
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 14 April 2022
Sec. Pediatric Neurology
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.872469
This article is part of the Research TopicInsights in Pediatric Neurology: 2021View all 20 articles
 Jan Stubberud1,2,3*
Jan Stubberud1,2,3* Ruth Hypher3
Ruth Hypher3 Anne E. Brandt4,5
Anne E. Brandt4,5 Torun G. Finnanger4
Torun G. Finnanger4 Eva Skovlund6
Eva Skovlund6 Stein Andersson1,7
Stein Andersson1,7 Kari Risnes4,5
Kari Risnes4,5 Torstein B. Rø4,5
Torstein B. Rø4,5Objective: Among the variety of domains that may be impacted after pediatric acquired brain injury (pABI) are functional school outcomes. The purpose of this study was to identify demographic, medical, and psychological factors associated with impairments in functional school outcomes, defined as school absence, need of educational and psychological services, quality of life (QoL) in the school setting, and academic performance in children with pABI, with a specific emphasis on the significance of fatigue.
Materials and Method: We used baseline data from a randomized controlled trial. The sample consisted of seventy-six children aged 10 to 17 (M = 13 yrs) with pABI in the chronic phase (>1 year). All completed assessments of school-related QoL, academic performance, global functioning, fatigue, IQ, behavioral problems, and executive function.
Results: Fatigue, IQ, global functioning, behavioral problems, and sex emerged as potential predictors for functional school outcomes. Of note, overall fatigue emerged as the strongest potential predictor for parent-reported QoL in school (β = 0.548; p < 0.001) and self-reported QoL in school (β = 0.532; p < 0.001).
Conclusions: Following pABI, specific psychological, medical, and demographic factors are associated with functional school outcomes. Neither of the injury-related variables age at insult and time since insult were associated with functional school outcomes. Overall, our findings may suggest that a reintroduction to school with personalized accommodations tailored to the child's specific function and symptoms, such as fatigue, is recommended.
Pediatric acquired brain injury (pABI), such as traumatic brain injury (TBI) or non-traumatic injuries (e.g., brain tumor, stroke, hypoxia, or infections /inflammation to the brain), is one of the leading causes of lifelong disabilities in school age children (1, 2). Consequences may include persistent impairments in cognition, emotional health, adaptive behavior, and school functioning (3–11). Functional school outcome is of particular concern, here broadly defined as school absence, aid from Educational and Psychological Service (EPS), quality of life (QoL) in the school setting, and academic performance in children (12, 13). School is the principal location for the development of not only academic skills such as mastering the school curriculum, but also cognitive, social, and community-related skills during childhood. For many, return to school life after pABI represent an indicator of a return to normality (14). However, despite significant improvements in medical treatment after pABI, functional school impairments often emerge over time, for example when returning to school after cancer treatment, and are characterized by poor school performance, high rates of grade retention, and need of external educational services (10, 11, 15–17).
For many children, pABI can be viewed as a chronic disease process that initiates ongoing and possibly lifelong changes that influence several organ systems, physical and sensory limitations, in addition to neurocognitive impairment, emotional distress, and fatigue, that may have a cumulative negative effect on functional school outcome. Indeed, functional school outcomes may be influenced and explained by multiple variables and factors which display the complex and interdependent relationship between demographic [e.g., age and sex; (18, 19)], medical [e.g., injury-related variables such as age at injury, time since injury and functional outcome; (20)], and psychological variables [e.g., IQ, executive function (EF), behavioral problems, fatigue; (9, 21–24)].
Typically, functional school outcome is negatively affected during the initial 6 months after pABI, when compared to healthy children or children with orthopedic injuries (25, 26). While some aspects may improve in the first 6 to 12 months after injury, longitudinal studies indicate significant long-term impairments several years after pABI [e.g., (11)]. Age at injury is also a known predictor of outcome (27). Early injury [i.e., 7 years or younger; (28)], has been associated with poorer neurocognitive functions including IQ, attention, memory and EF, in addition to persisting disability (22, 23, 29, 30).
Importantly, neurocognitive and behavioral impairments may have adverse effects on school outcomes (9, 24). Post-pABI cognitive sequelae include deficits in IQ, attention, EF, memory and learning, and language skills (31–33). In particular, concurrent and longitudinal associations between EF and functional school outcomes have been demonstrated, with EF also being longitudinally predictive of academic difficulties and school dropout (34). Executive functions can be described as distinct, but related, higher-order neurocognitive processes responsible for purposeful, goal-directed behavior (35, 36). Relatedly, children with pABI are at risk for persistent symptoms of behavior problems, with potential debilitating effects on children's long-term functioning [e.g., (9, 26, 33, 37, 38)].
Demographic, medical, and psychological factors are central factors influencing functional school outcomes for children with pABI. However, fatigue has been largely overlooked as a potential predictor of functional school outcomes, despite being described as one of the most universal and debilitating symptoms following pABI (39–41), that may have adverse effects on academic outcomes. The etiology of fatigue after pABI is complex, primarily relating to changes in the central and peripheral nervous system and endocrine disturbances (42, 43). In addition, fatigue is related to exacerbating factors such as emotional disorders and cognitive impairment, and in particular executive dysfunction (42, 44). Previous research suggest that fatigue is associated with decreased QoL, interfering with everyday activities (e.g., social and physical activities) and school function (41, 45–48). There is preliminary evidence to suggest an association between fatigue and unfavorable functional school outcomes (i.e., schoolwork being negatively affected and worse academic performance) (46, 47, 49). Beyond these studies, the associations between fatigue and functional school outcome are scarcely examined in the pABI population. However, studies of other conditions provide support to the relationship; for example, there is evidence showing that fatigue is associated with worse cognitive and academic outcomes in pediatric multiple sclerosis (50), as well as with unfavorable functional outcomes of young adult cancer survivors and stroke patients (51, 52). Similarly, disadvantageous social outcomes relating to employment and substantial government benefits in long-term survivors of pediatric brain tumors have been found to be strongly associated with fatigue and executive dysfunction (31). Furthermore, Berrin et al. (53) observed that fatigue is an important determinant in understanding how diagnostic subtypes of cerebral palsy translates into problems with school functioning.
There are, however, several methodological shortcomings in existing studies on functional school outcome in the field of pABI, such as small sample size, inferior measures of fatigue (e.g., yes/no questions) and too narrow definition and assessment of functional school outcome (e.g., no inclusion of objective functional school data), limiting the generalizability and validity of findings. Importantly, most studies evaluating functional school outcome in the context of post-pABI fatigue have been limited by the use of relatively narrow definitions of functional school outcome, such as describing it merely in terms of school performance/work (46, 47, 49). Beyond performance/work, domains of functioning including QoL in the school setting and objective functional school data, such as information regarding school absence and aid from external educational services, have not been formally investigated in children with pABI. To our knowledge, functional school outcome in relation to fatigue after pABI has only been assessed with questionnaires (46, 47) and interviews addressing school performance/work (54). Notably, no studies have examined the association between fatigue and different categories of specific functional school outcomes, or examined these associations in children aged 10–17 years, including both TBI and non-traumatic brain injuries.
In sum, there is an urgent need to employ a broader, more holistic approach to assessing functional school outcome and identify potential predictors of functional school outcome in children with pABI that may assist in developing evidence based personalized interventions to advance school functioning. Thus, the purpose of this study was to investigate how demographic, medical, and psychological factors, with a specific emphasis on fatigue, are associated with impairments in functional school outcomes in children with pABI. Given the lack in previous studies, the present study will have a more exploratory approach and attempt to answer the following questions:
1. Do Demographic, Medical, and Psychological Factors Predict Impairments in Functional School Outcomes, Indicated by School Absence, aid From the EPS, Self- and Parent Reported QoL in School Setting, and Academic Performance?
2. Do Parent-Reported Fatigue Emerge as a Significant Predictor for any of the Functional School Outcomes?
This cross-sectional study presents baseline data derived from a dual site, evaluator-blinded, parallel group randomized controlled trial (RCT) on the efficacy of cognitive rehabilitation for children and adolescents with pABI (55, 56). The original RCT was preregistered at clinical.trials.gov (NCT03215342), approved by the Regional Committee for Medical and Health Research Ethics (2017/772), Norway, and conducted in accordance with principles of Good Clinical Practice, the Helsinki Declaration and the standards for Ethical Research Involving Children (ChildWatch International and UNICEF).
Seventy-six participants (mean age 13.4 years, SD = 2.3, 57% girls), with pABI resulting from non-traumatic (brain tumor, stroke, hypoxia/anoxia, and brain infections/inflammations; n = 58) and traumatic (TBI; n = 18) injuries, and who were between the age of 10 to 17 years at time of invitation, were recruited from trauma referral centers from the north, mid- and south-east regions of Norway (see Table 1 for demographic and medical characteristics). Information related to the inclusion and exclusion criteria was collected by a semi-structured interview [for more details about the semi-structured interview see (56)]. Inclusion required executive complaints in daily life as determined by a free description of the child‘s function in daily-life and specific EF questions (e.g., “Does the child handle doing more than one thing at the same time? Does the child manage to plan activities? Is the child easily distracted?) in the semi-structured interview, in addition to minimum 12 months since injury/illness or completion of cancer therapy. The exclusion criteria consisted of: (i) pABI before 2 years of age; (ii) cognitive, sensory, physical or language impairment affecting the capacity to attend regular school (i.e., follow educational goals of peers and regular teaching) and/or complete the intervention; (iii) preinjury neurological disease, severe psychiatric disorder and/or stimulant medication; (iv) recently detected brain tumor relapse [see also (56)].
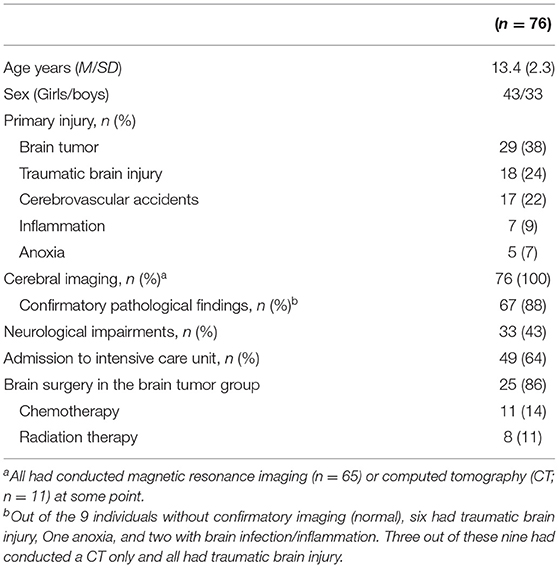
Table 1. Demographic and medical characteristics in study sample.
Potential participants were identified based on discharge diagnosis and received a written invitation (n = 223). In the case of a positive response, written informed consent was obtained from participants (>16 years) or primary caregivers (participants <16 years). Following this, a semi-structured screening interview was conducted to determine eligibility for study inclusion. Parents reported for participants <16 years of age, and participants older than 16 years of age could attend the interview [for more details about the semi-structured interview see (56)]. Ninety-nine individuals were eligible for screening. Out of these, ten participants did not meet inclusion criteria (i.e., 9 with insufficient EF complaints, and 1 was excluded based on information indicating obvious violation of eligibility not previously communicated) and were as such excluded, while two participants declined to participate. Following randomization (n = 87), 76 participants completed a baseline assessment. Pre-inclusion attrition comprised 11 participants (e.g., due to worsening of illness) (see also 57). In the present study, the children were assessed pre-intervention (baseline) at the hospital during one workday by experienced test-technicians, a study nurse, and psychology students (master level) under the supervision of clinical neuropsychologists. To compensate for the potential variation associated with several assessors and to ensure consistent results for the study, a Standard Operating Procedure (SOP) described the protocol and procedures for the assessments, and the test administrators received training from experienced clinical neuropsychologists in addition to being blinded to the type of intervention to be received.
Demographic information, in addition to school absence and aid from EPS, was collected in a structured interview. Medical and injury characteristics were extracted from medical records. This data included brain imaging findings [computerized tomography (CT), magnetic resonance imaging (MRI)] from the first year post injury or disease onset, data regarding admission to intensive care unit, and treatment (e.g., chemotherapy, radiation therapy, brain surgery in brain tumor group). Neurological status (cranial nerve, motor function, balance, sensibility), was obtained in a medical examination by a physician.
School absence was measured by asking parents: “To what degree has your child been absent from school during the last 6 months?” The degree of absence was indicated using the following response set: <10, 10–50 or >50%. Due to a very low number of responses indicating >50%, we ended up using categories <10 and >10% for the present study.
Typically, EPS provides assessments and advice regarding special educational needs in the school setting. In the present study, parents were asked the following question in order to obtain data on EPS aid: “Has your child received any support from EPS?” The following two categories were employed: “no aid” and “current or previous aid.”
Quality of life in the school setting was investigated by employing the 5-item School Functioning subscale from the Pediatric Quality of Life Inventory (PedsQL parent report) (57). The format, instructions, Likert response scale, and scoring method are identical to the PedsQL MFS, with higher scores indicating better QoL in the school setting. Items on the PedsQL school scale assess problems regarding “keeping up with schoolwork,” “paying attention in class,” and “forgetting things.” Furthermore, the scale score has good reliability (α = 0.72) and validity in several health conditions, including pABI (58–60). Finally, good internal consistency (α = 0.93) was demonstrated for the PedsQL (parent) in the present study.
The participants' teachers were administered the Teacher's Report Form ages 6-18 (TRF/6-18) from the Achenbach System of Empirically Based Assessment (ASEBA; 62) to assess the children's academic performance. The TRF/6-18 provide scores for the child's current performance in academic subjects. Here, teachers rate the child's school performance using a 5-point scale ranging from 1 (far below grade level) to 5 (far above grade level) for each academic subject. For adaptive characteristics in school, teachers rate the child on 7-point scales (“Much less,” “Somewhat less,” “Slightly less,” “About average,” “Slightly more,” “Somewhat more,” “Much more”) in four areas: dedication to schoolwork, appropriateness of behavior in school, ability to learn, and happiness. Acceptable internal consistency was found for academic performance (α = 0.72).
Symptoms of fatigue were measured using the 18-item Pediatric Quality of Life Inventory-Multidimensional Fatigue Scale (PedsQL MFS, parent report) (60). It is comprised of three dimensions, General, Sleep/rest and Cognitive fatigue, as well as a total score. The total score was used as outcome in the present study. Items are rated on a 5-point scale (“Never,” “Almost Never,” “Sometimes,” “Often,” and “Almost Always”). Respondents are asked how much of a problem each item have been during the past month (e.g., “feel too tired to spend time with friends”). Items are reverse scored and linearly transformed to a 0–100 scale, so that higher scores indicate better QoL (i.e., less fatigue symptoms). The scale scores of this measure have demonstrated strong evidence of reliability and validity across various pediatric health conditions, including pABI (61–63). In the present study good internal consistency was found for the parent-report (α = 0.93).
Behavioral problems was assessed with the Child Behavior CheckList for ages 6–18 from ASEBA (CBCL/6-18; 62). It consists of 113 questions, scored on a three-point Likert scale (0 = absent, 1= occurs sometimes, 2 = occurs often). Here, a parent is instructed to report on the child's problems. The form yields various subscales and three composite scores, of which Total problems (M = 50, SD = 10), the sum of scores of all the problem items, i.e., behavioral problems, was employed in the present study. The questionnaire has robust psychometric properties with adequate internal consistency (α = 0.82) (64).
The Behavioral Assessment of the Dysexecutive Syndrome for Children (BADS-C; 66) consists of six subtests; the Playing Cards Test, the Water Test, the Key Search Test, Zoo Map Tests 1 and 2, and the Six Part Test. It was developed to reflect different EFs (e.g., shifting, planning and goal-directed behavior, estimation abilities and inhibition) in everyday life and is used as a global measure of EF in the present study. A total age-scaled score is converted to an overall scaled score, ranging from 49 to 146. The scores can be classified functionally like this: impaired performance (overall scaled score range 49–68); borderline performance (overall scaled score range 70–78); low average performance (overall scaled score range 80–88); average performance (overall scaled score range 90–109); high average performance (overall scaled score range 111–119), and superior performance (overall scaled score range 121–146) (65).
Full scale IQ was estimated by using six subscales (i.e., Vocabulary, Similarities, Digit Span, Coding, Block Design and Matrix reasoning) from the Wechsler Intelligence Scale for Children- Fifth Edition (WISC-V) (66). The WISC-V is an individually administered test battery (M = 100, SD = 15, subscales M = 10, SD = 3).
The Glasgow Outcome Scale Extended, pediatric version (GOS-E) is designed to provide a functional outcome, assessing global disability and recovery after brain injury, i.e., inside and outside the home, capacity for work/school, participation in social and leisure activities, and family and peer interactions (67). It consists of a scale with 19 items and eight levels: Level 1 = dead, Level 2 = vegetative state, Level 3 = low severe disability, Level 4 = upper severe disability, Level 5 = low moderate disability, Level 6 = upper moderate disability, Level 7 = low good recovery, and Level 8 = upper good recovery. The GOS-E has demonstrated good psychometric properties (67, 68), and has been found to be strongly associated with functional independence (69).
Frequency distributions, means, medians, standard deviations (SD), and range were calculated for demographic characteristics, potential predictor variables and functional school outcomes (dependent variables). School absence, aid from EPS, QoL in school setting (parent- and self-report), and academic performance were the dependent variables in separate multiple linear regression equations with demographic, medical, and psychological factors as potential predictor variables. Bivariate correlations between potential predictor variables (independent variables) and functional school outcome variables (dependent variables) were computed using Spearman's rho. Variables showing significant correlations (p < 0.05) with the functional school outcome variables were then entered into regression equations. Multiple linear regression models were employed for the continuous dependent variables and logistic regression was used for the dichotomized categorical dependent variables. Preliminary analyses were conducted to ensure no violation of the assumptions of normality, linearity, and homoscedasticity, including Mahalanobis distances to find multivariate outliers (removed if present in each equation) (70). To avoid multicollinearity, independent variables demonstrating correlations of >0.70 with other independent variables were removed from the equation (71). In addition, variance inflation factor and tolerance statistics were checked in relation to collinearity (70). In deciding the strength of the relationships, Cohen's (72) guidelines were employed: r = 0.10 to 0.29 (small), r = 0.30 to 0.49 (moderate), and r > 0.50 (large). All statistical testing used an alpha value of 0.05 (two-tailed). Data analyses were conducted using IBM-SPSS version 26.
Seventy-six participants were included in the present study. Demographic and medical characteristics are summarized in Table 1. Brain tumor was the dominant cause of injury (n = 29), followed by TBI (n = 18), and other etiologies accounted for 29 (38%). Almost all had confirmatory cerebral imaging findings (88%), 43% had clinical neurological findings and 64% had been admitted to an intensive care unit. For the brain tumor group, almost all had conducted brain surgery, 38% had received chemotherapy, and 28% had received radiation therapy.
Scores on potential predictor variables and functional school outcomes are presented in Table 2. The mean age when injured was 8 years (SD = 3.6), ranging from 1 to 15 years of age. Mean time since insult was almost 5 years (SD = 2.7). Regarding global functioning, the GOS-E yielded a mean score of 5.7 (SD = 1.4) placing the majority of the sample in the category “upper moderate disability.” Concerning the PedsQL MFS, the group mean fell below the clinically important cutoff score (<70) (60). The sample displayed general intellectual ability, executive test performance and perceived behavioral functioning within the normal range, i.e., the group mean was within 1.5 SD from the normative scores on the IQ measure (i.e., WISC-V), the executive test (i.e., BADS-C), and the questionnaire CBCL, respectively.
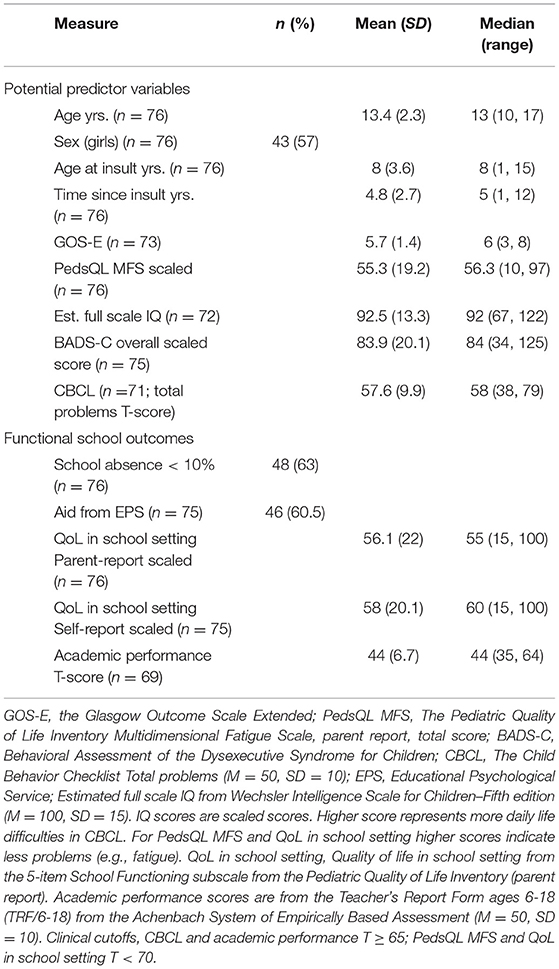
Table 2. Scores on potential predictor variables and functional school outcomes.
As seen in Table 2, a majority (n = 48) had <10% school absence during the last 6 months, and a majority had received aid from EPS (n = 46). The group means for both self- and parent-reports of QoL in school setting were below normal (<70) (60). Finally, academic performance was rated by the participant's teachers to be normal, with a group mean T-score of 44 (SD = 6.7).
Correlations between potential predictors (independent variables) and functional school outcome variables were first examined and are presented in Table 3. Statistically significant correlations are described below, including the strength of the relationships:
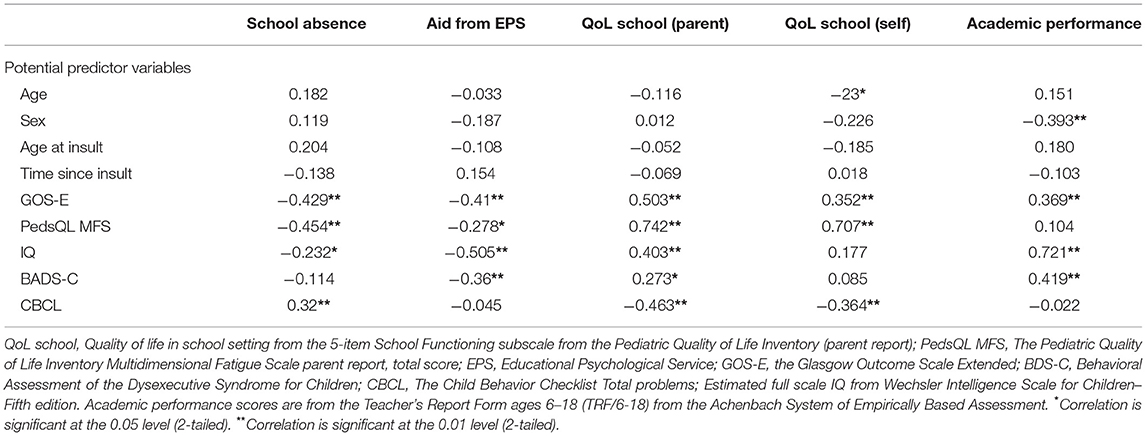
Table 3. Correlations between functional school outcome variables and potential predictor variables.
PedsQL MFS, GOS-E, and IQ were negatively correlated with school absence, indicating that more overall fatigue, lower global functioning, and poorer IQ is associated with less school attendance (p < 0.05). CBCL (total problems) was correlated with school absence, indicating that fewer behavioral problems are associated with higher school attendance (p < 0.01). All correlations between school absence and potential predictors were moderate except IQ (small).
GOS-E, PedsQL MFS, IQ, and BADS-C were negatively correlated with aid from EPS, indicating that that lower global functioning, more fatigue, poorer IQ, and worse EF performance is associated with receiving more support from EPS (p < 0.05). Moreover, all correlations between aid from EPS and potential predictors were moderate except PedsQL MFS (small).
Higher QoL school (parent) scores were significantly associated with higher GOS-E, PedsQL MFS, IQ, and BADS-C scores (p < 0.05), indicating that better parent-reported QoL in the school setting is associated with higher global functioning, lower levels of overall fatigue, higher IQ and better EF performance. Additionally, QoL school scores were negatively associated with CBCL scores, indicating that worse parent-reported QoL in the school setting is associated with more behavioral problems (p < 0.01). All correlations between QoL school (parent) and potential predictors were moderate to large except BADS-C (small).
Higher QoL school (self) scores were significantly associated with higher GOS-E and PedsQL MFS (p < 0.01), indicating that better self-reported QoL in the school setting is associated with higher global functioning and lower levels of overall fatigue. Furthermore, QoL school scores were negatively associated with age and CBCL scores, indicating that poorer self-reported QoL in the school setting is associated with lower age and more behavioral problems (p < 0.05). All correlations between QoL school (self) and potential predictors were moderate to large except age (small).
Academic performance was negatively associated with sex, indicating that better academic performance is associated with being female (p < 0.01). Moreover, GOS-E, IQ, and BADS-C scores were positively correlated with academic performance, indicating that better academic performance is associated with higher global functioning, higher IQ, and better EF performance (p < 0.05). Of note, all correlations between academic performance and potential predictors were moderate to large.
A post-hoc correlation analysis was conducted to further explore the relationship between the PedsQL MFS subscales (General fatigue: M = 58, SD = 22.6; Sleep/rest fatigue: M = 59.2, SD = 23.7; and Cognitive fatigue: M = 49.1. SD = 21.6) and functional school outcomes.
All PedsQL MFS subscales were significantly associated with QoL in school (self and parent) and school absence (p < 0.05), indicating that lower levels of overall fatigue are associated with better parent- and self-reported QoL in the school setting and lower rates of school absence. General and Cognitive fatigue scores were additionally associated with aid from EPS, indicating that less symptoms of General and Cognitive fatigue are associated with less aid from EPS (p < 0.05). All correlations between the PedsQL MFS subscales and potential predictors were moderate to large except between Cognitive fatigue and school absence and Cognitive fatigue and aid from EPS (small).
Potential predictor variables showing significant correlations (p < 0.05) with the functional school outcome variables were entered as independent variables into regression equations, with the functional school outcome variables as the dependent variables (Tables 4–6). When running the model's residual plots as well as normality plots were produced and visually inspected. No violation of the assumptions of normality, linearity, multicollinearity, nor homoscedasticity was detected.
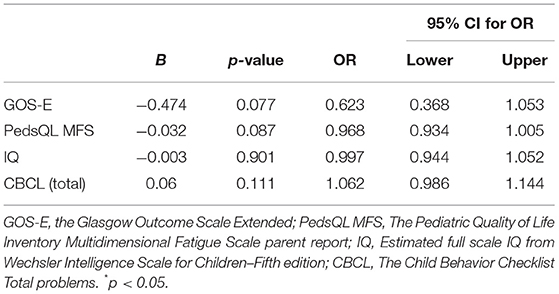
Table 4. Logistic regression predicting likelihood of school absence.
The full model containing all predictors was statistically significant, X2 (4, N = 64) = 17.92, p = 0.001. The model explained between 24.4 % (Cox and Snell R square) and 33.7% (Nagelkerke R square) of the variance in school absence and correctly classified 73.4 % of cases. None of the independent variables made a unique statistically significant contribution to the model (Table 4).
The full model containing all predictors was statistically significant, X2 (4, N = 68) = 21.11, p < 0.001. The model explained between 26.7 % (Cox and Snell R square) and 35.8 % (Nagelkerke R square) of the variance in school absence and correctly classified 75 % of cases. Only IQ made a unique statistically significant contribution to the model [OR.939, 95% CI (0.886, 0.996); Table 5].
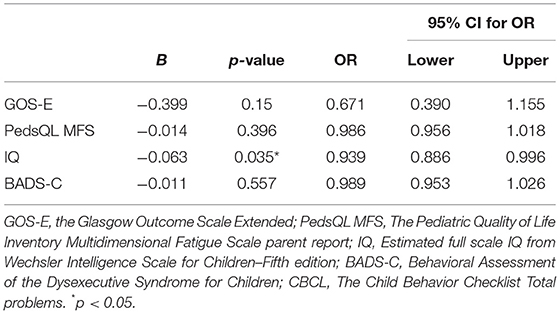
Table 5. Logistic regression predicting likelihood of aid from EPS.
A total of 63% of the variance in QoL school (parent) was explained, F(5, 60) = 23.1; p < 0.001, with PedsQL MFS [β = 0.548; p < 0.00; B 95% CI (2.131, 4.165)], GOS-E [β = 0.206; p < 0.05; B 95% CI (1.669, 29.796)], and CBCL total problems [β = −0.205; p < 0.05; B 95% CI (-1.03, 1.224)] as significant predictors (Table 6).
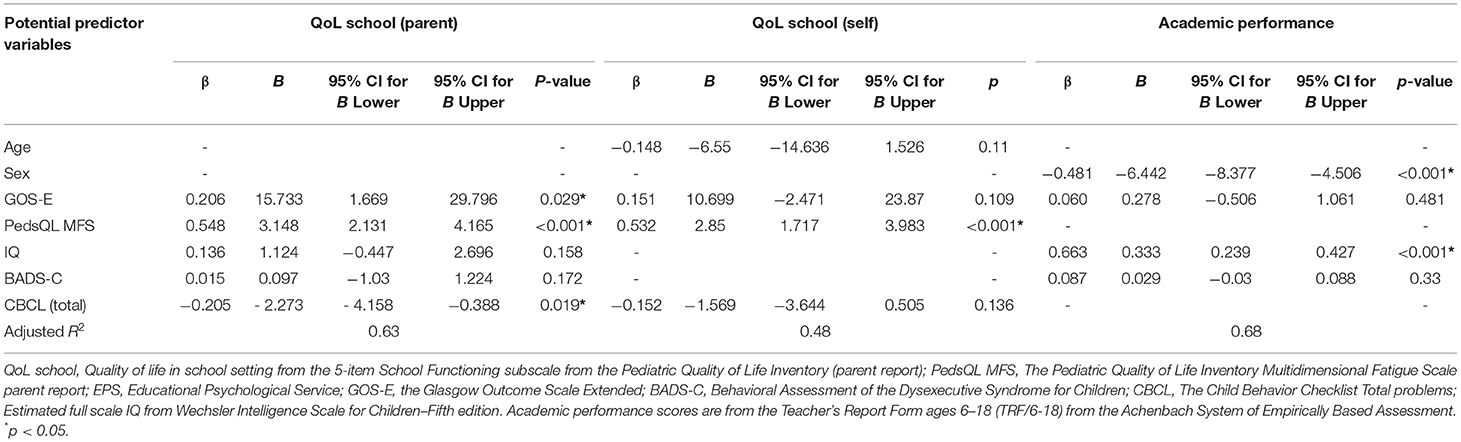
Table 6. Multiple linear regression models with functional school outcome variables as dependent variables and demographic, medical, and psychological factors as independent variables: β, B, CIs, p-values and adjusted R2.
For QoL school (self), 48% of the variance was explained, F(4, 63) = 16.18; p < 0.001, with PedsQL MFS [β = 0.532; p < 0.001; B 95% CI (1.717, 3.983)] as a significant predictor (Table 6).
A total of 68% of the total variance in academic performance was explained, F(4, 63) =34.83; p < 0.001, with IQ [β =0.663; p < 0.001; B 95% CI (0.239, 0.427)] and sex [β = −0.481; p < 0.001; B 95% CI (-8.377,−4.506)] as significant predictors (Table 6).
The aim of this study was to extend our knowledge about the ability of demographic, medical, and psychological factors, and in particular fatigue, to predict different categories of specific functional school outcomes in a pABI sample. The main finding of this study was that these factors were associated with all functional school variables examined, except school absence. Secondly, fatigue made the strongest unique contribution in explaining self- and parent reported QoL in the school setting.
Return to school after pABI may pose several challenges for families and school personnel. The complex constellation of neurocognitive, emotional and physical symptoms can hamper learning and cause increased absence rates. In the present study, fatigue and IQ emerged as the strongest contributors in explaining less favorable functional school outcomes, followed by global functioning, behavior problems and sex. Indeed, fatigue was the strongest contributor for overall QoL in the school setting (including both parent- and self-reports) when the variance explained by all other variables in the models was controlled for. Specifically, greater fatigue severity was associated with poorer school-related QoL. This is a central aspect of school functioning, and to our knowledge, no previous research has demonstrated these specific associations in a pABI sample with different etiologies. Although more conjectural, the post-hoc analysis showing that all dimensions of fatigue (i.e., General, Sleep/rest and Cognitive) were significantly associated with overall QoL in school, suggest that this relationship is driven by several aspects of fatigue. However, a high level of caution is needed in making inferences from the exploratory analyses. In relation to these findings, it is also important to consider the potential overlap in item content between fatigue and QoL measures. The association between fatigue and QoL measures is potentially driving the relationship (i.e., correlations of > 0.7 reported in Table 3). Nevertheless, these findings are in accordance with findings from previous research. Fatigue has been associated with functional school outcomes (i.e., schoolwork being negatively affected and worse school performance) in a variety of pABI types [e.g., (46, 47, 49)]. In addition, post-ABI fatigue has also been associated with health-related QoL, with increased fatigue being associated with greater perceived negative impact of health issues on a range of daily activities in adult ABI populations [e.g., (73)]. In a study by Macartney et al. (49), pediatric brain tumor survivors described how they felt too tired to attend school following pABI, in addition to experiencing cognitive problems (e.g., memory and concentration problems) that contributed to learning difficulties. We were able to extend previous findings by providing preliminary evidence of associations of post-pABI fatigue also being associated with other functional school outcomes (i.e., QoL in the school and school absence), beyond questionnaires and interviews only addressing performance/work employed in previous research [e.g., (46, 47, 49)]. Although none of the independent variables were able to predict school absence, there was a certain trend toward significance for fatigue (p = 0.087), and the post-hoc analysis showed that all dimensions of fatigue (i.e., General, Sleep/rest and Cognitive) were significantly associated with school absence. In a similar vein, the association between fatigue (PedsQL MFS total score) and aid from EPS may primarily be driven by Cognitive and General fatigue. Although speculative, given the exploratory nature of the analyses, these findings might indicate that fatigue also may be associated with school absence. However, our study included only children with reported EF problems in daily life, which may have contributed to a sample with higher levels of fatigue compared to the general pABI population. Moreover, despite fatigue being one of the most common symptoms across ABI conditions, there is no consensus framework, and importantly no single, valid and reliable instrument for the assessment of fatigue due to its subjective and multidimensional nature (41, 74).
IQ emerged as a potential predictor for aid from EPS and academic performance, suggesting that higher IQ is associated with receiving less aid from EPS and better academic performance. This finding was not unexpected when considering that IQ is vital for independent participation in activities such as education, self-care, and later in life, employment and living independently [e.g., (75)]. Notably, there is broad agreement that there is a moderate to strong association between cognitive or general intellectual ability and educational achievement overall (21, 76, 77). The role of EPS is to ensure that expert assessments are prepared when this is necessary, in order to improve the adaptation of the education for pupils with special needs. Special educational needs typically refer to children with learning problems or disabilities that make it more difficult for them to learn compared to most children at the same age (78). The need for this kind of service is less likely when having a higher IQ (21). A high IQ may indicate a good cognitive reserve (i.e., cognitive enrichment) and may as such may be advantageous after a pABI, with less negative behavioral manifestations (79). Of note, many studies have reported that lower cognitive reserve is associated with worse outcomes after ABI [e.g., (80)]. Our findings are also in accordance with a study by Prasad et al. (20) who found that children with TBI have higher rates of school support services than children with orthopedic injuries and healthy comparison children. In a similar vein, Lahteenmaki et al. (81) reported that children who had been treated for cancer had a greater need for help from extra lessons. It is also important to keep in mind that academic performance may be affected by the adverse effect on the learning opportunities caused by neurological changes due to chemotherapy and radiotherapy, and absence from school due to hospitalization.
Global functioning (GOS-E) emerged as a potential predictor for parent-reported QoL in the school setting. Specifically, worse global function after brain injury was associated with poorer school-related QoL. This finding is perhaps not surprising when considering that the GOS-E was designed to provide a global outcome with developmental specificity in the pediatric population, assessing functional status, independence, and participation in relevant societal roles (67). For example, the physical and/or psychological changes caused by cancer treatment can delay a child's return to school, reduce the desire to attend school, and cause more absence from school (82). It is, however, important to keep in mind that the broad categories in GOS-E may inadequately account for the multidimensional nature of pABI outcomes with limited sensitivity to change within specific functional domains (83). The lack of available normative rates of school absence makes it difficult to interpret our findings and understand the extent and implications. Since school is a fundamental context for development, reduced QoL in this context, with the risk of increased absence, has the potential to produce deviations in normal development (84), adding to the existing risk caused by the injury in a developing brain. Acquired brain injuries can disrupt subsequent brain development, causing significant short- and long-term alterations in several functional abilities (4, 33). Interestingly, only parent-reported, not self-reported, QoL in the school setting was associated with global functioning. This can be a result of parents overestimating the impact of global functioning to QoL in the school setting, or that the children underestimate the impact of global functioning, or a combination of the two. It is, however, important to keep in mind that there are several factors that may contribute to the discrepancy between self- and parent reports (85), such as response bias due to parental anxiety or expectations (86), and reduced awareness (87). The nature of self- and parent reporting is complex (88), emphasizing the need of including healthy controls in addition to self- and parent report in future studies.
Children with pABI, and in particular TBI, are at higher risk than non-injured children of behavioral problems, with potential detrimental effects on children's long-term functioning and QoL [e.g., (9)]. There are many studies that provide data for the CBCL as a valid tool to assess co-occurring emotional and behavioral problems in children (89). In the present study, the overall extent of both emotional and behavioral problems (CBCL total behavioral problems) emerged as a potential predictor for parent-reported QoL in school, suggesting that behavioral problems have adverse effects on QoL in school. Of note, behavioral impairments after pABI is common (37), and may negatively impact school performance and educational progress, by hindering both the continued development of current skills and acquisition of new skills (9, 24, 26, 33, 38, 90). For example, behavioral impairments may put children at risk for ineffective interactions with the environment, leading to poor functional school outcome. In fact, emotional ill health in children has been associated with a range of adverse functional school outcomes such as educational failure and higher rates of school absence (91–93). Although not specifically assessed in the present study, it is important to mention that difficulties in emotional regulation are among the most common consequences of ABI, with potential detrimental effects in all life domains [e.g., (5, 94–96)]. Emotional regulation can be described as an important aspect of EF (97). In our study, EF did not emerge as a significant predictor for any of the functional school outcomes. This is somewhat surprising, as EF include cognitive processes such as shifting, inhibition, and updating of working memory (35, 98), processes that are essential to learning, academic achievement, and behavioral competence [e.g., (34, 99, 100)]. However, there is a lack of consensus on the definition of EF, and the assessment of the construct is a known challenge (e.g., “task impurity”) (101, 102). In particular, the highly structured and examiner-guided setting in which the examination takes place (e.g., BADS-C), makes less demand on the child's goal setting, structuring and decision-making abilities than the real-life setting (101, 102).
Finally, sex emerged as a potential predictor for academic performance (academic subjects and adaptive characteristics in school), suggesting that better academic performance is associated with being female. Previous research has shown that boys perform less well in school assessments when compared to girls, despite similar cognitive test scores (103, 104). There are, however, a couple of issues that needs to be considered when discussing these findings. Although the teachers rate the child's school performance for each academic subject it is possible that there are more complex academic skills not captured by the CBCL (e.g., comprehension, written expression). Moreover, for adaptive characteristics in school, teachers rate the child regarding commitment to schoolwork, appropriateness of behavior in school, ability to learn, and happiness. These areas may be difficult to rate, especially when considering the context of many of these children, being survivors of life-threatening insults, in addition to the consequences following pABI that may include changes in emotional, behavioral, and cognitive functions. Hence, further research into this area is warranted.
Surprisingly, neither of the injury-related variables age at insult and time since insult showed significant correlations with functional school outcome variables. This is not in commensurate with previous research whereby age at insult and time since insult has been associated with functional school outcomes (e.g., 25, 26–28). Most of the cited previous research, however, involved TBI samples, while the present sample consisted of different pABI etiologies with brain tumor as the dominant cause of injury. Additionally, since we included children ranging from 1 to 12 years post-injury, they were at different stages in their recovery processes. Relatedly, the impact of developmental factors has not been studied in the present study. A young brain has the capacity for more efficient neural restitution, by neural regrowth and anatomical reorganization (105, 106), in addition to being more vulnerable to more severe, diffuse and persistent impairments after pABI compared to the adult brain (107, 108). Furthermore, previous research has demonstrated that insult severity (e.g., Glasgow Coma Scale) is as a predictor of outcome after TBI [e.g., (7)]. However, a generally accepted categorization of severity in atraumatic insults is lacking. Since there is no widely recognized measure of injury severity across different etiologies, we were unable to explore the potential impact of insult severity in the present study. Although severe psychiatric disorder was an exclusion criterium and the sample as a whole displayed normal behavioral functioning, some of the participants may have concurrent mental disorders such as anxiety, depression, or posttraumatic stress disorder. Hence, it is recommended to examine factors such as developmental factors, insult severity, and concurrent mental disorders in more detail in future studies.
Research evidence on how to optimize the return to school process after pABI is lacking. Our findings may suggest a reintroduction to school with academic accommodations tailored to the child's specific symptoms, such as fatigue and behavioral problems, and global functioning and intellectual ability (e.g., GOS-E and IQ). Importantly, taking a broader approach to assessing functional school outcomes may be necessary to get a more nuanced understanding of the impact of pABI and to help inform targeted strategies that can support a child's successful return to school and improve educational outcomes following pABI.
Strengths of the present study include the large sample size relative to other pABI studies, robust and standardized assessment methods with both child and proxy report and objective functional school data, and the inclusion of both traumatic and non-traumatic brain injuries, increasing the generalizability and validity our findings. However, future research might also want to consider additional fatigue outcomes, such as objective fatigue measures [e.g., (109)]. In addition to the potential overlap in item content between fatigue and QoL measures, factors such as awareness, social desirability bias, response set bias (tendency to respond similarly to all/many items), and over/under reporting of symptoms may influence the accuracy of questionnaire responding. Also, for future research inter-rater reliability should be measured to ensure consistent results. Importantly, our results are based on correlational analyses and self/parent reports, so it cannot be definitively determined whether described predictors had a direct causal impact on the functional school outcomes. In the present study we focused on a restricted number of outcomes. However, there are other variables of interest that may be considered for future research that could impact school outcomes and/or performance on cognitive assessments, such as sleep, pain, parental health and education, other psychosocial and medical variables (e.g., depression, health-related quality of life, social function). Importantly, the present study did not explore the potential impact of injury severity. This should be investigated in future studies. Data regarding level of TBI, type of tumor, cause of cerebrovascular accidents or anoxia should also be collected in future research to better describe the sample. Another important limitation in the present study is that only participants with reported executive difficulties were included, with all being motivated for a cognitive rehabilitation intervention addressing cognitive difficulties. Perceived executive dysfunction may have contributed to a higher fatigue load in the sample. Awareness questionnaires should be considered for future studies. Moreover, a larger sample size may allow for analyses exploring potential between- and within-injury differences. Given the novelty of the study, with very few studies that have examined functional school outcomes and fatigue in a pABI context, a more exploratory approach was employed to the statistical analyses; we did not correct for multiple comparisons. Accordingly, our selection of predictors exceed the recommended predictor/sample size ratio (71). Hence, cautious interpretation of findings is necessitated by the exploratory nature of the analyses and design of the study. Relatedly, regression analyses in a cross-sectional design study with a limited sample also necessitates caution when interpreting findings. Regarding the generalizability of our findings outside of Norway; the participants were recruited from trauma referral centers from the north, mid- and south-east regions of Norway (nationwide), which allows us to generalize the results to other countries with a healthcare and school system comparable to the Norwegian, e.g., the Nordic countries. A potential advantage to our study is that factors such as race, ethnicity, socioeconomic status, health insurance status, care access (rural/urban), and school access/quality inequities do not play a large role in health outcomes in Norway (110). Finally, the cross-sectional design of our study prevents investigation of the trajectory of functional school outcome over time in addition to factors that might influence change in school outcome over time. To expound these matters, future research could include a larger sample and longitudinal methods to examine the course of predictors and school outcomes over time.
Following pABI, fatigue, IQ, global functioning, behavioral problems, and sex is associated with functional school outcomes. This may suggest that a reintroduction to school with personalized adaptations to the child's specific symptoms, such as fatigue and behavioral problems, and global outcome and intellectual ability is recommended. Importantly, fatigue represents a potentially modifiable treatment target for children with pABI and may, in turn, improve functional school outcome. Finally, out findings support a recommendation to employ a broad approach with information from different sources when assessing functional school outcome to obtain a more comprehensive understanding of pABI.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Regional Committees for Medical and Health Research Ethics, Norway. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
JS, RH, AB, TF, ES, SA, KR, and TR have developed study protocol for this study. JS wrote the article with input from all authors. All authors contributed to the final manuscript, including final approval of the version published. Finally, all authors have agreed to be accountable for all aspects of the work.
This work was supported by the Norwegian Research Council [Grant Number 260680/H10].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the participants and their families, Head of Clinics, patient advisers, and the staff at St. Olavs Hospital, Trondheim University Hospital and Oslo University Hospital for their participation and support. We would especially thank our research nurses, occupational therapists test-technicians, neuropsychologists and pediatricians involved in this study. We also would like to thank the Unit for Applied Clinical Research, Norwegian University of Science and Technology (NTNU) responsible for the monitoring and developing the webCRF.
1. Langlois JA, Rutland-Brown W, Thomas KE. The incidence of traumatic brain injury among children in the United States: differences by race. J Head Trauma Rehabil. (2005) 20:229–38. doi: 10.1097/00001199-200505000-00006
2. Thurman DJ. The epidemiology of traumatic brain injury in children and youths: a review of research since 1990. J Child Neurol. (2016) 31:20–7. doi: 10.1177/0883073814544363
3. Anderson V, Catroppa C. Advances in postacute rehabilitation after childhood-acquired brain injury: a focus on cognitive, behavioral, and social domains. Am J Phys Med Rehabil. (2006) 85:767–78. doi: 10.1097/01.phm.0000233176.08480.22
4. Ryan NP, Anderson V, Godfrey C, Beauchamp MH, Coleman L, Eren S, et al. Predictors of very-long-term sociocognitive function after pediatric traumatic brain injury: evidence for the vulnerability of the immature “social brain”. J Neurotrauma. (2014) 31:649–57. doi: 10.1089/neu.2013.3153
5. Ponsford JL, Downing MG, Olver J, Ponsford M, Acher R, Carty M, et al. Longitudinal follow-up of patients with traumatic brain injury: outcome at two, five, and ten years post-injury. J Neurotrauma. (2014) 31:64–77. doi: 10.1089/neu.2013.2997
6. Beauchamp M, Anderson V. Cognitive and psychopathological sequelae of pediatric traumatic brain injury. Handb Clin Neurol. (2013) 112:913–20. doi: 10.1016/B978-0-444-52910-7.00013-1
7. Catroppa C, Anderson V. Traumatic brain injury in childhood: rehabilitation considerations. Dev Neurorehabil. (2009) 12:53–61. doi: 10.1080/17518420802634476
8. Karver CL, Wade SL, Cassedy A, Taylor HG, Stancin T, Yeates KO, et al. Age at injury and long-term behavior problems after traumatic brain injury in young children. Rehabil Psychol. (2012) 57:256. doi: 10.1037/a0029522
9. Li L, Liu J. The effect of pediatric traumatic brain injury on behavioral outcomes: a systematic review. Dev Med Child Neurol. (2013) 55:37–45. doi: 10.1111/j.1469-8749.2012.04414.x
10. Ewing-Cobbs L, Fletcher JM, Levin HS, Iovino I, Miner ME. Academic achievement and academic placement following traumatic brain injury in children and adolescents: a two-year longitudinal study. J Clin Exp Neuropsychol. (1998) 20:769–81. doi: 10.1076/jcen.20.6.769.1109
11. Jaffe KM, Polissar NL, Fay GC, Liao S. Recovery trends over three years following pediatric traumatic brain injury. Arch Phys Med Rehabil. (1995) 76:17–26. doi: 10.1016/S0003-9993(95)80037-9
12. Cortes Pascual A, Moyano Munoz N, Quilez Robres A. The relationship between executive functions and academic performance in primary education: review and meta-analysis. Front Psychol. (2019) 10:1582. doi: 10.3389/fpsyg.2019.01582
13. Knight SJ, Politis J, Garnham C, Scheinberg A, Tollit MA. School functioning in adolescents with chronic fatigue syndrome. Front Pediatr. (2018) 6:302. doi: 10.3389/fped.2018.00302
14. Bradley Eilertsen ME, Jozefiak T, Rannestad T, Indredavik MS, Vik T. Quality of life in children and adolescents surviving cancer. Eur J Oncol Nurs. (2012) 16:185–93. doi: 10.1016/j.ejon.2011.08.001
15. Dollman AK, Figaji AA, Schrieff-Elson LE. Academic and behavioral outcomes in school-age South African children following severe traumatic brain injury. Front Neuroanat. (2017) 11:121. doi: 10.3389/fnana.2017.00121
16. Bruce BS, Chapman A, MacDonald A, Newcombe J. School experiences of families of children with brain tumors. J Pediatr Oncol Nurs. (2008) 25:331–9. doi: 10.1177/1043454208323619
17. Bonneau J, Lebreton J, Taque S, Chappe C, Bayart S, Edan C, et al. School performance of childhood cancer survivors: mind the teenagers! J Pediatr. (2011) 158:135–41. doi: 10.1016/j.jpeds.2010.07.008
18. Navarro JJ, Garcia-Rubio J, Olivares PR. The relative age effect and its influence on academic performance. PLoS ONE. (2015) 10:e0141895. doi: 10.1371/journal.pone.0141895
19. Denham SA, Bassett HH, Thayer SK, Mincic MS, Sirotkin YS, Zinsser K. Observing preschoolers' social-emotional behavior: structure, foundations, and prediction of early school success. J Genet Psychol. (2012) 173:246–78. doi: 10.1080/00221325.2011.597457
20. Prasad MR, Swank PR, Ewing-Cobbs L. Long-term school outcomes of children and adolescents with traumatic brain injury. J Head Trauma Rehabil. (2017) 32:E24–32. doi: 10.1097/HTR.0000000000000218
21. Deary IJ, Strand S, Smith P, Fernandes C. Intelligence and educational achievement. Intelligence. (2007) 35:13–21. doi: 10.1016/j.intell.2006.02.001
22. Anderson V, Catroppa C, Morse S, Haritou F, Rosenfeld J. Functional plasticity or vulnerability after early brain injury? Pediatrics. (2005) 116:1374–82. doi: 10.1542/peds.2004-1728
23. Grimwood K, Anderson P, Anderson V, Tan L, Nolan T. Twelve year outcomes following bacterial meningitis: further evidence for persisting effects. Arch Dis Child. (2000) 83:111–6. doi: 10.1136/adc.83.2.111
24. Babikian T, Asarnow R. Neurocognitive outcomes and recovery after pediatric TBI: meta-analytic review of the literature. Neuropsychology. (2009) 23:283–96. doi: 10.1037/a0015268
25. Ewing-Cobbs L, Prasad MR, Kramer L, Cox CS, Baumgartner J, Fletcher S, et al. Late intellectual and academic outcomes following traumatic brain injury sustained during early childhood. J Neurosurg. (2006) 105:287–96. doi: 10.3171/ped.2006.105.4.287
26. Fulton JB, Yeates KO, Taylor HG, Walz NC, Wade SL. Cognitive predictors of academic achievement in young children 1 year after traumatic brain injury. Neuropsychology. (2012) 26:314–22. doi: 10.1037/a0027973
27. Taylor HG, Alden J. Age-related differences in outcomes following childhood brain insults: an introduction and overview. J Int Neuropsychol Soc. (1997) 3:555–67. doi: 10.1017/S1355617797005559
28. Anderson V, Moore C. Age at injury as a predictor of outcome following pediatric head injury: a longitudinal perspective. Child Neuropsychology. (1995) 1:187–202. doi: 10.1080/09297049508400224
29. Verger K, Junqué C, Jurado MA, Tresserras P, Bartumeus F, Nogués P, et al. Age effects on long-term neuropsychological outcome in paediatric traumatic brain injury. Brain Inj. (2000) 14:495–503. doi: 10.1080/026990500120411
30. Radcliffe J, Bunin GR, Sutton LN, Goldwein JW, Phillips PC. Cognitive deficits in long-term survivors of childhood medulloblastoma and other noncortical tumors: age-dependent effects of whole brain radiation. Int J Dev Neurosci. (1994) 12:327–34. doi: 10.1016/0736-5748(94)90081-7
31. Puhr A, Ruud E, Anderson V, Due-Tønnessen BJ, Skarbø AB, Finset A, et al. Social attainment in physically well-functioning long-term survivors of pediatric brain tumour; the role of executive dysfunction, fatigue, and psychological and emotional symptoms. Neuropsychol Rehabil. (2021) 31:129–53. doi: 10.1080/09602011.2019.1677480
32. Rey-Casserly C, Diver T. Late effects of pediatric brain tumors. Curr Opin Pediatr. (2019) 31:789–96. doi: 10.1097/MOP.0000000000000837
33. Babikian T, Merkley T, Savage RC, Giza CC, Levin H. Chronic aspects of pediatric traumatic brain injury: review of the literature. J Neurotrauma. (2015) 32:1849–60. doi: 10.1089/neu.2015.3971
34. Spiegel JA, Goodrich JM, Morris BM, Osborne CM, Lonigan CJ. Relations between executive functions and academic outcomes in elementary school children: a meta-analysis. Psychol Bull. (2021) 147:329–51. doi: 10.1037/bul0000322
35. Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn Psychol. (2000) 41:49–100. doi: 10.1006/cogp.1999.0734
36. Friedman NP, Miyake A. Unity and diversity of executive functions: Individual differences as a window on cognitive structure. Cortex. (2017) 86:186–204. doi: 10.1016/j.cortex.2016.04.023
37. Catroppa C, Godfrey C, Rosenfeld JV, Hearps SS, Anderson VA. Functional recovery ten years after pediatric traumatic brain injury: outcomes and predictors. J Neurotrauma. (2012) 29:2539–47. doi: 10.1089/neu.2012.2403
38. Jonsson CA, Catroppa C, Godfrey C, Smedler AC, Anderson V. Cognitive recovery and development after traumatic brain injury in childhood: a person-oriented, longitudinal study. J Neurotrauma. (2013) 30:76–83. doi: 10.1089/neu.2012.2592
39. Gagner C, Landry-Roy C, Lainé F, Beauchamp MHJJoN. Sleep-wake disturbances and fatigue after pediatric traumatic brain injury: a systematic review of the literature. J Neurotrauma. (2015) 32:1539–52. doi: 10.1089/neu.2014.3753
40. Wilkinson J, Marmol NL, Godfrey C, Wills H, van Eijndhoven Q, Botchway EN, et al. Fatigue following paediatric acquired brain injury and its impact on functional outcomes: a systematic review. Neuropsychol Rev. (2018) 28:73–87. doi: 10.1007/s11065-018-9370-z
41. Crichton A, Knight S, Oakley E, Babl FE, Anderson V. Fatigue in child chronic health conditions: a systematic review of assessment instruments. Pediatrics. (2015) 135:e1015–31. doi: 10.1542/peds.2014-2440
42. Armstrong TS, Cron SG, Bolanos EV, Gilbert MR, Kang DH. Risk factors for fatigue severity in primary brain tumor patients. Cancer. (2010) 116:2707–15. doi: 10.1002/cncr.25018
43. Kluger BM, Krupp LB, Enoka RM. Fatigue and fatigability in neurologic illnesses: proposal for a unified taxonomy. Neurology. (2013) 80:409–16. doi: 10.1212/WNL.0b013e31827f07be
44. van Markus-Doornbosch F, de Kloet AJ, Berger MA, Lambregts SA, Wolterbeek R, Vliet Vlieland TP. Factors related to fatigue after paediatric acquired brain injury (ABI). Brain Inj. (2016) 30:1533–41. doi: 10.1080/02699052.2016.1197968
45. Meeske K, Katz ER, Palmer SN, Burwinkle T, Varni JW. Parent proxy-reported health-related quality of life and fatigue in pediatric patients diagnosed with brain tumors and acute lymphoblastic leukemia. Cancer. (2004) 101:2116–25. doi: 10.1002/cncr.20609
46. Borg J, Christie D, Coen PG, Booy R, Viner RM. Outcomes of meningococcal disease in adolescence: prospective, matched-cohort study. Pediatrics. (2009) 123:e502–9. doi: 10.1542/peds.2008-0581
47. Eisenberg MA, Meehan WP, Mannix R. Duration and course of post-concussive symptoms. Pediatrics. (2014) 133:999–1006. doi: 10.1542/peds.2014-0158
48. Hypher R, Andersson S, Finnanger TG, Brandt AE, Hoorelbeke K, Lie HC, et al. Fatigue following pediatric acquired brain injury: Interplay with associated factors in a clinical trial population compared to healthy controls. Neuropsychology. (2021) 35:609–21. doi: 10.1037/neu0000753
49. Macartney G, Stacey D, Harrison MB, VanDenKerkhof E. Symptoms, coping, and quality of life in pediatric brain tumor survivors: a qualitative study. Oncol Nurs Forum. (2014) 41:390–8. doi: 10.1188/14.ONF.390-398
50. Goretti B, Portaccio E, Ghezzi A, Lori S, Moiola L, Falautano M, et al. Fatigue and its relationships with cognitive functioning and depression in paediatric multiple sclerosis. Mult Scler J. (2012) 18:329–34. doi: 10.1177/1352458511420846
51. Langeveld N, Ubbink M, Smets EJEJoON. ‘I don't have any energy': the experience of fatigue in young adult survivors of childhood cancer. Eur J Oncol Nurs. (2000) 4:20–8. doi: 10.1054/ejon.1999.0063
52. Naess H, Nyland HI, Thomassen L, Aarseth J, Myhr KM. Fatigue at long-term follow-up in young adults with cerebral infarction. Cerebrovasc Dis. (2005) 20:245–50. doi: 10.1159/000087706
53. Berrin SJ, Malcarne VL, Varni JW, Burwinkle TM, Sherman SA, Artavia K, et al. Pain, fatigue, and school functioning in children with cerebral palsy: a path-analytic model. J Pediatr Psychol. (2006) 32:330–7. doi: 10.1093/jpepsy/jsl017
54. Macartney G, Harrison MB, VanDenKerkhof E, Stacey D, McCarthy P. Quality of life and symptoms in pediatric brain tumor survivors: a systematic review. J Pediatr Oncol Nurs. (2014) 31:65–77. doi: 10.1177/1043454213520191
55. Hypher RE, Brandt AE, Risnes K, Ro TB, Skovlund E, Andersson S, et al. Paediatric goal management training in patients with acquired brain injury: study protocol for a randomised controlled trial. BMJ Open. (2019) 9:e029273. doi: 10.1136/bmjopen-2019-029273
56. Brandt AE, Finnanger TG, Hypher RE, Ro TB, Skovlund E, Andersson S, et al. Rehabilitation of executive function in chronic paediatric brain injury: a randomized controlled trial. BMC Med. (2021) 19:253. doi: 10.1186/s12916-021-02129-8
57. Varni JW, Seid M, Kurtin PS. PedsQL 4. 0: reliability and validity of the Pediatric Quality of Life Inventory version 40 generic core scales in healthy and patient populations. Med Care. (2001) 39:800–12. doi: 10.1097/00005650-200108000-00006
58. Varni JW, Brown J, Seid M, Szer IS. The PedsQL as a patient-reported outcome in children and adolescents with fibromyalgia: An analysis of OMERACT domains. Health Qual Life Outcomes. (2007). 5, 9. doi: 10.1186/1477-7525-5-9
59. McCarthy ML, MacKenzie EJ, Durbin DR, Aitken ME, Jaffe KM, Paidas CN, et al. The Pediatric Quality of Life Inventory: an evaluation of its reliability and validity for children with traumatic brain injury. Arch Phys Med Rehabil. (2005) 86:1901–9. doi: 10.1016/j.apmr.2005.03.026
60. Varni JW, Limbers CA. The pediatric quality of life inventory: measuring pediatric health-related quality of life from the perspective of children and their parents. Pediatr Clin North Am. (2009) 56:843–63. doi: 10.1016/j.pcl.2009.05.016
61. Crichton AJ, Babl F, Oakley E, Greenham M, Hearps S, Delzoppo C, et al. Prediction of multidimensional fatigue after childhood brain injury. J Head Trauma Rehabil. (2017) 32:107–16. doi: 10.1097/HTR.0000000000000248
62. Panepinto JA, Torres S, Bendo CB, McCavit TL, Dinu B, Sherman-Bien S, et al. PedsQL™ multidimensional fatigue scale in sickle cell disease: feasibility, reliability, and validity. Pediatr Blood Cancer. (2014) 61:171–7. doi: 10.1002/pbc.24776
63. Varni JW, Beaujean AA, Limbers CA. Factorial invariance of pediatric patient self-reported fatigue across age and gender: a multigroup confirmatory factor analysis approach utilizing the PedsQL™ multidimensional fatigue scale. Qual Life Res. (2013) 22:2581–94. doi: 10.1007/s11136-013-0370-4
64. Achenbach TM, Rescorla LA. Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families (2001).
65. Emslie H, Wilson FC, Burden V, Nimmo-Smith I, Wilson BA. Behavioural Assessment of the Dysexecutive Syndrome for Children (BADS-C). London: Harcourt Assessment/The Psychological Corporation (2003).
66. Wechsler D. Wechsler Intelligence Scale for Children - Fifth Edition. London, TX: San Antonio: Psychological Corporation (2014).
67. Davis KC, Slomine BS, Salorio CF, Suskauer SJ. Time to follow commands and duration of posttraumatic amnesia predict gos-e peds scores 1 to 2 years after TBI in children requiring inpatient rehabilitation. J Head Trauma Rehabil. (2016) 31:E39–47. doi: 10.1097/HTR.0000000000000159
68. Beers SR, Wisniewski SR, Garcia-Filion P, Tian Y, Hahner T, Berger RP, et al. Validity of a pediatric version of the glasgow outcome scale-extended. J Neurotrauma. (2012) 29:1126–39. doi: 10.1089/neu.2011.2272
69. Hernandez AM, Oscarson B, Combs K, Stavinoha PL. Relationship of GOS-E peds to functional and cognitive outcome measures after pediatric TBI. J Head Trauma Rehabil. (2015) 3.
70. Field A. Discovering Statistics Using IBM SPSS Statistics. 5th ed. London: SAGE Publications (2017).
71. Tabachnick B, Fidell L. Using Multivariate Statistics. 4th ed. Boston, MA: Allyn and Bacon (2001).
72. Cohen J. Statistical Power Analysis For the Behavioral Sciences. 2nd ed. Hillsdale, NJ: L. Erlbaum Associates (1988). p. 567.
73. Cantor JB, Ashman T, Gordon W, Ginsberg A, Engmann C, Egan M, et al. Fatigue after traumatic brain injury and its impact on participation and quality of life. J Head Trauma Rehabil. (2008) 23:41–51. doi: 10.1097/01.HTR.0000308720.70288.af
74. Chaudhuri A, Behan PO. Fatigue in neurological disorders. Lancet. (2004) 363:978–88. doi: 10.1016/S0140-6736(04)15794-2
75. Yin Foo R, Guppy M, Johnston LM. Intelligence assessments for children with cerebral palsy: a systematic review. Dev Med Child Neurol. (2013) 55:911–8. doi: 10.1111/dmcn.12157
76. Bartels M, Rietveld MJ, Van Baal GC, Boomsma DI. Heritability of educational achievement in 12-year-olds and the overlap with cognitive ability. Twin Res. (2002) 5:544–53. doi: 10.1375/136905202762342017
77. Mackintosh NJ. IQ and Human Intelligence. 2nd ed. Oxford, NY: Oxford University Press (2011). p. 440.
78. Black A. A Picture of special educational needs in England – an overview. Front Educ. (2019) 4:79. doi: 10.3389/feduc.2019.00079
79. Donders J, Stout J. The influence of cognitive reserve on recovery from traumatic brain injury. Arch Clin Neuropsychol. (2019) 34:206–13. doi: 10.1093/arclin/acy035
80. Oldenburg C, Lundin A, Edman G, Nygren-de Boussard C, Bartfai A. Cognitive reserve and persistent post-concussion symptoms–A prospective mild traumatic brain injury (mTBI) cohort study. Brain Inj. (2016) 30:146–55. doi: 10.3109/02699052.2015.1089598
81. Lahteenmaki PM, Harila-Saari A, Pukkala EI, Kyyronen P, Salmi TT, Sankila R. Scholastic achievements of children with brain tumors at the end of comprehensive education: a nationwide, register-based study. Neurology. (2007) 69:296–305. doi: 10.1212/01.wnl.0000265816.44697.b4
82. Buizer AI, de Sonneville LM, Veerman AJ. Effects of chemotherapy on neurocognitive function in children with acute lymphoblastic leukemia: a critical review of the literature. Pediatr Blood Cancer. (2009) 52:447–54. doi: 10.1002/pbc.21869
83. Maas AIR, Menon DK, Adelson PD, Andelic N, Bell MJ, Belli A, et al. Traumatic brain injury: integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. (2017) 16:987–1048. doi: 10.1016/S1474-4422(17)30371-X
84. Lomholt JJ, Johnsen DB, Silverman WK, Heyne D, Jeppesen P, Thastum M. Feasibility study of back2school, a modular cognitive behavioral intervention for youth with school attendance problems. Front Psychol. (2020) 11:586. doi: 10.3389/fpsyg.2020.00586
85. Camara-Costa H, Francillette L, Opatowski M, Toure H, Brugel D, Laurent-Vannier A, et al. Self- and parent-reported fatigue 7 years after severe childhood traumatic brain injury: results of the traumatisme grave de l'enfant prospective longitudinal study. J Head Trauma Rehabil. (2020) 35:104–16. doi: 10.1097/HTR.0000000000000502
86. Sato I, Higuchi A, Yanagisawa T, Mukasa A, Ida K, Sawamura Y, et al. Factors influencing self- and parent-reporting health-related quality of life in children with brain tumors. Qual Life Res. (2013) 22:185–201. doi: 10.1007/s11136-012-0137-3
87. Krasny-Pacini A, Limond J, Evans J, Hiebel J, Bendjelida K, Chevignard M. Self-awareness assessment during cognitive rehabilitation in children with acquired brain injury: a feasibility study and proposed model of child anosognosia. Disabil Rehabil. (2015) 37:2092–106. doi: 10.3109/09638288.2014.998783
88. de Ruiter MA. Schouten-van Meeteren AYN, van Vuurden DG, Maurice-Stam H, Gidding C, Beek LR, et al. Psychosocial profile of pediatric brain tumor survivors with neurocognitive complaints. Qual Life Res. (2016) 25:435–46. doi: 10.1007/s11136-015-1091-7
89. Biederman J, Petty CR, Fried R, Wozniak J, Micco JA, Henin A, et al. Child behavior checklist clinical scales discriminate referred youth with autism spectrum disorder: a preliminary study. J Dev Behav Pediatr. (2010) 31:485–90. doi: 10.1097/DBP.0b013e3181e56ddd
90. Keenan HT, Bratton SL. Epidemiology and outcomes of pediatric traumatic brain injury. Dev Neurosci. (2006) 28:256–63. doi: 10.1159/000094152
91. Finning K, Ukoumunne OC, Ford T, Danielsson-Waters E, Shaw L, Romero De Jager I, et al. The association between child and adolescent depression and poor attendance at school: a systematic review and meta-analysis. J Affect Disord. (2019) 245:928–38. doi: 10.1016/j.jad.2018.11.055
92. Finning K, Ukoumunne OC, Ford T, Danielson-Waters E, Shaw L, Romero De Jager I, et al. Review: the association between anxiety and poor attendance at school - a systematic review. Child Adolesc Ment Health. (2019) 24:205–16. doi: 10.1111/camh.12322
93. Egger HL, Costello EJ, Angold A. School refusal and psychiatric disorders: a community study. J Am Acad Child Adolesc Psychiatry. (2003) 42:797–807. doi: 10.1097/01.CHI.0000046865.56865.79
94. Konrad C, Geburek AJ, Rist F, Blumenroth H, Fischer B, Husstedt I, et al. Long-term cognitive and emotional consequences of mild traumatic brain injury. Psychol Med. (2011) 41:1197–211. doi: 10.1017/S0033291710001728
95. Engberg AW, Teasdale TW. Psychosocial outcome following traumatic brain injury in adults: a long-term population-based follow-up. Brain Inj. (2004) 18:533–45. doi: 10.1080/02699050310001645829
96. Wood RL, Liossi C, Wood L. The impact of head injury neurobehavioural sequelae on personal relationships: preliminary findings. Brain Inj. (2005) 19:845–51. doi: 10.1080/02699050500058778
97. Rath JF, Simon D, Langenbahn DM, Sherr RL, Diller L. Group treatment of problem-solving deficits in outpatients with traumatic brain injury: a randomised outcome study. Neuropsychol Rehabil. (2003) 13:461–88. doi: 10.1080/09602010343000039
98. Miyake A, Friedman NP. The nature and organization of individual differences in executive functions: four general conclusions. Curr Dir Psychol Sci. (2012) 21:8–14. doi: 10.1177/0963721411429458
99. Clark C, Prior M, Kinsella G. The relationship between executive function abilities, adaptive behaviour, and academic achievement in children with externalising behaviour problems. J Child Psychol Psychiatry. (2002) 43:785–96. doi: 10.1111/1469-7610.00084
100. Ellis LK, Rothbart MK, Posner MI. Individual differences in executive attention predict self-regulation and adolescent psychosocial behaviors. Ann N Y Acad Sci. (2004) 1021:337–40. doi: 10.1196/annals.1308.041
101. Toplak ME, West RF, Stanovich KE. Practitioner review: do performance-based measures and ratings of executive function assess the same construct? J Child Psychol Psychiatry. (2013) 54:131–43. doi: 10.1111/jcpp.12001
102. Chan RC, Shum D, Toulopoulou T, Chen EY. Assessment of executive functions: review of instruments and identification of critical issues. Arch Clin Neuropsychol. (2008) 23:201–16. doi: 10.1016/j.acn.2007.08.010
103. Fergusson DM, Horwood LJ. Gender differences in educational achievement in a New Zealand birth cohort. N Z J Educ Stud. (1997) 32:83–96.
104. Deary IJ, Thorpe G, Wilson V, Starr JM, Whalley LJ. Population sex differences in IQ at age 11: the Scottish mental survey 1932. Intelligence. (2003) 31:533–42. doi: 10.1016/S0160-2896(03)00053-9
105. Giza CC, Prins ML. Is being plastic fantastic? mechanisms of altered plasticity after developmental traumatic brain injury. Dev Neurosci. (2006) 28:364–79. doi: 10.1159/000094163
106. Kolb B, Pellis S, Robinson TE. Plasticity and functions of the orbital frontal cortex. Brain Cogn. (2004) 55:104–15. doi: 10.1016/S0278-2626(03)00278-1
107. Anderson V, Brown S, Newitt H, Hoile H. Long-term outcome from childhood traumatic brain injury: intellectual ability, personality, and quality of life. Neuropsychology. (2011) 25:176–84. doi: 10.1037/a0021217
108. Ylvisaker M, Feeney T. Pediatric brain injury: social, behavioral, and communication disability. Phys Med Rehabil Clin N Am. (2007) 18:133–44. doi: 10.1016/j.pmr.2006.11.007
109. Zhang H, Wang J, Geng X, Li C, Wang S. Objective assessments of mental fatigue during a continuous long-term stress condition. Front Hum Neurosci. (2021) 15:733426. doi: 10.3389/fnhum.2021.733426
110. Saunes IS, Karanikolos M, Sagan A. Norway: health system review. Health Syst Transit. (2020) 22:1–163. Retrieved from https://apps.who.int/iris/bitstream/handle/10665/331786/HiT-22-1-2020-eng.pdf
Keywords: fatigue, school, cognition, pediatric acquired brain injury, disability
Citation: Stubberud J, Hypher R, Brandt AE, Finnanger TG, Skovlund E, Andersson S, Risnes K and Rø TB (2022) Predictors of Functional School Outcome in Children With Pediatric Acquired Brain Injury. Front. Neurol. 13:872469. doi: 10.3389/fneur.2022.872469
Received: 09 February 2022; Accepted: 22 March 2022;
Published: 14 April 2022.
Edited by:
Kette D. Valente, Universidade de São Paulo, BrazilReviewed by:
Ellen Marise Lima, University of São Paulo, BrazilCopyright © 2022 Stubberud, Hypher, Brandt, Finnanger, Skovlund, Andersson, Risnes and Rø. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jan Stubberud, amFuLnN0dWJiZXJ1ZEBwc3lrb2xvZ2kudWlvLm5v
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.