 Dandan Zhang
Dandan Zhang Siyuan Chen†
Siyuan Chen† Xiaopeng Chen
Xiaopeng Chen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 22 July 2022
Sec. Dementia and Neurodegenerative Diseases
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.922535
Alzheimer's disease and epilepsy are common nervous system diseases in older adults, and their incidence rates tend to increase with age. Patients with mild cognitive impairment and Alzheimer's disease are more prone to have seizures. In patients older than 65 years, neurodegenerative conditions accounted for ~10% of all late-onset epilepsy cases, most of which are Alzheimer's disease. Epilepsy and seizure can occur in the early and late stages of Alzheimer's disease, leading to functional deterioration and behavioral alterations. Seizures promote amyloid-β and tau deposits, leading to neurodegenerative processes. Thus, there is a bi-directional association between Alzheimer's disease and epilepsy. Epilepsy is a risk factor for Alzheimer's disease and, in turn, Alzheimer's disease is an independent risk factor for developing epilepsy in old age. Many studies have evaluated the shared pathogenesis and clinical relevance of Alzheimer's disease and epilepsy. In this review, we discuss the clinical associations between Alzheimer's disease and epilepsy, including their incidence, clinical features, and electroencephalogram abnormalities. Clinical studies of the two disorders in recent years are summarized, and new antiepileptic drugs used for treating Alzheimer's disease are reviewed.
Alzheimer's disease (AD) and epilepsy are common nervous system diseases in older adults, and their incidence rates tend to increase with age. Epilepsy is approximately three times more common in individuals aged 65 years and older (1). Patients with mild cognitive impairment (MCI) and AD are more prone to have seizures (2). Specifically, the incidence of hippocampus-related degenerative diseases, such as AD and temporal lobe epilepsy (TLE), is increasing, partly because the hippocampus is susceptible to toxic substances such as excitatory amino acids, resulting in neuronal dysfunction, cognitive impairment, and death (3). Late-onset epilepsy is mostly secondary to brain diseases such as stroke, tumor, and neurodegenerative diseases, and many of them are of unknown etiology (4). In patients older than 65 years, neurodegenerative conditions accounted for ~10% of all late-onset epilepsy cases, most of which are AD (5). Epilepsy and seizure can occur in the early and late stages of AD, leading to functional deterioration and behavioral alterations (2). Evidence from both experimental and human studies has proven the existence of an association between epilepsy and AD (6). Transgenic mouse models with simulate familial AD can develop spontaneous epilepsy (7). Furthermore, seizures can lead to cognitive deficits, the trajectory of cognitive changes in patients with TLE differs from the pattern observed in healthy aging. Seizures also promote amyloid-β and tau deposits, leading to neurodegenerative processes (8). Thus, there is a bi-directional association between AD and epilepsy. Epilepsy is a risk factor for AD and, in turn, AD is an independent risk factor for developing epilepsy in old age (9). Many studies have evaluated the shared pathogenesis and clinical relevance of AD and epilepsy (5, 10, 11). In this review, we discuss the clinical associations between AD and epilepsy, including their incidence, clinical features, and electroencephalogram (EEG) abnormalities. Clinical studies of the two disorders in recent years are summarized (Table 1), and new antiepileptic drugs used for treating AD are reviewed.
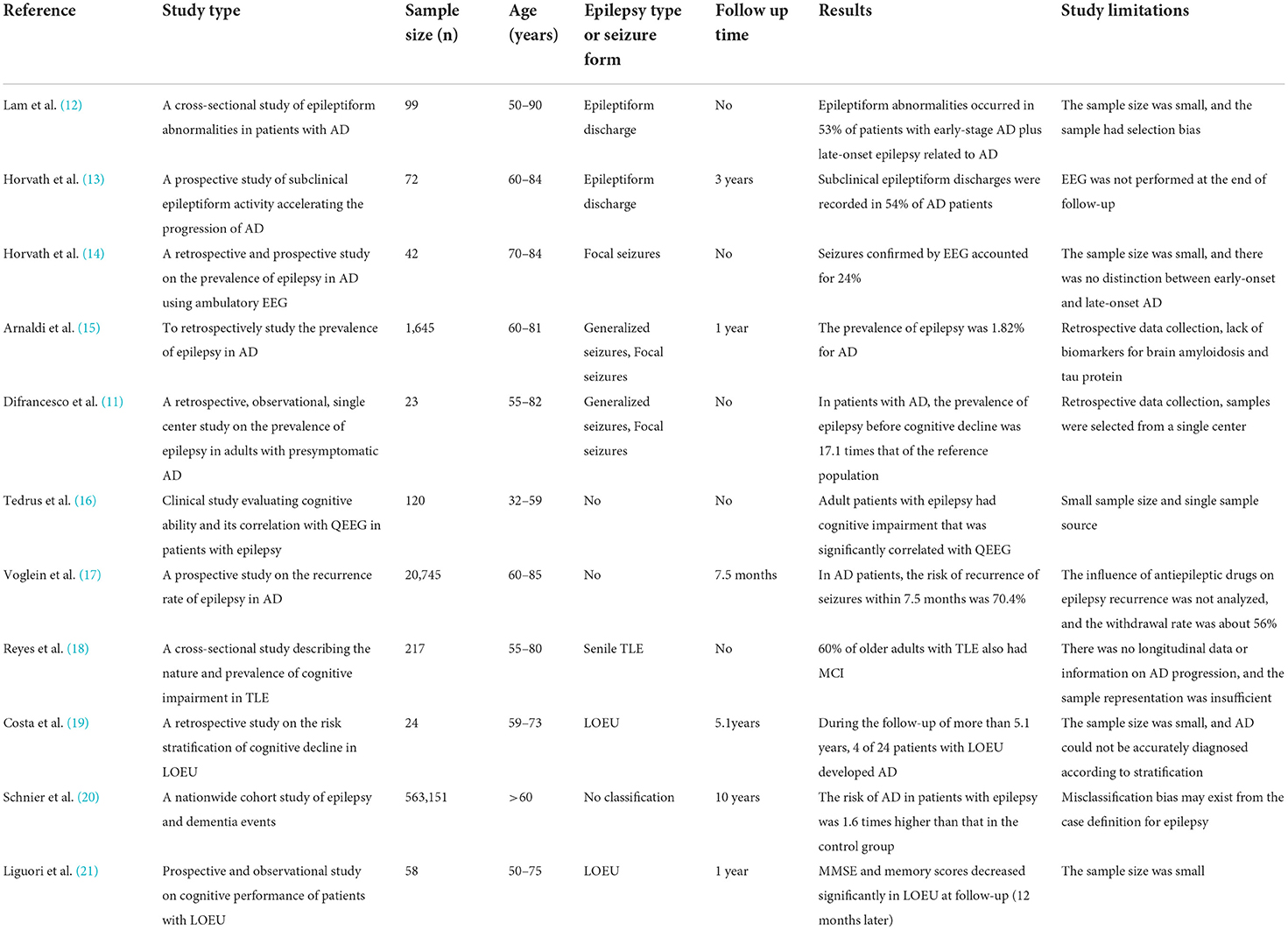
Table 1. Summary of clinical studies of AD and epilepsy.
The hippocampus shows similar pathological changes in patients with AD and individuals with epilepsy, such as loss of granulosa cells in the dentate gyrus, circuit reorganization, and damage to hippocampal neurons (22). The main pathological features of AD are amyloid β (Aβ) deposition outside neural cells and accumulation of hyperphosphorylated tau-protein in neurofibrillary tangles (23). These pathologies have also been observed in patients with TLE (24). In a study of 101 patients with TLE (aged 30–61 years) who underwent temporal lobectomy, 10 patients had Aβ plaques in brain samples (25). Tai et al. (26) performed pathological examinations on tissues from 33 patients aged 50–65 years who underwent temporal lobectomy for drug resistant TLE and found that 31 of the 33 patients (94%) had hyperphosphorylated tau. Hyperexcitability of nervous tissue is primarily responsible for increased seizure (27). Network hyperexcitability which induced by intracellular Aβ oligomers can occur in the early stages of AD and contribute to cognitive decline (28, 29). Recent studies have shown that presenilin 2 (PSEN2) knockout mice demonstrated early-life reductions in seizure threshold, and patients with PSEN gene variants also reported seizures (30). Furthermore, the increased tau pathology was associated with a greater decline in language learning, recall, and graded naming test scores (31). In patients with epilepsy, neurodegeneration occurs in the hippocampus, the temporal cortex, and the amygdala, with hippocampal sclerosis being the most characteristic structural change (32). Hippocampal sclerosis can cause neuronal loss and disruption of the balance between excitatory and inhibitory signaling in the sclerotic area, resulting in highly synchronous abnormal neuronal discharge (33). The hippocampus is an important part of the limbic system that plays a central role in memory function and is a site of early neurofibrillary tangle development (34). Therefore, pathological changes in the hippocampus may represent a link between AD and epilepsy.
Other neurochemical changes associated with both AD and epilepsy include GABAergic (35) and glutamatergic alterations (36), Aβ and tau protein deposition (37), neuroinflammation (10), and damage to the noradrenergic nervous system in the locus coeruleus (38) (Figure 1).
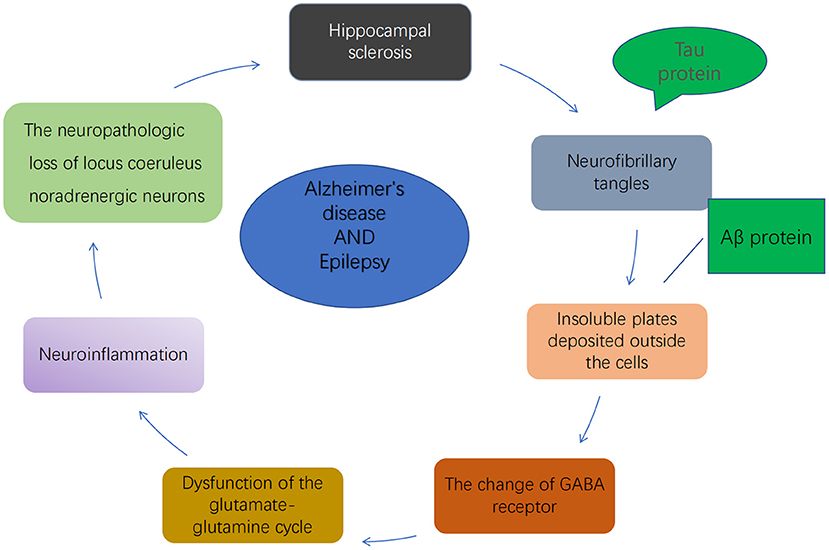
Figure 1. Possible mechanisms of AD and epilepsy association.
AD is an important cause of senile epilepsy. Increased AD duration is associated with a higher risk of epilepsy (39). In addition, the risk of epilepsy in patients with AD is 10 times higher than that of individuals without AD in people over the age of 65 years (40). Horvath et al. (13) conducted a 3-year prospective follow-up study that included yearly cognitive assessments on 38 patients with AD and 20 healthy individuals and found that subclinical epileptiform discharges were recorded more frequently in patients with AD (54%) than in healthy, elderly (25%) individuals. Subclinical epileptiform activity was also observed in patients with amnestic mild cognitive impairment (aMCI) or early AD (28). Patients with familial early-onset AD have a higher risk of having seizures (41). Haoudy et al. (42) studied 25 patients with early onset AD and positive cerebrospinal fluid AD biomarkers. Based on epilepsy expert consultation and EEG examination, the results showed that 10 (40%) of these patients had epilepsy.
Epilepsy may play a causal role in AD development. In some cases, seizures may begin concurrently with onset of cognitive decline or even precede onset of AD (28). In AD patients, increased susceptibility to seizures and silent epileptiform activity due to disruption of the excitatory /inhibitory balance occur much earlier than cognitive impairment. The increase of epileptiform activity may be the main pathology in the early stage, which directly contributes to cognitive impairment (43). In a postmortem study (44), chronic epilepsy was associated with increased tau neurofibrillary tangles at mid-braak stages in patients aged 40–65 years. AD is a chronic, progressive disease that includes MCI and aMCI. Because the typical symptoms of AD may occur only after repeated seizures for several years, increasing numbers of studies have evaluated cognition in epilepsy. In one study (19), 13 out of 24 patients with late onset epilepsy of unknown etiology (LOEU) who were followed for 5.1 years had MCI. Most LOEU patients had an MCI status during seizures (59%) (45). The use of various antiepileptic drugs in the successful treatment of cognitive impairment in patients with AD provides an additional link between epilepsy and AD (46).
In the UK, the prevalence of AD among patients with epilepsy is about 8% (47). In a population-based prospective study of seizures in adults aged > 17 years, Forsgren et al. (48) collected data of 563 patients with possible seizures in 34 months and found that seven cases were caused by AD (incidence 4%). In a cohort of 177 patients with newly diagnosed clinically with probable AD, 12 (6.8%) had a history of epilepsy and/or were using antiepileptic drugs at the time of diagnosis (49). Studies (50) have shown that 11% of adult patients with seizures suffer from AD. In a 10-year follow-up study, the 10-year cumulative incidence of dementia (including AD, vascular dementia) in patients with LOEU was 22% (51). To assess the relationship between epilepsy and dementia (including AD, vascular dementia) risk in Taiwan, Tsai et al. (52) conducted a retrospective cohort study that included 675 patients (age, ≥50 years) with epilepsy and 2,025 age-matched control subjects. Their results showed that individuals in the epilepsy cohort were at significantly increased risk of dementia compared with individuals in the control cohort. The risk of dementia in patients with epilepsy was also evaluated in the Framingham Heart Study (53). The study included follow-up information for 4,906 participants with epilepsy over the age of 65 years, and identified 51 cases of sporadic dementia (84% with AD type) in 43 patients with epilepsy and 129 controls without epilepsy. A study (54) of 247 untreated patients with newly diagnosed epilepsy showed that 49.4% of patients had impaired attention and executive function, and 47.8% had memory impairment.
Patients with epilepsy, especially late-onset epilepsy, often have cognitive impairment. Most seizure-related cognitive problems are affected by a variety of interrelated factors, including early age of seizure onset, seizure frequency, intensity and duration, and antiepileptic drug treatment (55). For example, patients diagnosed with LOEU show a significant decline in cognitive ability, unrelated to antiepileptic drug treatment, 12 months after diagnosis (21). In a study that assessed 38 elderly adults with epilepsy and 29 healthy controls, a comprehensive neuropsychological battery showed that the group with epilepsy had lower Mini-Mental State Examination (MMSE) and Dementia Rating Scale (DRS) total scores, performed worse on the attention and memory subscales of the DRS, and had poorer composite domain scores for verbal memory, visual memory, executive function, language, and processing speed when compared with controls (56). Wang et al. (57) studied 257 adult patients with epilepsy and observed that the overall cognitive function of patients with epilepsy was lower than the reference range for the Montreal Cognitive Assessment (MoCA) and clinical memory scale. Reyes et al. (18) studied 71 patients with TLE, 77 patients with aMCI, and 69 healthy controls. They found that 43 patients with TLE (60%) met the TLE-MCI standard and showed obvious memory and language defects. Subgroup analysis by age of seizure onset revealed that 63% of patients with early seizure onset (<50 years old) and 56% of patients with late seizure onset (≥50 years old) met the TLE-MCI standard. Patients with TLE-MCI showed greater language defects, while patients with aMCI forgot information more rapidly. Taylor et al. (58) found that memory and psychomotor speed were the most affected areas of cognitive function in patients with epilepsy.
Memory, processing speed, and higher executive function are the cognitive functions most prone to change within 12 months in newly diagnosed patients with epilepsy (59). For examples, when patterns of cortical atrophy and cognitive impairment were analyzed in 73 elderly patients with TLE (>55 years), 79 patients with aMCI, and 70 healthy controls were studied (60), results showed that the elderly patients with TLE exhibited medial temporal lobe atrophy similar to that observed in patients with aMCI. The TLE and aMCI groups also showed significant memory and language impairment when compared to the healthy control group. The association between medial temporal lobe atrophy and cognitive impairment in elderly people with TLE and aMCI demonstrates the risk of cognitive impairment associated with epilepsy. Johnson et al. (61) studied the relationship between late-onset epilepsy (LOE) and changes in cognitive ability over a 25 year period and found that LOE was associated with rapid declines in cognition, verbal memory, executive function, and word fluency.
Interictal epileptic discharge (IED) are the EEG signs of epilepsies between seizures (62). Some cognitive loss might evolve in some epilepsies and patients if many and long term (63). Interictal activity results in significant changes in cognitive function, especially learning and memory (64). In patients with long-term TLE, the occurrence of IED is strongly related to cognitive impairment, and the most obvious is frontal lobe function (65). Liu et al. (62) performed EEG examinations and global cognitive assessments on 167 adult patients with and without epilepsy and showed that verbal fluency and language scores were reduced in patients with IED. They also found that sleep-phase IEDs were associated with lower cognitive performance. Interictal spike, especially if frequent and extensive, can impair cognitive abilities through interference with waking learning and memory, as well as memory consolidation, during sleep (66).
Moreover, Ung et al. (67) found that interictal epileptic activity outside the left hemispheric seizure onset zone impacted memory encoding, recall, and retrieval, while those inside the seizure onset zone did not. Hippocampal interictal epileptiform activity disrupted memory maintenance and retrieval, but not encoding cognition in humans (68). Horak et al. (69) also collected data of 80 patients with epilepsy who participated in the delayed free recall task while undergoing intracranial EEG monitoring and found that IED in the inferior-temporal, medial-temporal, and parietal areas significantly affected memory.
Frequent seizures can reduce the power and frequency of theta waves (70). Quantitative EEG (QEEG) can be used to objectively evaluate the power of radio waves that reflect cognition. The association between epilepsy and QEEG was studied in 80 adult patients with epilepsy and 40 healthy controls. The results showed that adult patients with epilepsy had cognitive impairment that significantly correlated with QEEG changes. Thus, QEEG may aid in understanding the pathophysiology of epilepsy and serve as an early marker of the cognitive changes that occur in epilepsy (16). Further evidence of the association between QEEG and cognitive changes in epilepsy is provided by Elsherif et al. (71), who administered cognitive tests and performed QEEG evaluation of EEG markers (median frequency, peak frequency, and alpha-to-theta ratio) in 45 patients with TLE. Researchers showed a strong negative correlation between cognition in patients with TLE and measured EEG markers. Thus, QEEG of these three EEG markers may be used to identify early cognitive impairment in patients with epilepsy.
Epidemiological data on epilepsy in AD is limited, likely because neurodegeneration begins a few years prior to the emergence of clinical symptoms, and epilepsy may have been present in the pre-symptomatic stage of AD (15). The estimated prevalence of epilepsy in patients with dementia (including AD, vascular dementia, Lewy body disease) is about 5% (72). However, a recent prospective cohort study (73) with large sample size, long follow-up, and carefully characterized evaluations estimated the overall incidence of seizures in AD at ~1 per 200 person-years of observation, suggesting relatively lower frequencies than those reported in other studies. Vossel et al. (74) found that 42.4% of patients with AD exhibited epileptic activity compared with 10.5% in the control group. Furthermore, the overall cognitive ability of patients with epileptic activity decreased faster than that in the control group. Zelano et al. (75) assessed the risk of epilepsy in patients with AD. The results showed that the risk of epilepsy at 5 and 10 years after onset of AD was 2.1% and 4.0%, while that in the control group was 0.8 and 1.6%, respectively. However, Mahamud et al. (76) estimated that the risk of epilepsy diagnosis in the 5 years following a first, unprovoked seizure in patients with AD was 32%, compared to 31% in the control group. Cognitively asymptomatic individuals who harbor pathogenic autosomal dominant AD mutations were more likely to have seizures (77).
Seizures may be particularly difficult to diagnose in patients with AD, as most reports of seizure symptoms in AD patients are provided by caregivers. It may be difficult for caregivers to describe seizure symptoms and to distinguish these symptoms from common manifestations of AD (such as hallucinations and delusions) (40). TLE may be an early feature of sporadic AD (78). Among patients with aMCI or AD with epilepsy, complex partial seizures are most common, and more than half of these seizures are non-convulsive (28). A study (46) showed that generalized tonic-clonic seizures occurred in 15–40% of patients with advanced AD complicated with epilepsy, and 70% of seizures in these patients were focal. Horváth et al. (14) analyzed the characteristics of 18 seizures in 10 patients with AD and found that 11% of the seizures were generalized tonic-clonic, 72% were focal seizures with impaired awareness, and 55% were non-motor seizures. Haoudy et al. (42) investigated 40 patients with early onset AD (EOAD) and found that the most common seizure types were tonic-clonic (25%), typical temporal seizures (25%), myoclonic (25%), focal extra-temporal (8%), and other seizure types (17%). Subclinical epileptiform activity in patients with AD has also been associated with cognitive ability (79). Vossel et al. (74) found that patients with AD and subclinical epileptiform activity have a faster decline in overall cognitive ability, as evidenced by a decrease of 3.9 points per year in their MMSE score. This is compared to the 1.6 points per year decrease observed in patients with AD without epileptiform activity.
Costa et al. (80) showed that the incidence rate of late-onset cryptogenic epilepsy in patients with advanced AD was associated with higher concentrations of AD markers in CSF. They retrospectively selected and studied 13 patients who met the diagnostic criteria for MCI. All 13 patients also met the criteria for clinical diagnosis of epilepsy prior to MCI diagnosis. Interestingly, epilepsy appeared 4–7 years earlier than AD. This phenomenon was termed epileptic prodromal AD, and researchers suggested that epileptic prodromal AD is an epileptic variant of AD. Furthermore, they suggested that the spectrum of AD should be extended to include epilepsy variants. In summary, epilepsy should be used as a phenotypic marker of AD (78).
Focal seizures in AD may be difficult to identify and may not be detected by surface EEG electrodes that only detect cortical activity (81). In patients with AD, IED was usually detected in electrodes around the frontotemporal and temporal lobe brain regions (78). Vossel et al. (28) found temporal epileptiform abnormalities were the commonest finding, although frontal and generalized discharges were also seen. The results were consistent with Sarkis's study results (82).
Because non-convulsive seizures may be masked by cognitive impairment, detection of epileptic-like activity may require long-term EEG monitoring (83). Long-term EEG recording, including during sleep, may result in a higher diagnostic rate (84). In a preliminary study (85), EEG abnormalities during sleep were associated with cerebrospinal fluid biomarkers, particularly hyperphosphorylated tau protein levels, suggesting the presence of preclinical AD. Horvath et al. (14) recorded electric ictal patterns twice during a recording period in 2 of 10 patients with AD, and clinically identified seizures in 8 of the 10 patients with AD using ambulatory EEG. Yu et al. (86) summarized the results of several research groups and found that epileptiform discharges, especially those with the specific characteristics of frequent, small spikes, temporal intermittent rhythmic delta activities, and paroxysmal slow wave events recorded using long-term scalp EEG, provided sufficient sensitivity and specificity for detecting the epileptogenic nature of AD. Horvath et al. (13) found that epileptiform discharges were associated with lower memory scores. Lam et al. (12) found that epileptiform discharges tended to occur during periods of wakefulness and during rapid eye movement sleep (REM sleep). Frequent spikes were particularly associated with epileptiform EEG and may serve as markers of hyperexcitability in AD.
The sensitivity and daily distribution of epileptiform discharges are different during different periods throughout the day. For example, Horvath et al. (87) found that EEG epileptiform discharges were more likely to be recorded between 8:00 and 16:00, while 82% of epileptiform discharges in sleep occurred during non-REM sleep. Moreover, AD progression was related to the high recurrence of seizures. Voglein et al. (17) investigated 20,745 individuals from the National Alzheimer's Coordinating Center and found that the risk of epilepsy recurrence within the following 7.5-month period was 70.4% in patients with AD. Furthermore, seizure prevalence increased with increasing duration of AD.
The close relationship between epilepsy and AD indicates that both epilepsy and AD require active intervention. Antiepileptic drugs (AEDs) improve cognitive symptoms and have antiepileptic effects (88). Use of AEDs can directly inhibit seizures and hyperexcitability, which may reduce Aβ accumulation (89). However, because cognitive function is particularly susceptible to decline in patients with AD, the possible neurocognitive effects of these drugs must be considered when prescribing AEDs for AD (90). Use of AEDs may increase the risk of developing AD (91).
Elderly individuals are at higher risk for developing chronic diseases and often take a variety of oral medications. Thus, drug-drug interactions that alter drug metabolism and/or bioavailability must be considered when prescribing AEDs in elderly individuals. These types of drug-drug interactions may induce a variety of adverse effects that aggravate cognitive impairment (92). For example, benzodiazepines may enhance GABA secretion by astrocytes, resulting in an increased risk for developing AD (93, 94). Therefore, benzodiazepines are not recommended for treatment of seizures in AD patients. Valproic acid (VPA) should also be avoided, because it may lead to cognitive decline (95). A retrospective (96) analysis of ten antiepileptic drugs prescribed to elderly, showed that cognitive adverse efects are common in patients on topiramate (TPM) followed by those on zonisamide (ZNS) and gabapentin (GBP). A meta-analysis (97) reported that LTG was associated with a lower probability of seizure freedom than LEV and had a limited effect on cognition in older people with epilepsy. However, Liu et al. (98) performed a randomized controlled trial on drug intervention that indicated that LEV seemed to improve cognition, whereas phenobarbital and LTG could worsen cognition. Additional studies are needed to further characterize treatment of AD-related epilepsy with LTG.
LEV is a novel antiepileptic drug that has the ability to reverse cognitive impairment (99). Vossel et al. (100) studied the effect of LEV on cognitive ability in AD patients with and without epileptic activity and found that LEV improved spatial memory performance and executive ability in patients with AD with epileptic activity. This effect may be due to reduced AD-associated network hyperexcitability. Brivaracetam (BRV) is an antiepileptic drug that was approved by the FDA in 2013 for the treatment of partial seizures. Brodie et al. (101) followed up the tolerability, safety, and efficacy of BRV for adjunctive treatment of focal (partial-onset) seizures in patients aged ≥65 years. Thirty-two cases were included and the results showed that BRV was effective with no significant impact on cognition. In animal experiments, BRV reversed memory deficits in a mouse model of AD (102). A retrospective analysis of 71 patients with epilepsy (> 60 years old) who were treated with lacosamide (LCM) showed that 60% of patients continued to take LCM at their 12-month follow-up visit, and no patients discontinued taking LCM due to cognitive issues (103). Perampanel (PER) is a third-generation antiepileptic non-selective AMPA receptor antagonist used to treat patients over the age of 12 years who have epilepsy. Ahn et al. (104) recruited 17 patients with epilepsy and treated them with PER for 6 months. In this cohort, PER did not induce cognitive decline. Lattanzi et al. (105) reviewed and analyzed the adverse events experienced by elderly patients with epilepsy who took PER at 12 different Italian epilepsy centers. The results showed that the common adverse events in elderly individuals taking PER were dizziness, irritability, and drowsiness. Cognitive decline was not common. Rohracher et al. (106) conducted a critical narrative review on the use of new AEDs in elderly patients with epilepsy. The results showed that PER and LCM had the lowest interaction risk and were considered first-line drugs for epilepsy treatment in elderly patients. Other studies of these AEDs are summarized in Table 2.
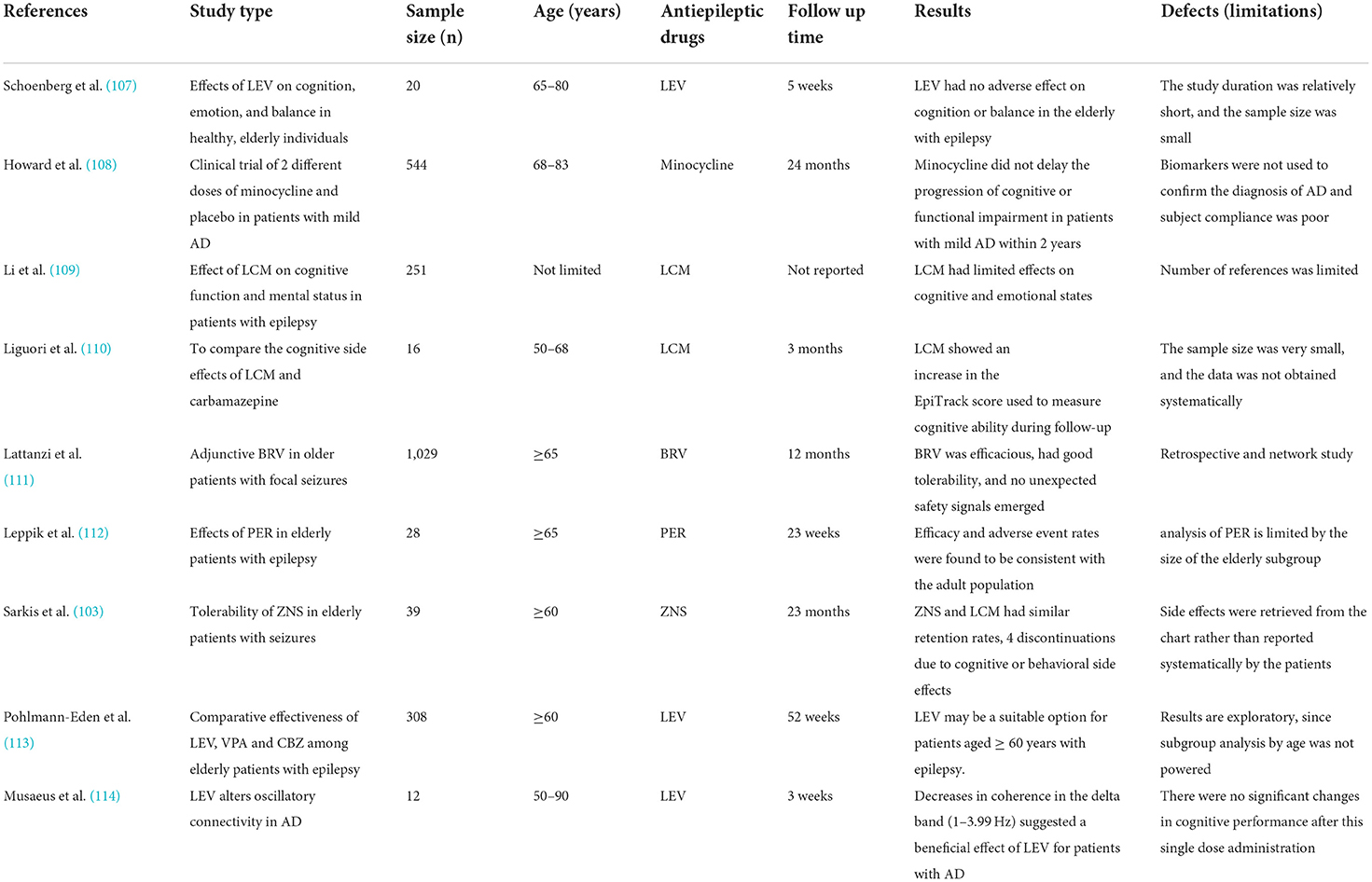
Table 2. Effects of new antiepileptic drugs on cognition.
Studies have shown that epilepsy and AD share a common underlying pathology. Seizures, especially generalized tonic-clonic and complex partial/non-convulsive ones are typically associated with a transitory cognitive impairment, even in case of incidental and single seizures. A thorough investigation of the risk and etiology of recurrent seizures is needed. Early identification of epilepsy in patients with AD and in the AD prodromal stage, through various diagnostic techniques (including EEG), is critical. Seizures related to AD may precede or coincide with the onset of the cognitive decline. Early identification of non-convulsive seizures and the recognition of epileptiform EEG activity is of crucial importance for patient outcome. The new generation of AEDs is more suitable for treatment of elderly patients with epilepsy and neurodegenerative diseases due to their superior pharmacokinetic characteristics. Timing of intervention is critical. Most research on hyperexcitability in AD has focused on Aβ and Tau, but other factors, such as presenilin 2 (PSEN2), may contribute to hyperexcitability in AD. Future studies should focus on multiple potential mechanisms of hyperactivity in AD, as this may lead to further characterization of the shared pathogenesis of AD and epilepsy and may allow for identification of novel therapies.
JW and SX searched the literature. WC and YZ conducted literature review and analysis. DZ and SC wrote original draft. XC did review and editing. XL was responsible for supervision. All authors contributed to the article and approved the submitted version.
This work was supported by the scientific research plan of the Affiliated People's Hospital of Jiangsu University (Y201933).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Banerjee PN, Filippi D, Allen Hauser W. The descriptive epidemiology of epilepsy-a review. Epilepsy Res. (2009) 85:31–45. doi: 10.1016/j.eplepsyres.2009.03.003
2. Amatniek JC, Hauser WA, DelCastillo-Castaneda C, Jacobs DM, Marder K, Bell K, et al. Incidence and predictors of seizures in patients with alzheimer's disease. Epilepsia. (2006) 47:867–72. doi: 10.1111/j.1528-1167.2006.00554.x
3. Sen A, Capelli V, Husain M. Cognition and dementia in older patients with epilepsy. Brain. (2018) 141:1592–608. doi: 10.1093/brain/awy022
4. Neri S, Mastroianni G, Gardella E, Aguglia U, Rubboli G. Epilepsy in neurodegenerative diseases. Epileptic Disord. (2022) 24:249–73. doi: 10.1684/epd.2021.1406
5. Friedman D, Honig LS, Scarmeas N. Seizures and epilepsy in alzheimer's disease. CNS Neurosci Ther. (2012) 18:285–94. doi: 10.1111/j.1755-5949.2011.00251.x
6. Tombini M, Assenza G, Ricci L, Lanzone J, Boscarino M, Vico C, et al. Temporal lobe epilepsy and alzheimer's disease: from preclinical to clinical evidence of a strong association. J Alzheimers Dis Rep. (2021) 5:243–61. doi: 10.3233/ADR-200286
7. Bakker A, Krauss GL, Albert MS, Speck CL, Jones LR, Stark CE, et al. Reduction of hippocampal hyperactivity improves cognition in amnestic mild cognitive impairment. Neuron. (2012) 74:467–74. doi: 10.1016/j.neuron.2012.03.023
8. Paudel YN, Angelopoulou E, Piperi C, Othman I, Shaikh MF. Revisiting the impact of neurodegenerative proteins in epilepsy: focus on alpha-synuclein, beta-amyloid, and tau. Biology. (2020) 9:122. doi: 10.3390/biology9060122
9. Altuna M, Olmedo-Saura G, Carmona-Iragui M, Fortea J. Mechanisms involved in epileptogenesis in alzheimer's disease and their therapeutic implications. Int J Mol Sci. (2022) 23:4307. doi: 10.3390/ijms23084307
10. Giorgi FS, Saccaro LF, Busceti CL, Biagioni F, Fornai F. Epilepsy and alzheimer's disease: potential mechanisms for an association. Brain Res Bull. (2020) 160:107–20. doi: 10.1016/j.brainresbull.2020.04.009
11. DiFrancesco JC, Tremolizzo L, Polonia V, Giussani G, Bianchi E, Franchi C, et al. Adult-onset epilepsy in presymptomatic alzheimer's disease: a retrospective study. J Alzheimers Dis. (2017) 60:1267–74. doi: 10.3233/JAD-170392
12. Lam AD, Sarkis RA, Pellerin KR, Jing J, Dworetzky BA, Hoch DB, et al. Association of epileptiform abnormalities and seizures in alzheimer disease. Neurology. (2020) 95:e2259–e70. doi: 10.1212/WNL.0000000000010612
13. Horvath AA, Papp A, Zsuffa J, Szucs A, Luckl J, Radai F, et al. Subclinical epileptiform activity accelerates the progression of alzheimer's disease: a long-term EEG study. Clin Neurophysiol. (2021) 132:1982–9. doi: 10.1016/j.clinph.2021.03.050
14. Horvath A, Szucs A, Hidasi Z, Csukly G, Barcs G, Kamondi A. Prevalence, semiology, and risk factors of epilepsy in alzheimer's disease: an ambulatory EEG study. J Alzheimers Dis. (2018) 63:1045–54. doi: 10.3233/JAD-170925
15. Arnaldi D, Donniaquio A, Mattioli P, Massa F, Grazzini M, Meli R, et al. Epilepsy in neurodegenerative dementias: a clinical, epidemiological, and EEG study. J Alzheimers Dis. (2020) 74:865–74. doi: 10.3233/JAD-191315
16. Tedrus GM, Negreiros LM, Ballarim RS, Marques TA, Fonseca LC. Correlations between cognitive aspects and quantitative EEG in adults with epilepsy. Clin EEG Neurosci. (2019) 50:348–53. doi: 10.1177/1550059418793553
17. Voglein J, Ricard I, Noachtar S, Kukull WA, Dieterich M, Levin J, et al. Seizures in alzheimer's disease are highly recurrent and associated with a poor disease course. J Neurol. (2020) 267:2941–8. doi: 10.1007/s00415-020-09937-7
18. Reyes A, Kaestner E, Edmonds EC, Christina Macari A, Wang ZI, Drane DL, et al. Diagnosing cognitive disorders in older adults with epilepsy. Epilepsia. (2021) 62:460–71. doi: 10.1111/epi.16780
19. Costa C, Vecchio F, Romoli M, Miraglia F, Nardi Cesarini E, Alu F, et al. Cognitive decline risk stratification in people with late-onset epilepsy of unknown etiology: an electroencephalographic connectivity and graph theory pilot study. J Alzheimers Dis. (2021). doi: 10.3233/JAD-210350. [Epub ahead of print].
20. Schnier C, Duncan S, Wilkinson T, Mbizvo GK, Chin RFM. A nationwide, retrospective, data-linkage, cohort study of epilepsy and incident dementia. Neurology. (2020) 95:e1686–e93. doi: 10.1212/WNL.0000000000010358
21. Liguori C, Costa C, Franchini F, Izzi F, Spanetta M, Cesarini EN, et al. Cognitive performances in patients affected by late-onset epilepsy with unknown etiology: a 12-month follow-up study. Epilepsy Behav. (2019) 101:106592. doi: 10.1016/j.yebeh.2019.106592
22. Scharfman HE, Chao MV. The entorhinal cortex and neurotrophin signaling in alzheimer's disease and other disorders. Cogn Neurosci. (2013) 4:123–35. doi: 10.1080/17588928.2013.826184
23. Zheng P, Shultz SR, Hovens CM, Velakoulis D, Jones NC, O'Brien TJ. Hyperphosphorylated tau is implicated in acquired epilepsy and neuropsychiatric comorbidities. Mol Neurobiol. (2014) 49:1532–9. doi: 10.1007/s12035-013-8601-9
24. Puvenna V, Engeler M, Banjara M, Brennan C, Schreiber P, Dadas A, et al. Is phosphorylated tau unique to chronic traumatic encephalopathy? phosphorylated tau in epileptic brain and chronic traumatic encephalopathy. Brain Res. (2016) 1630:225–40. doi: 10.1016/j.brainres.2015.11.007
25. Mackenzie IR, Miller LA. Senile plaques in temporal lobe epilepsy. Acta Neuropathol. (1994) 87:504–10. doi: 10.1007/BF00294177
26. Tai XY, Koepp M, Duncan JS, Fox N, Thompson P, Baxendale S, et al. Hyperphosphorylated tau in patients with refractory epilepsy correlates with cognitive decline: a study of temporal lobe resections. Brain. (2016) 139:2441–55. doi: 10.1093/brain/aww187
27. Tait L, Lopes MA, Stothart G, Baker J, Kazanina N, Zhang J, et al. A large-scale brain network mechanism for increased seizure propensity in alzheimer's disease. PLoS Comput Biol. (2021) 17:e1009252. doi: 10.1371/journal.pcbi.1009252
28. Vossel KA, Beagle AJ, Rabinovici GD, Shu H, Lee SE, Naasan G, et al. Seizures and epileptiform activity in the early stages of alzheimer disease. JAMA Neurol. (2013) 70:1158–66. doi: 10.1001/jamaneurol.2013.136
29. Fernandez-Perez EJ, Munoz B, Bascunan DA, Peters C, Riffo-Lepe NO, Espinoza MP, et al. Synaptic dysregulation and hyperexcitability induced by intracellular amyloid beta oligomers. Aging Cell. (2021) 20:e13455. doi: 10.1111/acel.13455
30. Beckman M, Knox K, Koneval Z, Smith C, Jayadev S, Barker-Haliski M. Loss of presenilin 2 age-dependently alters susceptibility to acute seizures and kindling acquisition. Neurobiol Dis. (2020) 136:104719. doi: 10.1016/j.nbd.2019.104719
31. Teixeira CM, Pallas-Bazarra N, Bolos M, Terreros-Roncal J, Avila J, Llorens-Martin M. Untold new beginnings: adult hippocampal neurogenesis and alzheimer's disease. J Alzheimers Dis. (2018) 64:S497–505. doi: 10.3233/JAD-179918
32. Scharfman HE. Alzheimer's disease and epilepsy: insight from animal models. Future Neurol. (2012) 7:177–92. doi: 10.2217/fnl.12.8
33. Kim S, Nam Y, Jeong YO, Park HH, Lee SK, Shin SJ, et al. Topographical visualization of the reciprocal projection between the medial septum and the hippocampus in the 5xfad mouse model of alzheimer's disease. Int J Mol Sci. (2019) 20:3992. doi: 10.3390/ijms20163992
34. Essa H, Peyton L, Hasan W, Leon BE, Choi DS. Implication of adult hippocampal neurogenesis in alzheimer's disease and potential therapeutic approaches. Cells. (2022) 11:286. doi: 10.3390/cells11020286
35. Sakimoto Y, Oo PM, Goshima M, Kanehisa I, Tsukada Y, Mitsushima D. Significance of gabaa receptor for cognitive function and hippocampal pathology. Int J Mol Sci. (2021) 22:12456. doi: 10.3390/ijms222212456
36. Dejakaisaya H, Kwan P, Jones NC. Astrocyte and glutamate involvement in the pathogenesis of epilepsy in alzheimer's disease. Epilepsia. (2021) 62:1485–93. doi: 10.1111/epi.16918
37. Paudel YN, Angelopoulou E, Jones NC, O'Brien TJ, Kwan P, Piperi C, et al. Tau related pathways as a connecting link between epilepsy and alzheimer's disease. ACS Chem Neurosci. (2019) 10:4199–212. doi: 10.1021/acschemneuro.9b00460
38. Szot P. Common factors among alzheimer's disease, parkinson's disease, and epilepsy: possible role of the noradrenergic nervous system. Epilepsia. (2012) 53(Suppl 1):61–6. doi: 10.1111/j.1528-1167.2012.03476.x
39. Imfeld P, Bodmer M, Schuerch M, Jick SS, Meier CR. Seizures in patients with alzheimer's disease or vascular dementia: a population-based nested case-control analysis. Epilepsia. (2013) 54:700–7. doi: 10.1111/epi.12045
40. Pandis D, Scarmeas N. Seizures in alzheimer disease: clinical and epidemiological data. Epilepsy Curr. (2012) 12:184–7. doi: 10.5698/1535-7511-12.5.184
41. Noebels J. A perfect storm: converging paths of epilepsy and alzheimer's dementia intersect in the hippocampal formation. Epilepsia. (2011) 52(Suppl 1):39–46. doi: 10.1111/j.1528-1167.2010.02909.x
42. Haoudy S, Jonveaux T, Puisieux S, Epstein J, Hopes L, Maillard L, et al. Epilepsy in early onset alzheimer's disease. J Alzheimers Dis. (2022) 85:615–26. doi: 10.3233/JAD-210681
43. Kang JQ. Epileptic mechanisms shared by alzheimer's disease: viewed via the unique lens of genetic epilepsy. Int J Mol Sci. (2021) 22:7133. doi: 10.3390/ijms22137133
44. Thom M, Liu JY, Thompson P, Phadke R, Narkiewicz M, Martinian L, et al. Neurofibrillary tangle pathology and braak staging in chronic epilepsy in relation to traumatic brain injury and hippocampal sclerosis: a post-mortem study. Brain. (2011) 134:2969–81. doi: 10.1093/brain/awr209
45. Nardi Cesarini E, Babiloni C, Salvadori N, Farotti L, Del Percio C, Pascarelli MT, et al. Late-onset epilepsy with unknown etiology: a pilot study on neuropsychological profile, cerebrospinal fluid biomarkers, and quantitative EEG characteristics. Front Neurol. (2020) 11:199. doi: 10.3389/fneur.2020.00199
46. Vossel KA, Tartaglia MC, Nygaard HB, Zeman AZ, Miller BL. Epileptic activity in alzheimer's disease: causes and clinical relevance. Lancet Neurol. (2017) 16:311–22. doi: 10.1016/S1474-4422(17)30044-3
47. Gaitatzis A, Sisodiya SM, Sander JW. The somatic comorbidity of epilepsy: a weighty but often unrecognized burden. Epilepsia. (2012) 53:1282–93. doi: 10.1111/j.1528-1167.2012.03528.x
48. Forsgren L, Bucht G, Eriksson S, Bergmark L. Incidence and clinical characterization of unprovoked seizures in adults: a prospective population-based study. Epilepsia. (1996) 37:224–9. doi: 10.1111/j.1528-1157.1996.tb00017.x
49. Lozsadi DA, Larner AJ. Prevalence and causes of seizures at the time of diagnosis of probable alzheimer's disease. Dement Geriatr Cogn Disord. (2006) 22:121–4. doi: 10.1159/000093664
50. Xu Y, Lavrencic L, Radford K, Booth A, Yoshimura S, Anstey KJ, et al. Systematic review of coexistent epileptic seizures and alzheimer's disease: incidence and prevalence. J Am Geriatr Soc. (2021) 69:2011–20. doi: 10.1111/jgs.17101
51. Ophir K, Ran B, Felix B, Amir G. Ten year cumulative incidence of dementia after late onset epilepsy of unknown etiology. J Clin Neurosci. (2021) 86:247–51. doi: 10.1016/j.jocn.2021.01.030
52. Tsai ZR, Zhang HW, Tseng CH, Peng HC, Kok VC, Li GP, et al. Late-onset epilepsy and subsequent increased risk of dementia. Aging. (2021) 13:3573–87. doi: 10.18632/aging.202299
53. Stefanidou M, Beiser AS, Himali JJ, Peng TJ, Devinsky O, Seshadri S, et al. Bi-directional association between epilepsy and dementia: the framingham heart study. Neurology. (2020) 95:e3241–e7. doi: 10.1212/WNL.0000000000011077
54. Witt JA, Helmstaedter C. Should cognition be screened in new-onset epilepsies? a study in 247 untreated patients. J Neurol. (2012) 259:1727–31. doi: 10.1007/s00415-012-6526-2
55. Novak A, Vizjak K, Rakusa M. Cognitive impairment in people with epilepsy. J Clin Med. (2022) 11:267. doi: 10.3390/jcm11010267
56. Miller LA, Galioto R, Tremont G, Davis J, Bryant K, Roth J, et al. Cognitive impairment in older adults with epilepsy: characterization and risk factor analysis. Epilepsy Behav. (2016) 56:113–7. doi: 10.1016/j.yebeh.2016.01.011
57. Wang L, Chen S, Liu C, Lin W, Huang H. Factors for cognitive impairment in adult epileptic patients. Brain Behav. (2020) 10:e01475. doi: 10.1002/brb3.1475
58. Taylor J, Kolamunnage-Dona R, Marson AG, Smith PE, Aldenkamp AP, Baker GA, et al. Patients with epilepsy: cognitively compromised before the start of antiepileptic drug treatment? Epilepsia. (2010) 51:48–56. doi: 10.1111/j.1528-1167.2009.02195.x
59. Baker GA, Taylor J, Aldenkamp AP, group S. Newly diagnosed epilepsy: cognitive outcome after 12 months. Epilepsia. (2011) 52:1084–91. doi: 10.1111/j.1528-1167.2011.03043.x
60. Kaestner E, Reyes A, Chen A, Rao J, Macari AC, Choi JY, et al. Atrophy and cognitive profiles in older adults with temporal lobe epilepsy are similar to mild cognitive impairment. Brain. (2021) 144:236–50. doi: 10.1093/brain/awaa397
61. Johnson EL, Krauss GL, Walker KA, Brandt J, Kucharska-Newton A, Mosley TH Jr, et al. Late-onset epilepsy and 25-year cognitive change: the atherosclerosis risk in communities (aric) study. Epilepsia. (2020) 61:1764–73. doi: 10.1111/epi.16616
62. Liu XY, Shi T, Yin WN, Ren ZY, Deng YL, Chen SD. Interictal epileptiform discharges were associated with poorer cognitive performance in adult epileptic patients. Epilepsy Res. (2016) 128:1–5. doi: 10.1016/j.eplepsyres.2016.09.022
63. Stafstrom CE, Carmant L. Seizures and epilepsy: an overview for neuroscientists. Cold Spring Harb Perspect Med. (2015) 5:a022426. doi: 10.1101/cshperspect.a022426
64. Landi S, Petrucco L, Sicca F, Ratto GM. Transient cognitive impairment in epilepsy. Front Mol Neurosci. (2018) 11:458. doi: 10.3389/fnmol.2018.00458
65. Dinkelacker V, Xin X, Baulac M, Samson S, Dupont S. Interictal epileptic discharge correlates with global and frontal cognitive dysfunction in temporal lobe epilepsy. Epilepsy Behav. (2016) 62:197–203. doi: 10.1016/j.yebeh.2016.07.009
66. Holmes GL. Interictal spikes as an EEG biomarker of cognitive impairment. J Clin Neurophysiol. (2022) 39:101–12. doi: 10.1097/WNP.0000000000000728
67. Ung H, Cazares C, Nanivadekar A, Kini L, Wagenaar J, Becker D, et al. Interictal epileptiform activity outside the seizure onset zone impacts cognition. Brain. (2017) 140:2157–68. doi: 10.1093/brain/awx143
68. Kleen JK, Scott RC, Holmes GL, Roberts DW, Rundle MM, Testorf M, et al. Hippocampal interictal epileptiform activity disrupts cognition in humans. Neurology. (2013) 81:18–24. doi: 10.1212/WNL.0b013e318297ee50
69. Horak PC, Meisenhelter S, Song Y, Testorf ME, Kahana MJ, Viles WD, et al. Interictal epileptiform discharges impair word recall in multiple brain areas. Epilepsia. (2017) 58:373–80. doi: 10.1111/epi.13633
70. Loughman A, Seneviratne U, Bowden SC, D'Souza WJ. Epilepsy beyond seizures: predicting enduring cognitive dysfunction in genetic generalized epilepsies. Epilepsy Behav. (2016) 62:297–303. doi: 10.1016/j.yebeh.2016.07.010
71. Elsherif M, Esmael A. Hippocampal atrophy and quantitative EEG markers in mild cognitive impairment in temporal lobe epilepsy versus extra-temporal lobe epilepsy. Neurol Sci. (2022) 43:1975–86. doi: 10.1007/s10072-021-05540-4
72. Subota A, Pham T, Jette N, Sauro K, Lorenzetti D, Holroyd-Leduc J. The association between dementia and epilepsy: a systematic review and meta-analysis. Epilepsia. (2017) 58:962–72. doi: 10.1111/epi.13744
73. Irizarry MC, Jin S, He F, Emond JA, Raman R, Thomas RG, et al. Incidence of new-onset seizures in mild to moderate alzheimer disease. Arch Neurol. (2012) 69:368–72. doi: 10.1001/archneurol.2011.830
74. Vossel KA, Ranasinghe KG, Beagle AJ, Mizuiri D, Honma SM, Dowling AF, et al. Incidence and impact of subclinical epileptiform activity in alzheimer's disease. Ann Neurol. (2016) 80:858–70. doi: 10.1002/ana.24794
75. Zelano J, Brigo F, Garcia-Patek S. Increased risk of epilepsy in patients registered in the Swedish dementia registry. Eur J Neurol. (2020) 27:129–35. doi: 10.1111/ene.14043
76. Mahamud Z, Mononen CP, Brigo F, Garcia-Ptacek S, Zelano J. Risk of epilepsy diagnosis after a first unprovoked seizure in dementia. Seizure. (2020) 82:118–24. doi: 10.1016/j.seizure.2020.09.001
77. Voglein J, Noachtar S, McDade E, Quaid KA, Salloway S, Ghetti B, et al. Seizures as an early symptom of autosomal dominant alzheimer's disease. Neurobiol Aging. (2019) 76:18–23. doi: 10.1016/j.neurobiolaging.2018.11.022
78. Cretin B, Sellal F, Philippi N, Bousiges O, Di Bitonto L, Martin-Hunyadi C, et al. Epileptic prodromal alzheimer's disease, a retrospective study of 13 new cases: expanding the spectrum of alzheimer's disease to an epileptic variant? J Alzheimers Dis. (2016) 52:1125–33. doi: 10.3233/JAD-150096
79. Ranasinghe KG, Kudo K, Hinkley L, Beagle A, Lerner H, Mizuiri D, et al. Neuronal synchrony abnormalities associated with subclinical epileptiform activity in early onset alzheimer's disease. Brain. (2021) 145:744–53. doi: 10.1093/brain/awab442
80. Costa C, Romoli M, Liguori C, Farotti L, Eusebi P, Bedetti C, et al. Alzheimer's disease and late-onset epilepsy of unknown origin: two faces of beta amyloid pathology. Neurobiol Aging. (2019) 73:61–7. doi: 10.1016/j.neurobiolaging.2018.09.006
81. Lam AD, Deck G, Goldman A, Eskandar EN, Noebels J, Cole AJ. Silent Hippocampal seizures and spikes identified by foramen ovale electrodes in alzheimer's disease. Nat Med. (2017) 23:678–80. doi: 10.1038/nm.4330
82. Sarkis RA, Dickerson BC, Cole AJ, Chemali ZN. Clinical and neurophysiologic characteristics of unprovoked seizures in patients diagnosed with dementia. J Neuropsychiatry Clin Neurosci. (2016) 28:56–61. doi: 10.1176/appi.neuropsych.15060143
83. Horvath A, Szucs A, Barcs G, Noebels JL, Kamondi A. Epileptic seizures in alzheimer disease: a review. Alzheimer Dis Assoc Disord. (2016) 30:186–92. doi: 10.1097/WAD.0000000000000134
84. Smith SJ. EEG in the diagnosis, classification, and management of patients with epilepsy. J Neurol Neurosurg Psychiatry. (2005) 76(Suppl 2):ii2–7. doi: 10.1136/jnnp.2005.069245
85. Lucey BP, Wisch J, Boerwinkle AH, Landsness EC, Toedebusch CD, McLeland JS, et al. Sleep and longitudinal cognitive performance in preclinical and early symptomatic alzheimer's disease. Brain. (2021) 144:2852–62. doi: 10.1093/brain/awab272
86. Yu T, Liu X, Wu J, Wang Q. Electrophysiological biomarkers of epileptogenicity in alzheimer's disease. Front Hum Neurosci. (2021) 15:747077. doi: 10.3389/fnhum.2021.747077
87. Horvath A, Szucs A, Barcs G, Kamondi A. Sleep EEG detects epileptiform activity in alzheimer's disease with high sensitivity. J Alzheimers Dis. (2017) 56:1175–83. doi: 10.3233/JAD-160994
88. Kanner AM, Helmstaedter C, Sadat-Hossieny Z, Meador K. Cognitive disorders in epilepsy I: clinical experience, real-world evidence and recommendations. Seizure. (2020) 83:216–22. doi: 10.1016/j.seizure.2020.10.009
89. Lehmann L, Lo A, Knox KM, Barker-Haliski M. Alzheimer's disease and epilepsy: a perspective on the opportunities for overlapping therapeutic innovation. Neurochem Res. (2021) 46:1895–912. doi: 10.1007/s11064-021-03332-y
90. Gimenez DeGeorge E, Fullen C, Gess J, Kleiner J, Larson-Prior L. Effects of age of onset and medication on cognitive performance and quality of life in patients with epilepsy. Epilepsy Behav. (2021) 121:108008. doi: 10.1016/j.yebeh.2021.108008
91. Carter MD, Weaver DF, Joudrey HR, Carter AO, Rockwood K. Epilepsy and antiepileptic drug use in elderly people as risk factors for dementia. J Neurol Sci. (2007) 252:169–72. doi: 10.1016/j.jns.2006.11.004
92. Sen A, Jette N, Husain M, Sander JW. Epilepsy in older people. Lancet. (2020) 395:735–48. doi: 10.1016/S0140-6736(19)33064-8
93. Pariente A, de Gage SB, Moore N, Begaud B. The benzodiazepine-dementia disorders link: current state of knowledge. CNS Drugs. (2016) 30:1–7. doi: 10.1007/s40263-015-0305-4
94. Billioti de Gage S, Moride Y, Ducruet T, Kurth T, Verdoux H, Tournier M, et al. Benzodiazepine use and risk of alzheimer's disease: case-control study. BMJ. (2014) 349:g5205. doi: 10.1136/bmj.g5205
95. Fleisher AS, Truran D, Mai JT, Langbaum JB, Aisen PS, Cummings JL, et al. Chronic divalproex sodium use and brain atrophy in alzheimer disease. Neurology. (2011) 77:1263–71. doi: 10.1212/WNL.0b013e318230a16c
96. Arif H, Buchsbaum R, Pierro J, Whalen M, Sims J, Resor SR Jr, et al. Comparative effectiveness of 10 antiepileptic drugs in older adults with epilepsy. Arch Neurol. (2010) 67:408–15. doi: 10.1001/archneurol.2010.49
97. Lezaic N, Gore G, Josephson CB, Wiebe S, Jette N, Keezer MR. The medical treatment of epilepsy in the elderly: a systematic review and meta-analysis. Epilepsia. (2019) 60:1325–40. doi: 10.1111/epi.16068
98. Liu J, Wang LN. Treatment of epilepsy for people with alzheimer's disease. Cochrane Database Syst Rev. (2021) 5:CD011922. doi: 10.1002/14651858.CD011922.pub4
99. Gonzalez HG, Contreras-Garcia IJ, Sanchez-Huerta K, Queiroz CMT, Gallardo Gudino LR, Mendoza-Torreblanca JG, et al. Levetiracetam reduced the basal excitability of the dentate gyrus without restoring impaired synaptic plasticity in rats with temporal lobe epilepsy. Brain Sci. (2020) 10:634. doi: 10.3390/brainsci10090634
100. Vossel K, Ranasinghe KG, Beagle AJ, La A, Ah Pook K, Castro M, et al. Effect of levetiracetam on cognition in patients with alzheimer disease with and without epileptiform activity: a randomized clinical trial. JAMA Neurol. (2021) 78:1345–54. doi: 10.1001/jamaneurol.2021.3310
101. Brodie MJ, Whitesides J, Schiemann J, D'Souza J, Johnson ME. Tolerability, safety, and efficacy of adjunctive brivaracetam for focal seizures in older patients: a pooled analysis from three phase III studies. Epilepsy Res. (2016) 127:114–8. doi: 10.1016/j.eplepsyres.2016.08.018
102. Nygaard HB, Kaufman AC, Sekine-Konno T, Huh LL, Going H, Feldman SJ, et al. Brivaracetam, but not ethosuximide, reverses memory impairments in an alzheimer's disease mouse model. Alzheimers Res Ther. (2015) 7:25. doi: 10.1186/s13195-015-0110-9
103. Sarkis RA, Nicolas J, Lee JW. Tolerability of lacosamide or zonisamide in elderly patients with seizures. Seizure. (2017) 49:1–4. doi: 10.1016/j.seizure.2017.04.010
104. Ahn SJ, Kim TJ, Cha KS, Jun JS, Byun JI, Shin YW, et al. Effects of perampanel on cognition and quantitative electroencephalography in patients with epilepsy. Epilepsy Behav. (2021) 115:107514. doi: 10.1016/j.yebeh.2020.107514
105. Lattanzi S, Cagnetti C, Foschi N, Ciuffini R, Osanni E, Chiesa V, et al. Adjunctive perampanel in older patients with epilepsy: a multicenter study of clinical practice. Drugs Aging. (2021) 38:603–10. doi: 10.1007/s40266-021-00865-3
106. Rohracher A, Kalss G, Kuchukhidze G, Neuray C, Leitinger M, Hofler J, et al. New anti-seizure medication for elderly epilepsy patients-a critical narrative review. Expert Opin Pharmacother. (2021) 22:621–34. doi: 10.1080/14656566.2020.1843636
107. Schoenberg MR, Rum RS, Osborn KE, Werz MA. A randomized, double-blind, placebo-controlled crossover study of the effects of levetiracetam on cognition, mood, and balance in healthy older adults. Epilepsia. (2017) 58:1566–74. doi: 10.1111/epi.13849
108. Howard R, Zubko O, Bradley R, Harper E, Pank L, O'Brien J, et al. Minocycline at 2 different dosages vs placebo for patients with mild alzheimer disease: a randomized clinical trial. JAMA Neurol. (2020) 77:164–74. doi: 10.1001/jamaneurol.2019.3762
109. Li KY, Huang LC, Chang YP, Yang YH. The effects of lacosamide on cognitive function and psychiatric profiles in patients with epilepsy. Epilepsy Behav. (2020) 113:107580. doi: 10.1016/j.yebeh.2020.107580
110. Liguori C, Izzi F, Manfredi N, Mercuri NB, Placidi F. Lacosamide may improve cognition in patients with focal epilepsy: epitrack to compare cognitive side effects of lacosamide and carbamazepine. Epilepsy Behav Case Rep. (2018) 10:35–7. doi: 10.1016/j.ebcr.2018.02.004
111. Lattanzi S, Canafoglia L, Canevini MP, Casciato S, Cerulli Irelli E, Chiesa V, et al. Adjunctive brivaracetam in older patients with focal seizures: evidence from the brivaracetam addon first italian network study (brivafirst). Drugs Aging. (2022) 39:297–304. doi: 10.1007/s40266-022-00931-4
112. Leppik IE, Wechsler RT, Williams B, Yang H, Zhou S, Laurenza A. Efficacy and safety of perampanel in the subgroup of elderly patients included in the phase iii epilepsy clinical trials. Epilepsy Res. (2015) 110:216–20. doi: 10.1016/j.eplepsyres.2014.11.015
113. Pohlmann-Eden B, Marson AG, Noack-Rink M, Ramirez F, Tofighy A, Werhahn KJ, et al. Comparative effectiveness of levetiracetam, valproate and carbamazepine among elderly patients with newly diagnosed epilepsy: subgroup analysis of the randomized, unblinded komet study. BMC Neurol. (2016) 16:149. doi: 10.1186/s12883-016-0663-7
Keywords: Alzheimer's disease, epilepsy, cognitive, temporal lobe epilepsy, antiepileptic drugs
Citation: Zhang D, Chen S, Xu S, Wu J, Zhuang Y, Cao W, Chen X and Li X (2022) The clinical correlation between Alzheimer's disease and epilepsy. Front. Neurol. 13:922535. doi: 10.3389/fneur.2022.922535
Received: 18 April 2022; Accepted: 30 June 2022;
Published: 22 July 2022.
Edited by:
Görsev Yener, İzmir University of Economics, TurkeyReviewed by:
Didem Öz, Global Brain Health Institute, United StatesCopyright © 2022 Zhang, Chen, Xu, Wu, Zhuang, Cao, Chen and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaopeng Chen, cGlhb3lpY3hwQDE2My5jb20=; Xuezhong Li, c3VkYWx4ekAxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.