 Zhihou Liang1†
Zhihou Liang1† Chuanzhou Li
Chuanzhou Li Zhijun Liu
Zhijun Liu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 27 March 2023
Sec. Dementia and Neurodegenerative Diseases
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1119326
Background: Mutations in the presenilin-1 (PSEN1), presenilin-2 (PSEN2), and amyloid precursor protein (APP) genes have been commonly identified in early-onset Alzheimer's disease (EOAD). Some of the mutations in the three causative genes, especially the PSEN1 gene, result in variable phenotypes and exhibit clinical heterogeneity among EOAD families.
Methods: Using next-generation sequencing (NGS), we performed genetic screening in a Chinese cohort of 18 patients with EOAD, consisting of five familial EOAD and 13 sporadic cases.
Results: We identified two likely pathogenic PSEN1 mutations (one novel) and a novel APP mutation in three cases of EOAD, where two are familial and one is sporadic, respectively. In addition, we detected a few variants of uncertain significance (VUS) in several genes, including not only the two known variants in PSEN2 (p.H169N and p.V214L) but also genes causal of other types of dementia or previously identified as risk factors for AD, suggesting the possible involvement of multiple genes in the etiopathology of AD. The patients carrying PSEN1 mutations had an earlier mean age at the onset than those with PSEN2 or APP variants. The initial symptoms varied greatly among patients in the EOAD cohort, from progressive memory impairment and epilepsy to uncommon motor symptoms such as involuntary tremors in the upper extremities.
Conclusions: In conclusion, our study provides further evidence of the genetic profile of patients with EOAD from China and expands the mutation spectrum of both PSEN1 and APP. In addition, our results highlight the clinical heterogeneity in patients with EOAD and mutations in PSEN1, PSEN2, and APP and suggest strong effects of genetic variants on clinical phenotypes. Future functional studies are needed to clarify the interaction between AD-causative gene mutations and phenotypic heterogeneity.
Alzheimer's disease (AD) is a devastating neurodegenerative disease, characterized by progressive memory loss and deficits of other cognition domains that may impair daily functioning as well as define pathological changes with abnormal extracellular aggregates of amyloid-β and hyperphosphorylation of neuronal tau. AD is the most common cause of dementia, affecting ~44 million people worldwide (1). According to the age of onset, AD can be divided into two subtypes: early-onset AD (EOAD) and late-onset AD (LOAD). EOAD is typically defined as onset occurring before the age of 65 years and accounts for ~5–10% of all cases of AD, while LOAD represents the much more common type of dementia affecting individuals aged 65 years and above. Patients with EOAD tend to display an atypical clinical presentation (e.g., visual dysfunction, aphasia, executive dysfunction, apraxia, and spastic paraparesis) (2) and have a more aggressive disease progression and a shorter survival time than patients with LOAD (3). The exact pathogenic mechanisms that underlie AD remains largely unknown, and no effective disease-modifying therapeutic interventions are currently available for AD.
Both LOAD and EOAD have a high heritability, estimated to be 70–80% and 92–100%, respectively (4). Approximately 90–95% of patients with EOAD appear to be sporadic, whereas the remaining 5–10% of cases are familial and have dominant inherited mutations in amyloid protein precursor (APP), presenilin-1 (PSEN1), and presenilin-2 (PSEN2). Mutations in all three genes are known to cause enhanced production and deposition of amyloid beta (Aβ). Advances in next-generation sequencing (NGS) and its wide applications enable the rapid identification of a growing number of pathogenic variants or mutations associated with AD. To date, more than 450 mutations have been reported in the three causative genes that result in familial AD (FAD). Among them, PSEN1 gene mutations are responsible for ~75% of genetic EOAD cases (https://www.alzforum.org/mutations). However, cases of high-penetrant mutations in these three genes could explain only 5–10% of EOAD cases, leaving a large group of EOAD families unexplained genetically (5). The genetics of LOAD are much less well-understood compared to EOAD, with a highly polygenic architecture of complex traits. The ε4 allele of the apolipoprotein E (APOE) gene has been recognized as the strongest genetic risk factor for LOAD, with a 2–3 times increase in risk in heterozygous and a 15 times increase in homozygous (5). More recently, a large genome-wide association study (GWAS) has identified 75 independent risk loci for AD and related dementias (ADD), of which 33 have been previously reported to be associated with ADD (6). Pathway-enrichment analysis supported the involvement of microglia in AD, perhaps by modulating Aβ aggregation/degradation (6).
Genotype–phenotype relationships have previously been examined for APP (7), PSEN1 (8, 9), and PSEN2 mutations (10), but at present, no clear pattern of genotype–phenotype correlation has been well-established in AD. In general, the age at onset (AAO) of AD is relatively consistent within families carrying the same FAD-linked mutations but differs markedly between individuals carrying different mutations. Patients with PSEN1 mutations are seen to manifest an early symptom onset, with a mean AAO of 8.4 years earlier than in APP mutation carriers (42.9 vs. 51.3 years) and 14.2 years earlier than in PSEN2 cases (57.1 years) (11). The mean duration of symptoms in PSEN1-related AD families is significantly shorter (ranging from 5.8 to 6.8 years) than in PSEN2 (ranging from 4.4 to 10.8 years) and APP mutations carriers (ranging from 9.0 to 16 years), indicating that the severity of disease is associated with specific PSEN1 mutations. Moreover, Ryan et al. (12) analyzed the genotype and phenotype correlation for autosomal dominant familial AD in the UK and Ireland populations. The researchers emphasized the phenotypic heterogeneity of familial AD and suggested that high variability in AAO and clinical presentations were determined by specific mutations as well as by causative genes (12).
Although a growing number of pathogenic mutations in APP, PSEN1, and PSEN2 have been identified for EOAD families, the identification of additional EOAD-causative genes remains challenging. In this study, we conduct targeted panels and whole-exome sequencing (WES) in a cohort of patients with EOAD from the central-southern region of China, with an emphasis on the evaluation of the genetic spectrum and clinical features of patients with clinically suspected EOAD.
This cohort consisted of 18 patients, including 12 (66.7%) men and six women (33.3%), clinically diagnosed with EOAD with a mean onset age of 48.9 ± 6.1 years (ranging from 32 to 60 years). In total, 27.8% (5/18) of patients had a positive family history of dementia. All patients were of Han Chinese origin and were recruited from the neurology department of Wuhan Union hospital and from the central-southern region of China between March 2018 and September 2022. All affected patients were evaluated by at least two neurologists and were diagnosed according to the National Institute of Aging-Alzheimer's Association criteria (13). All patients underwent a comprehensive neurological assessment, including past medical history, family history, and neuropsychological assessment. Cerebrospinal fluid (CSF) and topographical markers (18F-AV-45 PET-CT) were assessed as well in 72.2% (12/18) and 22.2% (4/18) of all subjects, respectively. Written informed consent was obtained from all participants.
Genomic DNA was extracted from peripheral blood samples using a standard extraction method. The whole-exome sequencing (WES) and targeted panels comprising 168 genes potentially associated with AD and other types of dementia were used to perform comprehensive genomic testing. Sequencing was performed using the Illumina Hiseq2000/2500 system. Sequenced data analysis was carried out as described previously (14). Sanger sequencing was used to validate the candidate variants after variant calling and filtering. Co-segregation analysis of variants was performed in the families with available DNA samples.
In general, ~98.57% of the target bases were covered with at least 30 × per individual, and the mean depth of coverage for all target regions was 177.39. Only those protein function-altering variants with a low minor allele frequency in the datasets from 1,000 Genomes, ESP5400, and ExAC were retained after filtering and were assumed to be pathogenic. Finally, we identified five potentially pathogenic variants in APP, PSEN1, and PSEN2, including a novel pathogenic APP mutation (c.2061A > C, p.K687N), two pathogenic PSEN1 mutations (p.I143T and p.L235dup), and two known variants of uncertain significance (VUS) in PSEN2 (p.H169N, and p.V214L) in five unrelated EOAD families (Table 1). All of these variants were confirmed by Sanger sequencing (Figure 1). The novel mutation (p.L235dup) in PSEN1 was not found in the public genetic variant database. Segregation analysis revealed that the two known missense variants (APP p.K687N and PSEN2 p.H169N) were co-segregated through their other family members. In addition, we also detected another three VUS in several autosomal dominant genes which can lead to other types of dementia or are recognized as risk factors for AD, such as GRN and SORL1 (Table 1).
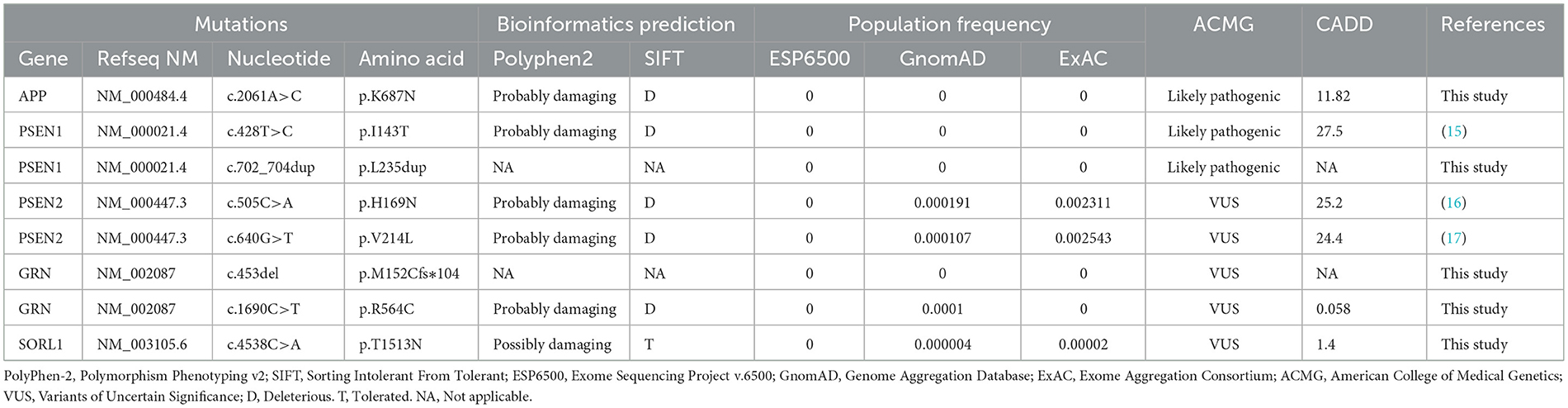
Table 1. Rare variants in AD-related genes identified in this study.
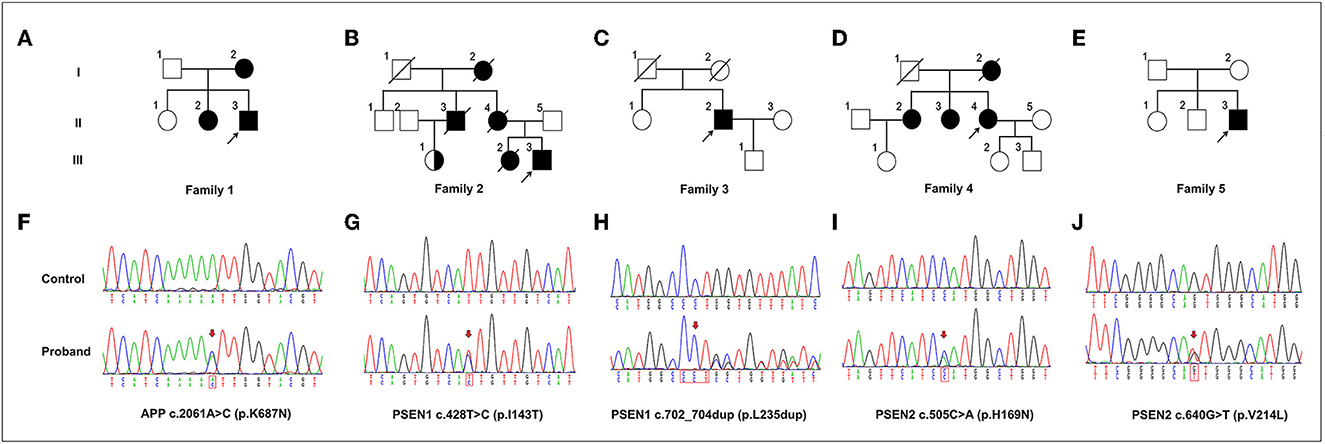
Figure 1. The variants in APP, PSEN1, and PSEN2 genes identified in this study. (A–E) Pedigrees carrying the variants in APP, PSEN1, and PSEN2. Arrows indicate the proband of each family. (F–J) Sequencing chromatograms of the identified variants in APP (p.K687N), PSEN1 (p.I143T and p.L235dup), and PSEN2 (p.H169N and p.V214L). Arrows indicate the variant sites.
We analyzed the possible effects of mutations using the complex structure of amyloid precursor protein and human gamma-secretase (PDB ID: 6IYC) (Figure 2). The structure model suggests that the K687N mutation in APP likely impairs the direct interaction with nicastrin in the complex. The L235 residue in presenilin-1 is embedded inside the transmembrane domain and is close to the binding APP; as a result, the duplication of PS1-L235 residue may affect the stability of the transmembrane complex or the processing of APP via direct binding.
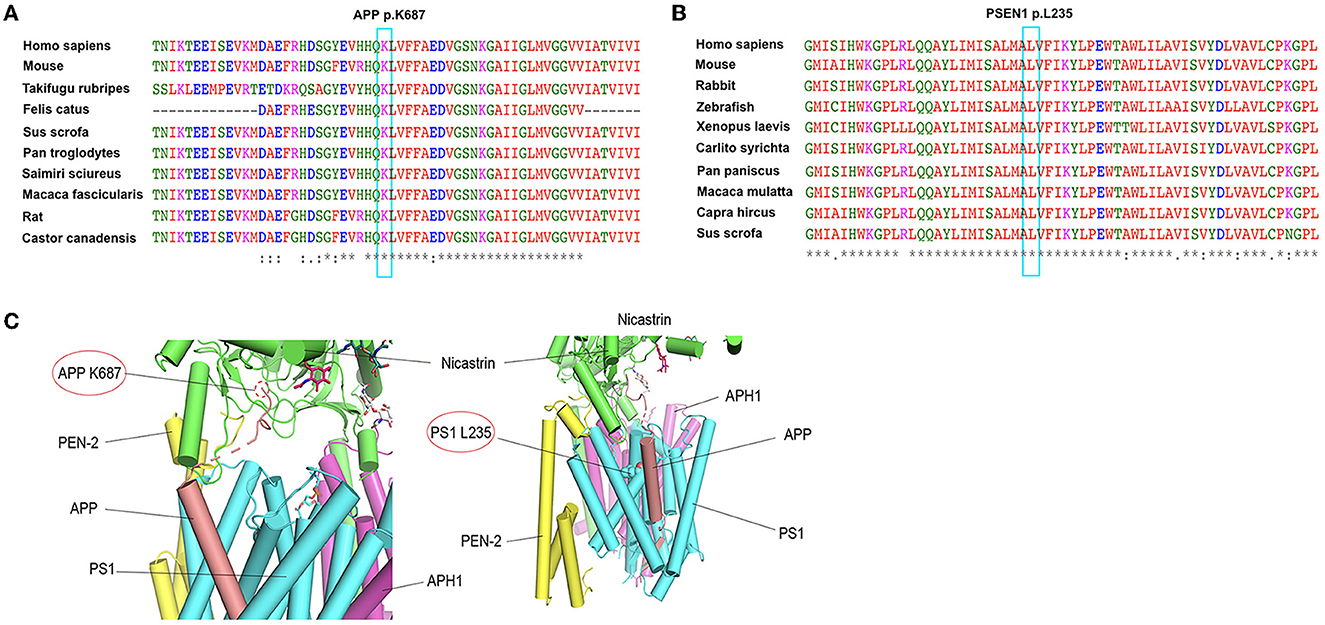
Figure 2. Conservation analysis of the two mutations (APP K687N and PSEN1 L235dup) and protein structure prediction. (A) Alignment of APP sequences from different species. Arrow indicates the mutation site. (B) Alignment of PSEN1 sequences from different species. Arrow indicates the mutation site. (C) The possible effects of two mutations, APP K687N and PSEN1 L235dup, using the complex structure of Amyloid Precursor Protein and Human gamma-secretase (PDB ID: 6IYC).
Of the five patients with identified mutations in APP, PSEN1, and PSEN2, the mean AAO was 44.8 ± 7.9 years and 40% (2/5) of patients were women. The clinical characteristics of these patients are summarized in Table 2. The main clinical presentations of EOAD in our cohort include memory impairment, psychosocial and behavioral problems, epilepsy, and rare tremors, consistent with other previously reported EOAD cases. However, there is no difference in the amyloid/tau profile between cases of familial AD and others with sporadic AD. The clinical manifestations of patients are described in detail later.
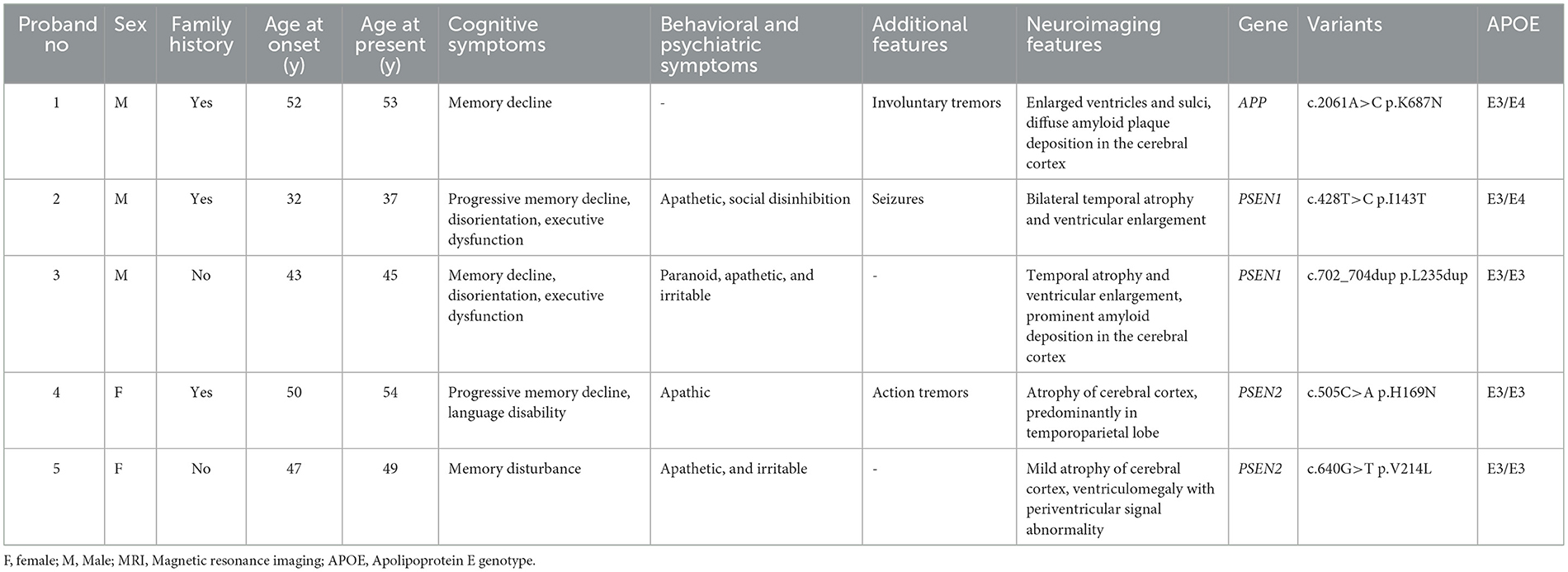
Table 2. The clinical characteristics and genetic analysis of five probands carrying mutations in APP, PSEN1, and PSEN2.
Proband 1 (II:3) was a 53-year-old man, carrying the c.2061A > C (p.K687N) mutation in APP, who was initially admitted to our inpatient ward because of short-term memory impairment within 1 year. He had difficulty figuring out how to put on his clothes and finding his way to a familiar place. Involuntary resting tremors of both upper extremities appeared frequently and progressed gradually. He scored 22/30 on the mini-mental state examination (MMSE) and 20/30 on the Montreal Cognitive Assessment (MoCA). MRI scans revealed enlarged ventricles and sulci, indicating generalized cerebral atrophy. Brain AV-45 PET-CT scans showed diffuse amyloid plaque deposition in the cerebral cortex, particularly in the occipital cortical areas (Figure 3D). The levels of Aβ42 and Aβ40 in the CSF were 4.1 pg/mL (≥651) and 242.8 pg/mL, respectively, and those of total tau and phosphorylated tau were 628 pg/mL (<290) and 87.2 pg/mL (≤61), respectively. A similar onset age and memory impairment phenotype were described in his affected mother (I:2) and older sister (II:2). Genetic analysis revealed that both his mother and sister carry the same mutation.
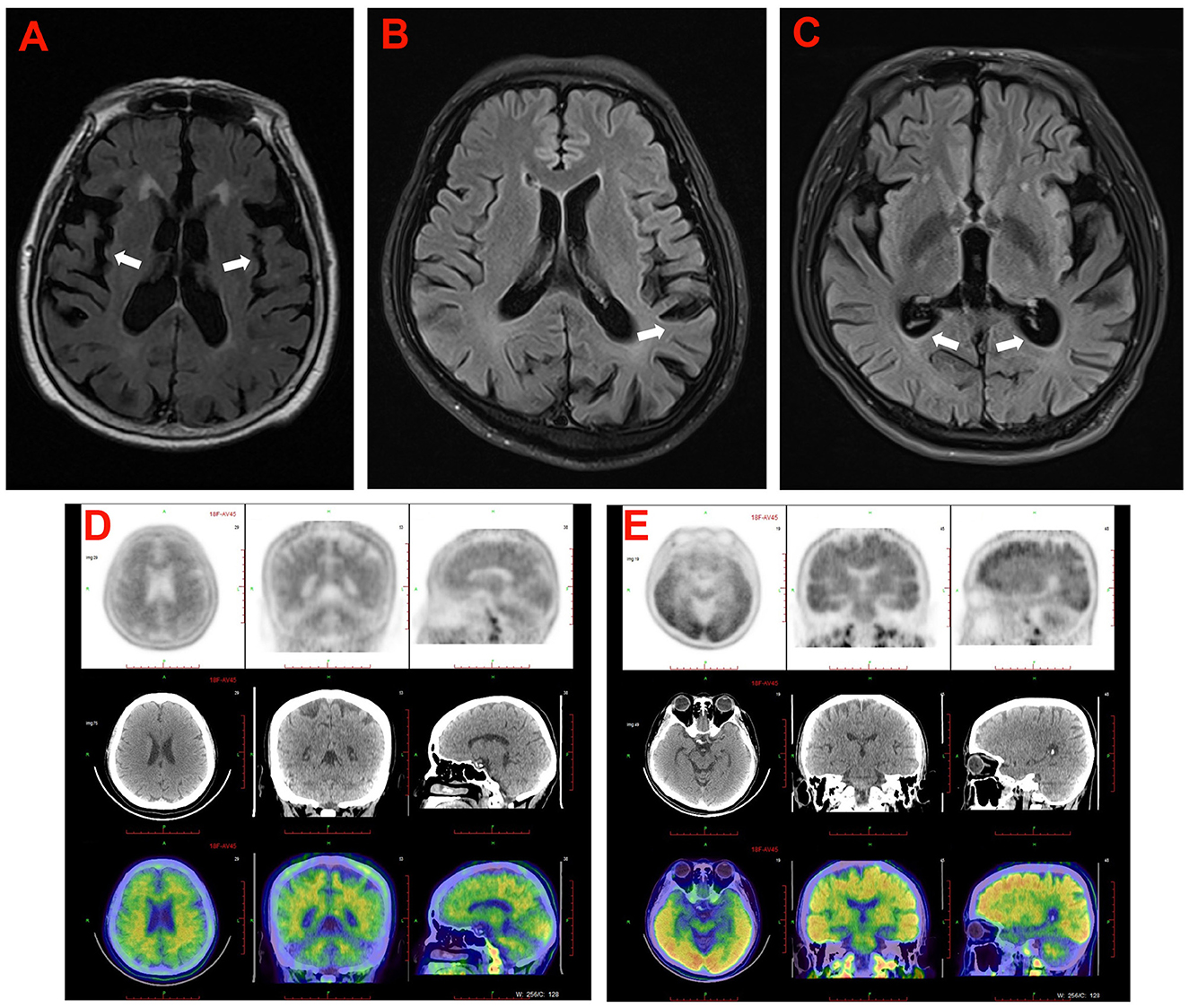
Figure 3. The cranial neuroimaging of the probands in the five families. (A) The T2 weighed image showed atrophy of cerebral cortex (arrowhead) and mild ventriculomegaly with periventricular signal abnormality in proband (II-3) in family 5. (B) The T2 FLAIR image showed atrophy of cerebral cortex (arrowhead) predominantly in temporoparietal lobe of the proband (II-4) in family 4. (C) The T2 FLAIR image showed atrophy of cerebral cortex (arrowhead) and mild ventriculomegaly in proband (III-3) of family 2. (D, E) 18F-AV45 brain images of the proband (II-3) in family 1 (D), and the proband (II-2) in family 3 (E).
Proband 2 (III:3) in family 2, carrying the c.428T > C (p.I143T) mutation in PSEN1, was a 37-year-old man who was admitted to our department because of a 5-year history of cognitive decline. The patient initially complained of problems with recalling recent events, frequent oversights, and word-finding difficulty. After 2 months, he developed generalized seizures. His seizures were well controlled with the antiepileptic drug carbamazepine. During the following years, the cognitive disturbances progressively worsened, and he gradually became more apathetic and socially disinhibited, with less spontaneous speech. His MMSE score was 17/30 at 34 years of age. Neurological examination showed disorientation, comprehension deficits, slurred speech, and severe impairment in episodic memory and executive functions. The patient's medical record was unremarkable, except for a history of illicit drug addiction. Brain MRI showed significant temporal lobe atrophy and ventricular enlargement (Figure 3C). The family history revealed that the proband's mother (II:4) and older sister (III:2) experienced similar symptoms at 45 and 34 years of age, respectively, and his grandmother (I:2) had died at 60 years of age, with an onset at 48 years. Unfortunately, the proband's mother and older sister are no longer available because they have passed away. The proband's cousin (III:1) also had the same mutation but was clinically asymptomatic.
Proband 3 (II:2) in family 3, carrying a duplication mutation (c.702_704dup and p.L235dup) in the PSEN1 gene, was a 45-year-old man who was admitted to our department because of a 2-year history of cognitive decline. The patient complained of frequent memory problems, including difficulty in word finding and remembering recent events. His daily tasks and activities appear to be affected as well. After 1 year, he exhibited behavioral symptoms such as paranoia, apathy, and irritability. The scores of the MMSE and MoCA tests were 22/30 and 18/30, respectively. Neurological examination revealed mild impairment in disorientation, spatial memory, and executive functions. Brain MRI revealed conspicuous hippocampal atrophy and ventricular enlargement. Brain AV-45 PET-CT scans showed prominent amyloid deposition in the frontal, temporal, parietal, and occipital cortical areas (Figure 3E). There was no history of AD or other neurological diseases in his family. His father and mother died from heart disease and lung cancer, respectively, before the age of 65 years. DNA testing could not be carried out because his parents' DNA was no longer available.
Proband 4 (II:4) was a 54-year-old woman, carrying a known missense variant (c.505C>A, p.H169N) in PSEN2, who presented with fast shaking of her left leg at the age of 50 years, that had started insidiously and had progressively worsened over the last half year, eventually resulting in involuntary trembling of the whole body. The shaking occurred mainly during activities and was relieved by resting. There were no significant findings on neurologic examination at that time. Thus, an initial diagnosis of essential tremors was made. From the age of 52 years, she gradually exhibited forgetfulness, apathy, and non-fluent speech. Physical examination revealed deficits in episodic memory and slurred speech, together with pronounced tremors when holding her arms outstretched and incoordination in movements. She scored 21/30 on the MMSE test. Brain MRI revealed a prominent atrophy of the cerebral cortex, predominantly in the temporoparietal lobe (Figure 3B). Family analysis revealed that her two older sisters (II:2 and II:3) carried the same variant and experienced similar tremor symptoms in their early 50s. The proband's mother (I:2) had similar phenotypes and died at the age of 58 years, with an onset at 45 years.
Proband 5 (II:3) was a 49-year-old man, carrying a heterozygous missense variant (c.640G > T, p.V214L) in PSEN2, who had problems with memory disturbance. In the past 2 years, he gradually became forgetful, apathetic, and irritable. Brain MRI revealed mild atrophy of the cerebral cortex and mild ventriculomegaly with periventricular signal abnormality (Figure 3A). Decreased levels of Aβ42 (339.73 pg/mL) and an elevation in tau species (p-tau 93.14 pg/mL) were observed in the CSF of the proband. There was no medical record of dementia or other neurological disorders in his family members. His father and mother refused to take genetic testing.
We identified three different variants of uncertain significance in GRN and SORL1. Of these variants, the c.453del (p.M152Cfs*104) variant in GRN was found in a sporadic AD case, who developed memory disturbance and apathy at the age of 54 years. The other GRN variant, R564C, was identified in a sporadic patient who was diagnosed with AD at 62 years of age. It is noteworthy that the SORL1 variant, c.4384T > G (p.F1462V), has been identified in a sporadic case with AD who became forgetful at the age of 47 years and progressed to dementia at 51 years of age.
Early-onset Alzheimer's disease represents a highly genetically heterogeneous group of progressive dementia that overlaps in its clinical presentation with LOAD. Characterization of the clinical and genetic determinants of EOAD is crucial for fully understanding the etiology of AD and developing more effective targets for prevention and treatment. In our EOAD cohort, we found that 40% (2/5) of familial EOAD and 7.69% (1/13) of sporadic EOAD patients carried pathogenic or likely pathogenic variants, including a known pathogenic PSEN1 mutation and two novel pathogenic mutations in PSEN1 and APP, respectively. We also detected two known VUS in PSEN2 (p.H169N and p.V214L). In addition, we found some rare variants in several genes, either causal for other types of dementia or previously identified as risk factors for AD, suggesting the possible involvement of multiple genes in the etiopathology of AD. The two variants, GRN R564C and SORL1 p.T1513N, may be risk factors for AD clinical phenotypes. Based on our findings, the majority of cases (at least 13/18, 72.22%) in the cohort still remain genetically unexplained, which may also contribute to the missing genetic etiology of EOAD.
The mean AAO (44.8 ± 7.9 years) in our patients with identified mutations in APP, PSEN1, and PSEN2 was similar to that previously described in a Chinese cohort (18). Our study verified that families carrying PSEN1 mutations have an earlier mean AAO than those with APP or PSEN2 variants. In the present study, we identified a novel PSEN1 mutation, p.L235dup, associated with EOAD. The mutation frequency was absent in any public databases, indicating that this mutation is very rare. Unfortunately, both parents are not available for genetic testing in this case because they have passed away. Remarkably, three known missense mutations (L235V/L235P/L235R) at the same residue of PSEN1 have been previously reported in patients with EOAD in different populations (19–21). Yang et al. (22) reported that transgenic mice expressing PSEN1-L235P showed an increased production of Aβ, together with increased phosphorylation of tau and synaptic protein loss. Therefore, based on the 2015 American College of Medical Genetics and Genomics/Association for Molecular Pathology (ACMG/AMP) guidelines, the p.L235dup mutation was classified as pathogenic. In addition to having an earlier onset, patients with PSEN1 mutations more frequently manifested atypical cognitive symptoms and additional neurological features (behavioral change, language impairment, dyscalculia or executive impairment, myoclonus, seizures, pyramidal, extrapyramidal, or cerebellar signs) when compared to APP mutation carriers (12). It was reported that PSEN1 mutations occurring after codon 200 were more frequently associated with spastic paraparesis and visuospatial impairment as well as an earlier AOO, while mutations before codon 200 were more frequently associated with seizures and myoclonus (23, 24). In our cohort, the proband with the p.I143T mutation developed seizures and bradykinesia in his 30s, while the p.L235dup mutation carrier exhibited typical patterns of memory loss and behavioral change. The known mutation in PSEN1 p.I143T has been found in several families worldwide, with the age of onset between 30 and 41 years, but clinical phenotypes of mutations were different in these families (15, 25, 26). Most of these carriers presented with typical AD symptoms, including memory impairment, disorientation, dyspraxia, and dysphasia. In the later stages of the disease, patients with this mutation may develop movement disorders (limb apraxia, rigidity, dystonia, myoclonus, or seizures) as well as paranoid delusions, hallucinations, and aggressiveness. However, our patient with the same mutation initially presented with seizures for 3 months, followed by apraxia and rigidity, which were rarely reported in the early stage of the disease or as initial symptoms. Together, our data suggest that PSEN1 mutations are associated with very early disease onset and a variable phenotype.
Unlike PSEN1 carriers, mutations in PSEN2 cause AD with milder phenotypes and later onset age (27). Some PSEN2 mutation carriers may exhibit variable clinical phenotypes of AD. The known variant in PSEN2, p.H169N, has been found in several individuals of East Asian ancestry (15, 28, 29). The variant was classified as VUS, with higher frequency in a much higher population frequency in East Asian ancestry. It is essential to establish the relationship between the PSEN2 variant, p.H169N, and AD; functional assessment of this variant may be required. The p.H169N carriers were reported to experience typical AD symptoms with memory decline at the beginning. In this study, we present an EOAD family carrying the p.H169N variant in which, on initial presentation, the affected individuals had symptoms of uncommon action tremors. Symptoms such as forgetfulness, apathy, and speech impairment developed later during the development of this disease. Although rare, extrapyramidal signs may also be observed in the early stage of EOAD or as initial symptoms. Our findings extend the current knowledge of the phenotypic heterogeneity of EOAD families carrying the PSEN2 variant, p.H169N. In addition, the PSEN2 p.V214L variant has also been reported in many East Asian ethnic groups, with prominent memory impairment and visuospatial deficits which commonly occur between 48 and 69 years of age (15, 17, 30, 31). Although structural changes were predicted in silico, the pathogenicity of the PSEN2 variant, p.V214L, associated with EOAD was questioned, based on its much higher frequency in the East Asian population. This variant was reported as either disease-causing with reduced penetrance or as a risk factor for EOAD (32). Therefore, functional assessment of the variant (PSEN2 p.V214L) is required to establish its pathogenicity in EOAD.
The heterozygous mutation in APP (c.2061A>C, p.K687N) was first identified in our study, and this mutation was found to co-segregate with the disease in family 1. Another variant (c.2061A > T, p.K687N) affecting the same amino acid sequence of APP was previously reported as a pathogenic variant in a German EOAD family, which exhibited a similar phenotype to the family in our study (33). In vitro functional studies provide some evidence that the p.K687N mutation may have a damaging effect on protein function (33). The p.K687N mutation was not classified by Alzforum and this variant was previously observed in a single-affected family without any evidence of co-segregation. Moreover, a known mutation, p.K687Q, at the same residue has been previously reported in two unrelated Chinese EOAD families (18, 34). Thus, this variant was re-classified as a pathogenic/likely pathogenic variant, based on the 2015 ACMG-AMP criteria. In addition to a decline in progressive memory, other rare motor symptoms, such as rest tremors, were also observed in our patient during the course of the disease. Scarmeas et al. (35) found that motor decline, for example, in speech/facial expression, rigidity, bradykinesia, or posture/gait occurs frequently and progresses rapidly in AD, but that tremors were less frequent throughout the course of the disease. To the best of our knowledge, isolated rest tremors have not yet been reported in patients with APP-related EOAD. Our findings expand the phenotypic spectrum of APP-related EOAD.
There were still some limitations to this study that need to be noted. First, we failed to perform screening of copy number variation (deletions or duplications) in the prion protein gene (PRNP), C9ORF72 (chromosome 9 open reading frame 72), and APP, which might be responsible for a proportion of EOAD and other types of dementia (36–38). The second limitation is the lack of functional assessment of the potentially pathogenic variants. Third, it should be noted that intronic variants might participate in the genetic determinism of both familial EOAD and sporadic forms. For negatively screened families and sporadic cases, whole-genome sequencing may be helpful for the identification of additional causative genes and for expanding our understanding of genetic mechanisms in EOAD.
In summary, our study provides further evidence of the genetic profile of patients with EOAD from China and expands the mutation spectrum of both PSEN1 and APP. In addition, our results highlight the clinical heterogeneity in patients with EOAD and mutations in PSEN1, PSEN2, and APP and suggest the strong effect of genetic variants on clinical phenotypes. Next-generation techniques provide a useful means to investigate the genetic determinants in clinical cases showing heterogeneous clinical presentation and reduced penetrance. Future functional studies are needed to clarify the interaction between causative gene mutations and phenotypic heterogeneity.
The data presented in the study has been deposited in the DDBJ repository, https://getentry.ddbj.nig.ac.jp/, accession numbers LC756953 and LC756954.
The studies involving human participants were reviewed and approved by Ethics Committee of Wuhan Union Hospital. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
ZLia and YW: data acquisition and analysis, visualization, and writing the original draft. ZLiu and CL: study design and conceptualization, data analysis, writing–review and editing, and funding acquisition. All authors contributed to the article and approved the submitted version.
This study was supported by Grants from the National Natural Science Foundation of China to ZLiu (82101504) and Grants from the National Natural Science Foundation of China (32070961) to CL.
The authors thank the participants for their help and support. We thank Prof. Hong jun Yu for the help in the structure prediction of new variations.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Dumurgier J, Sabia S. Epidemiology of Alzheimer's disease: latest trends. Rev Prat. (2020) 70:149–51.
2. van der Flier WM, Pijnenburg YA, Fox NC, Scheltens P. Early-onset versus late-onset Alzheimer's disease: the case of the missing APOE varepsilon4 allele. Lancet Neurol. (2011) 10:280–8. doi: 10.1016/S1474-4422(10)70306-9
3. Bateman RJ, Aisen PS, De Strooper B, Fox NC, Lemere CA, Ringman JM, et al. Autosomal-dominant Alzheimer's disease: a review and proposal for the prevention of Alzheimer's disease. Alzheimers Res Ther. (2011) 3:1. doi: 10.1186/alzrt59
4. Wingo TS, Lah JJ, Levey AI, Cutler DJ. Autosomal recessive causes likely in early-onset Alzheimer disease. Arch Neurol. (2012) 69:59–64. doi: 10.1001/archneurol.2011.221
5. Hoogmartens J, Cacace R, Van Broeckhoven C. Insight into the genetic etiology of Alzheimer's disease: a comprehensive review of the role of rare variants. Alzheimers Dement. (2021) 13:e12155. doi: 10.1002/dad2.12155
6. Bellenguez C, Kucukali F, Jansen IE, Kleineidam L, Moreno-Grau S, Amin N, et al. New insights into the genetic etiology of Alzheimer's disease and related dementias. Nat Genet. (2022) 54:412–36. doi: 10.1038/s41588-022-01024-z
7. Liu Y, Xiao X, Liu H, Liao X, Zhou Y, Weng L, et al. Clinical characteristics and genotype-phenotype correlation analysis of familial Alzheimer's disease patients with pathogenic/likely pathogenic amyloid protein precursor mutations. Front Aging Neurosci. (2022) 14:1013295. doi: 10.3389/fnagi.2022.1013295
8. Larner AJ. Genotype-phenotype correlation in early-onset Alzheimer disease with presenilin 1 gene mutations. Arch Neurol. (2004) 61:801. doi: 10.1001/archneur.61.5.801-a
9. Larner AJ. Presenilin-1 mutations in Alzheimer's disease: an update on genotype-phenotype relationships. J Alzheimers Dis. (2013) 37:653–9. doi: 10.3233/JAD-130746
10. Canevelli M, Piscopo P, Talarico G, Vanacore N, Blasimme A, Crestini A, et al. Familial Alzheimer's disease sustained by presenilin 2 mutations: systematic review of literature and genotype-phenotype correlation. Neurosci Biobehav Rev. (2014) 42:170–9. doi: 10.1016/j.neubiorev.2014.02.010
11. Cruts M, Theuns J, Van Broeckhoven C. Locus-specific mutation databases for neurodegenerative brain diseases. Hum Mutat. (2012) 33:1340–4. doi: 10.1002/humu.22117
12. Ryan NS, Nicholas JM, Weston PSJ, Liang Y, Lashley T, Guerreiro R, et al. Clinical phenotype and genetic associations in autosomal dominant familial Alzheimer's disease: a case series. Lancet Neurol. (2016) 15:1326–35. doi: 10.1016/S1474-4422(16)30193-4
13. McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR Jr., Kawas CH, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. (2011) 7:263–9. doi: 10.1016/j.jalz.2011.03.005
14. Liu ZJ, Lin HX, Wei Q, Zhang QJ, Chen CX, Tao QQ, et al. Genetic spectrum and variability in Chinese patients with amyotrophic lateral sclerosis. Aging Dis. (2019) 10:1199–206. doi: 10.14336/AD.2019.0215
15. Xu Y, Liu X, Shen J, Tian W, Fang R, Li B, et al. The whole exome sequencing clarifies the genotype- phenotype correlations in patients with early-onset dementia. Aging Dis. (2018) 9:696–705. doi: 10.14336/AD.2018.0208
16. Giau VV, Bagyinszky E, Yang YS, Youn YC, An SSA, Kim SY, et al. Genetic analyses of early-onset Alzheimer's disease using next generation sequencing. Sci Rep. (2019) 9:8368. doi: 10.1038/s41598-019-44848-2
17. Jia L, Fu Y, Shen L, Zhang H, Zhu M, Qiu Q, et al. PSEN1, PSEN2, and APP mutations in 404 Chinese pedigrees with familial Alzheimer's disease. Alzheimers Dement. (2020) 16:178–91. doi: 10.1002/alz.12005
18. Jiang B, Zhou J, Li HL, Chen YG, Cheng HR, Ye LQ, et al. Mutation screening in Chinese patients with familial Alzheimer's disease by whole-exome sequencing. Neurobiol Aging. (2019) 76:e215–e221. doi: 10.1016/j.neurobiolaging.2018.11.024
19. Antonell A, Balasa M, Oliva R, Llado A, Bosch B, Fabregat N, et al. A novel PSEN1 gene mutation (L235R) associated with familial early-onset Alzheimer's disease. Neurosci Lett. (2011) 496:40–2. doi: 10.1016/j.neulet.2011.03.084
20. Janssen JC, Beck JA, Campbell TA, Dickinson A, Fox NC, Harvey RJ, et al. Early onset familial Alzheimer's disease: Mutation frequency in 31 families. Neurology. (2003) 60:235–9. doi: 10.1212/01.WNL.0000042088.22694.E3
21. Zarea A, Charbonnier C, Rovelet-Lecrux A, Nicolas G, Rousseau S, Borden A, et al. Seizures in dominantly inherited Alzheimer disease. Neurology. (2016) 87:912–9. doi: 10.1212/WNL.0000000000003048
22. Yang X, Yang Y, Liu J, Li G, Yang E. Increased phosphorylation of tau and synaptic protein loss in the aged transgenic mice expressing familiar Alzheimer's disease-linked presenilin 1 mutation. Neurochem Res. (2012) 37:15–22. doi: 10.1007/s11064-011-0575-2
23. Ryan NS, Biessels GJ, Kim L, Nicholas JM, Barber PA, Walsh P, et al. Genetic determinants of white matter hyperintensities and amyloid angiopathy in familial Alzheimer's disease. Neurobiol Aging. (2015) 36:3140–51. doi: 10.1016/j.neurobiolaging.2015.08.026
24. Shea YF, Chu LW, Chan AO, Ha J, Li Y, Song YQ, et al. A systematic review of familial Alzheimer's disease: Differences in presentation of clinical features among three mutated genes and potential ethnic differences. J Formos Med Assoc. (2016) 115:67–75. doi: 10.1016/j.jfma.2015.08.004
25. Keller L, Welander H, Chiang HH, Tjernberg LO, Nennesmo I, Wallin AK, et al. The PSEN1 I143T mutation in a Swedish family with Alzheimer's disease: clinical report and quantification of Abeta in different brain regions. Eur J Hum Genet. (2010) 18:1202–8. doi: 10.1038/ejhg.2010.107
26. Arai N, Kishino A, Takahashi Y, Morita D, Nakamura K, Yokoyama T, et al. Familial cases presenting very early onset autosomal dominant Alzheimer's disease with I143T in presenilin-1 gene: implication for genotype-phenotype correlation. Neurogenetics. (2008) 9:65–7. doi: 10.1007/s10048-007-0104-2
27. Bekris LM, Yu CE, Bird TD, Tsuang DW. Genetics of Alzheimer disease. J Geriatr Psychiatry Neurol. (2010) 23:213–27. doi: 10.1177/0891988710383571
28. Shi Z, Wang Y, Liu S, Liu M, Liu S, Zhou Y, et al. Clinical and neuroimaging characterization of Chinese dementia patients with PSEN1 and PSEN2 mutations. Dement Geriatr Cogn Disord. (2015) 39:32–40. doi: 10.1159/000366272
29. Giau VV, Pyun JM, Bagyinszky E, An SSA, Kim S. A pathogenic PSEN2 p.His169Asn mutation associated with early-onset Alzheimer's disease. Clin Interv Aging. (2018) 13:1321–9. doi: 10.2147/CIA.S170374
30. Youn YC, Bagyinszky E, Kim H, Choi BO, An SS, Kim S, et al. Probable novel PSEN2 Val214Leu mutation in Alzheimer's disease supported by structural prediction. BMC Neurol. (2014) 14:105. doi: 10.1186/1471-2377-14-105
31. An SS, Park SA, Bagyinszky E, Bae SO, Kim YJ, Im JY, et al. A genetic screen of the mutations in the Korean patients with early-onset Alzheimer's disease. Clin Interv Aging. (2016) 11:1817–22. doi: 10.2147/CIA.S116724
32. Hsu S, Pimenova AA, Hayes K, Villa JA, Rosene MJ, Jere M, et al. Systematic validation of variants of unknown significance in APP, PSEN1 and PSEN2. Neurobiol Dis. (2020) 139:104817. doi: 10.1016/j.nbd.2020.104817
33. Kaden D, Harmeier A, Weise C, Munter LM, Althoff V, Rost BR, et al. Novel APP/Abeta mutation K16N produces highly toxic heteromeric Abeta oligomers. EMBO Mol Med. (2012) 4:647–59. doi: 10.1002/emmm.201200239
34. Yi Y, Xiaobin Y, Hui C, Yufa Z, Qiaowei Z, Xingyue H, et al. An APP mutation family exhibiting white matter hyperintensities and cortical calcification in East China. Neurol Sci. (2020) 41:2921–8. doi: 10.1007/s10072-020-04342-4
35. Scarmeas N, Hadjigeorgiou GM, Papadimitriou A, Dubois B, Sarazin M, Brandt J, et al. Motor signs during the course of Alzheimer disease. Neurology. (2004) 63:975–82. doi: 10.1212/01.WNL.0000138440.39918.0C
36. Sleegers K, Brouwers N, Gijselinck I, Theuns J, Goossens D, Wauters J, et al. APP duplication is sufficient to cause early onset Alzheimer's dementia with cerebral amyloid angiopathy. Brain. (2006) 129:2977–83. doi: 10.1093/brain/awl203
37. McNaughton D, Knight W, Guerreiro R, Ryan N, Lowe J, Poulter M, et al. Duplication of amyloid precursor protein (APP), but not prion protein (PRNP) gene is a significant cause of early onset dementia in a large UK series. Neurobiol Aging. (2012) 33:e413–21. doi: 10.1016/j.neurobiolaging.2010.10.010
Keywords: early-onset AD, APP, PSEN1, PSEN2, phenotype heterogeneity
Citation: Liang Z, Wu Y, Li C and Liu Z (2023) Clinical and genetic characteristics in a central-southern Chinese cohort of early-onset Alzheimer's disease. Front. Neurol. 14:1119326. doi: 10.3389/fneur.2023.1119326
Received: 08 December 2022; Accepted: 21 February 2023;
Published: 27 March 2023.
Edited by:
Xiaopu Zhou, Hong Kong University of Science and Technology, Hong Kong SAR, ChinaReviewed by:
Eva Bagyinszky, Gachon University, Republic of KoreaCopyright © 2023 Liang, Wu, Li and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhijun Liu, bGl1emhpanVuaHViZWlAMTYzLmNvbQ==; Chuanzhou Li, Y2h1YW56aG91bGlAaHVzdC5lZHUuY24=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.