
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Neurol. , 12 April 2023
Sec. Stroke
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1082275
 Ana Luíza Vieira de Araújo1Raul D. Santos2,3
Ana Luíza Vieira de Araújo1Raul D. Santos2,3 Marcio Sommer Bittencourt4Roberto Nery Dantas Jr.2,3
Marcio Sommer Bittencourt4Roberto Nery Dantas Jr.2,3 Carlos André Oshiro1Cesar Higa Nomura2,3
Carlos André Oshiro1Cesar Higa Nomura2,3 Edson Bor-Seng-Shu1
Edson Bor-Seng-Shu1 Marcelo de Lima Oliveira1
Marcelo de Lima Oliveira1 Claudia da Costa Leite5
Claudia da Costa Leite5 Maria da Graça Morais Martin5Maramelia Miranda Alves6
Maria da Graça Morais Martin5Maramelia Miranda Alves6 Gisele Sampaio Silva6Victor Marinho Silva1
Gisele Sampaio Silva6Victor Marinho Silva1 Adriana Bastos Conforto1*
Adriana Bastos Conforto1*Background: The coronary calcium score (CAC) measured on chest computerized tomography is a risk marker of cardiac events and mortality. We compared CAC scores in two multiethnic groups without symptomatic coronary artery disease: subjects in the chronic phase after stroke or transient ischemic attack and at least one symptomatic stenosis ≥50% in the carotid or vertebrobasilar territories (Groupathero) and a control group (Groupcontrol).
Methods: In this cross-sectional study, Groupathero included two subgroups: GroupExtraorIntra, with stenoses in either cervical or intracranial arteries, and GroupExtra&Intra, with stenoses in at least one cervical and one intracranial artery. Groupcontrol had no history of prior stroke/transient ischemic attacks and no stenoses ≥50% in cervical or intracranial arteries. Age and sex were comparable in all groups. Frequencies of CAC ≥100 and CAC > 0 were compared between Groupathero and Groupcontrol, as well as between GroupExtraorIntr, GroupExtra&Intra, and Groupcontrol, with bivariate logistic regressions. Multivariate analyses were also performed.
Results: A total of 120 patients were included: 80 in Groupathero and 40 in Groupcontrol. CAC >0 was significantly more frequent in Groupathero (85%) than Groupcontrol (OR, 4.19; 1.74–10.07; p = 0.001). Rates of CAC ≥100 were not significantly different between Groupathero and Groupcontrol but were significantly greater in GroupExtra&Intra (n = 13) when compared to Groupcontrol (OR 4.67; 1.21–18.04; p = 0.025). In multivariate-adjusted analyses, “Groupathero” and “GroupExtra&Intra” were significantly associated with CAC.
Conclusion: The frequency of coronary calcification was higher in subjects with stroke caused by large-artery atherosclerosis than in controls.
Unlike myocardial infarction which is caused by atherosclerosis in more than 90% of the cases (1), only ~25% of ischemic strokes (IS) are attributable to atherosclerosis (2–4). Classification systems based on results of clinical, neuroimaging, and laboratory tests aim to determine the most likely stroke etiology. According to TOAST (Trial of Org 10172 in Acute Stroke Treatment) criteria, a diagnosis of “large-artery atherosclerosis” can be made in the presence of clinical and brain imaging findings consistent with >50% stenosis or occlusion of a major brain artery or a branch cortical artery, presumably due to atherosclerosis (5). A diagnosis of “evident large-artery atherosclerosis” can be made according to the Causative Classification of Stroke System (CCS), if the severity of the stenosis is ≥50% in intracranial or cervical arteries that supply the territory affected by the stroke, and other causes are excluded (6).
Patients with IS may have polyvascular disease with concomitant coronary (20%) or peripheral artery disease (22%) (7–9). Two seminal studies assessed the rates of asymptomatic coronary artery disease (CAD) in patients with IS or transient ischemic attack (TIA) in countries with predominantly White populations. Rokey et al. prospectively assessed patients with mild IS or TIA with Thallium-201 scintigraphy and exercise radionuclide ventriculography (10). Abnormal cardiac scans consistent with CAD were found in 41.2% (14/34) of the patients with no history or ECG signs of myocardial ischemia. Chimowitz et al. (11) specifically addressed the rates of asymptomatic CAD in patients with cerebrovascular ischemic disease of different etiologies. Abnormal stress tests were significantly more frequent (50%; 15/30) in patients with large-artery IS or TIA and no symptoms of CAD than in patients with other causes of brain ischemia (23%; 9/39). In studies performed more than a decade later, asymptomatic coronary artery stenosis ≥50% was described in 18–20% of French patients with non-cardioembolic IS and associated with an increased risk of death (12, 13).
The coronary calcium score (CAC) quantified on chest non-contrast computed tomography (CT) is an excellent non-invasive predictor of atherosclerotic cardiovascular risk (14–16). CAC is a surrogate of coronary plaque burden and is independently associated with the risk of myocardial infarction or mortality (17–19). In the MESA study, the annual frequencies of cardiovascular events in asymptomatic subjects were: CAC = 0, 0.4%; CAC 1–99, 0.8%; and CAC ≥ 100, 2.4% (20).
In the MESA study, CAC = 0 identified a group of individuals with a very low risk of events in 11 years of follow-up. CAC > 0 encompasses all positive scores and significantly identifies individuals with a greater risk of events in comparison with those with CAC = 0. CAC ≥ 100 has been classically used to make comparisons with CAC = 0 and is a marker of atherosclerotic cardiovascular disease (ASCVD) events consistent with the recommendation of the ACC/AHA guidelines of ≥0.75% per year risk of myocardial infarction, death, and stroke-a value considered as a threshold to justify the use of statins in primary prevention for people without overt hypercholesterolemia (21).
In Japanese patients with IS not caused by cardiac embolism or symptomatic carotid artery disease, without symptoms of CAD, absolute CAC scores were significantly higher than in controls, suggesting a greater risk of MI or death (22). In Korean patients with IS, without symptoms of CAD, CAC scores were associated with severe CAD assessed by computed tomography coronary angiography. Severe CAD was also associated with the presence of stenoses due to atherosclerosis in cervicocephalic arteries (23). In Chinese patients, CAC scores were significantly higher in patients with acute IS caused by atherosclerosis than in a control group composed of subjects with asymptomatic carotid atherosclerosis (24).
There is limited information about subclinical coronary artery disease in multiethnic patients with ischemic stroke caused by large-artery atherosclerosis. The main goal of this study was to compare CAC scores in subjects with IS specifically caused by large-artery atherosclerosis (Groupathero) and in controls (Groupcontrol) in Brazil, a country with a highly miscegenated population. We hypothesized that the frequency of CAC ≥100 and CAC >0, as well as absolute CAC scores, would be higher in Groupathero than in Groupcontrol. In addition, we expected that patients with symptomatic cervical and intracranial stenoses ≥50% due to atherosclerosis (GroupExtra&Intra) would have a greater extent of subclinical CAD than patients with symptomatic, exclusively cervical or intracranial stenoses ≥50% (GroupExtraorIntra).
In this cross-sectional study, patients were recruited from two outpatient stroke clinics at public university hospitals (Hospital das Clínicas/São Paulo University and São Paulo Hospital/São Paulo Federal University) in Brazil between September 2015 and March 2018. Controls with comparable age and sex distributions were recruited from non-consanguineous companions of patients in order to include subjects with similar socioeconomic status and access to healthcare in a large urban center of a middle-income country. Age and sex of the included patients were continuously updated in the enrollment log. A subject would be invited to participate in Groupcontrol if he/her had the same sex of a patient and his/her age matched the age of the patient ± 10 years. The protocol was approved by the Institutional Review Board (protocol number 1.175.113), and all patients provided written informed consent.
Subjects aged 45–80 years were included. History/symptoms of coronary heart disease or pathologic Q waves in the electrocardiogram were exclusion criteria for both groups. Electrocardiograms were performed in all subjects prior to inclusion. Specific criteria for patients with atherosclerosis (Groupathero) and controls (Groupcontrol) are listed below.
Inclusion criteria: The inclusion criteria were as follows: IS in the internal carotid artery or vertebrobasilar territory in the past 15 years, confirmed by computerized tomography (CT) or magnetic resonance imaging; stenosis ≥50% in cervical, intracranial, or both segments of these arteries, diagnosed by computed tomography angiography, magnetic resonance angiography (MRA), or digital subtraction angiography within 6 months post-stroke.
Exclusion criterion: IS etiology different from evident or probable large-artery atherosclerosis, according to the CCS (5, 21).
Groupathero was divided into two subgroups: GroupExtraorIntra (stenoses ≥50% in either a cervical or an intracranial artery supplying the territory affected by IS) and GroupExtra&Intra (stenoses ≥50% in at least one cervical and at least one intracranial artery).
Inclusion criteria were age and sex comparable to those of subjects in Groupathero. Exclusion criteria were a history of transient ischemic attack (TIA) or stroke; stenoses ≥50% in a cervical or intracranial artery diagnosed by MRA or transcranial Doppler and cervical Doppler. Cervical and intracranial MRA or cervical and transcranial Doppler were performed in all subjects.
Demographic data, history of hypertension, diabetes, hypercholesterolemia, peripheral artery disease, smoking, and metabolic syndrome were assessed on the day of inclusion in the study. Definitions are shown in Supplementary material 1. The use of antihypertensive, antidiabetic, antiplatelet drugs, or statins was also registered. The results of routine laboratory exams from Groupathero were retrieved from electronic records. Tests were ordered for controls and patients if no blood workup had been performed within 6 months prior to enrollment.
Cardiovascular risk was estimated by the pooled cohort equations (PCE), a well-established, global measure of vascular risk according to the 2013 ACC/AHA recommendations, assessed according to the following variables: sex, age, race, total cholesterol, HDL cholesterol, systolic blood pressure, diabetes, and smoking status (25). This quantitative risk assessment method predicts the 10-year risk of developing a first cardiovascular event, defined as non-fatal myocardial infarction, death from CAD, or fatal or non-fatal stroke among people with no cardiovascular disease (26, 27).
The severity of neurological impairments caused by stroke was defined by scores in the National Institutes of Health Stroke Scale (NIHSS) (28–30) and the severity of disability was evaluated by the modified Rankin Scale (29). Both scales were evaluated on the day of inclusion in the study.
The primary outcome was CAC ≥100 in the two main groups (Groupathero and Groupcontrol). The secondary outcomes were CAC >0 and CAC absolute values in the main groups and CAC ≥100, CAC >0, and absolute CAC values in subgroups (GroupExtraorIntra and GroupExtra&Intra). Outcome analyses were adjusted for PCE scores.
Coronary calcium score was acquired by a 320-detector row CT scanner (Aquilion ONE, Canon Medical System Corporation, Otawara, Japan) at the Heart Institute (InCor)/University of São Paulo Medical School, São Paulo, Brazil.
The protocol consisted of a prospective acquisition in the inspiratory apnea, under electrocardiographic gating with a tube voltage of 120 kV, and the current was adjusted according to the patient's body mass index. The collimation pattern of the apparatus was 320 × 0.5 mm and the rotation speed time was 0.35 s. Sequential slices with 3.0 mm spacing were obtained, which is the standard method in clinical practice, as previously described (17). The effective radiation dose (in mSv) was calculated and controlled in all cases.
The images were fully analyzed through a dedicated workstation (Aquarius, Intuition Edition, TeraRecon Inc., Version 4.4.11, California, USA) by a single experienced cardiologist (RD) blinded to clinical data using the scoring system previously described by Agatston et al. (17). All subjects were categorized in CAC ≥100 or < 100, as well as in CAC = 0 or >0.
Continuous variables are expressed as mean ± standard deviation (SD), whereas categorical variables are presented as frequencies. Between-group comparisons of baseline characteristics were performed with unpaired t-tests, Mann–Whitney tests, likelihood tests, chi-square tests, or Fisher's exact tests, according to the nature and distribution of the data.
Frequencies of CAC = 0 or >0 and CAC < 100 or ≥100 between Groupathero and Groupcontrol, as well as between subgroups GroupExtraorIntra or GroupExtra&Intra and Groupcontrol, were compared with bivariate logistic regression. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated. The sample size was not formally estimated because no preliminary data were available.
Multiple logistic regression was performed to identify independently associated factors of CAC ≥100 or CAC >0. In Model 1, the independent variables were PCE and Groupathero (Model 1).
In addition, in Model 2, we calculated “PCEwithoutstatinuse” for statin users by estimating the likely LDL-C level in the absence of statin use as previously described [LDL-C level+(30% x LDL-C level)] (31). This analysis was performed because there is evidence that statin therapy may influence CAC (32). The independent variables were PCEwithoutstatinuse and Groupathero.
Comparisons of absolute CAC values between groups were performed with the Mann–Whitney test and between GroupExtraorIntra, GroupExtra&Intra, and Groupcontrol, with the Kruskal–Wallis test. Post-hoc analyses were made with Dunn's multiple comparisons.
We also evaluated absolute calcium scores as a continuous variable, using the base-10 logarithm of the sum of the coronary calcium score plus 1 [log10 (CAC + 1)]. The addition of 1 to the calcium score before logarithmic transformation was performed so that patients with a calcium score of zero could be included in the analysis as previously described.
A p-value of < 0.05 was considered statistically significant. The tests were performed using SPSS for Windows version 22.0.
Figure 1 shows the flowchart of inclusion. Table 1 shows the baseline characteristics of the subjects in Groupathero (n = 80) and Groupcontrol (n = 40). In Groupathero, the median modified Rankin score was 2 (IQR, 2); the median NIHSS at the time of inclusion was 1.5 (IQR, 3.3), and the median time from stroke onset was 2 years (0–11.5). More than half (55%) of the patients were assessed within the 1st-year post-stroke and 32.5% within 2–5 years.
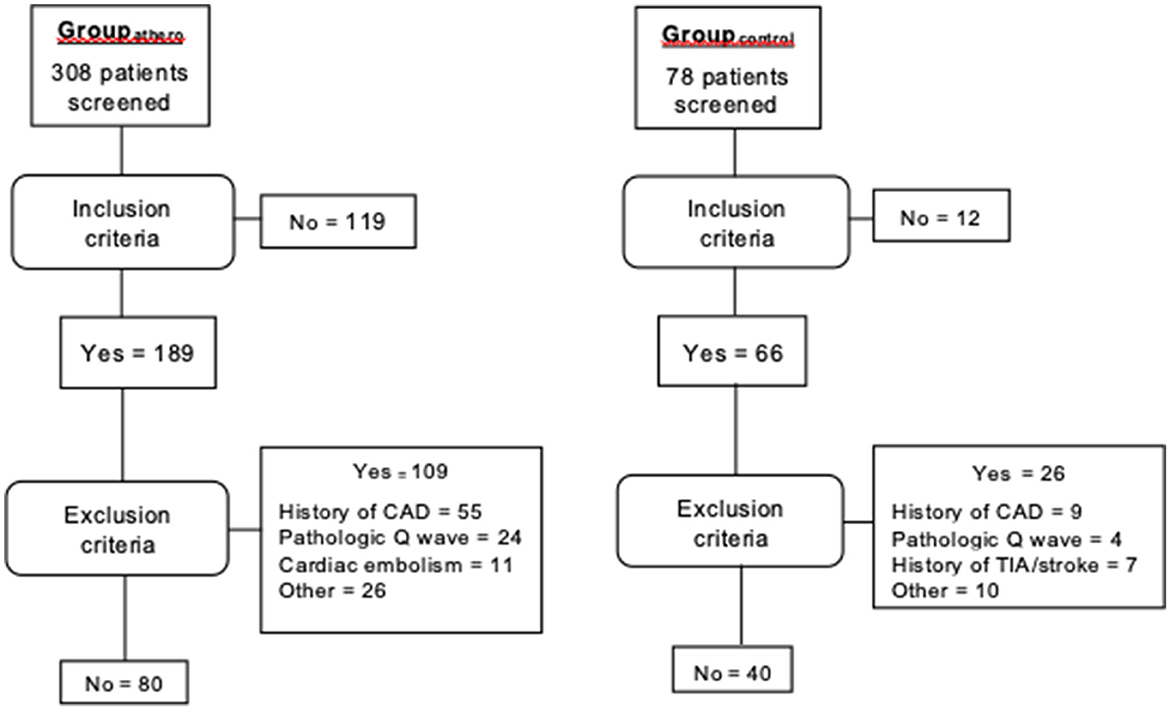
Figure 1. Flow diagram. CAD, coronary artery disease; TIA, transient ischemic attack. Some subjects had more than one exclusion criteria.
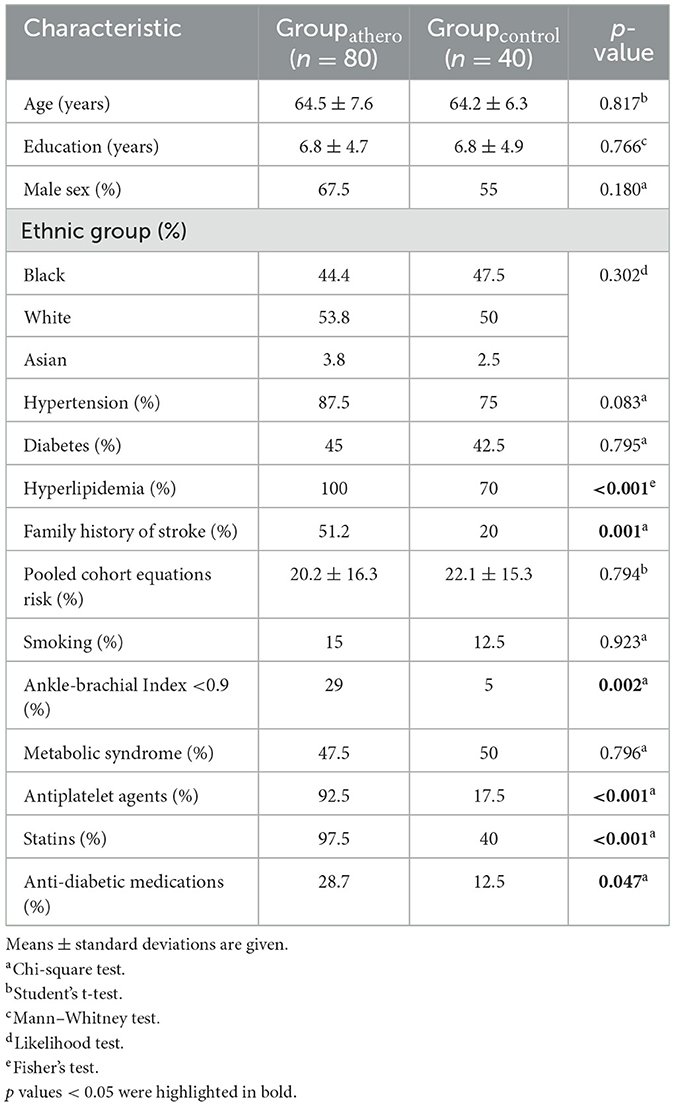
Table 1. Characteristics of the subjects.
There were no significant differences between groups in relation to age, sex, rates of hypertension, diabetes mellitus, smoking, metabolic syndrome, or in the estimated cardiovascular risk according to PCE. Hyperlipidemia, family history of stroke, abnormal ankle-brachial index, use of antiplatelet drugs, statins, and antidiabetic and antihypertensive drugs were more frequent in Groupathero than in Groupcontrol.
There were no significant differences in characteristics between subjects in GroupExtra&Intra and in GroupExtraorIntra (Supplementary Table 1).
CAC ≥100 was present in 46.3% (n = 37) subjects in Groupathero and 32.5% (n = 13) in Groupcontrol (OR, 1.79; 95% CI, 0.81–3.96; p = 0.152). Table 2 shows the results of univariate subgroup analyses. CAC ≥100 was significantly more frequent in GroupExtra&Intra than in patients in Groupcontrol. There were no differences between proportions of CAC ≥100 in GroupExtra&Intra and in GroupExtraorIntra.

Table 2. Comparisons in rates of coronary calcium scores (CAC) ≥100 or >0 between Groupcontrol, GroupExtraorIntra, or GroupExtra&Intra.
CAC >0 was found in 85% (n = 68) subjects in Groupathero and 57.5% (n = 23) in Groupcontrol (OR, 4.19; 95% CI, 1.74–10.07; p = 0.001). Table 2 shows the results of subgroup analyses. CAC >0 was significantly more frequent in GroupExtraorIntra or GroupExtra&Intra than in Groupcontrol.
CAC scores were significantly higher in Groupathero (median, 75.4; range: 0–2766.1) compared to Groupcontrol (median, 11.7; range: 0–2153.7) (p = 0.024).
CAC absolute values were significantly greater in GroupExtra&Intra (median 109.51; range: 0–2766) and GroupExtraorIntra (median 56.26; range: 0–1817) than in Groupcontrol (p = 0.028), but the post-hoc analysis did not show significant differences between GroupExtraorIntra and Groupcontrol (p = 0.194), GroupExtra&Intra and Groupcontrol (p = 0.075), or GroupExtraorIntra compared to GroupExtra&Intra (p = 0.308).
In multiple logistic regression, the variable “Groupathero” was significantly associated with CAC >0 and Log (CAC + 1) (Table 3).
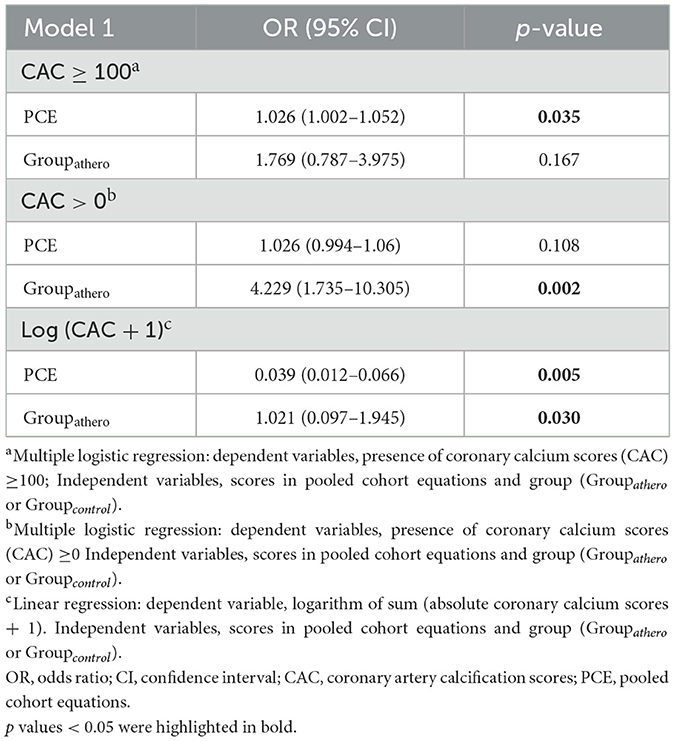
Table 3. Multivariate analyses.
Figure 2 shows subgroup analyses of CAC absolute values. Only GroupExtra&Intra was significantly associated with Log (CAC + 1) (95% CI, 0.40–3.43; p = 0.013).
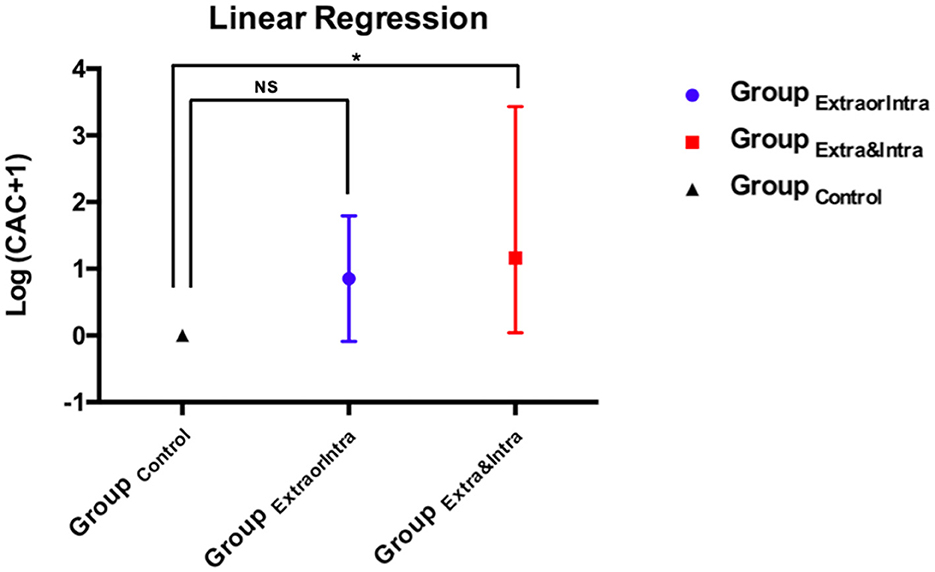
Figure 2. Linear regression of log (CAC + 1) between subgroups (Groupcontrol, GroupExtraorIntra, GroupExtra&Intra). The asterisk indicates the statistically significant difference in reference to the control group. NS, non-statistically significant difference.
The results of Model 2 are shown in Supplementary Table 2. The results of multivariate analyses, with calculated “PCEwithoutstatinuse” for statin users, were similar to those obtained in Model 1.
The main finding of this study was a significantly greater burden of subclinical coronary atherosclerosis in individuals with IS caused by cervicocephalic atherosclerosis than in controls. In Groupathero, 85% of the patients had CAC >0 despite the absence of CAD symptoms. After adjusted analysis, stroke due to large-artery atherosclerosis was significantly associated with CAC >0 or CAC scores in comparison with controls.
The frequency of more extensive CAC (CAC ≥100) was higher in Groupathero than in Groupcontrol, but this difference was not statistically significant. Interestingly, CAC ≥100 was significantly more frequent in the subgroup with the biggest load of atherosclerosis (GroupExtra&Intra) than in the subgroup with atherosclerosis restricted to intra- or extracranial arteries (GroupExtraorIntra). Multivariate analysis also showed a statistically significant association between GroupExtra&Intra and higher absolute levels of CAC, implying that patients with more extensive cervicocephalic atherosclerosis may be at a greater risk of subclinical coronary atherosclerosis and therefore a greater future risk of coronary events, than those with either cervical or intracranial atherosclerosis. This greater risk could point to a need for a more detailed assessment of CAD in these patients, especially considering that many subjects with stroke have physical disabilities that could mask the onset of angina symptoms related to mobility and, therefore, delay the diagnosis of obstructive CAD (33, 34). In addition, these results pave the way for future studies to investigate the effects of more aggressive treatment measures for this very high-risk subgroup, such as the use of PCSK9 inhibitors (35–37). Future clinical trials are needed to confirm this hypothesis.
Ethnicity may influence the distribution of atherosclerotic plaques across vascular beds. Intracranial atherosclerosis, for instance, predominates in Black, Hispanic, and Asian populations (38). CAC scores are higher in Black and Hispanic subjects than in White and Asian individuals (39). In our study, 44.4% of the patients were Black. Our results are in line with those of prior studies that investigated rates of subclinical CAD in patients from countries with predominantly White or Asian populations and IS caused by diverse etiologies (40, 41), non-cardioembolic stroke (12, 13), or atherosclerosis (24).
Patients with IS caused by atherosclerosis have a greater risk of cardiovascular events or all-cause mortality than controls with comparable estimated vascular risk (8). Antiplatelet drugs, statins, and other medications as well as behavioral interventions to control vascular risk factors are recommended for patients with IS caused by atherosclerosis according to current guidelines. However, adherence to secondary prevention measures may be challenging in clinical practice. Awareness of their great risk of cardiovascular death may strengthen the drive for patients to optimize compliance with medical therapy and changes in lifestyle.
CAC scores are associated with the risk of CAD and stroke in asymptomatic subjects (42, 43). In the present study, despite the lack of symptoms and the absence of stenoses ≥50% in cervical or intracranial arteries due to atherosclerosis, subjects in the control group were found to be at high cardiovascular risk according to PCE scores. Despite their high-risk profile, subjects in Groupcontrol were significantly less likely to use medications to treat hypertension, diabetes, or dyslipidemia. This finding may reflect the underdiagnosis and treatment of these conditions in asymptomatic subjects in low- and middle-income countries like Brazil (44). Unfortunately, measures to control risk factors for vascular disease may only start after a major cardiovascular event such as stroke.
This study has some limitations. It has limited power for the comparison of rates of CAC ≥100 between Groupathero and controls. A multicenter study would be advisable to include a greater number of subjects for this comparison. The control group included subjects without cerebrovascular disease or stenoses ≥50% in cervical or intracranial arteries. Other studies are necessary to compare CAC scores in subjects with IS caused by large-artery atherosclerosis and in those with other IS etiologies. Moreover, the inclusion of time from a stroke in Groupathero, up to 15 years, might lead to bias. Over the years, there might be a progression of coronary calcification as well as the worsening of control of cardiovascular risk factors. However, it is unlikely that this may have influenced our results because: First, more than half of the patients were assessed within the 1st year and < 15% more than 5 years post-stroke. Second, PCE scores were comparable between subjects with IS and controls. Age, a variable that substantially influences CAC scores (45), was also comparable between the groups. Third, the use of medications to control risk factors was found to be greater in the stroke group than in the control group. This could make the finding of greater CAC scores in the stroke group, compared to controls, less likely. Despite this, we found that the “stroke status” was an independent predictor of CAC >0 and, hence, greater cardiovascular risk. Fourth, multivariate analysis (Model 2), with “PCEwithoutstatinuse” for statin users (estimation of the likely LDL-C level in the absence of statin use), showed the same results compared to Model 1, in which the independent variables were PCE and Groupathero.
The frequency of coronary calcification was higher in subjects with stroke caused by large-artery atherosclerosis than in controls. Stroke caused by large-artery atherosclerosis should be considered a red flag for subclinical coronary atherosclerosis, particularly in subjects with stenoses >50% in cervical and intracranial arteries.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comissão de Ética para Análise de Projetos de Pesquisa—CAPPesq—Hospital das Clínicas/São Paulo University. The patients/participants provided their written informed consent to participate in this study.
AA and AC contributed to the concept, design, analysis, interpretation of data for the article, and drafted the manuscript. RS, MB, CN, EB-S-S, RD, MM, MA, GS, VS, and CO contributed to the acquisition, analysis, and interpretation of data for the work. RS, MB, CL, and GS critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
This research was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP, grant no. 2014/03950-2). RS is a recipient of a scholarship from the Conselho Nacional de Pesquisa e Desenvolvimento Tecnologico (CNPq) grant no. 303734/2018-3. AC is a recipient of a scholarship from the Conselho Nacional de Pesquisa e Desenvolvimento Tecnologico (CNPq) grant no. 303070/2019-6. MB is a recipient of a scholarship from the Conselho Nacional de Pesquisa e Desenvolvimento Tecnologico (CNPq) grant no. 310255/2018-0.
We thank Prof. Marc Chimowitz for his comments and suggestions.
RS has received honoraria related to consulting, research and or speaker activities from: Amgen, Aché, Astra Zeneca, Esperion, Kowa, Merck, Novo-Nordisk, PTC, Pfizer, and Sanofi/Regeneron. MB has received speaker fees from GE healthcare.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1082275/full#supplementary-material
1. Crea F, Liuzzo G. Pathogenesis of acute coronary syndromes. J Am Coll Cardiol. (2013) 61:1–11. doi: 10.1016/j.jacc.2012.07.064
2. Grau AJ, Weimar C, Buggle F, Heinrich A, Goertler M, Neumaier S, et al. Risk factors, outcome, and treatment in subtypes of ischemic stroke. Stroke. (2001) 32:2559–66. doi: 10.1161/hs1101.098524
3. Hart RG, Diener H-C, Coutts SB, Easton JD, Granger CB, O'Donnell MJ, et al. Embolic strokes of undetermined source: the case for a new clinical construct. Lancet. (2014) 13:429–38. doi: 10.1016/S1474-4422(13)70310-7
4. Lange MC, Cabral NL, Moro CH, Longo AL, Goncalves AR, Zetola VF, et al. Incidence and mortality of ischemic stroke subtypes in Joinville, Brazil: a population-based study. Arq Neuropsiquiatr. (2015) 73:648–54. doi: 10.1590/0004-282X20150081
5. Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. (1993) 24:35–41. doi: 10.1161/01.STR.24.1.35
6. Ay H, Benner T, Arsava EM, Furie KL, Singhal AB, Jensen MB, et al. A computerized algorithm for etiologic classification of ischemic stroke: the Causative Classification of Stroke System. Stroke. (2007) 38:2979–84. doi: 10.1161/STROKEAHA.107.490896
7. Sander D, Carolei A, Diehm C, Hennerici MG, Rothwell PM. Challenges to the management of high-risk stroke patients with multiple-site occlusive vascular disease. Cerebrovasc Dis. (2011) 31:315–21. doi: 10.1159/000322603
8. Lackland DT, Elkind MS, D'Agostino R, Dhamoon MS, Goff DC, Higashida RT, et al. Inclusion of stroke in cardiovascular risk prediction instruments: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2012) 43:1998–2027. doi: 10.1161/STR.0b013e31825bcdac
9. Steg PG, Bhatt DL, Wilson PWF, D'Agostino R, Ohman EM, Röther J, et al. One-year cardiovascular event rates in outpatients with atherothrombosis. JAMA. (2007) 297:1197–206. doi: 10.1001/jama.297.11.1197
10. Rokey RRL, Harati Y, Kutka N, Verani MS. Coronary artery disease in patients with cerebrovascular disease: a prospective study. Ann Neurol. (1984) 16:50–3. doi: 10.1002/ana.410160110
11. Chimowitz MI, Poole RM, Starling MR, Schwaiger M, Gross MD. Frequency and severity of asymptomatic coronary disease in patients with different causes of stroke. Stroke. (1997) 28:941–5. doi: 10.1161/01.STR.28.5.941
12. Calvet D, Touze E, Varenne O, Sablayrolles JL, Weber S, Mas JL. Prevalence of asymptomatic coronary artery disease in ischemic stroke patients: the PRECORIS study. Circulation. (2010) 121:1623–9. doi: 10.1161/CIRCULATIONAHA.109.906958
13. Beigneux Y, Sablayrolles JL, Varenne O, Mas JL, Calvet D. Coronary artery calcium score improves the prediction of occult coronary artery stenosis in ischemic stroke patients. J Am Heart Assoc. (2016) 5:e003770. doi: 10.1161/JAHA.116.003770
14. Gill EA, Blaha MJ, Guyton JR. JCL roundtable: coronary artery calcium scoring and other vascular imaging for risk assessment. J Clin Lipidol. (2019) 13:4–14. doi: 10.1016/j.jacl.2019.01.008
15. Yeboah J, McClelland RL, Polonsky TS, Burke GL, Sibley CT, O'Leary D, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate-risk individuals. JAMA. (2012) 308:788–95. doi: 10.1001/jama.2012.9624
16. Yeboah J, Young R, McClelland RL, Delaney JC, Polonsky TS, Dawood FZ, et al. Utility of nontraditional risk markers in atherosclerotic cardiovascular disease risk assessment. J Am Coll Cardiol. (2016) 67:139–47. doi: 10.1016/j.jacc.2015.10.058
17. Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, Grundy SM, et al. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the (2000) Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. (2007) 49:378–402. doi: 10.1016/j.jacc.2006.10.001
18. Pletcher MJ, Tice JA, Pignone M, Browner WS. Using the coronary artery calcium score to predict coronary heart disease events. Arch Intern Med. (2004) 164:1285–92. doi: 10.1001/archinte.164.12.1285
19. Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. (2008) 358:1336–45. doi: 10.1056/NEJMoa072100
20. Miedema MD, Duprez DA, Misialek JR, Blaha MJ, Nasir K, Silverman MG, et al. Use of coronary artery calcium testing to guide aspirin utilization for primary prevention: estimates from the multi-ethnic study of atherosclerosis. Circ Cardiovasc Qual Outcomes. (2014) 7:453–60. doi: 10.1161/CIRCOUTCOMES.113.000690
21. Budoff MJ, Young R, Burke G, Jeffrey Carr J, Detrano RC, Folsom AR, et al. Ten-year association of coronary artery calcium with atherosclerotic cardiovascular disease (ASCVD) events: the multi-ethnic study of atherosclerosis (MESA). Eur Heart J. (2018) 39:2401–8. doi: 10.1093/eurheartj/ehy217
22. Iwasaki K, Haraoka K, Hamaguchi T, Imamura T, Kawada S, Ohno M, et al. Prevalence of subclinical coronary artery disease in ischemic stroke patients. J Cardiol. (2015) 65:71–5. doi: 10.1016/j.jjcc.2014.04.004
23. Choi HY, Shin SJ, Yoo J, Lee K, Song D, Kim YD, et al. Coronary calcium score for the prediction of asymptomatic coronary artery disease in patients with ischemic stroke. Front Neurol. (2020) 11:206. doi: 10.3389/fneur.2020.00206
24. Zheng C, Yan S, Fu F, Zhao C, Guo D, Wang Z, et al. Cervicocephalic spotty calcium for the prediction of coronary atherosclerosis in patients with acute ischemic stroke. Front Neurol. (2021) 12:659156. doi: 10.3389/fneur.2021.659156
25. Goff DC, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB, Gibbons R, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. (2014) 129 (25 Pt B):S49–73. doi: 10.1161/01.cir.0000437741.48606.98
26. Cesena FHY, Laurinavicius AG, Valente VA, Conceicao RD, Santos RD, Bittencourt MS. The expected cardiovascular benefit of plasma cholesterol lowering with or without LDL-C targets in healthy individuals at higher cardiovascular risk. Arq Bras Cardiol. (2017) 108:518–25. doi: 10.5935/abc.20170089
27. Cesena FHY, Laurinavicius AG, Valente VA, Conceicao RD, Santos RD, Bittencourt MS. Cardiovascular risk stratification and statin eligibility based on the Brazilian vs. North American guidelines on blood cholesterol management. Arq Bras Cardiol. (2017) 108:508–17. doi: 10.5935/abc.20170088
28. Brott T, Adams HP, Olinger CP, Marler JR, Barsan WG, Biller J, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. (1989) 20:864–70. doi: 10.1161/01.STR.20.7.864
29. Cincura C, Pontes-Neto OM, Neville IS, Mendes HF, Menezes DF, Mariano DC, et al. Validation of the National Institutes of Health Stroke Scale, modified Rankin Scale and Barthel Index in Brazil: the role of cultural adaptation and structured interviewing. Cerebrovasc Dis. (2009) 27:119–22. doi: 10.1159/000177918
30. Williams LS, Yilmaz EY, Lopez-Yunez AM. Retrospective assessment of initial stroke severity with the NIH stroke scale. Stroke. (2000) 31:858–62. doi: 10.1161/01.STR.31.4.858
31. Benn M, Watts GF, Tybjaerg-Hansen A, Nordestgaard BG. Familial hypercholesterolemia in the Danish general population: prevalence, coronary artery disease, and cholesterol-lowering medication. J Clin Endocrinol Metab. (2012) 97:3956–64. doi: 10.1210/jc.2012-1563
32. Henein M, Granasen G, Wiklund U, Schmermund A, Guerci A, Erbel R, et al. High dose and long-term statin therapy accelerate coronary artery calcification. Int J Cardiol. (2015) 184:581–6. doi: 10.1016/j.ijcard.2015.02.072
33. Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. Recovery of walking function in stroke patients: the Copenhagen Stroke Study. Arch Phys Med Rehabil. (1995) 76:27–32. doi: 10.1016/S0003-9993(95)80038-7
34. Hill K, Ellis P, Bernhardt J, Maggs P, Hull S. Balance and mobility outcomes for stroke patients: a comprehensive audit. Aust J Physiother (1997) 43:173–180. doi: 10.1016/S0004-9514(14)60408-6
35. Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. (2017) 376:1713–22. doi: 10.1056/NEJMoa1615664
36. Ferrari F, Stein R, Motta MT, Moriguchi EH. PCSK9 Inhibitors: Clinical relevance, molecular mechanisms, and safety in clinical practice. Arq Bras Cardiol. (2019) 112:453–60. doi: 10.5935/abc.20190029
37. Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. (2018) 379:2097–107. doi: 10.1056/NEJMoa1801174
38. Suri MF, Johnston SC. Epidemiology of intracranial stenosis. J Neuroimaging. (2009) 1:11S–6. doi: 10.1111/j.1552-6569.2009.00415.x
39. Orimoloye OA, Budoff MJ, Dardari ZA, Mirbolouk M, Uddin SI, Berman DS, et al. Race/ethnicity and the prognostic implications of coronary artery calcium for all-cause and cardiovascular disease mortality: the Coronary Artery Calcium Consortium. J Am Heart Assoc. (2018) 7:e010471. doi: 10.1161/JAHA.118.010471
40. Gunnoo T, Hasan N, Khan MS, Slark J, Bentley P, Sharma P. Quantifying the risk of heart disease following acute ischaemic stroke: a meta-analysis of over 50,000 participants. BMJ Open. (2016) 6:e009535. doi: 10.1136/bmjopen-2015-009535
41. Amarenco P, Lavallée PC, Labreuche J, Ducrocq G, Juliard JM, Feldman L, et al. Prevalence of coronary atherosclerosis in patients with cerebral infarction. Stroke. (2011) 42:22–9. doi: 10.1161/STROKEAHA.110.584086
42. Devarashetty S, Zamora DI, Patel GS, Grossman I, Rodriguez K, Soni M, et al. Coronary artery calcium score – a reliable indicator of coronary artery disease? Cureus. (2021) 13:e20149. doi: 10.7759/cureus.20149
43. Tramontano L, Punzo B, Clemente A, Seitun S, Saba L, Bossone E, et al. Prognostic value of coronary calcium score in asymptomatic individuals: a systematic review. J Clin Med. (2022) 11:5842. doi: 10.3390/jcm11195842
44. Schmidt MI, Duncan BB, Mill JG, Lotufo PA, Chor D, Barreto SM, et al. Cohort profile: longitudinal Study of Adult Health (ELSA-Brasil). Int J Epidemiol. (2015) 44:68–75. doi: 10.1093/ije/dyu027
Keywords: ischemic stroke, coronary calcium score, subclinical coronary artery disease, coronary atherosclerosis, cervicocephalic atherosclerosis
Citation: de Araújo ALV, Santos RD, Bittencourt MS, Dantas RN Jr, Oshiro CA, Nomura CH, Bor-Seng-Shu E, Oliveira MdL, Leite CdC, Martin MdGM, Alves MM, Silva GS, Silva VM and Conforto AB (2023) Ischemic stroke caused by large-artery atherosclerosis: a red flag for subclinical coronary artery disease. Front. Neurol. 14:1082275. doi: 10.3389/fneur.2023.1082275
Received: 28 October 2022; Accepted: 24 February 2023;
Published: 12 April 2023.
Edited by:
Jean-Claude Baron, University of Cambridge, United KingdomReviewed by:
João Pedro Marto, Centro Hospitalar de Lisboa Ocidental, PortugalCopyright © 2023 de Araújo, Santos, Bittencourt, Dantas, Oshiro, Nomura, Bor-Seng-Shu, Oliveira, Leite, Martin, Alves, Silva, Silva and Conforto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adriana Bastos Conforto, YWRyaWFuYS5jb25mb3J0b0BoYy5mbS51c3AuYnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.