
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol., 17 March 2022
Sec. Stroke
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.840892
 E. M. Vos1*
E. M. Vos1* V. J. Geraedts1,2
V. J. Geraedts1,2 A. van der Lugt3
A. van der Lugt3 D. W. J. Dippel4
D. W. J. Dippel4 M. J. H. Wermer2
M. J. H. Wermer2 J. Hofmeijer5,6
J. Hofmeijer5,6 A. C. G. M. van Es7,8Y. B. W. E. M. Roos9
A. C. G. M. van Es7,8Y. B. W. E. M. Roos9 C. M. P. C. D. Peeters-Scholte2I. R. van den Wijngaard1,2
C. M. P. C. D. Peeters-Scholte2I. R. van den Wijngaard1,2Background: Clinical trials of neuroprotection in acute ischemic stroke (AIS) have provided disappointing results. Reperfusion may be a necessary condition for positive effects of neuroprotective treatments. This systematic review provides an overview of efficacy of neuroprotective agents in combination with reperfusion therapy in AIS.
Methods: A literature search was performed on the following databases, namely PubMed, Embase, Web of Science, Cochrane Library, Emcare. All databases were searched up to September 23rd 2021. All randomized controlled trials in which patients were treated with neuroprotective strategies within 12 h of stroke onset in combination with intravenous thrombolysis (IVT), endovascular therapy (EVT), or both were included.
Results: We screened 1,764 titles/abstracts and included 30 full reports of unique studies with a total of 16,160 patients. In 15 studies neuroprotectants were tested for clinical efficacy, where all patients had to receive reperfusion therapies, either IVT and/or EVT. Heterogeneity in reported outcome measures was observed. Treatment was associated with improved clinical outcome for: 1) uric acid in patients treated with EVT and IVT, 2) nerinetide in patients who underwent EVT without IVT, 3) imatinib in stroke patients treated with IVT with or without EVT, 4) remote ischemic perconditioning and IVT, and 5) high-flow normobaric oxygen treatment after EVT, with or without IVT.
Conclusion: Studies specifically testing effects of neuroprotective agents in addition to IVT and/or EVT are scarce. Future neuroprotection studies should report standardized functional outcome measures and combine neuroprotective agents with reperfusion therapies in AIS or aim to include prespecified subgroup analyses for treatment with IVT and/or EVT.
Intravenous thrombolytic therapy (IVT) has become standard care for acute ischemic stroke (AIS), but only a small minority (12%) of patients is eligible for IVT because of the limited time window and contra-indications (1). The absolute benefit of treatment with IVT is limited and is estimated to be 4–10% (2). In the last decade, endovascular therapy (EVT) to mechanically reopen the occluded cerebral artery has led to an improvement of functional outcome in patients with AIS caused by large vessel occlusion (LVO) (3). However, despite high recanalization rates (70–90%) chances of good functional outcome after EVT remain relatively low (30–60%) (3, 4). Currently only 10% of patients after EVT are without stroke symptoms at 3 months follow-up with a modified Rankin Scale (mRS) score of 0 (3, 5). This implies the need for additional treatment and systems-based interventions to further improve recovery of patients with AIS. A wide range of neuroprotective agents has been investigated in the past to reduce brain injury and thereby improve patient recovery. Despite promising results from animal studies, none of the tested neuroprotective strategies appeared effective in clinical trials (6). Earlier trials may have failed due to a lack of recanalization in treating patients with AIS. As ischemic tissue will eventually become infarcted if blood flow is not restored, adequate reperfusion is probably a necessary condition for recovery with or without additional neuroprotective treatments (4, 7–9). The four primary treatment targets are reduction of excitotoxicity, oxidative stress, inflammation, and cellular apoptosis (10). In patients with adequate recanalization, another targeted mechanism is reducing reperfusion injury (7, 11). With the introduction of IVT and EVT, drugs with neuroprotective properties can now be investigated in combination with reperfusion therapy. This systematic review provides an overview of randomized controlled trials (RCTs) of neuroprotective agents in AIS as an adjunct to IVT and/or EVT.
This systematic review adhered to The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 statement and focused on RCTs in patients with AIS undergoing reperfusion therapy and neuroprotective therapy within 12 h of stroke onset. We selected studies by searching electronic databases (PubMed, Embase, Web of Science, Cochrane Library, Emcare) up to and including September 23rd 2021 using the search query specified in Box 1 (Supplementary Material). Two authors (EMV and VJG) independently screened the search results by reading titles and abstracts. All disagreements between raters were included for full text screening. Full text screening was done by two authors authors (EMV and IRW), all disagreements were re-evaluated until consensus was achieved.
RCTs studying neuroprotective agents in patients with AIS in addition to any form of reperfusion therapy within 12 h of stroke onset were selected. Exclusion criteria included non-English articles, an unclear inclusion interval or unclear timing of treatment with the neuroprotective agent, and articles not reporting exact numbers of patients treated with reperfusion treatments (Figure 1). The reference lists of all relevant articles were screened for additional studies.
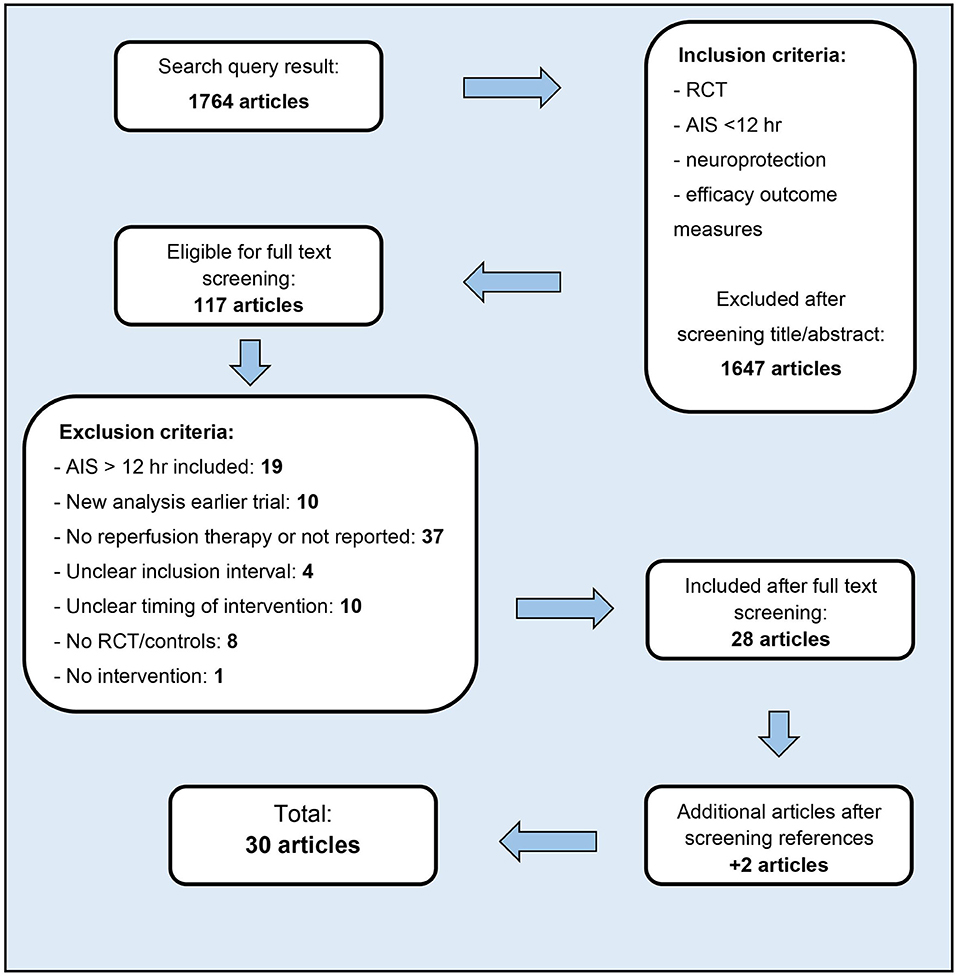
Figure 1. Article selection.
Analyzed primary outcomes were mRS, National Institutes of Health Stroke Scale (NIHSS), Barthel Index (BI), mortality, and risk of hemorrhage. Analyzed secondary outcomes were radiological markers including rate of recanalization measured with the thrombolysis in cerebral infarction (TICI) grading scale, and infarct volume measured by CT or MRI if available. Odds ratios (OR) for good functional outcome (mRS 0–2 vs. 3–6) and mortality (mRS 6) were calculated with reported mRS score distributions if available. All populations were assessed for type of reperfusion therapy (IVT, EVT, or both) and percentage of LVO. When no data were available on percentage of LVO in the cohort, associated radiological information was documented. Time to reperfusion therapy was noted. Neuroprotective treatment regimens were extracted including time between start of reperfusion therapy and neuroprotective treatment. Whether neuroprotective treatment was started before or after reperfusion therapy was noted. Results were grouped according to the main mechanism of action.
The extraction form is available in the Supplementary Material. All data may be shared upon request.
All included articles were evaluated with the modified Cochrane collaboration tool to assess risk of bias for RCTs.
The authors received no funding for this study. Funders of the trials included in this review did not have any influence on the design, interpretation, and reporting of this review.
The search performed on September 23rd 2021 (initial search date: November 13th 2020) yielded 1,764 articles, of which 117 were selected for full text screening. Ultimately, 30 studies were included in this systematic review, encompassing a total of 16160 patients. Results are presented in Tables 1, 2, subdivided into studies combining neuroprotection with either IVT or EVT, and further categorized by presumed mechanism of action: reduction of excitotoxicity, oxidative stress, inflammation, cellular apoptosis, and other/non-pharmacological. Most neuroprotective agents have an effect on multiple mechanisms. Figure 2 shows an overview of neuroprotective agents and their assumed mechanisms of action. In the majority of studies (26/30), patients were treated within minutes to several hours after IVT or before completion of EVT. Three studies reported on pre-hospital administration of neuroprotective treatment; only one specifically administered neuroprotective treatment after recanalization with EVT. Fifteen studies were specifically designed to investigate effects of neuroprotective treatment in addition to reperfusion therapy, i.e., all patients had to receive reperfusion therapy, either IVT and/or EVT. Of these 15 studies with 100% reperfusion therapy, in only 3 studies all patients were treated with EVT. Five of these 15 studies showed a positive result of neuroprotective treatment on functional outcome. In the other 15 studies not all patients were treated with reperfusion therapy. The number of patients treated with IVT or EVT was limited or predefined subgroup analyses on patients receiving IVT or EVT were not reported. Our calculated ORs for good clinical outcome (mRS 0–2) did not reach statistical significance in any of the reported trials. The OR for mortality (mRS 6) was only significantly lower in the study reporting on normobaric oxygen. An overview of unadjusted ORs for good functional outcome and mortality is presented in the Supplementary Material. Risk of bias assessment is presented in Table 3. Studies in which <25% of patients was treated with IVT are summarized in Tables 1, 2, but not separately mentioned in the results below.
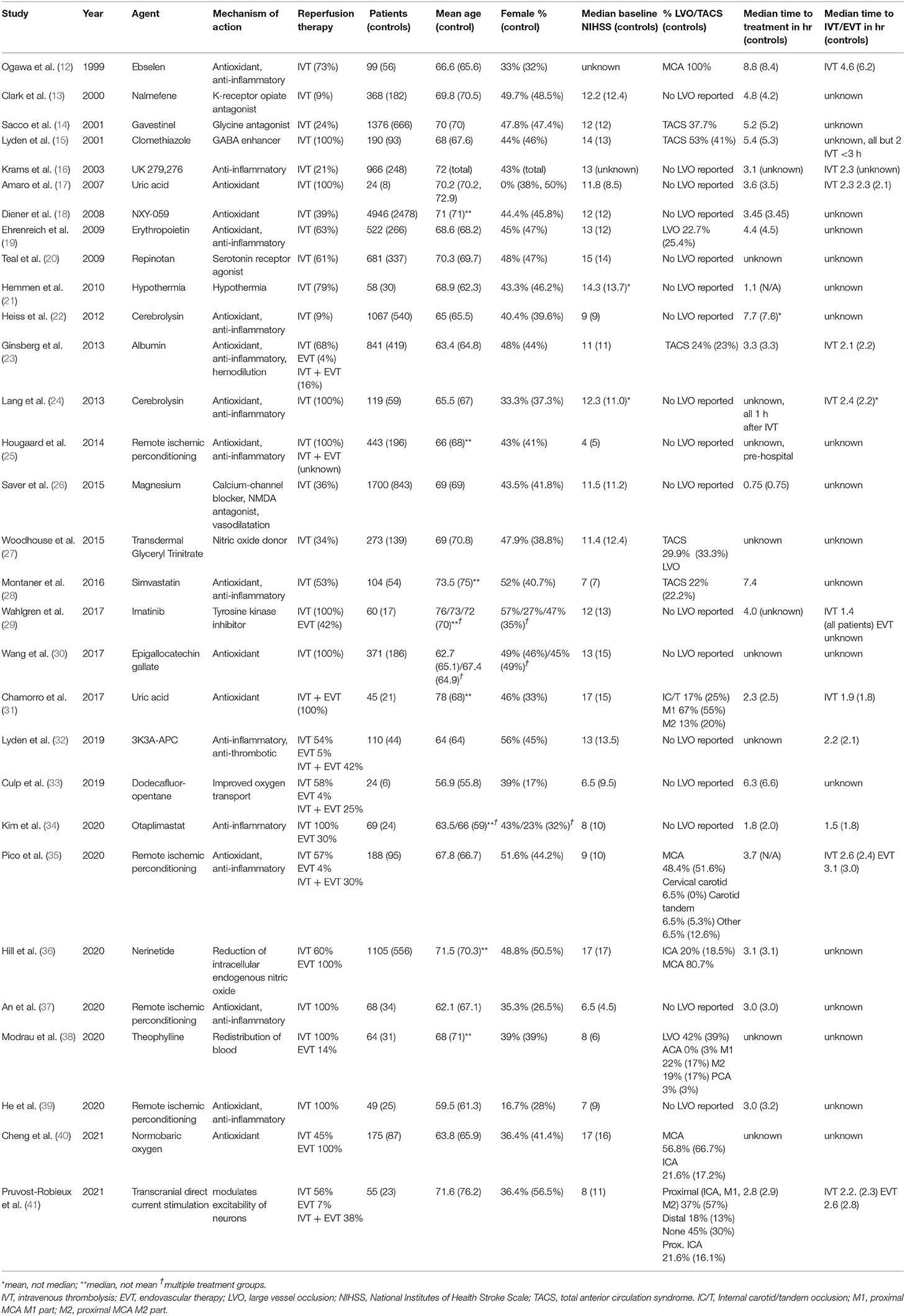
Table 1. Overview of neuroprotective trials using reperfusion therapy.
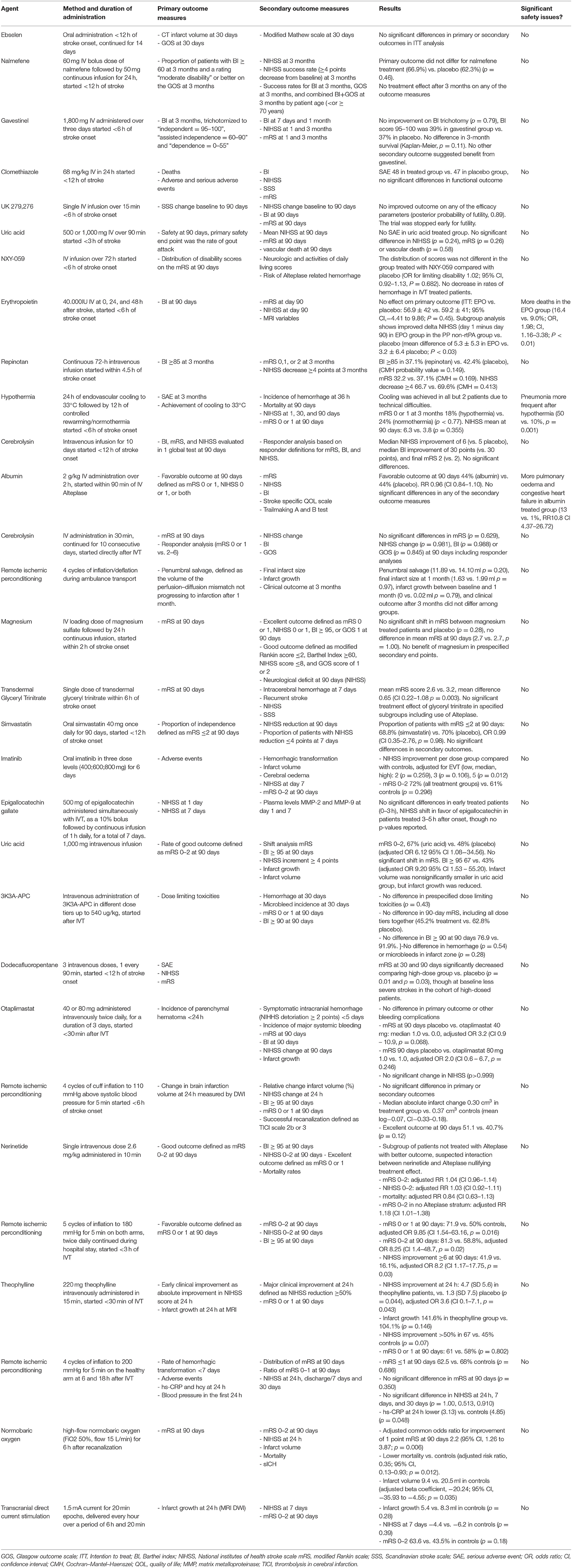
Table 2. Interventions, outcome measures, and results in neuroprotective trials.
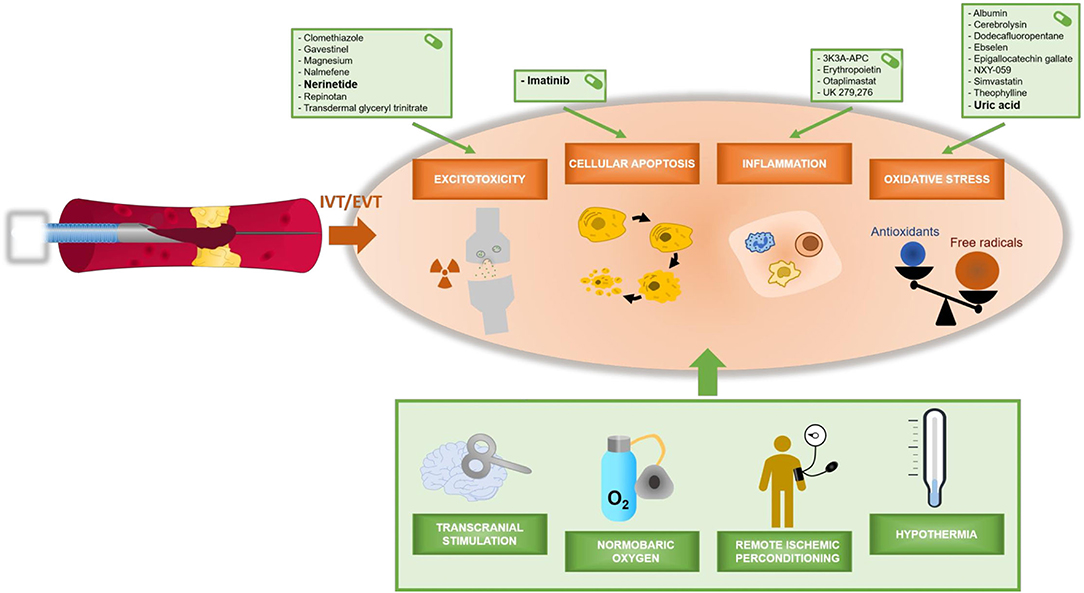
Figure 2. Overview of neuroprotective agents and their assumed mechanisms of action.
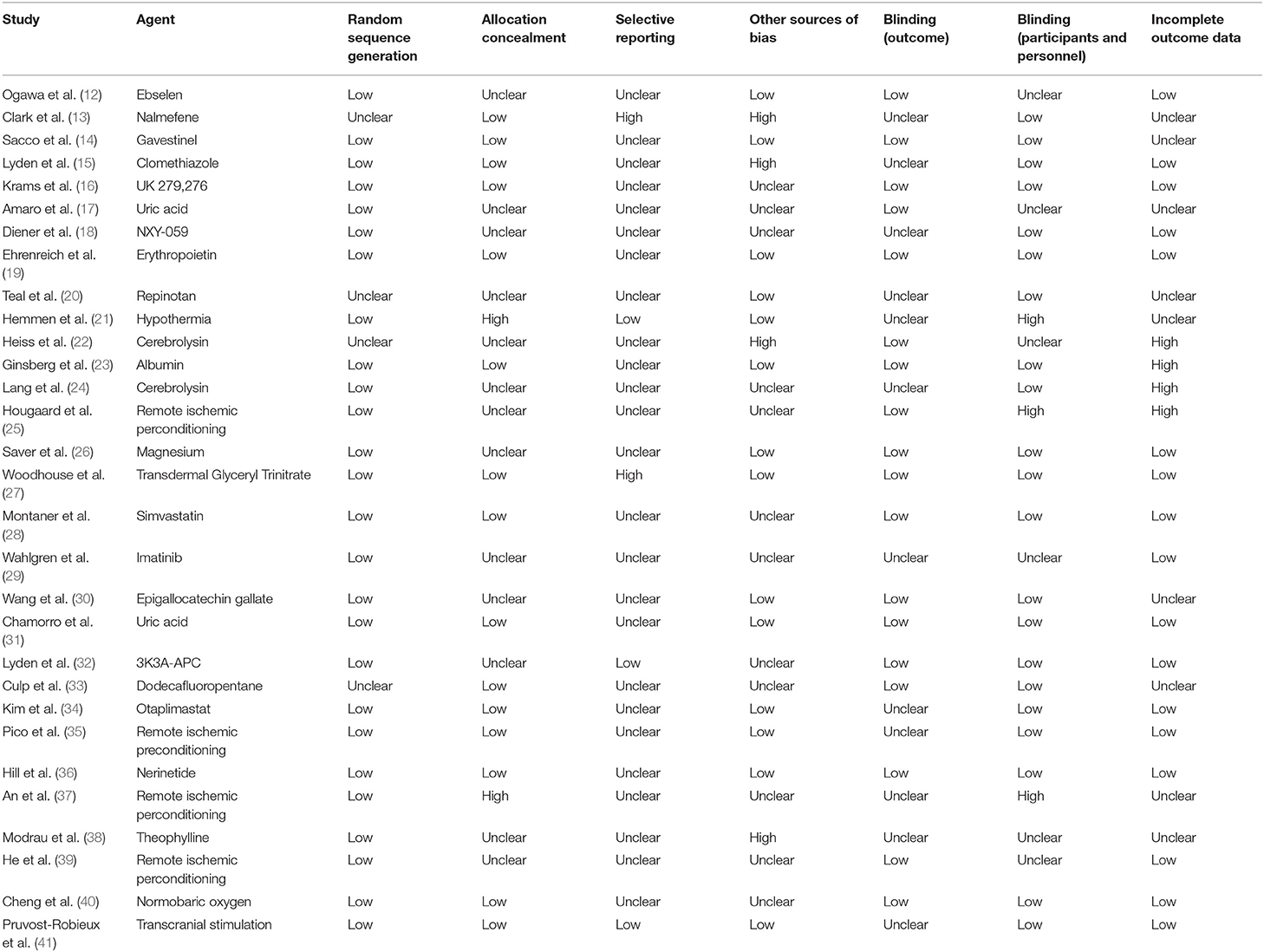
Table 3. Cochrane risk of bias assessment.
Clomethiazole is a positive allosteric modulator of GABA (42). The CLASS-T trial (15) tested the effect of clomethiazole in patients concomitantly treated with IVT. All patients (n = 190) received IVT within 3 h of stroke onset, and 53% of patients had total anterior circulation stroke (TACS). No effect of clomethiazole was found on the main clinical outcome: the Barthel Index score. In the TACS subgroup, 53% of the clomethiazole patients scored a BI >60 vs. 45% of controls (OR 1.4, 95%CI 0.6–3.2). MRS score distributions were not reported.
The use of pre-hospital intravenous magnesium was investigated in 2015 (26). In total 1700 patients were treated, of whom 73% (n = 1,246) had ischemic stroke. Of these patients, 36% received IVT. Main outcome was the mRS at 90 days. Mean mRS scores did not differ between the magnesium group and controls (2.7 in each group). Good functional outcome was observed in 52.4% of the magnesium treated group and 52.8% in controls (OR 1.0; 95%CI 0.8–1.2).
Transdermal glyceryl trinitrate (GTN), a nitric oxide donor, was tested in patients presenting with symptoms of stroke in 2015 (43). Additional analyses were published on a predefined subgroup of early treated patients (<6 h) in this trial (27). All types of stroke were included, of which 76% (n = 208) was ischemic stroke. One third of AIS patients was treated with IVT. Patients that randomized early to GTN had a significant shift toward a lower mRS (adjusted common OR 0.5; 95%CI 0.3–0.8). Good functional outcome was 48,6% in the GTN group and 39,5% in controls (OR 1.4; 95%CI 0.9–2.3). No subgroup analysis for patients treated with IVT was performed.
Repinotan is a serotonin (5-HT)1A receptor agonist. Its intravenous use was investigated in 681 stroke patients (20). In addition, 61% of patients was treated with IVT (stratified during inclusion). Primary outcome was the BI, secondary outcomes included the mRS. The proportion of patients with a BI>85 at 3 months was 37 vs. 42% in controls (OR 0.8, 95%CI 0.6–1.1) and 32.4% of patients had an mRS of 0–2 at 3 months vs. 37.8% in controls (OR 0.8, 95%CI 0.6–1.1).
NXY-059 is a free radical trapping agent. Two large, RCTs (18) included a total of 4946 patients who were treated with intravenous NXY-059 within 6 hof stroke onset; over one third received IVT as well. Primary outcome was the mRS at 3 months. Among patients treated with IVT, there was no association between NXY-059 treatment and mRS score (mRS 0–2 43.0 vs. 42.4%, OR 1.1; 95%CI 0.9–1.1).
Cerebrolysin is a porcine brain-derived preparation of low-molecular-weight neuropeptides with free amino acids that show pharmacodynamic properties similar to those of naturally occurring neurotrophic factors. In 2013, cerebrolysin was studied in 119 patients, all treated with concomitant IVT (24). Primary outcome was the mRS at 90 days. The study was halted prematurely because of futility after the third interim analysis, showing no significant differences between cerebrolysin and placebo (mRS 0–2 67.2 vs. 66.1%, OR 1.1; 95%CI 0.5–2.3).
In 2016 simvastatin was investigated treating 104 patients with AIS, randomized between orally administered simvastatin or placebo for 90 days (28). In total, 53% of patients were treated with IVT. Primary outcome was the mRS. The trial yielded neutral results (mRS 0–2 at 3 months: adjusted OR 1.0, 95%CI 0.4–2.8). A post-hoc analysis showed a possible benefit for patients treated with IVT, with a higher proportion of patients improving >7 points on the NIHSS (adjusted OR 4.1, 95%CI 1.2–14.4).
Epigallocatechin gallate (EGCG) is a naturally occurring polyphenol from green tea extracts. It was tested in 371 AIS patients all treated with IVT (30). The trial reported positive results with lower NIHSS scores in the EGCG treated group in patients treated 3–5 h compared to placebo, though it is unclear whether these differences were significant since no ratios or confidence intervals were reported. MRS scores were not reported.
Ebselen is a lipid-soluble seleno-organic compound that was tested in 99 stroke patients for its possible neuroprotective properties reducing oxidative stress (12). It was administered orally within 12 h of stroke onset. More than two thirds of patients were treated with IVT. Primary outcome was CT infarct volume and the Glasgow Outcome Scale. Mean CT infarct volume was 11.4 ml in Ebselen treated patients vs. 13.4 in controls (p = 0.099). No mRS scores were reported.
The use of recombinant human erythropoietin (EPO) was studied in 2009 (19). Within 6 h of AIS symptom onset, EPO was infused intravenously in 522 patients. Almost two thirds of patients were treated with IVT, which was stratified for in the inclusions. Subgroup analysis revealed that the ΔNIHSS (Day 1 minus Day 90) showed a larger improvement with EPO than with placebo in the non-IVT-subgroup (mean difference of 5.3 ± 5.3 in EPO vs. 3.2 ± 6.4 in placebo; P = 0.03). This difference was not observed in the IVT subgroup. The trial raised safety concerns as there were significantly more deaths in the EPO treated group than in controls (16.4 vs. 9.0%, OR 2.0; 95%CI 1.2–3.4). Overall, the trial did not show a significant effect on any of the efficacy outcomes including mRS (mRS 0–2 39.9 vs. 41.1%, OR 1.1; 95%CI 0.8–1.7).
No studies fulfilled the inclusion criteria.
ICTuS-L tested induced hypothermia at 33°C in AIS patients who also received IVT (21). In total 58 patients were enrolled and 48 (79%) were treated with IVT. Though the primary objective of the study was to investigate safety, assessed efficacy outcomes were NIHSS and mRS. There were no differences in outcome, neither in the overall population, nor in subgroups according to IVT. At 3 months, 18% of patients in the hypothermia group had a mRS score of 0–1 vs. 24% in controls (P < 0.77). No OR for good clinical outcome was calculated as exact data on the distribution of mRS scores was not reported.
Remote ischemic perconditioning (rPerc) is inducing ischemia in one organ to increase tolerability in another. Four trials investigated the use of rPerc in stroke patients receiving reperfusion therapy: two combining rPerc with IVT, and two trials also treating patients with EVT (see paragraph on neuroprotection and EVT). In 2020 a single center trial (n = 68) reported significant results in a trial of rPerc in which patients with AIS were treated with IVT and subsequent ischemic perconditioning (37). Excellent recovery (mRS 0–1) at 3 months was obtained in 72% of patients in the rPerc group vs. 50% in controls (adjusted risk ratio, 9.85; 95%CI, 1.5 to 63.2), though patients with severe stroke (NIHSS >24) were excluded from this trial. A second trial investigated rPerc in 49 patients all treated with IVT (39). Primary outcome was the occurrence of hemorrhagic transformation or other adverse events. Secondary outcome measures included the ratio of mRS 0–1 at 90 days, distribution of mRS, and NIHSS scores. There were no differences in recovery between groups treated with and without rPerc (mRS 0–1 62.5 vs. 68.0% in controls, p = 0.69).
The eicosapeptide nerinetide was investigated in the NA-1 trial, comparing nerinetide treatment with placebo in 1105 patients with LVO eligible for EVT (36). The primary outcome was favorable outcome defined as an mRS 0–2 at 90 days. Concomitant alteplase was administered in 60% of patients. The primary outcome was achieved by 337 (61%) of 549 patients in the nerinetide group and 329 (59%) of 556 in controls (adjusted RR 1.0, 95%CI 1.0–1.1). Successful recanalization (eTICI ≥2b) was achieved in 86% of the placebo group and 87% of the nerinetide group. The average time between administration of nerinetide and reperfusion was 22 min. In a predefined post-hoc subgroup analysis, nerinetide was significantly associated with favorable outcome (risk ratio 1.2 (1.0–1.4) in the non-IVT subgroup (n = 446) and not in the IVT subgroup (n = 659). The authors hypothesize that an interaction between nerinetide and the use of IVT might have nullified treatment effect with nerinetide in the IVT subgroup.
Intravenous administration of albumin in 422 AIS patients was reported in 2013 (23). The majority of patients received IVT (68%), with a small subgroup receiving additional EVT (16%) or EVT alone (4%). Primary endpoint was favorable outcome (mRS 0–1, NIHSS 0–1, or both). The trial was halted prematurely because of futility after an unscheduled third interim analysis. The primary outcome was adjusted for the use of IVT and baseline NIHSS and did not differ between patients in the albumin group and controls (44.0 vs. 44.0%; risk ratio 1.0; 95%CI 0.8–1.1). The proportion of patients with good functional outcome did not differ between treatment groups (56.7 vs. 57.0%, OR 1.0; 95%CI 0.7–1.3). No subgroup analysis was done for the group of patients treated with EVT, and rates of successful recanalization were not reported.
Uric acid is a naturally occurring antioxidant. A pilot study was conducted in 2007 treating 16 patients with uric acid after IVT proving its safety (17). The URICO-ICTUS trial consequently studied a population of 411 stroke patients (44). In 2017 results from a prespecified subgroup analysis were reported with 45 patients who received IVT and EVT and were all treated with intravenous uric acid or placebo within 4.5 h of stroke onset (31). Recanalization was achieved in >80% of patients. Primary outcome was good functional outcome (mRS 0–2) and was observed in 16/24 (67%) patients treated with uric acid and 10/21 (48%) in controls (adjusted OR, 6.1, 95%CI 1.1–34.6). The unadjusted OR analysis did not show a significant effect (OR 2.0 95%CI 0.7–7.3) of uric acid on good functional outcome.
Dodecafluoropentane (DDFPe) is an oxygen transporting nanodroplet with neuroprotective properties (33). In 2019 administration in 24 patients with AIS was investigated, starting infusion within 12 h of stroke onset (44). Three different dose tiers were used. In total of 16/18 DDFPe treated patients received reperfusion therapy (IVT = 61%, EVT 6%, IVT + EVT 22%). Outcomes were (serious) adverse events, NIHSS and mRS scores. When only the high-dose group of DDFPe was compared to placebo, there was an improvement in both 30- and 90-day mRS (P = 0.01 and P = 0.03, respectively). No OR for good clinical outcome was calculated as exact data on the distribution of mRS scores were not reported. Sample sizes were too small for subgroup analyses in patients with LVO.
Theophylline is speculated to be neuroprotective due to its cerebral vasoactive properties (31). It was investigated as add-on to IVT in 64 patients with AIS (38). All patients received theophylline intravenously within 30 min of IVT and 14% of patients (n = 9) was also treated with EVT. A limited number of patients with LVO was included as the majority of patients with severe stroke was unable to provide informed consent. Outcomes were NIHSS improvement and infarct volume growth at 24 h. After 3.5 years the steering committee decided to stop the trial due to slow recruitment. Patients treated with theophylline improved on the NIHSS by 4.7 points (SD, 5.6) compared with an improvement of 1.3 points (SD, 7.5) after IVT alone (P = 0.044), though results did not reach significance after correction for multiplicity [adjusted estimated improvement 3.6 (95%CI, 0.1–7.1)]. The corresponding adjusted treatment effect on infarct growth was 35.2% (95%CI, −17.4–87.7). Good functional outcome did not differ between treatment groups (81% in both groups, OR 1.1; 95%CI 0.3–3.8). No treatment effect was found in the subgroup treated with EVT.
Otaplimastat is a cerebroprotectant that inhibits the matrix metalloprotease pathway (34). It was tested in AIS patients receiving IVT in 2019 (34). The trial was divided in a safety trial (n = 11) and randomized controlled efficacy trial (n = 69). The latter part compared two dose tiers (40/80 mg) vs. placebo. In total 29% of patients underwent EVT in addition to IVT. Primary endpoints were intracranial hemorrhage, systemic bleeding and the mRS. No significant differences in the occurrence of hemorrhagic transformation were found between groups. A non-significant shift in distribution of mRS was reported in the otaplimastat 40 mg group vs. placebo with an adjusted OR of 3.2 (95%CI 0.9–10.9). Good functional outcome did not differ between groups (75.0 vs. 76.2%, OR 0.9; 95%CI 0.3–3.2). Of patients treated with EVT, 77% achieved good recanalization (mTICI score ≥2b).
3K3A-APC is a modified version of Activated Protein C. The RHAPSODY trial investigated its intravenous use in treating AIS in combination with IVT (54%), EVT (5%) or both (42%) in 110 patients (32). Primary outcome was safety (maximum tolerated dose), secondary outcomes included mRS and NIHSS. There were no patients with an mRS ≥2 in both the 3K3A-APC group and control group (mRS 0: 88 vs. 93%, mRS 1: 12 vs. 7%).
Imatinib is a tyrosine kinase inhibitor which reduces cellular apoptosis by blocking the signaling of platelet-derived growth factor alpha. It was investigated in 60 stroke patients in three different dose levels (400, 600, and 800 mg, orally) (29). All patients received IVT and 42% of patients underwent EVT. Primary outcome measure was the occurrence of adverse events. Secondary outcomes included infarct volume, NIHSS improvement and good functional outcome (mRS 0–2). Treating AIS patients with imatinib was safe. Patients treated with imatinib had more NIHSS improvement than controls with a significant difference measured in the high dose group, adjusted for treatment with EVT [low, medium, and high dose: 2 points (p = 0.259), 3 points (p = 0.106), and 5 points (p = 0.012) respectively]. The mean NIHSS improvement adjusted for treatment with EVT was 0.6 per 100 mg imatinib (−0.6; 95%CI −1.1 to −0.1). Good functional outcome did not differ between groups (69.2% in all treatment groups vs. 61.0% controls, OR 1.2; 95%CI 0.4–4.1).
Two trials investigated the use of rPerc in stroke patients treated with EVT. The first trial investigated the pre-hospital use of rPerc in 443 stroke patients (25). All MRI proven stroke patients who underwent IVT were analyzed. Primary end point was penumbral salvage (volume of perfusion–diffusion mismatch not progressing to infarction after 1 month). No treatment effect of rPerc was found in median penumbral salvage (IQR): 11.9 mL (0.5–63.4) vs. 14.1 mL (1.6–79.8) nor good functional outcome (80 vs. 88%, OR 0.5; 95%CI 0.3–1.2). Though the authors report some patients being treated by EVT, no exact data about this is presented and no subgroup analyses were done. The second trial investigated in-hospital rPerc in 188 patients of who 87% received IVT and 34% received EVT (35). No differences were reported in terms of infarct growth (MRI) or functional outcome (NIHSS 24 h, BI 90 days). An excellent outcome (mRS 0–1) was observed in 46 patients (51%) in the intervention group vs. 37 (41%) in controls (OR 1.6; 95%CI 0.9–2.9).
Normobaric oxygen (NBO) potentially reduces secondary injury to penumbral tissue by reducing oxidative stress. The use of high-flow NBO (FiO2 50%, 15 L/min) was investigated in 175 stroke patients all treated with EVT (40). NBO was administered for 6 h following the EVT procedure. In addition, 45% of patients were treated with IVT. Stroke patients without recanalization (TICI score 0) after EVT were excluded. Primary outcome was the mRS, secondary outcomes included NIHSS at 24 h, infarct volume, and mortality. The common OR of NBO treatment indicating the improvement of 1 point on the mRS was 2.2 (95%CI, 1.3–3.9). In NBO treated patients, mortality was lower (adjusted risk ratio, 0.4; 95%CI 0.1–0.9) and NBO treated patients had smaller final infarct volumes (9.4 vs. 20.5 ml in controls (adjusted beta coefficient, −20.2; 95%CI −35.9 to −4.6). The proportion of patients with good functional outcome was 64.8% in the NBO treated group and 50.6% in controls (OR 1.4; 95%CI 0.7–1.6).
Cathodal transcranial direct current stimulation (C-tDCS) is a non-invasive neurostimulation method modulating the excitability of cortical neurons (41). It was investigated in acute stroke patients in 2021 (41). In total 45 patients were treated with C-tDCS or sham procedure, in 6 sessions of 20 min. Most patients (42/45) were treated with IVT, and over one third (20/45) (also) with EVT. The primary outcome was growth of infarct volume at 24 h. Secondary outcomes were NIHSS score at 7 days and mRS 0–2 at 90 days. No benefit of C-tDCS was found on any of the primary or secondary outcomes (mRS 0–2 63.6 vs. 43.5% in controls, OR 2.3; 95%CI 0.7–2.5).
This systematic review investigates effects of neuroprotective agents in combination with reperfusion therapy in AIS. Our search yielded 30 studies in which neuroprotective agents were tested. Only 15 studies specifically included patients treated with IVT and/or EVT and were designed to investigate effects of neuroprotective treatment in addition to reperfusion therapy. Of these 15 studies, five reported positive results of treatment on various clinical outcome measures as chosen by the investigators. These results indicate a high potential for some neuroprotective treatments in addition to reperfusion. Studies investigating neuroprotective treatment in addition to IVT that report a positive effect of neuroprotection on clinical outcome are the trials investigating GTN, imatinib and remote ischemic perconditioning (rPerc). Unfortunately, two thirds of patients did not receive reperfusion therapy in the GTN trial. Early treatment of stroke patients with GTN was recently investigated in the prehospital transdermal glyceryl trinitrate in patients with ultra-acute presumed stroke (RIGHT-2) trial (45). The trial did not show a beneficial effect of GTN in pre-hospital treatment of stroke. Since no subgroup analyses on patients treated with IVT were reported this study fell outside the scope of our current search. The trial investigating imatinib was primarily a safety trial with a limited number of patients. A follow up trial is currently ongoing and estimated to be completed in 2023. One of the four trials on rPerc found a larger probability of excellent outcome (mRS 0–1) with rPerc than without rPerc. These results should be interpreted with caution since outcome assessment in this trial was not blinded and the study was susceptible to allocation concealment bias.
Studies investigating neuroprotective treatment in addition to EVT that report a significant effect of neuroprotection on clinical outcome are the trials in which patients were treated with 1) the combined treatment of IVT and EVT with uric acid, 2) the use of nerinetide in stroke patients treated with EVT, and 3) the use of high-flow NBO in stroke patients successfully treated with EVT. The article on uric acid reported results from a predefined subgroup analysis with patients treated with IVT and EVT. All three studies were methodologically sound with a low risk of bias. A new trial investigating nerinetide (ESCPAPE-NEXT) is already recruiting patients to confirm these results (NCT04462536). A follow-up trial for uric acid has been planned as well (11).
By limiting our search to RCTs with the terms neuroprotection (and variants) and stroke, it is possible that some trials on neuroprotective agents and reperfusion therapy in AIS were not found. Indeed, by cross-checking references, two more articles were added to our results. A large number of neuroprotective agents has been investigated in AIS in the past. It is possible that a number of articles fell outside our search, despite the use of reperfusion therapy, simply because no data on the use of reperfusion therapy were reported. As we limited our search strategy to neuroprotection trials using efficacy as outcome, safety trials may have fallen outside the scope of our search. Different studies reported various outcome measures. Our calculated ORs for good clinical outcome (mRS 0–2) did not reach statistical significance in any of the reported trials. The heterogeneity in outcome, as well as variations in treatment administration (e.g. timing, dosage), and the lack of replication-studies impaired the development of a quantitative synthesis. Future studies should aim to report standardized functional outcome measures, most notably the mRS, as was proposed by the Stroke Therapy Academic Industry Roundtable (STAIR) (46), as well as strive to replicate and validate promising findings.
Recanalization rates in stroke patients treated with EVT are higher (60–90%) (4) than in patients treated with IVT (10–30%) (47, 48). Neuroprotective treatment may be more effective in these patients. As EVT is a relatively new treatment, a very limited number of neuroprotective agents has been tested in this setting. Future research should seek to combine EVT with neuroprotective strategies to test the hypothesis that neuroprotective treatment in combination with successful reperfusion leads to better outcomes in patients with AIS. Rapid reperfusion can, however, also lead to reperfusion injury, induced by high levels of free oxygen radicals, when oxygen becomes again available in previous hypoxic-ischemic tissue. For that reason treatments, which target reduction in oxidative stress might be beneficial in the prevention of this reperfusion injury.
An overview of ongoing studies investigating neuroprotective agents in addition to EVT using efficacy outcome measures is shown in Table 4. Future pre-clinical research is needed to improve the targeting of neuroprotective agents as well as their action mechanism. STAIR X proposed the term neurovascular unit (NVU) to better recognize different parts of the brain susceptible to ischemia. The NVU consists of various cell types including astrocytes, neurons and endothelial cells with a differential vulnerability to ischemic injury. New research strategies may focus on neuroprotective strategies targeting one or multiple parts of the NVU (13). Indeed, the importance of solid pre-clinical research in neuroprotective strategies has already been recognized by the initiation of the Stroke Preclinical Assessment Network (SPAN), a project started by the National Institutes of Health (NIH) in 2018 in which 7 different laboratories seek to employ rigorous, clinical research practices while assessing the effectiveness of potential neuroprotective therapies in reducing ischemic brain injury. New pre-clinical research strategies may focus on neuroprotective strategies targeting one or multiple parts of the NVU.
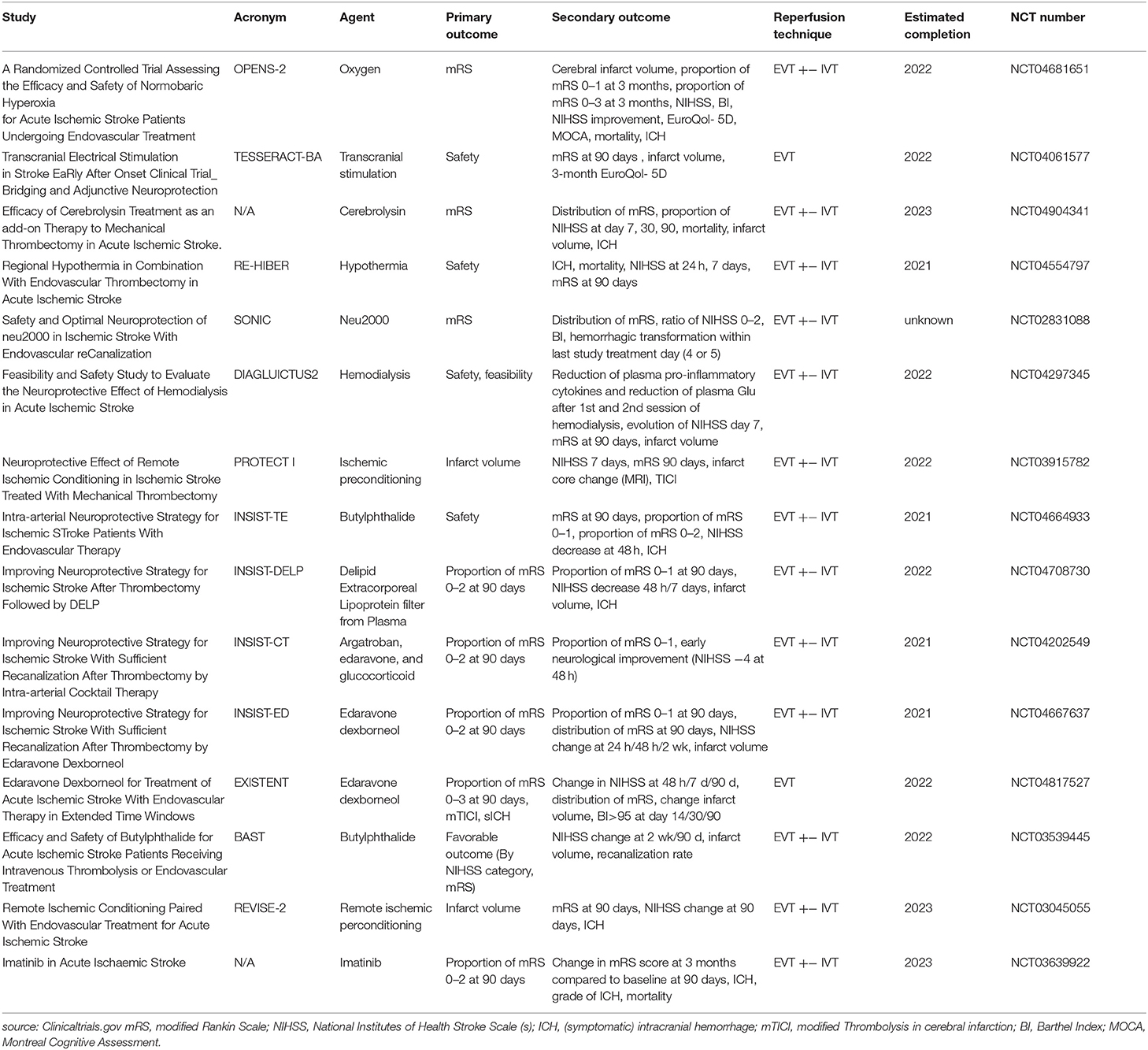
Table 4. Current trials combining neuroprotection and reperfusion.
Studies specifically investigating neuroprotection in addition to reperfusion treatment are scarce. Five of 15 studies report a positive treatment effect of neuroprotection in addition to reperfusion therapy. Positive results are reported for combining EVT and IVT with uric acid, nerinetide in addition to EVT without IVT, rPerc with IVT, and the use of imatinib and normobaric oxygen in patients treated with EVT and/or IVT, although various clinical outcome measures were reported and validation of these results needs to be established. Future neuroprotection studies should combine neuroprotective agents with reperfusion therapies in AIS or include prespecified subgroup analyses for treatment with IVT and/or EVT.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
EV, VG, and IW contributed to conception and design of the review. EV wrote the first draft of the manuscript. EV and VG performed the statistical analyses. VG, AL, DD, MW, JH, AE, YR, CP-S, and IW wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
This open access publication fee was funded by a grant from the Research Fund of Haaglanden Medisch Centrum.
CP-S is founder and consultant at Neurophyxia BV. She holds several patents and stocks of Neurophyxia BV. DD received grants from Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organisation for Health Research and Development, Health Holland Top Sector Life Sciences & Health, Stryker, Penumbra, Inc, Medtronic, Thrombolytic Science LLC, and Ceronovus. YR is a shareholder at Nicolab B.V. AL received grants from Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organisation for Health Research and Development, Health Holland Top Sector Life Sciences & Health, Stryker, Penumbra, Inc, Medtronic, Thrombolytic Science LLC, and Ceronovus. MJHW received grants from Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organisation for Health Research and Development and an unrestricted research grant from Electrocore.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank I. de Boer, MD, MSc, Department of Neurology, Leiden University Medical Center, for assistance in graphical abstract design.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.840892/full#supplementary-material
1. Vanacker P, Lambrou D, Eskandari A, Mosimann PJ, Maghraoui A, Michel P. Eligibility and predictors for acute revascularization procedures in a stroke center. Stroke. (2016) 47:1844–9. doi: 10.1161/STROKEAHA.115.012577
2. Wardlaw JM, Murray V, Berge E, del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev. (2014) 2014:CD000213. doi: 10.1002/14651858.CD000213.pub3
3. Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM et al. Endovascular thrombectomy after large-vessel ischemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. (2016) 387:1723–31. doi: 10.1016/S0140-6736(16)00163-X
4. Link TW, Santillan A, Patsalides A. Intra-arterial neuroprotective therapy as an adjunct to endovascular intervention in acute ischemic stroke: a review of the literature and future directions. Interv Neuroradiol. (2020) 26:405–15. doi: 10.1177/1591019920925677
5. Jansen IGH, Mulder MJHL, Goldhoorn RB. MR CLEAN Registry investigators. Endovascular treatment for acute ischemic stroke in routine clinical practice: prospective, observational cohort study (MR CLEAN Registry). BMJ. (2018) 360:k949. doi: 10.1136/bmj.k949
6. O'Collins VE, Macleod MR, Donnan GA, Horky LL, van der Worp BH, Howells DW. 1,026 experimental treatments in acute stroke. Ann Neurol. (2006). 59:467–77. doi: 10.1002/ana.20741
7. Savitz SI, Baron JC, Yenari MA, Sanossian N, Fisher M. Reconsidering neuroprotection in the reperfusion era. Stroke. (2017) 48:3413–9. doi: 10.1161/STROKEAHA.117.017283
8. Savitz SI, Baron JC, Fisher M. STAIR X consortium. stroke treatment academic industry roundtable x: brain cytoprotection therapies in the reperfusion era. Stroke. (2019) 50:1026–31. doi: 10.1161/STROKEAHA.118.023927
9. Xiong XY, Liu L, Yang QW. Refocusing neuroprotection in cerebral reperfusion era: new challenges and strategies. Front Neurol. (2018) 9:249. doi: 10.3389/fneur.2018.00249
10. Lakhan SE, Kirchgessner A, Hofer M. Inflammatory mechanisms in ischemic stroke: therapeutic approaches. J Transl Med. (2009) 7:97. doi: 10.1186/1479-5876-7-97
11. Chamorro Á, Lo EH, Renú A, van Leyen K, Lyden PD. The future of neuroprotection in stroke. J Neurol Neurosurg Psychiatry. (2021) 92:129–35. doi: 10.1136/jnnp-2020-324283
12. Ogawa A, Yoshimoto T, Kikuchi H, Sano K, Saito I, Yamaguchi T et al. Ebselen in acute middle cerebral artery occlusion: a placebo-controlled, double-blind clinical trial. Cerebrovasc Dis. (1999) 9:112–8. doi: 10.1159/000015908
13. Clark WM, Raps EC, Tong DC, Kelly RE. Cervene (Nalmefene) in acute ischemic stroke: final results of a phase III efficacy study. The Cervene Stroke Study Investigators. Stroke. (2000) 31:1234–9. doi: 10.1161/01.STR.31.6.1234
14. Sacco RL, DeRosa JT, Haley EC Jr, Levin B, Ordronneau P, Phillips SJ et al. Glycine antagonist in neuroprotection for patients with acute stroke: gain americas: a randomized controlled trial. JAMA. (2001) 285:1719–28. doi: 10.1001/jama.285.13.1719
15. Lyden P, Jacoby M, Schim J, Albers G, Mazzeo P, Ashwood T et al. The clomethiazole acute stroke study in tissue-type plasminogen activator-treated stroke (CLASS-T): final results. Neurology. (2001) 57:1199–205. doi: 10.1212/WNL.57.7.1199
16. Krams M, Lees KR, Hacke W, Grieve AP, Orgogozo JM, Ford GA. ASTIN Study Investigators. Acute Stroke Therapy by Inhibition of Neutrophils (ASTIN): an adaptive dose-response study of UK-279,276 in acute ischemic stroke. Stroke. (2003) 34:2543–8. doi: 10.1161/01.STR.0000092527.33910.89
17. Amaro S, Soy D, Obach V, Cervera A, Planas AM, Chamorro A. A pilot study of dual treatment with recombinant tissue plasminogen activator and uric acid in acute ischemic stroke. Stroke. (2007) 38:2173–5. doi: 10.1161/STROKEAHA.106.480699
18. Diener HC, Lees KR, Lyden P, Grotta J, Davalos A, Davis SM et al. NXY-059 for the treatment of acute stroke: pooled analysis of the SAINT I and II Trials. Stroke. (2008) 39:1751–8. doi: 10.1161/STROKEAHA.107.503334
19. Ehrenreich H, Weissenborn K, Prange H, Schneider D, Weimar C, Wartenberg K et al. Recombinant human erythropoietin in the treatment of acute ischemic stroke. Stroke. (2009) 40:e647–56. doi: 10.1161/STROKEAHA.109.564872
20. Teal P, Davis S, Hacke W, Kaste M, Lyden PD. Modified Randomized Exposure Controlled Trial Study Investigators. A randomized, double-blind, placebo-controlled trial to evaluate the efficacy, safety, tolerability, and pharmacokinetic/pharmacodynamic effects of a targeted exposure of intravenous repinotan in patients with acute ischemic stroke: modified Randomized Exposure Controlled Trial (mRECT). Stroke. (2009) 40:3518–25. doi: 10.1161/STROKEAHA.109.551382
21. Hemmen TM, Raman R, Guluma KZ, Meyer BC, Gomes JA, Cruz-Flores S et al. Intravenous thrombolysis plus hypothermia for acute treatment of ischemic stroke (ICTuS-L): final results. Stroke. (2010) 41:2265–70. doi: 10.1161/STROKEAHA.110.592295
22. Heiss WD, Brainin M, Bornstein NM, Tuomilehto J, Hong Z. Cerebrolysin Acute Stroke Treatment in Asia (CASTA) Investigators. Cerebrolysin in patients with acute ischemic stroke in Asia: results of a double-blind, placebo-controlled randomized trial. Stroke. (2012) 43:630–6. doi: 10.1161/STROKEAHA.111.628537
23. Ginsberg MD, Palesch YY, Hill MD, Martin RH, Moy CS, Barsan WG et al. High-dose albumin treatment for acute ischemic stroke (ALIAS) Part 2: a randomised, double-blind, phase 3, placebo-controlled trial. Lancet Neurol. (2013) 12:1049–58. doi: 10.1016/S1474-4422(13)70223-0
24. Lang W, Stadler CH, Poljakovic Z, Fleet D. Lyse Study Group. A prospective, randomized, placebo-controlled, double-blind trial about safety and efficacy of combined treatment with alteplase (rt-PA) and Cerebrolysin in acute ischemic hemispheric stroke. Int J Stroke. (2013) 8:95–104. doi: 10.1111/j.1747-4949.2012.00901.x
25. Hougaard KD, Hjort N, Zeidler D, Sørensen L, Nørgaard A, Hansen TM et al. Remote ischemic perconditioning as an adjunct therapy to thrombolysis in patients with acute ischemic stroke: a randomized trial. Stroke. (2014) 45:159–67. doi: 10.1161/STROKEAHA.113.001346
26. Saver JL, Starkman S, Eckstein M, Stratton SJ, Pratt FD, Hamilton S et al. Prehospital use of magnesium sulfate as neuroprotection in acute stroke. N Engl J Med. (2015) 372:528–36. doi: 10.1056/NEJMoa1408827
27. Woodhouse L, Scutt P, Krishnan K, Berge E, Gommans J, Ntaios G et al. Effect of hyperacute administration (within 6 hours) of transdermal glyceryl trinitrate, a nitric oxide donor, on outcome after stroke: subgroup analysis of the efficacy of nitric oxide in stroke (ENOS) trial. Stroke. (2015) 46:3194–201. doi: 10.1161/STROKEAHA.115.009647
28. Montaner J, Bustamante A, García-Matas S, Martínez-Zabaleta M, Jiménez C, de la Torre J et al. Combination of thrombolysis and statins in acute stroke is safe: results of the STARS randomized trial (stroke treatment with acute reperfusion and simvastatin). Stroke. (2016) 47:2870–3. doi: 10.1161/STROKEAHA.116.014600
29. Wahlgren N, Thorén M, Höjeberg B, Käll TB, Laska AC, Sjöstrand C et al. Randomized assessment of imatinib in patients with acute ischemic stroke treated with intravenous thrombolysis. J Intern Med. (2017) 281:273–83. doi: 10.1111/joim.12576
30. Wang XH, You YP. Epigallocatechin gallate extends therapeutic window of recombinant tissue plasminogen activator treatment for brain ischemic stroke: a randomized double-blind and placebo-controlled trial. Clin Neuropharmacol. (2017) 40:24–8. doi: 10.1097/WNF.0000000000000197
31. Chamorro Á, Amaro S, Castellanos M, Gomis M, Urra X, Blasco J et al. Uric acid therapy improves the outcomes of stroke patients treated with intravenous tissue plasminogen activator and mechanical thrombectomy. Int J Stroke. (2017) 12:377–82. doi: 10.1177/1747493016684354
32. Lyden P, Pryor KE, Coffey CS, Cudkowicz M, Conwit R, Jadhav A et al. Final results of the RHAPSODY trial: a multi-center, phase 2 trial using a continual reassessment method to determine the safety and tolerability of 3K3A-APC, a recombinant variant of human activated protein c, in combination with tissue plasminogen activator, mechanical thrombectomy or both in moderate to severe acute ischemic stroke. Ann Neurol. (2019) 85:125–36. doi: 10.1002/ana.25383
33. Culp WC, Onteddu SS, Brown A, Nalleballe K, Sharma R, Skinner RD et al. Dodecafluoropentane emulsion in acute ischemic stroke: a phase ib/ii randomized and controlled dose-escalation trial. J Vasc Interv Radiol. (2019) 30:1244–1250.e1. doi: 10.1016/j.jvir.2019.04.020
34. Kim JS, Lee KB, Park JH, Sung SM, Oh K, Kim EG et al. Safety and efficacy of otaplimastat in patients with acute ischemic stroke requiring tPA (SAFE-TPA): a multicenter, randomized, double-blind, placebo-controlled phase 2 study. Ann Neurol. (2020) 87:233–45. doi: 10.1002/ana.25644
35. Pico F, Lapergue B, Ferrigno M, Rosso C, Meseguer E, Chadenat ML et al. Effect of in-hospital remote ischemic perconditioning on brain infarction growth and clinical outcomes in patients with acute ischemic stroke: the RESCUE BRAIN randomized clinical trial. JAMA Neurol. (2020) 77:725–34. doi: 10.1001/jamaneurol.2020.0326
36. Hill MD, Goyal M, Menon BK, Nogueira RG, McTaggart RA, Demchuk AM et al. Efficacy and safety of nerinetide for the treatment of acute ischemic stroke (ESCAPE-NA1): a multicentre, double-blind, randomised controlled trial. Lancet. (2020) 395:878–87. doi: 10.1016/S0140-6736(20)30258-0
37. An JQ, Cheng YW, Guo YC, Wei M, Gong MJ, Tang YL et al. Safety and efficacy of remote ischemic postconditioning after thrombolysis in patients with stroke. Neurology. (2020) 95:e3355–63. doi: 10.1212/WNL.0000000000010884
38. Modrau B, Andersen G, Mikkelsen IK, Nielsen A, Hansen MB, Johansen MB et al. Theophylline as an add-on to thrombolytic therapy in acute ischemic stroke: a randomized placebo-controlled trial. Stroke. (2020) 51:1983–90. doi: 10.1161/STROKEAHA.119.027446
39. He YD, Guo ZN, Qin C, Jin H, Zhang P, Abuduxukuer R, et al. Remote ischemic conditioning combined with intravenous thrombolysis for acute ischemic stroke. Ann Clin Transl Neurol. (2020) 7:972–9. doi: 10.1002/acn3.51063
40. Cheng Z, Geng X, Tong Y, Dornbos D 3rd, Hussain M, Rajah GB, et al. Adjuvant high-flow normobaric oxygen after mechanical thrombectomy for anterior circulation stroke: a randomized clinical trial. Neurotherapeutics. (2021) 18:1188–97. doi: 10.1007/s13311-020-00979-3
41. Pruvost-Robieux E, Benzakoun J, Turc G, Marchi A, Mancusi RL, Lamy C, et al. Cathodal transcranial direct current stimulation in acute ischemic stroke: pilot randomized controlled trial. Stroke. (2021) 52:1951–1960. doi: 10.1161/STROKEAHA.120.032056
42. Wahlgren NG, Ranasinha KW, Rosolacci T, Franke CL, van Erven PM, Ashwood T, et al. Clomethiazole acute stroke study (CLASS): results of a randomized, controlled trial of clomethiazole versus placebo in 1360 acute stroke patients. Stroke. (1999) 30:21–8. doi: 10.1161/01.STR.30.1.21
43. ENOS Trial Investigators. Efficacy of nitric oxide, with or without continuing antihypertensive treatment, for management of high blood pressure in acute stroke (ENOS): a partial-factorial randomised controlled trial. Lancet. (2015). 385:617–28. doi: 10.1016/S0140-6736(14)61121-1
44. Chamorro A, Amaro S, Castellanos M, Segura T, Arenillas J, Martí-Fábregas J et al. Safety and efficacy of uric acid in patients with acute stroke (URICO-ICTUS): a randomised, double-blind phase 2b/3 trial. Lancet Neurol. (2014) 13:453–60. doi: 10.1016/S1474-4422(14)70054-7
45. RIGHT-2 Investigators. Prehospital transdermal glyceryl trinitrate in patients with ultra-acute presumed stroke (RIGHT-2): an ambulance-based, randomised, sham-controlled, blinded, phase 3 trial. Lancet. (2019). 393:1009–20. doi: 10.1016/S0140-6736(19)30194-1
46. Saver JL, Chaisinanunkul N, Campbell BCV, Grotta JC, Hill MD, Khatri P et al. Standardized nomenclature for modified rankin scale global disability outcomes: consensus recommendations from stroke therapy academic industry roundtable XI. Stroke. (2021) 52:3054–62. doi: 10.1161/STROKEAHA.121.034480
47. Menon BK, Al-Ajlan FS, Najm M, Puig J, Castellanos M, Dowlatshahi D et al. Association of clinical, imaging, and thrombus characteristics with recanalization of visible intracranial occlusion in patients with acute ischemic stroke. JAMA. (2018) 320:1017–26. doi: 10.1001/jama.2018.12498
Keywords: stroke, neuroprotection, reperfusion after ischemia, thrombectomy, intravenous thrombolysis
Citation: Vos EM, Geraedts VJ, van der Lugt A, Dippel DWJ, Wermer MJH, Hofmeijer J, van Es ACGM, Roos YBWEM, Peeters-Scholte CMPCD and van den Wijngaard IR (2022) Systematic Review - Combining Neuroprotection With Reperfusion in Acute Ischemic Stroke. Front. Neurol. 13:840892. doi: 10.3389/fneur.2022.840892
Received: 21 December 2021; Accepted: 17 February 2022;
Published: 17 March 2022.
Edited by:
Yuchuan Ding, Wayne State University, United StatesReviewed by:
Sonu M. M. Bhaskar, Department of Neurology and Neurophysiology, AustraliaCopyright © 2022 Vos, Geraedts, van der Lugt, Dippel, Wermer, Hofmeijer, van Es, Roos, Peeters-Scholte and van den Wijngaard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: E. M. Vos, ZS52b3NAaGFhZ2xhbmRlbm1jLm5s
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.