 Pasquale Viola1
Pasquale Viola1 Federico Maria Gioacchini2Alessia Astorina1
Federico Maria Gioacchini2Alessia Astorina1 Davide Pisani1
Davide Pisani1 Alfonso Scarpa3*†
Alfonso Scarpa3*† Gianmarco Marcianò4
Gianmarco Marcianò4 Alessandro Casarella4Emanuele Basile4Vincenzo Rania4
Alessandro Casarella4Emanuele Basile4Vincenzo Rania4 Massimo Re2
Massimo Re2 Giuseppe Chiarella1
Giuseppe Chiarella1- 1Unit of Audiology, Department of Experimental and Clinical Medicine, Regional Centre of Cochlear Implants and ENT Diseases, Magna Graecia University, Catanzaro, Italy
- 2ENT Unit, Department of Clinical and Molecular Sciences, Polytechnic University of Marche, Ancona, Italy
- 3Department of Medicine and Surgery, University of Salerno, Salerno, Italy
- 4Department of Health Science, School of Medicine, University “Magna Graecia” of Catanzaro, Catanzaro, Italy
Acute vestibular syndrome (AVS) represents a clinical picture that involves urgent management due to the important procession of symptoms accompanying the event, which can be positively or negatively influenced by therapeutic choices and intervention timing. This forces a differential diagnosis and therapeutic choices to be made in conditions that are not always favorable and often not in the specialist field. In this work, we will examine in detail the pharmacological therapeutic possibilities, correlating them to the differential and, as far as possible, to the etiological diagnosis. In particular, the pharmacological possibilities for the two main conditions we can face will be investigated, namely, vestibular neuritis and posterior circulation stroke.
Introduction
Vertigo and/or dizziness are frequently reported in patients admitted to the emergency department (ED), accounting for nearly 4% of admissions (1). There is a wide spectrum of causes including cardiovascular, neurological, vestibular, and systemic disorders (2). It has been observed that 10–20% of the patients admitted to ED due to persistent vertigo and dizziness have an acute vestibular syndrome (AVS) (3). AVS is defined as the sudden onset of acute, “continuous” vertigo (lasting longer than 24 h), associated with nausea, vomiting and head motion intolerance, gait instability, and nystagmus (ny). It results from a unilateral vestibular lesion that causes a sudden asymmetry of the neuronal nuclei firing rate and is largely associated with severe anxiety and vasovagal responses (2). The main causes of AVS are vestibular neuritis (VN), which nearly counts for 70% of cases, and posterior circulation stroke (PCS), accounting for 25% of diagnoses (1, 4). Discrimination between these pathologies is necessary for correct patient management, but despite a large investment of resources, PCS still too often escapes diagnosis and is sometimes missed (5). Approximately 10–20% of spontaneous AVS are due to stroke in the brainstem or cerebellum, nevertheless fewer than 20% present with focal neurological signs (6, 7). VN is the third most common, peripheral vestibular disorder, after benign positional paroxysmal vertigo (BPPV) and Meniere's disease (MD). The leading hypothesis involves reactivation of a latent neurotropic virus, for example, herpes simplex virus (HSV) types 1 and 2, and herpes zoster virus (HZV). VN has recently been related to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection, but this association is still uncertain and definitive evidence is lacking (8–10). Other supposed etiologies include vascular, immunologic, and inflammatory (11, 12). Stroke affects the brain circle, resulting in the death of neurons, according to oxygen and nutrients deprivation (13). Ischemic stroke is more likely to determine AVS, compared to hemorrhagic stroke. The stroke involves more frequently posterior inferior cerebellar artery (PICA) than anterior inferior cerebellar artery (AICA) (14). Some patients with AVS can show focal lesions in the nodulus of the cerebellum, in the cerebellar peduncles, in the dorsolateral pons, in the lateral medulla, in the root of the eighth cranial nerve at the pontomedullary junction, or in the vestibular nuclei (15–19). Other possible causes of AVS are MD, multiple sclerosis, thiamine deficiency, BPPV, and vestibular migraine. Multiple sclerosis is an uncommon and infrequent cause of acute vertigo (4%). Demyelinating plaques can be located in and around the eighth nerve fascicle or vestibular nuclei but also in the brainstem and cerebellar peduncles. Considering that demyelinating lesions during an acute attack may not be evident on MRI, clinical examination in AVS is essential. In these patients, more evident oculomotor signs are often present (limitation of ocular motility or vertical nystagmus) (20).
Thiamine deficiency underlying Wernicke encephalopathy (WE) should be considered in patients with nutritional deprivation and unexplained acute or subacute vestibular symptoms, even absent encephalopathy. The complete WE triad includes ophthalmoplegia, ataxia, and encephalopathy. In about 90% of cases, there is altered mental status and nystagmus with central features. Nystagmus was the only ocular feature in 65% of cases. The most common human vestibular finding in WE is bilateral vestibular hypofunction, occurring in about 90% of cases. In the pre-encephalopathy phase, thiamine-deficient patients presenting with predominantly vestibular symptoms and signs can mimic vestibular neuritis or stroke with acute, persistent, vertigo, severe vomiting, and gait ataxia for 48 h. MRI of the brain in the pre-encephalopathy phase may be normal. Subsequently, it can present alterations consistent with WE such as areas of increased fluid-attenuated inversion recovery/T2 signal in the midline thalami, upper midbrain, and pons. Vestibulopathy in WE disease is due to direct bilateral damage of brainstem most likely in the dorsal medulla and pons in the region of the medial vestibular nuclei and nucleus prepositus hypoglossi in the medulla. The therapy involves the administration of vitamin B1 which in most cases determines an improvement in the patient's condition (21, 22). However, these clinical entities are less frequent than VN and stroke in AVS-like presentation and should be held in account when other causes are not identified (5).
Differential diagnosis
Correctly distinguishing between VN and PCS is essential although it is not always easy, due to the possible similar clinical presentation. Hemiparesis, headache, diplopia, dysarthria, and ataxia are neurological deficits that may be signs of PCS; however, they are not present in all patients (2, 23). In stroke suspicion, anamnesis has a key role. Smoke, diabetes mellitus, hypertension, hypercholesterolemia, diet, physical activity, and cardiovascular disease are important clues (24). VN ny is generally horizontal, maintains the same direction after changing gaze side, and is attenuated by visual fixation. Conversely, ny of central origin is multidirectional, and its intensity is less affected by visual fixation. Although horizontal mixed torsional ny is possible in both central and peripheral pathologies, vertical or pure torsional ny is suggestive of a central origin. Negative clinical head impulse test (HIT), direction changing ny, and skew deviation (HINTS) are suggestive of central origin. HINTS test is highly sensitive and specific in detecting vestibular strokes, and it outperforms acute magnetic resonance imaging (MRI) within 48 h from symptoms onset (6, 25). MRI diagnosis of smaller strokes (<1 cm) indeed can fail up to 50% of the cases within the first 24 h (26). ABCD2 score is also useful to quantify the risk of stroke, evaluating age, blood pressure, clinical features, duration, and diabetes in subjects (27). In the acute setting, computed tomography (CT) is more useful to evaluate a patient with suspected stroke, because it is quicker and easily available. MRI is more sensible in detecting early signs of ischemia. Brain imaging is essential in patients with suspected PCS and who may need thrombolysis or thrombectomy. These choices should be made based on risk factors, signs, and symptoms (2, 23). MRI has been shown to be effective in detecting signs of recent PCS onset, and it, therefore, allows patients to be referred for thrombolysis within the time interval suggested by the guidelines (28, 29). The symptoms and signs in patients with an AVS associated with a stroke commonly evolve over hours and often require frequent monitoring. In patients with the AVS, the finding of ocular lateral deviation (OLD), although infrequent (8.4%), usually reflects lateral medullary syndrome (LMS), particularly when associated with hypometric corrective saccades on opening the eyes. OLD is a conjugate, ipsilesional, horizontal ocular deviation associated with brief (3–5 s) closing of the eyes that is highly specific for a central disturbance. OLD is easily tested at the bedside and can be a quick confirmatory sign when patients have a HINTS pattern of eye movements suggesting a central cause, particularly when initial imaging is negative. To maintain specificity, a complete horizontal deviation must be present after a brief period (3–5 s) of simply closing the eyes. Clinicians should look for OLD with brief, gentle eyelid closure and for a series of hypometric, corrective saccades back to straight ahead on opening the eyes. Both findings point to a central lesion that usually is in the lateral medulla on the same side as the OLD (30).
Also, the “STANDING” appears to show high sensitivity and specificity to detect central vestibulopathy, with good reliability in the emergency setting, and seems to be associated with a reduction of neuroimaging burden and hospital admission rates. STANDING is an acronym for the four-step clinical algorithm based on ny observation, and diagnostic maneuvers (Dix-Hallpike and Pagnini-McClure positionings) include the discrimination between SponTAneous and positional nystagmus, the evaluation of the Nystagmus Direction, the head Impulse test, and the evaluation of equilibrium (staNdinG) (31).
Larger cerebellar strokes (usually PICA, or less commonly SCA territory) with only vestibular and ocular motor signs need close monitoring in the intensive care unit for the development of malignant ischemic edema, which may be delayed at times for several days. Treatment may require hypertonic saline or different surgical interventions (external ventricular drain) or resection of necrotic tissue with good post outcome. Videonystagmography, electronystagmography, and/or vestibular evoked myogenic potentials (VEMPs) are useful to better qualify and quantify vestibular deficit (26).
Pharmacological treatment
Vestibular neuritis
The VN pharmacological management is aimed to reduce symptoms and inflammation in the acute phase. In fact, most people undergo complete resolution, but imbalance may last for weeks (11, 32, 33). Vestibular suppressants and antiemetics are useful for short intervals of time. If their administration is prolonged, they may obstacle VC (11, 26). In the acute setting, intravenous dimenhydrinate showed a major efficacy compared to intravenous lorazepam, in a randomized clinical trial by Marill and colleagues, in 74 patients (34). Antihistamines, benzodiazepines, anticholinergics, and dopamine receptor antagonists are possible therapeutic options in the first 2–3 days (33, 35). Corticosteroids use in VN is a controversial topic (36). Fishman et al. showed the absence of a long-term effect on symptoms. These compounds had a significant effect only on 1-month-performed caloric test (37). Other authors confirmed these results (38, 39). However, their use is a matter of fact and may provide symptoms relief in patients in the first 72 h (11, 26). Goudakos et al. experimental results sustain an earlier corticosteroids efficacy. However, the study was single blinded and had limitations (39). Vestibular rehabilitation has an important role in patient with long-term symptoms and seems to be comparable to corticosteroids in the main early outcomes (11, 33, 39). Nutraceuticals, including Ginkgo biloba, Salvia officinalis, Melissa officinalis, and Zingiber officinalis, may improve patient's conditions with a low amount of side effects (12). We previously treated these drugs' mechanism of actions, interactions, and side effects in a narrative review (35). Further details are summarized in Tables 1–3.
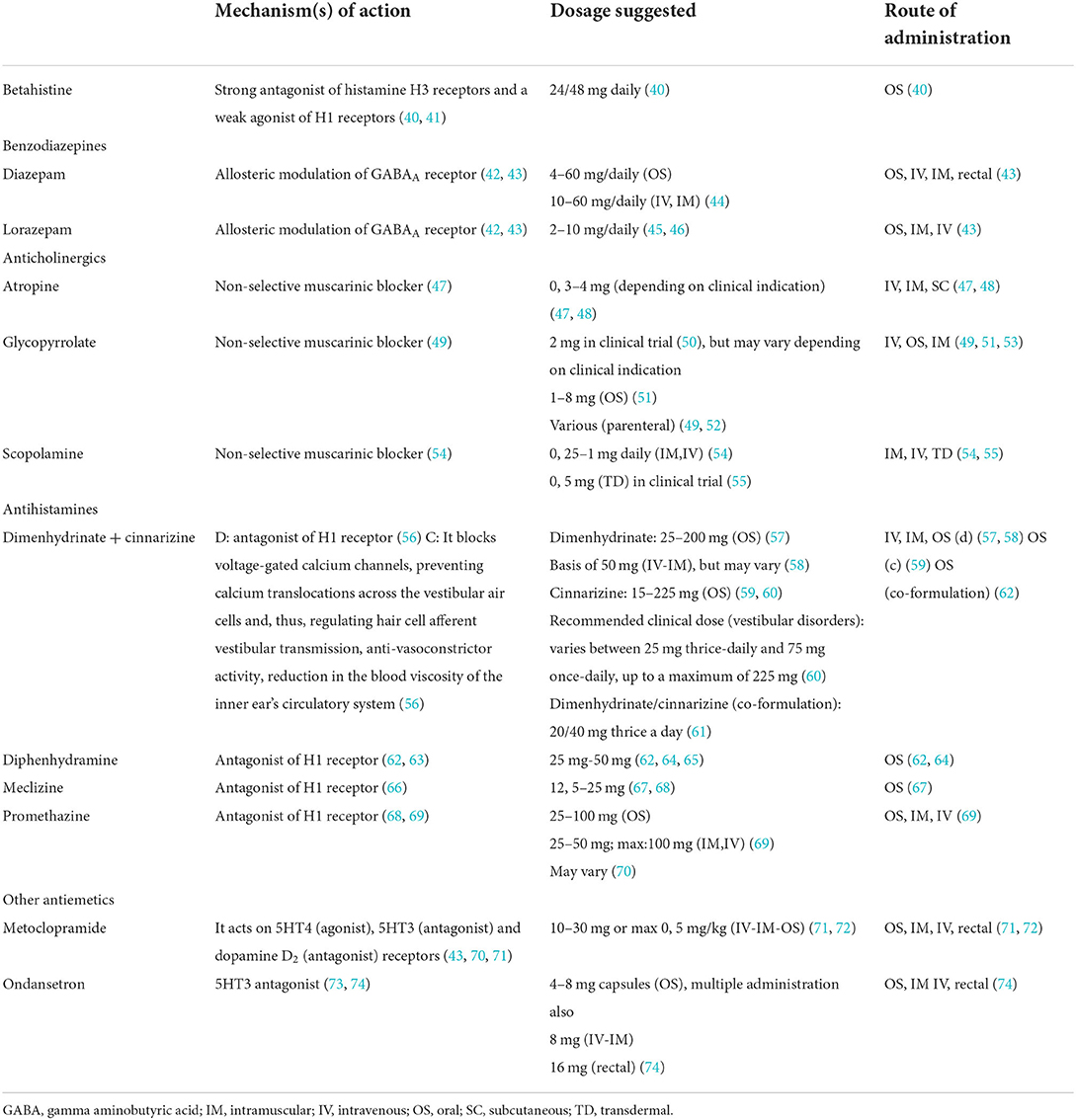
Table 1. Mechanism of action and dosage of vestibular neuritis drugs.
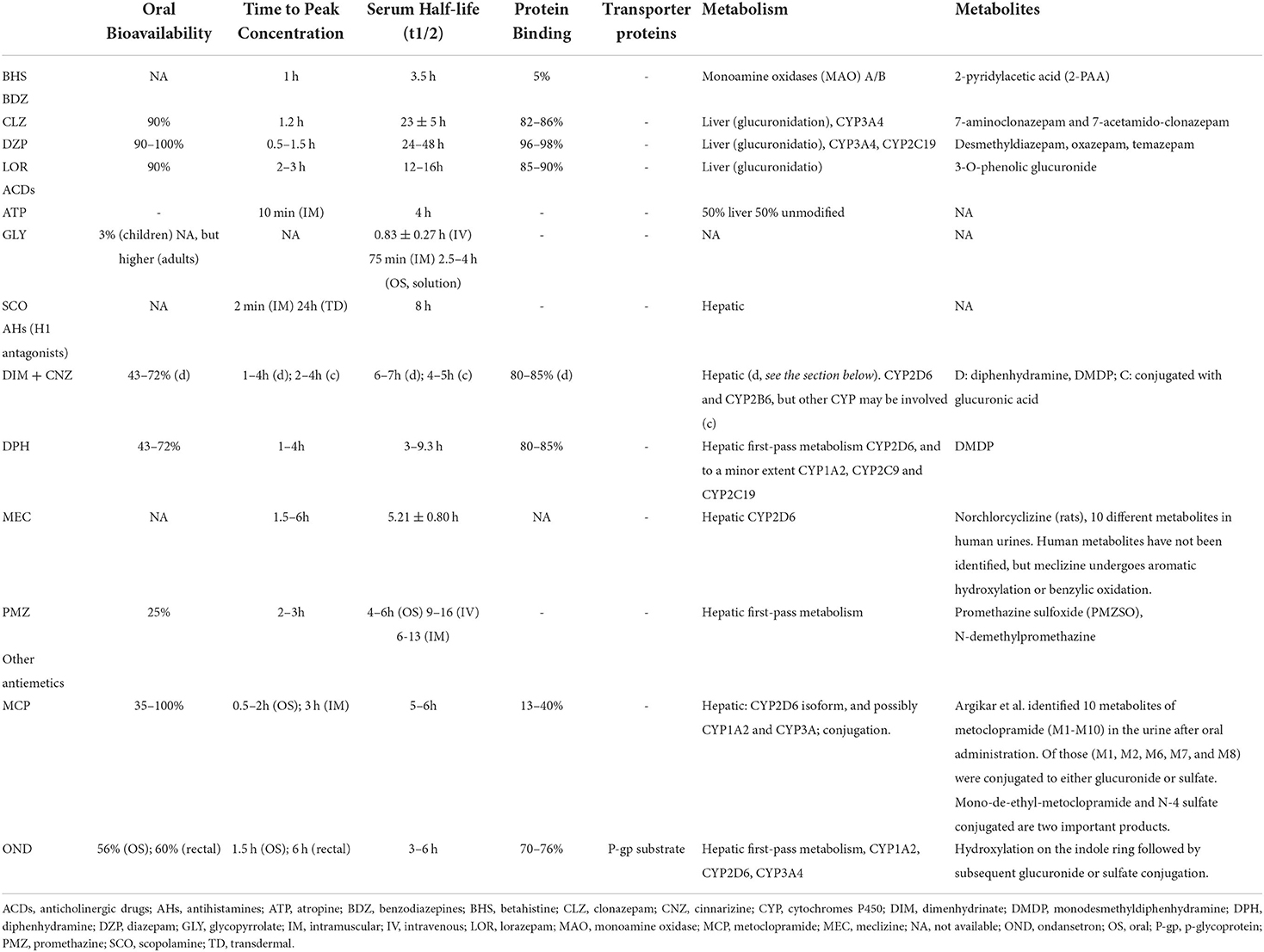
Table 2. Pharmacokinetics of drugs used in peripheral vestibular vertigo (part I).
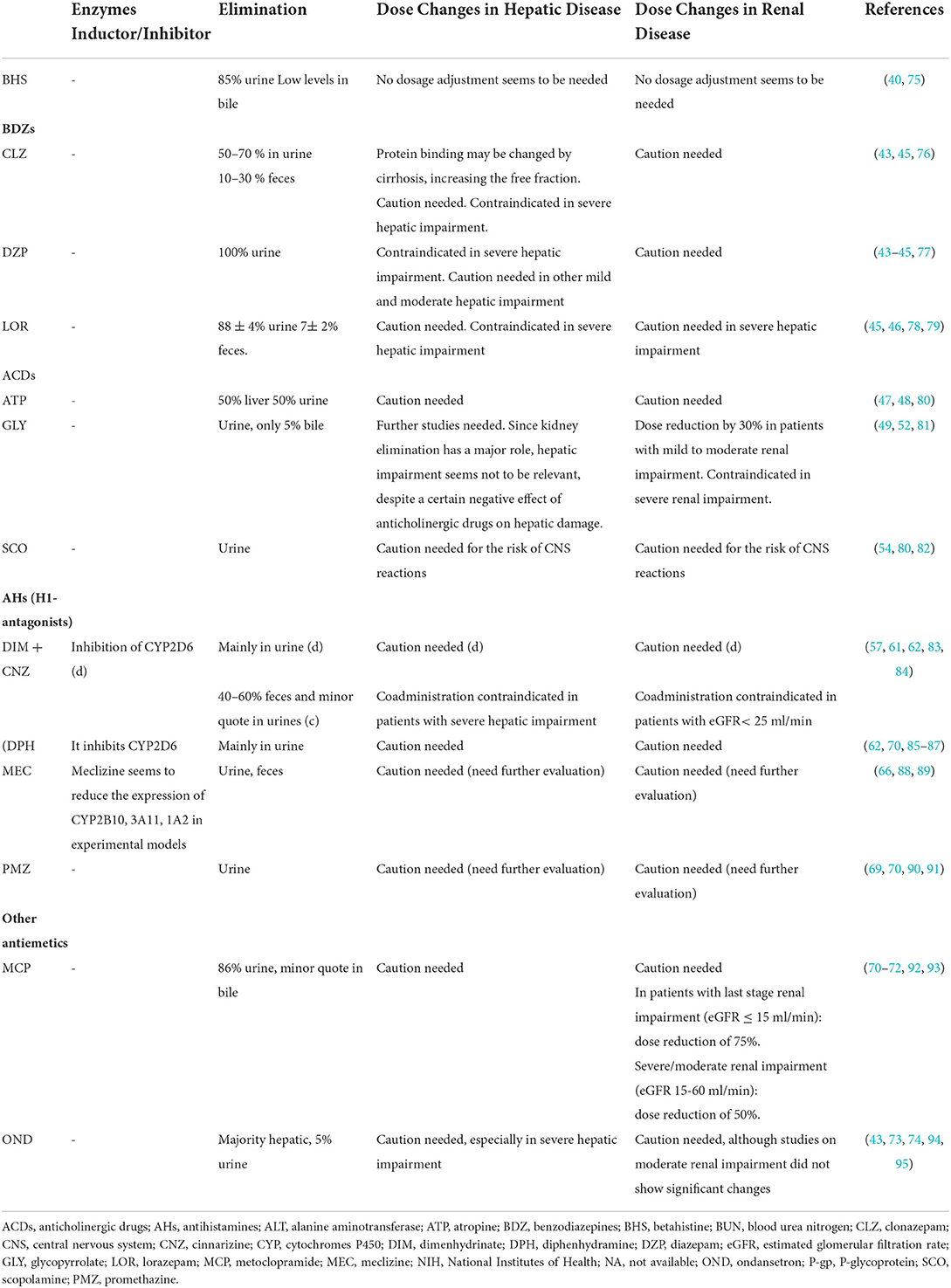
Table 3. Pharmacokinetics of drugs used in peripheral vestibular vertigo (part II).
Posterior circulation stroke
Tissue plasminogen activators
Alteplase and tenecteplase are tissue plasminogen activators. Their main activity consists in the conversion of plasminogen to plasmin: this action is responsible for fibrinolysis (96, 97). Alteplase IV administration (in patients ≥ 18 years: 0.9 mg/kg, maximum dose 90 mg over 60 min; in the beginning, 10% of dose must be given as a bolus over 1 min) is recommended until 4.5 h after stroke onset. Treatment should be started as soon as possible. In severe stroke, after 3–4.5 h from symptoms onset, some categories of patients must be excluded (or have a lower evidence indication) for the high risk of hemorrhage: patients >80 years; combined history of diabetes–stroke; warfarin assumption, without considering international normalized ratio (INR); and very severe stroke with National Institutes of Health Stroke Scale (NIHSS) > 25 (29, 98). Alteplase is recommended for patients with mild stroke and mild disabling symptoms (NIHSS 0–4/5) until 3 h, and may be a therapeutic option in the same category, in a 3–4.5 h interval. A weaker indication is present (3–4.5 h interval) for patients > 80 years, with severe stroke (NIHSS > 25) and diabetes–stroke history. However, the use in these categories may be effective (29).
Important contraindications are represented by severe hemorrhages/risk of bleeding (e.g., intracerebral hemorrhage; head trauma; coagulopathy; use of anticoagulants or antiaggregant medications; and low platelets count), glycemia <50 or >400 mg/dl, systolic blood pressure > 185 mmHg, or diastolic blood pressure >110 mmHg. Nevertheless, the concomitant administration of anticoagulant or antiaggregant drugs may not be contraindicated if patients take it for solid clinical reasons (29, 96). Besides, its possible interaction with drugs acting on coagulation/aggregation (e.g., direct oral anticoagulants, aspirin, and coumarols), angiotensin-converting enzyme (ACE) inhibitors, may increase the risk of hypersensitivity generated by alteplase (96). Angioedema is a possible, but less common, alteplase side effect. It is probably related to the increase of bradykinin by plasmin activation. Therefore, the coadministration of ACE inhibitors may result in a worsening of macroglossia and angioedema (99). Tenecteplase is a modified alteplase analog. It has a longer half-life, a more specific action on fibrin, and a minor susceptibility to inhibitors (100). In EXTEND-IA TNK trial, tenecteplase (0.25 mg/kg, higher total dose 25 mg) was associated with a better reperfusion, compared to alteplase, in stroke patients until 4.5 h (100). However, tenecteplase (0.4 mg/kg, higher total dose 40 mg) failed to demonstrate superiority with a similar safety profile in a mild stroke prevalent court (101). These results induce guidelines for a lower strength (and maybe temporary) recommendation (IIb) for patients eligible for mechanical thrombectomy and as an alternative in mild stroke (no severe deficits or occlusions). However, in a mild stroke court, Tenecteplase showed to be equal to alteplase (and then it can be used as an alternative). In a tougher clinical context (occlusion of MCA, basilar, carotid), tenecteplase has shown superiority, and these findings will be the object of further studies to maintain or change the indication (29, 100, 101). Tenecteplase has similar adverse events and contraindications compared to alteplase (97). No other tissue plasminogen activators are approved by guidelines (29) (see Tables 4, 5 for details). In patients with an uncertain time of onset, performing a diffusion-weighted MRI (DW-MRI) and fluid-attenuated inversion recovery (FLAIR) sequences is useful: no signal in FLAIR and DW-MRI lesion minor than one-third of middle cerebral artery (MCA) is eligible for fibrinolysis.
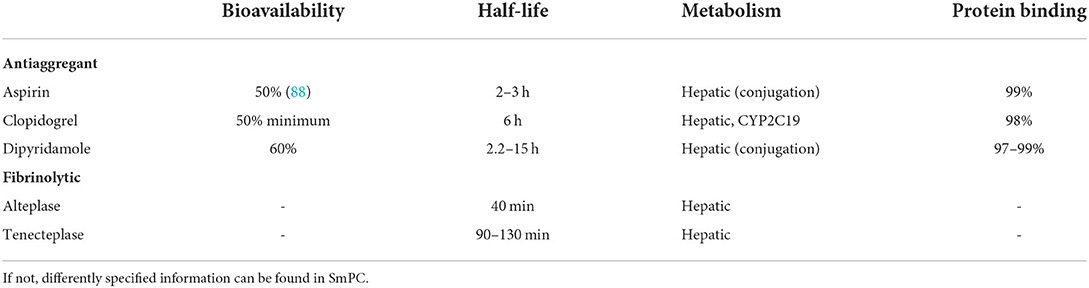
Table 4. Antiaggregant or fibrinolytic drugs (part I).
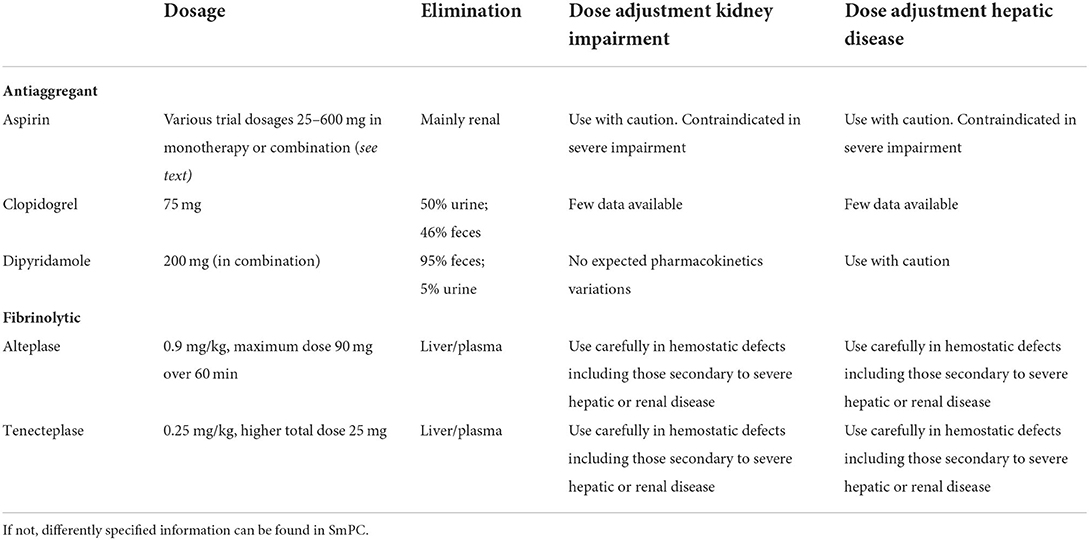
Table 5. Antiaggregant or fibrinolytic drugs (part II).
Antiplatelet treatment
Acetylsalicylic acid
Acetylsalicylic acid (ASA; also aspirin) exerts its antiplatelet activity by inhibiting cyclooxygenase 1 (COX-1) and depressing thromboxane synthesis (102–104). Aspirin is recommended in stroke patients 24–48 h after onset. In the case of alteplase administration, aspirin is delayed 24 h unless there are other clinical indications or benefits: in this case, it might be useful (29). Hemorrhagic risk should be evaluated carefully, especially in patients who consume multiple medications (29, 104). A systematic review by Sandercock et al. assessed that aspirin 160–300 mg OD (oral) significantly decreased death and complications (except hemorrhage, whose risk was low compared to benefits) (105). Combination therapy of clopidogrel and aspirin shows effectiveness in patients with non-cardioembolic ischemic stroke and NIHSS ≤ 3, not receiving alteplase (beginning in 24 h and continuing for 21 days) (29). The dosage was different in the two main trials. POINT trial randomized patients to a clopidogrel loading dose of 600 mg, followed by clopidogrel 75 mg/day, plus aspirin 50–325 mg/day, for 90 days, compared to aspirin alone. The results showed real effectiveness, but an increase in hemorrhagic risk. There was no benefit in stroke reduction risk after 30 days of treatment, whereas bleeding probability was enhanced after 7 days of treatment (101). A different dose (clopidogrel loading dose 300 mg, and then 75 mg/day, for 90 days, and aspirin 75 mg/day, for the first 21 days) was administered in the CHANCE trial, in comparison with aspirin. This therapeutic scheme generated similar percentages of hemorrhage (0.3%) in the two groups, increasing efficacy. Maybe these results are related to a smaller loading dose or limited duration of dual therapy (106, 107). Furthermore, CYP2C19 Asian polymorphisms may have a role in the development of adverse events, since clopidogrel may be variously transformed in its active metabolite, depending on ultrarapid/slow metabolism (106, 108). In a study by Khatri et al., alteplase was compared to aspirin in people with ischemic stroke, but minor disabling deficits (NIHSS 0-5). Aspirin was superior, despite some study limitations, according to guidelines recommendation. However, the results were not conclusive according to the trial brief duration (109). ASA may be used also in primary (risk factor management) and secondary prevention (50–325 mg daily) (29, 110, 111). ASA is not relevantly metabolized by cytochrome 450 (CYP450) enzymes, and it is not a substrate of transporters. It may compete with other non-steroidal anti-inflammatory drugs (NSAIDs) that also act on COX-1, lowering the ASA effect (112).
Interaction with selective serotonin reuptake inhibitors (SSRI) is also important. These antidepressant drugs reduce the platelet reuptake of serotonin, inhibiting aggregation. Therefore, increased hemorrhagic risk may result from coadministration (104, 112, 113). Another important interaction in this clinical setting involves antihypertensive drugs. In fact, NSAID may suppress renin activity, increase sodium retention, impair the activity of kidney prostaglandins (114), increase the risk of kidney injury, and impair diuretics activity (115). However, other authors suggest that low-dose aspirin does not have an important interaction with kidney and antihypertensive drugs. In fact, COX-2 is principally involved in the production of kidney prostaglandins 2, and aspirin acts on COX-1 (112) (see Tables 4, 5 for details).
Clopidogrel
Clopidogrel is an antiplatelet agent, which acts as a prodrug. The active compound is generated by CYP450 metabolism, and then, it blocks P2Y12 platelet receptor. Through this pharmacodynamic action, it prevents the binding of adenosine diphosphate (ADP) to the same target (116, 117). Activation of P2Y12 in physiological conditions leads to the activation of a pathway that determines the release of granules, a stronger platelet aggregation, and the activation of the glycoprotein IIb/IIIa receptor (GP IIb/IIIa) (118). Clopidogrel (75 mg) may be used in non-cardioembolic stroke or transient ischemic stroke (TIA) as secondary prevention for patients with risk factors. Antiplatelet treatment is strongly recommended by guidelines (10, 29). In this setting, aspirin (50–325 mg) alone, clopidogrel (75 mg) alone, and aspirin (25 mg) + dipyridamole (200 mg) are the main options. In non-cardioembolic stroke patients with NIHSS ≤ 3 or high-risk TIA (ABCD2 score ≥4), double antiplatelet therapy (DAPT) with aspirin plus clopidogrel in 12–24 h from clinical insurgence is the right option (if alteplase has not been administered). This therapy should be maintained up to 21–90 days, then switching to single antiplatelet therapy: a longer treatment period would result in increased bleeding risk without benefit (29, 111). Clopidogrel is mainly transformed by CYP2C19 that produces its active metabolite (R-130964), a thiol derivative. CYP1A2, 2B6, and 3A4 have a certain role in this process (116). Therefore, inhibition (e.g., some proton pump inhibitors [PPI], some SSRI, and some antifungal medication resulting in reduction of active metabolite production) or induction (rifampicin) of CYP2C19 may alter therapeutic action (116, 118). Bleeding or side effects related to reduced platelet action are the most common side effects (116, 119) (see Tables 4, 5 for details).
Antiplatelet combination therapy and other options
The ASA was tested in clinical trials in coadministration with dipyridamole. Dipyridamole has both, vasodilator and antiplatelet effects. This drug inhibits adenosine reuptake from red blood cell precursors and inhibits cyclic-3'5'-adenosine monophosphate (cAMP) phosphodiesterase. Therefore, cAMP accumulates and exerts an antiaggregant activity. Vasodilator effect is generated by cyclic-3'5'-guanosine monophosphate (cGMP) phosphodiesterase inhibition by dipyridamole. It results in an increase of cGMP and of its action on blood vessels (120). Some trials observed a better efficacy of aspirin plus dipyridamole compared to ASA alone in stroke secondary prevention (121). Clopidogrel plus ASA showed a better efficacy compared to ASA plus dipyridamole as antiaggregant therapy (122). However, ASA + clopidogrel DAPT has very specific indications, and dipyridamole + ASA is considered a good therapeutic option (111). Triple therapy (ASA + clopidogrel + dipyridamole) has been revealed to be dangerous, without any benefit, and it is contraindicated by guidelines (29, 122). An important statement is that, in case of cardiac disease/embolic origin of stroke, anticoagulants (direct anticoagulants or warfarin, varying in different indications) have a major role in secondary prevention (especially in atrial fibrillation). Nevertheless, antiplatelet agents may be used alone or in combination with anticoagulants, depending on etiology (111). Glycoprotein IIb/IIIa inhibitors are not useful in this pathology. Tirofiban and eptifibatide efficacy have not been observed, and abciximab administration may even be dangerous, especially when associated with alteplase (29). A systematic review by Ciccone et al. showed an increase of hemorrhagic risk without benefit in terms of clinical effectiveness. However, the majority of the studies included regarded abciximab. Although its dosage and specific indications have not been described, tirofiban showed an interesting potential in stroke (123, 124). Nevertheless, other authors denied eptifibatide and tirofiban safety and effectiveness. Guidelines used a IIb recommendation on tirofiban and eptifibatide, assessing the need of further trials and analysis (29, 125). Ticagrelor, a P2Y12 antagonist, has an uncertain role in stroke secondary prevention. Guidelines talk about a IIb recommendation, according to THALES trial. In fact, ticagrelor plus aspirin showed a better outcome of death stroke, compared to aspirin alone. The study included patients with a mild to moderate pathology assessment (NIHSS ≤ 5) or TIA. The risk of hemorrhage was increased with ticagrelor (111, 126). Ticagrelor alone was inferior to aspirin in SOCRATES trial in the management of minor acute stroke, with comparable safety outcomes (127) (see Tables 4, 5 for details).
Discussion
The AVS represents a dramatic clinical situation causing an important feeling of fear in the patients who experience this event. A rapid and correct diagnosis must be the main goal when evaluating a patient with AVS. In fact, a wrong or delayed diagnosis does not allow to formulate an effective treatment plan and may cause devastating consequences for the patient's health. The initial phase of AVS is mainly managed by general practitioner and emergency room doctors. Patient's complained symptoms show a wide variability, including vertigo, vomiting/nausea, dizziness, headache, confusion, hearing alteration, and neurological deficits. This makes difficult to achieve a correct diagnosis with a basic clinical evaluation, making it necessary to perform specialistic instrumental evaluation and/or imaging investigation. As mentioned above, CT and MRI represent two fundamental radiological aids that allow to detect the eventual signs of ischemia or hemorrhage. According to recent studies, VN occurs more frequently in people over the age of 70 years (128, 129). Its exact etiology still remains unclear. Regarding viral infection of the vestibular nerve, it is considered that viruses causing infections of the upper respiratory tract, such as influenza virus, adenovirus, HSV, cytomegalovirus, Epstein-Barr virus, parainfluenza virus, and, recently, SARS-CoV-2, could be VN related, because associations with preceding or concurrent viral infection in the upper respiratory tract occur in 43% to 46% (130). Among them, HSV type 1 is the most common cause of viral infection of the vestibular nerve and ganglion. Recently, in vivo work demonstrated that HSV infection can induce VN and sudden deafness in a mouse model (131). Immunological mechanisms have also been suggested as possible causes of VN. A pathological CD4/CD8 quotient, which appears in 48% of NV cases, further supports a causal immunological origin (11). The characteristic clinical features of VN are abrupt true-whirling vertigo, lasting for more than 24 h, with nausea and vomiting, in middle age without cochlear symptoms and other neurological symptoms and signs. Prodromal dizziness lasting few minutes, in the few days just before the full onset of symptoms, may precede prolonged spontaneous vertigo in about 25% of patients (132). Unlike BPPV and MD, the clinical features of VN can make this pathological entity resemble PCS. In fact, during BPPV the vertigo is caused by head movement, and exacerbations of MD typically present specific audiological symptoms associated with vertigo (133–135). For these reasons, VN must be considered as the main pathological condition that may mimic a CNS ischemic stroke. Various treatments have been reported for VN, which can be largely divided into symptomatic therapy, specific drug therapy, and vestibular rehabilitation. Vestibular suppressants are widely used because they are effective against dizziness, nausea, and vomiting. During the acute stage of VN, an intramuscular or intravenous route for vestibular suppressants and antiemetics is usually preferable because of severe nausea and decreased gastric motility. However, most vestibular suppressants can have sedative effects, so they should not be used when patients are engaged in activities that require a high level of alertness, such as driving, operating machinery, or participating in athletic activities. Regarding specific drug therapy, steroid therapy has been reported to relieve dizziness and promote VC in VN. Methylprednisolone is much more effective than placebo in reducing vertiginous symptoms in patients with acute vestibular vertigo, and early treatment of acute VN with high doses of glucocorticoids accelerates and improves the recovery of vestibular function (136). Nevertheless, a recent meta-analysis by Leong et al. concluded that corticosteroids appear to have short-term benefits in canal paresis but no long-term benefits in canal paresis and symptomatic recovery (137). Concerning VN long-term treatment, the gold standard for therapy is represented by vestibular rehabilitation. Its targets are to improve vertigo, gaze stability, postural stability, and daily living activities through VC and central neuroplasticity. Vestibular rehabilitation consists of a dynamic compensation of vestibular reflexes that are activated by movement, and it is composed of adaptation, habituation, and substitution. Vestibular rehabilitation exercises are safe, highly therapeutic, highly cost-effective, and significantly hasten vestibulospinal compensation in patients with VN (138–140). Balance and gait exercises significantly reduce the time required for vestibulospinal compensation. Voluntary eye movements, active head movements, goal-directed movements, and walking should be encouraged to restore postural control and balance as soon as possible. Patients with VN should exercise for at least 30 min, 3 times a day (132). An interesting therapeutic opportunity is also offered by nutraceuticals, especially in the intercritical phases of the disease or in the recovery of residual imbalance in some subjects. These are safe and effective compounds that can be administered without associated drugs or in combination to decrease their dosage (12, 141). The prognosis in patients with VN is generally good, but residual dizziness may remain in some patients after the acute phase, similar to persistent disabling imbalance after successful repositioning maneuvers for BPPV. This can be due to many factors, including inadequate central compensation, incomplete peripheral recovery, and psychophysiological and psychological characteristics. The decreasing postural control can affect the quality of life, contributing to falls and psychological problems (142). In contrast, approximately 20% of ischemic events involve tissue supplied by the posterior circulation territory, such as the cerebellum and brainstem. The incidence of cerebellar infarction in larger series of patients with stroke is approximately 1.5 %, with an average patient age of about 60 years (143). Tissue plasminogen activators and antiplatelet treatment represent the two principal categories of drugs for the prompt treatment of cerebral ischemic stroke. Regarding AVS, the main clinical goal is to obtain a fast and correct differential diagnosis between VN and cerebellar stroke. Indeed, the best therapeutic effects can be greatly reduced when stroke treatment is administered late. For this reason, when evaluating a patient with AVS, the crucial question is to clarify the correct etiology of the symptoms. Dizziness/vertigo is a common symptom in patients with isolated strokes of the cerebellum, usually with other neurological symptoms and signs. However, the diagnosis of isolated vertigo from brainstem and cerebellar stroke has increased markedly with recent developments in clinical neurotology and neuroimaging. Patients with infarction in the AICA territory may have isolated recurrent vertigo, acute hearing loss, and/or tinnitus as the initial symptoms (144). This particular clinical entity is also well defined as “labyrinthine infarction.” The acute hearing loss is usually caused by the thrombotic narrowing of the AICA or the basilar artery at the orifice of the AICA. Through this mechanism, decreased blood flow in the affected AICA might cause either a transient episode of selective ischemia to the inner ear, resulting in isolated prodromal vertigo, or permanent damage to the widespread areas involving the middle cerebellar peduncle, lateral pons, and anterior cerebellum, resulting in acute hearing loss and prolonged vertigo in addition to other central symptoms and signs (145). The apical region of the cochlea is particularly vulnerable to vascular damage and, therefore, low-frequency hearing loss is common in inner ear ischemia (146). To date, at least eight subgroups of AICA infarction have been identified, according to the pattern of neurotological presentations, among which the most common pattern of audiovestibular dysfunction is the combined loss of auditory and vestibular functions (147). Ischemia of the PICA usually produces no auditory symptoms, because it does not perfuse the auditory tract, generally. However, PICA infarction may rarely be associated with acute hearing loss as the internal auditory artery sometimes originates from the PICA or directly from the basilar artery (148). For a proper management, in all cases of AVS, it is very important to know when a patient needs an urgent brain scan, and what role does neuroimaging play in diagnosis. Because central signs, such as spontaneous vertical ny, direction-changing gaze-evoked ny, perverted head shaking ny, or severe postural instability with falling, are known to have high specificity, but low sensitivity, for detecting a central cause of vertigo, isolated acute vertigo due to cerebellar infarction at the bedside remains a diagnostic challenge. The cerebellum plays an important role in maintaining body posture, regulating the muscle tension associated with postural movements, and coordinating voluntary movements (149). The vermis is involved in the coordination of eye and body movements, provides visual and auditory input related to balance, and is involved in vestibular system regulation and in maintaining the position of the head (150). Unfortunately, pharmacotherapy and conventional rehabilitation treatments, including core strength exercises, visual feedback training, neurodevelopmental therapy, and proprioceptive neuromuscular facilitation, performed unsatisfactory results on balance recovery among stroke patients (151).
Conclusion
The therapeutic approach to AVS conditioned by the ability to make a correct differential diagnosis and as certain as possible from an etiological point of view. While we have sufficient tools to identify the location and mechanism of the damage, it is not always possible to have immediate evidence of the etiology. This can affect the accuracy of the therapeutic choice by forcing less specific therapies from a causal point of view. Furthermore, the correct pharmacological action lays the foundations for obtaining an effective VC. At the same time, another determining element, directly linked to the therapeutic choice, is the time factor. In fact, the precocity of intervention can guarantee, in general, better outcomes and, in some specific cases, can avoid the evolution toward much more critical clinical pictures and, in a significant percentage, toward non-compensation or transformations into persistent dizziness (152).
Author contributions
PV, FG, and GM: conceptualization, methodology, investigation, data analysis, visualization, and writing—original draft. AA, DP, and AS: investigation and data analysis. AC, EB, and VR: investigation, data analysis, and project administration. MR and GC: investigation, visualization, and software. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Newman-Toker DE, Hsieh YH, Camargo CA Jr, Pelletier AJ, Butchy GT, Edlow JA. Spectrum of dizziness visits to US emergency departments: cross-sectional analysis from a nationally representative sample. Mayo Clin Proc. (2008) 83:765–75. doi: 10.4065/83.7.765
2. Hotson JR, Baloh RW. Acute vestibular syndrome. N Engl J Med. (1998) 339:680–5. doi: 10.1056/NEJM199809033391007
3. Tarnutzer AA, Berkowitz AL, Robinson KA, Hsieh YH, Newman-Toker DE. Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. CMAJ. (2011) 183:E571–92. doi: 10.1503/cmaj.100174
4. Machner B, Choi JH, Trillenberg P, Heide W, Helmchen C. Risk of acute brain lesions in dizzy patients presenting to the emergency room: who needs imaging and who does not? J Neurol. (2020) 267:126–35. doi: 10.1007/s00415-020-09909-x
5. Kerber KA, Brown DL, Lisabeth LD, Smith MA, Morgenstern LB. Stroke among patients with dizziness, vertigo, and imbalance in the emergency department: a population-based study. Stroke. (2006) 37:2484–7. doi: 10.1161/01.STR.0000240329.48263.0d
6. Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. (2009) 40:3504–10. doi: 10.1161/STROKEAHA.109.551234
7. Tarnutzer AA, Lee SH, Robinson KA, Wang Z, Edlow JA, Newman-Toker DE, et al. misdiagnosis of cerebrovascular events in the era of modern neuroimaging: a meta-analysis. Neurology. (2017) 88:1468–77. doi: 10.1212/WNL.0000000000003814
8. Ricciardiello F, Pisani D, Viola P, Cristiano E, Scarpa A, Giannone A, et al. Sudden sensorineural hearing loss in mild COVID-19: case series and analysis of the literature. Audiol Res. (2021) 11:313–26. doi: 10.3390/audiolres11030029
9. Pisani D, Leopardi G, Viola P, Scarpa A, Ricciardiello F, Cerchiai N, et al. Sudden sensorineural hearing loss after covid-19 vaccine; A possible adverse reaction? Otolaryngol Case Rep. (2021) 21:100384. doi: 10.1016/j.xocr.2021.100384
10. Pisani D, Gioacchini FM, Viola P, Scarpa A, Astorina A, Re M, et al. Audiovestibular Disorders after COVID-19 vaccine: is there an association? Audiol Res. (2022) 12:212–23. doi: 10.3390/audiolres12030024
11. Le TN, Westerberg BD, Lea J. Vestibular neuritis: recent advances in etiology, diagnostic evaluation, and treatment. Adv Otorhinolaryngol. (2019) 82:87–92. doi: 10.1159/000490275
12. Chiarella G, Marcianò G, Viola P, Palleria C, Pisani D, Rania V, et al. Nutraceuticals for peripheral vestibular pathology: properties, usefulness, future perspectives and medico-legal aspects. Nutrients. (2021) 13:3646. doi: 10.3390/nu13103646
13. Mayo, Clinic,. Stroke. Available online at: https://www.mayoclinic.org/diseases-conditions/stroke/symptoms-causes/syc-20350113 (accessed June 12, 2022).
14. Kerber KA, Meurer WJ, Brown DL, Burke JF, Hofer TP, Tsodikov A, et al. Stroke risk stratification in acute dizziness presentations. Neurology. (2015) 85:1869–78. doi: 10.1212/WNL.0000000000002141
15. Kim HA, Lee H. Isolated vestibular nucleus infarction mimicking acute peripheral vestibulopathy. Stroke. (2010) 41:1558–60. doi: 10.1161/STROKEAHA.110.582783
16. Thömke F, Hopf HC. Pontine lesions mimicking acute peripheral vestibulopathy. J Neurol Neurosurg Psychiatry. (1999) 66:340–9. doi: 10.1136/jnnp.66.3.340
17. Kim JS. Vertigo and gait ataxia without usual signs of lateral medullary infarction: a clinical variant related to rostral-dorsolateral lesions. Cerebrovasc Dis. (2000) 10:471–4. doi: 10.1159/000016110
18. Yi HA, Kim HA, Lee H, Baloh RW. Body lateropulsion as an isolated or predominant symptom of a pontine infarction. J Neurol Neurosurg Psychiatry. (2007) 78:372–4. doi: 10.1136/jnnp.2006.106237
19. Bertholon P, Michel D, Convers P, Antoine JC, Barral FG. Isolated body lateropulsion caused by a lesion of the cerebellar peduncles. J Neurol Neurosurg Psychiatry. (1996) 60:356–7. doi: 10.1136/jnnp.60.3.356
20. Pula JH, Newman-Toker DE, Kattah JC. Multiple sclerosis as a cause of the acute vestibular syndrome. J Neurol. (2013) 260:1649–54. doi: 10.1007/s00415-013-6850-1
21. Kattah JC, Dhanani SS, Pula JH, Mantokoudis G, Tehrani ASS, Toker DEN. Vestibular signs of thiamine deficiency during the early phase of suspected Wernicke encephalopathy. Neurol Clin Pract. (2013) 3:460–8. doi: 10.1212/01.CPJ.0000435749.32868.91
22. Kattah JC, McClelland C, Zee DS. Vertical nystagmus in Wernicke's encephalopathy: pathogenesis and role of central processing of information from the otoliths. J Neurol. (2019) 266:139–45. doi: 10.1007/s00415-019-09326-9
23. Babu S A, Schutt C, Bojrab DI. Diagnosis and Treatment of Vestibular Disorders. Springer Nature Switzerland AG (2019). doi: 10.1007/978-3-319-97858-1
24. Boehme AK, Esenwa C, Elkind MS. Stroke risk factors, genetics, and prevention. Circ Res. (2017) 120:472–95. doi: 10.1161/CIRCRESAHA.116.308398
25. Chen L, Todd M, Halmagyi GM, Aw S. Head impulse gain and saccade analysis in pontine-cerebellar stroke and vestibular neuritis. Neurology. (2014) 83:1513–22. doi: 10.1212/WNL.0000000000000906
26. Saber Tehrani AS, Kattah JC, Mantokoudis G, Pula JH, Nair D, Blitz A, et al. Small strokes causing severe vertigo: frequency of false-negative MRIs and nonlacunar mechanisms. Neurology. (2014) 83:169–73. doi: 10.1212/WNL.0000000000000573
27. Newman-Toker DE, Kerber KA, Hsieh YH, Pula JH, Omron R, Saber Tehrani AS, et al. HINTS outperforms ABCD2 to screen for stroke in acute continuous vertigo and dizziness. Acad Emerg Med. (2013) 20:986–96. doi: 10.1111/acem.12223
28. Thomalla G, Simonsen CZ, Boutitie F, Andersen G, Berthezene Y, Cheng B, et al. MRI-guided thrombolysis for stroke with unknown time of onset. N Engl J Med. (2018) 379:611–22. doi: 10.1056/NEJMoa1804355
29. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the (2018). Guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2019) 50:e344–418. doi: 10.1161/STR.0000000000000211
30. Kattah JC, Badihian S, Pula JH, Tarnutzer AA, Newman-Toker DE, Zee DS. Ocular lateral deviation with brief removal of visual fixation differentiates central from peripheral vestibular syndrome. J Neurol. (2020) 267:3763–72. doi: 10.1007/s00415-020-10100-5
31. Vanni S, Pecci R, Edlow JA, Nazerian P, Santimone R, Pepe G, et al. Differential diagnosis of vertigo in the emergency department: a prospective validation study of the STANDING algorithm. Front Neurol. (2017) 8:590. doi: 10.3389/fneur.2017.00590
32. Cousins S, Kaski D, Cutfield N, Arshad Q, Ahmad H, Gresty MA, et al. Predictors of clinical recovery from vestibular neuritis: a prospective study. Ann Clin Transl Neurol. (2017) 4:340–6. doi: 10.1002/acn3.386
33. Hain TC, Uddin M. Pharmacological treatment of vertigo. CNS Drugs. (2003) 17:85–100. doi: 10.2165/00023210-200317020-00002
34. Marill KA, Walsh MJ, Nelson BK. Intravenous Lorazepam versus dimenhydrinate for treatment of vertigo in the emergency department: a randomized clinical trial. Ann Emerg Med. (2000) 36:310–9. doi: 10.1067/mem.2000.110580
35. Di Mizio G, Marcianò G, Palleria C, Muraca L, Rania V, Roberti R, et al. Drug-drug interactions in vestibular diseases, clinical problems, and medico-legal implications. Int J Environ Res Public Health. (2021) 18:12936. doi: 10.3390/ijerph182412936
36. Strupp M, Zingler VC, Arbusow V, Niklas D, Maag KP, Dieterich M, et al. Methylprednisolone, valacyclovir, or the combination for vestibular neuritis. N Engl J Med. (2004) 351:354–61. doi: 10.1056/NEJMoa033280
37. Fishman JM, Burgess C, Waddell A. Corticosteroids for the treatment of idiopathic acute vestibular dysfunction (vestibular neuritis). Cochrane Database Syst Rev. (2011) (5):CD008607. doi: 10.1002/14651858.CD008607.pub2
38. Bronstein AM, Dieterich M. Long-term clinical outcome in vestibular neuritis. Curr Opin Neurol. (2019) 32:174–80. doi: 10.1097/WCO.0000000000000652
39. Goudakos JK, Markou KD, Psillas G, Vital V, Tsaligopoulos M. Corticosteroids and vestibular exercises in vestibular neuritis single-blind randomized clinical trial. JAMA Otolaryngol - Head Neck Surg. (2014) 140:434–40. doi: 10.1001/jamaoto.2014.48
40. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Betaistina. (2021).
41. Basura GJ, Adams ME, Monfared A, Schwartz SR, Antonelli PJ, Burkard R, et al. Clinical practice guideline: Ménière's disease. Otolaryngol - Head Neck Surg (United States). (2020) 162:S1–S55. doi: 10.1177/0194599820909439
42. Nielsen S. Benzodiazepines. Curr Top Behav Neurosci. (2015) 34:141–59. doi: 10.1007/7854_2015_425
43. Laurence Brunton RHD. The pharmacological basis of therapy 13th ed. New York, NY: McGraw-Hill Education (2018).
44. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Rome: Valium (2021).
45. Altamura AC, Moliterno D, Paletta S, Maffini M, Mauri MC, Bareggi S. Understanding the pharmacokinetics of anxiolytic drugs. Expert Opin Drug Metab Toxicol. (2013) 9:423–40. doi: 10.1517/17425255.2013.759209
46. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Lorazepam Almus. (2021)
47. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Atropina. (2018).
48. National Institutes of Health Atropine-Label. (2016). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=85225d12-3d96-427a-8027-a4530b8840b0#La57aa34a-5fd5-4d6a-9619-fc7b55a524f1
49. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Glicopirronio. (2020)
50. Storper IS, Spitzer JB, Scanlan M. Use of glycopyrrolate in the treatment of Meniere's disease. Laryngoscope. (1998) 108:1442–5. doi: 10.1097/00005537-199810000-00004
51. National Institutes of Health Glycopyrrolate tablet-Label. (2020). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=26cdd84d-ffa0-4e52-b359-4acef4bd8093 (accessed June 5, 2022).
52. National National Institutes of Health Glycopyrrolate injection solution-Label. (2021). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=88d3e865-8dca-4c89-b6f7-a34c481f75b9
53. Chabicovsky M, Winkler S, Soeberdt M, Kilic A, Masur C, Abels C. Pharmacology, toxicology and clinical safety of glycopyrrolate. Toxicol Appl Pharmacol. (2019) 370:154–69. doi: 10.1016/j.taap.2019.03.016
54. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Scopolamina bromidrato. (2016)
55. Rahko T, Karma P. Transdermal scopolamine for peripheral vertigo (A double-blind study). J Laryngol Otol. (1985) 99:653–6. doi: 10.1017/S0022215100097425
56. Plescia F, Salvago P, Dispenza F, Messina G, Cannizzaro E, Martines F. Efficacy and pharmacological appropriateness of cinnarizine and dimenhydrinate in the treatment of vertigo and related symptoms. Int J Environ Res Public Health. (2021) 18:4787. doi: 10.3390/ijerph18094787
57. AIFA. Agenzia Italiana del Farmaco- Riassunto delle caratteristiche del prodotto. Rome: Dimenidrinato (2021).
58. National National Institutes of Health Dimenhydrinate injection solution-Label. (2020). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=bc71539e-1a33-4709-8a24c2894e8dbc1c (accessed June 5, 2022).
59. AIFA. Agenzia Italiana del Farmaco Riassunto delle Caratteristiche del Prodotto. Rome: Cinnarizina (2018)
60. Hausler R, Sabani E RM. L'effet de la Cinnarizine sur divers types de vertiges. Résultats cliniques et électronystagmographiques d'une étude en double aveugle. Acta Otorhinolaryngol Belg. (1989) 43:177–85.
61. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Rome: Arlevertan (2016)
62. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Rome: Difenidramina (2017)
63. Takatani T, Ito J, Matsuoka I, Sasa M, Takaori S. Effects of diphenhydramine iontophoretically applied onto neurons in the medial and lateral vestibular nuclei. Jpn J Pharmacol. (1983) 33:557–61. doi: 10.1016/S0021-5198(19)52491-X
64. National Institutes of Health Diphenhydramine-Label. (2019). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=f3b177ef-55d5-4525-bf33-99205c414a5b (accessed June 5, 2022).
65. National Institutes of Health. NIGHTTIME SLEEP AID MAXIMUM STRENGTH- diphenhydramine hydrochloride 50 mg capsule, liquid filled (2019). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2b1af499-623e-4f6a-949b-21abf276b65d (accessed June 5, 2022).
66. Huang W, Zhang J, Wei P, Schrader WT, Moore DD. Meclizine is an agonist ligand for mouse constitutive androstane receptor (CAR) and an inverse agonist for human CAR. Mol Endocrinol. (2004) 18:2402–8. doi: 10.1210/me.2004-0046
67. National Institutes of Health Meclizine-Label. (2017). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=b13cb390-20ed-43ce-aa74-5a754539f6e2 (accessed June 5, 2022).
68. National Institutes of Health MECLIZINE HCL 12.5 MG tablet-Label. (2017). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=76efad7e-e765-430f-9232-63553d02f2c5 (accessed June 5, 2022).
69. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Rome: Prometazina (2021).
70. Zabirowicz ES, Gan TJ. 34 - Pharmacology of Postoperative Nausea and Vomiting. Second Edition Philadelphia, PA: Elsevier Inc. (2019). doi: 10.1016/B978-0-323-48110-6.00034-X
71. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto. Metoclopramide (Oral). (2021).
72. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto-Metoclopramide (Intravenous). (2016).
75. Tighilet B, Léonard J, Watabe I, Bernard-Demanze L, Lacour M. Betahistine treatment in a cat model of vestibular pathology: Pharmacokinetic and pharmacodynamic approaches. Front Neurol. (2018) 9:1–11. doi: 10.3389/fneur.2018.00431
76. National Institutes of Health-Clonazepam. (2008). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=acbce0e8-5098-4785-943b-8bdb5ff17fab (accessed June 5, 2022).
77. National National Institutes of Health Diazepam-injection solution. (2020). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=1e6c2f52-73ff-429b-8f1b-9b5b61ce1ac5 (accessed June 5, 2022).
78. National Institutes of Health Lorazepam injection. (2021). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=b5b17cde-a94c-4105-871c-54e7d2bd47e8 (accessed June 5, 2022).
79. National Institutes of Health Lorazepam tablet-Label. (2021). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=ad2a0633-50fe-4180-b743-c1e49fc110c6 (accessed June 5, 2022).
80. Cornelissen AS, Klaassen SD, van Groningen T, Bohnert S, Joosen MJA. Comparative physiology and efficacy of atropine and scopolamine in sarin nerve agent poisoning. Toxicol Appl Pharmacol. (2020) 396:114994. doi: 10.1016/j.taap.2020.114994
81. EMA. European Medicines Agency Summary of product characteristics. Amsterdam, NL: Glycopyrronium (2021).
82. NIH. National Institutes of Health Scopolamine transdermal system-scolopamine transdermal system patch, extended release. (2019). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=cb93bfad-3e37-4a27-92f6-f21703ae7bdf
83. Kariya S, Isozaki S, Narimatsu S, Suzuki T. Oxidative metabolism of cinnarizine in rat liver microsomes. Biochem Pharmacol. (1992) 44:1471–4. doi: 10.1016/0006-2952(92)90552-T
84. Kariya S, Isozaki S, Uchino K, Suzuki T, Narimatsu S. Oxidative metabolism of flunarizine and cinnarizine by microsomes from B-lymphoblastoid cell lines expressing human cytochrome P450 enzymes. Biol Pharm Bull. (1996) 19:1511–14. doi: 10.1248/bpb.19.1511
85. Nguyen T, Polyakova B, Cerenzio J, Ramilo JR. Diphenhydramine use in end-stage kidney disease. Am J Ther. (2021) 28:232–7. doi: 10.1097/MJT.0000000000001057
87. Akutsu T, Kobayashi K, Sakurada K, Ikegaya H, Furihata T. Identification of human cytochrome P450 isozymes involved in diphenhydramine N -demethylation. Curr Drug Metab. (2007) 35:72–8. doi: 10.1124/dmd.106.012088
89. Wang Z, Lee B, Pearce D, Qian S, Wang Y. Meclizine metabolism and pharmacokinetics : formulation on its absorption. J Clin Pharmacol. (2012) 52:1343–9. doi: 10.1177/0091270011414575
90. National Institutes of Health Promethazine-Label. (2015). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=51e3baab-eba7-460c-9de1-bf6cfc378310 (accessed June 5, 2022).
91. Taylor G, Houston JB, Shaffer J, Maweri G. Pharmacokinetics of promethazine and its sulphoxide metabolite after intravenous and oral administration to man. Br J Clin Pharmacol. (1983) 15:287–93. doi: 10.1111/j.1365-2125.1983.tb01501.x
92. National Institutes of Health Metoclopramide tablet-Label. (2010). Available online at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=55f1ee88-a455-44ba-b51a-2fcefe8eda65
93. Shakhatreh M, Jehangir A, Malik Z, Parkman HP, Shakhatreh M, Jehangir A, et al. Metoclopramide for the treatment of diabetic gastroparesis Metoclopramide for the treatment of diabetic gastroparesis. Expert Rev Gastroenterol Hepatol. (2019) 13:711–21. doi: 10.1080/17474124.2019.1645594
94. Lemon LS, Zhang H, Hebert MF, Hankins GD, Haas DM, Caritis SN, Venkataramanan R. Ondansetron exposure changes in a pregnant woman. Pharmacotherapy. (2016) 36:139–41. doi: 10.1002/phar.1796
95. Scott JA, Wood M, Flood P. The pronociceptive effect of ondansetron in the setting of P-glycoprotein inhibition. Anesth Analg. (2006) 103:742–6. doi: 10.1213/01.ane.0000228861.80314.22
96. AIFA. Agenzia Italiana del Farmaco Riassunto delle caratteristiche del prodotto-Acitlyse. AIFA (2021).
98. Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. Thrombolysis with Alteplase 3 to 45 hours after acute ischemic stroke. N Engl J Med. (2011) 359:1317–29. doi: 10.1056/NEJMoa0804656
99. Yayan J. Lingual angioedema with macroglossia during the treatment of acute ischemic stroke with Alteplase. Int J Gen Med. (2012) 5:183–6. doi: 10.2147/IJGM.S29200
100. Campbell BCV, Mitchell PJ, Churilov L, Yassi N, Kleinig TJ, Dowling RJ, et al. Tenecteplase versus alteplase before thrombectomy for ischemic stroke. N Engl J Med. (2018) 378:1573–82. doi: 10.1056/NEJMoa1716405
101. Logallo N, Novotny V, Assmus J, Kvistad CE, Alteheld L, Rønning OM, et al. Tenecteplase versus Alteplase for management of acute ischaemic stroke (NOR-TEST): a phase 3, randomised, open-label, blinded endpoint trial. Lancet Neurol. (2017) 16:781–8. doi: 10.1016/S1474-4422(17)30253-3
102. Rocca B, Petrucci G. Variability in the responsiveness to low-dose Aspirin: pharmacological and disease-related mechanisms. Thrombosis. (2012) 2012:376721. doi: 10.1155/2012/376721
103. Yokoyama H, Mastumura T, Soeda S, Suzuki Y, Watanabe M, Kashiwakura E, et al. The evaluation method for antiplatelet effect of acetylsalicylic acid. Eur J Drug Metab Pharmacokinet. (2014) 39:327–33. doi: 10.1007/s13318-013-0170-9
104. AIFA. Agenzia Italiana del Farmaco Aspirina- Riassunto delle caratteristiche del prodotto. (2021).
105. Sandercock PAG, Counsell C, Tseng MC, Cecconi E. Oral antiplatelet therapy for acute ischaemic stroke. Cochrane Database Syst Rev. (2014) 2014:CD000029. doi: 10.1002/14651858.CD000029.pub3
106. Johnston SC, Easton JD, Farrant M, Barsan W, Conwit RA, Elm JJ, et al. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA. N Engl J Med. (2018) 379:215–25. doi: 10.1056/NEJMoa1800410
107. Wang Y, Wang Y, Zhao X, Liu L, Wang D, Wang C, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med. (2013) 369:11–9. doi: 10.1056/NEJMoa1215340
108. Xu J, Wang A, Wangqin R, Mo J, Chen Z, Dai L, et al. Efficacy of clopidogrel for stroke depends on CYP2C19 genotype and risk profile. Ann Neurol. (2019) 86:419–26. doi: 10.1002/ana.25535
109. Khatri P, Kleindorfer DO, Devlin T, Sawyer RN, Starr M, Mejilla J, et al. Effect of Alteplase vs aspirin on functional outcome for patients with acute ischemic stroke and minor nondisabling neurologic deficits the PRISMS randomized clinical trial. JAMA - J Am Med Assoc. (2018) 320:156–66. doi: 10.1001/jama.2018.8496
110. Caprio FZ, Sorond FA. Cerebrovascular disease: primary and secondary stroke prevention. Med Clin North Am. (2019) 103:295–308. doi: 10.1016/j.mcna.2018.10.001
111. Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, et al. 2021 Guideline for the prevention of stroke in patients with stroke and transient ischemic attack; A guideline from the American Heart Association/American Stroke Association. Stroke. (2021) 52:E364–467. doi: 10.1161/STR.0000000000000375
112. Russo NW, Petrucci G, Rocca B. Aspirin, stroke and drug-drug interactions. Vascul Pharmacol. (2016) 87:14–22. doi: 10.1016/j.vph.2016.10.006
113. Andrade C, Sharma E. Serotonin reuptake inhibitors and risk of abnormal bleeding. Psychiatr Clin North Am. (2016) 39:413–26. doi: 10.1016/j.psc.2016.04.010
114. Webster J. Interactions of NSAIDs with diuretics and β-blockers: mechanisms and clinical implications. Drugs. (1985) 30:32–41. doi: 10.2165/00003495-198530010-00004
115. Lapi F, Azoulay L, Yin H, Nessim SJ, Suissa S. Concurrent use of diuretics, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers with non-steroidal anti-inflammatory drugs and risk of acute kidney injury: Nested case-control study. BMJ. (2013) 346:e8525. doi: 10.1136/bmj.e8525
116. EMA. European Medicines Agency Plavix-Summary of product characteristics. Amsterdam, NL (2021).
117. Patti G, Micieli G, Cimminiello C, Bolognese L. The role of clopidogrel in 2020: a reappraisal. Cardiovasc Ther. (2020) 2020:8703627. doi: 10.1155/2020/8703627
118. Jiang X-L, Samant S, Lesko LJ, Schmidt S. Clinical pharmacokinetics and pharmacodynamics of clopidogrel. Clin Pharmacokinet. (2015) 54:147–66. doi: 10.1007/s40262-014-0230-6
119. Mangalpally KKR, Kleiman NS. The safety of clopidogrel. Expert Opin Drug Saf. (2011) 10:85–95. doi: 10.1517/14740338.2011.532485
120. Caplain H. Enhanced antiplatelet effects of clopidogrel plus acetylsalicylic acid compared with acetylsalicylic acid alone or combined with extended-release dipyridamole in healthy volunteers. Cerebrovasc Dis. (2005) 19:214–9. doi: 10.1159/000083885
121. Chaturvedi S. Acetylsalicylic acid + extended-release dipyridamole combination therapy for secondary stroke prevention. Clin Ther. (2008) 30:1196–205. doi: 10.1016/S0149-2918(08)80046-X
122. Bath PM, Woodhouse LJ, Appleton JP, Beridze M, Christensen H, Dineen RA, et al. Antiplatelet therapy with aspirin, clopidogrel, and dipyridamole versus clopidogrel alone or aspirin and dipyridamole in patients with acute cerebral ischaemia (TARDIS): a randomised, open-label, phase 3 superiority trial. Lancet. (2018) 391:850–9. doi: 10.1016/S0140-6736(17)32849-0
123. Yang M, Huo X, Miao Z, Wang Y. Platelet glycoprotein IIb/IIIa receptor inhibitor tirofiban in acute ischemic stroke. Drugs. (2019) 79:515–29. doi: 10.1007/s40265-019-01078-0
124. Ciccone A, Motto C, Abraha I, Cozzolino F, Santilli I. Glycoprotein IIb-IIIa inhibitors for acute ischaemic stroke. Cochrane Database Syst Rev. (2014) 2014:CD005208. doi: 10.1002/14651858.CD005208.pub3
125. Liu J, Yang Y, Liu H. Efficacy outcomes and safety measures of intravenous tirofiban or eptifibatide for patients with acute ischemic stroke: a systematic review and meta-analysis of prospective studies. J Thromb Thrombolysis. (2021) 53:898–910. doi: 10.1007/s11239-021-02584-3
126. Johnston SC, Amarenco P, Denison H, Evans SR, Himmelmann A, James S, et al. Ticagrelor and aspirin or aspirin alone in acute ischemic stroke or TIA. N Engl J Med. (2020) 383:207–17. doi: 10.1056/NEJMoa1916870
127. Johnston SC, Amarenco P, Albers GW, Denison H, Easton JD, Evans SR, et al. Ticagrelor versus aspirin in acute stroke or transient ischemic attack. N Engl J Med. (2016) 375:35–43. doi: 10.1056/NEJMoa1603060
128. Strupp M, Magnusson M. Acute unilateral vestibulopathy. Neurol Clin. (2015). 33:669–85. doi: 10.1016/j.ncl.2015.04.012
129. Hülse R, Biesdorf A, Hörmann K, Stuck B, Erhart M, Hülse M, et al. Peripheral vestibular disorders: an epidemiologic survey in 70 million individuals. Otol Neurotol. (2019) 40:88–95. doi: 10.1097/MAO.0000000000002013
130. Viola P, Ralli M, Pisani D, Malanga D, Sculco D, Messina L, et al. Tinnitus and equilibrium disorders in COVID-19 patients: preliminary results. Eur Arch Otorhinolaryngol. (2021) 278:3725–30. doi: 10.1007/s00405-020-06440-7
131. Esaki S, Goshima F, Kimura H, Ikeda S, Katsumi S, Kabaya K, et al. Auditory and vestibular defects induced by experimental labyrinthitis following herpes simplex virus in mice. Acta Otolaryngol. (2011) 131:684–91. doi: 10.3109/00016489.2010.546808
132. Kim JS. When the room is spinning: experience of vestibular neuritis by a neurotologist. Front Neurol. (2020) 11:157. doi: 10.3389/fneur.2020.00157
133. De Luca P, Cassandro C, Ralli M, Di Stadio A, Viola P, Cassandro E, et al. Therapeutic options in Meniere's disease: our experience. Am J Otolaryngol. (2021) 42:102939. doi: 10.1016/j.amjoto.2021.102939
134. Scarpa A, Ralli M, Viola P, Cassandro C, Alicandri-Ciufelli M, Iengo M, et al. Food-induced stimulation of the antisecretory factor to improve symptoms in Meniere's disease: our results. Eur Arch Otorhinolaryngol. (2020) 277:77–83. doi: 10.1007/s00405-019-05682-4
135. Viola P, Pisani D, Scarpa A, Cassandro C, Laria C, Aragona T, et al. The role of endogenous Antisecretory Factor (AF) in the treatment of Ménière's Disease: a two-year follow-up study. Preliminary results. Am J Otolaryngol. (2020) 41:102673. doi: 10.1016/j.amjoto.2020.102673
136. Sjögren J, Magnusson M, Tjernström F, Karlberg M. Steroids for acute vestibular neuronitis-the earlier the treatment, the better the outcome? Otol Neurotol. (2019) 40:372–4. doi: 10.1097/MAO.0000000000002106
137. Leong KJ, Lau T, Stewart V, Canetti EFD. Systematic review and meta-analysis: effectiveness of corticosteroids in treating adults with acute vestibular neuritis. Otolaryngol Head Neck Surg. (2021) 165:255–66. doi: 10.1177/0194599820982910
138. Hillier S, McDonnell M. Is vestibular rehabilitation effective in improving dizziness and function after unilateral peripheral vestibular hypofunction? An abridged version of a Cochrane Review. Eur J Phys Rehabil Med. (2016) 52:541–56.
139. Jeong SH, Kim HJ, Kim JS. Vestibular neuritis. Semin Neurol. (2013) 33:185–94. doi: 10.1055/s-0033-1354598
140. McDonnell MN, Hillier SL. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database Syst Rev. (2015) 1:CD005397. doi: 10.1002/14651858.CD005397.pub4
141. Karkos PD, Leong SC, Arya AK, Papouliakos SM, Apostolidou MT, Issing WJ. 'Complementary ENT': a systematic review of commonly used supplements. J Laryngol Otol. (2007) 121:779–82. doi: 10.1017/S002221510600449X
142. Casani AP, Navari E, Albera R, Agus G, Asprella Libonati G, Chiarella G, et al. Approach to residual dizziness after successfully treated benign paroxysmal positional vertigo: effect of a polyphenol compound supplementation. Clin Pharmacol. (2019) 11:117–25. doi: 10.2147/CPAA.S210763
143. Savitz SI, Caplan LR. Vertebrobasilar disease. N Engl J Med. (2005) 352:2618–26. doi: 10.1056/NEJMra041544
145. Lee H. Recent advances in acute hearing loss due to posterior circulation ischemic stroke. J Neurol Sci. (2014) 338:23–9. doi: 10.1016/j.jns.2013.12.048
146. Oas JG, Baloh RW. Vertigo and the anterior inferior cerebellar artery syndrome. Neurology. (1992) 42:2274–9. doi: 10.1212/WNL.42.12.2274
147. Bodranghien F, Bastian A, Casali C, Hallett M, Louis ED, Manto M, et al. Consensus paper: revisiting the symptoms and signs of cerebellar syndrome. Cerebellum. (2016) 15:369–91. doi: 10.1007/s12311-015-0687-3
148. Sunderland S. The arterial relations of the internal auditory meatus. Brain. (1945) 68:23–27. doi: 10.1093/brain/68.1.23
149. Manto M, Bower JM, Conforto AB, Delgado-García JM, da Guarda SN, Gerwig M, et al. Consensus paper: roles of the cerebellum in motor control–the diversity of ideas on cerebellar involvement in movement. Cerebellum. (2012) 11:457–87. doi: 10.1007/s12311-011-0331-9
150. Fujita H, Kodama T, du Lac S. Modular output circuits of the fastigial nucleus for diverse motor and nonmotor functions of the cerebellar vermis. Elife. (2020) 9:e58613. doi: 10.7554/eLife.58613
151. Wang L, Huang G, Zhang L, Yang J, Ren C, Liang C, et al. Effects of the intermittent theta burst stimulation of the cerebellar vermis on balance recovery after stroke: a study protocol for a randomized controlled trial. Front Aging Neurosci. (2022) 14:881311. doi: 10.3389/fnagi.2022.881311
Keywords: acute vestibular syndrome, vestibular neuritis, posterior circulation stroke, vertigo, pharmacologic treatment
Citation: Viola P, Gioacchini FM, Astorina A, Pisani D, Scarpa A, Marcianò G, Casarella A, Basile E, Rania V, Re M and Chiarella G (2022) The pharmacological treatment of acute vestibular syndrome. Front. Neurol. 13:999112. doi: 10.3389/fneur.2022.999112
Received: 21 July 2022; Accepted: 17 August 2022;
Published: 09 September 2022.
Edited by:
Salvatore Martellucci, Hospital Santa Maria Goretti, ItalyReviewed by:
Jorge Kattah, University of Illinois at Chicago, United StatesRoberto Gallus, Mater Olbia Hospital, Italy
Copyright © 2022 Viola, Gioacchini, Astorina, Pisani, Scarpa, Marcianò, Casarella, Basile, Rania, Re and Chiarella. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alfonso Scarpa, YWxmb25zb3NjYXJwYUB5YWhvby5pdA==
†ORCID: Alfonso Scarpa orcid.org/0000-0001-9219-6175