 Qian Lu
Qian Lu Yang-Yang Wang
Yang-Yang Wang Hui-Min Chen1,2
Hui-Min Chen1,2 Li-Ping Zou
Li-Ping Zou
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 27 September 2022
Sec. Pediatric Neurology
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.982050
Objective: SCN1A, encoding the alpha 1 subunit of the sodium channel, is associated with a range of related epilepsy. This study aims to assess saliva and urine pH in children with SCN1A-related epilepsy.
Methods: A prospective controlled observational study with a 1:1 ratio was conducted on seven patients with SCN1A-related epilepsy and seven healthy children of the same family, gender, and age but without a history of seizures. The pH of saliva and urine was measured by pH test paper. Parents of patients with epilepsy recorded seizures to compare the relationship between pH and seizures.
Results: The fourteen participants were all males, aged 1 to 14 years. Seven patients had different pathogenic SCN1A variants. The pH of saliva and urine was monitored for 21–95 days. The pH of saliva and urine was higher in patients with SCN1A-related epilepsy than in the healthy group. The urine pH in Dravet syndrome patients was high compared with other epilepsy patients. The urine pH in patients with seizures was higher than that in patients without seizures, which occurred during the study.
Conclusions: The pH of saliva and urine was chronically high in patients with SCN1A-related epilepsy, and urine pH was higher in patients with seizures and with Dravet syndrome.
Epilepsy is a common chronic neurological disease and affects about 0.5–1% of children (1). About 50 million people worldwide have epilepsy, of which 25% are children under 15 years of age (2, 3). The etiology of epilepsy is complex and includes genetic, structural, infectious, immune, metabolic, and unknown etiologies (4). Voltage-gated sodium ion channels (VGSCs) are involved in the generation of action potentials in neural cells, and mutations associated with these channel genes are common causes of genetic epilepsies (5).
SCN1A locates at 2q24.3 and encodes the α1 subunit of the sodium channel (Nav1.1). Nav1.1 is mainly distributed in neuron cell bodies, dendrites, and the initial segment of axons in the central nervous system (6). SCN1A-related diseases have a wide range of clinical phenotypes, which are associated with a variety of epileptic types, such as febrile seizure and Dravet syndrome (7). Sudden and repeated seizures not only affect the health of children but also cause psychological burdens for their parents.
Elevated pH leads to increased neural excitability. An increase in brain pH was observed during seizures in a rat model of febrile seizures (8). Hot water bathing could induce respiratory alkalosis in Scn1a mutant rats (9). Inhalation of carbon dioxide rapidly terminates hyperthermia-induced seizures in febrile seizure rats and Scn1a mutant rats (8, 9). We previously found that 5% CO2 reduced the seizures of the kainic acid rat model by reducing the cortex pH (10).
Seizures cause pH fluctuations in the brain. Functional magnetic resonance imaging is a non-invasive method used to detect brain pH (11). Although this method is sensitive, it cannot continuously monitor brain pH. Blood pH analysis is inconvenient, especially during the COVID-19 pandemic. For children, non-invasive methods such as saliva and urine collection are simple and can be performed daily at home.
Therefore, we aimed to assess the pH of saliva and urine in a series of patients with SCN1A-related epilepsy. In this study, the pH of saliva and urine were compared between patients and controls of the same age, gender, and family.
We included ten patients with epilepsy with pathogenic SCN1A variants who were treated in the Department of Pediatrics, the First Medical Center of PLA General Hospital from November 2019 to January 2021. Seven healthy children of the same age, gender, and family but without a history of seizures were included in the control group. Three patients with epilepsy were excluded because they could not find suitable healthy children in the control group (Figure 1). We collected the age, gender, home address, birth history, family history, and history of medication of participants. This study obtained informed consent from the guardians and was conducted following the Declaration of Helsinki.
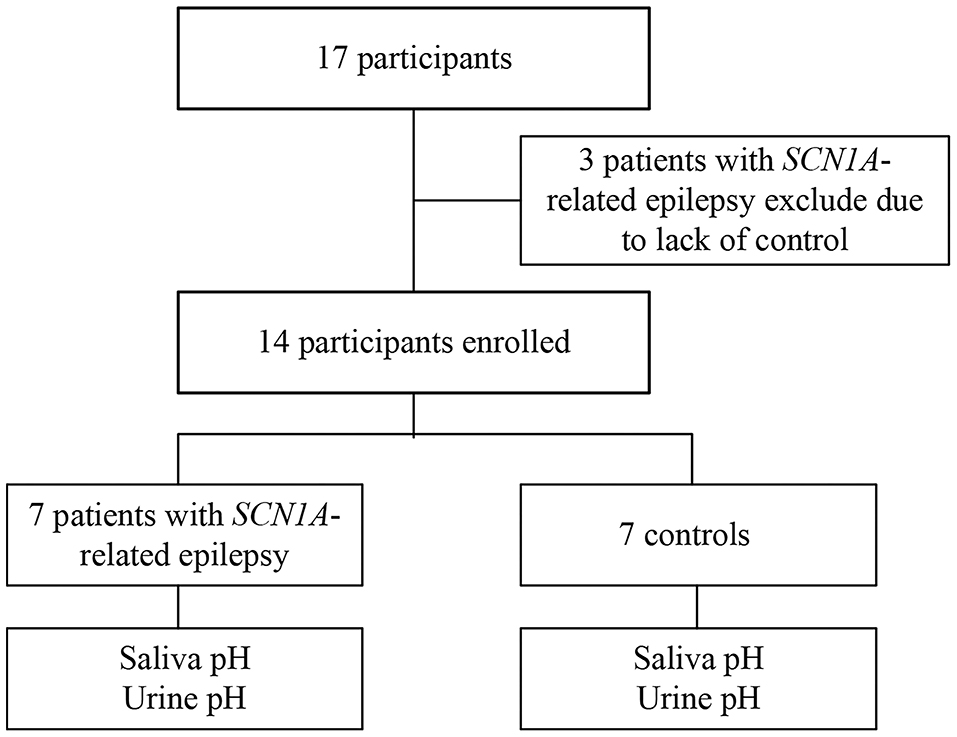
Figure 1. Flow diagram of study participants.
The pH of saliva and urine was measured for all participants by their patients using pH test paper (Geshan OB/440100710745-2007) (Supplementary Figure 1), and the measurement range of pH was 4.50–9.00. Before the beginning of the study, parents had been trained to interpret the color of the pH test paper. Parents must truthfully record pH values. Saliva pH was measured after getting up in the morning without oral activities such as eating and gargling before measurement. The pH test paper was placed in the middle of the tongue. After the test paper was soaked with saliva, it was taken out and compared with the standard color card to record the saliva pH. Urine pH was measured in clean-catch midstream urine in the morning. After the test paper was soaked with urine, it was taken out and compared with the standard color card to record the urine pH.
Genomic DNA was extracted from the whole blood of patients with epilepsy and their parents. Patients 1, 3, and 6 were subjected to the whole exome-sequencing with an average sequencing depth of 100× and covering upstream and downstream 50 bp. A febrile seizure panel with 189 genes related to febrile seizure was performed on patients 2 and 5. An epilepsy gene panel with 152 genes related to epilepsy was performed on patient 4. Sanger sequencing of SCN1A was performed on patient 7. Variants were screened for the various types, genetic patterns, population frequencies, and a list of genes associated with the main phenotypic characteristics of the patients. All parents were validated by Sanger sequencing. The pathogenicity of the variants was evaluated by Mutation Taster and PolyPhen-2.
Non-normally distributed data were presented as median with interquartile. SPSS24.0 was used for statistical analysis. Wilcoxon test was used to assess the difference between the two groups. A p-value of < 0.05 indicated statistical significance.
Fourteen children were included in this study. Seven children were patients with SCN1A-related epilepsy, including two Dravet syndrome patients (patients 1 and 7). Seven healthy children of the same family, age, and gender without a history of seizures were classified as the healthy group (Table 1). The children were boys aged 1 to 14 years. The monitoring time of pH ranged from 21 to 95 days. The onset age of seven patients with epilepsy was <1 year old. Four patients had tonic–clonic seizures, one patient had tonic seizures, one patient had clonic seizures, and one patient had epileptic spasms seizures. Three patients took more than two antiseizure medications. Patients 1, 3, and 7 had seizures during the study.
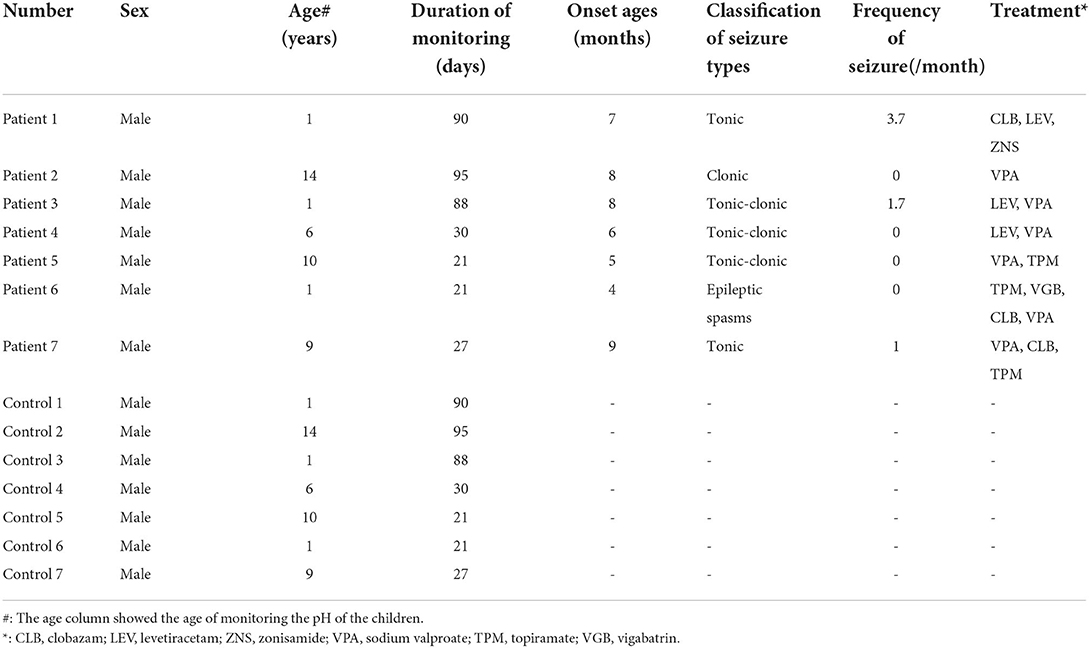
Table 1. Clinical characteristics of the fourteen participants.
Seven patients with SCN1A-related epilepsy had seven different SCN1A variants (NM_001165963.4) (Table 2). Figure 2 shows the distribution of SCN1A variant sites. Patient 1 (c.4465C>T p.Gln1489*) had a de novo nonsense variant. Patient 5 (c.1662G>A p.Gln554=) had a de novo synonymous variant, which was reported to be associated with epilepsy (12) and was pathogenic in the ClinVar database (https://www.ncbi.nlm.nih.gov/clinvar/variation/206771/). Patient 7 (c.2589 +3A>T) had a de novo splicing variant located in intron 14, which was reported to be associated with epilepsy (12) and was also included in the SCN1A variants database (http://scn1a.caae.org.cn/scn1a_variant.php). Patient 4 (c.4834G>A p.Val1612Ile) had a missense variant, the same variant as his mother, which was associated with epilepsy in infancy and also inherited from the mother (13). The three other patients had de novo missense variants. Variants in patient 2 (c.5086A>G p.Lys1696Glu), patient 3 (c.5752T>C p.Ser1918Pro) and patient 6 (c.4105T>A p.Phe1369Ile) were not reported. The evaluation results of Mutation Taster and Polyphen-2 and the American College of Medical Genetics and Genomics (ACMG) classification of all patients are shown in Table 2.
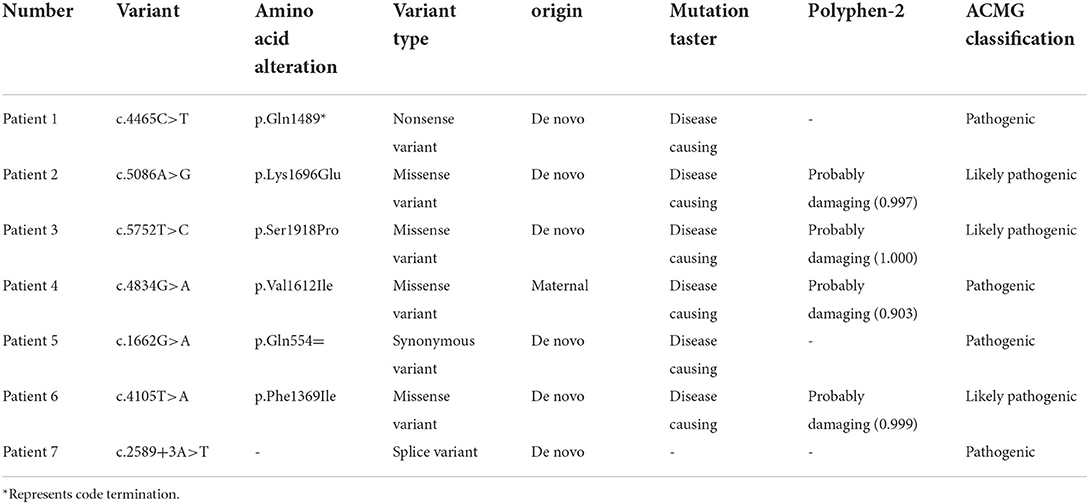
Table 2. Analysis of SCN1A variants of seven patients. (NM_001165963.4).
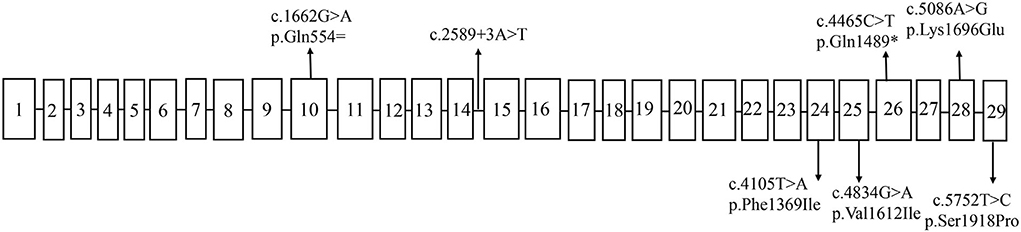
Figure 2. The distribution of SCN1A variants sites.
The saliva and urine pH of the participants are shown in Figure 3. The red square represents patients with SCN1A-related epilepsy, and the blue triangle represents the control group. The saliva pH of the patients was higher than that in the control group [6.5 (6.25, 6.75) vs. 6.00 (5.50, 6.50), p < 0.001]. The urine pH of the patients was higher than that in the control group [6.25 (5.75, 6.50) vs. 6.00 (5.75, 6.25), p < 0.001].

Figure 3. The pH of fourteen participants. (A) Shows saliva pH. The saliva pH distribution of patients with SCN1A-related epilepsy was higher than that in the healthy group, and the average pH curve was higher than that in the healthy group. (B) Shows urine pH, which distribution of patients was higher than that in the healthy group. The horizontal axis is the number of monitoring days, the vertical axis is the pH, and the curve is the average pH. The blue triangle is the pH of the healthy group, and the red square is the pH of patients with SCN1A-related epilepsy.
Patients 1 and 7 were diagnosed with Dravet syndrome. The saliva pH of the two Dravet syndrome patients (the mean pH is 6.38) was lower than that of other epilepsy patients (the mean pH is 6.54) (p < 0.001). The urine pH of the two Dravet syndrome patients was higher than that of other epilepsy patients [6.50 (6.00, 6.75) vs. 6.00(5.75, 6.50), p < 0.001] (Supplementary Figure 2).
Patients with SCN1A-related epilepsy were divided into two groups according to whether they had seizures during the study. Patients 1, 3, and 7 had seizures during the study. The saliva pH of the three patients who had seizures was higher than that of the healthy group [6.50 (6.40, 6.75) vs. 5.75 (5.00, 6.00), p < 0.001]. The urine pH of the three patients who had seizures was higher than that of the healthy control group [6.25 (6.00, 6.75) vs. 6.00 (5.75, 6.25), p < 0.001].
We compared the saliva and urine pH in patients who had seizures or not. Patients with seizures had higher urine pH than those without seizures that occurred during the study [6.25 (6.00, 6.75) vs. 6.00 (5.74, 6.50), p < 0.001]. There was no difference in saliva pH between the two groups (p= 0.114) (Supplementary Figure 3).
The saliva and urine pH were chronically high in this series of patients with SCN1A-related epilepsy. There was no study on the saliva and urine pH in patients with SCN1A-related epilepsy. However, there are more studies on epilepsy and acidosis (8–10). We previously reported that 5% CO2 inhalation can suppress hyperventilation-induced absence seizures in children (14). Acid-sensing ion channel 1a (ASIC1a) is widely expressed in the central nervous system and is sensitive to extracellular pH. Disrupting mouse ASIC1a increased the severity of seizures and CO2 inhalation did not terminate seizures, while overexpressing ASIC1a had the opposite effect (15). Acidosis and ASIC1a play an important role in epilepsy (16, 17). Inhalation of CO2 can suppress seizures by reducing brain pH and activating ASIC1a. Acidosis activates ASIC1a and inhibits N-methyl-D-Aspartate (NMDA) receptors to reduce seizures (18). Acidosis also terminates seizures by activating ASIC1a and inhibiting interneurons (15). From the studies, we know that acid and base changes have a great impact on epilepsy. Thus, we chose a non-invasive method to measure the pH in children with SCN1A-related epilepsy.
Antiseizure medications, such as valproic acid, levetiracetam, and carbonic anhydrases, could decrease brain pH, suggesting that acidosis contributes to antiepileptic effects (19–21). Topiramate is a carbonic anhydrase inhibitor used to treat many types of epilepsy. Studies have found that topiramate can appropriately lower the pH of neuronal cells (22, 23). Topiramate has specific adverse effects, such as hypohidrosis and hyperthermia (24, 25). In epileptic children, the body temperature can reach 38.8°C (26). Hyperthermia is contraindicated for heat-sensitive epilepsy (SCN1A-related epilepsy such as Dravet syndrome). However, topiramate is effective in patients with Dravet syndrome, and approximately 35–78% of patients have reduced seizures by more than 50% (27). In our study, topiramate was used in three patients (patients 5, 6, and 7). The saliva pH of the three patients treated with topiramate (the mean pH is 6.43) was lower than that of those (the mean pH is 6.51) not treated with topiramate (p = 0.004). Three patients had higher urine pH than those not treated with topiramate [6.75 (6.50, 6.75) vs. 6.50 (6.25, 6.50), p < 0.001]. Studies have shown that TPM increases urine pH (28), and so does our patient's urine pH.
Saliva pH was measured with an electrode pH meter in the previous study (29). We used pH test paper to measure pH, which is easy to operate and cheap. And it is highly accepted by parents. Our study investigated the pH levels of saliva and urine in patients with SCN1A-related epilepsy, blood pH was not involved in the study. Diets rich in cereal grains and animal protein may decrease pH. A high intake of fruits and vegetables may increase the urine pH (30). Therefore, saliva and urine pH monitoring could guide the diet of epilepsy patients.
The study has limitations. We recruited a small number of patients. Diet will affect the pH of saliva and urine. We selected children from the same family as the control group to reduce the influence of diet. Therefore, we did not strictly control the diet of the participants.
The pH of saliva and urine was chronically higher in patients with SCN1A-related epilepsy than in the control group. This is the first study to evaluate the pH of saliva and urine in SCN1A-related epilepsy patients, which would be the first step in the application of preventive therapeutic strategies for patients with SCN1A-related epilepsy.
The data that support the conclusions of this article are available from the corresponding author, upon reasonable request.
The studies involving human participants were reviewed and approved by Chinese PLA General Hospital. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. Written informed consent was obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
QL and L-PZ participated in the study design, data analysis, and manuscript drafting. Y-YW contributed to the data analysis and manuscript drafting. H-MC, Q-HW, and X-YY conducted data collection. All authors have read and approved the final manuscript.
We sincerely acknowledge the support of all of the participants who contributed to this study. We thank Li-Na Tang for contacting patients.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.982050/full#supplementary-material
VGSCs, Voltage-gated sodium ion channels; Nav1.1, α1 subunit of the sodium channel; CLB, clobazam; LEV, levetiracetam; ZNS, zonisamide; VPA, sodium valproate; TPM, topiramate; VGB, vigabatrin; ACMG, the American College of Medical Genetics and Genomics; ASIC1a, Acid-sensing ion channel 1a; NMDA, N-methyl-D-Aspartate.
1. Aaberg KM, Gunnes N, Bakken IJ, Lund Søraas C, Berntsen A, Magnus P, et al. Incidence and prevalence of childhood epilepsy: a nationwide cohort study. Pediatrics. (2017) 139:3098. doi: 10.1542/peds.2016-3908
2. Guerrini R. Epilepsy in children. Lancet). (2006) 367:499–524. doi: 10.1016/S0140-6736(06)68182-8
3. Megiddo I, Colson A, Chisholm D, Dua T, Nandi A, Laxminarayan R. Health and economic benefits of public financing of epilepsy treatment in India: an agent-based simulation model. Epilepsia. (2016) 57:464–74. doi: 10.1111/epi.13294
4. Scheffer IE, Berkovic S, Capovilla G, Connolly MB, French J, Guilhoto L, et al. ILAE classification of the epilepsies: position paper of the ILAE commission for classification and terminology. Epilepsia. (2017) 58:512–21. doi: 10.1111/epi.13709
5. Ademuwagun IA, Rotimi SO, Syrbe S, Ajamma YU, Adebiyi E. Voltage gated sodium channel genes in epilepsy: mutations, functional studies, and treatment dimensions. Front Neurol. (2021) 12:600050. doi: 10.3389/fneur.2021.600050
6. Menezes LFS, Sabiá Júnior EF, Tibery DV, Carneiro LDA, Schwartz EF. Epilepsy-related voltage-gated sodium channelopathies: a review. Front Pharmacol. (2020) 11:1276. doi: 10.3389/fphar.2020.01276
7. Scheffer IE, Nabbout R. SCN1A-related phenotypes: epilepsy and beyond. Epilepsia. (2019) 60 Suppl 3:S17–s24. doi: 10.1111/epi.16386
8. Schuchmann S, Schmitz D, Rivera C, Vanhatalo S, Salmen B, Mackie K, et al. Experimental febrile seizures are precipitated by a hyperthermia-induced respiratory alkalosis. Nat Med. (2006) 12:817–23. doi: 10.1038/nm1422
9. Ohmori I, Hayashi K, Wang H, Ouchida M, Fujita N, Inoue T, et al. Inhalation of 10% carbon dioxide rapidly terminates Scn1a mutation-related hyperthermia-induced seizures. Epilepsy Res. (2013) 105:220–4. doi: 10.1016/j.eplepsyres.2013.01.003
10. Shi XY, Hu LY, Liu MJ, Zou LP. Hypercapnia-induced brain acidosis: Effects and putative mechanisms on acute kainate induced seizures. Life Sci. (2017) 176:82–7. doi: 10.1016/j.lfs.2017.03.018
11. Magnotta VA, Heo HY, Dlouhy BJ, Dahdaleh NS, Follmer RL, Thedens DR, et al. Detecting activity-evoked pH changes in human brain. Proc Natl Acad Sci U S A. (2012) 109:8270–3. doi: 10.1073/pnas.1205902109
12. Lindy AS, Stosser MB, Butler E, Downtain-Pickersgill C, Shanmugham A, Retterer K, et al. Diagnostic outcomes for genetic testing of 70 genes in 8565 patients with epilepsy and neurodevelopmental disorders. Epilepsia. (2018) 59:1062–71. doi: 10.1111/epi.14074
13. Kwong AK, Fung CW, Chan SY, Wong VC. Identification of SCN1A and PCDH19 mutations in Chinese children with Dravet syndrome. PLoS ONE. (2012) 7:e41802. doi: 10.1371/journal.pone.0041802
14. Yang XF, Shi XY, Ju J, Zhang WN, Liu YJ Li XY, et al. 5% CO2 inhalation suppresses hyperventilation-induced absence seizures in children. Epilepsy Res. (2014) 108:345–8. doi: 10.1016/j.eplepsyres.2013.11.012
15. Ziemann AE, Schnizler MK, Albert GW, Severson MA, Howard MA III, Welsh MJ, et al. Seizure termination by acidosis depends on ASIC1a. Nat Neurosci. (2008) 11:816–22. doi: 10.1038/nn.2132
16. Chiacchiaretta M, Latifi S, Bramini M, Fadda M, Fassio A, Benfenati F, et al. Neuronal hyperactivity causes Na(+)/H(+) exchanger-induced extracellular acidification at active synapses. J Cell Sci. (2017) 130:1435–49. doi: 10.1242/jcs.198564
17. Mango D, Nisticò R. Neurodegenerative disease: what potential therapeutic role of acid-sensing ion channels? Front Cell Neurosci. (2021) 15:730641. doi: 10.3389/fncel.2021.730641
18. Quade BN, Parker MD, Occhipinti R. The therapeutic importance of acid-base balance. Biochem Pharmacol. (2021) 183:114278. doi: 10.1016/j.bcp.2020.114278
19. Bonnet U, Bingmann D, Leniger T, Scherbaum N, Widman G, Hufnagel A, et al. Valproate acidifies hippocampal CA3-neurons–a novel mode of action. Eu Neuropsychopharmacol: J Eu Coll Neuropsychopharmacol. (2002) 12:279–85. doi: 10.1016/S0924-977X(02)00023-8
20. Leniger T, Wiemann M, Bingmann D, Widman G, Hufnagel A, Bonnet U. Carbonic anhydrase inhibitor sulthiame reduces intracellular pH and epileptiform activity of hippocampal CA3 neurons. Epilepsia. (2002) 43:469–74. doi: 10.1046/j.1528-1157.2002.32601.x
21. Leniger T, Thöne J, Bonnet U, Hufnagel A, Bingmann D, Wiemann M. Levetiracetam inhibits Na+-dependent Cl-/HCO3- exchange of adult hippocampal CA3 neurons from guinea-pigs. Br J Pharmacol. (2004) 142:1073–80. doi: 10.1038/sj.bjp.0705836
22. Bonnet U, Wiemann M. Topiramate decelerates bicarbonate-driven acid-elimination of human neocortical neurons: strategic significance for its antiepileptic, antimigraine and neuroprotective properties. CNS Neurol Disord Drug Targets. (2020) 19:264–75. doi: 10.2174/1871527319666200604173208
23. Leniger T, Thöne J, Wiemann M. Topiramate modulates pH of hippocampal CA3 neurons by combined effects on carbonic anhydrase and Cl-/HCO3- exchange. Br J Pharmacol. (2004) 142:831–42. doi: 10.1038/sj.bjp.0705850
24. Zou LP, Lin Q, Qin J, Cai FC, Liu ZS, Mix E. Evaluation of open-label topiramate as primary or adjunctive therapy in infantile spasms. Clin Neuropharmacol. (2008) 31:86–92. doi: 10.1097/WNF.0b013e3180986d43
25. Yilmaz K, Tatli B, Yaramiş A, Aydinli N, Calişkan M, Ozmen M. Symptomatic and asymptomatic hypohidrosis in children under topiramate treatment. Turk J Pediatr. (2005) 47:359–63.
26. Cerminara C, Seri S, Bombardieri R, Pinci M, Curatolo P. Hypohidrosis during topiramate treatment: a rare and reversible side effect. Pediatr Neurol. (2006) 34:392–4. doi: 10.1016/j.pediatrneurol.2005.10.004
27. Wirrell EC, Nabbout R. Recent Advances in the Drug Treatment of Dravet Syndrome. CNS Drugs. (2019) 33:867–81. doi: 10.1007/s40263-019-00666-8
28. Corbin Bush N, Twombley K, Ahn J, Oliveira C, Arnold S, Maalouf NM, et al. Prevalence and spot urine risk factors for renal stones in children taking topiramate. J Pediatric Urol. (2013) 9(6 Pt A):884–9. doi: 10.1016/j.jpurol.2012.12.005
29. Aframian DJ, Davidowitz T, Benoliel R. The distribution of oral mucosal pH values in healthy saliva secretors. Oral Dis. (2006) 12:420–3. doi: 10.1111/j.1601-0825.2005.01217.x
Keywords: SCN1A, Dravet syndrome, epilepsy, saliva pH, urine pH
Citation: Lu Q, Wang Y-Y, Chen H-M, Wang Q-H, Yang X-Y and Zou L-P (2022) A rise in saliva and urine pH in children with SCN1A-related epilepsy: An exploratory prospective controlled study. Front. Neurol. 13:982050. doi: 10.3389/fneur.2022.982050
Received: 30 June 2022; Accepted: 01 September 2022;
Published: 27 September 2022.
Edited by:
Kette D. Valente, University of São Paulo, BrazilReviewed by:
Silvia Vincentiis, University of São Paulo, BrazilCopyright © 2022 Lu, Wang, Chen, Wang, Yang and Zou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Li-Ping Zou, em91bGlwaW5nMjFAaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.