
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 07 March 2022
Sec. Stroke
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.824091
This article is part of the Research TopicTranslational Research on Thrombus Characteristics in Ischemic StrokeView all 6 articles
 Daniela Dumitriu LaGrange1*
Daniela Dumitriu LaGrange1* Vincent Braunersreuther2
Vincent Braunersreuther2 Isabel Wanke3,4,5
Isabel Wanke3,4,5 Jatta Berberat6,7Siri Luthman1
Jatta Berberat6,7Siri Luthman1 Seán Fitzgerald8,9
Seán Fitzgerald8,9 Karen M. Doyle8,9Olivier Brina1Philippe Reymond1Alexandra Platon10Michel Muster1
Karen M. Doyle8,9Olivier Brina1Philippe Reymond1Alexandra Platon10Michel Muster1 Paolo Machi1Pierre-Alexandre Poletti10
Paolo Machi1Pierre-Alexandre Poletti10 Maria Isabel Vargas1
Maria Isabel Vargas1 Karl-Olof Lövblad1
Karl-Olof Lövblad1Background: Characterization of the clot occluding the arteries in acute ischemic stroke received ample attention, in terms of elucidating the relationship between the clot composition, its etiology and its amenability for pharmacological treatment and mechanical thrombectomy approaches. Traditional analytical techniques such as conventional 2D histopathology or electron microscopy sample only small parts of the clot. Visualization and analysis in 3D are necessary to depict and comprehend the overall organization of the clot. The aim of this study is to investigate the potential of microCT for characterizing the clot composition, structure, and organization.
Methods: In a pilot study, we analyzed with microCT clots retrieved from 14 patients with acute ischemic stroke. The following parameters were analyzed: overall clot density, clot segmentation with various density thresholds, clot volume.
Results: Our findings show that human clots are heterogeneous in terms of CT intra-clot density distribution. After fixation in formalin, the clots display a shift toward negative values. On average, we found the mean HU values of red clots retrieved from patients to be −153 HU, with SD = 23.8 HU, for the intermediate clots retrieved from patients −193 HU, SD = 23.7 HU, and for the white clots retrieved from patients −229 HU, SD = 64.8 HU.
Conclusion: Our study shows that volumetric and density analysis of the clot opens new perspectives for clot characterization and for a better understanding of thrombus structure and composition.
The composition of occlusive clots in acute ischemic stroke has received vast attention through two dimensional (2D) histopathology investigations (1–3). Knowledge about human clots composition allowed valuable developments regarding the preparation of clot analogs (4) which best reproduce in terms of cellular and fibrin content the composition of clots retrieved from patients. Clot analogs with predefined compositions were successfully used to define the most effective clinical imaging protocols, computed tomography (CT) (5) or magnetic resonance imaging (MRI) (6), or to study in vitro thrombectomy techniques (4). While clot analogs are a valuable tool for studying clinical imaging and optimizing interventional techniques, the clots retrieved from patients remain the most valuable substrate for research on clot behavior (7). Traditional techniques, such as conventional 2D histopathology and electron microscopy, provide a wealth of information on clot composition, etiology and markers associated with resistance to treatment (8, 9). These techniques, which often sample small representative areas of the clot, provide qualitative information. However, techniques suitable for retrieving quantitative information about the structure and organization of human clots are underdeveloped. When available, such techniques could help establishing meaningful correlations between the clot characteristics and clinical aspects in stroke. Volumetric analysis of the clot is necessary in order to gather quantitative information. Emerging approaches in the field of three dimensional (3D) visualization of clots are fluorescent labeling of clots after optical clearing (10), or integration of signals provided by optical coherence tomography (11). X-rays based imaging techniques, such as microCT, although they have been extensively used for various tissues characterization (12, 13), are still underappreciated in terms of clot characterization.
In our study we perform a preliminary investigation into the potential that microCT holds for characterizing clots retrieved from patients with acute ischemic stroke. We illustrate that clots retrieved from patients vary in terms of CT density, which can be correlated with the clot composition, and display a heterogenous distribution of CT density.
We included in the study 14 patients (7 males, 7 females, age 41–95 years) who were referred to our institution suffering acute stroke, underwent dual-source CT in the emergency department, and did not qualify for thrombolytic treatment prior thrombectomy. Thrombectomy was performed according to the standard clinical practice.
In addition, three types of clot analogs, prepared according to the protocols described elsewhere (4), were made available for imaging with microCT in our study.
Ex vivo experiments were carried out on a low dose X-Ray micro computed tomography scanner (Quantum GX, Perkin Elmer). The scanner uses a cone beam X-ray source and a flat panel X-ray detector to acquire high quality slice images, which are rendered for 3D visualization. The detector was calibrated as such that Hounsfield Units (HU) values were adjusted for air (−1,000) and water (0). Clots were imaged upon placing them in a sealed falcon tube, to maintain moisture and prevent tissue degradation prior to imaging, either as retrieved from patient (fresh) before and after rinsing with saline solution NaCl 0.9%, or after fixation in formalin. Each formalin-fixed clot was rinsed with saline solution, drained on sterile pads and subsequently placed in the sealed falcon tube. The clots were imaged with the low noise imaging protocol (14 min), with 90 kV X-ray energy, 88 μA, and 50 μm voxel size. Segmentation and quantification of clots attenuation ex vivo was performed in 3D Slicer1 (14).
Histology staining was performed after embedding the formalin-fixed clots in paraffin, on 3 micrometers thick slices, according to standard protocols (1) with Martius Scarlet Blue (MSB) and Hematoxylin and Eosin (HE).
The statistics were calculated using SPSS version 25 (SPSS Inc., Chicago, IL, USA). The normality of data distribution was assessed with Shapiro-Wilk test. The relationships between variables (retrieved clot volume and volume of dense part of the clot, average density of the retrieved clot, and retrieved clot volume) were examined using the Spearman rank correlation test.
We included in this preliminary study only patients which did not qualify for thrombolytic therapy. Baseline characteristics are presented in Table 1. The table includes information on the antithrombotic medication prior to thrombotic event, time elapsed from the thrombotic event (when > 4.5 h), conditions contraindicating the thrombolytic therapy, thrombectomy interventions and outcome.
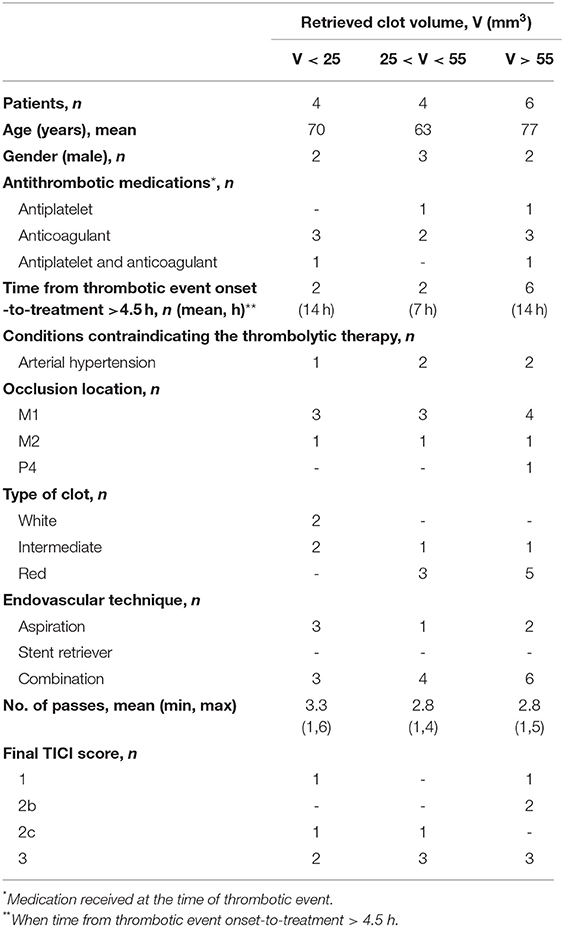
Table 1. Baseline characteristics of patients with acute ischemic stroke included in this pilot study.
Our results are showing that clots retrieved from patients are more diverse in terms of CT density, and display a widespread distribution, compared to clot analogs with pre-established compositions (Figure 1). We observed a systematic decrease in clot density, measured in HU, from fresh (as collected) state, after rinsing with saline solution, and further after fixation in formalin. The mean HU values for human formalin-fixed clots are in negative range. After fixation in formalin, we found an average of mean HU values within red clots group equal to −153 HU, with standard deviation (SD) = 23.8 HU, an average of mean HU within intermediate clots group −193 HU, SD = 23.7 HU, and an average of mean HU within white clots group −229 HU, SD = 64.8 HU. For each clot, no differences were observed in CT density regardless the fixation time (2 h, 6 h, or 3 days), which indicates an initial stabilization in the structural features which are detected with CT, within the first 2 h of fixation in formalin.
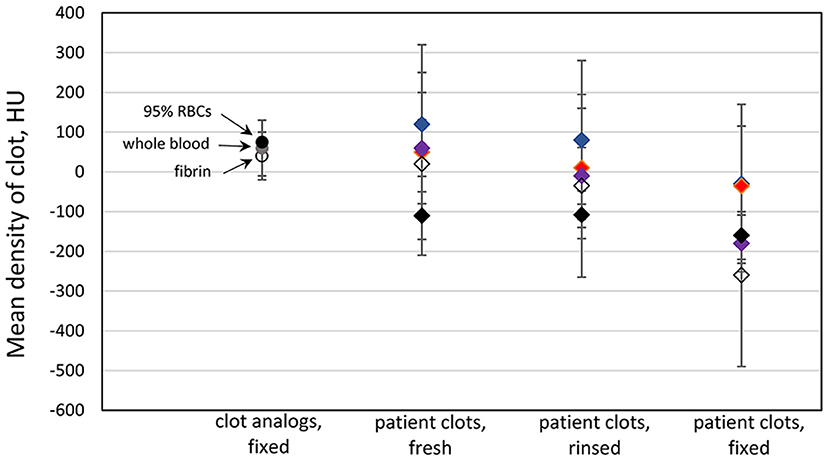
Figure 1. Clot density in microCT—comparison of clot analogs and human clots at different processing stages. Data points represent the mean HU values for each clot, and the bars indicate the standard deviation of the density distribution within each clot. Same color of diamond shape data points was used for each individual clot. The clots were imaged in three states: fresh, rinsed in saline, and after being fixed in formalin.
The microCT appearance of human clots is highly heterogeneous. Typically, a thin region (100–200 micrometers) of low density (−850 to −200 HU) is associated with the partial filling of the voxels at the outer surface of the sample, most likely related with a discontinuous layer of plasma proteins and water (serum) in fresh samples and, especially, in fixed samples, with the surface roughness. An example is illustrated in Figure 2. We observe the presence of dense regions (for which we defined a threshold of 10 HU, density values above those of water range), persistent throughout rinsing and fixing in formalin (Figure 2).
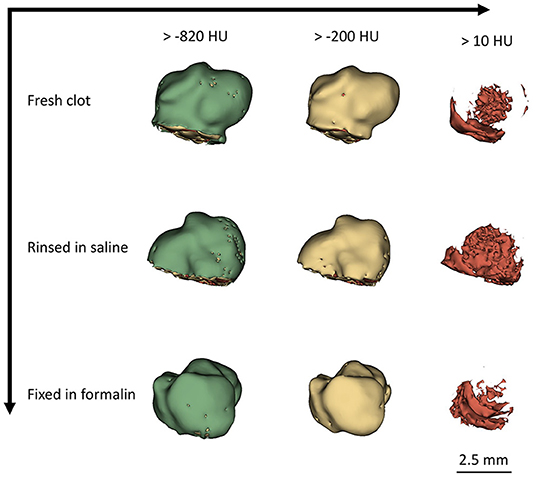
Figure 2. Segmentation of clot at different processing stages.
In a first attempt to investigate how the microCT features relate to the histology of the clot, we performed a side-by-side comparison with histological staining (Figure 3), and information included in Supplemental Material. In absence of 3D histological rendering, an unequivocal assignment of histological features to CT density ranges is not possible. Only a qualitative interpretation of the information rendered by the two techniques, using 2D depiction, can be performed. As such, our data suggest that red blood cells (RBCs) can span a wide range in density (-200 to 200 HU), which is partially overlapped by the density of water (−30 to 10 HU, blue color code in Figure 3A). We observed that in the RBCs rich sample the highest density regions (> 10 HU, above water density) for the clot in wet state (Figure 3A) do translate in the paraffin embedded sample also as relatively augmented CT density regions (Figure 3B) and correspond to compact regions of RBCs in histologically stained slices (Figures 3C,D; Supplemental Material). However, in clots with lower concentrations of RBCs, such as intermediate clots, as presented in Supplementary Figures 1, 2, the regions that appear most dense in wet state fade in density after embedding the clot in paraffin. Only a partial overlap can be observed between the densest regions in wet state with the RBCs agglomerates observed in histological staining.
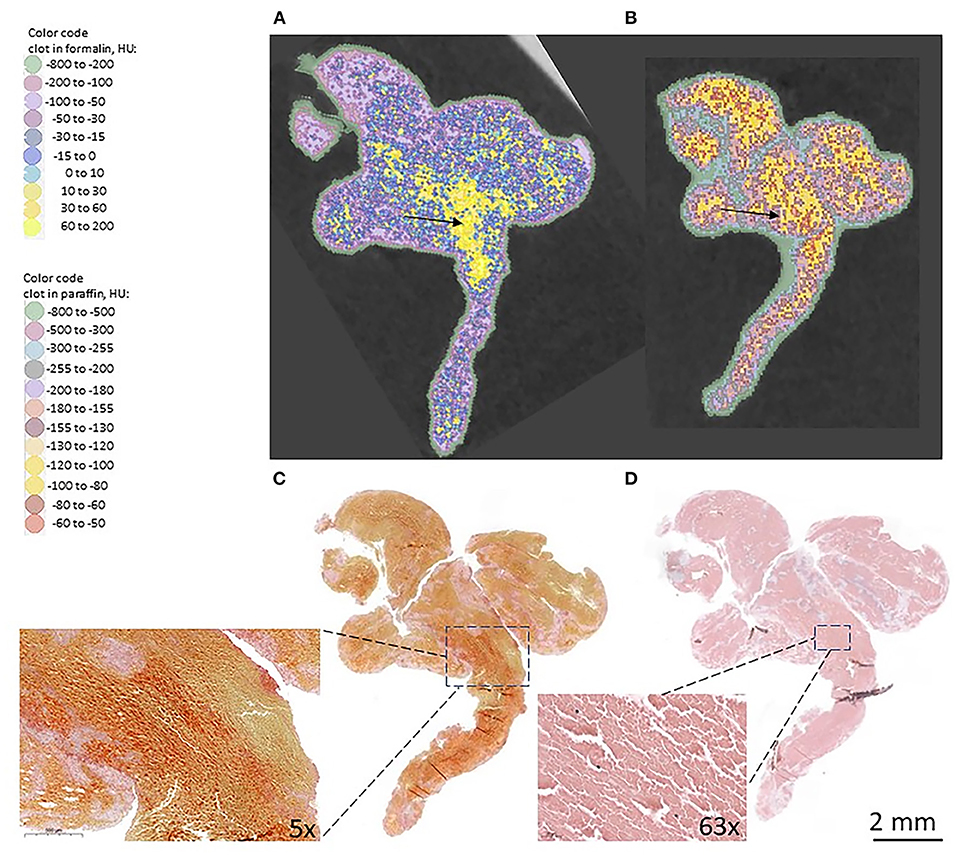
Figure 3. Comparison microCT and histological staining: (A) microCT slice of formalin-fixed clot; (B) microCT slice of clot embedded in paraffin; (C) Histological staining of the clot with Martius Scarlet Blue (MSB), in which RBCs appear yellow and fibrin appears red; (D) Histological staining of the clot with hematoxylin and eosin (HE). In the inset: RBCs rich region.
Platelets and fibrin regions, as identified by histological staining, consistently appear in microCT of fixed samples in low density regions (water density or below) and in paraffin embedded samples overlap, for the most part, with the density of paraffin (−500 to −180 HU, mean 345 HU).
Heterogeneity in various tissues can be analyzed through textural features computed from CT scans (15). Similar algorithms can be applied for analyzing clots retrieved from patients. As an example, maps computed for gray level co-occurrence matrices (GLCM) and gray-level run length matrices (GLRLM) for a retrieved clot are presented in Supplementary Figure 3.
We studied the volumetric CT density distribution of the clots included in our study. In brief, the average volumetric content in regions with density > 10 HU (vd %) is changing as following: 5.34 vol%, with SD = 2.31 vol% for red clots, 3.35 vol%, with SD = 1.19 vol% for intermediate clots, and 0.98 vol% with SD = 0.50 vol% for white clots. We also examined the relation between the volume of dense regions (vd, with >10 HU, above the density of water) and the overall volume of the clot. We found a large positive relationship between the two sets of values, with a Spearman correlation factor r(12) = 0.943 (two-tailed p < 0.001) (Figure 4A). This finding is not surprising, since we observed larger retrieved clot volumes for red clots, compared to the white clots. Contrasting to this finding, we identified only a non-significant medium positive association between the mean HU values of each overall clot and the clot volume [r(12) = 0.4593, two-tailed p value = 0.1043] (Figure 4B), which we consider an indicator for the non-uniform contribution of the porosity to the overall density values of the clot.
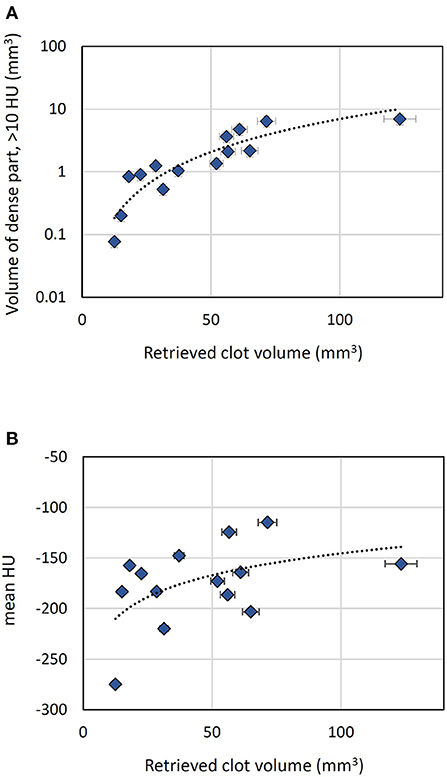
Figure 4. Volumetric analysis of the retrieved clots (data points refer to formalin-fixed clots). (A) Correlation between the volume of dense part of the clot and the overall clot volume. (B) Variation of clot average density (mean HU) with the clot volume.
Occlusive clots causing ischemic stroke, including both thrombi and emboli, form under complex blood flow conditions and have various etiologies. Therefore, the clots retrieved from patients differ from the clot analogs and vary with respect to each other in terms of composition, overall porosity, size, distribution of cellular aggregates, and fibrin organization.
Our study shows that microCT can capture information regarding the heterogeneous intra-clot distribution of density, which we illustrate with segmentations performed for various density ranges. We exemplify that through volumetric analysis of clot CT density we can define quantitative variables which can be correlated with clot organization. A limitation of this study is the small sample size, which does not allow performing correlative links between the textural features and clot composition.
A drawback of the study is a limited access to fresh clots. More research is necessary to elucidate how interstitial blood and residual contrast agent are contributing to the CT density of fresh clots, as retrieved. The CT imaging of fixed clots is most likely devoid of such additional contributions. CT imaging of human clots has the potential to be rendered relevant for histological features of the clot. Imaging fresh clots could become a valuable characterization technique prior to biomechanical testing.
The shift toward negative density values after fixing the clot in formalin is not surprising. We consider it a consequence of the clot dehydration due to the fixation process, which results in hydrophobic effects that trigger an increase in porosity of the overall clot, once removed from formalin solution.
The preparation conditions for histological staining involve some degree of distortion of the original histological material, and a direct compositional correlation between histology slides renderings and microCT cross sectional view is difficult. The microCT slices have a thickness (50 micrometers) much larger than the thickness of the clot slices used for histological staining (3 micrometers). Therefore, the microCT slices integrate more information related to the composition and structure of the clot, compared to the information rendered by each individual histological slide. Especially in small clots with intermediate composition, for which the size of compositionally distinct regions is small, establishing a correspondence between the histological staining and microCT density is unlikely when resolution limits are at play and partial filling effects of individual voxels with different histological structures and media (water or paraffin) occur. However, we still consider the highest density range observed for the clots included in our study (>10 HU and up to 200 HU in wet samples) as being related to the compactness of the clot in preferential regions, most likely with the presence of RBCs agglomerates. We rule out the presence of calcifications as being responsible for the above-mentioned density range (10–200 HU). Calcifications are not specific for red and intermediate clots (16, 17), and, as described in Supplementary Figure 4, the density we observe for calcifications having similar size and distribution as the dense (typically 10–200 HU) regions in red clots is much higher (1,000 HU and above).
Arterial, red clots in acute ischemic stroke are often characterized by core regions of compact RBCs, also known as polyhedrocites, while the outer regions are formed by biconcave RBCs and fibrin (8). Agglomerates of compact RBCs are a marker for clot intravital contraction (8, 18–20). While the clinical implications of clot contraction in acute ischemic stroke remain to be elucidated, it has been hypothesized that clot contraction can be an underlying mechanism that reduces vessel occlusion and allows blood flow past clot (21). MicroCT could be, for example, useful in quantifying the degree of clot contraction and in exploring how clot contraction affects the clinical manifestation of stroke.
Within the limitations of our study, we showed that an attribution of the dense regions found in microCT of fixed clots to RBCs rich compact regions is reasonable. This remains a strong hypothesis, to be verified by future studies, which will be using fiducials to compare microCT volumetric renderings with serial 3D histopathology findings. While handling fresh clots for microCT characterization can prove to be difficult, due to perishability of fresh samples and limited sample availability during normal working hours when microCT operation is possible, handling formalin-fixed samples is much more convenient. A large sample size of clots, measured in fresh and in fixed state, might provide standardized means to best exploit the information gathered from CT characterization of clots retrieved from patients.
Our study shows that volumetric analysis of the clot opens new perspectives for clot characterization. In perspective, correlations between 3D histopathology and microCT can provide quantification of clot composition in terms of CT density.
Our study illustrates that microCT can be used for volumetric characterization of clots retrieved from acute ischemic stroke patients, for which both the intra-clot heterogeneity and inter-patient variability can be addressed.
MicroCT imaging emerges as a characterization technique which can bring new insights about the correlation between the human clots structure and clinical aspects in stroke.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study was approved, under the project ID 2018-00476, by the Cantonal Commission of Research Ethics (Commission cantonale d'éthique de la recherche, CCER) Geneva, who waived the requirement for written informed consent, in accordance with national legislation and institutional requirements.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The project has been funded by grants of the Swiss National Science Foundation (32003B_182382 and 320030_188942), by a grant of University Hospitals of Geneva, Radiology Department Startup fund, and a grant of the Science Foundation Ireland (13/RC/2073_2).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
MicroCT scans were performed using the equipment available within Small Animal Preclinical Imaging Platform (PIPPA), at University of Geneva.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2022.824091/full#supplementary-material
1. ^Available online at: http://www.slicer.org.
1. Staessens S, Denorme F, Francois O, Desender L, Dewaele T, Vanacker P, et al. Structural analysis of ischemic stroke thrombi: histological indications for therapy resistance. Haematologica. (2020) 105:498–507. doi: 10.3324/haematol.2019.219881
2. Staessens S, Fitzgerald S, Andersson T, Clarençon Clarençon F, Denorme F, Gounis M, et al. Histological stroke clot analysis after thrombectomy: technical aspects and recommendations. Int J Stroke. (2020) 15:467–76. doi: 10.1177/1747493019884527
3. Staessens S, De Meyer SF. Thrombus heterogeneity in ischemic stroke. Platelets. (2021) 32:331–9. doi: 10.1080/09537104.2020.1748586
4. Fitzgerald ST, Liu Y, Dai D, Mereuta OM, Abbasi M, Larco JLA, et al. Novel human acute ischemic stroke blood clot analogs for in vitro thrombectomy testing. Am J Neuroradiol. (2021) 42:1250–7. doi: 10.3174/ajnr.A7102
5. Ding YH, Abbasi M, Michalak G, Leng S, Dai D, Fitzgerald S, et al. Characterization of thrombus composition with multimodality CT-based imaging: an in-vitro study. J NeuroInterventional Surg. (2021) 13:738–40. doi: 10.1136/neurintsurg-2020-016799
6. Ding Y, Abbasi M, Liu Y, Dai D, Kadirvel R, Kallmes DF, et al. In vitro study of blood clot identification and composition assessment by different magnetic resonance sequences. Cureus. (2021) 13:e16229. doi: 10.7759/cureus.16229
7. Boodt N, Snouckaert van Schauburg PRW, Hund HM, Fereidoonnezhad B, McGarry JP, Akyildiz AC, et al. Mechanical characterization of thrombi retrieved with endovascular thrombectomy in patients with acute ischemic stroke. Stroke. (2021) 52:2510–7. doi: 10.1161/STROKEAHA.120.033527
8. Weisel JW, Litvinov RI. Visualizing thrombosis to improve thrombus resolution. Res Pract Thromb Haemost. (2021) 5:38–50. doi: 10.1002/rth2.12469
9. Jolugbo P, Ariëns RAS. Thrombus composition and efficacy of thrombolysis and thrombectomy in acute ischemic stroke. Stroke. (2021) 52:1131–42. doi: 10.1161/STROKEAHA.120.032810
10. Höök P, Brito-Robinson T, Kim O, Narciso C, Goodson HV, Weisel JW, et al. Whole blood clot optical clearing for nondestructive 3D imaging and quantitative analysis. Biomed Opt Express. (2017) 8:3671. doi: 10.1364/BOE.8.003671
11. Liu H, Abbasi M, Ding YH, Polley EC, Fitzgerald S, Kadirvel R, et al. Characterizing thrombus with multiple red blood cell compositions by optical coherence tomography attenuation coefficient. J Biophotonics. (2021) 14:e202000364. doi: 10.1002/jbio.202000364
12. de Bournonville S, Vangrunderbeeck S, Kerckhofs G. Contrast-enhanced MicroCT for virtual 3D anatomical pathology of biological tissues: a literature review. Contrast Media Mol Imaging. (2019) 2019:8617406. doi: 10.1155/2019/8617406
13. Senter-Zapata M, Patel K, Bautista PA, Griffin M, Michaelson J, Yagi Y. The role of Micro-CT in 3D histology imaging. Pathobiology. (2016) 83:140–7. doi: 10.1159/000442387
14. Fedorov A, Beichel R, Kalpathy-Cramer J, Finet J, Fillion-Robin JC, Pujol S, et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn Reson Imaging. (2012) 30:1323–41. doi: 10.1016/j.mri.2012.05.001
15. Lubner MG, Smith AD, Sandrasegaran K, Sahani DV, Pickhardt PJ. CT texture analysis: definitions, applications, biologic correlates, and challenges. RadioGraphics. (2017) 37:1483–503. doi: 10.1148/rg.2017170056
16. Chernysh IN, Nagaswami C, Kosolapova S, Peshkova AD, Cuker A, Cines DB, et al. The distinctive structure and composition of arterial and venous thrombi and pulmonary emboli. Sci Rep. (2020) 10:5112. doi: 10.1038/s41598-020-59526-x
17. Mereuta OM, Rossi R, Douglas A, Gil SM, Fitzgerald S, Pandit A, et al. Characterization of the ‘White' appearing clots that cause acute ischemic stroke. J Stroke Cerebrovasc Dis. (2021) 30:106127. doi: 10.1016/j.jstrokecerebrovasdis.2021.106127
18. Cines DB, Lebedeva T, Nagaswami C, Hayes V, Massefski W, Litvinov RI, et al. Clot contraction: compression of erythrocytes into tightly packed polyhedra and redistribution of platelets and fibrin. Blood. (2014) 123:1596–603. doi: 10.1182/blood-2013-08-523860
19. Tutwiler V, Mukhitov AR, Peshkova AD, Le Minh G, Khismatullin RR, Vicksman J, et al. Shape changes of erythrocytes during blood clot contraction and the structure of polyhedrocytes. Sci Rep. (2018) 8:17907. doi: 10.1038/s41598-018-35849-8
20. Tutwiler V, Peshkova AD, Le Minh G, Zaitsev S, Litvinov RI, Cines DB, et al. Blood clot contraction differentially modulates internal and external fibrinolysis. J Thromb Haemost. (2019) 17:361–70. doi: 10.1111/jth.14370
Keywords: clot, acute ischemic stroke, CT density, red blood cells, fibrin
Citation: Dumitriu LaGrange D, Braunersreuther V, Wanke I, Berberat J, Luthman S, Fitzgerald S, Doyle KM, Brina O, Reymond P, Platon A, Muster M, Machi P, Poletti P-A, Vargas MI and Lövblad K-O (2022) MicroCT Can Characterize Clots Retrieved With Mechanical Thrombectomy From Acute Ischemic Stroke Patients–A Preliminary Report. Front. Neurol. 13:824091. doi: 10.3389/fneur.2022.824091
Received: 28 November 2021; Accepted: 31 January 2022;
Published: 07 March 2022.
Edited by:
Nishant K. Mishra, Yale University, United StatesReviewed by:
Stefan Schob, University Hospital in Halle, GermanyCopyright © 2022 Dumitriu LaGrange, Braunersreuther, Wanke, Berberat, Luthman, Fitzgerald, Doyle, Brina, Reymond, Platon, Muster, Machi, Poletti, Vargas and Lövblad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniela Dumitriu LaGrange, RGFuaWVsYS5EdW1pdHJpdUxhZ3JhbmdlQHVuaWdlLmNo
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.