
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 16 June 2022
Sec. Neuro-Oncology and Neurosurgical Oncology
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.900377
This article is part of the Research Topic Updates on Current Protocols for the Management of Brain and Spine Malignancies View all 15 articles
 Aleksandrs Krigers
Aleksandrs Krigers Daniel Pinggera
Daniel Pinggera Matthias Demetz
Matthias Demetz Lisa-Marie Kornberger
Lisa-Marie Kornberger Johannes Kerschbaumer
Johannes Kerschbaumer Claudius Thomé
Claudius Thomé Christian F. Freyschlag*
Christian F. Freyschlag*Introduction: Tumor-treating fields (TTFs) are a specific local oncological treatment modality in glioblastoma multiforme WHO° IV (GBM). Their mechanism of action is based on the effect of electrical fields interfering with the mitotic activity of malignant cells. Prospective studies have demonstrated efficacy, but TTF benefits are still controversially discussed. This treatment was implemented in our center as the standard of care in January 2016. We thus discuss the current state of the art and our long-term experience in the routine application of TTF.
Methods: The data of 48 patients suffering from GBM and treated with TTF were assessed and compared with previously published studies. Up-to-date information from open sources was evaluated.
Results: A total of 31 males and 17 females harboring a GBM were treated with TTF, between January 2016 and August 2021, in our center. In 98% of cases, TTFs were started within 6 weeks after concomitant radiochemotherapy (Stupp protocol). Mean overall survival was 22.6 months (95% CI: 17.3–27.9). Current indications, benefits, and restrictions were evaluated. Future TTF opportunities and ongoing studies were reviewed.
Conclusion: TTFs are a feasible and routinely applicable specific oncological treatment option for glioblastoma multiforme WHO° IV. Further research is ongoing to extend the indications and the efficacy of TTF.
Glioma is the most frequent primary malignant tumor of the central nervous system (CNS) (1). High-grade glioma, especially glioblastoma multiforme WHO° IV (GBM), behaves aggressively with the corresponding unfavorable outcome and thus limited life expectancy (2). The established standardized treatment consists of a neurologically safe tumor resection (3–5), followed by adjuvant concomitant radiochemotherapy and six cycles of temozolomide (TMZ) monotherapy thereafter. This strategy is known as the Stupp protocol (6, 7). The disease, however, is considered incurable and there is a lack of efficient treatment options in the case of recurrent or progressive disease (8, 9).
Therefore, the demand for new approaches and targeted treatment options remains high. Although there is extensive research in this field, very few promising treatment options succeeded in the translation to clinical routine. One of them is the targeted application of tumor-treating fields (TTFs) (10). This method is based on the local effect of electric fields to interfere with the mitotic activity of the tumor. Proliferating cells are blocked in metaphase and anaphase as the formation of the mitotic spindle is disturbed, which results in slower cell replication or apoptosis (11–14).
TTFs are FDA- and EMA-approved for the treatment of adults with newly diagnosed GBM. In this case, TTFs are started within 6 weeks after the end of concomitant radiochemotherapy, ideally simultaneously with TMZ monotherapy (15, 16). Alternatively, TTF therapy can be an optional treatment in the case of recurrent GBM, overcoming the side effects of systemic second-line chemotherapeutics (17). Nevertheless, controversies considering TTF benefits are still conveyed (18).
Practically, four soft non-invasive adhesive electrode arrays are placed on the shaved head of the patient. The electric field is generated between the poles of the electrode arrays, which are supplied through a wire. The control device with pace-maker and the changeable accumulator is placed in a carry-on bag or backpack. Therapeutic success was seen when the device was worn for at least 18 h per day, with increasing benefits for every additional hour (15–17, 19). TTF therapy normally does not require an in-patient stay or additional oncological follow-ups. Technical assistance is provided by the service team of the manufacturer. Still, daily support by a person from the patient's household remains mandatory.
This kind of treatment in the case of GBM is incorporated in the international clinical guidelines (4, 20) and is implemented as a standard of care in our center since January 2016. During the following years, we gained practical know-how in TTF initiating, namely, informed consent, compliance, and follow-up. Thus, we aimed to discuss the current state of the art together with our long-term experience with the routine application of TTF. Moreover, we evaluated current indications, benefits, restrictions and also future TTF opportunities and ongoing studies.
According to international guidelines (4, 20) and consequently internal standard operating procedures, all patients harboring a histologically proven new or recurrent glioblastoma WHO° IV since January 2016 were considered for TTF therapy. Neuropathological tumor assessment was performed in all cases according to the revised 4th WHO classification of CNS tumors (21). The TTF indication was individually confirmed by the multidisciplinary neuro-oncological tumor board. Regardless of TTF, elective clinical and MRI follow-ups were performed every 3 months, in which the general and neurological condition, compliance, potential side effects, and oncological status were checked. In the case of recurrent or progressive disease, the eligibility for TTF was discussed in the multidisciplinary neuro-oncological tumor board. If there were no beneficial options for oncological resection, targeted systemic, or radiotherapy, TTF could be offered in case of expected compliance. TTF therapy is accepted by the Austrian healthcare insurance and, after formal approval of the indication, treatment costs are covered.
We assessed all patients who received the entire neuro-oncological treatment (surgery, radiation therapy, and chemotherapy) from the TTF starting in January 2016 till August 2021 from the institutional database. Patients who received either one of recommended treatments in external institutions were excluded. Each case data, namely, epidemiological, clinical, neuropathological, and follow-up records, was collected in the institutional database. The evaluation of this information for the scientific purpose was approved by the ethics committee of the Medical University of Innsbruck (No.: 1402/2020). It was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
All available publications and open-source data considering TTF application in high-grade gliomas were gathered and evaluated.
A total of 48 patients harboring a GBM treated with TTF were evaluated. Surgical intervention was performed in all cases, whereas gross neurologically safe resection was performed in 44 (92%) and biopsy in 4 (8%) patients. Among the patients, which were treated with TTF in our center, 31 (65%) were men and 17 (35%) were women with a median age of 57 years (interquartile range (IqR): 44–62), whereas 18 (38%) patients were older than 60 years and one was 16. The isocitrate dehydrogenase (IDH) status was routinely evaluated in 38 cases: IDH was mutated in 9 (23%) and remained wild-type in 30 (67%) tumors. In 22 (60%) patients, O(6)-methylguanine-DNA methyltransferase (MGMT) promoter was methylated and in 15 (40%) it stayed unmethylated. The Karnofsky performance index before surgery amounted to 80–100. Epileptic seizures before the surgery were reported in 13 patients. During TTF treatment, epileptic seizures were found in 6 patients, whereas in 2 cases a patient had them before the surgery and in 4 cases epilepsy developed de novo after it. TTFs were administered for the recurrent GBM in a single case only.
If the eligible patient agreed with the initiation of TTF, the service team arranged an appointment, which was usually held in our outpatient department. During this meeting, the technical and everyday aspects were discussed, and the patient and the assistant were trained to operate the device. The service team is available for technical questions around the clock. It was essential, that a person from the patient's household was ready to help in daily activities considering device management. As it is crucial, that the system is active for at least 75% of the time, the automatically generated compliance reports were sent to our center monthly. At the same time, no report concerning the interaction between a patient and the service team was usually available. Of course, any unplanned or urgent visit to our center remained possible.
The daily support was mostly provided by a partner (15/25, 60%), children (5/25, 20%), parents (3/25, 12%), siblings (1/25, 4%), or friends (1/25, 4%). No defined assistant was specified by 23 patients.
No TTF-associated serious adverse effects were reported during the median follow-up of 17 months (IqR: 11–23). No interruption of follow-ups or technical service, hence, TTF application, was noticed due to the COVID-19 pandemic, the associated lock-down, or due to limited access to healthcare facilities.
Mean overall survival inside our cohort according to Kaplan–Meier assessment was 22.6 months (95% CI: 17.3–27.9). IDH-status did not predict OS among patients with TTF therapy, which remained 25.7 months (95% CI: 14.0–37.4) in case of IDH mutation or 20.8 months (95% CI: 15.6–26.1) in case of IDH wild-type tumor, LogRank p = 0.549. At the same time, OS was significantly more favorable in the case of methylated MGMT promoter: 29.7 months (95% CI: 22.4–37.0) vs. 16.7 months (95% CI: 11.4–22.0), LogRank p = 0.002.
Tumor-treating fields are an established option in case of recurrent or newly diagnosed GBM. Their practical and routine application is feasible, nevertheless, some points require attention.
In the PubMed database, 274 results were associated with the term “Tumor-Treating Fields,” showing a strong rise in recent years: 15 papers were published in 2015, 39 papers in 2019, and already 57 in 2021. Nevertheless, more than 80% of them are reviews, preclinical studies or are attributed to non-CNS tumors. Thus, even if TTF as a specific oncological option is widely discussed, the translational and applied experience remains limited.
Tumor-treating fields are the first treatment option in many years, that has shown successful results in GBM therapy (10). It is labeled as the fourth modality in cancer therapy among surgery, systemic pharmacological, and radiation therapy (22).
The EF-11 study from 2012 was performed on 237 patients (1:1 randomization). Even if it did not demonstrate the superiority of TTF compared to the local standard of care in the case of recurrent GBM, the safety and routine feasibility of TTF were proven (17). The pivotal EF-14 trial on 695 patients (2:1 randomization), which was published in 2015 and consistently actualized in 2017, showed a statistically significant overall survival benefit of 4.9 months for patients harboring newly diagnosed GBM. Moreover, 2- and 5-year survival was significantly more favorable in the TTF group compared to the control arm as well – 43 vs. 31% (p < 0.001) and 13 vs. 5% (p = 0.004), respectively (15, 16, 23). According to both studies, the TTF was approved for newly diagnosed and recurrent GBM by FDA and EMA and consequently included in the guidelines (4, 20). Our survival data are concordant to EF-14 published material with comparable overall survival of 22.6 vs. 20.9 months, whereas selection bias in the case of clinical routine could play a role. According to our data, MGMT promoter methylation provides significant additional survival benefits even within the TTF cohort.
In our center, TTF was only applied to a single patient with recurrent GBM. It is known that a prolonged period of time is necessary until TTF effects can be observed (24). In the case of recurrent GBM, the length of therapy remains short and usually consists only of several months, as was shown in the EF-11 and PriDE studies (17, 25).
There are practical advantages of TTF compared to other specific oncological treatment modalities with the noninvasiveness being a key point. Moreover, during hygienic procedures, sports, and MRI the device can be put off. More than one-third of the patient in our cohort were older than 60 years. The feasibility and safety of an elderly population were also shown in the subgroup analysis of the EF-14 study (26). Hence, TTFs are also feasible in the case of an aged population, even when the full dose of radiochemotherapy is not suggested. Another point is that TTF localized treatment allows it to be considered in settings where conventional cytotoxic chemotherapy may be contraindicated due to systemic complications and/or adverse events.
No clinically relevant TTF interaction with the radiotherapy field was found (27). Moreover, TTFs delay DNA damage repair following conventional photon-beam radiotherapy (28) and work as a sensitizer for proton-beam therapy (29). According to the literature, dexamethasone administration does also not interfere with TTF (30).
There were concerns that the COVID-19 pandemic could interfere with the TTF support (31). In our center, however, no interruption of the TTF service and follow-ups were observed.
Even if TTFs are permitted by FDA and EMA, their limitations and potential drawbacks remain intensely discussed. The approval EF-11 and EF-14 studies were open-labeled, thus, providing potential bias. On the other hand, there was no technical possibility to randomize by imitation of the working device, as the arrays cause a superficial warmth sensation. Another potential drawback is the lack of industry-independent validation trials, which, however, is the case for most (pharmaceutical) oncological treatment studies as well. In addition, EF-11 was criticized due to the heterogeneous previous treatment and control population.
We did not observe any severe adverse effects in the routine application of the TTF system. Only skin irritation was reported as a device-related side effect in the EF-11 and EF-14 studies. In 2% of cases, severe local skin damage was described. In the EF-14 trial for newly diagnosed GBM patients, where the treatment exposure was longer than that for recurrent disease, grades 1 and 2 skin reactions were reported in 43% of patients. Similar data were shown during a phase 4 study with 11.000 patients (32). Therefore, sensitivity to the conductive hydrogel, which is used as an adhesive agent for the electrodes, is mentioned as a limitation for starting the therapy. Recently, the prediction algorithm for skin irritation probability was presented. According to it, the variation of array positioning reduced the risk of skin irritation by about one-third (33). Moreover, practical suggestions for dermatological symptomatic treatment have been distributed (34).
We have mentioned that the daily help in routine maintenance of the device from the side of relatives or another assisting person is needed. Every 3-day shaving, application of adhesive electrodes, technical device management, and even contact with the service team is time-consuming. The favorable effect of TTF is magnified if the device is active for more than 18 h per day based on the post-hoc subgroup analysis of the EF-14 trial. Moreover, the survival benefit rises with each added hour (19). Thus, even if a patient showed a high-performance index like KPI 80–100 as in our series, external support remains essential. On the other hand, even if the daily life of patients might be affected by the TTF, two-thirds of them would decide in favor of the treatment (35). The quality of life and TTF acceptance remained high (36, 37). Moreover, the technical upgrade of the device like reduced weight and higher accumulator capacity solved some problems (38).
Another point is the limited data in the case of an implanted CSF shunt or pacemaker that can potentially interfere with TTF. Nevertheless, case reports and a retrospective study demonstrated a high likelihood of to use of TTF devices even in these patients (39, 40), but larger trials would be necessary.
The cost-effectiveness was discussed, as monthly costs of about 20.000e are to be considered (35, 41, 42) and the high price was thought to limit the access to this treatment option (41). Nevertheless, the insurances in the United States and several European countries do cover the routine application of TTF, preventing costs for patients.
Thus, the TTF therapy is nowadays advisable for all patients harboring GBM, including frailty ones, when demanding high-dose radiochemotherapy could not be applied. The efficacy of dexamethasone or radiotherapy is not negatively interfered with. Nevertheless, the external support from relatives and compliance stays crucial. There are also other restrictions like cranial or active implants. Skin irritation does not look to be an inevitable restriction. The summary of positive and negative points considering the TTF application is provided in Table 1.
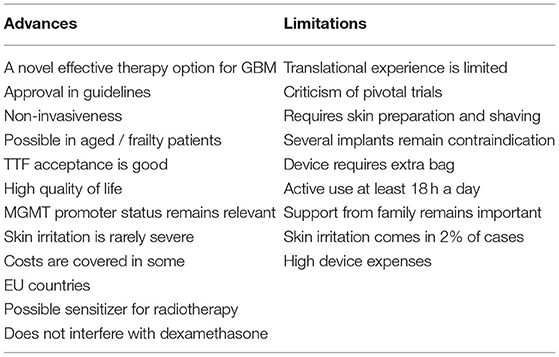
Table 1. Applied advances and limitations of TTF therapy nowadays.
Research regarding further applications of TTF is ongoing. The TRIDENT (EF-32, NCT04471844) study was recently initiated to demonstrate the potential benefits of TTF starting parallel to concomitant radiochemotherapy in the case of newly diagnosed GBM. The feasibility and safety were checked on 10 patients during a phase 1 study (43). The results of an analogous 1:1 randomized phase 2 study (NCT03869242) on 60 patients with an estimated completion date is December 2021 have not been published yet.
The combined treatment option of TTF and bevacizumab (BEV) in the case of recurrent GBM was suggested already in 2014 (44). Nevertheless, the study evaluating concomitant TTF with BEV and hypofractionated stereotactic radiotherapy was abandoned due to poor recruiting in 2019 (NCT01925573). On the other hand, there are reports that BEV with concomitant TTF is applied in an off-label fashion. In one retrospective study, all 48 patients received BEV as monotherapy or in combination with other systemic chemotherapeutics concomitant to TTF. However, due to the lack of a control arm, which would include BEV cases without TTF therapy, no conclusion regarding a potential co-influence of TTF and BEV is possible (45).
According to the guidelines, the treatment strategy in the case of anaplastic glioma is often similar to glioblastoma (4, 20). Nevertheless, the data considering TTF application for anaplastic glioma are limited. Due to the high clinical demand, a respective study is currently ongoing (46).
No sufficient data are available for pediatric cases. According to a case series of 4 patients under 16 (2 of them with GBM) 53–92% compliance without severe adverse effects was described (47). In another publication, the partial response was shown in 5 pediatric high-grade glioma cases (48). Large trials on a pediatric population are ongoing (49).
There is a single spinal glioma case, in which TTF was applied for primary thoracolumbar anaplastic astrocytoma. After decompression surgery and adjuvant chemoradiotherapy, one adhesive array was placed above the tumor projection on the back and another below it. According to the virtual modeling, this way of application provided sufficient TTF power density at the target site (50).
An enhancing effect of TTF after skull remodeling surgery was described. For superficial tumors, removal of a standard craniotomy bone flap increased the electrical field strength by up to 70% (51). A phase 1 safety study on 15 patients with recurrent GBM confirmed the safety of this approach (52) and a phase 2 study was announced (53).
The exact molecular pathways of the TTF effect remain unclear (54). Multiple studies here are ongoing. On the other hand, there is encouraging preclinical data considering increased synergistic efficacy of checkpoint inhibitor anti-PD-1 therapy when combined with TTF. It was demonstrated that the volume of two tumor models declined and the number of cancer-infiltration immune cells raised when TTF was added to the anti-PD-1 therapy (55). Similar results were shown in another study of non-small cell lung cancer (NSCLC), where the concomitant TTF and checkpoint inhibitor treatment led to a decrease in the tumor volume (56).
Tumor-treating field (TTF) application is being investigated also for other solid cancers: the LUNAR trial for lung cancer, HEPANOVA for hepatocellular cancer, INNOVATE-3 for ovarian cancer, PANOVA-3 for pancreatic cancer, and METIS for brain metastasis (57). According to the results of the STELLAR study, a specific device modification is approved by FDA for adult patients harboring unresectable, advanced, and malignant pleural mesothelioma together with standard chemotherapy (58).
Tumor-treating fields are a feasible and routinely applicable specific oncological treatment option in the case of glioblastoma multiforme WHO° IV. As TTF provides additional overall survival, this option should be presented and advised to all GBM patients. Nevertheless, practical restrictions stay relevant, which limit the usage of this modality like insufficient external assistance. Additional work is necessary and is intensely ongoing to extend the indications and the efficacy of TTF and to reduce restrictions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Medical University of Innsbruck. Written informed consent from the patients/participants or patients/participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
AK: acquisition, analysis of data, interpretation of data, and drafting the article. JK, DP, MD, and L-MK: acquisition and interpretation of data. CFF and CT: design of the study and revisions. CFF: conception/design of the study and interpretation of data. All authors have approved the submitted version and have agreed with both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, have been appropriately investigated, resolved, and the resolution documented in the literature.
CFF declares he is participating in a speaker bureau and an advisory board of Novocure.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ostrom QT, Patil N, Cioffi G, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2013-2017. Neuro Oncol. (2020) 22:iv1–1v96. doi: 10.1093/neuonc/noaa200
2. Poon MTC, Sudlow CLM, Figueroa JD, Brennan PM. Longer-term (>/= 2 years) survival in patients with glioblastoma in population-based studies pre- and post-2005: a systematic review and meta-analysis. Sci Rep. (2020) 10:11622. doi: 10.1038/s41598-020-68011-4
3. Weller M, van den Bent M, Hopkins K, Tonn JC, Stupp R, Falini A, et al. European Association for Neuro-Oncology Task Force on Malignant, EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol. (2014) 15:e39515:4t doi: 10.1016/S1470-2045(14)70011-7
4. Wen PY, Weller M, Lee EQ, Alexander BM, Barnholtz-Sloan JS, Barthel FP, et al. Glioblastoma in adults: a Society for Neuro-Oncology (SNO) and European society of neuro-oncology (EANO) consensus review on current management and future directions. Neuro Oncol. (2020) 22:1073–073: doi: 10.1093/neuonc/noaa106
5. Stupp R, Brada M, Van Den Bent MJ, Tonn JC, Pentheroudakis GE. High-grade glioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2014) 25(Suppl 3):iii93–101. doi: 10.1093/annonc/mdu050
6. Stupp R, Hegi ME, Mason WP, Van Den Bent MJ, Taphoorn MJ, Janzer RC, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide vs. radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. (2009) 10 459–66. doi: 10.1016/S1470-2045(09)70025-7
7. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. National Cancer Institute of Canada Clinical Trials, Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma N Engl J Med. (2005) 352:987–96. doi: 10.1056/NEJMoa043330
8. Weller M, Cloughesy T, Perry JR, Wick W. Standards of care for treatment of recurrent glioblastoma–are we there yet? Neuro Oncol. (2013) 15:4Onco doi: 10.1093/neuonc/nos273
9. Chen W, Wang Y, Zhao B, Liu P, Liu L, Wang Y, et al. Optimal therapies for recurrent glioblastoma: a bayesian network meta-analysis. Front Oncol. (2021) 11:641878. doi: 10.3389/fonc.2021.641878
10. M. Penas-Prado. Practice-changing abstracts from the 2016 society for neuro-oncology annual scientific meeting. Am Soc Clin Oncol Educ Book. (2017) 37:187kk B doi: 10.1200/EDBK_175563
11. Carrieri FA, Smack C, Siddiqui I, Kleinberg LR, Tran PT. Tumor treating fields: at the crossroads between physics and biology for cancer treatment. Front Oncol. (2020) 10:575992. doi: 10.3389/fonc.2020.575992
12. Wenger C, Giladi M, Bomzon Z, Salvador R, Basser PJ, Miranda PC. Modeling Tumor Treating Fields (TTFields) application in single cells during metaphase and telophase. Annu Int Conf IEEE Eng Med Biol Soc. (2015) 2015:6892–89 doi: 10.1109/EMBC.2015.7319977
13. Silginer M, Weller M, Stupp R, Roth P. Biological activity of tumor-treating fields in preclinical glioma models. Cell Death Dis. (2017) 8:e2753. doi: 10.1038/cddis.2017.171
14. Gera N, Yang A, Holtzman TS, Lee SX, Wong ET, Swanson KD. Tumor treating fields perturb the localization of septins and cause aberrant mitotic exit. PLoS ONE. (2015) 10:e0125269. doi: 10.1371/journal.pone.0125269
15. Stupp R, Taillibert S, Kanner A, Read W, Steinberg D, Lhermitte B, et al. Effect of tumor-treating fields plus maintenance temozolomide vs. maintenance temozolomide alone on survival in patients with glioblastoma: a randomized clinical trial. JAMA. (2017) 318:2306–306 doi: 10.1001/jama.2017.18718
16. Stupp R, Taillibert S, Kanner AA, Kesari S, Steinberg DM, Toms SA. Maintenance therapy with tumor-treating fields plus temozolomide vs. temozolomide alone for glioblastoma: a randomized clinical trial. JAMA. (2015) 314:2535–535 doi: 10.1001/jama.2015.16669
17. Stupp R, Wong ET, Kanner AA, Steinberg D, Engelhard H, Heidecke V, et al. NovoTTF-100A vs. physician's choice chemotherapy in recurrent glioblastoma: a randomised phase III trial of a novel treatment modality. Eur J Cancer. (2012) 48:2192–192: doi: 10.1016/j.ejca.2012.04.011
18. Lassman AB, Joanta-Gomez AE, Pan PC, Wick W. Current usage of tumor treating fields for glioblastoma. Neurooncol Adv. (2020) 2: vdaa069. doi: 10.1093/noajnl/vdaa069
19. Toms SA, Kim CY, Nicholas G, Ram Z. Increased compliance with tumor treating fields therapy is prognostic for improved survival in the treatment of glioblastoma: a subgroup analysis of the EF-14 phase III trial. J Neurooncol. (2019) 141:467lolp doi: 10.1007/s11060-018-03057-z
20. Nabors LB, Portnow J, Ahluwalia M, Baehring J, Brem H, Brem S, et al. Central nervous system cancers, version 3.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2020) 18:1537–70. doi: 10.6004/jnccn.2020.0052
21. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World health organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. (2016) 131:803ollt doi: 10.1007/s00401-016-1545-1
22. Mun EJ, Babiker HM, Weinberg U, Kirson ED, Von Hoff DD. Tumor-treating fields: a fourth modality in cancer treatment. Clin Cancer Res. (2018) 24:266Res doi: 10.1158/1078-0432.CCR-17-1117
23. Taphoorn MJB, Dirven L, Kanner AA, Lavy-Shahaf G, Weinberg U, Taillibert S, et al. Influence of treatment with tumor-treating fields on health-related quality of life of patients with newly diagnosed glioblastoma: a secondary analysis of a randomized clinical trial. JAMA Oncol. (2018) 4:495colis doi: 10.1001/jamaoncol.2017.5082
24. Zhu P, Zhu JJ. Tumor treating fields: a novel and effective therapy for glioblastoma: mechanism, efficacy, safety and future perspectives. Chin Clin Oncol. (2017) 6:41. doi: 10.21037/cco.2017.06.29
25. Mrugala MM, Engelhard HH, Dinh Tran D, Kew Y, Cavaliere R, Villano JL, et al. Clinical practice experience with NovoTTF-100A system for glioblastoma: the patient registry dataset (PRiDe). Semin Oncol. (2014) 41 Suppl 6:S4–S13. doi: 10.1053/j.seminoncol.2014.09.010
26. Ram Z, Kim CY, Hottinger AF, Idbaih A, Nicholas G, Zhu JJ. Efficacy and safety of tumor treating fields (TTFields) in elderly patients with newly diagnosed glioblastoma: subgroup analysis of the Phase 3 EF-14 clinical trial. Front Oncol. (2021) 11:671972. doi: 10.3389/fonc.2021.671972
27. Straube C, Oechsner M, Kampfer S, Scharl S, Schmidt-Graf F, Wilkens JJ, et al. Dosimetric impact of tumor treating field (TTField) transducer arrays onto treatment plans for glioblastomas - a planning study. Radiat Oncol. (2018) 13:31. doi: 10.1186/s13014-018-0976-3
28. Giladi M, Munster M, Schneiderman RS, Voloshin T, Porat Y, Blat R. Tumor treating fields (TTFields) delay DNA damage repair following radiation treatment of glioma cells. Radiat Oncol. (2017) 12:206. doi: 10.1186/s13014-017-0941-6
29. Lee WS, Seo SJ, Chung HK, Park JW, Kim JK, Kim EH, et al. Tumor-treating fields as a proton beam-sensitizer for glioblastoma therapy. Am J Cancer Res. (2021) 11:4582–94.
30. Linder B, Schiesl A, Voss M, Rodel F, Hehlgans S, Gullulu O, et al. Dexamethasone treatment limits efficacy of radiation, but does not interfere with glioma cell death induced by tumor treating fields. Front Oncol. (2021) 11:715031. doi: 10.3389/fonc.2021.715031
31. Gatson NTN, Barnholtz-Sloan J, Drappatz J, Henriksson R, Hottinger AF, Hinoul P. Tumor treating fields for glioblastoma therapy during the COVID-19 pandemic. Front Oncol. (2021) 11:679702. doi: 10.3389/fonc.2021.679702
32. Shi W, Blumenthal DT, Oberheim Bush NA, Kebir S, Lukas RV, Muragaki Y, et al. Global post-marketing safety surveillance of Tumor Treating Fields (TTFields) in patients with high-grade glioma in clinical practice. J Neurooncol. (2020) 148:489lols doi: 10.1007/s11060-020-03540-6
33. Nour Y, Pottgen C, Kebir S, Lazaridis L, Ludemann L, Guberina M, et al. Dosimetric impact of the positioning variation of tumor treating field electrodes in the PriCoTTF-phase I/II trial. J Appl Clin Med Phys. (2021) 22:242sPhy doi: 10.1002/acm2.13144
34. Lacouture ME, Anadkat MJ, Ballo MT, Iwamoto F, Jeyapalan SA, La Rocca RV M, et al. Prevention and management of dermatologic adverse events associated with tumor treating fields in patients with glioblastoma. Front Oncol. (2020) 10:1045. doi: 10.3389/fonc.2020.01045
35. Onken J, Goerling U, Heinrich M, Pleissner S, Krex D, Vajkoczy P, et al. Patient reported outcome (PRO) among high-grade glioma patients receiving TTFields treatment: a two center observational study. Front Neurol. (2019) 10:1026. doi: 10.3389/fneur.2019.01026
36. Zhu JJ, Demireva P, Kanner AA, Pannullo S, Mehdorn M, Avgeropoulos N, et al. Health-related quality of life, cognitive screening, and functional status in a randomized phase III trial (EF-14) of tumor treating fields with temozolomide compared to temozolomide alone in newly diagnosed glioblastoma. J Neurooncol. (2017) 135:545lole doi: 10.1007/s11060-017-2601-y
37. Onken J, Staub-Bartelt F, Vajkoczy P, Misch M. Acceptance and compliance of TTFields treatment among high grade glioma patients. J Neurooncol. (2018) 139:177lolm doi: 10.1007/s11060-018-2858-9
38. Kinzel A, Ambrogi M, Varshaver M, Kirson ED. Tumor treating fields for glioblastoma treatment: patient satisfaction and compliance with the second-generation optune((R)) system. Clin Med Insights Oncol. (2019) 13:1179554918825449. doi: 10.1177/1179554918825449
39. Kew Y, Oberheim NA. Safety profile of tumor treating fields in adult glioblastoma patients with implanted non-programmable shunts, programmable shunts, and pacemakers/defibrillators: 6-year updated retrospective analysis. Int J Radiation Oncol*Biol*Physics. (2018) 102:e269102. doi: 10.1016/j.ijrobp.2018.07.873
40. McClelland III S, Henrikson CA, Ciporen JN, Jaboin JJ, Mitin T. Tumor treating fields utilization in a glioblastoma patient with a preexisting cardiac pacemaker: the first reported case. World Neurosurg. (2018) 119:58–60. doi: 10.1016/j.wneu.2018.07.162
41. Connock M, Auguste P, Dussart C, Guyotat J, Armoiry X. Cost-effectiveness of tumor-treating fields added to maintenance temozolomide in patients with glioblastoma: an updated evaluation using a partitioned survival model. J Neurooncol. (2019) 143:605lole doi: 10.1007/s11060-019-03197-w
42. Bernard-Arnoux F, Lamure M, Ducray F, Aulagner G, Honnorat J, Armoiry X. The cost-effectiveness of tumor-treating fields therapy in patients with newly diagnosed glioblastoma. Neuro Oncol. (2016) 18:1129–129 doi: 10.1093/neuonc/now102
43. Bokstein F, Blumenthal D, Limon D, Harosh CB, Ram Z, Grossman R. Concurrent tumor treating fields (TTFields) and radiation therapy for newly diagnosed glioblastoma: a prospective safety and feasibility study. Front Oncol. (2020) 10:411. doi: 10.3389/fonc.2020.00411
44. Omar AI. Tumor treating field therapy in combination with bevacizumab for the treatment of recurrent glioblastoma. J Vis Exp. (2014) 27:e51638. doi: 10.3791/51638
45. Lu G, Rao M, Zhu P, Liang B, El-Nazer RT, Fonkem E, et al. Triple-drug therapy with bevacizumab, irinotecan, and temozolomide plus tumor treating fields for recurrent glioblastoma: a retrospective study. Front Neurol. (2019) 10:42. doi: 10.3389/fneur.2019.00042
46. O004290. ctive sacizumab, irinoT, Fu B, Bota D. Actr-41 A phase Ii, Single Arm study of optune® in bevacizumab-naive subjects with recurrent who grade Iii Malignant glioma. Neuro-Oncology. (2016) 18:vi1111i11. doi: 10.1093/neuonc/now212.039
47. Crawford J, Saria MG, Dhall G, Margol A, Kesari S. Feasibility of treating high grade gliomas in children with tumor-treating fields: a case series. Cureus. (2020) 12:e10804. doi: 10.7759/cureus.10804
48. Green AL, Mulcahy Levy JM, Vibhakar R, Hemenway M, Madden J, Foreman N, et al. Tumor treating fields in pediatric high-grade glioma. Childs Nerv Syst. (2017) 33:1043–04 doi: 10.1007/s00381-017-3431-0
49. Makimoto A, Nishikawa R, Terashima K, Kurihara J, Fujisaki H, Ihara S, et al. Tumor-treating fields therapy for pediatric brain tumors. Neurol Int. (2021) 13:151ntie doi: 10.3390/neurolint13020015
50. De Los Santos J, Arvatz S, Zeevi O. Innv-05. Tumor treating fields (Ttfields) treatment planning for a patient with astrocytoma in the spinal cord. Neuro-Oncol. (2020) 22:ii117-ii117. doi: 10.1093/neuonc/noaa215.489
51. Korshoej AR, Saturnino GB, Rasmussen LK, von Oettingen G, Sorensen JC, Thielscher A. Enhancing predicted efficacy of tumor treating fields therapy of glioblastoma using targeted surgical craniectomy: a computer modeling study. PLoS One. (2016) 11:e0164051. doi: 10.1371/journal.pone.0164051
52. Korshoej AR, Lukacova S, Lassen-Ramshad Y, Rahbek C, Severinsen KE, Guldberg TL, et al. OptimalTTF-1: Enhancing tumor treating fields therapy with skull remodeling surgery. A clinical phase I trial in adult recurrent glioblastoma. Neurooncol Adv. (2020) 2:vdaa121. doi: 10.1093/noajnl/vdaa121
53. Mikic N, Poulsen FR, Kristoffersen KB, Laursen RJ, Guldberg TL, Skjøth-Rasmussen J, et al. Study protocol for OptimalTTF-2: enhancing tumor treating fields with skull remodeling surgery for first recurrence glioblastoma: a phase 2, multi-center, randomized, prospective, interventional trial. BMC Cancer. (2021) 21:1010. doi: 10.1186/s12885-021-08709-4
54. Hong P, Kudulaiti N, Wu S, Nie J, Zhuang D. Tumor treating fields: a comprehensive overview of the underlying molecular mechanism. Expert Rev Mol Diag. (2021) 22:19–28. doi: 10.1080/14737159.2022.2017283
55. Voloshin T, Kaynan N, Davidi S, Porat Y, Shteingauz A, Schneiderman RS, et al. Tumor-treating fields (TTFields) induce immunogenic cell death resulting in enhanced antitumor efficacy when combined with anti-PD-1 therapy. Cancer Immunol Immunother. (2020) 69:1191–191: doi: 10.1007/s00262-020-02534-7
56. Weinberg U, Voloshin T, Yitzaki OT, Kaynan N, Giladi M, Shteingauz A, et al. Efficacy of Tumor Treating Fields (TTFields) and anti-PD-1 in non-small cell lung cancer (NSCLC) preclinical models. Annals Oncol. (2017) 28:ii11128 doi: 10.1093/annonc/mdx089.010
57. Available, online at: www.novocure.com, accessed online on 11.12.2021
58. Ceresoli GL, Aerts JG, Dziadziuszko R, Ramlau R, Cedres S, van Meerbeeck JP, et al. Tumor Treating Fields in combination with pemetrexed and cisplatin or carboplatin as first-line treatment for unresectable malignant pleural mesothelioma (STELLAR): a multicentre, single-arm phase 2 trial. Lancet Oncol. (2019) 20:1702–70 doi: 10.1016/S1470-2045(19)30532-7
Keywords: glioblastoma, TTF = tumor-treating field, neurosurgery, neurooncology, combined treatment approach
Citation: Krigers A, Pinggera D, Demetz M, Kornberger L-M, Kerschbaumer J, Thomé C and Freyschlag CF (2022) The Routine Application of Tumor-Treating Fields in the Treatment of Glioblastoma WHO° IV. Front. Neurol. 13:900377. doi: 10.3389/fneur.2022.900377
Received: 20 March 2022; Accepted: 25 April 2022;
Published: 16 June 2022.
Edited by:
Sara Grazia Maria Piccirillo, University of New Mexico Health Sciences Center, United StatesReviewed by:
Antonio Silvani, IRCCS Carlo Besta Neurological Institute Foundation, ItalyCopyright © 2022 Krigers, Pinggera, Demetz, Kornberger, Kerschbaumer, Thomé and Freyschlag. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian F. Freyschlag, Y2hyaXN0aWFuLmZyZXlzY2hsYWdAaS1tZWQuYWMuYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.