
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 30 June 2022
Sec. Endovascular and Interventional Neurology
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.925159
 David Hernández1
David Hernández1 Elena Serrano2
Elena Serrano2 Gemma Molins3Federico Zarco2
Gemma Molins3Federico Zarco2 Oscar Chirife4
Oscar Chirife4 Mariano Werner5Blanca Lara4
Mariano Werner5Blanca Lara4 Anna Ramos5
Anna Ramos5 Laura Llull2
Laura Llull2 Manuel Requena1Marta de Dios las Cuevas4
Manuel Requena1Marta de Dios las Cuevas4 Sebastián Remollo5Carlos Piñana1
Sebastián Remollo5Carlos Piñana1 Antonio López-Rueda2*
Antonio López-Rueda2*The purpose of this study is to evaluate the best endovascular approach (aspiration or stent-retriever) and the impact of stent retriever size and length on clinical and angiographic outcomes in patients with acute intracranial ICA occlusion. We conducted a retrospective analysis of a prospective database of consecutive patients with acute intracranial ICA occlusion undergoing endovascular treatment in four Comprehensive Stroke Center between June-2019 and December-2020. We include 121 patients; Stent-retriever (SR) was used as first technical approach in 107 patients (88.4%) and aspiration was used in 14 patients (11.6%). SR group had higher rate of FPE compared to aspiration group (29 vs. 0%, p = 0.02). In SR subgroup, treatment highlighted higher FPE in the 6 × 50 SR (37.7%), than in the rest of the SR which are 21.2% (4–5 mm size and 20–50 mm length SR) and 19% (6 mm size and 25–40 mm length SR), but it was not found to be statistically significant. There were no other significant differences across the groups regarding primary angiographic or clinical outcomes. In our intracranial ICA occlusion series, stent retrievers were superior to direct aspiration in obtaining FPEs and mFPEs, and longer devices achieved better results with no statistically significant difference. Further studies evaluating the effects of different ICA clot removal approaches are warranted to confirm these results.
Acute ischemic stroke (AIS) is a complex disease encompassing multiple subtypes with different underlying pathologies. Acute occlusion of the internal carotid artery (ICA) is one of the most devastating events, with an incidence of 6–15% in patients with AIS (1). Patient outcomes are poor with only 2–12% achieving good recovery, 40–69% experiencing permanent severe neurological deficits, and 16–55% dying from AIS (2). Recanalization rates after intravenous (IV) and intra-arterial (IA) therapy ranged from 4.4 to 12.5% and from 62 to 63%, respectively. The high clot burden and limited delivery of recombinant tissue plasminogen activator (rt-PA) to intracranial occlusions may explain the poor prognosis (3, 4).
Complete revascularization from a single thrombectomy device pass, known as the first-pass effect (FPE), is associated with higher rates of good clinical outcomes. Usually, it is less likely to be achieved in internal carotid artery terminal occlusion (5). There is no consensus on the most effective endovascular technique for the treatment of acute intracranial ICA occlusion, aspiration did not demonstrate higher recanalization rates compared to stent-retriever in the anterior circulation occlusions (6–9). This study aimed to evaluate the best endovascular approach (aspiration or stent retriever) and the impact of stent retriever size and length on clinical and angiographic outcomes in patients with acute intracranial ICA occlusion.
We conducted a retrospective analysis of a prospective database of consecutive patients with acute intracranial ICA occlusion undergoing endovascular treatment at four comprehensive stroke centers between June 2019 and December 2020. All participating centers received institutional review board approval from their respective institutions and patients or representatives and signed informed consent for the endovascular procedure and data analysis.
The inclusion criteria were patients aged ≥18 years, acute intracranial ICA occlusion confirmed on digital subtraction angiography, time from last seen well to treatment up to 24 h, baseline National Institutes of Health Stroke Scale (NIHSS) score ≥2, and premorbid modified Rankin Scale (mRS) score ≤ 3. Exclusion criteria include patients without available data to demonstrate efficacy or safety variables. No other exclusion criteria were addressed.
The patient demographics included age and sex. Clinical and radiological data included previous modified Rankin scale (mRS), National Institutes of Health Stroke Scale (NIHSS) score, administration of intravenous thrombolysis with rt-PA, presence of tandem extracranial lesions, laterality, and evidence of early ischemic changes on non-enhanced computed tomography (NECT) with ASPECTS (Alberta Stroke Program Early CT Score).
Procedural data included the time from last seen well to the groin puncture, first intracranial series, and final revascularization series. The type of anesthesia (local, sedation, or general), ICA recanalization after the first pass, number of passes to carotid recanalization, and final ICA recanalization were analyzed. Intracranially, the modified thrombolysis in cerebral infarction (mTICI) score after the first pass, the final number of passes, and the mTICI final score were collected. The primary angiographic outcomes were the rate of ICA recanalization after the first pass, first-pass effect (FPE) (defined as mTICI ≥2c, achieved after the first attempt), and modified first-pass effect (mFPE) (defined as mTICI ≥2b, achieved after the first attempt). The mTICI score, FPE and mFPE results are related to MCA territory.
Procedure-related complications such as distal embolism, arterial perforation (defined as angiographic contrast extravasation that occurred during the procedure), or arterial dissection (described as the presence of an intimal flap on the control angiogram obtained after thrombectomy) were also documented.
Regarding the technical approach, angioplasty and/or carotid stent placement in tandem occlusions as well as antiplatelet management, the use of balloon guide catheter (BGC), intermediate catheter, and stent retriever (size and length) were up to the treating neurointerventionalist' choice and were recorded, as well as the change to other material during the procedure. The use of stentriever with or without intermediate catheter were also up to the treating neurointerventionalist' choice. The aspiration technique was performed with large bore catheters and manual aspiration in the vast majority of patients.
The primary clinical outcome was the mRS score at 90 days post-procedure, and a favorable outcome was defined as an mRS score from 0 to 2. Safety evaluations included assessment of the NIHSS score at 24 h and the presence of symptomatic intracranial hemorrhage (defined as a documented hemorrhage associated with a decline of four or more points in the NIHSS score).
Descriptive analyses included frequencies and percentages for categorical variables and means [standard deviations (SDs)] or medians [interquartile ranges (IQRs)] for continuous variables. Endovascular approaches were dichotomized into aspiration or stent-retriever thrombectomy, and trichotomized in the stent-retriever group according to the size and length of the device. Primary angiographic and clinical outcomes were compared between different endovascular approaches. Student's t-test or Wilcoxon's rank-sum test for continuous variables and the chi-squared (χ2) test or Fisher's exact test for categorical variables were performed using the Statistical Package for the Social Sciences (SPSS) software for Windows version 20.0 (IBM SPSS, SPSS Inc., Chicago, Illinois, USA). Statistical significance was set at p <0.05.
We included 121 patients from four comprehensive stroke centers between June 2019 and December 2020. We did not exclude any patients because of the lack of available data. The demographic, clinical, radiological, procedural, and clinical outcome data are summarized in Table 1. Regarding procedural safety variables, 23 patients (19%) experienced complications during the procedure. Sixteen patients (13.2%) had a distal embolism to the anterior or middle cerebral artery, five patients (4.1%) experienced arterial perforation during the procedure, and two patients (1.7%) presented with dissection of the internal carotid artery during the endovascular treatment.
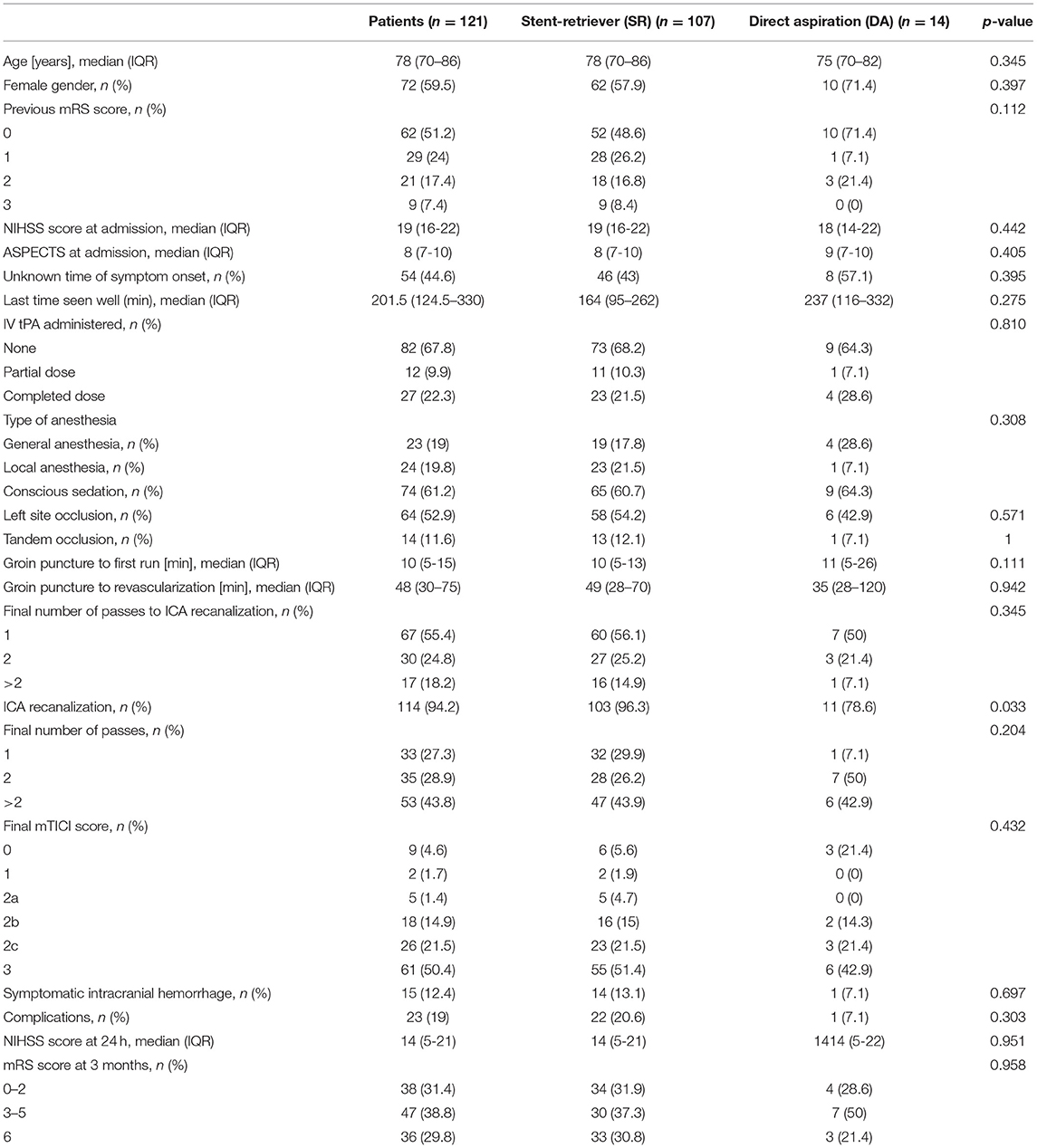
Table 1. Demographic, clinical, radiological, and procedural data.
Regarding the technical approach, a BGC was used in 45 patients (37.2%), an intermediate catheter in 108 patients (89.3%), and a stent retriever in 107 patients (88.4%). Direct aspiration (DA) was used as the first technical approach in 14 patients (11.6%) and a stent retriever (SR) was used in the remaining patients. Out of the 107 remaining patients in whom the stent retriever was used (88.4%), in 53 patients (43.8%), a 6 × 50 stent retriever was the one of choice; in 21 patients (17.4%) a 6 mm diameter and 25–40 mm long stent-retriever size was used; in 33 patients (27.3%) a 4–5 mm stent-retriever size was used.
The primary endovascular and clinical outcomes related to the endovascular approach are summarized in Tables 2, 3, respectively. Stent-retriever group had higher rate of FPE compared to aspiration group (29 vs. 0%, p = 0.02). There was no statistically significant difference regarding demographic, radiological and clinical data between stentretriever and direct aspiration groups.

Table 2. Primary endovascular and clinical outcomes related to the endovascular approach.

Table 3. Primary endovascular and clinical outcomes related to the stent-retriever size and length.
There were no other significant differences across the groups regarding primary angiographic or clinical outcomes. Our subgroup analysis of SR treatment highlighted higher FPE in the 6 × 50 SR (37.7%), than in the rest of the SR which are 21.2% (4–5 mm size and 20–50 mm length SR) and 19% (6 mm size and 25–40 mm length SR), but it was not found to be statistically significant. There was no statistically significant association between technical approaches and procedural safety variables.
This study included 121 patients with acute intracranial ICA occlusion treated with either an SR or DA. The rate of successful recanalization of the ICA occlusion after the first pass was 25.6%. A previous systematic review and meta-analysis demonstrated similar success rates, with a mean of 26.2% (10). We found a clear superiority in obtaining an FPE using SR compared to DA in out cohort. Additionally, the data suggest that higher success rates are associated with larger stent retrievers.
Only three studies have compared SR and DA in distal ICA occlusions; two of them demonstrated the superiority of SR (11, 12), whereas the third study revealed that DA is superior to SR if BGC was not used (13). Our data showed the superiority of SR over DA (FPE 29 vs. 0%; p = 0.020). One possible explanation for these results is that carotid terminus occlusions have larger thrombus burdens and distal aspiration catheters may not have the optimal size for the vessel diameter, which can be 3.6 ± 0.4 mm at the ICA terminus and 5 ± 0.6 mm at the cavernous segment (14). New large-bore aspiration catheters with a larger inner diameter (≥0.072 mm) (15) attempt to mitigate this issue. Another reason may be that the aspiration catheter must align perfectly with the thrombus, which may be difficult in tortuous anatomy.
In intracranial occlusions of the ICA, the thrombus may extend into the anterior cerebral artery or middle cerebral artery. If the total length of the thrombus is unknown, a longer device allows more segments to be covered with a lower chance of losing the target site. Additionally, this modification allows for a greater device/thrombus interaction, and the larger diameter maintains greater entrapment during clot traction (16). As a result, there is a greater chance of FPE and a reduction of embolisms to new territories.
Our subgroup analysis of SR treatment highlighted higher FPE and mFPE in the 6 × 50 SR (37.7 and 45.3%, respectively) than in the rest of the SR, but it was not found to be statistically significant. We believe that the failure to show significance was due to the small sample size. Previous comparisons between 4- and 6- mm diameter Solitaire stent retrievers also did not find differences in treatments for ICA occlusions, but they did not evaluate FPE and only focused on reperfusion TICI ≥ 2b or TICI ≥ 2c (17). Similarly, in the Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke (STRATIS) Registry, the SR diameter did not significantly affect the results of ICA recanalization (18).
Our results highlight a significant difference in the mFPE as fixed 6 mm diameter stents with the longest length were the most effective (45.3% in >50 mm and 19% in <50 mm; p = 0.037). These results are in accordance with previous literature, where length was the most important parameter in both in vitro studies of fibrin-rich clots (19), in vivo studies, and registries (18, 20).
In our multicenter study, a BGC was only used in 37.2% of cases. A recent systematic review showed benefits in the use of BGC with DA and SR but not with the combined technique (21), although data from the ASTER2 trial results suggest better efficacy in distal ICA occlusion when the combined approach is performed with BGC (22).
Our study has some limitations, as procedural outcomes were reported by neurointerventionalists without an independent core lab, which can lead to a reporter bias. There is also a lack of statistical power regarding the type of ICA occlusion that correlates with different collateral flow patterns and subsequent clinical outcomes (23, 24). We have not reported other etiologies either, except tandem occlusion, since it has been difficult to define whether it is reliable given the retrospective nature of the study. This study has other limitations, including the fact that it was a retrospective analysis and a multicentric study involving different procedural methodologies that might have influenced the results. For example, the low use of BGC might have an influence on the low rate of FPE. However, having different neuroendovascular approaches more realistically simulates the preferences of different neurointerventionalists, mirroring the real procedural practice. Likewise, it is an important limitation that the sample is unbalanced between stentriever and direct aspiration groups.
Since the most effective endovascular treatment is still unknown, future studies should include a larger number of patients as well as other possible technical approaches to recanalize an ICA occlusion, such as the use of the double-stent retriever technique or the association of BGC, larger-bore distal aspiration catheters, and the stent retriever.
In our intracranial ICA occlusion series, stent retrievers were superior to direct aspiration in obtaining FPEs and mFPEs, and longer devices achieved better results. A trend toward FPE was observed when using the 6 × 50 stent retriever. Further studies evaluating the effects of different ICA clot removal approaches are warranted to confirm these results.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité de Ética de la Investigación con medicamentos del Hospital Clinic de Barcelona (HCB/2020/1422). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
DH, ES, OC, MW, and AL-R: conceived and designed the analysis, collected the data, contributed data or analysis tools, performed the analysis, and wrote the paper. GM and FZ: conceived and designed the analysis, contributed data or analysis tools, performed the analysis, and critical review of the manuscript with intellectually relevant contributions. BL, AR, LL, MC, SR, and CP: collected the data, contributed data or analysis tools, performed the analysis, and critical review of the manuscript with intellectually relevant contributions. MR: collected the data, contributed data or analysis tools, performed the analysis, and wrote the paper. All authors have reviewed and approved the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the Cátedra de Neurorradiología Intervencionista, Universidad de Santiago de Compostela for their kind support.
1. Rubiera M, Ribo M, Delgado-Mederos R, Santamarina E, Delgado P, Montaner J, et al. Tandem internal carotid artery/middle cerebral artery occlusion: an independent predictor of poor outcome after systemic thrombolysis. Stroke. (2006) 37:2301–5. doi: 10.1161/01.STR.0000237070.80133.1d
2. Meyer FB, Sundt TM, Piepgras DG, Sandok BA, Forbes G. Emergency carotid endarterectomy for patients with acute carotid occlusion and profound neurological deficits. Ann Surg. (1986) 203:82–9. doi: 10.1097/00000658-198601000-00014
3. Endo S, Kuwayama N, Hirashima Y, Akai T, Nishijima M, Takaku A. Results of urgent thrombolysis in patients with major stroke and atherothrombotic occlusion of the cervical internal carotid artery. Am J Neuroradiol. (1998) 19:1169–75.
4. Zaidat OO, Suarez JI, Santillan C, Sunshine JL, Tarr RW, Paras VH, et al. Response to intra-arterial and combined intravenous and intra-arterial thrombolytic therapy in patients with distal internal carotid artery occlusion. Stroke. (2002) 33:1821–6. doi: 10.1161/01.STR.0000020363.23725.67
5. Zaidat OO, Castonguay AC, Linfante I, Gupta R, Martin CO, Holloway WE, et al. First pass effect: a new measure for stroke thrombectomy devices. Stroke. (2018) 49:660–6. doi: 10.1161/STROKEAHA.117.020315
6. Bernsen MLE, Goldhoorn RB, van Oostenbrugge RJ, van Zwam WH, Uyttenboogaart M, Roos YBWE, et al. Equal performance of aspiration and stent retriever thrombectomy in daily stroke treatment. J Neurointerv Surg. (2019) 11:631–6. doi: 10.1136/neurintsurg-2018-014270
7. Boulanger M, Lapergue B, Turjman F, Touzé E, Anxionnat R, Bracard S, et al. First-line contact aspiration vs stent-retriever thrombectomy in acute ischemic stroke patients with large-artery occlusion in the anterior circulation: systematic review and meta-analysis. Interv Neuroradiol. (2019) 25:244–53. doi: 10.1177/1591019918821074
8. Zhang X, Guo X, Yi Y, Cheng C, Liang A, Pu D, et al. First-line contact aspiration vs stent retriever for proximal occlusion in acute ischemic stroke: a systemic review and meta-analysis. J Stroke Cerebrovasc Dis. (2020) 29:105374. doi: 10.1016/j.jstrokecerebrovasdis.2020.105374
9. Texakalidis P, Giannopoulos S, Karasavvidis T, Rangel-Castilla L, Rivet DJ, Reavey-Cantwell J. Mechanical thrombectomy in acute ischemic stroke: a meta-analysis of stent retrievers vs direct aspiration vs a combined approach. Neurosurgery. (2020) 86:464–77. doi: 10.1093/neuros/nyz258
10. Bai X, Zhang X, Wang J, Zhang Y, Dmytriw AA, Wang T, et al. Factors influencing recanalization after mechanical thrombectomy with first-pass effect for acute ischemic stroke: a systematic review and meta-analysis. Front Neurol. (2021) 12:628523. doi: 10.3389/fneur.2021.628523
11. Diana F, Vinci SL, Ruggiero M, Semeraro V, Bracco S, Frauenfelder G, et al. Comparison of aspiration versus combined technique as first-line approach in terminal internal carotid artery occlusion: a multicenter experience. J Neurointerv Surg. (2022) 14:666–71. doi: 10.1136/neurintsurg-2021-017585
12. Brehm A, Maus V, Tsogkas I, Colla R, Hesse AC, Gera RG, et al. Stent-retriever assisted vacuum-locked extraction (SAVE) versus a direct aspiration first pass technique (ADAPT) for acute stroke: data from the real-world. BMC Neurol. (2019) 19:65. doi: 10.1186/s12883-019-1291-9
13. Xing PF, Yang PF Li ZF, Zhang L, Shen HJ, Zhang YX, et al. Comparison of aspiration versus stent retriever thrombectomy as the preferred strategy for patients with acute terminal internal carotid artery occlusion: a propensity score matching analysis. Am J Neuroradiol. (2020) 41:469–76. doi: 10.3174/ajnr.A6414
14. Rai AT, Hogg JP, Cline B, Hobbs G. Cerebrovascular geometry in the anterior circulation: an analysis of diameter, length and the vessel taper. J Neurointerv Surg. (2013) 5:371–5. doi: 10.1136/neurintsurg-2012-010314
15. Romano DG, Frauenfelder G, Diana F, Saponiero R. JET. 7 catheter for direct aspiration in carotid T occlusions: preliminary experience and literature review. Radiol Med. (2022) 127:330–40. doi: 10.1007/s11547-022-01451-2
16. Machi P, Jourdan F, Ambard D, Reynaud C, Lobotesis K, Sanchez M, et al. Experimental evaluation of stent retrievers' mechanical properties and effectiveness. J Neurointerv Surg. (2017) 9:257–63. doi: 10.1136/neurintsurg-2015-012213
17. Yang D, Hao Y, Zi W, Wang H, Zheng D, Li H, et al. Effect of retrievable stent size on endovascular treatment of acute ischemic stroke: a multicenter study. Am J Neuroradiol. (2017) 38:1586–93. doi: 10.3174/ajnr.A5232
18. Zaidat OO, Haussen DC, Hassan AE, Jadhav AP, Mehta BP, Mokin M, et al. Impact of stent retriever size on clinical and angiographic outcomes in the STRATIS Stroke Thrombectomy Registry. Stroke. (2019) 50:441–7. doi: 10.1161/STROKEAHA.118.022987
19. Girdhar G, Epstein E, Nguyen K, Gregg C, Kumar T, Wainwright J, et al. Longer 6-mm diameter stent retrievers are effective for achieving higher first pass success with fibrin-rich clots. Interv Neurol. (2020) 8:187–95. doi: 10.1159/000499974
20. Haussen DC, Al-Bayati AR, Grossberg JA, Bouslama M, Barreira C, Bianchi N, et al. Longer stent retrievers enhance thrombectomy performance in acute stroke. J Neurointerv Surg. (2019) 11:6–8. doi: 10.1136/neurintsurg-2018-013918
21. Podlasek A, Dhillon PS, Jewett G, Shahein A, Goyal M, Almekhlafi M. Clinical and procedural outcomes with or without balloon guide catheters during endovascular thrombectomy in acute ischemic stroke: a systematic review and meta-analysis with first-line technique subgroup analysis. Am J Neuroradiol. (2021) 42:1464–71. doi: 10.3174/ajnr.A7164
22. Lapergue B, Blanc R, Costalat V, Desal H, Saleme S, Spelle L, et al. Effect of thrombectomy with combined contact aspiration and stent retriever vs stent retriever alone on revascularization in patients with acute ischemic stroke and large vessel occlusion: the ASTER2 Randomized Clinical Trial. JAMA. (2021) 326:1158–69. doi: 10.1001/jama.2021.13827
23. Liebeskind DS, Flint AC, Budzik RF, Xiang B, Smith WS, Duckwiler GR, et al. Carotid I's, L's and T's: collaterals shape the outcome of intracranial carotid occlusion in acute ischemic stroke. J Neurointerv Surg. (2015) 7:402–7. doi: 10.1136/neurintsurg-2014-011231
24. Bradac GB, Venturi F, Bosco G, Garabello D, Coriasco M, Stura G, et al. Acute occlusion of the distal internal carotid artery : single center experience in 46 consecutive cases, review of the literature and proposal of a classification. Clin Neuroradiol. (2020) 30:67–76. doi: 10.1007/s00062-018-0743-8
Keywords: stent retriever, thrombectomy, internal carotid artery occlusion, revascularization, endovascular
Citation: Hernández D, Serrano E, Molins G, Zarco F, Chirife O, Werner M, Lara B, Ramos A, Llull L, Requena M, Cuevas MdDl, Remollo S, Piñana C and López-Rueda A (2022) Comparison of First-Pass Effect in Aspiration vs. Stent-Retriever for Acute Intracranial ICA Occlusion. Front. Neurol. 13:925159. doi: 10.3389/fneur.2022.925159
Received: 21 April 2022; Accepted: 09 June 2022;
Published: 30 June 2022.
Edited by:
José Manuel Pumar, University of Santiago de Compostela, SpainReviewed by:
Edgar a Samaniego, The University of Iowa, United StatesCopyright © 2022 Hernández, Serrano, Molins, Zarco, Chirife, Werner, Lara, Ramos, Llull, Requena, Cuevas, Remollo, Piñana and López-Rueda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio López-Rueda, YWxydWVkYTgxQGhvdG1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.