 Yong-hui Jia1†
Yong-hui Jia1† Hai-yin Jiang
Hai-yin Jiang Ai-juan Li
Ai-juan Li- 1Pharmacy Department, The 960th Hospital of PLA, Jinan, China
- 2State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China
Background: Evidence suggests that there is an increased risk of stroke after herpes zoster (HZ). However, reports on the effects of HZ vaccination (HZV) and antiviral treatment on stroke risk are inconsistent. Thus, we examined these associations in a meta-analysis.
Methods: To identify relevant studies, we searched three databases for articles published up to January 2023. Random-effect models were examined to determine overall pooled estimates and 95% confidence intervals (CIs).
Results: This review included 12 observational studies (six on HZV and seven on antiviral treatment). When comparing vaccinated and unvaccinated patients, vaccination was found to be associated with a lower risk of stroke (OR, 0.78; 95% CI 0.68–0.9; P = 0.001). A meta-analysis of self-controlled case series (SCCS) revealed evidence of a reduced OR in individuals who received the vaccine (OR, 1.14; 95% CI 0.94–1.37; P = 0.181) compared with unvaccinated individuals (OR, 1.36; 95% CI 1.15–1.61; P < 0.001). Compared with untreated patients, antiviral therapy was not associated with a reduced risk of stroke (OR, 1.13; 95% CI 0.94–1.36; P = 0.201). The meta-analysis of the SCCS showed no evidence of a reduced OR in individuals who received antiviral therapy (OR, 1.33; 95% CI 1.17–1.51; P < 0.001) compared to untreated individuals (OR, 1.45; 95% CI 1.25–1.69; P < 0.001).
Conclusions: This meta-analysis suggests that the HZV, but not antiviral treatment, decreases the odds of developing stroke.
Introduction
Primary infection with varicella zoster virus (VZV) usually occurs in childhood, causing chickenpox characterized by a vesicular pruritic rash, viremia, and fever (1). VZV becomes latent in the dorsal root ganglia and nerve cells and can reactivate to cause herpes zoster (HZ), which typically manifests as localized, painful, dermatomal vesicles or blisters (2). The incidence of HZ has increased from 1.7 in 1993 to 7.2 per 1,000 person-years in 2016, with a substantial negative impact on the health-related quality of life (3). In the last decade, infectious diseases have been identified as a new risk factor for stroke. Several pathogens have been recognized as being directly associated with the development of stroke (4–6). Preclinical studies have demonstrated that VZV triggers a variety of inflammatory effects that may contribute to thrombogenesis, atherosclerosis, and vasculopathy and thus to an increased risk of stroke (7–9). Recent research on the effect of HZ on stroke has reported an increased risk of stroke or myocardial infarction in HZ patients, especially ophthalmic zoster patients (10, 11). Given the high morbidity and mortality of stroke, any potential prevention strategy becomes increasingly important.
With the introduction of the zoster vaccine live (ZVL, Zostavax) in 2006 and the recombinant zoster vaccine (RCV, Shingrix) in 2017, HZ vaccination (HZV) has reduced the risk of developing HZ and postherpetic neuralgia (12, 13). Some studies have examined the association between HZV and post-HZ stroke, but the findings have been inconsistent (14–19). One study had a within-person study design but did not find a protective role of HZV (14). The most recent case–control study conducted to date found a reduced risk of stroke in vaccinated patients compared with unvaccinated patients (19). Additional studies have explored whether antiviral treatment modifies the risk of stroke after HZ. Some studies have demonstrated that antiviral treatment following HZ is associated with a reduced risk of stroke (20, 21), while others have found no difference in stroke risk between patients treated (or not) with antivirals (16, 22–25). To the best of our knowledge, the latest published review on this topic included articles in PubMed up to January 2017, including only two observational studies evaluating the association between antiviral treatment and stroke. Furthermore, this study did not conduct a meta-analysis (26); hence, the researchers were unable to provide an overall quantitative summary of their results. The effect of HZV and antiviral treatment on post-HZ stroke remains unclear. Therefore, we conducted a systematic review and meta-analysis on this topic, including all observational studies published up to January 2023 to examine whether HZV and antiviral treatment modify the risk of post-HZ stroke.
Methods
This meta-analysis is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (27).
Search strategy
This systematic review examined English-language publications in the EMBASE, PubMed, and Cochrane Library databases. The literature was searched using the following keywords from inception dates to 16 January 2023: “Herpes Zoster OR Shingles OR Zoster OR VZV OR zona” and “stroke OR cerebral arterial disease OR myocardial infarction OR ischemic attack OR cerebral ischemia.” The reference lists of identified publications and relevant reviews were also searched manually.
Study selection
Peer-reviewed publications were considered eligible for data extraction if they were observational studies with cross-sectional, case–control, case–crossover, self-controlled case series (SCCS), or cohort study designs; compared vaccinated with unvaccinated patients and/or antivirally treated with untreated patients; reported odds ratios (ORs), relative risks (RRs), incidence ratios (IRs), and/or hazard ratios (HRs) of associations; and included adequate data to derive risk estimates. Reviews, case reports, conference abstracts, editorials, correspondence, basics, and animal studies were excluded.
Data extraction and quality assessment
An Excel spreadsheet was used to record the details of the included studies, including the first author's name, year of publication, country, study design, study period, age, number of observation groups, information regarding HZ exposure, diagnostic criteria for stroke (stroke or myocardial infarction), outcome measures, and statistical adjustments.
Two authors evaluated study quality using the Newcastle–Ottawa Quality Assessment Scale (NOS), which was developed for assessing observational studies (28). This scale is divided into three domains: participant selection (four questions), study group comparability (two questions), and outcome (three questions), with all questions having a value of one. Studies with a quality score ≥7 were considered to be of high quality.
Data analysis
Meta-analysis was performed using STATA version 10.0 (StataCorp, USA). Heterogeneity among the included studies was assessed using the I2 statistic (29). I2 values of 25%, 50%, and 75% represent low, medium, and high heterogeneity, respectively (29). Due to differences in the study populations and methodology, effect estimates were combined using the random-effects generic inverse variance method of DerSimonian and Laird (30). A pooled OR was calculated. Publication bias was not assessed because fewer than 10 studies were included in the meta-analysis (31). Statistical significance for all analyses was set at a P-value of <0.05.
Results
Search results
Using the keywords, our comprehensive search identified 1,744 articles after excluding 239 duplicates, of which 996 were excluded after the initial screening of titles and abstracts. Then, the full text of 54 articles was reviewed to determine their eligibility. As a result, our analysis included 12 studies [six (14–19) on HZV and seven (16, 20–25) on antiviral exposure]. The screening and reason for exclusion at each step are shown in the PRISMA flow diagram (Figure 1).
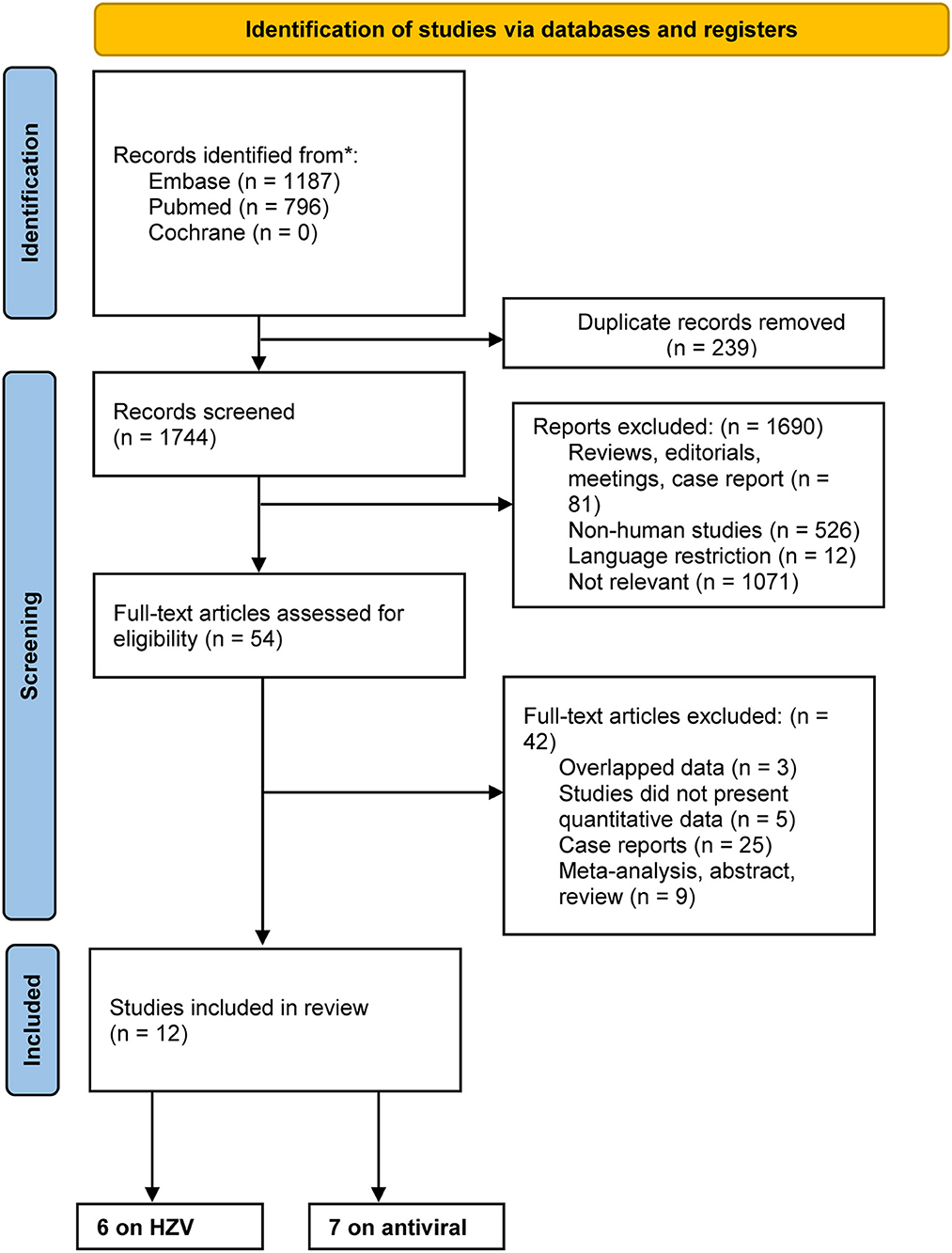
Figure 1. Flowchart of the search process and study selection.
Characteristics of the included studies investigating the association between HZV and stroke
Table 1 shows the characteristics of the six studies that investigated the association between HZV and stroke risk; there were three (14–16) SCCS studies, two (17, 18) cohort studies, and one (19) case–control study. Publication years ranged from 2015 to 2022, and five studies were conducted in the United States. Only one (18) was a hospital-based study; the others were population-based studies that analyzed database data. Participants in four studies (14–17) were older than 65 years old. Four studies (14–17) evaluated only ZVL (Zostavax), one study (18) evaluated only RZV (Shingrix), and the remaining study (19) evaluated both ZVL and RZV. Based on the NOS quality assessment scores, all studies were deemed to be of high quality. The score breakdown is presented in Supplementary Tables S1, S2.
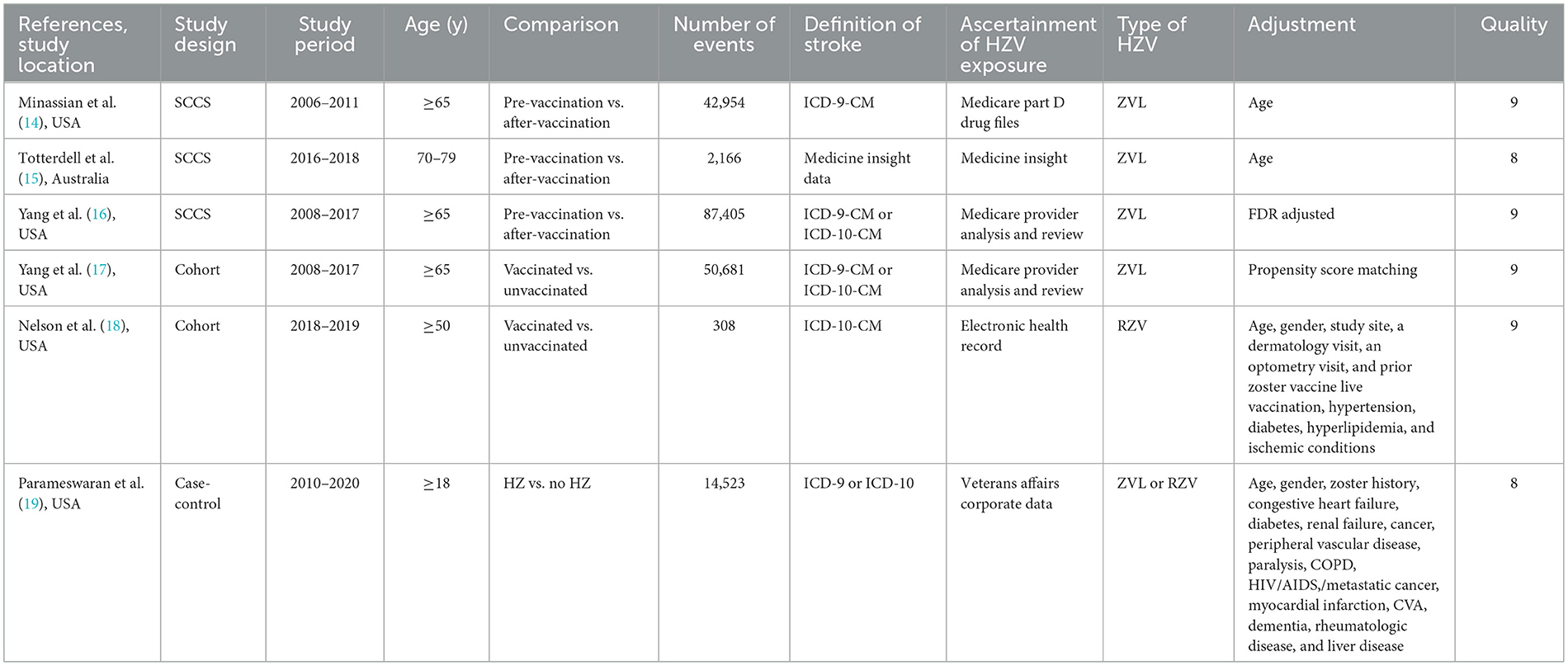
Table 1. Characteristics of the included studies investigating the association between HZV and cerebrovascular events.
Meta-analysis of HZV and risk of stroke
Three studies (17–19) evaluated the effect of HZV on stroke by comparing vaccinated and unvaccinated patients; the pooled data demonstrated that patients who received HZV were less likely to suffer from a stroke than those who did not (OR, 0.78; 95% CI 0.68–0.9; I2 = 78.4%; P = 0.001; Figure 2A).
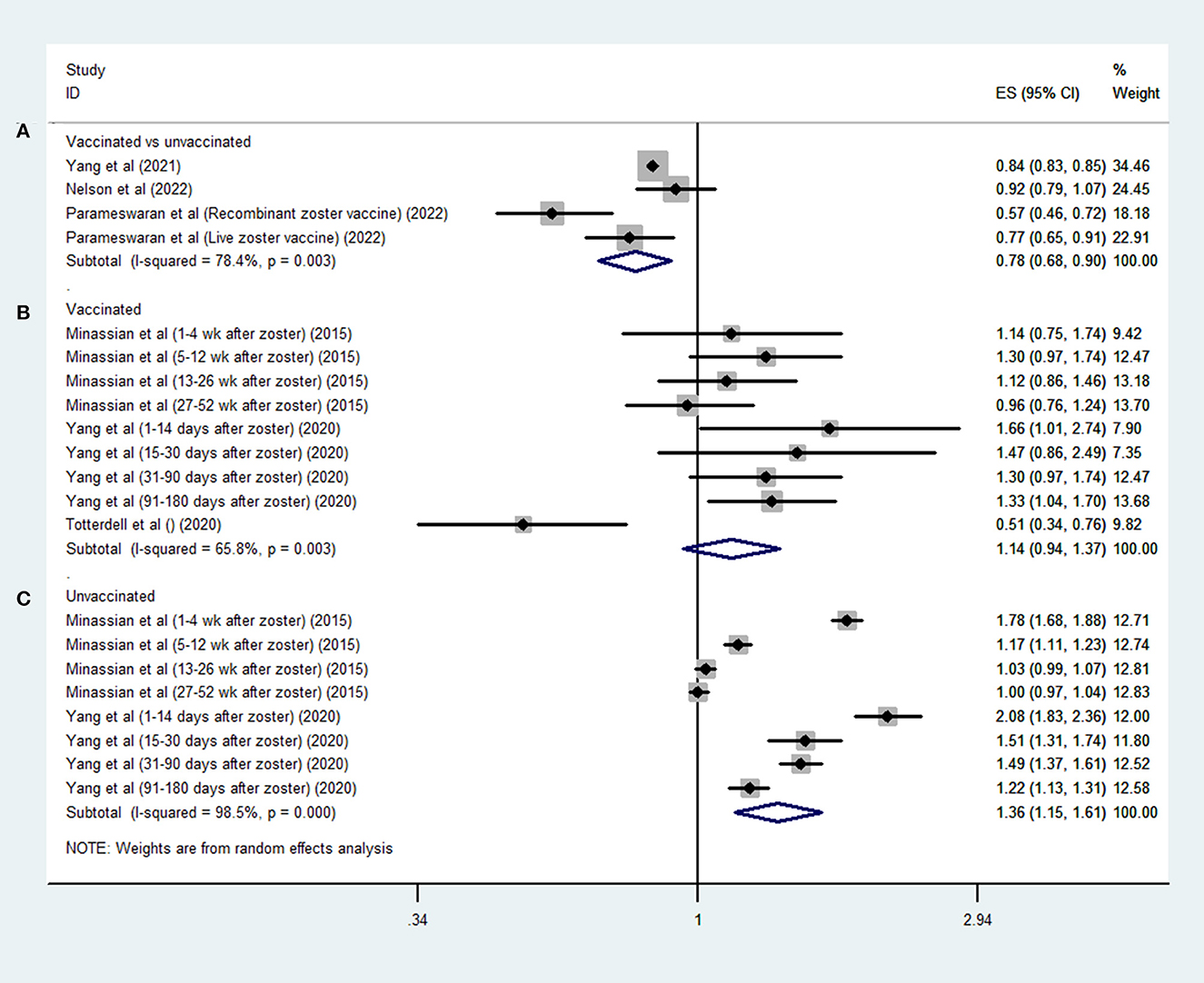
Figure 2. Forest plot of the overall risk of stroke in relation to HZV in (A) vaccinated vs. unvaccinated patients; (B) unvaccinated patients' own control; and (C) vaccinated patients' own control.
Three SCCS studies (14–16) assessed the risk of stroke in defined periods after HZ compared with other periods. Among the vaccinated patients, there was no positive association between HZ infection and stroke risk (OR, 1.14; 95% CI 0.94–1.37; I2 = 65.8%; P = 0.181; Figure 2B); however, a higher risk of stroke was observed among unvaccinated patients after HZ infection (OR, 1.36; 95% CI 1.15–1.61; I2 = 98.5%; P < 0.001; Figure 2C).
Characteristics of the included studies on the association between antiviral treatment and stroke
Table 2 presents the details of the seven studies that investigated the association between antiviral treatment and stroke risk; there were two SCCS studies (16, 23) and five cohort studies (20–22, 24, 25). The studies were published between 2010 and 2022. Three studies (16, 24, 25) were conducted in the United States, two (20, 21) in Asia, and two (22, 23) in Europe. Only one (25) was a hospital-based study; the others were population-based studies that analyzed database data. According to the NOS quality scores, six studies were deemed to be of high quality, with only one categorized as low quality. The score breakdown is presented in Supplementary Tables S3, S4.
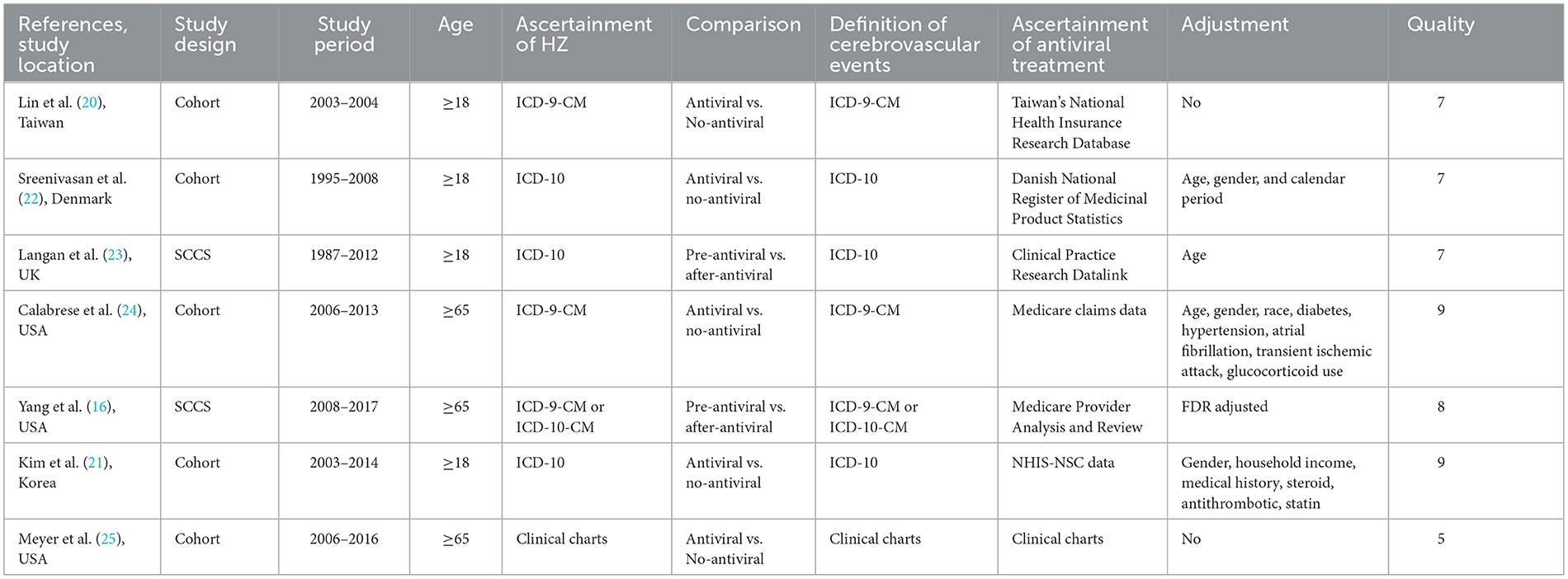
Table 2. Characteristics of the included studies investigating the association between antiviral treatment and cerebrovascular events among HZ patients.
Meta-analysis of antiviral treatment and risk of stroke
Four studies (20–22, 25) evaluated the effect of antiviral treatment on stroke by comparing treated and untreated patients with HZ; the pooled data demonstrated that antiviral treatment was not associated with a reduced risk of stroke in these patients after HZ (OR, 1.13; 95% CI 0.94–1.36; I2 = 92%; P = 0.201; Figure 3A).
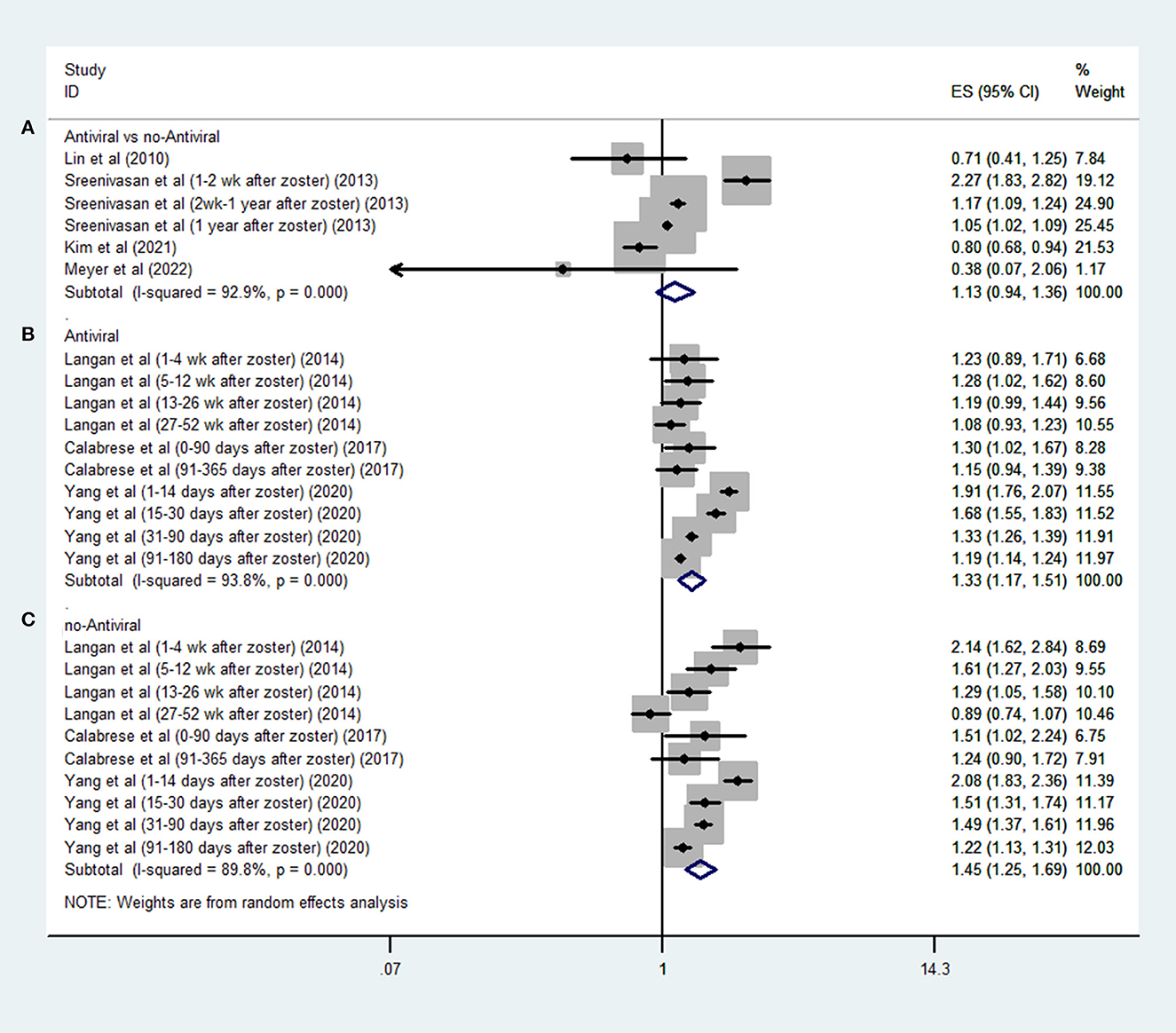
Figure 3. Forest plot of the overall risk of post-HZ stroke in relation to antiviral treatment (HZV): (A) antiviral vs. no-antiviral; (B) no-antiviral self-control; and (C) antiviral self-control of.
Three SCCS studies (16, 23, 24) evaluated the effect of antiviral treatment on the risk of stroke in defined periods after HZ compared to other periods; the pooled data demonstrated that both treated (OR, 1.33; 95% CI 1.17–1.51; I2 = 93.8%; P < 0.001; Figure 3B) and untreated (OR, 1.45; 95% CI 1.25–1.69; I2 = 89.8%; P < 0.001; Figure 3C) patients were at a higher risk of stroke after HZ.
Discussion
This systematic review and meta-analysis comprehensively investigated the current evidence on the effects of HZV and antiviral treatment on the risk of stroke; the pooled results showed that HZV was associated with a decreased risk of stroke, whereas no such protective modified effect was observed in patients with HZ who received antiviral treatment. The marked methodological variation among the studies and the limited number of included studies warrant a cautious interpretation of these findings.
Previous studies (10, 11, 26, 32) have focused on the relationship between HZ and stroke risk. Several biological mechanisms could explain such an association. One possible explanation is viral replication in the cerebral arteries. HZ virus can invade the arterial walls and thereby induce vasculopathy, which ultimately results in thrombosis, occlusion, infarction, aneurism, and hemorrhage (33). Inflammation also plays an important role in the etiology of stroke. A clinical study found inflammatory cells in the adventitia and intima in both early and late VZV vasculopathy (34). The inflammatory cytokines secreted by these inflammatory cells can potentially disrupt pre-existing atherosclerotic plaques (35). Consistent with the preclinical findings, the recent meta-analysis (10) based on 12 epidemiologic studies demonstrated an increased risk of stroke in the short term after herpes zoster infection. Therefore, prevention and treatment of HZ may modify the associated risk of stroke.
In previous studies, the live HZV vaccine was 51%−65% efficacious against zoster and post-herpetic neuralgia, and this increased to 90% efficacy for the recombinant zoster vaccine (12, 13). The protective effect of HZV was observed in our analysis by comparing the incidence of stroke between vaccinated and unvaccinated individuals. However, the pooled analysis of the SCCS studies did not support an effect of HZV in terms of modifying the risk of stroke. This may result from the designs of such studies. SCCS is a novel strategy to control for between-person confounders by comparing the risk and reference periods in each patient (36). Risk periods are defined as during or after an exposure. Considering the proven risk of stroke after HZ, the null association in vaccinated patients with HZ implies a protective effect of HZV. Meanwhile, the meta-analysis of the SCCS studies found an increased risk of stroke in unvaccinated patients with HZ.
Antiviral drugs are mainly used to treat acute HZ, and they can relieve pain, accelerate the healing of skin lesions, and reduce the spread of the virus (37). Theoretically, it follows that antiviral treatment may have the potential to reduce post-zoster stroke by reducing inflammation. However, our findings did not support the protective role of antiviral treatment on stroke, which may be due to the following reasons. First, antiviral treatment is likely to be used mainly in patients with severe symptoms. It is reasonable to speculate that a more severe disease confers a higher risk of stroke; further studies should consider the severity of HZ. Second, it is recommended that antiviral treatment should be started within 3 days of the onset of HZ. Early antiviral therapy has been proven to reduce the risk of post-herpetic neuralgia and other complications (38). Only one study included in our analysis evaluated the effect of the timing of antiviral treatment on the risk of cerebrovascular disease and found a protective role for prompt but not for delayed antiviral treatment (25). Therefore, delayed antiviral treatment may underestimate the beneficial effect of antiviral treatment on stroke. Third, patient age varied among the included studies, and increasing age is associated with a higher risk of stroke (39). Due to the low incidence of stroke in young people, the wide age range of the subjects enrolled in several of the included studies may have reduced our chance of finding a protective effect. Accordingly, one included study (21) performed a further age-stratified analysis and observed a protective effect of antiviral treatment only in patients aged ≥50 years. Hence, the protective effect of antiviral treatment may be age-dependent.
To the best of our knowledge, this study is the first systematic review of the effects of HZV and antiviral treatment on the risk of stroke. However, several limitations should be taken into account. First, the small number of included studies may have influenced the accuracy of our findings. Second, residual unknown confounders are always a concern in observational studies. Further well-designed studies that consider more covariates should examine these associations. Finally, the included studies were very heterogeneous in terms of data sources, definitions of stroke, age of enrolled subjects, and type of vaccination examined.
In conclusion, our findings suggest that HZV, but not antiviral treatment is associated with a reduced risk of post-HZ stroke. However, these conclusions should be interpreted with caution because of the high study heterogeneity and potential unknown confounders. Further well-designed studies with larger samples are needed to verify our findings.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
A-jL and Y-hJ searched the library and drafted the manuscript. Y-bD and H-yJ extracted the data and revised all articles. A-jL designed the manuscript. All authors reviewed the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1176920/full#supplementary-material
References
1. Gray WL. Simian varicella: a model for human varicella-zoster virus infections. Rev Med Virol. (2004) 14:363–81. doi: 10.1002/rmv.437
2. Heininger U, Seward JF. Varicella. Lancet. (2006) 368:1365–76. doi: 10.1016/S0140-6736(06)69561-5
3. Yawn BP, Gilden D. The global epidemiology of herpes zoster. Neurology. (2013) 81:928–30. doi: 10.1212/WNL.0b013e3182a3516e
4. Elkind MSV, Boehme AK, Smith CJ, Meisel A, Buckwalter MS. Infection as a stroke risk factor and determinant of outcome after stroke. Stroke. (2020) 51:3156–68. doi: 10.1161/STROKEAHA.120.030429
5. Palm F, Pussinen PJ, Aigner A, Becher H, Buggle F, Bauer MF, et al. Association between infectious burden, socioeconomic status, and ischemic stroke. Atherosclerosis. (2016) 254:117–23. doi: 10.1016/j.atherosclerosis.2016.10.008
6. Shakil SS, Emmons-Bell S, Rutan C, Walchok J, Navi B, Sharma R, et al. Stroke among patients hospitalized with COVID-19: results from the American Heart Association COVID-19 cardiovascular disease registry. Stroke. (2022) 53:800–7. doi: 10.1161/STROKEAHA.121.035270
7. Tuttolomondo A, Di Raimondo D, Pecoraro R, Maida C, Arnao V, Corte VD, et al. Early high-dosage atorvastatin treatment improved serum immune-inflammatory markers and functional outcome in acute ischemic strokes classified as large artery atherosclerotic stroke: a randomized trial. Medicine. (2016) 95:e3186. doi: 10.1097/MD.0000000000003186
8. Tuttolomondo A, Casuccio A, Corte VD, Maida C, Pecoraro R, Di Raimondo D, et al. Endothelial function and arterial stiffness indexes in subjects with acute ischemic stroke: relationship with TOAST subtype. Atherosclerosis. (2017) 256:94–9. doi: 10.1016/j.atherosclerosis.2016.10.044
9. Di Bona D, Scafidi V, Plaia A, Colomba C, Nuzzo D, Occhino C, et al. HLA and killer cell immunoglobulin-like receptors influence the natural course of CMV infection. J Infect Dis. (2014) 210:1083–9. doi: 10.1093/infdis/jiu226
10. Erskine N, Tran H, Levin L, Ulbricht C, Fingeroth J, Kiefe C, et al. A systematic review and meta-analysis on herpes zoster and the risk of cardiac and cerebrovascular events. PLoS ONE. (2017) 12:e0181565. doi: 10.1371/journal.pone.0181565
11. Yang S-Y, Li H-X, Yi X-H, Han G-L, Zong Q, Wang M-X, et al. Risk of stroke in patients with herpes zoster: a systematic review and meta-analysis. J Stroke Cerebrovasc Dis. (2017) 26:301–7. doi: 10.1016/j.jstrokecerebrovasdis.2016.09.021
12. Sanford M, Keating GM. Zoster vaccine (Zostavax): a review of its use in preventing herpes zoster and postherpetic neuralgia in older adults. Drugs Aging. (2010) 27:159–76. doi: 10.2165/10489140-000000000-00000
13. Cunningham AL, Lal H, Kovac M, Chlibek R, Hwang S-J, Díez-Domingo J, et al. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older. N Engl J Med. (2016) 375:1019–32. doi: 10.1056/NEJMoa1603800
14. Minassian C, Thomas SL, Smeeth L, Douglas I, Brauer R, Langan SM. Acute cardiovascular events after herpes zoster: a self-controlled case series analysis in vaccinated and unvaccinated older residents of the United States. PLoS Med. (2015) 12:e1001919. doi: 10.1371/journal.pmed.1001919
15. Totterdell J, Phillips A, Glover C, Chidwick K, Marsh J, Snelling T, et al. Safety of live attenuated herpes zoster vaccine in adults 70-79 years: a self-controlled case series analysis using primary care data from Australia's MedicineInsight program. Vaccine. (2020) 38:3968–79. doi: 10.1016/j.vaccine.2020.03.054
16. Yang Q, George MG, Chang A, Tong X, Merritt R, Hong Y. Effect of herpes zoster vaccine and antiviral treatment on risk of ischemic stroke. Neurology. (2020) 95:e708–e17. doi: 10.1212/WNL.0000000000010028
17. Yang Q, Chang A, Tong X, Merritt R. Herpes zoster vaccine live and risk of stroke among medicare beneficiaries: a population-based cohort study. Stroke. (2021) 52:1712–21. doi: 10.1161/STROKEAHA.120.032788
18. Nelson JC, Ulloa-Pérez E, Yu O, Cook AJ, Jackson ML, Belongia EA, et al. Active postlicensure safety surveillance for recombinant zoster vaccine using electronic health record data. Am J Epidemiol. (2023) 192:205–16. doi: 10.1093/aje/kwac170
19. Parameswaran GI, Wattengel BA, Chua HC, Swiderek J, Fuchs T, Carter MT, et al. Increased stroke risk following herpes zoster infection and protection with zoster vaccine. Clin Infect Dis. (2023) 76:e1335–e40. doi: 10.1093/cid/ciac549
20. Lin HC, Chien CW, Ho JD. Herpes zoster ophthalmicus and the risk of stroke: a population-based follow-up study. Neurology. (2010) 74:792–7. doi: 10.1212/WNL.0b013e3181d31e5c
21. Kim J, Jeon J, Lee HS, Lee K-Y. Association between the risk for cardiovascular events and antiviral treatment for herpes zoster. Clin Infect Dis. (2021) 73:758–64. doi: 10.1093/cid/ciaa1384
22. Sreenivasan N, Basit S, Wohlfahrt J, Pasternak B, Munch TN, Nielsen LP, et al. The short- and long-term risk of stroke after herpes zoster - a nationwide population-based cohort study. PLoS ONE. (2013) 8:e69156. doi: 10.1371/journal.pone.0069156
23. Langan SM, Minassian C, Smeeth L, Thomas SL. Risk of stroke following herpes zoster: a self-controlled case-series study. Clin Infect Dis. (2014) 58:1497–503. doi: 10.1093/cid/ciu098
24. Calabrese LH, Xie F, Yun H, Winthrop KL, Baddley JW, Calabrese C, et al. Herpes zoster and the risk of stroke in patients with autoimmune diseases. Arthritis Rheumatol. (2017) 69:439–46. doi: 10.1002/art.39855
25. Meyer JJ, Liu K, Danesh-Meyer HV, Niederer RL. Prompt antiviral therapy is associated with lower risk of cerebrovascular accident following herpes zoster ophthalmicus. Am J Ophthalmol. (2022) 242:215–20. doi: 10.1016/j.ajo.2022.06.020
26. Forbes HJ, Williamson E, Benjamin L, Breuer J, Brown MM, Langan SM, et al. Association of herpesviruses and stroke: systematic review and meta-analysis. PLoS ONE. (2018) 13:e0206163. doi: 10.1371/journal.pone.0206163
27. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
28. Higgins JP. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. (2014). Available online at: www.cochrane-handbook.org (acessed December 6, 2014).
29. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
30. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
31. Lau J, Ioannidis JPA, Terrin N, Schmid CH, Olkin I. The case of the misleading funnel plot. BMJ. (2006) 333:597–600. doi: 10.1136/bmj.333.7568.597
32. Zhang Y, Luo G, Huang Y, Yu Q, Wang L, Li K. Risk of stroke/transient ischemic attack or myocardial infarction with herpes zoster: a systematic review and meta-analysis. J Stroke Cerebrovasc Dis. (2017) 26:1807–16. doi: 10.1016/j.jstrokecerebrovasdis.2017.04.013
33. Gilden D, Cohrs RJ, Mahalingam R, Nagel MA. Varicella zoster virus vasculopathies: diverse clinical manifestations, laboratory features, pathogenesis, and treatment. Lancet Neurol. (2009) 8:731–40. doi: 10.1016/S1474-4422(09)70134-6
34. Haanpää M, Dastidar P, Weinberg A, Levin M, Miettinen A, Lapinlampi A, et al. CSF and MRI findings in patients with acute herpes zoster. Neurology. (1998) 51:1405–11. doi: 10.1212/WNL.51.5.1405
35. Ge P, Li H, Ya X, Xu Y, Ma L, He Q, et al. Single-cell atlas reveals different immune environments between stable and vulnerable atherosclerotic plaques. Front Immunol. (2022) 13:1085468. doi: 10.3389/fimmu.2022.1085468
36. Nie X, Xu L, Bai Y, Liu Z, Liu Z, Farrington P, et al. Self-controlled case series design in vaccine safety: a systematic review. Expert Rev Vaccines. (2022) 21:313–24. doi: 10.1080/14760584.2022.2020108
37. Opstelten W, Eekhof J, Neven AK, Verheij T. Treatment of herpes zoster. Can Fam Physician. (2008) 54:373–7.
38. Vander Straten M, Carrasco D, Lee P, Tyring SK. Reduction of postherpetic neuralgia in herpes zoster. J Cutan Med Surg. (2001) 5:409–16. doi: 10.1177/120347540100500508
Keywords: infection, vaccine, cerebrovascular, virus, pathogen
Citation: Jia Y-h, Dong Y-b, Jiang H-y and Li A-j (2023) Effects of herpes zoster vaccination and antiviral treatment on the risk of stroke: a systematic review and meta-analysis. Front. Neurol. 14:1176920. doi: 10.3389/fneur.2023.1176920
Received: 01 March 2023; Accepted: 24 April 2023;
Published: 17 May 2023.
Edited by:
Bernhard Sehm, University Hospital in Halle, GermanyReviewed by:
Christian Urbanek, Klinikum Ludwigshafen, GermanyNatasa Krsto Rancic, University of Niš, Serbia
Antonino Tuttolomondo, Università degli Studi di Palermo, Italy
Copyright © 2023 Jia, Dong, Jiang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ai-juan Li, bGlhaWp1YW4yMDIzQDE2My5jb20=
†These authors have contributed equally to this work