
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Neurol. , 16 December 2022
Sec. Neuro-Oncology and Neurosurgical Oncology
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.1086591
This article is part of the Research Topic Case Reports in Neuro-Oncology and Neurosurgical Oncology : 2022 View all 32 articles
 Ahmet Kursat Karaman1*†
Ahmet Kursat Karaman1*† Bora Korkmazer2
Bora Korkmazer2 Nil Urganci3Gülçin Baş4Serdar Arslan2Nil Comunoglu3Mehmet Murat Hanci4Osman Kızılkılıç2
Nil Urganci3Gülçin Baş4Serdar Arslan2Nil Comunoglu3Mehmet Murat Hanci4Osman Kızılkılıç2Background: Symptomatic spinal metastases of oligodendroglioma are rare. Moreover, none of the previously published cases demonstrated the typical IDH mutation and 1p/19q-codeletion for this glial tumor. This case presents an IDH mutant, 1p/19q-codeleted oligodendroglioma with multiple spinal drop metastases.
Case description: We report a case of a 55-year-old woman with left frontal grade 3 oligodendroglioma diagnosed 3 years ago. No tumor recurrence was observed in post-operative follow-up MRI examinations. However, she was admitted to our institution again with severe low back pain. Gadolinium enhanced MRI of the spine revealed an intradural, extramedullary metastatic lesion between T11–L1 levels and multiple enhancing metastatic tumor deposits around cauda equine roots between L4–S1. T11–T12 midline laminectomy was performed and gross total resection of metastatic lesions was achieved. Final histological diagnosis of the spinal lesions was WHO Grade 3 Oligodendroglioma, IDH-mutant, 1p/19q-codeleted.
Conclusion: This case is the first molecularly-defined spinal metastatic oligodendroglioma. The possibility of drop metastasis should be kept in mind in oligodendroglioma patients with spinal cord-related symptoms. There is no standard approach for the diagnosis and treatment of spinal metastases of this type of glial tumor.
Oligodendrogliomas are rare neuroepithelial tumors accounting for 2–5% of all brain tumors in adults (1). In the 5th edition of the WHO classification of CNS tumors, they are defined as diffuse gliomas that demonstrate IDH mutation and 1p/19q-codeletion. The characteristic 1p19q deletion in these tumors is also associated with greater response
to treatment and better clinical outcome (2). Microscopic spread of oligodendrogliomas via CSF to spinal subarachnoid spaces is a well-defined and relatively common event, reported up to 14%. However, clinically significant macroscopic spinal cord metastases are rare. In addition, to the best of our knowledge, 1p19q deletion has not been described in previously reported cases of oligodendroglioma with spinal drop metastasis (3, 4).
In this article, we report a case of IDH-mutant, 1p/19q-codeleted oligodendroglioma presenting with multiple spinal drop metastases 3 years after initial diagnosis.
A 55-year-old woman presented with a headache that had worsened over the past few months in June 2019. MRI of the brain revealed a large heterogeneous mass of 6.5 × 5.5 × 4.2 cm in the left frontal lobe and mild perilesional edema. The mass was compressing the left lateral ventricle and there was hyperintense signal on T1W and T2W images consistent with hemorrhage in its part in this region. No contrast enhancement was observed in the mass on post-contrast MR images (Figure 1). Total re-section of the tumor was performed and histopathological diagnosis was oligodendroglioma, WHO grade 3, IDH-mutant, and 1p/19q-codeleted. The patient was asymptomatic in the postoperative period. Adjuvant treatment (cranial radiotherapy combined with temozolomide) was recommended by oncologists, but she refused. No tumor recurrence was observed in follow-up MRI examinations.
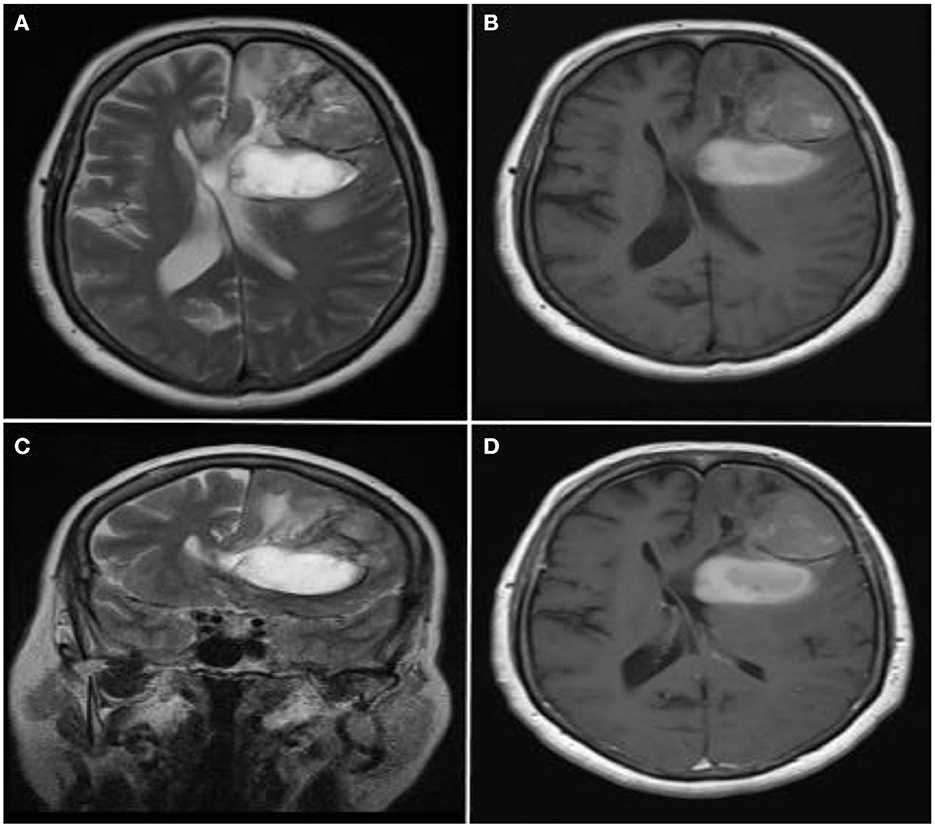
Figure 1. Radiological images of the primary lesion. (A–C) Axial T2-weighted, axial T1-weighted and coronal T2-weighted MR images show a large, heterogeneous, left lateral ventricle compressing mass and mild perilesional edema in the left frontal lobe. Hemorrhagic appearance is observed in the posterior-inferior part of the mass (hyperintense signal on T1-weighted and T2-weighted images). (D) There was no enhancement in the mass on the Gd-enhanced T1-weighted MR image.
However, in July 2022 (36 months after initial diagnosis), the patient was admitted to our institution with a 3-week history of severe low back pain. Neurological examination demonstrated mild paraparesis. No sensory deficit was found and deep tendon reflexes were normal. Gadolinium enhanced MRI of the spine revealed an intradural extramedullary lesion compressing the spinal cord between T11–L1 levels and multiple enhancing tumor deposits attached to cauda equina roots between L4–S1 levels (Figures 2A–F). There was no evidence of metastases outside the central nervous system. T11–T12 midline laminectomy was performed to decompress the spinal cord and obtain histological samples. A gray-hemorrhagic, soft tumoral extra medullary lesion was observed following the opening of the dura. Also, tumoral nodules surrounding the cauda equina roots were observed. Subtotal resection of all visible tumor was achieved. Early postoperative course was uneventful. Spinal radiotherapy was planned for residual tumor between T11–L1 levels and tumor deposits between L4–S1 levels.
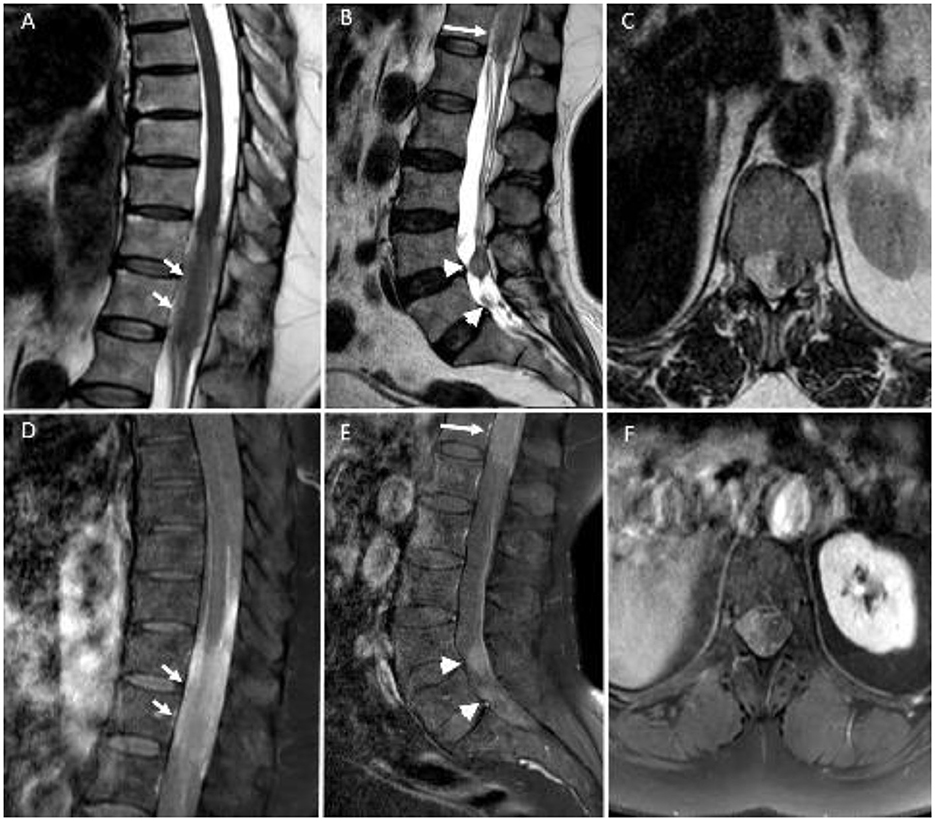
Figure 2. Sagittal T2-weighted (A,B) and post-contrast T1-weighted (D,E) MR images demonstrate multiple metastatic lesions with contrast enhancement between T11–L1 levels (long arrows) and around cauda equina roots (arrowheads). Axial T2-weighted (C) and post-contrast T1-weighted (F) images at T12 level show an extramedullary metastatic lesion compressing the spinal cord.
Histopathological examination revealed that the tumor consisted of small-medium cells with small, rounded nuclei, perinuclear clearing, and the presence of increased cellularity, pleomorphism, brisk mitosis and focal necrosis. Vascular endothelial proliferation was absent (Figure 3A). Immunohistochemical staining showed positive results for GFAP, EMA, Olig2 and mutant IDH-1 (Figures 3B,C). Immunohistochemistry for ATRX showed retained wild-type expression (Figure 3D). Ki-67 proliferation index was 30%. Fluorescence in situ hybridization studies revealed 1p/19q co-deletion (1p/1q ratio 85%, 19q/19p ratio 65%) in tumor cells (Figures 3E,F). Final histological diagnosis was WHO Grade 3 Oligodendroglioma, IDH-mutant, 1p/19q-codeleted.
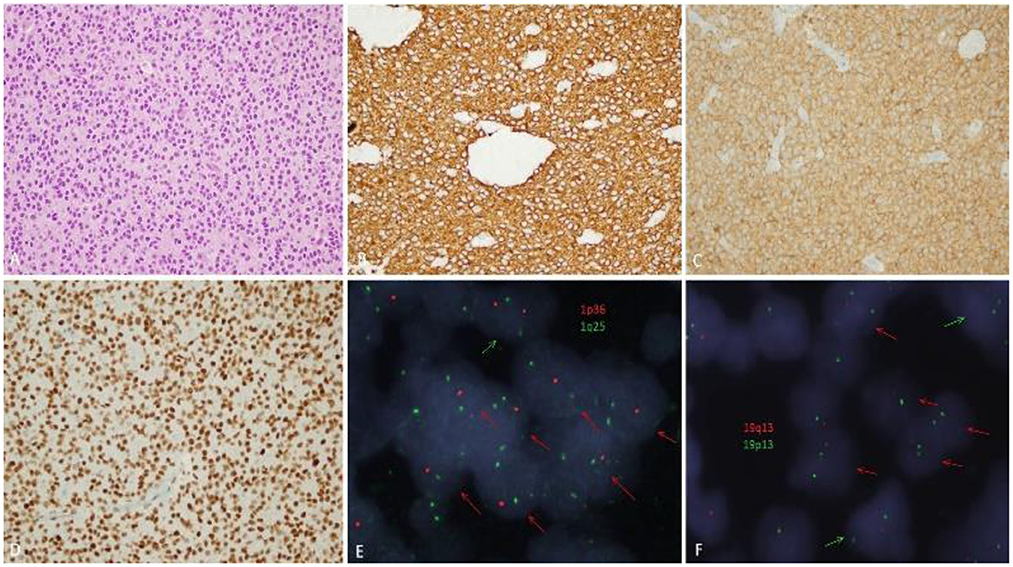
Figure 3. Pathological findings. (A) Microscopic examination (H & E, ×400) showed small-medium sized tumor cells with round nuclei and perinuclear haloes. (B) GFAP was diffusely positive in tumor cells. (C) Immunohistochemistry for IDH-1 R132H was positive (mutant). (D) ATRX immunohistochemistry showed retained wild-type expression. (E,F) 1p19q-codeletion in oligodendroglioma via fluorescence in situ hybridization. (E) 1p deletion of oligodendroglioma tumor cell nuclei (two green signals for 1q25, one red signal for 1p36). (F) 19q deletion of oligodendroglioma tumor cell nuclei (two green signals for 19p13 and one red signal for 19q13). Red arrows showed cells with deletion, and green arrows showed cells without deletion.
Oligodendrogliomas are the rarest type of primary brain tumor associated with distant metastases. In these tumors, the most frequent metastatic sites are bone, bone marrow and lymph nodes (5, 6). The occurrence of spinal drop metastases is exceptional, and according to our extensive literature search, there are 18 previously described cases with confirmed pathological diagnosis in the literature. However, none of the reported cases were evaluated for 1p/19q code-deletion or IDH mutation status as defined in the WHO 2021 CNS tumor classification (Table 1) (4, 7–20). Thus, the present case, with IDH mutation and 1p/19q deletion, is the first 'true' (molecularly proven) spinal drop metastasis of oligodendroglioma.

Table 1. Summary of previously reported oligodendroglioma cases with spinal drop metastasis.
Most spinal metastases from oligodendroglioma are extramedullary. However, intramedullary localization was observed in 5 of 18 reported cases (4, 13, 16, 19, 20). In addition, drop metastases may be diffuse, filling the entire spinal canal, or may be one or more tumor deposits involving a relatively short spinal segment (4). In our case, as in most of the previously described cases, extramedullary metastases were described and multiple tumoral lesions were detected between T11–L1 levels and around cauda equina fibers.
The primary advocated mechanism for metastasis to meningeal surfaces along the spinal cord is the transition of tumor cells to the cerebrospinal fluid (CSF) by disrupting the pia and ependyma, and then their seeding by following the normal CSF pathway with the help of gravitational forces. Previous cranial surgery and/or CSF shunting may be the initiating factor for this mechanism. Disruption of the integrity of the meningeal barriers secondary to surgical intervention may cause subarachnoid spread. Moreover, disruption of the blood-brain barrier integrity may facilitate hematogenous extracranial metastasis (21, 22). Except for the case reported by Natale et al. (4, 17), all cases in the published literature had a history of previous brain tumor surgery and spinal metastases occurred in the early or late period (3 months−7 years) after surgery. Spinal drop metastases were detected 36 months after primary tumor surgery in our case. Besides, spread along the Virchow-Robin spaces of the spinal cord is advocated for intramedullary metastases (17).
Tumor-related intrinsic factors that may play a role in subarachnoid metastasis of glial tumors are the malignant potential and location of the tumor. In general, most of the glial tumors that metastasize to the spinal cord are high-grade diffuse gliomas, as in our case (23). For oligodendrogliomas, however, the situation appears different; In half (9/18) of oligodendroglioma cases with spinal metastases, the primary tumor is low grade (WHO grade II) (4). In addition, the 1p/19q-codeletion in these tumors is not correlated with metastatic relapse. The contribution of this molecular alteration, typical for the diagnosis of oligodendroglioma, to distant metastatic potential is explained by its association with prolonged survival. As the patient's survival increases, the probability of tumor progression and distant metastasis increases (24). In our case, spinal metastasis occurred 3 years after the primary tumor diagnosis. As mentioned above, since the spread via CSF is the main pathway in spinal metastasis of oligodendroglioma, intraventricular location of the lesion or contact with the subarachnoid space may be a remarkable factor (4, 18). In 18% (3/18) of reported cases, the lesion location is intraventricular (7, 12, 17). Moreover, close proximity to the pericerebral subarachnoid area/ventricle was observed in most of the cases (17, 18). In our case, the primary lesion was located close to both the pericerebral subarachnoid space and the ventricle.
Since spinal drop metastasis of oligodendrogliomas is a rare entity, routine imaging of the entire neuraxis is not recommended in asymptomatic cases. In patients with spinal symptoms, imaging of the entire CNS with MRI seems reasonable (18, 22). Management of spinal metastases should be done in a case-based fashion. Surgery can be used for decompression, especially in cases without diffuse involvement. On the other hand, spinal radiotherapy can be performed in cases who are not suitable for surgical intervention (18, 19). In general, the presence of spinal metastases associated with intracranial oligodendrogliomas is considered as a poor prognostic factor. However, there is scarce data regarding the long-term follow-up results in the literature. In addition, the prognostic effect of this condition is controversial, as there is no spinal metastatic 'true' oligodendroglioma with the 1p/19q-codeletion (4, 15, 17).
Spinal drop metastasis of oligodendroglioma is not common. The fact that previously reported cases were not evaluated for the typical 1p/19q-codeletion and IDH mutation for this tumor in the current WHO classification suggests that the primary lesion may be other diffuse glial tumors in some of these cases. Therefore, the exact frequency of spinal metastatic oligodendrogliomas and their relationship with clinical outcome are unknown. Furthermore, there is no standard approach for the diagnosis and treatment of spinal metastases.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Conception and design: AK, BK, and OK. Data acquisition: SA, NU, and GB. Analysis and interpretation of data: BK, NU, and GB. Article drafting: AK and BK. Study supervision: OK, MH, and NC. Approved the final version of the manuscript on behalf of all authors: AK. Reviewed submitted version of the manuscript and critical revision of the article: all authors. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Koeller KK, Rushing EJ. From the archives of the AFIP: oligodendroglioma and its variants: radiologic-pathologic correlation. Radiographics. (2005) 25:1669–88. doi: 10.1148/rg.256055137
2. Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol. (2021) 23:1231–51. doi: 10.1093/neuonc/noab106
3. Engelhard HH. Current diagnosis and treatment of oligodendroglioma. Neurosurg Focus. (2002) 12:1–7. doi: 10.3171/foc.2002.12.2.3
4. Elefante A, Peca C, Del Basso De Caro ML, Russo C, Formicola F, Mariniello G, et al. Symptomatic spinal cord metastasis from cerebral oligodendroglioma. Neurol Sci. (2012) 33:609–13. doi: 10.1007/s10072-011-0769-z
5. Li G, Zhang Z, Zhang J, Jin T, Liang H, Gong L, et al. Occipital anaplastic oligodendroglioma with multiple organ metastases after a short clinical course: a case report and literature review. Diagn Pathol. (2014) 9:17. doi: 10.1186/1746-1596-9-17
6. Han SR, Yoon SW, Yee GT, Choi CY, Lee DJ, Sohn MJ, et al. Extraneural metastases of anaplastic oligodendroglioma. J Clin Neurosci. (2008) 15:946–9. doi: 10.1016/j.jocn.2006.09.013
7. Beck DJK, Russell DS. Oligodendrogliomatosis of cerebrospinal pathways. Brain. (1942) 65:352–72. doi: 10.1093/brain/65.4.352
8. Trowbridge WV, French JD. Disseminated oligodendroglioma. J Neurosurg. (1952) 9:643–8. doi: 10.3171/jns.1952.9.6.0643
9. Strang RR, Nordenstam H. Intracerebral oligodendroglioma with metastatic involvement of the cauda equina. J Neurosurg. (1961) 18:683–7. doi: 10.3171/jns.1961.18.5.0683
10. Reggiani R, Solimé F, Eugenio del Vivo R, Nizzoli V. Intracerebral oligodendroglioma with metastatic involvement of the spinal cord: case report. J Neurosurg. (1971) 35:610–3. doi: 10.3171/jns.1971.35.5.0610
11. Voldby B. Disseminated, mucin-producing oligodendroglioma. Acta Neurochir. (1974) 30:299–307. doi: 10.1007/BF01405586
12. Arseni C, Horvath L, Carp N, Constantinescu A, Ciurea V. Spinal dissemination following operation on cerebral oligodendroglioma. Acta Neurochir. (1977) 37:125–37. doi: 10.1007/BF01401931
13. Van Velthoven V, Calliauw L, Caemaert J. Intramedullary spread of a cerebral oligodendroglioma. Surg Neurol. (1988) 30:476–81. doi: 10.1016/0090-3019(88)90035-3
14. Wallner KE, Gonzales M, Sheline GE. Treatment of oligodendrogliomas with or without postoperative irradiation. J Neurosurg. (1988) 68:684–8. doi: 10.3171/jns.1988.68.5.0684
15. Ng HK, Sun DT, Poon WS. Anaplastic oligodendroglioma with drop metastasis to the spinal cord. Clin Neurol Neurosurg. (2002) 104:383–6. doi: 10.1016/S0303-8467(02)00011-2
16. Mcbryde CW, Hamid NA, Mitchell RD. Anaplastic oligodendroglioma with metastasis to the spinal cord. Br J Neurosurg. (2003) 17:364–6. doi: 10.1080/02688690310001601298
17. Natale M, Spennato P, Savarese L, Bocchetti A, Esposito S, Barbato R. Anaplastic oligodendroglioma presenting with drop metastases in the cauda equina. Clin Neurol Neurosurg. (2005) 107:417–20. doi: 10.1016/j.clineuro.2004.09.013
18. Ozişik PA, Işikay I, Oruçkaptan H, Söylemezoglu F, Ozcan OE. Unusual massive spinal metastasis of an intracranial oligodendroglioma. Turk Neurosurg. (2008) 18:276–80.
19. Oshiro S, Komatsu F, Tsugu H, Nabeshima K, Abe H, Ohkawa M, et al. A case of intramedullary cervical metastasis from cerebellar anaplastic oligodendroglioma without typical MR appearance for CSF dissemination. No Shinkei Geka. (2010) 38:279–85.
20. Maiguel Carrizosa CE, Sanchez Paez MG, Martinez Amado A, Gonzalez Gutierrez A, Garcia Ardila ME. Spinal metastases of two different grade oligodendrogliomas: a case report and review of literature. J Spine Surg. (2017) 3:468–74. doi: 10.21037/jss.2017.06.14
21. Hoffman HJ, Duffner PK. Extraneural metastases of central nervous system tumors. Cancer. (1985) 56:1778–82. doi: 10.1002/1097-0142(19851001)56:7+<1778::aid-cncr2820561309>3.0.co;2-i
22. Carlsen JG, Tietze A, Lassen YA, Rosendal F. Paraplegia due to drop metastases from anaplastic oligodendroglioma. Br J Neurosurg. (2012) 26:94–5. doi: 10.3109/02688697.2011.578767
23. Liwnicz BH, Rubinstein LJ. The pathways of extraneural spread in metastasizing gliomas: a report of three cases and critical review of the literature. Hum Pathol. (1979) 10:453–67. doi: 10.1016/S0046-8177(79)80051-9
Keywords: oligodendroglioma, IDH1 (R132H) mutation, drop metastases, spinal metastasis, 1p/19q-codeletion
Citation: Karaman AK, Korkmazer B, Urganci N, Baş G, Arslan S, Comunoglu N, Hanci MM and Kızılkılıç O (2022) Case report: Spinal drop metastasis of IDH-mutant, 1p/19q-codeleted oligodendroglioma. Front. Neurol. 13:1086591. doi: 10.3389/fneur.2022.1086591
Received: 01 November 2022; Accepted: 01 December 2022;
Published: 16 December 2022.
Edited by:
Luigi Rigante, KBM Neurosurgery, GermanyReviewed by:
Salvatore Massimiliano Cardali, University of Messina, ItalyCopyright © 2022 Karaman, Korkmazer, Urganci, Baş, Arslan, Comunoglu, Hanci and Kızılkılıç. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ahmet Kursat Karaman,  a3Vyc2F0LmthcmFtYW5AaXN0YW5idWwuZWR1LnRy
a3Vyc2F0LmthcmFtYW5AaXN0YW5idWwuZWR1LnRy
†ORCID: Ahmet Kursat Karaman orcid.org/0000-0002-4870-0597
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.