
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 21 December 2022
Sec. Neurorehabilitation
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.1095180
This article is part of the Research TopicJob Integration/Reintegration of People with Neuromuscular Disorders in the Epoch of “Industry 4.0”View all 5 articles
 Teresa Paolucci1
Teresa Paolucci1 Alessandro de Sire2*†
Alessandro de Sire2*† Francesco Agostini3,4
Francesco Agostini3,4 Andrea Bernetti3
Andrea Bernetti3 Angela Salomè3
Angela Salomè3 Marta Altieri5
Marta Altieri5 Vittorio Di Piero5
Vittorio Di Piero5 Antonio Ammendolia2
Antonio Ammendolia2 Massimiliano Mangone3
Massimiliano Mangone3 Marco Paoloni3
Marco Paoloni3Introduction: The aim of this randomized controlled trial was to evaluate the effect of an embodied rehabilitative protocol, in improving interoceptive awareness respect balance and motor performance in patients with mild multiple sclerosis (pwMS).
Methods: In this study patients with relapsing-remitting multiple sclerosis were enrolled. The rehabilitative treatment group (TG) participated in an embodied physiotherapy program consisting of 8 one-hour sessions in groups of 4 patients at a time, 1 per week and 2 one-hour sessions of neuro-cognitive exercise in single session during the rehabilitation program. All pwMS underwent a clinical assessment to measure the interoception sense for the Multidimensional Assessment of Interoceptive Awareness scale, balance for the Tinetti Mobility test and stabilometry, quality of life for the Short Form Health Survey-12 and body image perception for Trunk Appearance Perception Scale and Body Image Scale. All previous scales and tests were performed at baseline (T0), at the end of treatment (T1) and after 2 months of follow up (T2).
Results: Sixty patients were enrolled and randomized into two groups: TG (n = 30), aged 43.0 ± 10.2 years, and a control/waiting list (WLG) group (n = 30), aged 40.7 ± 10.4 years. Statistically significant improvements in interoceptive awareness, body image perception, balance and quality of life were reported in TG versus WLG (p < 0.05).
Discussion: This study suggests that enhancing interoceptive awareness could improve postural balance. Future studies with a larger sample of patients will be needed to better quantify the effects of an embodied rehabilitation.
Multiple sclerosis (MS) is a chronic disease of the central nervous system (CNS) that occurs in people of all ages and races often presenting major limitations of mobility and restriction of participation in activities of daily living (ADL) (1). Therefore, an early detection of functional impairment in patients with MS (pwMS) is crucial to monitor the disease progression and to define an early tailored pharmacological and rehabilitative intervention (2). Rehabilitation, including psychotherapy, symptomatic therapy, and physical activities, is the best form of treatment for the symptoms of MS and for improving motor performances, quality of life, etc. (3, 4). Furthermore, given the dysfunction in the adaptive compensatory mechanisms along the course of disease, rehabilitation is generally more effective in earlier phases of MS (5). Conventional rehabilitation in pwMS patients is based on physical therapies and therapeutic exercise to help the patient develop strategies for dealing with different disabilities interventions aimed at acquiring the maximum possible independence in the Activities of Daily Life (ADL) and return to work (6). The problem of “working with disability” will in pwMS continue to escalate if we do not act (7, 8). In fact, only 37% of those with mild MS are in work. Often, in mild MS, balance, mobility impairments and falls are common problematics, and it can complicate job management and independence (7). Therefore, by proposing early rehabilitation interventions, aimed at improving cognitive and functional skills to strengthen and contain future and more serious balance dysfunctions (reducing the risk of falls and limiting the movement of patients outside the protected environments), it is also possible to effect on autonomy and on returning to work after exacerbations (7, 8). In the early stages of the disease, the dysfunction of postural control, an increased risk of falls, is about 50–80% (1). Body awareness (BA) is an important channel in processing human information for perception and action that interact with balance control: in stroke patients, for example, a good BA was associated with a better postural control (9). MS patients present several alterations of bodily signals (10) and BA (11–15). The exploration of body listening, which we understand as interoceptive awareness, is a little studied topic in MS, especially in the context of rehabilitation. There are various proposals for neurorehabilitation that indirectly have inserted elements of “awareness” of the exercise intended as a neurocognitive task that the patient must solve through the execution of the function, but these aspects have not yet been addressed in patients with MS (6, 16). For example, when MS patients are used somatosensory cues for the perception of body orientation, or motor imagery, the rehabilitator tries to reconstruct a correct movement pattern through a new learning by the patient in pathological conditions, overcoming the discrepancy between perception, action, and posture (6, 17). Also, physiotherapy using MI, with the application of musical and verbal guides, can produce benefits on gait, fatigue and quality of life in pwMS with a low score in the Expanded Disability Status Scale (18). Also, Berthoz (19) remarked, in The Brain's Sense of Movement, the bridge between the interoception of perception and action as the mechanisms that maintain balance and coordinate the movement. On these premises, this study set out to assess the effect of an embodied rehabilitation treatment, that includes training exercises based on the principles of neurocognitive rehabilitation and specifically favoring, as far as possible, the interception and awareness during movement and respecting the principle to learn in pathological conditions (20). The term of embodied was used to define the novelty of the exercise proposal, where the physiotherapist always brought the patient's attention back to listening to the body and awareness of the movement, starting from the important relationship that exists between interoceptive awareness (IA), the sense of body, posture, and action. Therefore, by the present randomized controlled trial (RCT) we aimed to assess the efficacy of an embodied rehabilitation treatment in terms of interoceptive awareness, balance and motor performance in MS patients.
The protocol of this RCT was created in accordance with the Standard Protocol Items of the Consort Statement (21), registered at clinicaltrials.gov (NCT03711968) and approved by Ethic Committee of the Umberto I University Hospital in Rome (no. 5125).
Patients with the relapsing-remitting form of MS (MS-RR) diagnosed according to McDonald's diagnostic criteria (22) were voluntarily recruited from September to November 2018 and evaluated by a senior neurologist at Umberto I University Hospital in Rome and referred for a physiatrist consultation at the Rehabilitation Outpatient Clinic. Patients were consecutively enrolled and matched pairs randomized into two groups, according to a computer-generated simple randomization list with a 1:1 (block size 4) allocation ratio (software MATLAB R2007b®, The Matworks Inc., USA): an embodied rehabilitation treatment group (TG) and a waiting list group (WL = no rehabilitation treatment, patients were free to make exercise at home as global strengthening exercise and walking activity as usual). To respect allocation, black envelopes were used. All participants signed a written informed consent after receiving detailed information about the aim and procedures of the study, which was conducted in accordance with the Declaration of Helsinki (2013). For ethical reasons, to guarantee all patients access to rehabilitation treatment, at the end of the data collection, the WL patients started their rehabilitation program, and their results are independent of this research. Inclusion criteria were: age between 18 and 60 years, clinically definite MS-RR diagnosis, based on the well-established McDonald criteria (23), Expanded Disability Status Scale (EDSS) (24) score of between 0 and 2.5, body mass index (BMI) <30, Mini-Mental State Examination score ≥24 (25). Patients with relapses within the previous 30 days and with a history of psychiatric disorders, such as schizophrenia, bipolar I or II disorder, or substance-abuse disorders, were excluded, as were those with tumors, rheumatological or diabetic conditions, previous surgery on the spine, presence of a pacemaker, cardiovascular disease, or other neurological disorders. Further exclusion criteria were pregnancy and other ongoing rehabilitation treatments. Patients were on a stable FDA-approved disease-modifying therapy regimen for at least 6 months according to the indications of the reference neurologist.
The rehabilitation treatment was carried out in groups of five patients, for the first eight sessions, and two single sessions of neurocognitive rehabilitation by two physiotherapists experienced in neurocognitive rehabilitation and by the referring physiatrist (26). The rehabilitation program, aiming to potentiate interoceptive awareness and sensitivity, was based on the following items: (i) posture, (ii) proprioception, (iii) self-body image, (iv) diaphragmatic breathing, (v) relaxation of the body (self-perception), (vi) motor skills, (vii) coordination, (viii) visuo-spatial coordination, and (ix) balance. The program was composed of 8 one-hour sessions of group physical therapy (1 per week) and 2 one-hour sessions of single neurocognitive exercises (1 per month). Each physical therapy session consisted of: postural exercises to increase perception of the body in space, proprioceptive exercises to allow patients to explore and know their own self, visuo-spatial activities to enhance visuo-spatial orientation, coordination and strengthening training to improve balance and strengthen muscles, motor exercises to stimulate memory and coordination, and sporting activities combining fun, motivation and education. To enhance interoceptive awareness (the target of the entire program), the patients initially performed each exercise with EO and then with EC (Table 1). Each exercise session was repeated 8 to 10 times, for two repetitions in the 1st month, and subsequently, for three repetitions in the 2nd month. During the rehabilitation sessions the physiotherapist guided the patient through the voice and the “touch” when and where necessary. At the end of the session performed with the physiotherapist, the patient was instructed to repeat the same exercises at home. At the end of each session, patients performed breathing and relaxation exercises. Neurocognitive exercises were based on the same target following the principles of the Perfetti method (27). The patients worked on proprioception of the upper and lower limbs, short-term memory, spatial perception and orientation and the physiotherapist tested their problem-solving attitude. During the 2 months of rehabilitation treatment the physiotherapist taught the patients how to perform, safely, the same exercises at home for at least two more times a week; moreover, specific cognitive exercises were given designed to train their memory and attention (see Figure 1 for further details). The proposed rehabilitation protocol was designed to help patients improve and focus on interoceptive awareness: posture, body image and body self-awareness, proprioception, visuo-spatial coordination, balance, motor schema, diaphragmatic breathing and relaxation of the body (self-perception). When the exercises were proposed in EC, the patient tried to first imagine the movement, then to make it aware in the body and then, to listen to his/her own body during the execution of the movement itself. Likewise, in the exercises with OE the patient could observe his own movement in the mirror and was always invited to report his own sensations with respect to his/her body in action.
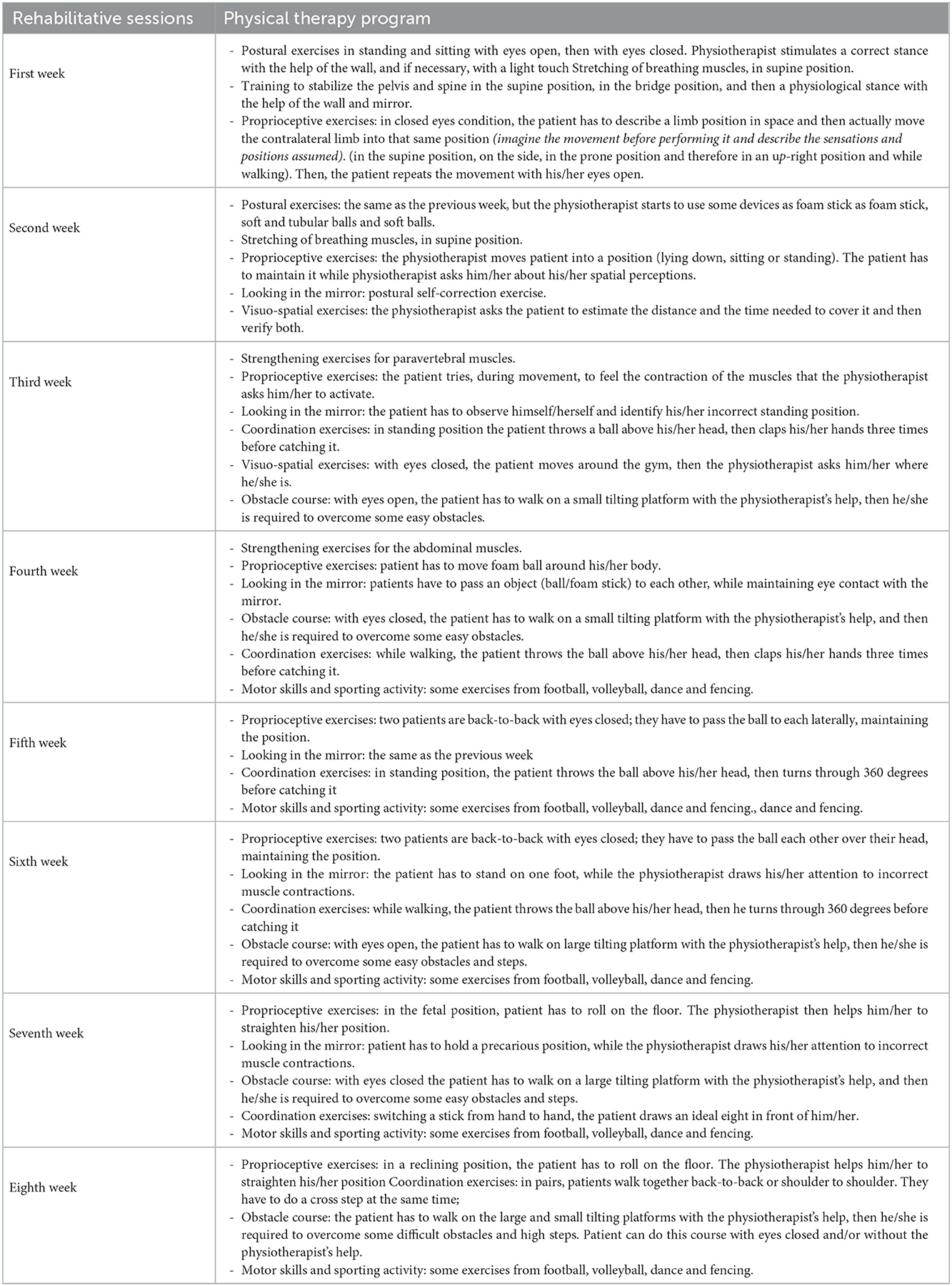
Table 1. Rehabilitation plan.
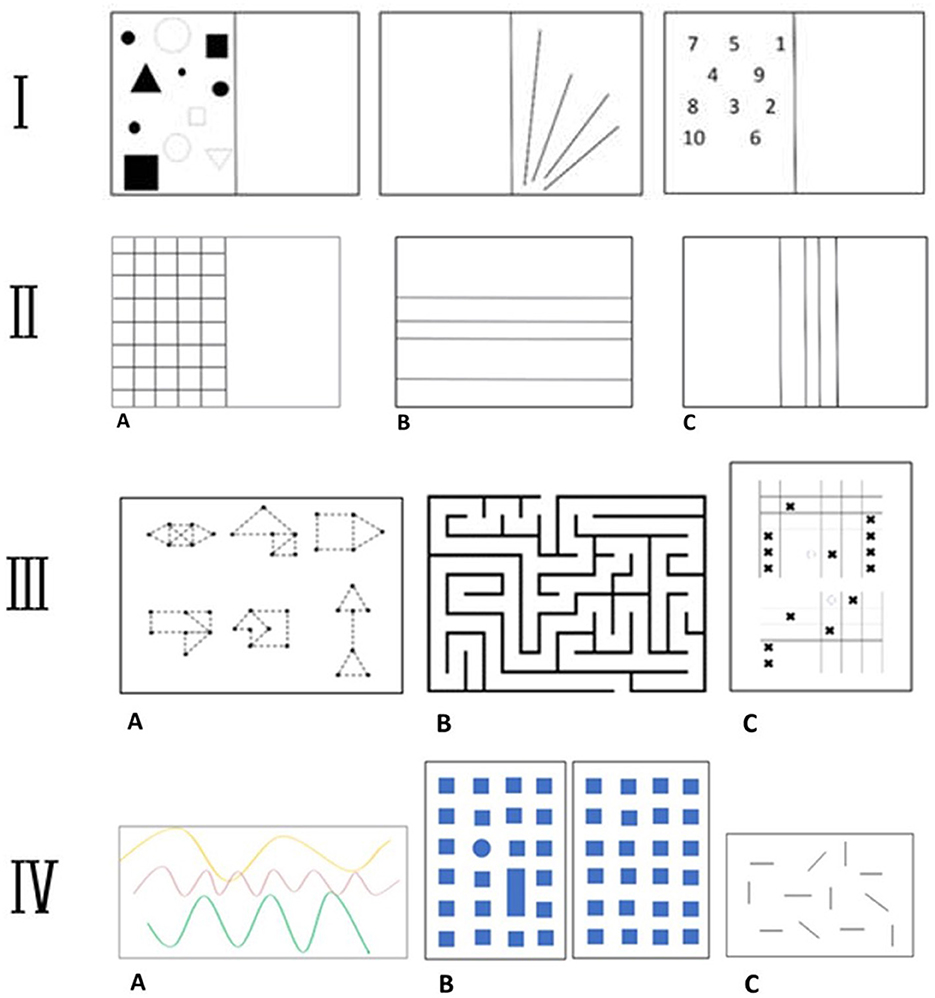
Figure 1. Rehabilitation protocol. (I) Cognitive exercise. The physiotherapist gives the patient time to study the image's shapes/lines/numbers (position, size, etc.), before covering up the completed half of the page and asking him/her to draw one or more elements in the same position (short-term memory). (II) Cognitive exercise. (A) The physiotherapist gives the patient a few minutes to study the image; then, with his/her eyes closed, the patient has to put his/her finger in a requested position (upper limb proprioception). (B, C) The patient has to study the distance between the lines. The physiotherapist will then ask him to draw new lines in specific positions (spatial perception). (III) Problem-solving test. (A) The patient has to join the dots, without going through any of them twice. (B) A labyrinth. (C) Patient plays against physiotherapist, seeking to the completion of the line with the same symbol. (IV) Cognitive exercise. (A) The physiotherapist shows the patient three paths painted on the floor. They walk along each of them together paying attention to bends and changes of direction. Then physiotherapist then guides the patient, with eyes closed, along one of the paths and he/she should recognize which it is (motor skills). (B) The physiotherapist shows the patient a path on the map. The patient then replicates that path (short-term memory and spatial orientation). (C) The Barrage Test (visuo-spatial perception).
To minimize bias and maximize the reproducibility of the present RCT, the outcome measures were assessed by physicians unaware of the intervention or control conditions (i.e., by treatment-blinded assessors). Outcome assessments were performed in each group at baseline (T0, before rehabilitative treatment), at the end of 2 months of treatment (T1) consisting of 8 weekly sessions conducted in small groups of five patients, plus two individual sessions (one per month), and after 2 months of follow-up (T2); each treatment session lasted an hour. Primary outcome was the Multidimensional Assessment of Interoceptive Awareness (MAIA) is a scale developed to investigate the different dimensions of IA (28). Among other things, it explores the ability to identify inner sensations and to discern subtle bodily cues indicating varying functional states of the body and the individual's emotional/physiological state. The MAIA scale consists of 32 items divided into eight subscales: Noticing, Not Distracting, Not Worrying, Attention Regulation, Emotional Awareness, Self -Regulation, Body Listening, Trusting. Individual subscale scores range from 5 (a greater degree of awareness) to 0 (a lesser degree of awareness). The maximum total score, indicating the highest degree of self-awareness, is 40 (28).
Secondary clinical outcomes were Tinetti Mobility Test, 12-Item Short Form Health Survey (SF-12), Trunk Appearance Perception Scale (TAPS), and Body Image Scale (BIS). The Tinetti Mobility Test is a recommended instrument for assessing mobility, balance, gait, and fall risk in the elderly. It is composed of a balance subscale (9 items, 16 points) and a gait subscale (8 items, 12 points) (29, 30). The SF-12 (Short Form Health Survey), which derives from the longer the SF-36, measures quality of life through 12 items. Each of its subscales is transformed into a score from 0 to 100, with lower scores indicating increased disability: the Physical and Mental Health Composite Scores (respectively, PCS and MCS) are calculated by specific software. The PCS is calculated by combining the physical functioning, role-physical, bodily pain, and general health scores. The MCS is calculated by a combining the vitality, social functioning, role-emotional, and mental health scores (31). The Trunk Appearance Perception Scale (TAPS) is a validated instrument for testing patient perceived trunk posture. The scale includes three sets of trunk drawings: from the back, from the front and in forward bending position (32). The Body Image Scale (BIS) is a 10-item questionnaire designed to briefly assess body dimension images in cancer patients. It uses a 4-point response scale (ranging from 0 = not at all to 3 = very much) and the final score is the sum of the 10 item scores, and thus ranges from 0 to 30. A score of zero represents no symptoms or distress and higher scores correspond to increasing symptoms and distress or greater body image concerns (33).
A stabilometric platform was used to collect and analyze (Milletrix software ©) data on Center of pressure (CoP) oscillation, sway area, length and velocity, both with eyes closed (EC) and with eyes open (EO). The stabilometry test was performed during quiet standing in both conditions (EC and EO) for 51.2 s. After receiving information about the test procedure, the TG and WL patients were instructed to stand erect, but not to attention, with their arms lying along the trunk, their feet at an angle of approximately 30 degrees open toward the front, and their heels aligned in the medio-lateral direction. All tests were performed by the same examiner; thus, the participants were supplied with the same instructions prior to each test. Three tests were conducted for each trial condition (EO and EC), and we report the average scores. In the EO condition, subjects fixated on a mark on a wall 1.5 m away at eye level. The order of trial conditions, EO-EC or EC-EO, was randomized. In order to obtain simulation of self-correction postures, we asked patients to “please stand straight” when performing the test. To minimize external disturbances, the environment was brightly lit naturally and quiet (34). Stabilometry evaluation performed at each time (T0, T1, T2).
The sample size was evaluated by considering the item of the MAIA scale: Trusting. We used one-tailed student t-tests for dependent samples considering: a power of 95%; α equal to 0.05; we used the following values for item trusting 2.17 ± 1.07 and 3.03 ± 0.97 (35). With these parameters, the required sample is 17 subjects per group. The sample was calculated using the G * Power Version 3.1.9.2 software. Respect, statistical analyses, the intention-to-treat principle was not considered because the dropout rate was <20% (36). Means and standard deviation values were calculated for all evaluated variables. Related-samples Friedman's two-way analysis of variance by rank test was carried out to assess the scale scores changes in each group over the three timepoints. The Mann-Whitney U test was used to compare scale scores between the two groups at each assessment timepoint. At baseline, we performed unpaired t-test to compare the two groups of subjects for age and BMI, we used a Chi-square test (χ2) to compare them for gender. All data analysis was performed using IBM SPSS Statistic version 24 software. The p-value threshold of significance was set at 0.05 for all tests. The sample size was not calculated, considering this pilot study with respect to the primary outcome considered (MAIA-scale). We also calculated the variations over time (Delta-Δ) for all scales and compared these between the two groups to consider the group-time interaction of these scales. We did a full statistical analysis for the MAIA scale score. We performed a 2-way mixed ANOVA test with a between subject factor (group) and a within factor (time).
Sixty-three (N = 63) patients were enrolled and randomized into two groups: one submitted to embodied rehabilitation treatment (TG, N = 31) and the other comprising patients allocated to the waiting list (WL, N = 32). During the two months of rehabilitation treatment, three patients dropped out: two WL patients and one TG patient. Therefore, we analyzed data of 60 patients (42 F, 18 M), 30 undergoing (70% female) the rehabilitation treatment and 30 (70% female) on the waiting list (the study flow diagram is depicted by Figure 2). The two groups were matched for age, gender, BMI and age at diagnosis (years) (see Table 2 for further details). Only one patient had exacerbations of MS symptoms during the rehabilitation intervention. No adverse events occurred during the course of the study.
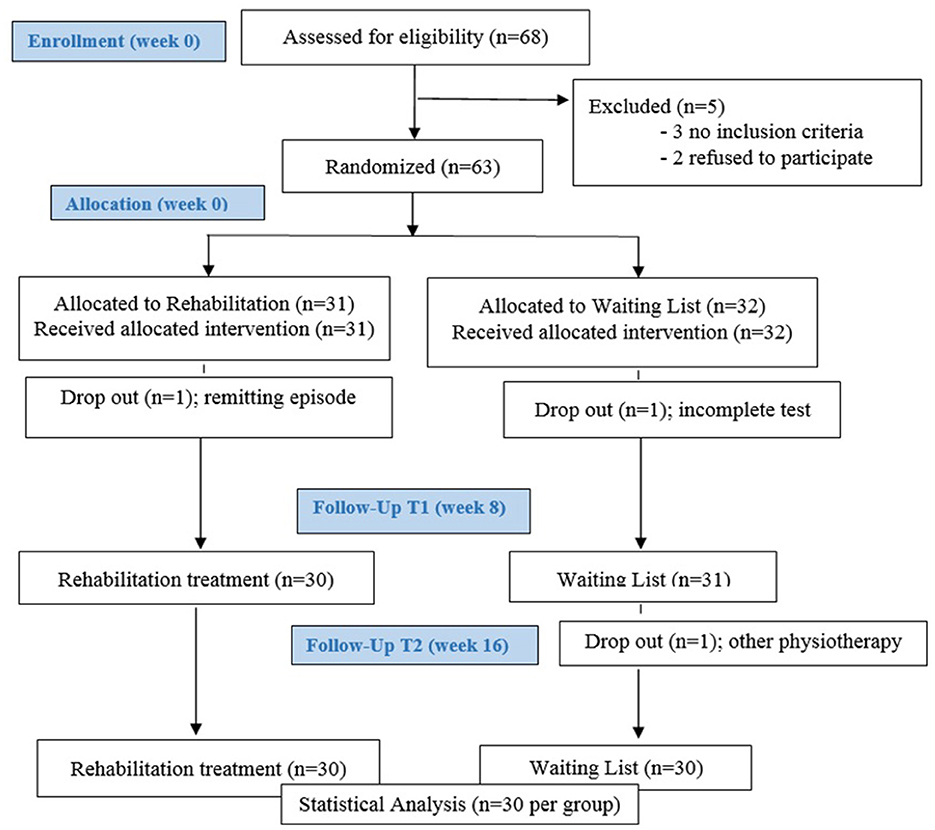
Figure 2. Flow chart.
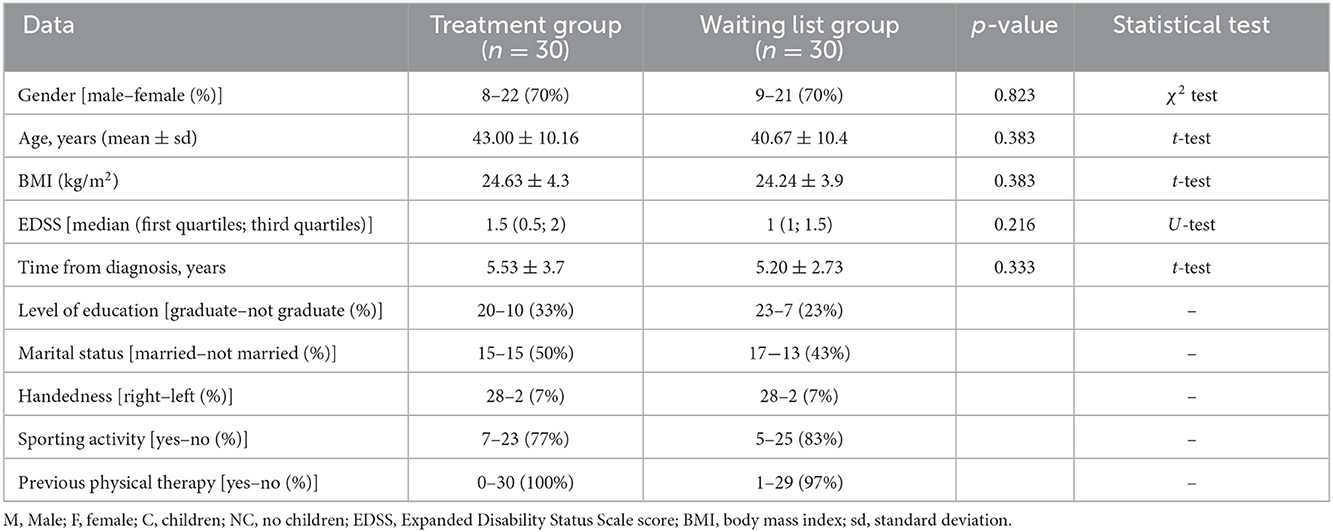
Table 2. Sample characteristics.
The TG showed statistically significant improvements (p = 0.0038) in the MAIA scale total score (MAIA tot): T0 = 21.5 (5.162), T1 = 25.01 (4.902), T2 = 24.05 (4.135) and in five MAIA sub-scales: Noticing (p = 0.01), Not Worrying (p < 0.001), Emotional Awareness (p < 0.001), Self -Regulation (p = 0.001) and Body Listening (p < 0.001), while in the WL group, there was only a worsening on the Not Distracting item (p = 0.002) (Tables 3, 4). Table 5 shows the post hoc analysis.
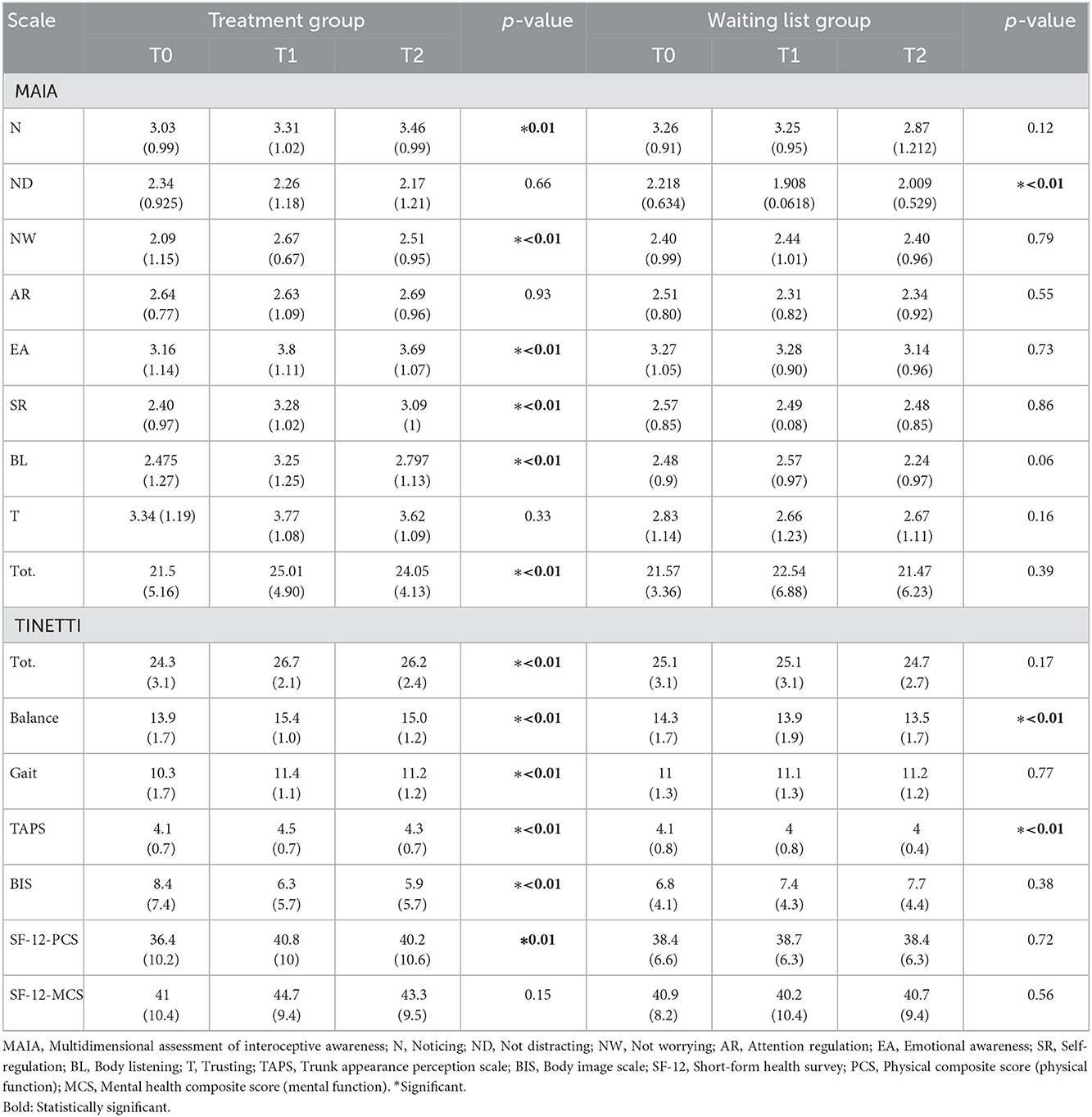
Table 3. Mean values, standard deviations and p-values of clinical scale scores at three timepoints in the two groups.
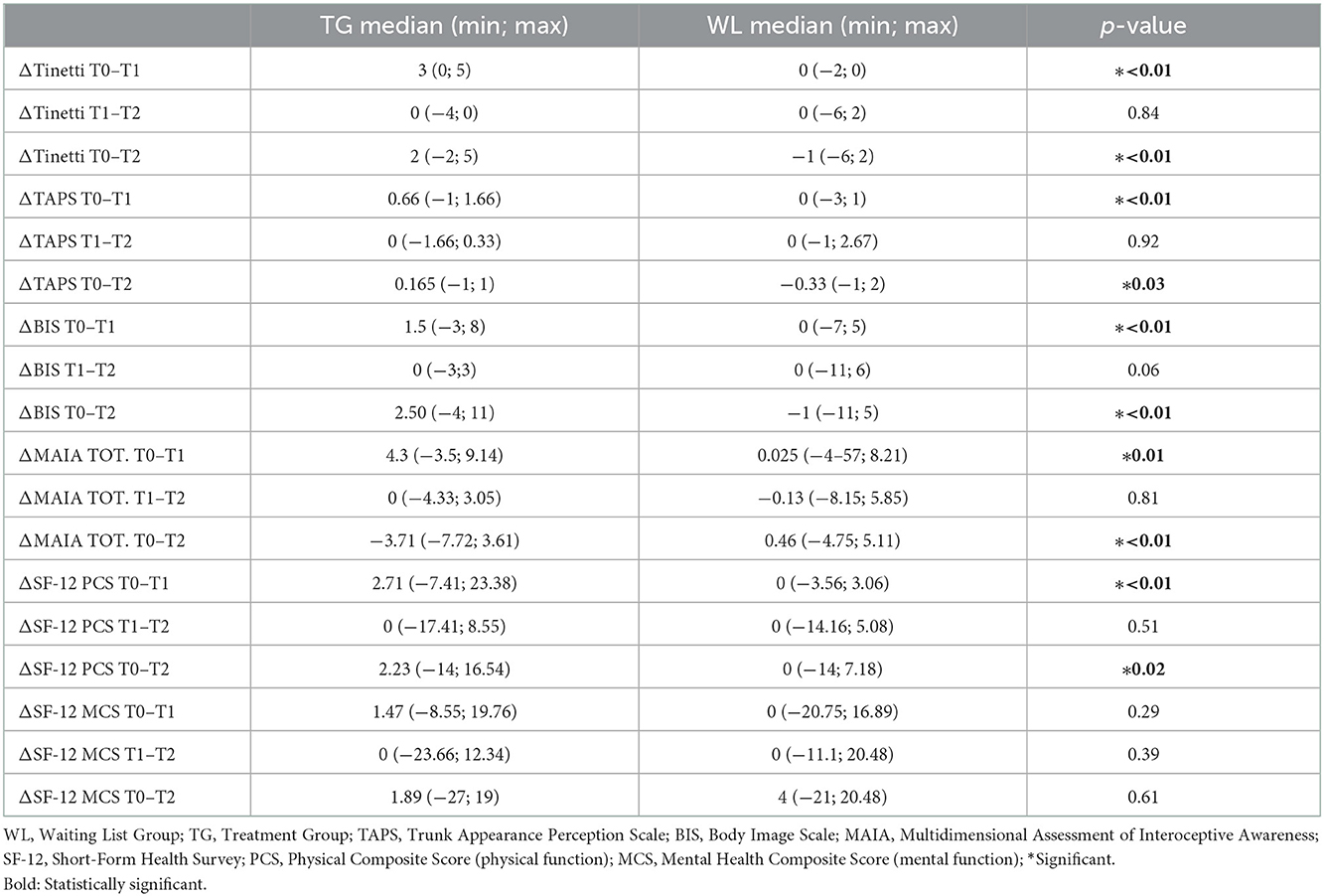
Table 4. The variations over time (Delta-Δ) for all scales.

Table 5. Simple main effect analysis for group for MAIA scale.
Mauchly's test of sphericity indicated that the assumption of sphericity was violated for the two-way interaction, χ2 = 6.37, p = 0.041. There was a statistically significant interaction between the intervention and time on MAIA scale score, F = 10.02, p < 0.001, partial η2 = 0.147 (Figure 3).

Figure 3. Interaction between the intervention and time on MAIA scale score.
We tested for the simple main effects for group that means testing differences in MAIA scale score groups at each category of the within subjects' factor, time (Table 5).
There was a statistically significant effect of time on MAIA scale score in the TG (p < 0.01) (Table 6).

Table 6. Simple main effect for time for MAIA scale.
The Tinetti scale (total score) results showed a statistically significant improvement in the TG patients after rehabilitation treatment and this was preserved at the follow-up, too: T0 = 24.3 (3.17), T1 = 26.7 (2.1), T2 = 26.23 (2.4) (p < 0.001). In the WL group, we observed a worsening of Tinetti balance items over the follow-ups: T0 = 14.3 (1.7), T1 = 13.9 (1.9), T2 = 13.5 (1.7) (p < 0.001) (Tables 3, 4).
Statistically significant improvements in the TAPS and BIS scores were observed in the TG: TAPS – T0 = 4.1 (0.7), T1 = 4.5 (0.7), T2 = 4.3 (0.7) (p < 0.001); BIS–T0 = 8.4 (7.4), T1 = 6.3 (5.7), T2 = 5.9 (5.7) (p < 0.001); instead, the WL group showed a worsening in TAPS scores at T2 and follow-up (Tables 3, 4).
Statistically significant improvements (p = 0.0170) in SF-12 physical function scores were recorded at T1 and T2 in the TG: T0 = 36.4 (10.2), T1 = 40.8 (10) and T2 40.2 (10.6) (see Tables 3, 4).
In the TG, considering the CoP parameters, we found a reduction of the sway area in the neutral posture with EO after rehabilitation (p = 0.01175). In the same group in the neutral posture with EC, we noted a reduction of the sway area (p = 0.0396), an increase of the ball length (p = 0.00964) and of average velocity (p = 0.00025). Furthermore, in these patients we observed an increase in average velocity (p = 0.0470) in the self-correction posture with EO, but a decrease of the sway area (p = 0.00065) and an increase in average velocity (p = 0.01003) in the self-correction posture with EC (Table 7). In the WL, considering the CoP parameters, we observed a statistically significant increase in average velocity (p < 0.001) in the self-correction posture with EO (Table 7).
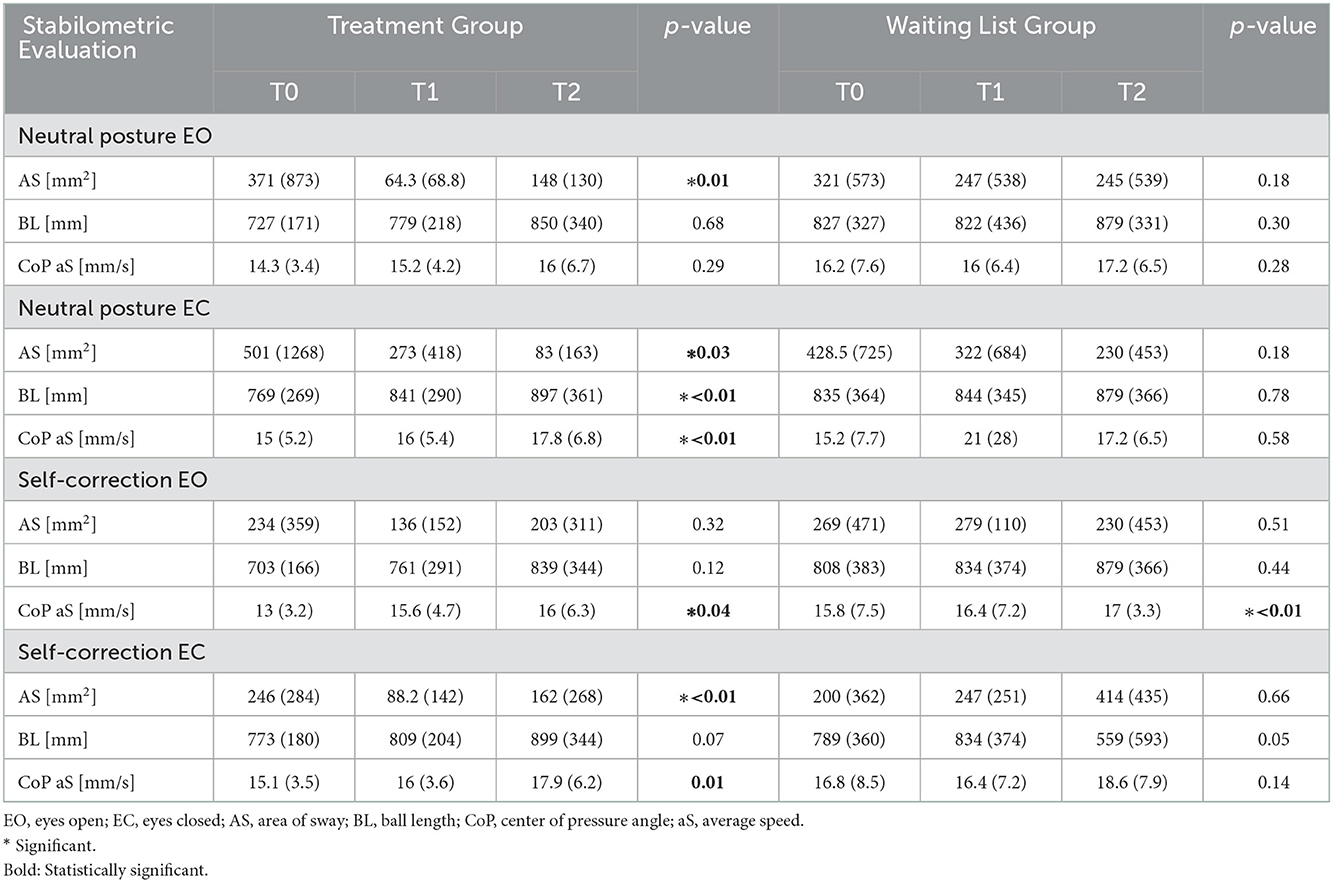
Table 7. Mean values, standard deviation and p-values of postural parameters measured during the stabilometric platform test at three timepoints in the two groups.
In the TG we identified statistically significant values with regard to the primary outcome (MAIA scores): total score (T1 p = 0.0141; T2 p = 0.0345), Emotional Awareness (T1 p = 0.0462; T2 p = 0.0214), Self-Regulation (T1 p = 0.0030; T2 p = 0.0168), Body Listening (T1 p = 0.0298; T2 p = 0.0684).A statistically significant differences in the Tinetti total score (T1 p = 0.0072; T2 p = 0.0074), Tinetti balance scale (T1 p = 0.0007; T2 p = 0.0003) and TAPS scores (T1 p = 0.0015; T2 p = 0.0302) were reported. The BIS scores also differed significantly between the groups at follow-up (T2 p = 0.0228). We did not find any statistically significant difference in the SF-12 scores. Regarding postural assessment and stabilometry, we found statistically significant changes in the sway area value in self-correction posture with EO (T1 p = 0.0736; T2 p = 0.0203) and in path length with EO and EC (T2 p = 0.0130).
Our study set out to evaluate the effect of an embodied rehabilitation treatment in mild MS. This treatment was designed to improve interoceptive awareness and enhance balance and motor skills in the early stages of the disease, with a limited and mild disability, in patients who had never yet undergone a rehabilitation process. It is termed embodied because it comprises exercises intended to increase body awareness and, specifically, interoceptive awareness.
In pwMS, the functional reduction represents one of the most disabling aspects since it limits the patient's functionality in ADL, not allowing a complete and timely return to work, fundamental to an individual's social self-determination (6). This loss of autonomy and social self-definition, due to the impossibility in the return to work, lead the patient to completely abandon work activities, as feeling no longer able to do it, and to isolate themselves socially (6). Therefore, by virtue of such a complex pathology and with extremely varied symptoms, all aspects of disability must be investigated and addressed.
In our study, the TG showed improvements on several MAIA subscales, namely Not Worrying, Emotional Awareness, Self-Regulation and Body Listening, both after treatment and at follow-up; these improvements were not observed in the WL group. According to the results, exercises, both with EO and with EC, could be helpful in making patients focus on their own body awareness. The embodied rehabilitation treatment, based on kinesthetic, proprioceptive, and tactile stimuli, could be a new strategy for helping patients to learn about their own bodies. In fact, during each session, the patients focused on their perception of their own body both in neutral posture and during movements, also helped by physiotherapist's voice and touch because some exercises were performed in the EC condition and, in each neurocognitive session, patients performed cognitive training to enhance attention, memory and orientation. Other research studies (37–39) have provided novel evidence about the effectiveness, in the rehabilitation protocol, of training involving specific, graded discrimination tasks with attentive exploration of stimuli with vision occluded, deliberate anticipation and quantitative feedback. Moreover, in pwMS, exercises while walking could improve learning, memory, and hippocampal properties (40) and structured physical activity programs may contribute to cognitive function stability or improvement, while physical activity can enhance balance and gait (41). The results suggested as the embodied rehabilitation program can improve balance, as shown by the Tinetti scale results and interoception as shown by the MAIA scale results. In accordance with Zamariola et al. (42), we observed improved interoception awareness together with TAPS and BIS. Moreover, perception of our own body, feelings, posture, and mental attitude relates to interoception and body image: all of these elements form our own personal identity and contribute to our general well-being (43, 44). Moreover, in self-correction posture with EO, the stabilometric test data showed an increase of CoP velocity and a decrease of sway area, while there was an increase in CoP velocity and a statistically significant reduction in sway area in the same posture with EC. Sway area reduction corresponds to good postural stability maintenance with low energy expenditure, while CoP velocity increase is an effective and quick strategy for constantly seeking center of gravity equilibrium. In neutral posture with EO and with EC, the data showed sway area reduction, but in the EC condition there were also increases in CoP velocity and path length. In summary, better posture control could be achieved through improved interoceptive awareness; sway area reduction was found to be a key result in EC/EO neutral/self-correction postural control in our TG. Postural control relies on the integration of inputs from the visual, somatosensory and vestibular systems, which are frequently impaired in patients with MS and an increase in sway area is an indicator of poor walking and balance capabilities in MS. Therefore, it could be hypothesized that the patient's sense of his own body in space, in static and in dynamic conditions, can represent an additional sense for postural control, particularly considering the virtual reality rehabilitation programs (45, 46). Posturography is considered the gold standard objective measure of standing postural control in pwMS, even in early-stage disease: sway area, length, oscillation, and trajectories are key parameters and appropriate outcomes capable of indicating disability deterioration in MS. Future studies specifically focusing on postural self-correction mechanisms and postural balance would be desirable. This study is not free from limitations. Firstly, the relatively short-period intervention (i.e., 2 months) and short follow-up observation period, thus not examining the sustainability and durability of the intervention over time. We included patients with an EDSS score between 0 and 2.5 (no or minimal / mild disability in one or two functional systems). Also, there is a lack of comparison with other kinds of exercise or mindfulness treatments. Lastly, patients included in the study did not undergo the same drug therapy. These limitations will be addressed in future studies, with more patients' details, using the same drug therapy, and longer follow-up, to increase the scientific literature on this subject. A desirable goal in future studies, to deepen the results that have been observed, will be to use the ICF model as a reference also as outcomes.
Taken together, the findings of this double-blind RCT showed that an embodied rehabilitation treatment was effective in terms of enhancing interoceptive awareness and finding a balance between body and mind. Our results are encouraging in favoring modalities of proposals for rehabilitation exercise that focus attention on the awareness of the body in motion, using strategies that make the exercise itself a moment of learning and stimulation, including attention and memory strategies in MS. Also, MS is frequently affecting adults of working age, resulting in a range of physical, cognitive and psychosocial deficits that impact on workforce participation, then it is important to take care of the patient from the early stages of the disease, ensuring a rapid return to work especially after the flare-up phases of the disease. Specific future studies focusing on postural self-correction mechanisms, postural balance in MS patients in order to improve their independence and work capacity despite MS-related disability.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The work has been approved by the Ethical Committee of the Umberto I University Hospital in Rome (no. 5125) and followed ethical guidelines for experimentation with human subjects in accordance with the 1964 Declaration of Helsinki. The patients/participants provided their written informed consent to participate in this study.
Conceptualization: TP and MP. Methodology: TP and ASi. Investigation: FA, AB, and ASa. Formal analysis: FA, AB, and MM. Data curation: TP, FA, and MM. Writing—original draft preparation: TP, ASi, and FA. Writing—review and editing: AA, MM, and MP. Visualization: AB, ASa, MA, and VD. Supervision: TP, ASi, and MP. All authors read and approved the final version of the manuscript.
This study has been supported by Italian Ministry of Health (Ricerca Corrente).
We would like to thank Chiara La Russa, Silvia Sbardella, and Pino Maggi.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kidd T, Carey N, Mold F, Westwood S, Miklaucich M, Konstantara E, et al. A systematic review of the effectiveness of self-management interventions in people with multiple sclerosis at improving depression, anxiety and quality of life. PLoS ONE. (2017) 12:e0185931. doi: 10.1371/journal.pone.0185931
2. Solaro C, de Sire A, Messmer Uccelli M, Mueller M, Bergamaschi R, Gasperini C, et al. Efficacy of levetiracetam on upper limb movement in multiple sclerosis patients with cerebellar signs: a multicenter double-blind, placebo-controlled, crossover study. Eur J Neurol. (2020) 27:2209–16. doi: 10.1111/ene.14403
3. de Sire A, Bigoni M, Priano L, Baudo S, Solaro C, Mauro A. Constraint-Induced Movement Therapy in multiple sclerosis: Safety and three-dimensional kinematic analysis of upper limb activity. A randomized single-blind pilot study. NeuroRehabil. (2019) 45:247–54. doi: 10.3233/NRE-192762
4. Coulter EH, Bond S, Dalgas U, Paul L. The effectiveness of interventions targeting physical activity and/or sedentary behaviour in people with Multiple Sclerosis: a systematic review. Disabil Rehabil. (2020) 42:594–612. doi: 10.1080/09638288.2018.1503737
5. Wens I, Dalgas U, Vandenabeele F, Grevendonk L, Verboven K, Hansen D, et al. High intensity exercise in multiple sclerosis: effects on muscle contractile characteristics and exercise capacity, a randomised controlled trial. PLoS ONE. (2015) 10:e0133697. doi: 10.1371/journal.pone.0133697
6. Paolucci T, Bernetti A, Sbardella S, La Russa C, Murgia M, Salomè A, et al. Straighten your back! Self-correction posture and postural balance in “non rehabilitative instructed” multiple sclerosis patients. NeuroRehabil. (2020) 46:333–41. doi: 10.3233/NRE-192987
7. Cancelliere C, Donovan J, Stochkendahl MJ, Biscardi M, Ammendolia C, Myburgh C, et al. Factors affecting return to work after injury or illness: best evidence synthesis of systematic reviews. Chiropr Man Therap. (2016) 24:32. doi: 10.1186/s12998-016-0113-z
8. Cardone A. Having the conversation about work with people with multiple sclerosis: a guide for healthcare professionals. Neurodegener Dis Manag. (2017) 7:41–4. doi: 10.2217/nmt-2017-0041
9. Ahn SN. Differences in body awareness and its effects on balance function and independence in activities of daily living for stroke. J Phys Ther Sci. (2018) 30:1386–9. doi: 10.1589/jpts.30.1386
10. Salamone PC, Esteves S, Sinay VJ, García-Cordero I, Abrevaya S, Couto B, et al. Altered neural signatures of interoception in multiple sclerosis. Hum Brain Mapp. (2018) 39:4743–54. doi: 10.1002/hbm.24319
11. Craig AD. How do you feel–now? The anterior insula and human awareness. Nat Rev Neurosci. (2009) 10:59–70. doi: 10.1038/nrn2555
12. Garfinkel SN, Seth AK, Barrett AB, Suzuki K, Critchley HD. Knowing your own heart: distinguishing interoceptive accuracy from interoceptive awareness. Biol Psychol. (2015) 104:65–74. doi: 10.1016/j.biopsycho.2014.11.004
13. Brener J, Ring C. Towards a psychophysics of interoceptive processes: the measurement of heartbeat detection. Philos Trans R Soc Lond B Biol Sci Nov. (2016) 19:371. doi: 10.1098/rstb.2016.0015
14. Owens AP, Allen M, Ondobaka S, Friston KJ. Interoceptive inference: From computational neuroscience to clinic. Neurosci Biobehav Rev. (2018) 90:174–83. doi: 10.1016/j.neubiorev.2018.04.017
15. Hanken K, Francis Y, Kastrup A, Eling P, Klein J, Hildebrandt H, et al. On the role of the amygdala for experiencing fatigue in patients with multiple sclerosis. Mult Scler Relat Disord. (2018) 20:67–72. doi: 10.1016/j.msard.2017.12.014
16. Marotta N, de Sire A, Marinaro C, Moggio L, Inzitari MT, Russo I, et al. Efficacy of Transcranial Direct Current Stimulation (tDCS) on balance and gait in multiple sclerosis patients: a machine learning approach. J Clin Med. (2022) 11:3505. doi: 10.3390/jcm11123505
17. Hanson M, Concialdi M. Motor imagery in multiple sclerosis: exploring applications in therapeutic treatment. J Neurophysiol. (2019) 121:347–9. doi: 10.1152/jn.00291.2018
18. Gil-Bermejo-Bernardez-Zerpa A, Moral-Munoz JA, Lucena-Anton D, Luque-Moreno C. Effectiveness of motor imagery on motor recovery in patients with multiple sclerosis: systematic review. Int J Environ Res Public Health. (2021) 18:498. doi: 10.3390/ijerph18020498
20. Raimo S, Boccia M, Di Vita A, Iona T, Cropano M, Ammendolia A, et al. Interoceptive awareness in focal brain-damaged patients. Neurol Sci. (2020) 41:1627–31. doi: 10.1007/s10072-019-04172-z
21. Schulz KF, Altman DG, Moher D, CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomized trials. BMC Med. (2010) 8:18. doi: 10.1186/1741-7015-8-18
22. Kamińska J, Koper OM, Piechal K, Kemona H. Multiple sclerosis—etiology and diagnostic potential. Postepy Hig Med Dosw (Online). (2017) 71:551–63. doi: 10.5604/01.3001.0010.3836
23. McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP, Lublin FD, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann Neurol. (2001) 50:121–7. doi: 10.1002/ana.1032
24. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. (1983) 33:1444–52. doi: 10.1212/WNL.33.11.1444
25. Crum RM, Anthony JC, Bassett SS, Folstein MF. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA. (1993) 269:2386–91. doi: 10.1001/jama.1993.03500180078038
26. Basso MR, Beason-Hazen S, Lynn J, Rammohan K, Bornstein RA. Screening for cognitive dysfunction in multiple sclerosis. Arch Neurol. (1996) 53:980–4. doi: 10.1001/archneur.1996.00550100046014
27. Morreale M, Marchione P, Pili A, Lauta A, Castiglia SF, Spallone A, et al. Early versus delayed rehabilitation treatment in hemiplegic patients with ischemic stroke: proprioceptive or cognitive approach? Eur J Phys Rehabil Med. (2016) 52:81–9.
28. Mehling WE, Price C, Daubenmier JJ, Acree M, Bartmess E, Stewart A, et al. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE. (2012) 7:e48230. doi: 10.1371/journal.pone.0048230
29. Tinetti ME, Williams TF, Mayewski R. Fall risk index for elderly patients based on number of chronic disabilities. Am J Med. (1986) 80:429–34. doi: 10.1016/0002-9343(86)90717-5
30. Capone F, Capone G, Motolese F, Voci A, Caminiti ML, Musumeci G, et al. Spinal cord dysfunction contributes to balance impairment in multiple sclerosis patients. Clin Neurol Neurosurg. (2019) 184:105451. doi: 10.1016/j.clineuro.2019.105451
31. Jenkinson C, Layte R, Jenkinson D, Lawrence K, Petersen S, Paice C, et al. A shorter form health survey: can the SF-12 replicate results from the SF-36 in longitudinal studies? J Public Health Med. (1997) 19:179–86. doi: 10.1093/oxfordjournals.pubmed.a024606
32. Matamalas A, D'Agata E, Sanchez-Raya J, Bago J. Trunk appearance perception scale for physicians (TAPS-Phy)—a valid and reliable tool to rate trunk deformity in idiopathic scoliosis. Scoliosis Spinal Disord. (2016) 11:24. doi: 10.1186/s13013-016-0085-8
33. Cheli S, Agostini A, Herd-Smith A, Caligiani L, Martella F, Fioretto L, et al. The Italian version of body image scale—reliability and sensitivity in a sample of breast cancer patients. Psicoterapia Cognitiva e Comportamentale. (2016) 22:65–79.
34. Scoppa F, Capra R, Gallamini M, Shiffer R. Clinical stabilometry standardization: basic definitions–acquisition interval—sampling frequency. Gait Posture. (2013) 37:290–2. doi: 10.1016/j.gaitpost.2012.07.009
35. Eggart M, Todd J, Valdés-Stauber J. Validation of the Multidimensional Assessment of Interoceptive Awareness (MAIA-2) questionnaire in hospitalized patients with major depressive disorder. PLoS ONE. (2021) 16:e0253913. doi: 10.1371/journal.pone.0253913
36. Streiner DL. Missing data and the trouble with LOCF. Evid Based Ment Health. (2008) 11:3–5. doi: 10.1136/ebmh.11.1.3-a
37. Shumway-Cook A, Woollacott M. Motor learning and recovery of function. In: Motor Control Translating Research into Clinical Practice, 4th edition (Philadelphia, PA: Lippincott Williams & Wilkin). (2012).
38. Mhizha-Murira JR, Drummond A, Klein OA, dasNair R. Reporting interventions in trials evaluating cognitive rehabilitation in people with multiple sclerosis: a systematic review. Clin Rehabil. (2018) 32:243–54. doi: 10.1177/0269215517722583
39. Bernetti A, Agostini F, de Sire A, Mangone M, Tognolo L, Di Cesare A, et al. Neuropathic pain and rehabilitation: a systematic review of international guidelines. Diagnostics (Basel). (2021) 11:74. doi: 10.3390/diagnostics11010074
40. Sandroff BM, Johnson CL, Motl RW. Exercise training effects on memory and hippocampal viscoelasticity in multiple sclerosis: a novel application of magnetic resonance elastography. Neuroradiology. (2017) 59:61–7. doi: 10.1007/s00234-016-1767-x
41. Morrison JD, Mayer L. Physical activity and cognitive function in adults with multiple sclerosis: an integrative review. Disabil Rehabil. (2017) 39:1909–20. doi: 10.1080/09638288.2016.1213900
42. Zamariola G, Cardini F, Mian E, Serino A, Tsakiris M. Can you feel the body that you see? On the relationship between interoceptive accuracy and body image. Body Image. (2017) 20:130–6. doi: 10.1016/j.bodyim.2017.01.005
43. Paolucci T, Zangrando F, Iosa M, De Angelis S, Marzoli C, Piccinini G, et al. Improved interoceptive awareness in chronic low back pain: a comparison of Back school versus Feldenkrais method. Disabil Rehabil. (2017) 39:994–1001. doi: 10.1080/09638288.2016.1175035
44. Badoud D, Tsakiris M. From the body's viscera to the body's image: Is there a link between interoception and body image concerns? Neurosci Biobehav Rev. (2017) 77:237–46. doi: 10.1016/j.neubiorev.2017.03.017
45. Mangone M, Paoloni M, Procopio S, Venditto T, Zucchi B, Santilli V, et al. Sagittal spinal alignment in patients with ankylosing spondylitis by rasterstereographic back shape analysis: an observational retrospective study. Eur J Phys Rehabil Med. (2020) 56:191–6. doi: 10.23736/S1973-9087.20.05993-6
Keywords: balance, exercise, interoceptive awareness, neurocognitive, posture, rehabilitation
Citation: Paolucci T, de Sire A, Agostini F, Bernetti A, Salomè A, Altieri M, Di Piero V, Ammendolia A, Mangone M and Paoloni M (2022) Efficacy of interoceptive and embodied rehabilitative training protocol in patients with mild multiple sclerosis: A randomized controlled trial. Front. Neurol. 13:1095180. doi: 10.3389/fneur.2022.1095180
Received: 10 November 2022; Accepted: 02 December 2022;
Published: 21 December 2022.
Edited by:
Alberto Ranavolo, National Institute for Insurance Against Accidents at Work (INAIL), ItalyReviewed by:
Tiwana Varrecchia, National Institute for Insurance Against Accidents at Work (INAIL), ItalyCopyright © 2022 Paolucci, de Sire, Agostini, Bernetti, Salomè, Altieri, Di Piero, Ammendolia, Mangone and Paoloni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessandro de Sire,  YWxlc3NhbmRyby5kZXNpcmVAdW5pY3ouaXQ=
YWxlc3NhbmRyby5kZXNpcmVAdW5pY3ouaXQ=
†ORCID: Alessandro de Sire orcid.org/0000-0002-5541-8346
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.