
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 03 February 2023
Sec. Epilepsy
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1101370
This article is part of the Research TopicAdvances in diagnosing and treating new-onset refractory status epilepticus (NORSE)View all 14 articles
 Marie Benaiteau1,2*
Marie Benaiteau1,2* Luc Valton2,3*
Luc Valton2,3* Ludovic Gardy3
Ludovic Gardy3 Marie Denuelle2,3Rachel Debs2Valentin Wucher1,4Florence Rulquin2
Marie Denuelle2,3Rachel Debs2Valentin Wucher1,4Florence Rulquin2 Emmanuel J. Barbeau3,5
Emmanuel J. Barbeau3,5 Fabrice Bonneville5,6,7Jérémie Pariente2,5,6
Fabrice Bonneville5,6,7Jérémie Pariente2,5,6 Jonathan Curot2,3,5*
Jonathan Curot2,3,5*While new-onset status epilepticus (NOSE) is a harbinger of chronic epilepsy, prospective medical data are sparse in terms of specifying whether the evolution of status epilepticus (SE) and seizure expression in NOSE resembles what occurs in patients who have already been diagnosed with epilepsy [non-inaugural SE (NISE)] in all aspects apart from its inaugural nature. The aim of this study was to compare the clinical, MRI, and EEG features that could distinguish NOSE from NISE. We conducted a prospective monocentric study in which all patients ≥18 years admitted for SE over a 6-month period were included. A total of 109 patients (63 NISE and 46 NOSE cases) were included. Despite similar modified Rankin scores before SE, several aspects of the clinical history distinguished NOSE from NISE patients. NOSE patients were older and frequently had neurological comorbidity and preexisting cognitive decline, but they had a similar prevalence of alcohol consumption to NISE patients. NOSE and NISE evolve in the same proportions as refractory SE (62.5% NOSE, 61% NISE) and share common features such as the same incidence (33% NOSE, 42% NISE, and p = 0.53) and volumes of peri-ictal abnormalities on MRI. However, in NOSE patients, we observed greater non-convulsive semiology (21.7% NOSE, 6% NISE, and p = 0.02), more periodic lateral discharges on EEG (p = 0.004), later diagnosis, and higher severity according to the STESS and EMSE scales (p < 0.0001). Mortality occurred in 32.6% of NOSE patients and 21% of NISE patients at 1 year (p = 0.19), but with different causes of death occurring at different time points: more early deaths directly linked to SE at 1 month occurred in the NOSE group, while there were more remote deaths linked to causal brain lesions in the NISE group at final follow-up. In survivors, 43.6% of the NOSE cases developed into epilepsy. Despite acute causal brain lesions, the novelty related to its inaugural nature is still too often associated with a delay in diagnosing SE and a poorer outcome, which justifies the need to more clearly specify the various types of SE to constantly raise awareness among clinicians. These results highlight the relevance of including novelty-related criteria, clinical history, and temporality of occurrence in the nosology of SE.
It is interesting to note that recent acronyms and definitions of status epilepticus (SE) include the following references to time and the novelty of occurrence: new-onset status epileptic (NOSE) (1), new-onset refractory SE (NORSE) (2, 3), late-onset absence SE (4), and subacute encephalopathy syndrome in alcoholics (SESA) (5). Could the mode of onset, novelty, and temporal context be key to understanding SE? What makes NOSE a specific clinically relevant pathological entity that is distinguishable from other types of SE, i.e., non-inaugural SE that occurs in patients with epilepsy (NISE)?
Only recently have the temporality of onset and novelty become an integral part of the definitions of SE. Since the pioneer definitions of SE (4), many “mechanistic” or “operational” definitions of SE have been proposed (4, 6–10). Until now, they have been exclusively based on semiology (convulsive or non-convulsive, generalized or focal, etc.). The temporal dimension has long been considered regarding the duration of SE but not in the context of its onset. Operationally, NOSE is defined as “prolonged seizures lasting more than 5 min or the presence of recurrent seizures without return to baseline in between in patients with no previous history of epilepsy” (11). However, this definition remains non-consensual. SE nosology is constantly evolving due to the clinical heterogeneity of its semiology, a complex poorly understood pathophysiology (12, 13), multiple etiologies (14), and difficulties conducting prospective studies.
Clarifying the definition of NOSE is essential as the incidence is significant. Approximately half of all adult cases of SE (up to 59%) are inaugural in non-epileptic patients (15–20). The incidence of NOSE was found to be 16.3/100,000 to 36/100,000 adults per year depending on the cohort and whether or not the new ILAE 2015 definition and classification of SE was taken into account (21, 22). However, despite the incidence, knowledge of the clinical, EEG, and MRI spectrum of NOSE in adults is mostly based on retrospective data (11, 20, 23–25).
One of the few consensual elements concerning NOSE is a poor prognosis and a possible progression to refractory SE (i.e., NORSE) (24, 26–28). Mortality in 1 month is 20–61% depending on the cohort. Factors of poor prognosis are the age of the patient [especially over 65 years (11)], etiology, and the duration of the SE (15–17, 23, 24, 29, 30). Tracheal intubation and co-infections are additional factors of adverse outcomes (23).
In survivors, a poor prognosis for NOSE also suggests the onset of a chronic illness. More than 58% of survivors may experience seizures, mainly related to acute or progressive brain injury, the duration of SE (significant threshold at 24 h) being the only independent predictor of the development of chronic epilepsy after SE (27). Paradoxically, some series also showed that progression to NORSE had no influence on functional outcome or mortality at the last follow-up, while SE semiology (non-convulsive vs. convulsive and loss of consciousness) or age above or equal to 65 did not predict progression to NORSE (11).
If NOSE is a precursor to chronic epilepsy, it could be hypothesized that its presentation resembles NISE in all aspects apart from its inaugural nature. However, the medical literature is unable to demonstrate this. None of the studies cited above investigated the discriminating features between NOSE and NISE. In addition, little information is available on the paraclinical aspects associated with NOSE, and the most recent publications frequently focused on the refractory subtype of these de novo SE (2, 3, 31).
Although it is now well-established that NOSE can develop into epilepsy, to our knowledge, there is no prospective trial that compares the clinical, MRI, and EEG patterns that may distinguish NOSE from NISE. Does the mechanism that leads to epilepsy result in a specific clinical pattern of SE? Are there imaging and electrophysiological criteria that distinguish NOSE from NISE? Do NOSE and NISE progress similarly and have the same prognosis?
To clarify these questions, we conducted a prospective monocentric study to multimodally compare NOSE and NISE at baseline (before SE), during SE, and at follow-up in 1, 3, and 12 months. The aims of this study were (1) to compare clinical and paraclinical (brain imagery and electrophysiological recordings) features of NOSE (including NORSE) and NISE; (2) to study the outcome of SE at 1, 3, and 12 months as well as the prognostic factors; and (3) more specifically to analyze peri-ictal MRI abnormalities. We hypothesized that NOSE and NISE each have their own specificities, particularly in terms of outcomes. We hoped to identify new markers for positive diagnosis and the prognosis of inaugural SE.
Our work is a prospective, observational, descriptive, single-center study (Figure 1). We collected clinical, neuroradiological, and electrophysiological data for each patient admitted consecutively to Toulouse University Hospital from December 2015 to June 2016 (1) for SE and (2) SE not clinically diagnosed immediately on admission but subsequent to the first EEG. To select these patients, all EEGs performed during this period and all requests for EEGs for SE were screened. The inclusion criteria were a diagnosis of SE confirmed by a neurologist, exclusion of post-anoxic SE, age of 18 years and older, and non-refusal to participate in the study. The use of the data in our study was approved by the Regional Ethics Committee at Toulouse University Hospital (CPP Sud-Ouest no. 04-1215).
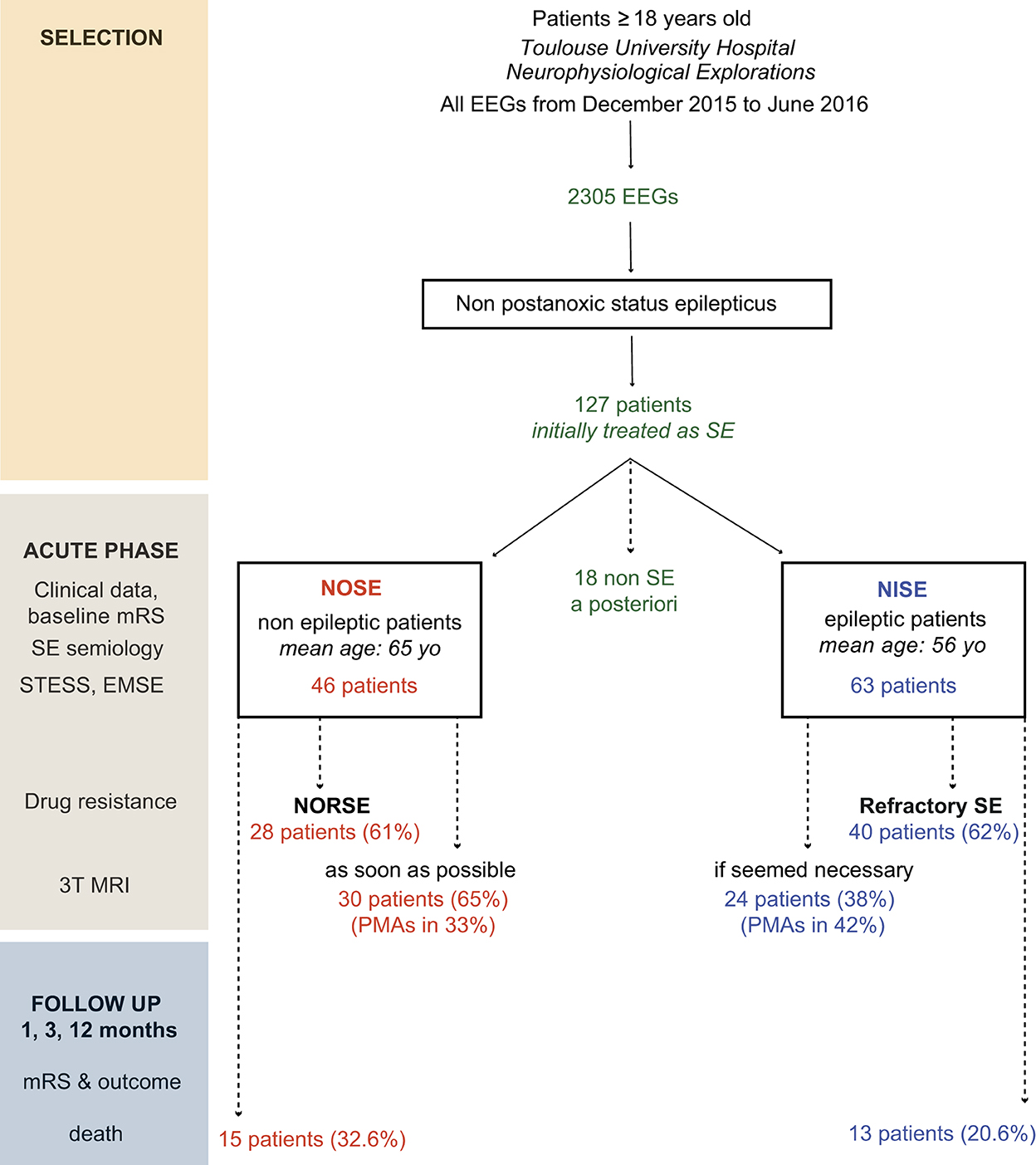
Figure 1. Study design, selection of patients, and SE classification. Five patients were secondarily excluded from the NOSE group (1 with myoclonus of the left upper limb secondary to spinal cord ischemia, 1 with vigilance fluctuations due to a post-traumatic brainstem lesion, 1 with a reactive coma and abnormal movements secondary to severe intra-parenchymal hemorrhage, 1 with psychomotor agitation and vagal discomfort with the loss of consciousness due to pain, and 1 with a first psychogenic non-epileptic status). A total of 13 patients were secondarily excluded from the NISE group (6 with a psychogenic non-epileptic status, 3 with serial seizures but complete clinical recovery between seizures, 3 with a prolonged post-ictal deficit and/or post-ictal agitation, and 1 with chronic meningitis on ventriculoperitoneal shunt, abnormal eye movements, and intracranial hypertension with no argument for seizures).
Epilepsy is defined as a lasting predisposition to generate seizures and the cognitive, behavioral, psychological, and social consequences of this condition (32). NOSE was defined as the occurrence in patients without a history of SE or uncured epilepsy (cured epilepsy is the absence of seizures in the absence of treatment for more than 5 years). The following functional and semiological definitions were used for either NOSE or NISE.
The definitions used for generalized and focal convulsive SE were (10, 21, 33) the occurrence of at least two epileptic seizures in a short interval without complete recovery of a stable neurological status between seizures; ictal clinical or electrical activity lasting 5 min or more for generalized seizures and 10 min or more for focal seizures; serial seizures; and seizures followed by a coma or persistent confusion.
The definition used for non-convulsive SE (NCSE) was based on the Salzburg consensus criteria (34, 35). We considered that an NCSE was certain if there was an association with an acute qualitative or quantitative alteration of consciousness without prominent motor symptoms or persistent after a clinical seizure with motor manifestation, not otherwise explained, and electrical confirmation by EEG (pattern of epileptiform discharges at a frequency >2.5 Hz present for more than 10 recorded seconds). When epileptiform discharges were present <2.5 Hz in the worst 10-s epoch or there was no epileptiform discharge but only continuous rhythmic delta-theta activity >0.5 Hz, the following secondary criteria were fulfilled: (a) typical spatio-temporal evolution or (b) subtle clinical ictal phenomena were present during the patterns, or (c) a clear clinical and EEG improvement after intravenous administration of an appropriately chosen anti-seizure medication (ASM) was documented.
In the acute phase, we collected the following data: age, gender, personal history, modified Rankin score (mRS) before SE (at baseline), medications, clinical symptoms of the seizures observed during SE, and post-ictal deficit. Severe and life-threatening complications were specified: respiratory distress, including infectious pneumonia, hemodynamic instability (systolic blood pressure <90 mmHg; the need for vasoamines), and traumatic complications.
SE duration was calculated or estimated through a combination of clinical and EEG data. SE was considered refractory if it persisted 30 min after the introduction of a first- and second-line ASM (9, 36) and super-refractory if it persisted at least 24 h after the start of general anesthesia (37, 38).
The etiologies and/or contributing factors of SE were classified according to the ILAE Task Force definition: acute etiologies, sequelae or old structural abnormalities, progressive etiologies, known epileptic syndromes, and unknown etiologies (21, 39). SE severity was rated by two scales, namely, the Status Epilepticus Severity Score (STESS) (40) and the Epidemiology-Based Mortality Score in Status Epilepticus (EMSE) (41).
The cognitive status of non-epileptic patients before SE was estimated using the long version (a 26-item questionnaire) of the IQ CODE (42). In the literature, the threshold chosen for diagnosing dementia is 3.4/5 (43).
The chronology of follow-up was 1, 3, and 12 months to detect early, medium-term, and late complications, respectively (mRS, onset of recurrent epileptic seizures or new SE, and death). Cognitive complaint and focal neurological deficit were specified at 3 months.
Scalp-EEGs (9–21 surface electrodes, 256 Hz sampling rate) combined with video and ECG were recorded with the Deltamed system (Natus Medical Incorporated). At least 20 min were recorded for each patient (12 patients were monitored for several hours). The time period between the first EEG and the onset of symptoms was noted. EEG recordings were analyzed by clinical electrophysiologists (JC, MB, MD, RD, and LV). EEGs were classified as “normal,” “sedation EEG,” “ictal,” or “post-ictal” EEG. Epileptic activities were divided into “periodic discharges,” “rhythmic delta discharges,” and “paroxysmal abnormalities” (i.e., spikes, polyspikes, and spikes-and-waves) (21).
We used two 3T imagers (Magnetom Skyra, Siemens Healthcare and Achieva, Philips Medical System) in the clinical neuroradiology department. An MRI was performed urgently as soon as the patient's condition allowed, ideally within 72 h of the diagnosis of NOSE and if considered necessary for the care of patients with NISE. A minimum of the following sequences was performed: DWI, ADC mapping, fluid-attenuated inversion recovery (FLAIR), T1 with gadolinium, and gradient-recalled echo T2*. The presence of PMAs in DWI and FLAIR sequences, the volume of PMAs in DWI, the presence and type of old cerebral lesions, and SE etiology were analyzed by a trained neuroradiologist and neurologist (FB and MB). When other lesions (peritumoral edema, gliosis, acute stroke, etc.) could explain the abnormalities in DWI and FLAIR, these were not considered as PMAs.
We semi-automatically quantified the PMA volume in DWI using OLEA software in a one-shot analysis with manual correction [Olea Sphere® version 2.3, cutting thickness of 3 or 4 mm, technique validated for ischemic stroke (44)]. The PMA volume was estimated using the average of three different segmentations for each patient. The standard zones of the magnetic susceptibility artifact were systematically trimmed.
If an MRI control was required, it was scheduled on the same 3T machines within 3 months of the SE.
To compare the NOSE and NISE groups, we used the chi-square test for qualitative variables, except when the theoretical numbers were <5, in which case, Fisher's test was used. To compare quantitative variables, we used the Wilcoxon test. To limit the risk of type-1 errors associated with multiple comparisons, we corrected the alpha values using the Bonferroni method. The alpha values to be considered are indicated below the figures or tables (in general, the alpha value = 0.05/90). Due to the inherent heterogeneity of clinical data and the multiple comparisons made, we considered “tendencies” for p < 0.05 but above the corrected threshold. We only considered significant p-values below the corrected alpha values. For post-hoc analyses, Tukey's test was used (p-values automatically adjusted for multiple comparisons).
To study the impact on outcome (mRS) at different timestamps for predictive factors such as the presence or absence of PMA, drug resistance, or status epilepticus, we performed multiple linear regressions. We used linear mixed-effects models in which the variable “patient” was considered a random effect. The variables “measurement time” (baseline, first month, third month, and twelfth month), drug resistance (1/0), with or without PMA (1/0), and new-onset status epilepticus (1/0) were considered as fixed effects. Finally, Pearson correlations were performed. The corrected p-value was considered for the significance threshold for linear mixed-effect models, and the Pearson correlation was 0.017 (0.05/3).
During the 6 months, 2,305 EEGs were performed, allowing the inclusion of 127 patients who had been treated for SE. A total of 18 patients initially considered as having SE were excluded after revision of the diagnosis a posteriori: five patients from the NOSE group and 13 epileptic patients from the NISE group. Therefore, 109 patients (46 NOSE and 63 NISE cases) were finally included (Figure 1).
Clinical data are presented in Table 1. Despite a similar level of autonomy on the mRS before SE, patients experiencing NOSE tended to be older (p < 0.01, alpha = 0.0006). The same proportion of excessive alcohol consumption, psychiatric history, and use of psychotropic drugs was found in both groups. Alcohol abuse or dependence was directly involved in 5 NOSE patients and 6 NISE patients. The IQ code before SE was obtained for the NOSE group only: 28/46 (61%) patients had a score of ≥3.4/5, which is above the threshold indicating significant cognitive impairment that affects autonomy in daily life. All patients in the NISE group had been on ASM (median = 1, min = 1, max = 5). In total, 24 of 57 NISE patients (42%) had a history of SE (data are lacking for six subjects). Epilepsy was considered stabilized (seizure-free patients) for 38 of 59 patients before the onset of SE (data are lacking for four patients).

Table 1. Clinical characteristics of NOSE and NISE patients.
Acute brain lesions on imagery were significantly more frequent in the NOSE group (n = 10, p < 0.0001, and alpha = 0.0006). This included three severe traumatic brain injuries, three infectious diseases (pneumococcal meningitis, HSV1 herpes meningoencephalitis, and empyema with extensive cerebral venous thrombosis), 1 posterior reversible encephalopathy syndrome, 1 inflammatory cerebral amyloid angiopathy, 1 junctional ischemic stroke (M1 stenosis), and 1 undetermined meningoencephalitis leading to NORSE. Cases of acute brain etiologies in NISE patients were 2 severe head traumas (one of which was due to acute alcohol intoxication) and 1 ischemic stroke during meningioma surgery.
Progressive etiologies were all already known before SE in the NISE group and included a large majority of brain tumors (5 glioblastomas, 3 meningiomas, 2 brain metastases, and 1 cerebral lymphoma) and 1 patient with Alzheimer's disease and cerebral amyloid angiopathy, whereas 5 of 7 were discovered during SE evaluation in the NOSE group (2 glioblastomas, 1 brain metastases due to small cell lung cancer, 1 brain lymphoma recurrence, 1 cerebral cavernoma, and 2 cases of Alzheimer's disease).
Remote brain lesions were mainly post-traumatic and of a vascular, ischemic, or hemorrhagic nature.
Other acute triggers could be associated and included forgetting ASM for 13 NISE patients (20.6%), sleep deprivation (4 NISE patients), stress (2 NISE patients), fever/sepsis (5 NOSE and 8 NISE patients), and drugs that lower the epileptic threshold (4 NOSE and 6 NISE patients). Among the 4 patients in the NOSE group with no etiology found at the time of SE, two were chronically heavy consumers of cannabis.
NOSE tended to be diagnosed later, with a maximal delay in the diagnosis of 15 days (vs. 30 h for NISE, p = 0.06, alpha = 0.0006) and a median of 60 min for NOSE vs. 10 min for NISE, resulting in diagnostic and therapeutic delays (p = 0.006 and p = 0.09, respectively, alpha = 0.0006) (Table 1). SE duration was heterogeneous: on average 62 h for NOSE vs. 23 h for NISE (p = 0.33). In both groups, SE lasted ≥24 h in one-third of the patients and if associated with severe complications required resuscitation management in 35% of the cases. The mean duration of hospitalization was 13 days for the NOSE group [min = 4, max = 96, median = 10 days] and 10 days for the NISE group [min = 1, max = 117, median = 7 days]. Progression to refractory SE was not significantly different between the groups (p = 0.93).
The following heterogeneous types of SE were encountered in both NOSE and NISE: generalized convulsive, focal convulsive, initially non-convulsive, or secondary generalized convulsive in similar proportions (Table 1). However, secondary non-convulsive SE tended to be more prevalent in NOSE than in NISE (21.7% in NOSE, 6% in NISE, p = 0.02, alpha = 0.0006). NOSE patients tended to have more post-ictal focal neurological deficits and a greater number of severe complications, especially hemodynamic complications (p = 0.04 and alpha = 0.0006).
SE severity was significantly higher in NOSE than in NISE. STESS and EMSE scores were above the poor prognosis threshold in 78% of NOSE vs. 36.5% of NISE patients (36/46 ≥ 3/6 vs. 23/63; p < 0.0001; alpha = 0.0006) and 63% vs. 28.5% (29/46 ≥ 64/255 vs. 18/63; p < 0.0001; and alpha = 0.0006), respectively.
There was no global effect of the inaugural or non-inaugural nature of SE on the outcome (p = 0.373) according to a mixed-effects model. Nevertheless, there was an interaction between the type of SE and the mRS at baseline, and in 1, 3, and 12 months (p < 0.017). This suggests that mRS between baseline and 12 months changes at a different speed between the two groups of patients (Figures 2, 3). For NISE patients, mRS at baseline was only different from the mRS at 12 months (Tukey's HSD test, diff = 1.05, and p = 0.0005). For NOSE patients, the mRS at baseline was different from the mRS at 1 month (Tukey's HSD test; diff = 1.28; and p = 0.0033), 3 months (Tukey's HSD test, diff = 1.46, and p = 0.0006), and 12 months (Tukey's HSD test, diff = 1.76; and p = 0).
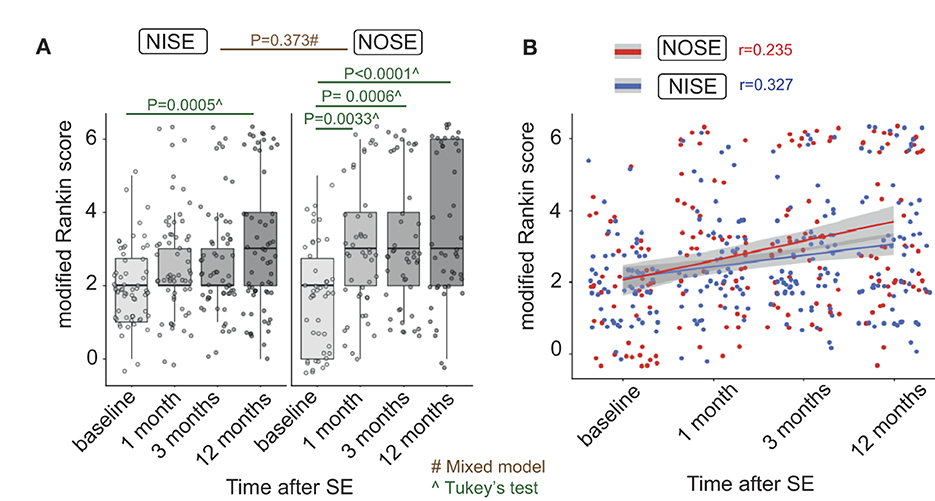
Figure 2. Outcome assessed by mRS between baseline and 12 months changes in different proportions in NOSE and NISE. (A) Individual mRS at each time point in NOSE and NISE groups. NISE patients had an average mRS of 2.02 at baseline, 2.6 at 1 month, 2.6 at 3 months, and 3.06 at 12 months. In contrast, NOSE patients had an average mRS of 2.02 at baseline, 3.3 at 1 month, 3.47 at 3 months, and 3.78 at 12 months. Therefore, we performed post-hoc analyses on these two groups independently. (B) Correlations between time after SE and outcome (Pearson correlations, r = 0.376 in the PMA group, r = 0.252 in the non-PMA group). Alpha = 0.05/3 = 0.017.
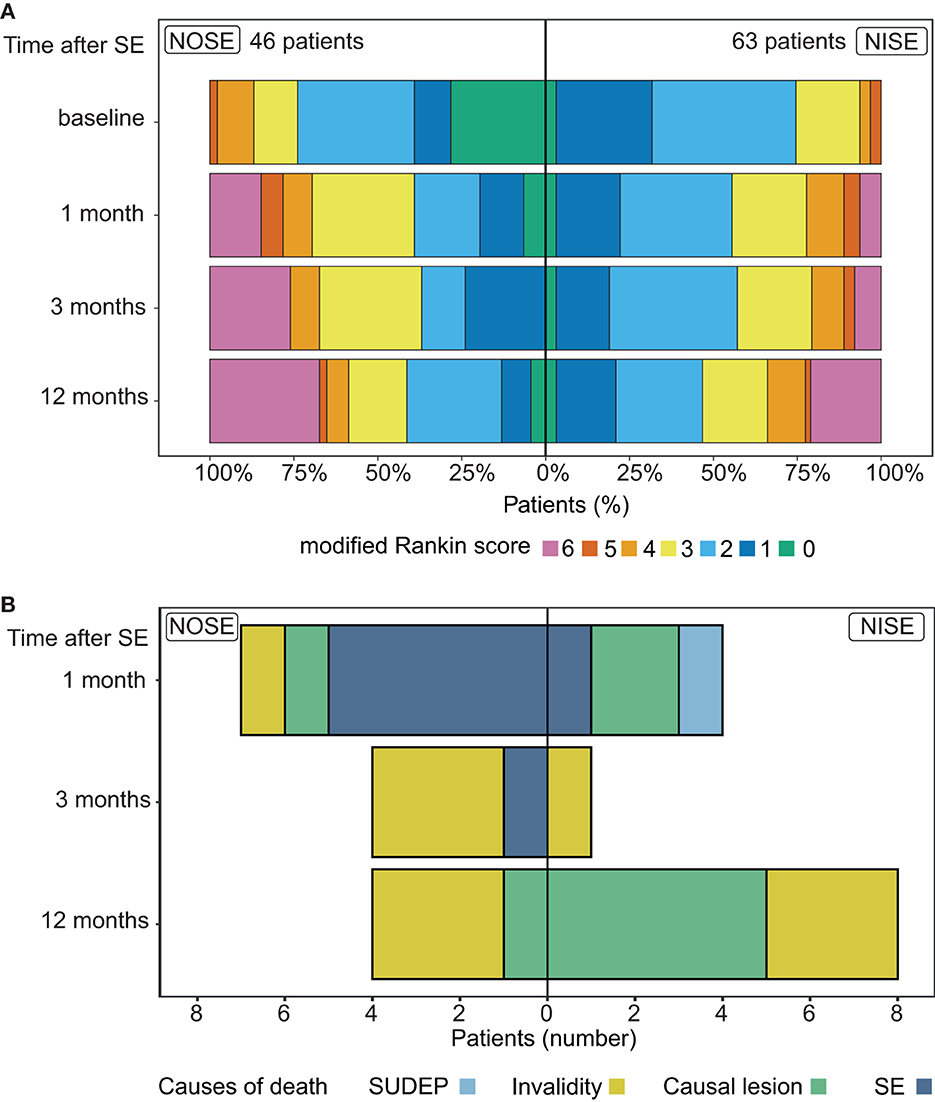
Figure 3. Outcome and causes of mortality in NOSE and NISE. (A) Outcome (mRS) changes in each group at each time point. Proportions of patients in NOSE and NISE groups for each mRS value. (B) Causes of mortality at each time point in NOSE and NISE groups.
Finally, in NOSE and NISE combined, we observed positive correlations between outcomes at the final follow-up (mRS at 12 months) and in descending order on both the STESS (Pearson correlations, r = 0.455, p = 1−06, and alpha <0.017) and EMSE scores (Pearson correlations, r = 0.326, p = 0.0006, and alpha <0.017) as well as the duration of SE (Pearson correlations, r = 0.217, p = 0.002, and alpha <0.017).
There was a recurrence of SE in 13 patients with NOSE (28.2%) and in 15 patients with NISE (23.8%) at 1 year but at different times: there was a recurrence in the first month in 7 cases of NOSE but only in 1 case of NISE (Fisher test, p = 0.01). For patients who did not die during the acute phase of SE, 17 of 39 patients with NOSE developed epilepsy (43.6%) and 29 of 52 patients with NISE had a recurrence of seizures in the year following SE (55.7%, data lacking for 11 patients). In survivors at 3 months, there was a cognitive complaint in 57% of the NOSE patients (57%) vs. 71% of the NISE patients and a focal (motor of language) deficit in 26% of NOSE and 43% of NISE cases.
At the final follow-up, mortality was observed in 32.6% of NOSE vs. 20.6% of NISE patients (p = 0.19). However, rates of death varied according to time points (Figure 3). This occurred within the first month in 15% of NOSE patients and 6% of NISE patients. The cumulated rate increased to 24% and 8% at 3 months (p = 0.02 and alpha = 0.0006; Table 1). The patients who died in 1 year all had refractory SE except for 1 NOSE and 2 NISE cases (25 refractory SE/28 deaths, 89%). The causes of death were diverse and variable according to the time.
In the NISE group, at 1 month, death was related to the direct consequence of a refractory SE (1 patient), to the causal lesion induced by SE (2 patients with glioblastomas), and to a probable SUDEP (1 patient); at 3 months to invalidity (one 90-year-old patient); and at 1 year, to brain tumors (3 patients with glioblastomas and 2 patients with brain metastases), and to invalidity (3 patients with multiple pathologies).
In the NOSE group, at 1 month, death was related to the direct consequence of SE (five 54- to 95-year-old patients with organ failure after NORSE), at 3 months, to organ failure in super-refractory SE (one 56-year-old man) and to invalidity after SE in a context of multiple pathologies (three 72- to 91-year-old patients), and at 1 year, to glioblastoma (1 patient) and to progressive invalidity (three 62- to 101-year-old patients).
We observed similar numbers of pharmacoresistant NOSE and NISE cases (62% and 61%, respectively). According to the mixed-effects model, there was no global effect of refractoriness on the outcome, but there was an interaction between refractoriness and the time of the mRS assessment. This indicates that between baseline and 12 months, mRS changed in different proportions in refractory and non-refractory SE (considering both NOSE and NISE). Refractory SE had an average mRS of 2.01 at baseline, 3.08 at 1 month, 3.24 at 3 months, and 3.60 at 12 months. Non-refractory SE had an average mRS of 2.01 at baseline, 3.08 at 1 month, 2.58 at 3 months, and 2.97 at 12 months. Considering that the time of mRS assessment had a different effect on refractory and non-refractory SE, we analyzed these two groups independently. For refractory SE, baseline mRS was different from the mRS at 1 month (diff = 1.06, p = 0.003), 3 months (diff = 1.24, p = 0.0004), and 12 months (diff = 1.6, p = 0). For non-refractory SE, mRS after SE was different from baseline only at 12 months (diff = 0.95, p = 0.002).
A total of 54 patients (30 NOSE and 24 NISE cases) had a 3T MRI during the initial hospitalization for SE (MRI performed within the first 72 h of admission in 35 patients). MRI revealed an acute brain etiology in 9 patients with NOSE (30%), none in NISE patients, and old brain lesions in 18 patients in each group (66%).
PMAs were demonstrated in 20 patients (incidence of 37%, 10 patients in each group; Figures 1, 4, 5A). PMAs were present in 5 NOSE patients who responded to ASM, 5 NORSE, 6 refractory NISE, and 4 non-refractory NISE patients who experienced prolonged SE (180, 240, 700, and 2,000 min, respectively). The distribution of PMA and their aspect on the different MRI sequences were comparable in the 2 groups (Figure 4, Table 2). We noted the following two exceptions: a temporal punctiform gadolinium enhancement in two patients with non-refractory NOSE and a hyperintensity of the claustrum in one NOSE patient corresponding to SESA (Figure 4). There was no significant difference in PMA volume (Figure 5B, p = 0.36) between the 2 groups, but there was an outlier in the NISE group with a much higher volume than the others at 290 cc.
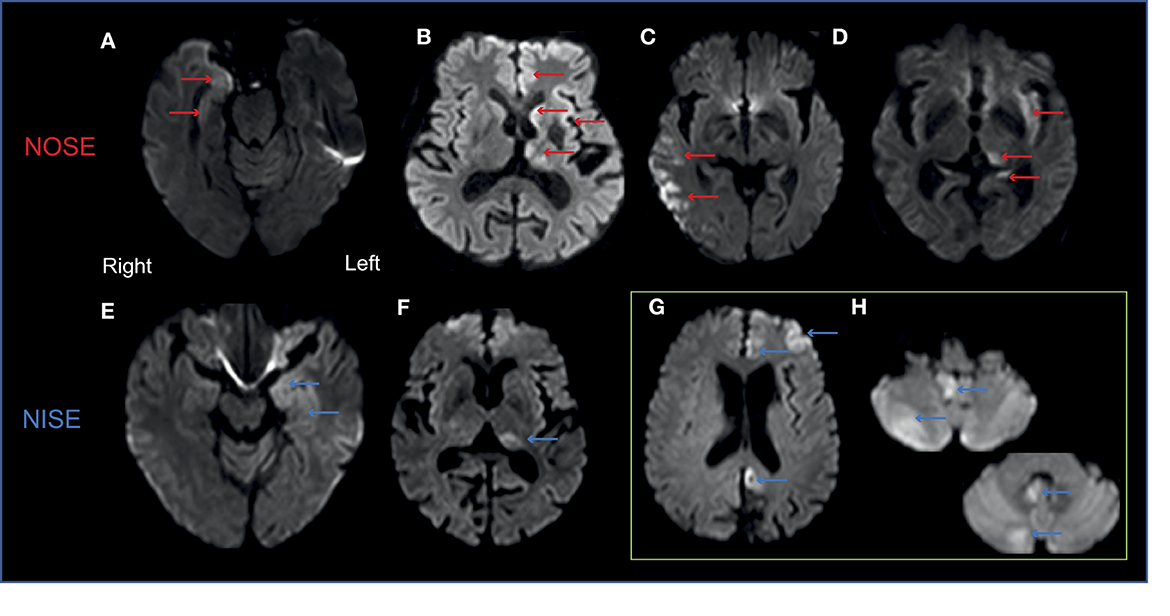
Figure 4. Generally similar patterns of PMA in NOSE and NISE. Examples of axial DWI views in 4 patients. (A) Right medial temporal hyperintensity in an 86-year-old woman with focal convulsive refractory NOSE. (B) Left thalamic, caudate nucleus, and frontal cortex hyperintensities in a 56-year-old man with generalized convulsive secondary non-convulsive super-refractory NOSE. (C) Right temporo-parietal cortex hyperintensity in a 79-year-old man with refractory generalized convulsive secondary non-convulsive NOSE. (D) Claustrum hyperintensity in the left hemisphere associated with a homolateral pulvinar and hippocampal hyperintensity in a 69-year-old alcoholic male with pharmacosensitive non-convulsive NOSE (SESA). (E) Left medial temporal hyperintensity in a 48-year-old man with pharmacosensitive focal non-convulsive NISE. (F) Left pulvinar hyperintensity in a 70-year-old man with pharmacosensitive focal non-convulsive NISE. (G, H) Right cerebellum hyperintensity and contralateral cortical hyperintensity in a 63-year-old man with a non-convulsive super-refractory NISE.
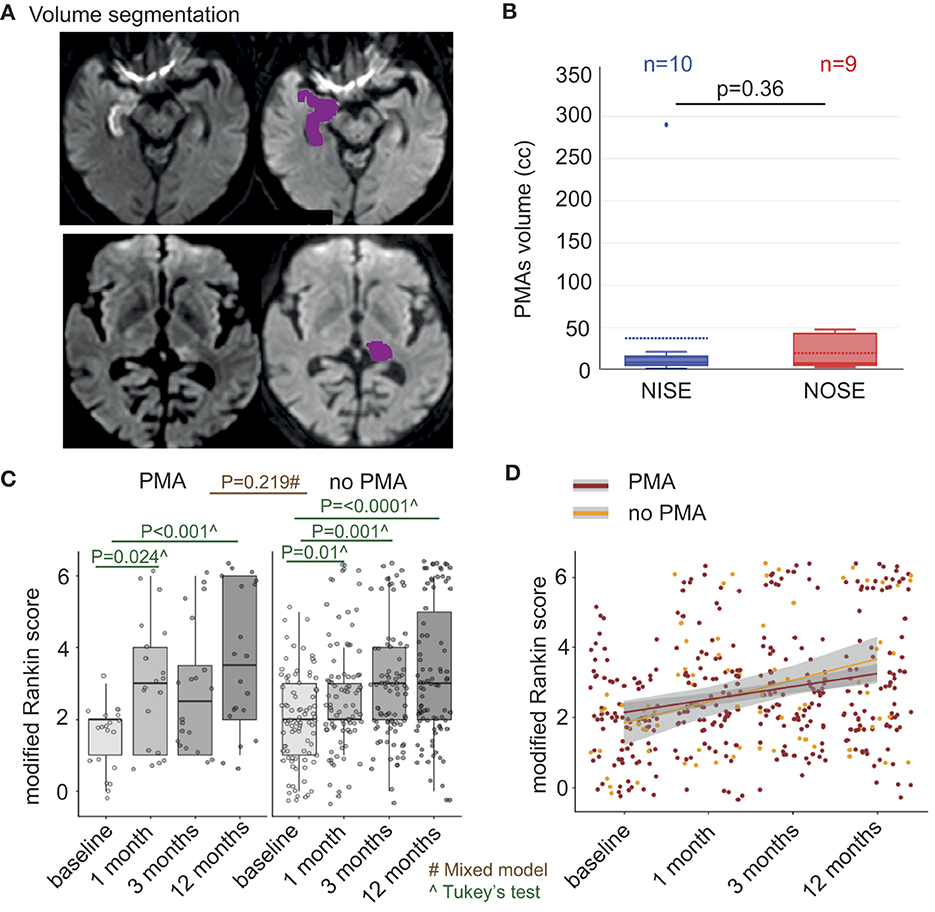
Figure 5. PMA volumes are similar in NOSE and NISE patients and PMA is related to prognosis. (A) PMA volumetry in DWI sequences. Semi-automatic quantification in one-shot analysis by OLEA (PMA is circumscribed in purple; colors were changed for purposes concerning the figure). Right mesial temporal hypersignal including the hippocampus (upper panel) and left posterior thalamic hypersignal (bottom panel). (B) Mean PMA volumes in each group. The two groups had a similar PMA volume (p = 0.36); note that there was an outlier in the NISE group with a much higher volume than the others at 290 ml, with a hypersignal in DWI of the majority of the left hemisphere cortex, the thalamus and at 7 days a right cerebellar diaschisis of partial NCSE secondarily generalized in a 52-year-old man institutionalized for encephalopathy evolving since childhood. (C) Individual mRS in patients with PMA and those without PMA. Patients with PMA had an average mRS of 1.5 at baseline, 3.1 at 1 month, 2.8 at 3 months, and 3.6 at 12 months. Patients without PMA had an average mRS of 1.5 at baseline, 2.2 at 1 month, 2.8 at 3 months, and 2.7 at 12 months. (D) Correlations between PMA evolution and outcome (mRS) at different time points (Pearson correlations, r = 0.376 in the PMA group, r = 0.252 in the non-PMA group). Alpha = 0.05/3 = 0.017.
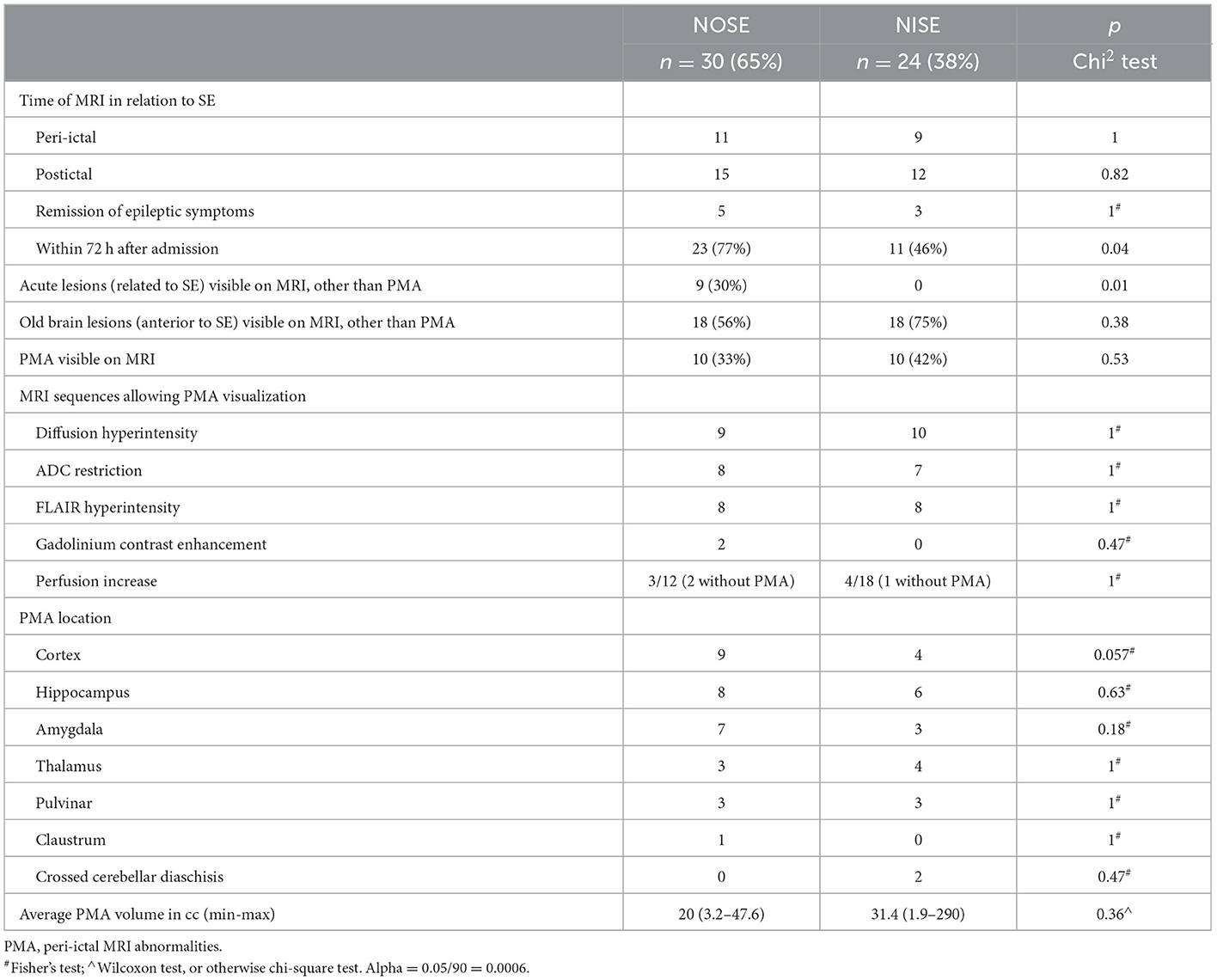
Table 2. MRI results in NOSE and NISE groups.
According to the mixed-effects model for NOSE and NISE combined, there was no global effect of the occurrence of PMA on the outcome (p = 0.22). Nevertheless, there was an interaction between the occurrence of PMA and the moment of mRS assessment (baseline, at 1, 3, and 12 months; p = 0.000), which suggests that between baseline and 12 months, mRS changed in different proportions in the two groups of patients (Figure 5C). We analyzed PMA and non-PMA groups independently using Tukey's HSD tests. For patients with PMA, the mRS at baseline was different from the mRS at 1 month (diff = 1.55 and p = 0.02) and at 12 months (diff = 2.1 and p = 0.001). In patients without PMA, mRS at baseline was different from mRS at 1 month (diff = 0.73 and p = 0.01), 3 months (diff = 0.89 and p = 0.001), and 12 months (diff = 1.18 and p = 0) (Figure 5D).
Concerning PMA changes during follow-up (7 of 10 patients with PMA in each group had an MRI control at 3 months), we noted a complete regression of PMA in only 5 patients (2 NOSE and 3 NISE cases) despite systematic normalization of the DWI due to the persistence of FLAIR hyperintensity in 8 patients (4 NOSE and 4 NISE cases) and the appearance of focal atrophy in 7 patients (5 NOSE and 2 NISE cases).
The median time before the first EEG was similar in both groups (~17 h). Different types of ictal abnormalities recorded on EEG are summarized in Table 3, and examples are provided in Figure 6. We analyzed spikes, spike-and-wave patterns, rhythmic delta discharges, and periodic epileptiform activities without identifying any specific type of epileptic activity that could be related to either NOSE or NISE. However, periodic lateralized activities tended to be more frequent in NOSE (p = 0.004 and alpha = 0.0006).
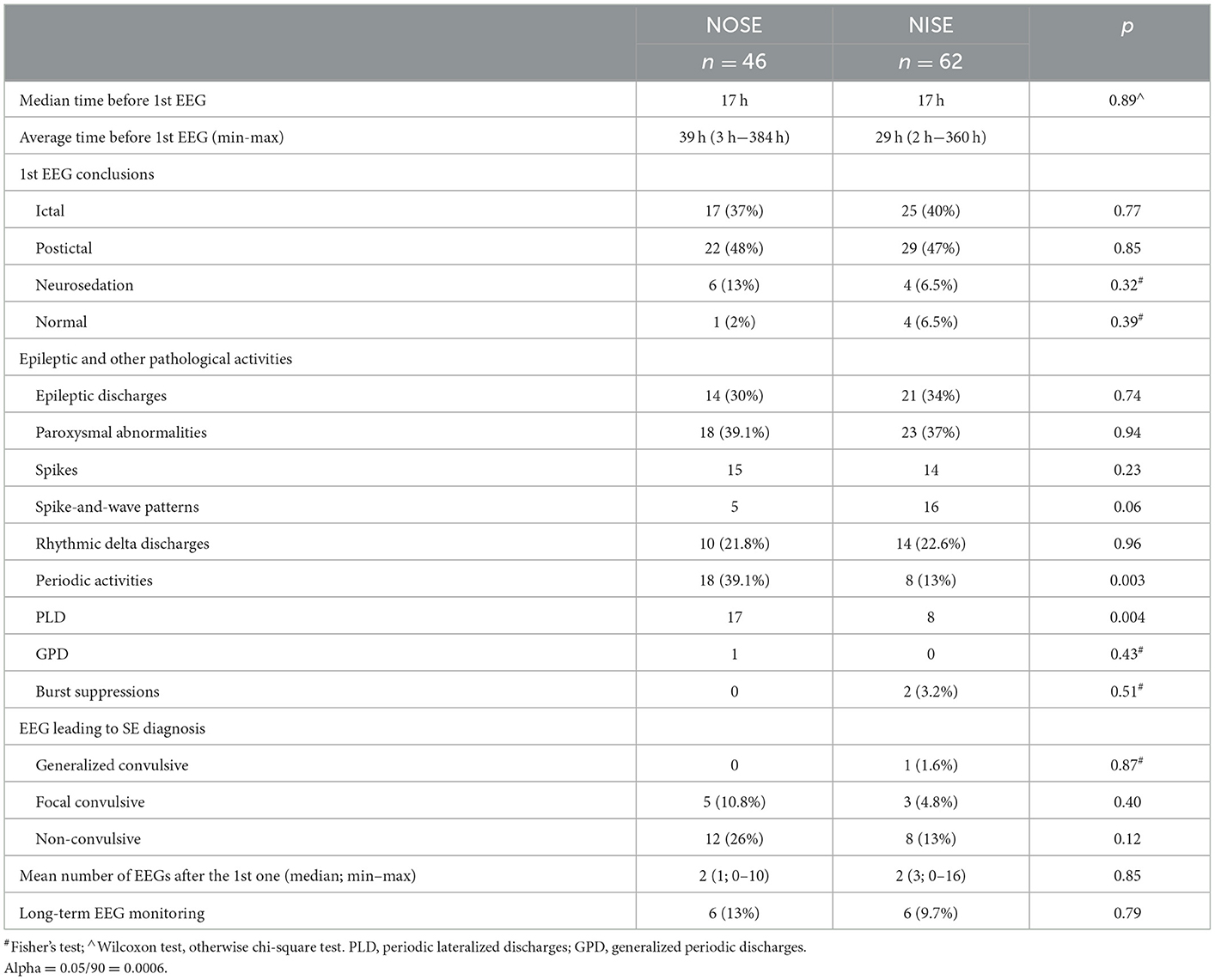
Table 3. EEG patterns during NOSE and NISE.
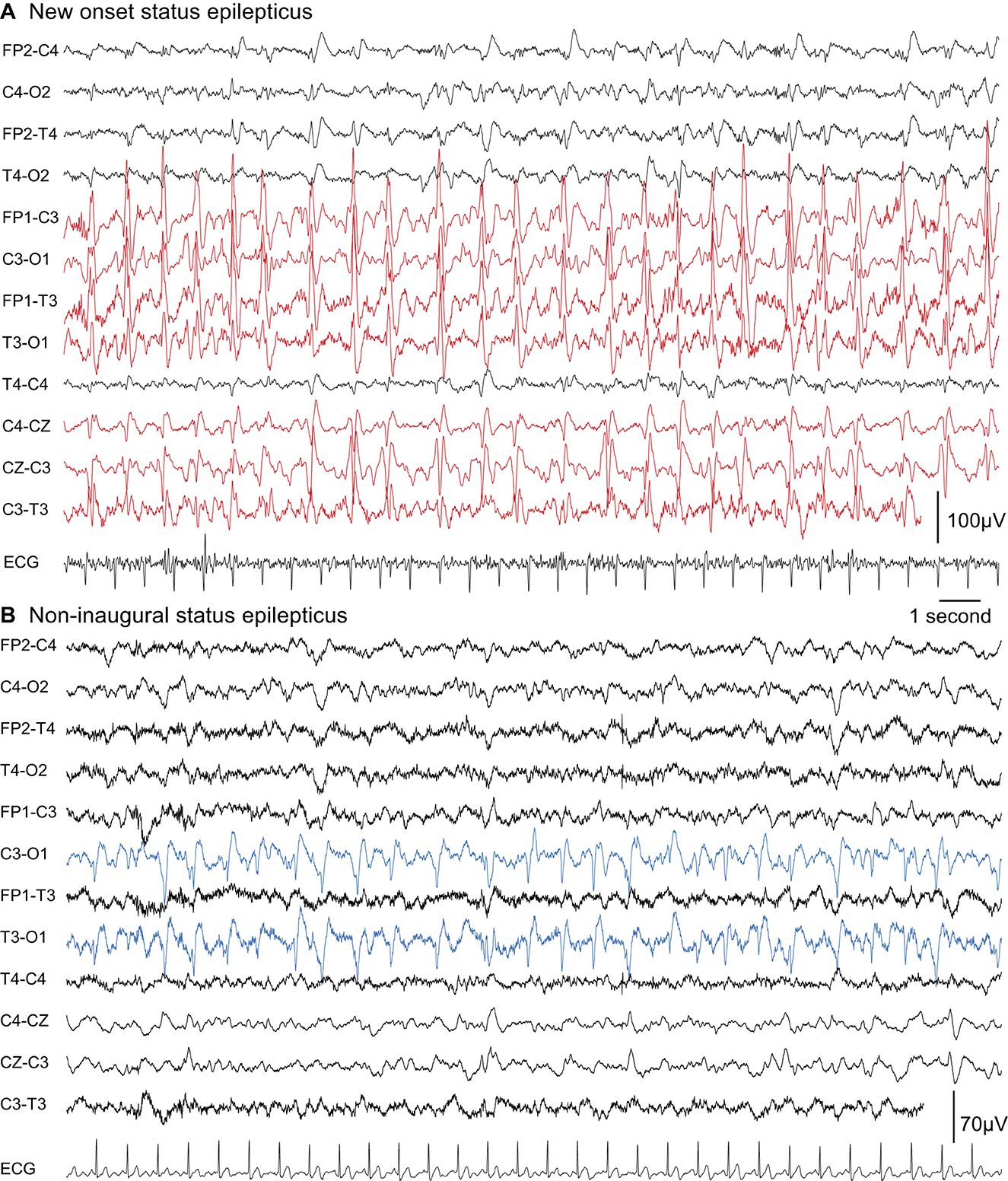
Figure 6. Two examples of EEG patterns that can be observed in NOSE and NISE. PLDs could be observed in the two types of SE but were more prevalent in NOSE. Here on the left hemisphere. (A) NOSE in a 56-year-old man (chronic psychiatric disorders and alcoholism with decompensated cirrhosis, left cerebral middle artery ischemic sequelae) who presented with a generalized convulsive SE, which became secondarily non-convulsive and super-refractory (SE lasted 41 days until death). PMAs were observed on MRI on the left hemisphere. (B) NISE in a 63-year-old man who presented with refractory non-convulsive SE (SE lasted 8 days). A context of stroke sequelae in the left middle cerebral artery region due to atheroma, alcoholism, and urinary tract infection. PMA was observed on MRI. After an initial stay of 54 days, there was an SE recurrence in 80 days leading to death in 4 months.
Our study reveals a paradox: NOSE was more severe with more patients experiencing a poor outcome at the last follow-up but was not more refractory than NISE. Causes of death also differed at different time points of follow-up, with more early deaths directly linked to SE at 1 month in the NOSE group and more remote deaths related to causal brain lesions at the final follow-up in the NISE group.
We are aware of the limitations of our study: the clinical heterogeneity of the patients, heterogeneous types of SE and etiologies, outliers, MRI performed only in approximately half of the patients, and the difficulty assessing the kinetics of PMA. However, such limits are inherent in this type of prospective research precisely because of the severity of SE that can limit inclusion. Including more than 100 patients is rare and we were able to provide longitudinal data, without any patients lost to follow-up. Moreover, when available, MRI was always performed at a high resolution (3T) and within relatively homogeneous time frames.
There is an undeniable fragility in NOSE patients at the onset: 61% had a preexisting cognitive decline (IQ Code ≥ 3.4). This fragility was not limited to the NOSE group: two-thirds of the patients had a significant disability (mRS ≥ 2) in both groups. The mean age of the patients in our study was 60 years, similar to the ages in previous cohorts: 60–65 years according to the cohort (15, 17, 23, 24, 45–47). However, NOSE generally occurs in older subjects (65 years vs. 56 years in NISE patients). Therefore, it is interesting to note that epileptic and non-epileptic patients were comparable in the literature for neurological and psychiatric history, previous psychotropic drug use, and alcohol abuse or dependence (16, 17, 24, 48). In particular, SESA was not overrepresented in NOSE.
In both groups, SE was long, lasting ≥24 h in one-third of our patients, and if associated with severe complications required resuscitation management in 35% of the cases. This is consistent with previous studies in which the duration of SE was ≥ 24 h in 24–33% of the cases (15, 16) and only 7% of SE lasted <30 min (45).
In our study, the proportions of pharmacoresistance in SE (more than 60% of the cases in both groups) contrast with the 20–40% of refractoriness reported in the literature (16, 17, 45, 48, 49), although we used the same definitions of drug resistance and clinical management according to the national recommendations for therapeutic escalation (33).
However, as in the literature, NOSE was more severe than NISE. Indeed, the severity scales of NOSE were higher (p < 0.001), the duration was longer (62 vs. 23 h on average), and the diagnostic tardiness was greater (60 vs. 10 min) resulting in a therapeutic delay. NOSE patients had more post-ictal focal neurological deficits (80% vs. 62% in NISE) and more serious complications (50% vs. 30% in NISE), especially hemodynamic complications. The length of hospital stay was also longer for NOSE patients than for NISE patients, on average 3 days. This is in line with the previously identified prognostic factors of SE, such as the age of the patient, the rapidity of the diagnosis and suitable therapeutic management, and the duration and etiology of SE (15–17, 19, 24, 47, 50, 51).
In our cohort, 36.7% of the SE were non-convulsive (NCSE), whereas NCSE accounts for 25% of the SE in the literature (21, 22, 52). NCSE is frequent (up to 47% of the SE managed in the Intensive Care Unit (53, 54) but is underestimated due to the misleading and non-specific clinical features. In fact, the diagnosis is mainly based on the EEG, and quite frequently there is a diagnostic delay and high pharmacoresistance in nearly one-third of the cases (55–58). NCSE has been associated with a longer duration and a worse prognosis than the other subtypes of SE, especially when it is inaugural because of its frequent refractoriness (50). The mortality rate of the inaugural NCSE [nearly 69% of NCSE in some cohorts (58)] can be as high as 40%, whereas it is ~10% for the other SE (59).
In a recent retrospective cohort including 85 NOSE patients, the main etiologies were acute symptomatic NOSE in 53.9%, unknown in 25.9%, progressive in 11.8%, and remote in 9.4%. For adults below the age of 60 years, the main etiology remained unknown (36.3%) followed by autoimmune-related SE (16.4%), while in the elderly (≥60 years), the primary etiology was central nervous system infection (23.3%) followed by cerebrovascular disease (20%) and intracranial tumors (20%) (23). In the 89 patients reported by Santamarina et al. (mean age of 69 years), NOSE had an acute etiology for 66.3% of the patients (46.1% brain lesions and 20.2% toxic/metabolic causes), a remote or progressive etiology for 19.1% of the patients, and remained cryptogenic for 14.6% of the patients (27).
If the etiologies overlap with these references, we emphasize different proportions according to these causes in our cohort (perhaps related to the fact that our NOSE cohort was smaller). The etiology of NOSE was acute in 43.5% of the cases vs. 8% in NISE (p < 0.0001), including an acute cerebral etiology in 21.7% of NOSE vs. 4.8% of NISE cases (p = 0.01). The etiology remained unknown in only 8.7% of the NOSE cases. However, by systematically comparing them to NISE, our results highlight the etiologies shared by both types of SE. For instance, we observed no autoimmune encephalitis, whereas this was the etiology for epilepsy in two NISE patients. We also noted 3 cases of non-convulsive NOSE that met the subacute encephalopathy and seizures in alcoholics (SESA) criteria (5, 60, 61), all with PMA on ictal MRI.
To the best of our knowledge, the only study that has prospectively compared NOSE and NISE was restricted to 122 patients >60 years old with convulsive SE. It showed that comorbidities, a low Glasgow scale score, and an inaugural nature were poor prognostic factors (62). By including younger subjects and all types of SE, we were able to demonstrate the frailty and older age of NOSE subjects.
We also observed that the mRS increased at each assessment time in both groups. However, after post-hoc analyses, baseline mRS (before SE) for NOSE was statistically different from mRS at 1, 3, and 12 months, while for NISE, it was only different from mRS at 12 months.
In our cohort, 43.6% of the NOSE patients who survived developed epilepsy in the ensuing months. For Santamarina et al., it was close to 58.7% (27), which highlights the relevance of long-term maintenance of an ASM after SE. A total of 25.7% of patients had a recurrence of SE during follow-up, including 28.2% NOSE cases [twice the rate found in a previous prospective cohort (45)]. There were more early recurrences of SE in NOSE patients (p = 0.01), probably associated with difficulty in controlling the initial SE and the underlying etiology.
We noted a high frequency of focal neurological deficits (34.4%) and cognitive complaints (70%) in both groups at 3 months but which were higher for NISE. Cognitive consequences are frequently reported in the literature and have a significant impact on quality of life (50, 63, 64). Therefore, in the clinical management of any SE, it would be relevant to conduct psychometric and standardized cognitive assessment some distance in time after NOSE and NISE to propose cognitive remediation adapted to these fragile patients.
The overall mortality of our population was high: 10%, 17%, and 26% at 1, 3, and 12 months, respectively. These rates are comparable to the mortality found in cohorts with any type of SE (NOSE and NISE, excluding post-anoxic encephalopathies) (17, 48) or even studies including only refractory SE with 24.5–25.4% mortality at 1 year (38, 65). Similarities to these rates can probably be explained by the high drug resistance in our cohort. In specific NORSE cohorts, mortality reached 22% (3, 28).
In our study, a higher global proportion of death was observed in NOSE than in NISE. The absence of statistical difference at the final follow-up does not exclude differences at distant time points and may reflect different mechanisms: more early deaths in the NOSE group directly linked to SE at 1 month and more remote deaths linked to causal brain lesions in the NISE group at final follow-up. In addition, it has been previously shown that NOSE is associated with a 15-fold increase in the risk of death in those older than 60 years (66).
The description and location of PMA in our cohort were comparable to previously published data (67–71): DWI hyperintensity with a moderate ADC restriction and FLAIR hyperintensity, preferentially in the hippocampus, the cortex, the amygdala, and the thalamus. In our cohort, both NOSE and NISE had PMAs that were comparable in appearance, location, and volume. These results are important because contrary to common belief, PMAs are not exclusive to NORSE and in general and are not exclusive to NOSE. The overall incidence of PMAs (37%) is close to the incidences found in studies that did not consider only abnormal MRI: 27.5% (25), 28% (72), and 42.5% (67). The incidence of PMAs was somewhat higher in the NISE group (42% vs. 33%) but their MRIs were performed later than those for NOSE patients. This difference could be due to the kinetics of the occurrence of PMAs.
A significant correlation has already been described between the presence of PMAs and the presence of PLDs on EEG with vigilance in the acute phase of SE, but no association was found with patient age, comorbidity, or mortality (25). Our clinical experience suggests that there is a very good anatomical correlation between the clinical symptoms of SE, the site of EEG abnormalities, and the location of PMA when present. Post-ictal motor deficits have also been more frequently associated with PMAs (53.3%) than with normal MRI (34.4%) (67). In our data, the outcome at the last follow-up changed in different proportions in the patients with PMA and those without PMA, while no correlation exists between PMA volume and mRS during follow-up. There does not appear to be any specific feature (volume, locations, and change) of PMAs that can distinguish a peri-ictal from a post-ictal state. Rapid brain imagery is recommended in the etiological assessment of any SE (10, 33). Our results highlight that in addition to the diagnostic potential and the identification of acute lesions, MRI provides prognostic information that may prove valuable in long-term patient management.
In the neuroimaging studies cited above, MRI monitoring was not systematic and completion time was extremely variable (interval of up to 1 year between the two MRIs) (68–70). In our study, MRI time was more homogeneous at ~3 months and complete reversibility of PMA was noted in 36% of patients. Although diffusion was normalized, FLAIR hyperintensity was found in 57% of patients and focal atrophy in 50% of patients, predominantly in the temporal-hippocampal regions. These sequelae raise questions about the epileptogenic value and the clinical consequences of these permanent structural abnormalities.
We observed a tendency for more periodic lateral discharges (PLDs) in NOSE, while the median time before the first EEG was similar in both groups. Despite a later diagnosis in NOSE, accessibility to EEG was not different for NOSE and NISE, which is a crucial point to remember in clinical practice. PLDs were indicative of the presence of a cortical brain lesion and associated with more frequent vigilance disorders as previously described (73). PLDs were also associated with high morbidity and mortality in studies conducted in the eighties or nineties (74–76). We were unable to determine whether there is a PLD pattern (morphology, periodicity, and amplitude) specific to each type of SE. Further studies that analyze the appearance of PLDs according to the etiology, lesion, and type of SE are warranted.
NOSE was not more refractory than NISE. Unfortunately, our data were not sufficient to highlight specificities between the particular cases of NORSE and non-inaugural refractory SE (NIRSE).
Are there certain etiologies that are particularly represented in refractory SE? In other series that focused specifically on the NORSE subgroup, the most common etiology was autoimmune encephalitis, while 52% of the cases of NORSE remained cryptogenic (3, 28, 31, 77). No autoimmune encephalitis was identified in our NOSE cohort although this etiology was repeatedly suspected and sought, while two cases of autoimmune encephalitis were included in our NISE group with a refractory SE. Two patients in our cohort met the criteria for cryptogenic NORSE: the first died within a few days despite appropriate resuscitative management while the second patient had severe cognitive impairment and loss of autonomy at 3 months.
Moreover, our data were not sufficient to isolate specific patterns of PMA between NOSE and NORSE. However, particularities in three patients should be noted: a case of claustrum hyperintensity in the NOSE group corresponding to SESA with non-refractory NCSE. In a recent study, claustral changes were reported as infrequent, occurring in 9.1% of NORSE patients (78) although the etiology for NORSE patients with claustrum involvement has not yet been elucidated. The claustrum sign has been associated with an aggressive refractory form of SE in particular cases of FIRES with cryptogenic etiology (78, 79) but never with SESA as far as we know. Two NISE patients presented with crossed cerebellar diaschisis with involvement of the cortex and the pulvinar ipsilateral to the refractory SE. Some identical cases have been described in the literature with reversible damage or the appearance of cerebellar atrophy associated with an unfavorable clinical course (80–84).
NOSE and NISE evolved in the same proportions as refractory SE and shared common patterns, such as the same types of PMAs on MRI. However, NOSE was distinguishable by the severity, a more fragile and older population at onset, and a frequent non-convulsive semiology. The causes of death differed in the early and late stages (at 1 year) in NOSE and NISE. Despite acute causal brain lesions, the inaugural character was still too often associated with a delay in diagnosis in SE, which justifies the need to more clearly specify the types of SE to constantly raise awareness among clinicians. These results also highlight the relevance of including novelty-related criteria, clinical history, and the temporality of occurrence in the nosology of status epilepticus.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Regional Ethics Committee at Toulouse University Hospital (CPP Sud-Ouest no. 04-1215). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
MB and JC: writing of the manuscript, major role in data acquisition and study design, data analysis and interpretation, and expert analysis of EEG. LV: revision of the manuscript, expert analysis of EEG, data analysis and interpretation, major role in the study design, and help with data acquisition. MD, FR, and RD: expert analysis of EEG and revision of the manuscript. EB: revision of the manuscript, data analysis, and interpretation. FB: expert analysis of MRI, major role in study design, and help with data acquisition. LG: statistical analyses and revision of the manuscript. VW: support for figures and statistical analyses. All authors contributed to the article and approved the submitted version.
MB received a Grant for Young Researchers from Toulouse University Hospital in 2015–2016.
The authors acknowledge Vanessa Rousseau, Jean-Marc Olivot, and the Neurological Intensive Care Unit Team at Toulouse University Hospital; the Neuroradiologists at Toulouse University Hospital; and Neuropsychologist, Hélène Mirabel, for all their help in acquiring data or methodology-related advice.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ASM, Anti-seizure medication; CSF, Cerebrospinal fluid; EEG, Electroencephalogram; EMSE, Epidemiology-based mortality score in status epilepticus; FLAIR, Fluid-attenuated inversion recovery; GPDs, Generalized periodic discharges; MRI, Magnetic resonance imaging; mRS, Modified Rankin Scale; NCSE, Non-convulsive status epilepticus; NOSE, New-onset status epilepticus; NORSE, New-onset refractory status epilepticus; NIRSE, Non-inaugural refractory status epilepticus; NISE, Non-inaugural status epilepticus; PLDs, Periodic lateralized discharges; PMAs, Peri-ictal MRI abnormalities; SE, Status epilepticus; SESA, Subacute encephalopathy with seizures in alcoholics; STESS, Status epilepticus severity score.
1. Jafarpour S, Hodgeman RM, De Marchi Capeletto C, de Lima MTA, Kapur K, Tasker RC, et al. New-onset status epilepticus in pediatric patients: causes, characteristics, and outcomes. Pediatr Neurol. (2018) 80:61–9. doi: 10.1016/j.pediatrneurol.2017.11.016
2. Hirsch LJ, Gaspard N, van Baalen A, Nabbout R, Demeret S, Loddenkemper T, et al. Proposed consensus definitions for new-onset refractory status epilepticus (NORSE), febrile infection-related epilepsy syndrome (FIRES), and related conditions. Epilepsia. (2018) 59:739–44. doi: 10.1111/epi.14016
3. Sculier C, Gaspard N. New onset refractory status epilepticus (NORSE). Seizure. (2019) 68:72–8. doi: 10.1016/j.seizure.2018.09.018
4. Brigo F, Tavernelli V, Nardone R, Trinka E. De novo late-onset absence status epilepticus or late-onset idiopathic generalized epilepsy? A case report and systematic review of the literature. Epileptic Disord Int Epilepsy J Videotape. (2018) 20:123–31. doi: 10.1684/epd.2018.0961
5. Fernández-Torre JL, Kaplan PW. Subacute encephalopathy with seizures in alcoholics (SESA syndrome) revisited. Seizure. (2014) 23:393–6. doi: 10.1016/j.seizure.2014.02.002
6. Gastaut H, Roger J, Roger A. The significance of certain epileptic fugues; concerning a clinical and electrical observation of temporal status epilepticus. Rev Neurol (Paris). (1956) 94:298–301.
7. Gastaut H. Clinical and electroencephalographical classification of epileptic seizures. Epilepsia. (1970) 11:102–13. doi: 10.1111/j.1528-1157.1970.tb03871.x
8. Berg AT, Berkovic SF, Brodie MJ, Buchhalter J, Cross JH, van Emde Boas W, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia. (2010) 51:676–85. doi: 10.1111/j.1528-1167.2010.02522.x
9. Lowenstein DH. Status epilepticus: an overview of the clinical problem. Epilepsia. (1999) 40 Suppl 1:S3-8; discussion S21-22. doi: 10.1111/j.1528-1157.1999.tb00872.x
10. Brophy GM, Bell R, Claassen J, Alldredge B, Bleck TP, Glauser T, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. (2012) 17:3–23. doi: 10.1007/s12028-012-9695-z
11. Chakraborty T, Hocker S. The clinical spectrum of new-onset status epilepticus. Crit Care Med. (2019) 47:970–4. doi: 10.1097/CCM.0000000000003776
12. Wasterlain CG, Fujikawa DG, Penix L, Sankar R. Pathophysiological mechanisms of brain damage from status epilepticus. Epilepsia. (1993) 34 Suppl 1:S37–53. doi: 10.1111/j.1528-1157.1993.tb05905.x
13. Chen JWY, Wasterlain CG. Status epilepticus: pathophysiology and management in adults. Lancet Neurol. (2006) 5:246–56. doi: 10.1016/S1474-4422(06)70374-X
14. Valton L, Benaiteau M, Denuelle M, Rulquin F, Hachon Le Camus C, Hein C, et al. Etiological assessment of status epilepticus. Rev Neurol (Paris). (2020) 176:408–26. doi: 10.1016/j.neurol.2019.12.010
15. Hesdorffer DC, Logroscino G, Cascino G, Annegers JF, Hauser WA. Incidence of status epilepticus in Rochester, Minnesota, 1965–1984. Neurology. (1998) 50:735–41. doi: 10.1212/WNL.50.3.735
16. Coeytaux A, Jallon P, Galobardes B, Morabia A. Incidence of status epilepticus in French-speaking Switzerland: (EPISTAR). Neurology. (2000) 55:693–7. doi: 10.1212/WNL.55.5.693
17. Knake S, Rosenow F, Vescovi M, Oertel WH, Mueller HH, Wirbatz A, et al. Incidence of status epilepticus in adults in germany: a prospective, population-based study. Epilepsia. (2001) 42:714–8. doi: 10.1046/j.1528-1157.2001.01101.x
18. Vignatelli L, Rinaldi R, Galeotti M, de Carolis P, D'Alessandro R. Epidemiology of status epilepticus in a rural area of northern Italy: a 2-year population-based study. Eur J Neurol. (2005) 12:897–902. doi: 10.1111/j.1468-1331.2005.01073.x
19. Sutter R, Marsch S, Fuhr P, Rüegg S. Mortality and recovery from refractory status epilepticus in the intensive care unit: a 7-year observational study. Epilepsia. (2013) 54:502–11. doi: 10.1111/epi.12064
20. Malter MP, Nass RD, Kaluschke T, Fink GR, Burghaus L, Dohmen C. New onset status epilepticus in older patients: clinical characteristics and outcome. Seizure. (2017) 51:114–20. doi: 10.1016/j.seizure.2017.08.006
21. Trinka E, Cock H, Hesdorffer D, Rossetti AO, Scheffer IE, Shinnar S, et al. A definition and classification of status epilepticus–Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia. (2015) 56:1515–23. doi: 10.1111/epi.13121
22. Leitinger M, Trinka E, Giovannini G, Zimmermann G, Florea C, Rohracher A, et al. Epidemiology of status epilepticus in adults: A population-based study on incidence, causes, and outcomes. Epilepsia. (2019) 60:53–62. doi: 10.1111/epi.14607
23. Deng B, Dai Y, Wang Q, Yang J, Chen X, Liu TT, et al. The clinical analysis of new-onset status epilepticus. Epilepsia Open. (2022) 7:771–780. doi: 10.1002/epi4.12657
24. Tsai MH, Chuang YC, Chang HW, Chang WN, Lai SL, Huang CR, et al. Factors predictive of outcome in patients with de novo status epilepticus. QJM Mon J Assoc Physicians. (2009) 102:57–62. doi: 10.1093/qjmed/hcn149
25. Rennebaum F, Kassubek J, Pinkhardt E, Hübers A, Ludolph AC, Schocke M, et al. Status epilepticus: clinical characteristics and EEG patterns associated with and without MRI diffusion restriction in 69 patients. Epilepsy Res. (2016) 120:55–64. doi: 10.1016/j.eplepsyres.2015.12.004
26. Treiman DM, Meyers PD, Walton NY, Collins JF, Colling C, Rowan AJ, et al. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med. (1998) 339:792–8. doi: 10.1056/NEJM199809173391202
27. Santamarina E, Gonzalez M, Toledo M, Sueiras M, Guzman L, Rodríguez N, et al. Prognosis of status epilepticus (SE): relationship between SE duration and subsequent development of epilepsy. Epilepsy Behav. (2015) 49:138–40. doi: 10.1016/j.yebeh.2015.04.059
28. Gaspard N, Foreman BP, Alvarez V, Cabrera Kang C, Probasco JC, Jongeling AC, et al. New-onset refractory status epilepticus: etiology, clinical features, and outcome. Neurology. (2015) 85:1604–13. doi: 10.1212/WNL.0000000000001940
29. Delanty N, French JA, Labar DR, Pedley TA, Rowan AJ. Status epilepticus arising de novo in hospitalized patients: an analysis of 41 patients. Seizure. (2001) 10:116–9. doi: 10.1016/S1059-1311(00)90482-5
30. Loiseau P. Morbidity and mortality of status epilepticus. Neurophysiol Clin Clin Neurophysiol. (2000) 30:155–60. doi: 10.1016/s0987-7053(00)00206-9
31. Werbaneth K, Mausolf M, Seliger J, Le S. A retrospective cohort study of new-onset refractory status epilepticus (NORSE): clinical features, timing of immunotherapy and outcomes. Epileptic Disord Int Epilepsy J Videotape. (2022) 24:867–76. doi: 10.1684/epd.2022.1466
32. Fisher RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross JH, Elger CE, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. (2014) 55:475–82. doi: 10.1111/epi.12550
33. Outin H, Blanc T, Vinatier I, le groupe d'experts. Emergency and intensive care unit management of status epilepticus in adult patients and children (new-born excluded) Société de réanimation de langue française experts recommendations. Rev Neurol (Paris). (2009) 165:297–305. doi: 10.1016/j.neurol.2009.01.048
34. Leitinger M, Beniczky S, Rohracher A, Gardella E, Kalss G, Qerama E, et al. Salzburg consensus criteria for non-convulsive status epilepticus–approach to clinical application. Epilepsy Behav. (2015) 49:158–63. doi: 10.1016/j.yebeh.2015.05.007
35. Leitinger M, Trinka E, Gardella E, Rohracher A, Kalss G, Qerama E, et al. Diagnostic accuracy of the Salzburg EEG criteria for non-convulsive status epilepticus: a retrospective study. Lancet Neurol. (2016) 15:1054–62. doi: 10.1016/S1474-4422(16)30137-5
36. Mayer SA, Claassen J, Lokin J, Mendelsohn F, Dennis LJ, Fitzsimmons BF. Refractory status epilepticus: frequency, risk factors, and impact on outcome. Arch Neurol. (2002) 59:205–10. doi: 10.1001/archneur.59.2.205
37. Ferlisi M, Shorvon S. The outcome of therapies in refractory and super-refractory convulsive status epilepticus and recommendations for therapy. Brain J Neurol. (2012) 135(Pt 8):2314–28. doi: 10.1093/brain/aws091
38. Kantanen AM, Reinikainen M, Parviainen I, Ruokonen E, Ala-Peijari M, Bäcklund T, et al. Incidence and mortality of super-refractory status epilepticus in adults. Epilepsy Behav EB. (2015) 49:131–4. doi: 10.1016/j.yebeh.2015.04.065
39. Trinka E, Kälviäinen R. 25 years of advances in the definition, classification and treatment of status epilepticus. Seizure. (2017) 44:65–73. doi: 10.1016/j.seizure.2016.11.001
40. Rossetti AO, Logroscino G, Milligan TA, Michaelides C, Ruffieux C, Bromfield EB. Status Epilepticus Severity Score (STESS): a tool to orient early treatment strategy. J Neurol. (2008) 255:1561–6. doi: 10.1007/s00415-008-0989-1
41. Leitinger M, Höller Y, Kalss G, Rohracher A, Novak HF, Höfler J, et al. Epidemiology-based mortality score in status epilepticus (EMSE). Neurocrit Care. (2015) 22:273–82. doi: 10.1007/s12028-014-0080-y
42. Jorm AF, Jacomb PA. The Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): socio-demographic correlates, reliability, validity and some norms. Psychol Med. (1989) 19:1015–22. doi: 10.1017/S0033291700005742
43. Jorm AF. The Informant Questionnaire on cognitive decline in the elderly (IQCODE): a review. Int Psychogeriatr IPA. (2004) 16:275–93. doi: 10.1017/S1041610204000390
44. Nicoli F, Scalzo F, Saver JL, Pautot F, Mitulescu A, Chaibi Y, et al. The combination of baseline magnetic resonance perfusion-weighted imaging-derived tissue volume with severely prolonged arterial-tissue delay and diffusion-weighted imaging lesion volume is predictive of MCA-M1 recanalization in patients treated with endovascular thrombectomy. Neuroradiology. (2014) 56:117–27. doi: 10.1007/s00234-013-1310-2
45. Tsetsou S, Novy J, Rossetti AO. Recurrence of status epilepticus: prognostic role and outcome predictors. Epilepsia. (2015) 56:473–8. doi: 10.1111/epi.12903
46. Pan Y, Feng Y, Peng W, Cai Y, Ding J, Wang X. Timing matters: there are significant differences in short-term outcomes between two time points of status epilepticus. BMC Neurol. (2022) 22:348. doi: 10.1186/s12883-022-02868-y
47. Roberg LE, Monsson O, Kristensen SB, Dahl SM, Ulvin LB, Heuser K, et al. Prediction of long-term survival after status epilepticus using the ACD score. JAMA Neurol. (2022) 79:604–13. doi: 10.1001/jamaneurol.2022.0609
48. Aukland P, Lando M, Vilholm O, Christiansen EB, Beier CP. Predictive value of the Status Epilepticus Severity Score (STESS) and its components for long-term survival. BMC Neurol. (2016) 16:213. doi: 10.1186/s12883-016-0730-0
49. Kantanen AM, Kälviäinen R, Parviainen I, Ala-Peijari M, Bäcklund T, Koskenkari J, et al. Predictors of hospital and one-year mortality in intensive care patients with refractory status epilepticus: a population-based study. Crit Care Lond Engl. (2017) 21:71. doi: 10.1186/s13054-017-1661-x
50. Power KN, Gramstad A, Gilhus NE, Engelsen BA. Adult nonconvulsive status epilepticus in a clinical setting: semiology, aetiology, treatment and outcome. Seizure. (2015) 24:102–6. doi: 10.1016/j.seizure.2014.09.007
51. Choi SA, Lee H, Kim K, Park SM, Moon HJ, Koo YS, et al. Mortality, disability, and prognostic factors of status epilepticus: a nationwide population-based retrospective cohort study. Neurology. (2022) 99:e1393–401. doi: 10.1212/WNL.0000000000200912
52. Cascino GD. Nonconvulsive status epilepticus in adults and children. Epilepsia. (1993) 34 Suppl 1:S21–28. doi: 10.1111/j.1528-1157.1993.tb05903.x
53. Rudin D, Grize L, Schindler C, Marsch S, Rüegg S, Sutter R. High prevalence of nonconvulsive and subtle status epilepticus in an ICU of a tertiary care center: a three-year observational cohort study. Epilepsy Res. (2011) 96:140–50. doi: 10.1016/j.eplepsyres.2011.05.018
54. Laccheo I, Sonmezturk H, Bhatt AB, Tomycz L, Shi Y, Ringel M, et al. Non-convulsive status epilepticus and non-convulsive seizures in neurological ICU patients. Neurocrit Care. (2015) 22:202–11. doi: 10.1007/s12028-014-0070-0
55. Kaplan PW. Assessing the outcomes in patients with nonconvulsive status epilepticus: nonconvulsive status epilepticus is underdiagnosed, potentially overtreated, and confounded by comorbidity. J Clin Neurophysiol Off Publ Am Electroencephalogr Soc. (1999) 16:341–52 (discussion 353). doi: 10.1097/00004691-199907000-00006
56. Sutter R, Kaplan PW. The neurophysiologic types of nonconvulsive status epilepticus: EEG patterns of different phenotypes. Epilepsia. (2013) 54 Suppl 6:23–7. doi: 10.1111/epi.12269
57. Sutter R, Semmlack S, Kaplan PW. Nonconvulsive status epilepticus in adults - insights into the invisible. Nat Rev Neurol. (2016) 12:281–93. doi: 10.1038/nrneurol.2016.45
58. Baysal-Kirac L, Cakar MM, Altiokka-Uzun G, Guncan Z, Guldiken B. Electroclinical patterns in patients with nonconvulsive status epilepticus: etiology, treatment, and outcome. Epilepsy Behav. (2021) 114(Pt A):107611. doi: 10.1016/j.yebeh.2020.107611
59. Rossetti AO, Trinka E, Stähli C, Novy J. New ILAE versus previous clinical status epilepticus semiologic classification: analysis of a hospital-based cohort. Epilepsia. (2016) 57:1036–41. doi: 10.1111/epi.13403
60. Fernández-Torre JL, Kaplan PW. Subacute encephalopathy with seizures in alcoholics syndrome: a subtype of nonconvulsive status epilepticus. Epilepsy Curr. (2019) 19:77–82. doi: 10.1177/1535759719835676
61. LaRoche SM, Shivdat-Nanhoe R. Subacute encephalopathy and seizures in alcoholics (SESA) presenting with non-convulsive status epilepticus. Seizure. (2011) 20:505–8. doi: 10.1016/j.seizure.2011.02.008
62. Verma A, Kumar A, Sachan D. Comparison of clinical profile and outcome of de novo convulsive status epilepticus with those with a past history of epilepsy in the elderly populace. Acta Neurol Taiwanica. (2022) 31:131–6.
63. Adachi N, Kanemoto K, Muramatsu R, Kato M, Akanuma N, Ito M, et al. Intellectual prognosis of status epilepticus in adult epilepsy patients: analysis with Wechsler Adult Intelligence Scale-revised. Epilepsia. (2005) 46:1502–9. doi: 10.1111/j.1528-1167.2005.05005.x
64. Sheppard E, Lippé S. Cognitive outcome of status epilepticus in children. Epilepsy Res Treat. (2012) 2012:984124. doi: 10.1155/2012/984124
65. Delaj L, Novy J, Ryvlin P, Marchi NA, Rossetti AO. Refractory and super-refractory status epilepticus in adults: a 9-year cohort study. Acta Neurol Scand. (2016) 135:92–9. doi: 10.1111/ane.12605
66. Canouï-Poitrine F, Bastuji-Garin S, Alonso E, Darcel G, Verstichel P, Caillet P, et al. Risk and prognostic factors of status epilepticus in the elderly: a case-control study. Epilepsia. (2011) 52:1849–56. doi: 10.1111/j.1528-1167.2011.03168.x
67. Nakae Y, Kudo Y, Yamamoto R, Dobashi Y, Kawabata Y, Ikeda S, et al. Relationship between cortex and pulvinar abnormalities on diffusion-weighted imaging in status epilepticus. J Neurol. (2016) 263:127–32. doi: 10.1007/s00415-015-7948-4
68. Cianfoni A, Caulo M, Cerase A, Della Marca G, Falcone C, Di Lella GM, et al. Seizure-induced brain lesions: a wide spectrum of variably reversible MRI abnormalities. Eur J Radiol. (2013) 82:1964–72. doi: 10.1016/j.ejrad.2013.05.020
69. Ohe Y, Hayashi T, Deguchi I, Fukuoka T, Horiuchi Y, Maruyama H, et al. MRI abnormality of the pulvinar in patients with status epilepticus. J Neuroradiol J Neuroradiol. (2014) 41:220–6. doi: 10.1016/j.neurad.2013.09.003
70. Szabo K, Poepel A, Pohlmann-Eden B, Hirsch J, Back T, Sedlaczek O, et al. Diffusion-weighted and perfusion MRI demonstrates parenchymal changes in complex partial status epilepticus. Brain J Neurol. (2005) 128(Pt 6):1369-76. doi: 10.1093/brain/awh454
71. Chatzikonstantinou A, Gass A, Förster A, Hennerici MG, Szabo K. Features of acute DWI abnormalities related to status epilepticus. Epilepsy Res. (2011) 97:45–51. doi: 10.1016/j.eplepsyres.2011.07.002
72. Yoshimura H, Matsumoto R, Ueda H, Ariyoshi K, Kawamoto M, Ishii J, et al. Status epilepticus in the elderly: prognostic implications of rhythmic and periodic patterns in electroencephalography and hyperintensities on diffusion-weighted imaging. J Neurol Sci. (2016) 370:284–9. doi: 10.1016/j.jns.2016.09.062
73. Dunand AC, Jallon P. Pseudoperiodic and paroxysmal electroencephalographic activities. Neurophysiol Clin Clin Neurophysiol. (2002) 32:2–37. doi: 10.1016/s0987-7053(01)00288-x
74. Snodgrass SM, Tsuburaya K, Ajmone-Marsan C. Clinical significance of periodic lateralized epileptiform discharges: relationship with status epilepticus. J Clin Neurophysiol Off Publ Am Electroencephalogr Soc. (1989) 6:159–72. doi: 10.1097/00004691-198904000-00003
75. Treiman DM, Walton NY, Kendrick C. A progressive sequence of electroencephalographic changes during generalized convulsive status epilepticus. Epilepsy Res. (1990) 5:49–60. doi: 10.1016/0920-1211(90)90065-4
76. Jaitly R, Sgro JA, Towne AR, Ko D, DeLorenzo RJ. Prognostic value of EEG monitoring after status epilepticus: a prospective adult study. J Clin Neurophysiol Off Publ Am Electroencephalogr Soc. (1997) 14:326–34. doi: 10.1097/00004691-199707000-00005
77. Lattanzi S, Leitinger M, Rocchi C, Salvemini S, Matricardi S, Brigo F, et al. Unraveling the enigma of new-onset refractory status epilepticus: a systematic review of aetiologies. Eur J Neurol. (2022) 29:626–47. doi: 10.1111/ene.15149
78. Kim HJ, Lee SA, Kim HW, Kim SJ, Jeon SB, Koo YS. The timelines of MRI findings related to outcomes in adult patients with new-onset refractory status epilepticus. Epilepsia. (2020) 61:1735–48. doi: 10.1111/epi.16620
79. Meletti S, Giovannini G, d'Orsi G, Toran L, Monti G, Guha R, et al. New-onset refractory status epilepticus with claustrum damage: definition of the clinical and neuroimaging features. Front Neurol. (2017) 8:111. doi: 10.3389/fneur.2017.00111
80. Massaro AM. Teaching neuroimages: crossed cerebellar diaschisis in hemispheric status epilepticus. Neurology. (2012) 79:e182. doi: 10.1212/WNL.0b013e318274de51
81. Al-Jafen BN, Alanazy MH, Scott JN, Pillay N. Magnetic resonance imaging of crossed cerebellar diaschisis and bright pulvinar in status epilepticus. Neurosci Riyadh Saudi Arab. (2012) 17:259–61.
82. Ahn HS, Kim KK. Two cases of crossed cerebellar diaschisis with or without thalamic lesion on brain MRI in status epilepticus. J Epilepsy Res. (2014) 4:74–7. doi: 10.14581/jer.14015
83. Graffeo CS, Snyder KA, Nasr DM, Murphy ME, Carr CM, Hocker SE. Prognostic and mechanistic factors characterizing seizure-associated crossed cerebellar diaschisis. Neurocrit Care. (2016) 24:258–63. doi: 10.1007/s12028-015-0155-4
Keywords: status epilepticus, new-onset status epilepticus, new-onset refractory status epilepticus (NORSE), peri-ictal MRI abnormalities, outcome, epilepsy, refractory status epilepticus (RSE)
Citation: Benaiteau M, Valton L, Gardy L, Denuelle M, Debs R, Wucher V, Rulquin F, Barbeau EJ, Bonneville F, Pariente J and Curot J (2023) Specific profiles of new-onset vs. non-inaugural status epilepticus: From diagnosis to 1-year outcome. Front. Neurol. 14:1101370. doi: 10.3389/fneur.2023.1101370
Received: 17 November 2022; Accepted: 06 January 2023;
Published: 03 February 2023.
Edited by:
Julia Jacobs, University of Freiburg Medical Center, GermanyReviewed by:
Jagarlapudi M. Murthy, Care Hospitals, IndiaCopyright © 2023 Benaiteau, Valton, Gardy, Denuelle, Debs, Wucher, Rulquin, Barbeau, Bonneville, Pariente and Curot. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie Benaiteau,  bWFyaWUuYmVuYWl0ZWF1QGNodS1seW9uLmZy; Luc Valton, dmFsdG9uLmxAY2h1LXRvdWxvdXNlLmZy; Jonathan Curot, am9uYXRoYW4uY3Vyb3RAY25ycy5mcg==
bWFyaWUuYmVuYWl0ZWF1QGNodS1seW9uLmZy; Luc Valton, dmFsdG9uLmxAY2h1LXRvdWxvdXNlLmZy; Jonathan Curot, am9uYXRoYW4uY3Vyb3RAY25ycy5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.