVyYUBnbmEub3JnLmNv
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.