
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 04 March 2022
Sec. Neuromuscular Disorders and Peripheral Neuropathies
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.816636
This article is part of the Research Topic Updating Amyloid Neuropathy Knowledge: From Diagnosis to Treatment View all 5 articles
 Erica Irene Uneus1Christer Wilhelmsson2David Bäckström1Intissar Anan3,4Jonas Wixner3Björn Pilebro5
Erica Irene Uneus1Christer Wilhelmsson2David Bäckström1Intissar Anan3,4Jonas Wixner3Björn Pilebro5 Katrine Riklund6Mattias Ögren6Margareta Ögreen6
Katrine Riklund6Mattias Ögren6Margareta Ögreen6 Jan Axelsson7Ole B. Suhr3*
Jan Axelsson7Ole B. Suhr3* Torbjörn Sundström6
Torbjörn Sundström6Introduction: Hereditary transthyretin (ATTRv) amyloidosis caused by the V30M (p. V50M) mutation is a fatal, neuropathic systemic amyloidosis. Liver transplantation has prolonged the survival of patients and central nervous system (CNS) complications, attributed to amyloid angiopathy caused by CNS synthesis of variant transthyretin, have emerged. The study aimed to ascertain amyloid deposition within the brain in long-term ATTRv amyloidosis survivors with neurological symptoms from the CNS.
Methods: A total of 20 patients with ATTR V30M having symptoms from the CNS and a median disease duration of 16 years (8–25 years) were included in this study. The cognitive and peripheral nervous functions were determined for 18 patients cross-sectionally at the time of the investigation. Amyloid brain deposits were examined by [18F]flutemetamol PET/CT. Five patients with Alzheimer's disease (AD) served as positive controls.
Result: 60% of the patients with ATTRv had a pathological Z-score in the cerebellum, compared to only 20% in the patients with AD. 75% of the patients with transient focal neurological episodes (TFNEs) displayed a pathological uptake only in the cerebellum. Increased cerebellar uptake was related to an early age of onset of the ATTRv disease. 55% of the patients with ATTRv had a pathological Z-score in the global cerebral region compared to 100% of the patients with AD.
Conclusion: Amyloid deposition within the brain after long-standing ATTRv amyloidosis is common, especially in the cerebellum. A cerebellar amyloid uptake profile seems to be related to TFNE symptoms.
The aggregation, distribution, and neurotoxicity of deposited amyloid species in the brain are well-described for the most common neurodegenerative disorder, Alzheimer's disease (AD) (1), but are much less studied in hereditary transthyretin amyloid (ATTRv) amyloidosis. ATTRv is a fatal systemic amyloidosis caused by mutations in the transthyretin (TTR) gene. Amyloid deposition and symptoms are noted for numerous organs such as the peripheral nervous system, heart, eyes, kidneys, and gastrointestinal tract, but rarely for the central nervous system (CNS) (2–4). Currently, more than 140 various mutations are reported with wide variation in the phenotype between the different mutations and within the same mutation (5).
The mechanism behind the phenotypical variation between various mutations has not been established. However, it has been suggested that the combination of low serum levels of mutant relative to wild type TTR together with a mutation that produces a low kinetic and thermodynamic stability of the TTR tetramer predispose to CNS complication. This has been shown for the D18G (pD38G) and A25T (p.A45T) TTR mutations (6, 7). Since this is not the case for the V30M (p.V50M) mutation, this may explain the low occurrence of CNS complications in the natural history of patients with ATTR V30M.
V30M (p.V50M) gives rise to a predominantly neuropathic disease but the phenotype varies. The neuropathic phenotype with early onset (below the age of 50) is associated with an otherwise rarely found type of transthyretin amyloid (ATTR) fibril that consists only of full-length TTR (type B). However, the phenotype characterized by later onset and neuropathy, and cardiomyopathy, is associated with the more common fibril type of a mixture of fragmented and full-length ATTR fibrils (type A) (8).
The disease is relentlessly progressive, and before 1990 when liver transplantation (LTx) was introduced as a treatment, the median survival was 10–13 years for Swedish patients (2, 9). The rationale for LTx was to replace the amyloidogenic mutant TTR produced by the liver with a liver that produced wild-type TTR only. The outcome was encouraging, but continuous deterioration, especially of heart function, was noted for patients with non-TTR V30M and late-onset V30M; this was probably related to amyloid fibril composition (10–12).
Later on, medical treatments have become available, i.e., TTR tetrameric stabilizers since 2011, and recently gene silencing (13–16). However, none of the current treatments affect the variant TTR synthesized by the choroid plexus of the brain or by the retina of the eye, and continuous amyloid formation in the eye has been reported for LTx and medically treated patients (17–19) and also continuous amyloid formation in the leptomeninges after LTx in the TTR Y114C (p.134Y) mutation, a mutation characterized by CNS complications in its natural history (17). In addition, amyloid deposition derived from variant TTR within the brain of patients with long-term surviving LTx was reported from two studies where CNS symptoms attributed to cerebral amyloid angiopathy (CAA) were commonly encountered (20, 21).
The improved survival may provide the necessary time needed for amyloid formation from variant TTR within the brain. However, atrial fibrillation and embolization leading to transient ischemic attack (TIA) and stroke is also common complication in patients with ATTR V30M, and it may be difficult to separate from symptoms of amyloid angiopathy (22).
Detection of ATTR-type CAA by MR examination with gadolinium enhancement has been used to identify meningeal ATTR (23). Further, PET [11C]Pittsburgh component P ([11C]PIB) examination has been used successfully to assess beta-amyloid deposition in the brains of patients with AD and patients with ATTRv (21, 24, 25) and to detect cardiac ATTR (26, 27). However, [11C]PIB's short half-life has promoted the development of newer tracers with longer half-lives and equal imaging properties (28).
Magnetic resonance imaging is suggested to be the most reliable tool in identifying CAA according to modified Boston criteria (29). Since even MRI-secure pacemakers complicate MRI examination, PET with an amyloid tracer appears to be an attractive alternative to detect brain amyloid depositions in patients with ATTRv.
The objective of this study was to visualize the amyloid deposition within the brain in patients with long-standing ATTR V30M amyloidosis and symptoms from the CNS, using PET/CT examinations with a more stable tracer ([18F]flutemetamol). Our primary aim was to evaluate any correlations between the brain amyloid deposition and the symptoms and other disease characteristics of patients. A secondary aim was to see if the amyloid deposition in patients with ATTRv amyloidosis could be distinguished from that of patients with AD. Therefore, patients with AD served as positive controls.
In this cross-sectional observational study, 27 long-term V30M ATTR amyloidosis survivors (≥ 8 years after diagnosis) in the counties of Västerbotten and Norrbotten, Sweden, with symptoms from the CNS were identified. Their CNS symptoms should have had an onset after the diagnosis. All the patients have had their diagnosis settled by genetic testing and a positive biopsy for ATTR. In 11 patients, the fibril type had been determined by Western blot analysis (8).
Seven patients did not participate in this study for various reasons that included dementia and advanced disease. Thus, 20 patients underwent PET/CT examination and their medical records were reviewed. Eighteen patients were liver transplanted and the immune suppression regimes were based on tacrolimus for 13 patients, and on cyclosporine A for 4 patients. Data for one patient were not available. Two patients had been treated by TTR stabilizers (diflunisal or tafamidis). No patient had diabetes and no patient had kidney failure requiring dialysis [four patients had an estimated glomerular filtration rate (eGFR), below 60 ml/min/1.73 m2 based on the CKD-EPI equation]. Clinical data are given in Table 1.
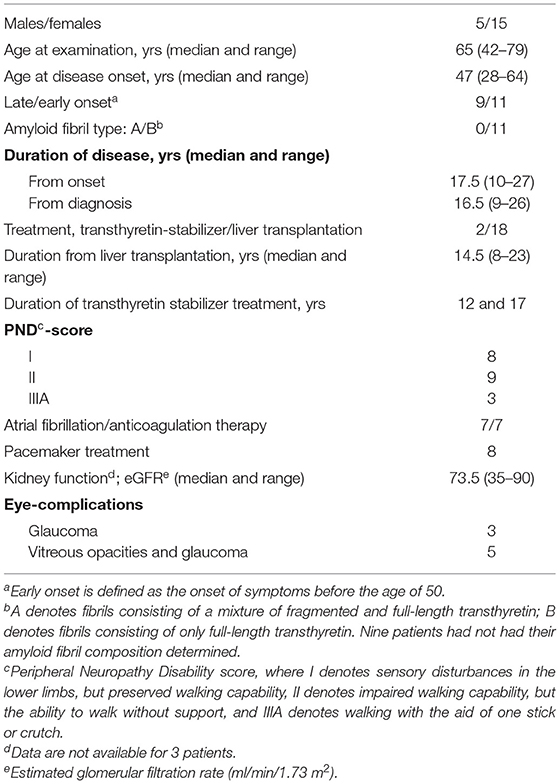
Table 1. Clinical data of the 20 patients with hereditary transthyretin amyloid amyloidosis.
One patient died from septicemia before the planned neurological assessment and one patient desired not to be informed of the outcome of the PET examination or to undergo neurological assessment. Thus, 18 patients underwent clinical evaluation.
Five male patients (age 58–75 years, 3–8 years of cognitive decline), all diagnosed with AD by 18F-fluorodeoxyglucose PET/CT examination and cerebrospinal fluid A-beta levels, were included as a positive control group.
A total of 18 patients with ATTRv amyloidosis were evaluated with interviews and clinical examinations between October 2018 and April 2019 after completion of the PET/CT examination. The assessments were done by one examiner (co-author EU). The patients were interviewed for neurological symptoms, especially those indicating transient focal neurological episodes (TFNEs) (30). The peripheral neuropathy disability (PND) score (I–IV) was used to grade the neuropathy and mobilization of patients, where I denotes sensory disturbances in the lower limbs but preserved walking capability, and IV denotes confined to a wheelchair or bedridden (31). Cognitive assessment was made with the Montreal Cognitive Assessment (MoCA) score that has high sensitivity and specificity for mild cognitive impairment and mild AD (90–100% and 87–100, respectively) when a cut-off score of 26 is used (32). The neuropathy was assessed by the Neuropathy Impairment Score-Lower Limbs (NIS-LL), which is well-validated as a reliable measure of ATTR neuropathy (33).
This study did not include concomitant MR brain imaging. Eight patients wore a pacemaker, which prevents MR examination for research purposes. A majority of the patients (13/20) had undergone a CT or MR examination within 4 years. Six of these patients had MR imaging (of which three were with gadolinium contrast), and seven had CT brain imaging (of which four showed ischemic stroke). One of the three patients who had MR imaging with gadolinium contrast had a pronounced leptomeningeal enhancement.
All the PET/CT examinations were acquired with a GE Discovery 690 PET/CT scanner (General Electric, Wisconsin, USA). The participants were injected intravenously with 173–195 MBq (4.7–5.3 mCi) [18F]flutemetamol that was manufactured according to PET Current Good Manufacturing Practice (cGMP) standards (34, 35). Following a low-dose CT (120 kV, 10 mA, 0.8 s rotation time), a 30-min PET scan of the brain was performed that started 90 min postinjection. All the PET images were reconstructed to a voxel size of 1.95 × 1.95 × 3.27 mm3 with the VuePoint SharpIR iterative algorithm (6 iterations, 24 subsets, 3.0 mm cutoff filter) employing time-of-flight, decay, attenuation, and scatter correction (28, 36).
Data were analyzed with the CortexID software (GE Healthcare) that compares brain regions to a built-in atlas of healthy (age 30–85 years) 18F-flutemetamol scans (37). Relative uptake is quantified for each region as the uptake is divided by the uptake in the reference region pons. The Z-score relative to the healthy-subject database is calculated for each region. In addition, a global composite Z-score for multiple brain regions is calculated (38). A Z-score above two is classified as an abnormally increased amyloid burden. Cortex-ID has no age correction for [18F]flutemetamol because amyloid density measured by amyloid PET in negative patients has a very weak correlation with the age of the patient.
Non-parametrical methods were used for descriptive and statistical analysis. Differences between groups were analyzed by the Mann–Whitney U test and correlations by the Spearman's test. A P-value below 0.05 was accepted as statistically significant.
This study was approved on April 4, 2017 by the regional Ethics Committee at the Umeå University (2017/84-31). All the patients, and when appropriate for patients with AD a close relative, were informed orally and in writing of this study, and all had agreed to participate and signed a consent form.
The neurological symptoms and findings are shown in Table 2. All 11 the patients, who had had their ATTR fibril type determined had type B fibrils, and their [18F]flutemetamol uptake was not different from that of the remaining 9 patients; therefore, we believe that we have a homogeneous group of mostly type B patients. The outcome of [18F]flutemetamol PET is shown in Table 3 and given in Figure 1.
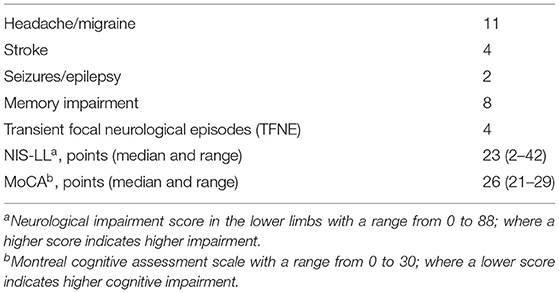
Table 2. Neurological symptoms and findings.
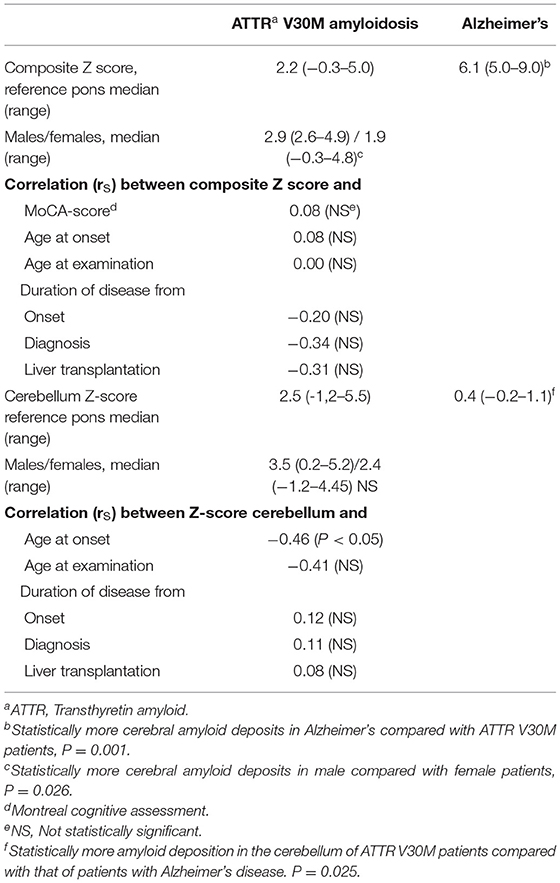
Table 3. Outcome of [18F]flutemetamol PET/CT examination.
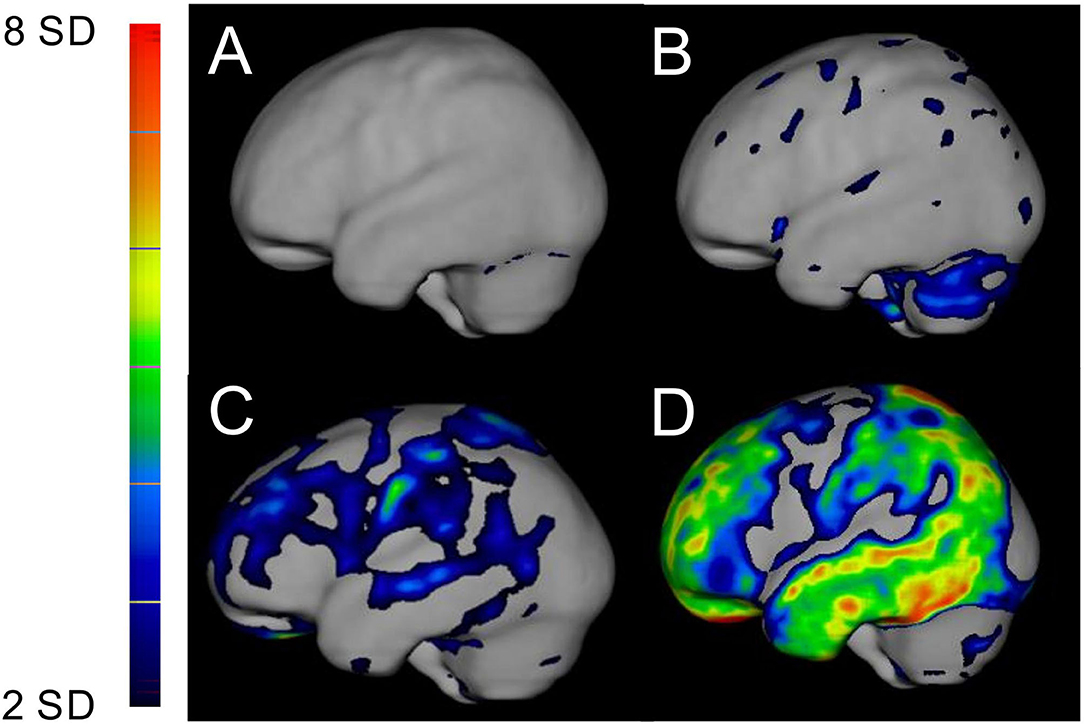
Figure 1. PET/CT examination of [18F]flutemetamol shown as Z-score in the brain in relation to pons from a left lateral view of the brain. The intensity of the uptakes is visualized on the left panel and is graded from low increased uptake in blue (Z-score +2SD) to high increased uptake in red (Z-score +8SD). (A) An ATTR V30M patient with 15 years of disease showing no increased uptake; (B) an ATTR V30M patient with 16 years of disease showing increased uptake in the cerebellum, (C) an ATTR V30M patient with 27 years of disease showing diffuse increased uptake in the brain, and (D) an Alzheimer's patient with generalized increased uptake in the frontoparietotemporal regions.
55% of the patients with ATTRv amyloidosis had an abnormally increased cerebral amyloid burden (global composite Z-score > 2) compared to 100% in the patients with AD.
The composite Z-score was significantly lower in the patients with ATTRv amyloidosis compared to the patients with AD. There was no correlation between the patients with ATTRv amyloidosis global composite Z-score and ATTRv disease duration, onset, time of diagnosis, or MoCA score (Table 3). However, the male patient displayed a higher uptake than female patients. Seventy-five percent of the patients with ATTRv had a pathological Z-score in either the global composite cerebral or cerebellar region.
In the cerebellum, the Z-score was pathological (Z-score > 2) in 60% of the patients compared to 20% in the patients with AD. The patients with ATTRv amyloidosis had a significantly higher Z-score in the cerebellum than the patients with AD (P = 0.025). There was no correlation with the duration of the disease (Table 3). However, the cerebellar Z-score of patients with ATTRv amyloidosis was correlated with their age at disease onset, where younger patients showed a higher cerebellar [18F]flutemetamol uptake (Figure 2 and Table 3).
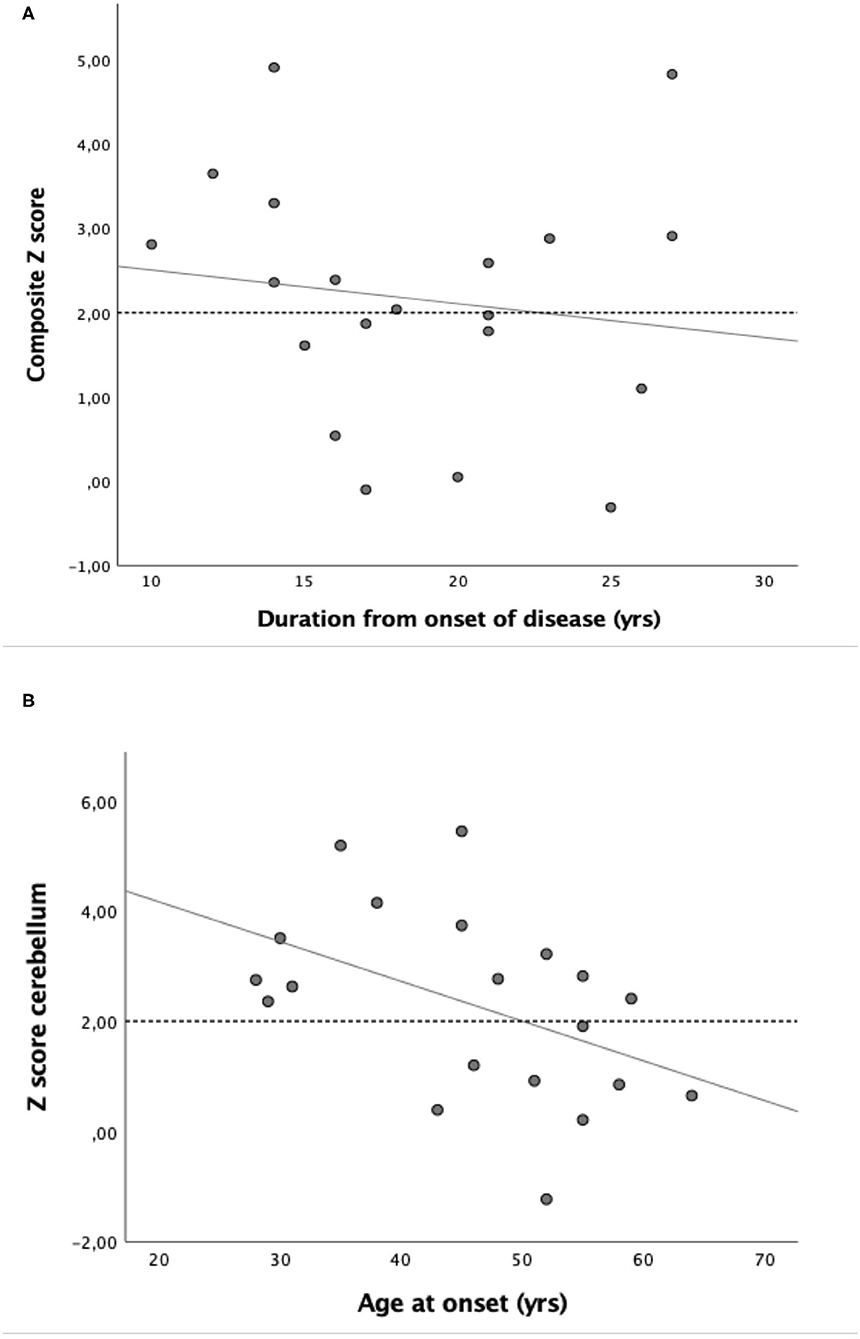
Figure 2. Scatter plot of the relationship between (A) composite Z-score and duration of disease from diagnosis (rS = −0.20; NS) and (B) relationship between Z-score cerebellum and age at onset (rS = −0.45; P < 0.05).
Figure 2 indicates that the patients with ATTR V30M appear to consist of two groups; one with an age of onset above 40 years in which the increased brain amyloid deposition (Z-score > 2) is evenly distributed between the different regions, and another group with a disease onset below the age of 40 in which the amyloid distribution is noted especially in the cerebellum. Five patients with ATTRv showed a pathological Z-score only in the cerebellum (and a non-pathological global composite Z-score). No significant difference in uptake between males and females was noted.
In Figure 3, we have summarized the Z-score pattern for all the brain regions in patients with ATTRv below and over 40 years of age together with patients with AD. In contrast to the older group, the younger group shows a pattern with pathological Z-score in the cerebellum, sensorimotor cortex, and mesial temporal regions. In all the other regions, between 30 and 70% of the patients with ATTR V30M showed a pathological Z-score compared to almost 100% in the AD group. Interestingly, the younger age group (<40 years at onset) had a higher percentage of pathological Z-scores in the mesial temporal region compared to that of patients with AD.
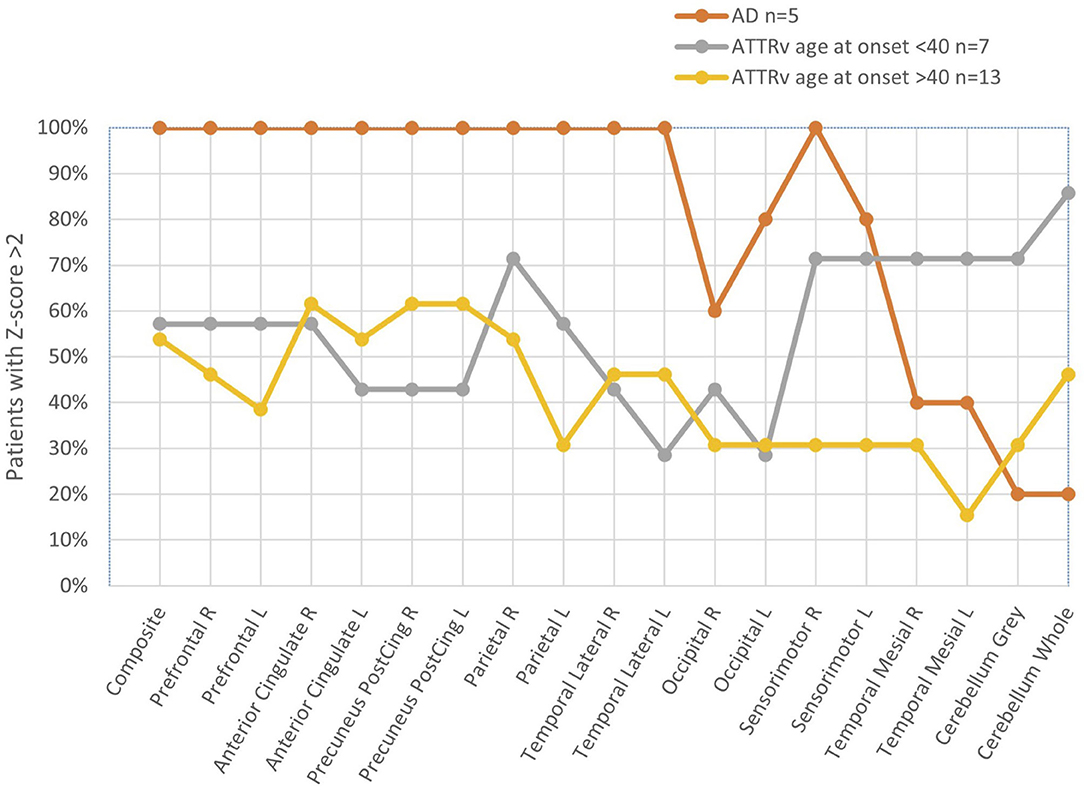
Figure 3. Fraction of patients with pathological Z-score (>2) in different brain regions. Curves represent patient groups: AD (orange), ATTR V 30M age <40 (gray), and ATTR V30M age >40 years (yellow).
No correlation was noted for any region between cognitive impairment (MoCA) and amyloid uptake (pre-frontal, anterior and posterior cingulate, precuneus, parietal, mesial and lateral temporal, occipital, sensorimotor, and cerebellum).
Four patients had transient focal neurological episodes (TFNEs) that included speech difficulties or aphasia, migrating paraesthesia in one arm, and for one patient a status epilepticus. Interestingly, three of the four patients with TFNEs belonged to the group of five patients with pathological cerebellar uptake, but normal global composite Z-scores (the 4th patient with TFNE had no signs of CNS amyloid). In addition, the patient with abnormal contrast enhancement on MR examination and symptoms consistent with TFNEs displayed a high cerebellar Z-score (4.15), but a normal global composite Z-score (1.87). None of the patients with TFNEs, including the patient with status epilepticus, had a composite Z-score >2.
Four other patients displayed a radiological confirmed ischemic stroke. All of these patients had atrial fibrillation and a composite median Z-score of 2.42 (−0.1 to 4.84).
The main findings in this study were that even though the amyloid deposition in the brain, visualized with the amyloid tracer [18F]flutemetamol in long-term ATTR V30M survivors was higher compared with the healthy-subject database (28), not all the patients developed abnormal amyloid deposits in the brain, irrespective of long disease duration. Furthermore, the depositions were especially confined to the cerebellum, which was related to age at disease onset, but not to disease duration. The latter is in contrast to the findings reported from Japan, where the uptake was correlated with disease duration (21). Since Japanese and Portuguese patients with ATTR V30M are generally younger at their disease onset, this may explain the higher reported incidence of CNS complications in their populations (20, 21).
Our findings indicate that a subgroup of patients is more susceptible to brain ATTR amyloid formation. It can be speculated, that an early onset of the disease implies that the ability of the chaperone system to degrade misfolded proteins is impaired at a young age. We have previously shown, that livers from patients with ATTR V30M have an impaired ER/protein folding pathway with differences in gene expression of chaperones [(39) #70]. The situation may be similar in the TTR producing choroid plexus of the brain, i.e., that an early onset of the disease is associated with an early and a more profound dysfunction of the chaperone system.
We observed that the probability of pathological cerebellar uptake was three times higher in patients with ATTRv than in patients with AD. It may be speculated that the molecular structure (i.e., the strain conformation) of deposited amyloid in ATTRv is different from amyloid-β fibrils deposited in AD in such a way that amyloid seeding will preferentially target different cell populations and structures (i.e., occurring with a cerebellar distribution rather than occurring more diffusely in the neocortex as in AD) (40). However, the molecular and functional differences between brain amyloid formation in ATTRv and AD are not well-understood. The higher uptake in the cerebellum of patients with ATTRv amyloidosis compared with that of patients with AD was previously reported (21).
For patients characterized by CNS symptoms in the natural history of the disease, a poor outcome has generally been observed after LTx (12). However, for the Y114C, the outcome has been acceptable even though an increased meningeal amyloid accumulation after transplantation was noted (17, 41).
A secondary aim of this study was to see if patients with ATTRv having CNS amyloid could be distinguished from patients with AD using PET/CT examinations. Since patients with ATTRv had a more pronounced cerebellar distribution than patients with AD, we suggest that a pathological cerebellar [18F]flutemetamol uptake in patients with ATTRv points to ATTR deposition rather than AD.
Three patients with TFNEs displayed pathological cerebellar uptake with non-significant global cerebral uptake, a finding that supports the clinical relevance of increased cerebellar uptake as a marker of ATTR CAA in patients with TFNEs. Interestingly, vascular amyloid depositions in the cerebellum, is usually confined to cerebellar cortical and leptomeningeal vessels (42), and a robust association between a strictly superficial cerebellar microbleed pattern and CAA has been noted (43).
CAA symptoms were suggested to be caused by an “amyloid spell” leading to micro-bleedings (44). Interestingly, microbleedings were previously been reported in long-term ATTR amyloidosis survivors (20, 45). It should be mentioned that [11C]PIB PET did not show increased uptake in a Japanese patient with biopsy verified amyloid depositions within the brain, but MR examination showed late gadolinium enhancement of the meninges (46). It would be interesting to compare amyloid PET with gadolinium contrast MR in these patients.
Atrial fibrillation and cardiac embolization are well-recognized complications for this group of patients (22), and four of our patients with ischemic stroke had atrial fibrillation and were on anticoagulation therapy. Their composite Z-scores varied from normal to clearly increased. However, our findings suggest that if a PET examination with an amyloid tracer displays no increased amyloid depositions within the cerebellum, a search for intermittent atrial fibrillation should be considered.
We still treat atrial fibrillation with anticoagulation (22), but we recommend novel oral anticoagulants (NOAC), even though the evidence is lacking for a decreased bleeding risk for NOAC treated patients with ATTRv (47).
All patients that had their amyloid fibril type determined had type B, i.e., full-length TTR. In a previous heart study, a higher affinity of [18F]flutemetamol and [11C]PIB was noted for patients with type B fibrils (26, 48). However, the fibril type in ATTR CAA has not been determined in any patient, and we do not know if the fibril type found in fat pad biopsies also represents the fibril type within the brain.
We noted that memory disturbances were reported by nearly 50% of the patients. Although there was no correlation between composite Z and MoCA scores, the frequently reported memory disturbances merit further investigation. All patients with increased Z-score, and who complained of memory disturbances were offered further evaluation according to the study protocol.
We did not have a reference group of healthy age-matched controls. We acknowledged that the ethical consequences of investigating healthy individuals could be problematic, since it is well-recognized that accumulation of amyloid within the brain occurs years before the individual displays any symptoms of AD, so we did not achieve ethical permission to investigate healthy controls. It would also have been interesting to investigate patients with mutations characterized by CNS complications in the natural history of the disease; however, no such patients were available.
In the evaluation of cerebral amyloid load, the analysis method was adapted from that used for patients with AD. One limitation could be that ATTRv is a systemic amyloid disease affecting all regions probably including the reference pons region. This might lead to false-negative results since the method relies on a ratio toward the reference region. Some of the patients with a high cerebellar uptake might have an accompanying increased uptake in adjacent pons leading to an underestimated Z-score.
In addition, the amyloid fibril composition within the brain has not been determined in any patient and considering the lower affinity of the tracer for type A fibrils, patients with type A ATTR depositions within the bran may have been missed.
Amyloid deposition within the brain after long-standing ATTRv amyloidosis is common, especially in the cerebellum. A cerebellar amyloid uptake profile seems to be related to TFNE symptoms suggestive of a possible CNS phenotype.
The raw data supporting the conclusions of this article will be made available by the authors on reasonable request and in accordance with Swedish data security rules.
The studies involving human participants were reviewed and approved by the Regional Ethics Committee at Umeå University, Umeå, Sweden. The patients/participants provided their written informed consent to participate in this study.
OS, EU, IA, JW, BP, and TS: initiation and planning of the study. EU, CW, IA, MÖgren, MÖgreen, JA, OS, and TS: investigation and data acquisition. JA and TS: methodology. OS and EU: project administration. OS and KR: resources. EU: writing original draft. EU, CW, DB, IA, JW, BP, KR, JA, OS, and TS: writing—review and editing. All authors contributed to the article and approved the submitted version.
This study was funded by grants from the Swedish Heart and Lung Foundation grant no. 20160787 (OS), an ALF-grant from the Region of Västerbotten, Hjärnfonden (DB), and from the patients' organization FAMY and FAMY Norbotten and the AMYL foundation (JW and IA).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors are indebted to the patients and their families for participating in this study and to Albert Crenshaw for editing the language.
1. Serpell LC. Alzheimer's amyloid fibrils: structure and assembly. Biochim Biophys Acta. (2000) 1502:16–30. doi: 10.1016/S0925-4439(00)00029-6
2. Andersson R. Familial amyloidosis with polyneuropathy. A clinical study based on patients living in northern Sweden. Acta Med Scand Suppl. (1976) 590:1–64.
3. Benson MD, Kincaid JC. The molecular biology and clinical features of amyloid neuropathy. Muscle Nerve. (2007) 36:411–23. doi: 10.1002/mus.20821
4. Plante-Bordeneuve V, Said G. Familial amyloid polyneuropathy. Lancet Neurol. (2011) 10:1086–97. doi: 10.1016/S1474-4422(11)70246-0
5. Rowczenio D, Wechalekar A. Mutations in Hereditary Amyloidosis. Available online at: http://amyloidosismutations.com/ (accessed January 20, 2022).
6. Hammarstrom P, Sekijima Y, White JT, Wiseman RL, Lim A, Costello CE, et al. D18G transthyretin is monomeric, aggregation prone, and not detectable in plasma and cerebrospinal fluid: a prescription for central nervous system amyloidosis? Biochemistry. (2003) 42:6656–63. doi: 10.1021/bi027319b
7. Sekijima Y, Hammarstrom P, Matsumura M, Shimizu Y, Iwata M, Tokuda T, et al. Energetic characteristics of the new transthyretin variant A25T may explain its atypical central nervous system pathology. Lab Invest. (2003) 83:409–17. doi: 10.1097/01.LAB.0000059937.11023.1F
8. Ihse E, Ybo A, Suhr O, Lindqvist P, Backman C, Westermark P. Amyloid fibril composition is related to the phenotype of hereditary transthyretin V30M amyloidosis. J Pathol. (2008) 216:253–61. doi: 10.1002/path.2411
9. Suhr O, Danielsson A, Holmgren G, Steen L. Malnutrition and gastrointestinal dysfunction as prognostic factors for survival in familial amyloidotic polyneuropathy. J Intern Med. (1994) 235:479–85. doi: 10.1111/j.1365-2796.1994.tb01106.x
10. Ericzon BG, Wilczek HE, Larsson M, Wijayatunga P, Stangou A, Pena JR, et al. Liver transplantation for hereditary transthyretin amyloidosis: after 20 years still the best therapeutic alternative? Transplantation. (2015) 99:1847–54. doi: 10.1097/TP.0000000000000574
11. Gustafsson S, Ihse E, Henein MY, Westermark P, Lindqvist P, Suhr OB. Amyloid fibril composition as a predictor of development of cardiomyopathy after liver transplantation for hereditary transthyretin amyloidosis. Transplantation. (2012) 93:1017–23. doi: 10.1097/TP.0b013e31824b3749
12. Suhr OB, Larsson M, Ericzon BG, Wilczek HE, FAPWTR's investigators. Survival after transplantation in patients with mutations other than Val30Met: extracts from the FAP world transplant registry. Transplantation. (2016) 100:373–81. doi: 10.1097/TP.0000000000001021
13. Adams D, Gonzalez-Duarte A, O'Riordan WD, Yang CC, Ueda M, Kristen AV, et al. Patisiran, an RNAi therapeutic, for hereditary transthyretin amyloidosis. N Engl J Med. (2018) 379:11–21. doi: 10.1056/NEJMoa1716153
14. Benson MD, Waddington-Cruz M, Berk JL, Polydefkis M, Dyck PJ, Wang AK, et al. Inotersen treatment for patients with hereditary transthyretin amyloidosis. N Engl J Med. (2018) 379:22–31. doi: 10.1056/NEJMoa1716793
15. Berk JL, Suhr OB, Obici L, Sekijima Y, Zeldenrust SR, Yamashita T, et al. Repurposing diflunisal for familial amyloid polyneuropathy: a randomized clinical trial. JAMA. (2013) 310:2658–67. doi: 10.1001/jama.2013.283815
16. Coelho T, Maia LF, Martins da Silva A, Waddington Cruz M, Plante-Bordeneuve V, Lozeron P, et al. Tafamidis for transthyretin familial amyloid polyneuropathy: a randomized, controlled trial. Neurology. (2012) 79:785–92. doi: 10.1212/WNL.0b013e3182661eb1
17. Ando Y, Terazaki H, Nakamura M, Ando E, Haraoka K, Yamashita T, et al. A different amyloid formation mechanism: de novo oculoleptomeningeal amyloid deposits after liver transplantation. Transplantation. (2004) 77:345–9. doi: 10.1097/01.TP.0000111516.60013.E6
18. Casal I, Monteiro S, Beirao JM. Tafamidis in hereditary ATTR amyloidosis – our experience on monitoring the ocular manifestations. Amyloid. (2016) 23:262–3. doi: 10.1080/13506129.2016.1236332
19. Sandgren O, Kjellgren D, Suhr OB. Ocular manifestations in liver transplant recipients with familial amyloid polyneuropathy. Acta ophthalmologica. (2008) 86:520–4. doi: 10.1111/j.1600-0420.2007.01098.x
20. Maia LF, Magalhaes R, Freitas J, Taipa R, Pires MM, Osorio H, et al. CNS involvement in V30M transthyretin amyloidosis: clinical, neuropathological and biochemical findings. J Neurol Neurosurg Psychiatry. (2015) 86:159–67. doi: 10.1136/jnnp-2014-308107
21. Sekijima Y, Yazaki M, Oguchi K, Ezawa N, Yoshinaga T, Yamada M, et al. Cerebral amyloid angiopathy in posttransplant patients with hereditary ATTR amyloidosis. Neurology. (2016) 87:773–81. doi: 10.1212/WNL.0000000000003001
22. Wange N, Anan I, Ericzon BG, Pennlert J, Pilebro B, Suhr OB, et al. Atrial fibrillation and central nervous complications in liver transplanted hereditary transthyretin amyloidosis patients. Transplantation. (2018) 102:e59–66. doi: 10.1097/TP.0000000000001975
23. Blevins G, Macaulay R, Harder S, Fladeland D, Yamashita T, Yazaki M, et al. Oculoleptomeningeal amyloidosis in a large kindred with a new transthyretin variant Tyr69His. Neurology. (2003) 60:1625–30. doi: 10.1212/01.WNL.0000065901.18353.AB
24. Hellstrom-Lindahl E, Westermark P, Antoni G, Estrada S. In vitro binding of [H]PIB to human amyloid deposits of different types. Amyloid. (2014) 21:21–7. doi: 10.3109/13506129.2013.860895
25. Klunk WE, Engler H, Nordberg A, Wang Y, Blomqvist G, Holt DP, et al. Imaging brain amyloid in Alzheimer's disease with Pittsburgh Compound-B. Ann Neurol. (2004) 55:306–19. doi: 10.1002/ana.20009
26. Pilebro B, Arvidsson S, Lindqvist P, Sundstrom T, Westermark P, Antoni G, et al. Positron emission tomography (PET) utilizing Pittsburgh compound B (PIB) for detection of amyloid heart deposits in hereditary transthyretin amyloidosis (ATTR). J Nucl Cardiol. (2018) 25:240–8. doi: 10.1007/s12350-016-0638-5
27. Takasone K, Katoh N, Takahashi Y, Abe R, Ezawa N, Yoshinaga T, et al. Non-invasive detection and differentiation of cardiac amyloidosis using (99m)Tc-pyrophosphate scintigraphy and C-Pittsburgh compound B PET imaging. Amyloid. (2020) 27:266–74. doi: 10.1080/13506129.2020.1798223
28. Vandenberghe R, Van Laere K, Ivanoiu A, Salmon E, Bastin C, Triau E, et al. 18F-flutemetamol amyloid imaging in Alzheimer disease and mild cognitive impairment: a phase 2 trial. Ann Neurol. (2010) 68:319–29. doi: 10.1002/ana.22068
29. Charidimou A, Martinez-Ramirez S, Reijmer YD, Oliveira-Filho J, Lauer A, Roongpiboonsopit D, et al. Total magnetic resonance imaging burden of small vessel disease in cerebral amyloid angiopathy: an imaging-pathologic study of concept validation. JAMA Neurol. (2016) 73:994–1001. doi: 10.1001/jamaneurol.2016.0832
30. Charidimou A, Baron JC, Werring DJ. Transient focal neurological episodes, cerebral amyloid angiopathy, and intracerebral hemorrhage risk: looking beyond TIAs. Int J Stroke. (2013) 8:105–8. doi: 10.1111/ijs.12035
31. Suhr OB, Holmgren G, Steen L, Wikstrom L, Norden G, Friman S, et al. Liver transplantation in familial amyloidotic polyneuropathy. Follow-up of the first 20 Swedish patients. Transplantation. (1995) 60:933–8. doi: 10.1097/00007890-199511150-00009
32. Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
33. Adams D, Coelho T, Obici L, Merlini G, Mincheva Z, Suanprasert N, et al. Rapid progression of familial amyloidotic polyneuropathy: a multinational natural history study. Neurology. (2015) 85:675–82. doi: 10.1212/WNL.0000000000001870
34. Koole M, Lewis DM, Buckley C, Nelissen N, Vandenbulcke M, Brooks DJ, et al. Whole-body biodistribution and radiation dosimetry of 18F-GE067: a radioligand for in vivo brain amyloid imaging. J Nucl Med. (2009) 50:818–22. doi: 10.2967/jnumed.108.060756
35. Nelissen N, Van Laere K, Thurfjell L, Owenius R, Vandenbulcke M, Koole M, et al. Phase 1 study of the Pittsburgh compound B derivative 18F-flutemetamol in healthy volunteers and patients with probable Alzheimer disease. J Nucl Med. (2009) 50:1251–9. doi: 10.2967/jnumed.109.063305
36. Bettinardi V, Presotto L, Rapisarda E, Picchio M, Gianolli L, Gilardi MC. Physical performance of the new hybrid PETCT Discovery-690. Med Phys. (2011) 38:5394–411. doi: 10.1118/1.3635220
37. Lundqvist R, Lilja J, Thomas BA, Lotjonen J, Villemagne VL, Rowe CC, et al. Implementation and validation of an adaptive template registration method for 18F-flutemetamol imaging data. J Nucl Med. (2013) 54:1472–8. doi: 10.2967/jnumed.112.115006
38. Thurfjell L, Lilja J, Lundqvist R, Buckley C, Smith A, Vandenberghe R, et al. Automated quantification of 18F-flutemetamol PET activity for categorizing scans as negative or positive for brain amyloid: concordance with visual image reads. J Nucl Med. (2014) 55:1623–8. doi: 10.2967/jnumed.114.142109
39. Norgren N, Olsson M, Nystrom H, Ericzon BG, de Tayrac M, Genin E, et al. Gene expression profile in hereditary transthyretin amyloidosis: Differences in targeted and source organs. Amyloid. (2014) 21:113. doi: 10.3109/13506129.2014.894908
40. Qiang W, Yau WM, Lu JX, Collinge J, Tycko R. Structural variation in amyloid-beta fibrils from Alzheimer's disease clinical subtypes. Nature. (2017) 541:217–21. doi: 10.1038/nature20814
41. Yamashita T, Ando Y, Ueda M, Nakamura M, Okamoto S, Zeledon ME, et al. Effect of liver transplantation on transthyretin Tyr114Cys-related cerebral amyloid angiopathy. Neurology. (2008) 70:123–8. doi: 10.1212/01.wnl.0000287089.28847.b5
42. Yamada M, Tsukagoshi H, Otomo E, Hayakawa M. Cerebral amyloid angiopathy in the aged. J Neurol. (1987) 234:371–6. doi: 10.1007/BF00314080
43. Pasi M, Pongpitakmetha T, Charidimou A, Singh SD, Tsai HH, Xiong L, et al. Cerebellar microbleed distribution patterns and cerebral amyloid angiopathy. Stroke. (2019) 50:1727–33. doi: 10.1161/STROKEAHA.119.024843
44. Charidimou A, Law R, Werring DJ. Amyloid “spells” trouble. Lancet. (2012) 380:1620. doi: 10.1016/S0140-6736(12)61333-6
45. Salvi F, Pastorelli F, Plasmati R, Morelli C, Rapezzi C, Bianchi A, et al. Brain microbleeds 12 years after orthotopic liver transplantation in Val30Met amyloidosis. J Stroke Cerebrovasc Dis. (2015) 24:e149–51. doi: 10.1016/j.jstrokecerebrovasdis.2015.02.015
46. Yamada Y, Fukushima T, Kodama S, Shimizu H, Kakita A, Makino K, et al. A case of cerebral amyloid angiopathy-type hereditary ATTR amyloidosis with Y69H (p. Y89H) variant displaying transient focal neurological episodes as the main symptom. Amyloid. (2019) 26:251–2. doi: 10.1080/13506129.2019.1632829
47. Mitrani LR, De Los Santos J, Driggin E, Kogan R, Helmke S, Goldsmith J, et al. Anticoagulation with warfarin compared to novel oral anticoagulants for atrial fibrillation in adults with transthyretin cardiac amyloidosis: comparison of thromboembolic events and major bleeding. Amyloid. (2021) 28:30–4. doi: 10.1080/13506129.2020.1810010
Keywords: amyloidosis-hereditary, amyloid angiopathy, [18F]flutemetamol, positron emission tomography, transthyretin
Citation: Uneus EI, Wilhelmsson C, Bäckström D, Anan I, Wixner J, Pilebro B, Riklund K, Ögren M, Ögreen M, Axelsson J, Suhr OB and Sundström T (2022) Cerebellar and Cerebral Amyloid Visualized by [18F]flutemetamol PET in Long-Term Hereditary V30M (p.V50M) Transthyretin Amyloidosis Survivors. Front. Neurol. 13:816636. doi: 10.3389/fneur.2022.816636
Received: 16 November 2021; Accepted: 12 January 2022;
Published: 04 March 2022.
Edited by:
Giuseppe Vita, University of Messina, ItalyReviewed by:
Márcia A. Liz, Universidade do Porto, PortugalCopyright © 2022 Uneus, Wilhelmsson, Bäckström, Anan, Wixner, Pilebro, Riklund, Ögren, Ögreen, Axelsson, Suhr and Sundström. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ole B. Suhr, b2xlLnN1aHJAdW11LnNl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.