 Tien Hoang-Anh
Tien Hoang-Anh Quy Duong-Minh
Quy Duong-Minh Nhi Nguyen-Thi-Y1
Nhi Nguyen-Thi-Y1 Sy Duong-Quy
Sy Duong-Quy
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 21 June 2023
Sec. Sleep Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1132014
This article is part of the Research TopicSleep Disorders and Airway DiseasesView all 16 articles
Introduction: Obstructive Sleep Apnea Syndrome (OSAS) is the most common respiratory disorder during sleep. Many studies have shown an association between obstructive sleep apnea syndrome and stroke, and OSAS has not been adequately considered in Vietnam compared to the actual clinical dangers. This study aims to assess the prevalence and general characteristics of obstructive sleep apnea syndrome in patients with cerebral infarction and investigate the relationship between obstructive sleep apnea syndrome and the severity of cerebral infarction.
Methods: Descriptive cross-sectional study. We identified 56 participants from August 2018 to July 2019. Subacute infarcts were identified by neuroradiologists. For each participant, vascular risk factors, medications, clinical symptoms, and neurological examination were abstracted from the medical record. Patients were taken for history and clinical examination. The patients were divided into two groups according to their AHI (Apnea-Hypopnea Index) (<5 and ≥5).
Results: A total of 56 patients were registered for the study. The mean age is 67.70 ± 11.07. The proportion of men is 53.6%. AHI has a positive correlation with neck circumference (r = 0.4), BMI (r = 0.38), the Epworth Sleepiness Scale (r = 0.61), LDL cholesterol (r = 0.38), the Modified Rankin Scale (r = 0.49), NIHSS (National Institutes of Health Stroke Scale) (r = 0.53), and an inverse correlation with SpO2 (r = 0.61).
Conclusion: Obstructive sleep apnea Syndrome is a factor in the prognosis of cerebral infarction as well as cardiovascular diseases such as hypertension. Thus, understanding the risk of stroke in people with sleep apnea is necessary and working with a doctor to diagnose and treat sleep apnea is important.
Obstructive sleep apnea (OSA) is a chronic sleep-related breathing disorder characterized by recurrent partial or complete cessation of airflow due to upper airway obstruction during sleep that results in sleep fragmentation, intermittent hypoxia, and hypercapnia leading to increased sympathetic nervous system activity (1). OSA has a prevalence reaching 8.5% of the adult population in Viet Nam considering all OSA severities (2). Night-to-night AHI variability does not have a definitive explanation but is reported in polysomnography measurements and should be considered in treatment decisions (3, 4).
Patients with OSA may exhibit loud and chronic snoring, gasping episodes during sleep, sleepiness, obesity, and increased neck circumference (5). OSA is associated with physical examination alterations and systemic complaints, including daytime fatigue and impaired concentration (6). OSA is also an independent risk factor for arterial hypertension, stroke, ischemic heart disease, cardiac arrhythmia, and heart failure (1).
Cerebral infarction tends to increase because the risk factors for the disease do not decrease such as a sedentary lifestyle, a high-fat diet such as fast food, high-sugar drinks, stress and high blood pressure, diabetes, and smoking become common (7).
Patients with ischemic stroke often develop sleep apnea and are common within the first 24 h. Disorderly breathing can be worse if the stroke happens while patients are asleep. OSA is the most common kind of sleep apnea that takes place after a stroke. OSA affects up to 70% of people with a stroke, compared to 30% of the overall population. A major aspect of medical care is the detection and treatment of OSA, as a treatment for OSA may enhance a person's recovery and decrease the risk of additional strokes. The relationship between stroke and OSA is bidirectional:
Kim et al. studied 80 patients with stroke and concluded that OSAS could cause dysfunction in patients with cerebrovascular accidents (8).
Ahn et al., when studying 293 patients with 159 men and 134 women with acute cerebral infarction, 63.1% (111 men, 74 women) had SAS, mainly OSAS with AHI >10 and at the same time concluded the relationship between SAS and the score of the National Institutes Of Health Stroke Scale (NIHSS: National Institutes Of Health Stroke Scale) and the adjusted Rankin Scale (mRankin: Modified Rankin Scale) high and worse long-term outcomes compared with the group without SAS (9).
Mattaliano et al. when studying 130 patients with acute cerebral infarction, the results showed that 61.9% had OSAS, most of which were men accounting for 67.1%. This study confirms the high prevalence of OSA in stroke patients and shows an association between OSA and target organ damage (10).
Researchers have identified OSA as an independent risk factor for stroke. This means that people with OSA are at higher risk of stroke, even if there are no other risk factors. There are several possible reasons for why people with OSA have a higher risk of stroke. Repeated collapses of the airway during sleep create negative air pressure within the chest, which may slow the flow of blood to the brain, thereby altering cerebral vascular abnormalities. OSA increases the risk of developing heart disease, hypertension, diabetes, and heart arrhythmias. These and other health consequences of OSA can increase the risk of stroke. These and other effects may be associated with an increased risk of stroke.
Many studies have shown an association between obstructive sleep apnea syndrome and hypertension, coronary artery disease, arrhythmia, and systolic heart failure (11, 12). Numerous studies have also mentioned the association between sleep apnea syndrome and stroke (13, 14). Based on this situation, we conducted a study that aims to achieve two objectives:
1. Evaluation of prevalence and general characteristics of obstructive sleep apnea syndrome in patients with cerebral infarction.
2. Investigate the relationship between obstructive sleep apnea syndrome and the severity of cerebral infarction.
A total of 56 patients were diagnosed with subacute cerebral infarction and treated at the Cardiology Department of Hue University of Medicine and Pharmacy Hospital.
Obstructive sleep apnea Diagnostic Criteria were recommended by the American Academy of Sleep Medicine 2008 (AASM: American Academy of Sleep Medicine) (15). The patient suspected of OSAS must fulfill criterion A or B, plus criterion C. These are as follows:
A. Excessive daytime sleepiness that is not better explained by other factors.
B. Two or more of the following that are not better explained by other factors:
- Choking or gasping during sleep
- Recurrent awakenings from sleep
- Unrefreshing sleep
- Daytime fatigue
- Impaired concentration
C. Overnight monitoring demonstrates five or more obstructed breathing events per hour during sleep. These events may include any combination of obstructive apneas/hypopneas or respiratory effort–related arousals, as defined below.
All subjects aged over 15 and fulfilling the criteria for a clinician-confirmed diagnosis of subacute cerebral infarction as defined by neuroradiologists were included in the study.
- Patients with acute and severe diseases, chronic obstructive pulmonary disease or chronic respiratory failure, and cerebral diseases such as cerebral tumors, meningitis, and encephalitis.
- Patients who do not agree or cannot participate in the study.
- The patient is taking drugs that affect respiratory polygraph.
We identified 56 participants from August 2018 to July 2019. Subacute infarcts were determined by neuroradiologists. For each participant, vascular risk factors, medications, clinical symptoms, NIHSS, Epworth, and neurological examination were abstracted from the medical record. The study sample included 40 subacute cerebral infarction patients with OSA and 16 subacute cerebral infarction patients without OSA. Assess outcomes at 3 months after stroke with mRankin, face-to-face visit, or telephone.
It was a descriptive cross-sectional research method with follow-up.
Patients were weighed using a calibrated scale to the nearest 0.1 kg, and height (to 0.1 cm) was measured with a stadiometer (Medisol, Vietnam). Body mass index (BMI) was classified by WHO in 1986.
The respiratory polygraphy system used in the study is the Embletta GOLD. Embletta GOLD recorded nasal airflow, snoring using a nasal pressure cannula, blood oxygen saturation, heart rate by pulse oximetry, and respiratory effort using a thoracic piezoelectric chest belt.
The device will be provided to patients with an explanation of how to use it in advance, as well as precise instructions on the correct positioning of the equipment's sensors and monitoring. Patients will also conduct several tests to familiarize themselves with the instrument's operating instructions. When the device is returned the next day, raw data files will be uploaded to a computer and recorded automatically and manually by trained physicians from the Study Group. A respiratory polygraphy recording will be deemed valid if the recording duration is ≥5 h. Sections with artifacts or poor signals will be excluded from the analysis. If respiratory polygraphy is not valid, it will be repeated within the next 7 days.
The diagnostic criteria for adult OSA as defined by the American Academy of Sleep Medicine (16).
Overnight monitoring demonstrates five or more obstructed breathing events per hour during sleep. These events may include any combination of obstructive apneas/hypopneas or respiratory effort–related arousals, as defined below.
This report also proposed a grading of severity of OSAS based on the frequency of abnormal respiratory events during sleep: Mild: ≥5 but <15 events/hour of sleep; Moderate: 15–30 events/hour of sleep; Severe: More than 30 events/hour of sleep.
Classification of cerebral infarction by time (17):
- Acute cerebral infarction: from the first day of the 1st week after symptom onset.
- Subacute cerebral infarction: from the second week to 1 month.
- Chronic cerebral infarction: After 1 month.
The severity of cerebral infarction was based on NIHSS and mRankin. Stroke severity was categorized as follows: no stroke symptoms (0), minor stroke (1–4), moderate stroke (5–15), moderate to severe stroke (16–20), and severe stroke (21–42). In our study, the highest score was 14, thus, we divided it into two groups: 0–4 and 5–14 (18).
The original mRankin defined grade 1 as “No significant disability: able to carry out all usual duties,” and defined grade 2 as “Slight disability: unable to carry out some of the previous activities.” Patients with an mRs score ≤ 2 by definition are independent (19).
All data on age, gender, height, weight, BMI, medical and family history, clinical characteristics, and respiratory polygraphy parameters (AHI, SpO2, pulse, and frequency of snoring) of the study subjects were collected for statistical analyses.
All procedures performed in studies involving human participants followed the institutional and/or national research committee's ethical standards and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Hue University of Medicine and Pharmacy Institutional Ethical Review Board. Informed consent was obtained from all individual participants included in the study.
SPSS 22.0 software (IBM Corporation, Armonk, NY, USA) was used to analyze these collected data. Qualitative data are expressed as percentages or rates and compared with the Chi-squared test. Continuous variables were presented as mean ± standard deviation (SD) and compared with a t-test between 2 groups and a one-way analysis of variance among groups, followed by paired comparison with the least-significant difference test. A value of p < 0 0.05 was considered statistically significant.
During the study period, 56 patients with subacute infarcts met the inclusion criteria and were enrolled in this study. The demographic characteristics (gender, age, neck circumference, waist circumference, and BMI) of the study population are shown in Table 1. There was no statistically significant difference between age and gender for both groups. The mean age is 67.70 ± 11.07. The proportion of men is 53.6% (Table 1).
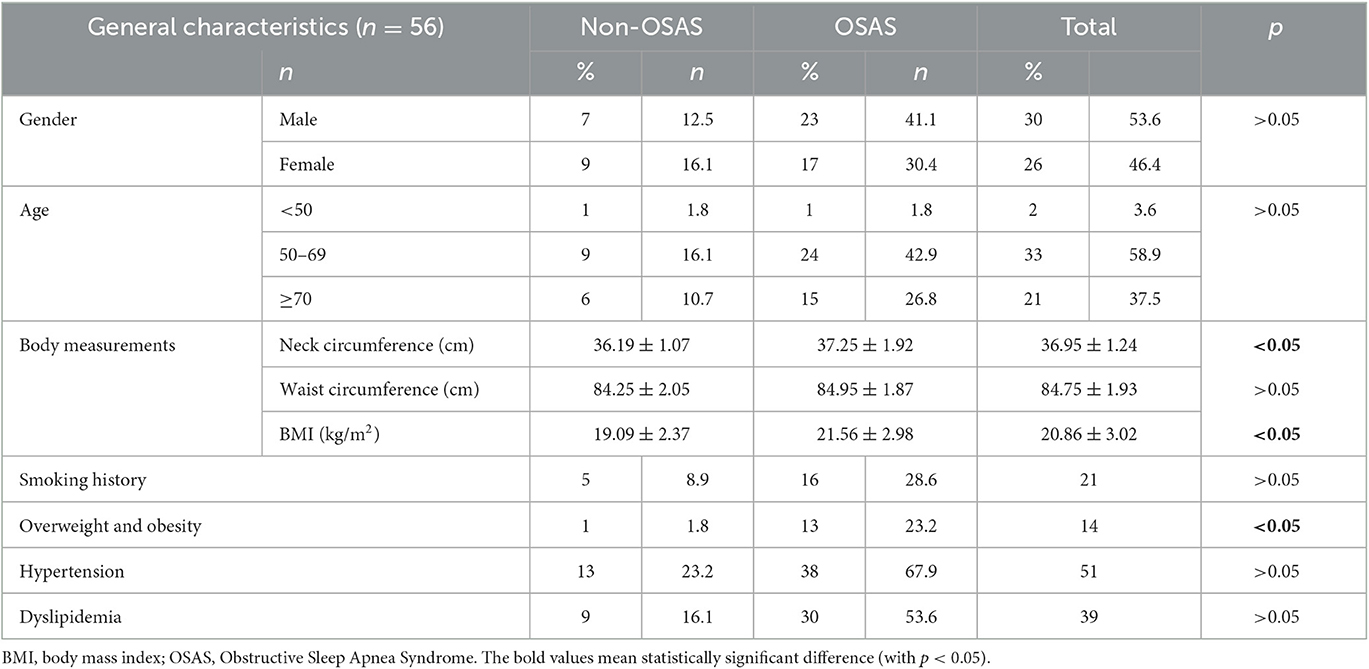
Table 1. Age group, gender, body measurements, and cardiovascular disease risk factors.
The OSAS group was statistically higher in neck circumference and BMI (Body Mass Index) than the group without OSAS (p < 0.05).
Cardiovascular risk factors include smoking history, overweight and obesity, hypertension, and dyslipidemia. The results of this study noted that the prevalence of overweight and obesity was statistically higher in the group with OSAS (p < 0.05).
Table 2 summarizes the severity of OSA based on AHI results measured from respiratory polygraphs. According to our research, the moderate OSA group accounted for the highest rate of 75%; the mild and severe OSA groups accounted for the same with 12.5% (Table 2).
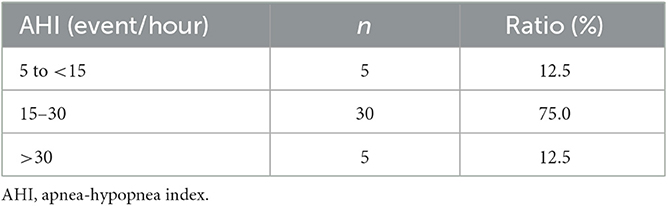
Table 2. The classification of OSA severity.
The results table below shows the index for the respiratory polygraph and the characteristics of blood pressure which include average SpO2, Lowest SpO2, measurement time, systolic blood pressure, and diastolic blood pressure. The average and lowest SpO2 were statistically smaller in the OSA group than in the non-OSA group (p < 0.05). We are interested in systolic blood pressure and diastolic blood pressure. In addition, we found that diastolic blood pressure in the OSAS group was statistically higher than in the non-OSAS group (p < 0.05) (Table 3).
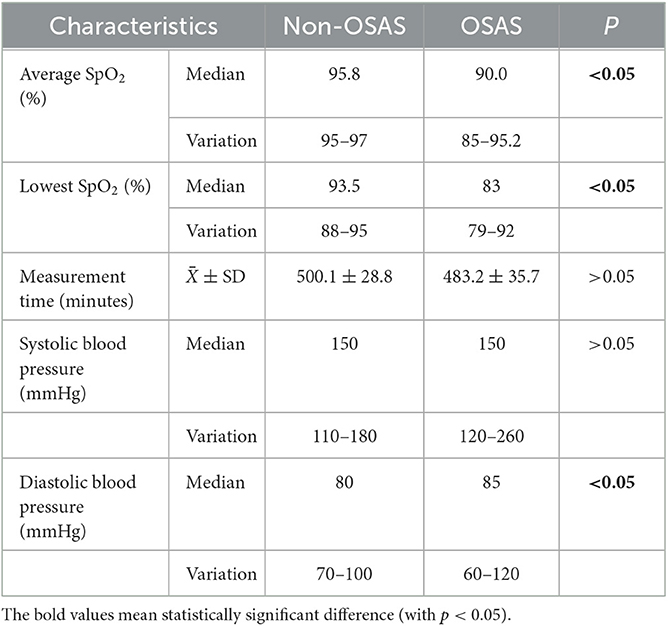
Table 3. Index for the respiratory polygraph and characteristics of blood pressure.
Among the symptoms of patients with cerebral infarction, hemiplegia was the highest at 76.8%. Followed by facial paralysis, aphasia, and headache with respect ratio is 26.8, 21.4, and 19.6%. In addition, patients may have dizzy (10.7%), sensory disturbances (14.3%), and nausea (5.4%) (Figure 1).
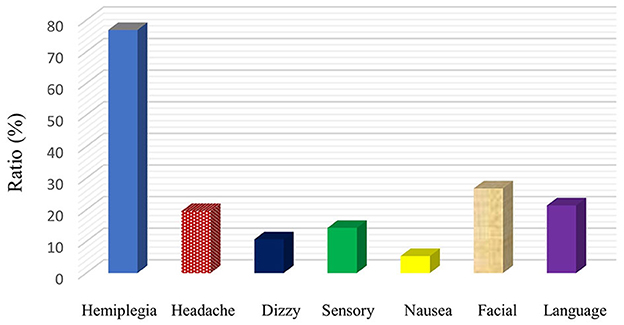
Figure 1. Clinical symptoms on admission.
Table 4 describes the characteristics of NIHSS and mRankin of study groups (compare between OSAS and non-OSAS groups). NIHSS in the OSAS group was statically higher than in the non-OSAS group (The median NIHSS for each group was 5 vs. 2) (p < 0.05) Similarly, the mRankin score in the OSAS group was also statistically higher than in the non-OSAS group (48.21 and 23.21% vs. 26.79 and 1.79%) (p < 0.05) (Table 4).
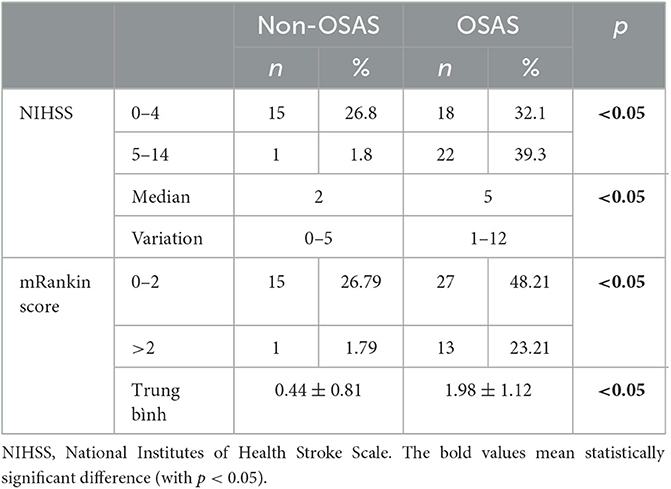
Table 4. Characteristics of NIHSS.
Figure 2 summarizes the clinical symptoms of obstructive sleep apnea including loud snoring, non-breathing during sleep, excessive daytime sleepiness, waking up a lot during the night, morning headache, and poor memory. Loud snoring during sleep accounted for the highest rate (38/56 patients); ~80% of patients in the OSAS group have loud snoring.
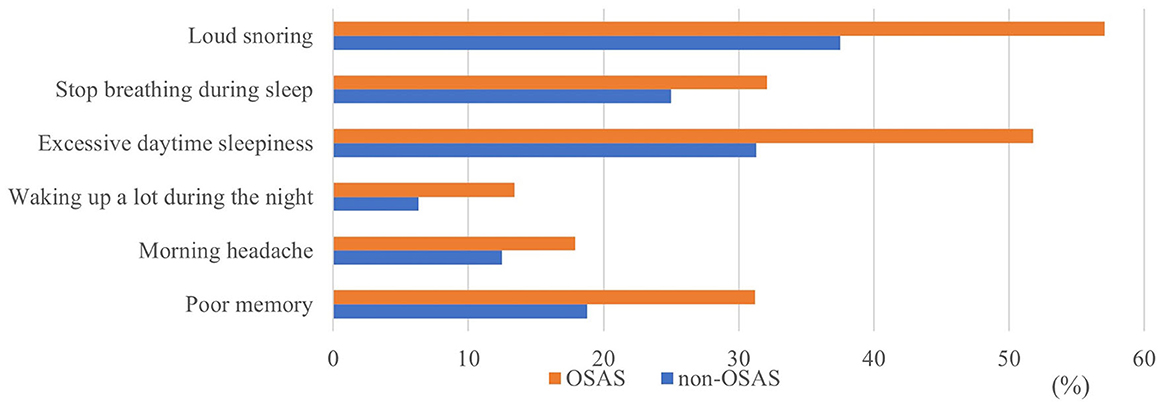
Figure 2. Symptoms of obstructive sleep apnea.
The main objective of this study is to investigate the relationship between obstructive sleep apnea syndrome and the severity of cerebral infarction. Therefore, we analyzed in relation to risk factors such as neck circumference, BMI, LDL cholesterol, mRankin, and NIHSS. The results are shown by linear equations. There is a moderate positive correlation between AHI and neck circumference (r = 0.4, p < 0.05) (Figure 3). There are similar results between AHI and BMI (r = 0.38, p < 0.05) (Figure 4); AHI and LDL Cholesterol (r = 0.38, p < 0.05) (Figure 5); AHI and mRankin (r = 0.49, p < 0.05) (Figure 6). Especially, we find a strong positive correlation between AHI and NIHSS (r = 0.53, p < 0.05) (Figure 7).
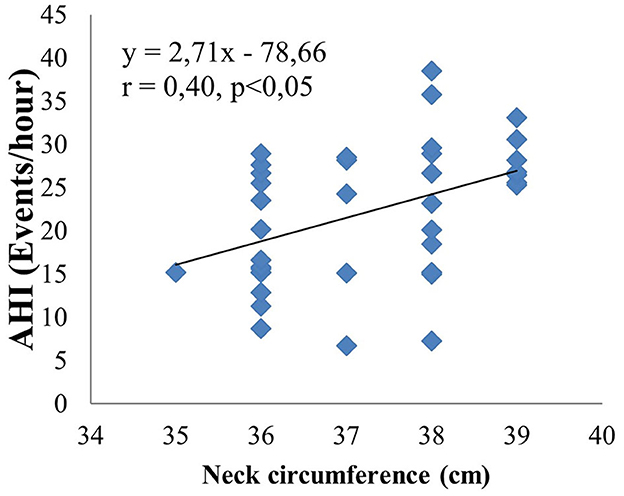
Figure 3. Correlation between AHI and neck circumference.
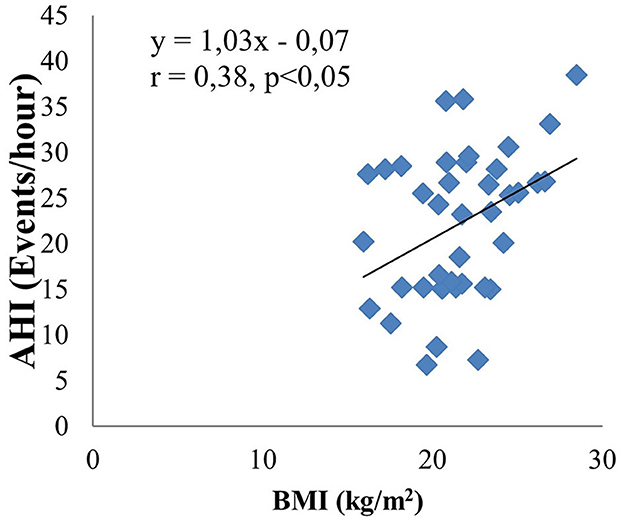
Figure 4. Correlation between AHI and BMI.
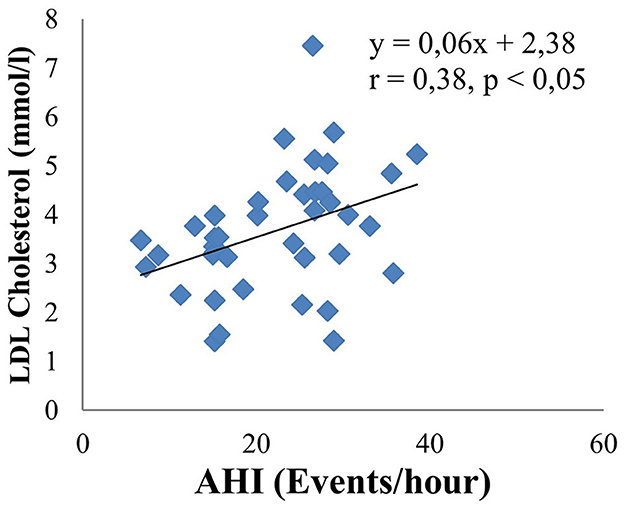
Figure 5. Correlation between AHI and LDL Cholesterol.
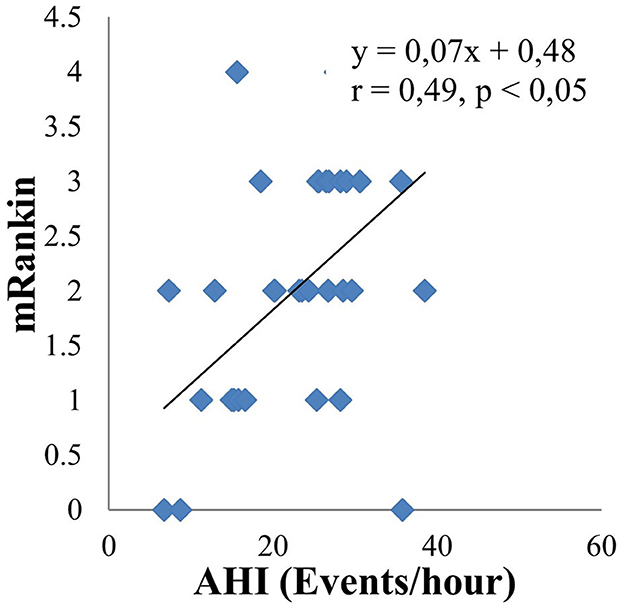
Figure 6. Correlation between AHI and mRankin.
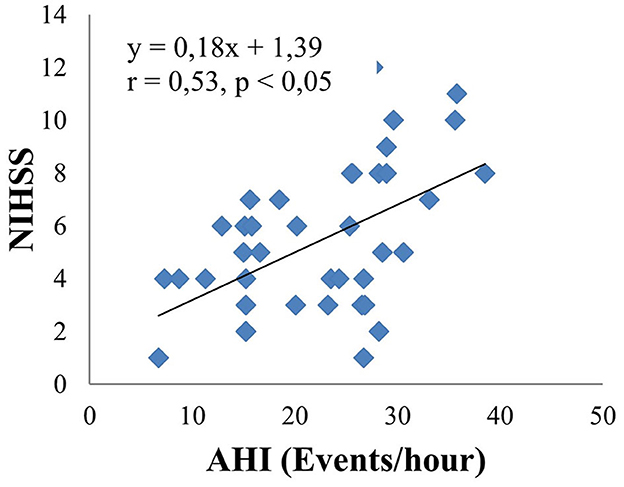
Figure 7. Correlation between AHI and NIHSS.
Regarding the general characteristics of the study subjects, this study was conducted on 56 patients with cerebral infarction with an average age of 67.70 ± 11.07. The study did not show a statistically significant age difference between the OSAS and non-OSAS groups. Age is also one of the critical risk factors for OSAS. The prevalence of OSA increases with age among adults and tends to stabilize by age 65 (20). In the OSAS group, men account for 53.6%. This result is consistent with several studies, such as the study of Asha'ari Zamzil Amin with a male-female ratio of 80/38, and author Sy Duong Quy gave the result that this ratio is 1.2/1 (2, 21). This result has been documented in the literature as the prevalence of OSA is higher in men than in women, and most population-based studies show that the prevalence of OSA is 2 to 3 times higher in men (22, 23). In fact, women often do not present with the classic symptoms of OSA (loud snoring, sleep apnea, and excessive sleepiness). They mainly complain of a lack of energy and fatigue. Sex hormones may have an important role in the pathogenesis of OSA. Evidence is that OSA is more common in post-menopausal women than in premenopausal women, and hormone replacement therapy for post-menopausal women may protect them against the disorder (24).
Our study has the result that BMI in the OSAS group is 21.56 ± 2.98 (kg/m2), statistically higher than the non-OSAS group [19.09 ± 2.37 (kg/m2) (p < 0.05)]. This result is similar to Duong Quy Sy's study with the mean BMI in the group with OSAS of 23.85 ± 3.43 (kg/m2), which is statistically significantly higher than in the non-OSAS group with 21.58 ± 2.98 (kg/m2) (p < 0.05) (2). This result shows the relation between BMI and OSAS, which is also consistent with the research results of Carmine F. et al. by finding a moderate positive correlation between BMI and AHI (r = 0.33, p < 0.001) (25). Overweight and obesity increase the severity of OSAS because fat accumulation in some areas, especially around the upper respiratory tract, easily leads to the risk of fat deposition near the pharynx causing narrowing of the upper airway; changes in neural compensatory mechanisms to maintain airway openness; the respiratory control system is unstable. In our study, the rate of overweight and obesity was 25% (23.2% in the OSAS group and 1.8% in the non-OSAS, p < 0.05).
In our study, the neck circumference in the OSAS group was 37.25 ± 1.92 (cm) higher than in the non-OSAS group. This result can be explained because neck circumference is one of the manifestations of upper body fat, which is one of the important factors of OSAS. Therefore, neck circumference is a better predictor of OSAS than waist circumference and other metabolic syndrome factors. However, the direct role of neck circumference in the pathogenesis of OSAS has not been clearly defined (26).
The lowest median SpO2 in the OSAS group was statistically significantly lower than that in the non-OSAS group (p < 0.05). The background SpO2 in the OSAS group was also significantly lower than that of the non-OSAS group (p < 0.05). The results are quite similar to a few other studies around the world. Following Mattaliano et al., the background SpO2 in the OSAS group (+) was 92.7 ± 2.9, which was statistically significantly lower than the OSAS group (–) was 94.0 ± 2.2. Meanwhile, the lowest SpO2 in the OSAS group (+) was 81.9 ± 7.6, which was statistically significant compared with the OSAS group (–) was 87.7 ± 4.3 (p < 0.01) (10).
Snoring is one of the symptoms of OSAS and has the highest prevalence in this study. It is a sound produced by the vibration of the upper respiratory tract soft tissues during sleep. A 14-year longitudinal study found that 13% of adults snore. Factors associated with snoring include male gender, obesity, smoking, and asthma. In addition, snoring is strongly associated with increased all-cause mortality (27). The study's results also have shown that excessive daytime sleepiness is higher in the OSAS group than in the non-OSAS group. This result is an important and common symptom of OSAS. Daytime sleepiness can mean losing alertness or falling asleep under inappropriate circumstances. People are considered excessively sleepy when they are not alert enough to perform the tasks of daily living.
In this study, diastolic blood pressure in the OSAS group was statistically higher than in the non-OSAS group. The study of Chen et al. in the chronic cerebral infarction group showed similar results that there was a statistical difference in hypertension between the group with OSAS and the control group (28). This result can be explained by the fact that OSAS patients with apnea sleep lead to increased sympathetic activities and endothelial dysfunction, ultimately resulting in vascular structural modifications, vasoconstriction, cardiovascular events, and hypertension (14).
The NIHSS and mRankin scores were statistically higher in the OSAS group than in the non-OSAS group. The study of Ahn et al. showed that the mRankin score in the OSAS group (1.68 ± 1.89) was statistically higher than in the non-OSAS group (1.18 ± 1.65) and this result is quite similar to our study.
Obstructive sleep apnea Syndrome is independently associated with hypertension, insulin resistance, impaired glucose tolerance, and dyslipidemia. Our results show that the concentration of total cholesterol, LDL-C in the OSAS group was statistically significantly higher than that in the non-OSAS group. The remaining indexes such as fasting intravenous glucose, HDL cholesterol, and triglyceride had no statistically significant differences between the two groups. There is a statistically significant mean positive correlation between LDL-C and AHI with the regression equation: y = 0.06x + 2.38; r = 0.38; p < 0.05. Analyzing the multivariate correlation between AHI and other factors, we found that if AHI increased by 1 event/hour, the NIHSS increased by 0.23 points. In contrast, when LDL cholesterol increased by 1 mmol/l, the NIHSS decreased by 0.78 points. In addition, the study also showed a strong positive correlation between AHI and NIHSS (r = 0.53, p < 0.05), as well as a moderate positive correlation between AHI and mRankin score (r = 0.49, p < 0.05). Therefore, it shows a correlation between the severity of sleep apnea syndrome and the severity and disability of patients with cerebral infarction through the NIHSS and mRankin scales. The mechanism of that combination can be explained as follows:
First, apnea and the resulting persistent O2 deficiency in patients with OSAS causes increased sympathetic tone and endothelial dysfunction. Vascular remodeling and vasoconstriction lead to cardiovascular complications, nocturnal hypertension, and other cardiovascular dysfunctions.
Second, oxidative stress which is produced by repeated hypoxemia and episodes of apnea leads to endothelial dysfunction and the rise of proinflammatory chemical mediators, such as Cyclooxygenase (COX-2), tumor necrosis factor-α (TNF-α), Interleukins and other pro-inflammatory chemical mediators. It easily leads to the initiation and progression of atherosclerotic plaque blood and insulin resistance.
Third, hypertension and arrhythmia, carotid intima-media thickness, and carotid atherosclerosis in the sleep apnea group are more common than in the normal group. Gonzaga found that the risk of hypertension was strongly associated with the potential severity of OSA after 4 years of follow-up (29). The blood flow in the middle cerebral artery remains unchanged due to the reaction of Angiotensin II, Noradrensine, Isoproterenol, and Bradykinin. Simultaneously, inhibition of plasminogen-1 and platelet activation leads to increased risk factors for vascular thrombosis.
There is a significant proportion of cerebral infarction patients with OSA and this should be considered if the patient has symptoms such as loud snoring during sleep, excessive daytime sleepiness and large neck circumference, and high BMI. In addition, OSA is also a factor in predicting the severity of ischemic stroke patients.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of Hue University of Medicine and Pharmacy. The patients/participants provided their written informed consent to participate in this study.
QD-M, TH-A, and SD-Q conceived the study and designed the study protocol. QD-M organized, performed the study investigations, and supported the recruitment of the patients. TH-A performed the statistical analyses. QD-M, TH-A, and NN-T-Y wrote the first draft of the manuscript. All authors have made substantial contributions, critically revised the manuscript for important intellectual content, and read and approved the final manuscript.
The authors would like to thank the Department of Cardiology, Hue University of Medicine and Pharmacy Hospital, Vietnam, for support during patient data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1132014/full#supplementary-material
OSAS, Obstructive Sleep Apnea Syndrome; AHI, Apnea-Hypopnea Index; NIHSS, National Institutes of Health Stroke Scale; AASM, American academy of sleep medicine; BMI, Body Mass Index.
1. Kohler M, Stradling JR. Mechanisms of vascular damage in obstructive sleep apnea. Nat Rev Cardiol. (2010) 7:677–85. doi: 10.1038/nrcardio.2010.145
2. Duong-Quy S, Hua-Huy T, Tran-Mai-Thi HT, Le-Dong NN, Craig TJ, Dinh-Xuan AT. Study of exhaled nitric oxide in subjects with suspected obstructive sleep apnea: a pilot study in Vietnam. Pulm Med. (2016) 2016:3050918. doi: 10.1155/2016/3050918
3. Anitua E, Duran-Cantolla J, Almeida GZ, Alkhraisat MH. Predicting the night-to-night variability in the severity of obstructive sleep apnea: the case of the standard error of measurement. Sleep Sci. (2019) 12:72. doi: 10.5935/1984-0063.20190063
4. Bittencourt LRA, Suchecki D, Tufik S, Peres C, Togeiro SM, Bagnato MDC, et al. The variability of the apnoea–hypopnoea index. J Sleep Res. (2001) 10:245–51. doi: 10.1046/j.1365-2869.2001.00255.x
5. Arnold J, Sunilkumar M, Krishna V, Yoganand SP, Kumar MS, Shanmugapriyan D. Obstructive sleep apnea. J Pharmacy Bioallied Sci. (2017) 9(Suppl. 1):S26. doi: 10.4103/jpbs.JPBS_155_17
6. Slowik JM, Sankari A, Collen JF. Obstructive Sleep Apnea, in StatPearls. StatPearls Publishing (2022).
7. Feigin VL, Stark BA, Johnson CO, Roth GA, Bisignano C, Abady GG, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. (2021) 20:795–820. doi: 10.1016/S1474-4422(21)00252-0
8. Kim J, Kim Y, Yang KI, Kim DE, Kim SA. The relationship between sleep disturbance and functional status in mild stroke patients. Ann Rehabil Med. (2015) 39:545–52. doi: 10.5535/arm.2015.39.4.545
9. Ahn SH, Kim JH, Kim DU, Choo IS, Lee HJ, Kim HW. Interaction between sleep-disordered breathing and acute ischemic stroke. J Clin Neurol. (2013) 9:9–13. doi: 10.3988/jcn.2013.9.1.9
10. Mattaliano P, Lombardi C, Sangalli D, Faini A, Corrà B, Adobbati L, et al., Impact of obstructive sleep apnea on cardiac organ damage in patients with acute ischemic stroke. J Hypertens. (2018) 36:1351–9. doi: 10.1097/HJH.0000000000001697
11. Zhang L, Meng R, Shang S, Wu C, Wu D, Shang S, et al. Obstructive sleep apnea before ischemic stroke: clinical relevance to infarction volume and neurological recovery. J Stroke Cerebrovasc Dis. (2019) 28:2132–9. doi: 10.1016/j.jstrokecerebrovasdis.2019.04.008
12. McEvoy RD, Antic NA, Heeley E, Luo Y, Ou Q, Zhang X, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. (2016) 375:919–31. doi: 10.1056/NEJMoa1606599
13. Camilo MR, Schnitman SV, Sander HH, Eckeli AL, Fernandes RM, Leite JP, et al. Sleep-disordered breathing among acute ischemic stroke patients in Brazil. Sleep Med. (2016) 19:8–12. doi: 10.1016/j.sleep.2015.11.008
14. Gupta A, Shukla G, Afsar M, Poornima S, Pandey RM, Goyal V, et al. Role of positive airway pressure therapy for obstructive sleep apnea in patients with stroke: a randomized controlled trial. J Clin Sleep Med. (2018) 14:511–21. doi: 10.5664/jcsm.7034
15. McNicholas WT. Diagnosis of obstructive sleep apnea in adults. Proc Am Thorac Soc. (2008) 5:154–60. doi: 10.1513/pats.200708-118MG
16. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. Sleep. (1999) 22:667–89. doi: 10.1093/sleep/22.5.667
17. Oppenheimer S, Hachinski V. Complications of acute stroke. Lancet. (1992) 339:721–4. doi: 10.1016/0140-6736(92)90607-5
18. Kogan E, Twyman K, Heap J, Milentijevic D, Lin JH, Alberts M. Assessing stroke severity using electronic health record data: a machine learning approach. BMC Med Inform Decis Making. (2020) 20:1–8. doi: 10.1186/s12911-019-1010-x
19. Uyttenboogaart M, Luijckx G-I, Vroomen PCAJ, Stewart RE, De Keyser J. Measuring disability in stroke: relationship between the modified Rankin scale and the Barthel index. J Neurol. (2007) 254:1113–7. doi: 10.1007/s00415-007-0646-0
20. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. (2002) 165:1217–39. doi: 10.1164/rccm.2109080
21. Asha'ari ZA, Hasmoni MH, Ab Rahman J, Yusof RA, Lope Ahmad RAR. The association between sleep apnea and young adults with hypertension. Laryngoscope. (2012) 122:2337–42. doi: 10.1002/lary.23379
22. Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. (2008) 5:136–43. doi: 10.1513/pats.200709-155MG
23. Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, et al., Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev. (2017) 34:70–81. doi: 10.1016/j.smrv.2016.07.002
24. Garvey JF, Pengo MF, Drakatos P, Kent BD. Epidemiological aspects of obstructive sleep apnea. J Thorac Dis. (2015) 7:920. doi: 10.3978/j.issn.2072-1439.2015.04.52
25. Gervasio CF, Riva G, Cicolin A, Caranzano F, Frigiolini F, Canale A, et al., Clinical and polygraphic features of obstructive sleep apnea syndrome in adult patients. Otorinolaringologia. (2018) 68:33–7. doi: 10.23736/S0392-6621.17.02128-2
26. Ahbab S, Ataoglu HE, Tuna M, Karasulu L, Cetin F, Temiz LU, et al., Neck circumference, metabolic syndrome and obstructive sleep apnea syndrome; evaluation of possible linkage. Med Sci Monitor. (2013) 19:111. doi: 10.12659/MSM.883776
27. Al-Jewair TS, Nazir MA, Al-Masoud NN, Alqahtani ND. Prevalence and risks of habitual snoring and obstructive sleep apnea symptoms in adult dental patients. Saudi Med J. (2016) 37:183. doi: 10.15537/smj.2016.2.12852
28. Chen CY, Chen CL, Yu CC, Chen TT, Tseng ST, Ho CH. Association of inflammation and oxidative stress with obstructive sleep apnea in ischemic stroke patients. Sleep Med. (2015) 16:113–8. doi: 10.1016/j.sleep.2014.07.027
Keywords: obstructive sleep apnea syndrome (OSAS), OSA, apnea-hypopnea index (AHI), stroke, respiratory polygraphy
Citation: Hoang-Anh T, Duong-Minh Q, Nguyen-Thi-Y N and Duong-Quy S (2023) Study of the obstructive sleep apnea syndrome in cerebral infarction patients. Front. Neurol. 14:1132014. doi: 10.3389/fneur.2023.1132014
Received: 26 December 2022; Accepted: 02 May 2023;
Published: 21 June 2023.
Edited by:
Giuseppe Magliulo, Sapienza University of Rome, ItalyReviewed by:
Fang Han, Peking University People's Hospital, ChinaCopyright © 2023 Hoang-Anh, Duong-Minh, Nguyen-Thi-Y and Duong-Quy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tien Hoang-Anh, aGF0aWVuQGh1ZXVuaS5lZHUudm4=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.