
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 28 November 2022
Sec. Neurological Biomarkers
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.1014102
This article is part of the Research Topic Biomarkers of Non-Motor Symptoms in Parkinson’s Disease and Parkinsonisms View all 5 articles
 Dora Valent*
Dora Valent* Marina Peball
Marina Peball Florian KrismerAnna LanbachSophie ZemannCorinne Horlings
Florian KrismerAnna LanbachSophie ZemannCorinne Horlings Werner Poewe
Werner Poewe Klaus Seppi
Klaus SeppiIntroduction: Sarcopenia and Parkinson's disease are closely related diseases of the elderly population leading to progressive disability and nursing-dependent care.
Objective: The aim of this study was to estimate the prevalence of sarcopenia in PD patients with three different approaches: (1) the screening tool SARC-F, (2) EWGSOP-1 criteria, and (3) EWGSOP-2 criteria. Moreover, we aimed to evaluate the diagnostic accuracy of the screening tool SARC-F to detect sarcopenia according to the updated EWGSOP-2 criteria.
Methods: Eighty-one patients with Parkinson's disease aged 65 years and above were interviewed in a cross-sectional study at a tertiary referral center. All patients were screened with the SARC-F questionnaire and were evaluated for motor and non-motor symptoms, exercise, quality of life, and frailty. Muscle mass was assessed with bioelectrical impedance analysis, handgrip strength with a dynamometer, and gait speed was assessed with the 8-m walk test. EWGSOP-2 criteria were considered the gold standard to diagnose sarcopenia in our study.
Results: Eighty-one patients were evaluated (mean age: 73.82; SD 5.30). The prevalence of sarcopenia was 28.4% according to the EWGSOP-2 criteria. The concordance between EWGSOP-2 and EWGSOP-1 was poor (weighted kappa of 0.361[95% 0.164–0.557]). The sensitivity of the SARC-F screening test for detecting sarcopenia was 60.9%. The corresponding AUC in the ROC curve analysis showed 0.598 (0.462, 0.734 CI). The item assessing strength was found to have the highest sensitivity (69.6%).
Conclusion: Sarcopenia prevalence in patients with PD in Tirol, Austria is higher with EWGSOP-1 criteria compared to EWGSOP-2 criteria. The sensitivity and specificity of the SARC-F scale to detect sarcopenia in this population are poor.
Sarcopenia is a skeletal muscle disorder manifesting in the progressive loss of muscle mass and strength leading to adverse health outcomes including, fractures and falls, lower quality of life, and mortality (1). Until 2019, pre-sarcopenia was operationalized by the European Working Group for Sarcopenia in Older People (EWGSOP) as decreased muscle mass. Sarcopenia was confirmed upon the addition of either decreased muscle strength or gait speed and a severe sarcopenic stage was fulfilled when all three components were met (i.e., EWGSOP-1 criteria) (2). In 2019, EWGSOP published a new set of criteria (i.e., EWGSOP-2), whereby low muscle strength, instead of muscle mass, was named the new primary indicator of sarcopenia, with low muscle mass confirming the diagnosis. Decreased gait speed renders sarcopenia severe. A systematic review estimated the prevalence to be 1–29% in the general population according to the EWGSOP-1 criteria (3). With EWGSOP-2 criteria, the prevalence decreased, with some studies reporting occurrences ranging from 0.2 to 13.7% (4–9). Agreement between the two criteria has been mostly inconsistent with some studies showing good (5, 10, 11) and most showing poor agreement (6, 8, 12–15). It was also suggested by EWGSOP to use the validated screening scale SARC-F to identify potential patients who might be suffering from sarcopenia (1). Using the SARC-F scale, 6–65% of the general elderly were found to be at risk for sarcopenia (16–23). Despite its ease of use in clinical settings, the validity of the SARC-F has been debated due to its low sensitivity (17, 24).
Sarcopenia and Parkinson's disease (PD) are both age-related disorders that may share a common underlying pathway (25), in at least a subpopulation of both diseases, leading to progressive disability through motor and non-motor symptoms. Elevated neuro-inflammatory mediators (26), reduction in grey matter in specific brain regions (27), reduced motor neuron units in the hand (28, 29), and altered testosterone levels (30) are examples of markers associated with both sarcopenia and PD. Moreover, sarcopenia has been reported to be more prevalent in this patient population which makes this an imminent topic for clinical prevention and research (31). Currently, no study has assessed the prevalence of sarcopenia in PD using the most recent EWGSOP criteria (EWGSOP-2) with the suggested European cut-off points, and the research conducted so far has yielded conflicting results.
The aim of this study was to estimate the proportion of PD patients with sarcopenia according to three different assessment tools, namely the SARC-F questionnaire, EWGSOP-1 criteria, and EWGSOP-2 criteria. Moreover, we sought to determine the sensitivity and specificity of the SARC-F questionnaire in this patient demographic to detect sarcopenia according to the most recent EWGSOP-2 criteria.
This was an observational, cross-sectional study in which patients with PD aged 65 years or older were recruited consecutively from the movement disorders outpatient clinic and neurological wards of the Medical University of Innsbruck between 2018 and 2021. In order to be included, all patients had to be diagnosed with PD according to the Movement Disorders Society clinical diagnostic criteria (32) and sign an informed consent form. The presence of another movement disorder or any contraindications to the bioelectrical impedance analysis (BIA) machine, such as deep brain stimulation and an apomorphine pump, were exclusion criteria.
Sarcopenia was assessed by three different methods: SARC-F, EWGSOP-1, and EWGSOP-2 criteria. Patients were administered the SARC-F, a simple screening questionnaire composed of five items: strength, climbing stairs, assistance with walking, rising from a chair, and falls (33). Each item is scored on a scale from 0 to 2 with a total score of 0–10 points. Because a score of 4 or greater is predictive of sarcopenia, patients with a score of 4 or greater were classified as sarcopenic, while those with a score of <4 were classified as non-sarcopenic. Diagnosis of sarcopenia according to the EWGSOP-1 criteria was the following: low muscle mass to be considered pre-sarcopenic, detection of low muscle strength or low gait speed to confirm sarcopenia, and fulfillment of all three criteria to be considered severely sarcopenic (2). Diagnosis of sarcopenia established by EWGSOP-2 criteria was the following: sarcopenia was probable when low muscle strength was detected, the addition of low muscle mass confirmed sarcopenia and the addition of low gait speed made the diagnosis severe (1). Respective cut-off values are shown in Table 1.
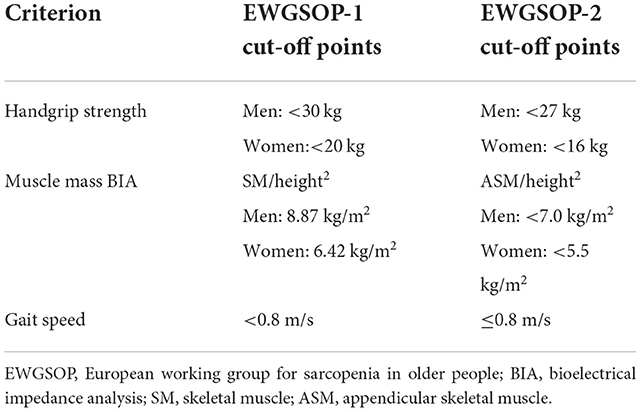
Table 1. EWGSOP-1 and EWGSOP-2 cut-off points for sarcopenia.
Muscle strength was assessed with a calibrated handheld dynamometer (CITEC CT3002). Two trials for each hand were performed and the best result from the strongest hand was used. Muscle mass was measured with the InBody 770 BIA machine at 50 kHz. Appendicular muscle mass was calculated based on the recommended equation developed by Sergi et al. (34). Walking speed, measured in meters/second (m/s), was evaluated by the 8-m gait test, where the participant walked along a straight 8-meter track and the time was measured by a stopwatch.
Demographic information (sex and age), anthropomorphic measurements (weight and height), disease duration, comorbidities (Charlson Comorbidity Index), and quality of life (PD Questionnaire-8) were collected. Disease stage and severity were established with the Hoehn and Yahr scale and the MDS-UPDRS.
The data were analyzed with the aid of the SPSS program version 21 (IBM Corp., Armonk, NY, USA). Data are presented as mean plus or minus standard deviation (SD) for continuous and as a percentage for categorical variables. Prevalence rates are given in percentage with a 95% confidence interval (CI). Score values ranging from 1 to 10 points for the SARC-F test were reported as a dichotomized outcome of the assessment (≥4 as sarcopenic and <4 as non-sarcopenic). Continuous variables were tested for normality using the Kolmogorov–Smirnov test. Parametric data are expressed as mean and standard deviation and compared using Student's t-test. Non-parametric data were tested with the Shapiro–Wilk test and are expressed as mean and standard deviation. We used the area under the receiver operating characteristic (ROC) curve to test the predictive accuracy. Kappa statistic according to Fleiss–Cohen was calculated to ascertain the level of agreement between the classifications of sarcopenia according to the different screening tools.
Demographic data of the cohort including sex differences are shown in Table 2. A total of 81 elderly patients with PD aged 73.8, SD 5.3 (44 men, 37 women) were included in the analyses. The mean duration of the disease was 11.5 ± 7.6 years and 39.5% were in H&Y stage III or above. No significant differences between gender were found regarding demographic and clinical characteristics (p > 0.05), except for in the number of comorbidities (p = 0.003) (Table 2).
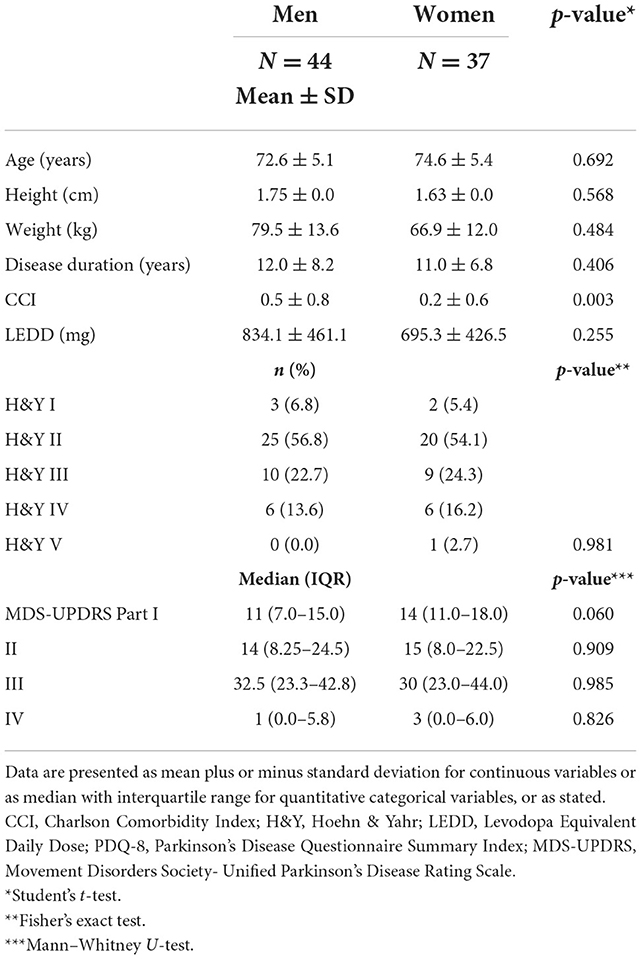
Table 2. Sex differences in demographic and clinical characteristics.
Table 3 compares the prevalence of sarcopenia using SARC-F, EWGSOP-1, and EWGSOP-2 criteria. The prevalence of sarcopenia including severe sarcopenia according to SARC-F was 44.4%, with EWGSOP-1 criteria at 51.9% and with EWGSOP-2 criteria at 28.4%. Agreement between the two EWGSOP criteria was poor (Kappa = 0.361[95% CI 0.164–0.557], data not shown in tables).
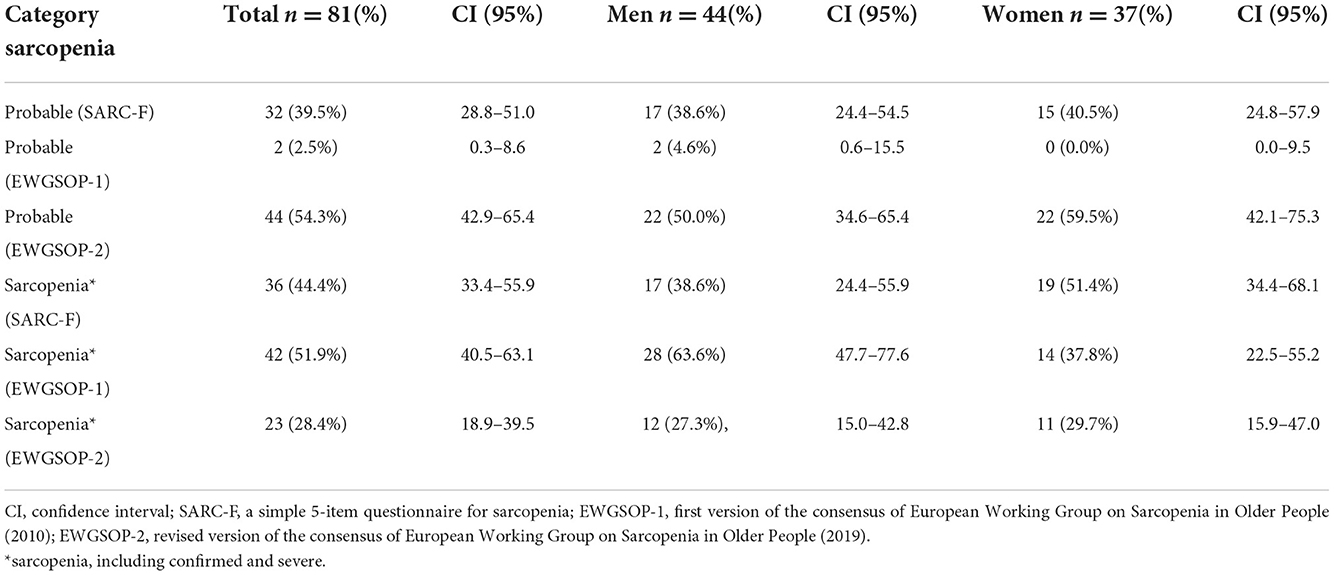
Table 3. Proportion of probable sarcopenia and sarcopenia according to different assessment tools.
The sensitivity of the SARC-F screening test for detecting sarcopenia (as per EWGSOP-2 criteria) was 60.9% (Table 4). The corresponding AUC in the ROC Curve analysis showed 0.598 (0.462, 0.734 CI). The specificity of the test was poor (62.1%) (Table 4). All five items on the questionnaire had similar sensitivities individually (ranging from 56.5 to 69.6%, Table 5) compared to the test as a whole. The specificity of the individual items is all poor, with all values falling below 62.1%. The positive predictive values of all the individual items were under 40%, while the negative predictive values were all above 68%. Thus, a non-sarcopenic person has a probability of under 40% being categorized as at risk for sarcopenia by one of these items (Table 5).
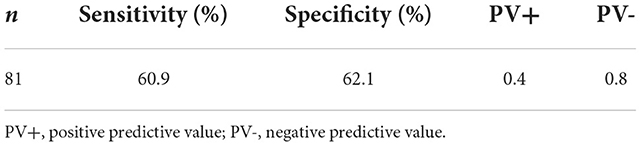
Table 4. Sensitivity and specificity of SARC-F with predictive values according to EWGSOP-2.
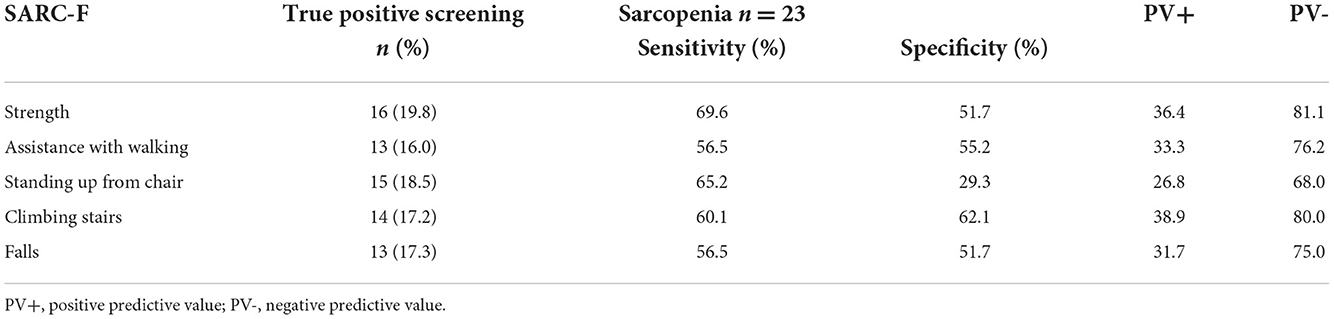
Table 5. Sensitivity of individual SARC-F items according to EWGSOP-2.
Here, we show that the SARC-F screening questionnaire as a whole has poor sensitivity (60.9%) and specificity (62.1%) in the detection of sarcopenia in patients with Parkinson's disease in Tirol, Austria when followed up by an assessment with the most current EWGSOP-2 criteria. Studies assessing PD patients with the EWGSOP-2 criteria are scarce. In their Brazilian PD cohort, Campos Lima da Luz et al. found similar specificity (68.1%) but lower sensitivity (23.1%) (35). Our results show a balance between sensitivity and specificity that is rather indicative of a cut-off value of greater or equal to 2 on the SARC-F questionnaire (36). Although other studies report high specificity in populations without PD, in this patient population, SARC-F does not seem to correctly identify patients who do not have sarcopenia according to the EWGSOP-2 criteria, which means that necessary therapeutic implementations might be allocated to the wrong patients. Studies show that adding a calf measurement to the screening process improves the identification of truly patients with sarcopenia (22, 35, 37, 38). Assessing the individual items on the instrument yielded equally poor sensitivity results, with each item apart for strength, having poor to negligible sensitivity, comparable to previous findings in a PD cohort (35). The highest sensitivity was calculated for the item “strength” at 69.6%. The “falls” item in the questionnaire is especially confounding when it comes to evaluating sarcopenia in patients with PD as recurrent falls are already reported more often by patients with PD compared with age-matched controls (39) and are a sign of advancing PD. Tailoring the questions on the questionnaire to fit a PD patient profile, increasing the cut-off values, or adding a calf circumference measurement to increase accuracy may lead to higher sensitivity or specificity among patients with PD.
To our best knowledge, we are the first study to evaluate the prevalence of sarcopenia among a European population in patients with PD assessed according to the criteria and cut-offs suggested by EWGSOP in 2019. According to EWGSOP-2, 28.4% of participants had confirmed sarcopenia, with men and women having 27.3 and 29.7%, respectively. These results are in line with another study that assessed sarcopenia in Brazilian PD participants (35). The prevalence of sarcopenia based on EWGSOP-1 was 51.9% in total (63.6% in men and 37.8% in women). Other studies have assessed sarcopenia in a PD population according to EWGSOP-1 criteria report numbers between 6 and 55% and varying differences between sex ratios (29, 35, 40–43).
Applying the EWGSOP-2 criteria resulted in a lower prevalence of sarcopenia due to stricter recommended cut-off values for handgrip strength and muscle mass and the adaptation of the operational definition of sarcopenia. When comparing the two criteria, other studies on non-PD populations have also found that the EWGSOP-1 criteria lead to higher prevalence (6, 9, 15, 44). A recent review proposes that the difference in prevalence is about 7% (7). Whether this difference is an overestimation by EWGSOP-1 or an underestimation by EWGSOP-2 has to be proven in longitudinal follow-up studies assessing outcomes and disease milestones. However, the EWGSOP-2 criteria should be more accurate than the first version as it uses muscle strength as the primary diagnostic factor. Muscle strength has been shown to be a better predictor of the adverse health outcomes that describe sarcopenia, namely quality of life, disability, and mortality (1, 45). Specifically, it has been shown that out of the three criteria defining sarcopenia, muscle strength is a better predictor of future mobility issues than muscle mass (46) and that it is also associated with recurrent falls independent of muscle mass (47). Moreover, with EWGSOP-2, the number of confirmed and severe cases was lower in comparison to EWGSOP-1, but the prevalence of probable cases was significantly higher, suggesting that muscle strength is more sensitive in identifying probable cases of sarcopenia (44, 48).
A recently published meta-analysis suggests that although sarcopenia seems to be common in patients with PD, the current evidence does not allow for the conclusion of a definitive prevalence of sarcopenia in patients with PD (31). Sarcopenia, indeed, was also common in our Austrian PD population. This can be due to a plethora of associated factors and symptoms, such as gait hypokinesia, which is present from an early stage of the disease (49). Recurrent falls are also reportedly higher in PD and can lead to physical inactivity and disability (39, 50). A decrease in the number of motor neurons due to dopaminergic dysfunction may also contribute to a higher proportion of people with PD having sarcopenia (28, 41). Additionally, a loss of lean muscle mass due to malnutrition in advanced PD has also been linked to sarcopenia (51).
The proportion of sarcopenia based on the SARC-F questionnaire was 44.4% which falls within the reported 6–65% in the general population (16–24). Two other studies report SARC-F-based prevalence in PD of 55.8% (39) and 30% (35), respectively; however, the latter reports numbers with a cut-off value of greater or equal to 6, making comparison difficult.
This study has several limitations. First, our study was limited by small sample size and the fact that all patients were recruited from a single center. Second, our results might be confounded by a regional bias in Tirol, Austria, where the population is generally active into old age. Thus, it is important to note that the prevalence data reported here have a geographical limit. A future multicenter study could yield more replicable data. Moreover, our study lacks a control population to compare the prevalence of sarcopenia according to the EWGSOP-2 criteria between patients with PD and the general population. It seems, indeed, that sarcopenia was more common in our PD population compared to the general population described in previous articles, 1–29% EWGSOP-1 (3), 10–11% EWGSOP-2 criteria (7, 8). EWGSOP-2 also suggests developing regional cut-off values to account for stature-dependent muscle strength and gait speed, which have been implemented by several other groups for Brazilian and Iranian and Asian populations (6, 9, 15).
We report the prevalence of sarcopenia in patients with PD in Tirol, Austria to be 28.4 % assessed with the EWGSOP-2 criteria. Our results are in line with other groups stating that EWGSOP-1 criteria overestimate sarcopenia prevalence compared to EWGSOP-2. Due to the low sensitivity and specificity of the SARC-F questionnaire, this scale is not conducive to detecting sarcopenia in a PD population.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethikkommission der Medizinischen Universität Innsbruck. The patients/participants provided their written informed consent to participate in this study.
DV: Research project: conception, organization, execution, Statistical analysis: design, execution, Manuscript: writing of the first draft. MP: Research project: conception, organization, execution, Statistical analysis: review and critique, Manuscript: review and critique. FK: Statistical analysis: execution, review and critique, Manuscript: review and critique. AL and SZ: Research project: execution. CH: Research project: conception, Manuscript: review and critique, WP: Research project: conception, KS: Research project: conception, Statistical analysis: review and critique, Manuscript: review and critique. All authors contributed to the article and approved the submitted version.
We want to thank all participants who voluntarily consented to provide information for this evaluation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
2. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in older people. Age Ageing. (2010) 39:412–23. doi: 10.1093/ageing/afq034
3. Cruz-Jentoft AJ, Landi F, Schneider SM, Zuniga C, Arai H, Boirie Y, et al. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the international sarcopenia initiative (EWGSOP and IWGS). Age Ageing. (2014) 43:748–59. doi: 10.1093/ageing/afu115
4. Purcell SA, Mackenzie M, Barbosa-Silva TG, Dionne IJ, Ghosh S, Olobatuyi O V, et al. Sarcopenia prevalence using different definitions in older community-dwelling Canadians. J Nutr Health Aging. (2020) 24:783–90. doi: 10.1007/s12603-020-1427-z
5. Wallengren O, Bosaeus I, Frändin K, Lissner L, Falk Erhag H, Wetterberg H, et al. Comparison of the 2010 and 2019 diagnostic criteria for sarcopenia by the European Working Group on Sarcopenia in Older People (EWGSOP) in two cohorts of Swedish older adults. BMC Geriatr. (2021) 21:600. doi: 10.1186/s12877-021-02533-y
6. Shafiee G, Heshmat R, Ostovar A, Khatami F, Fahimfar N, Arzaghi SM, et al. Comparison of EWGSOP-1and EWGSOP-2 diagnostic criteria on prevalence of and risk factors for sarcopenia among Iranian older people: the Bushehr Elderly Health (BEH) program. J Diabetes Metab Disord. (2020) 19:727–34. doi: 10.1007/s40200-020-00553-w
7. Fernandes LV, Paiva AEG, Silva ACB, de Castro IC, Santiago AF, de Oliveira EP, et al. Prevalence of sarcopenia according to EWGSOP1 and EWGSOP2 in older adults and their associations with unfavorable health outcomes: a systematic review. Aging Clin Exp Res. (2022) 34:505–14. doi: 10.1007/s40520-021-01951-7
8. Petermann-Rocha F, Balntzi V, Gray SR, Lara J, Ho FK, Pell JP, et al. Global prevalence of sarcopenia and severe sarcopenia: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. (2022) 13:86–99. doi: 10.1002/jcsm.12783
9. Yang L, Yao X, Shen J, Sun G, Sun Q, Tian X, et al. Comparison of revised EWGSOP criteria and four other diagnostic criteria of sarcopenia in Chinese community-dwelling elderly residents. Exp Gerontol. (2020) 130:110798. doi: 10.1016/j.exger.2019.110798
10. Yang M, Liu Y, Zuo Y, Tang H. Sarcopenia for predicting falls and hospitalization in community-dwelling older adults: EWGSOP vs. EWGSOP2. Sci Rep. (2019) 9:17636. doi: 10.1038/s41598-019-53522-6
11. Zhuang C-L, Shen X, Zou H-B, Dong Q-T, Cai H-Y, Chen X-L, et al. EWGSOP2 vs. EWGSOP1 for sarcopenia to predict prognosis in patients with gastric cancer after radical gastrectomy: analysis from a large-scale prospective study. Clin Nutr. (2020) 39:2301–10. doi: 10.1016/j.clnu.2019.10.024
12. Locquet M, Beaudart C, Petermans J, Reginster J-Y, Bruyère O. EWGSOP2 vs. EWGSOP1: impact on the prevalence of sarcopenia and its major health consequences. J Am Med Dir Assoc. (2019) 20:384–5. doi: 10.1016/j.jamda.2018.11.027
13. Phu S, Vogrin S, Zanker J, Bani Hassan E, Al Saedi A, Duque G. Agreement between initial and revised European working group on sarcopenia in older people definitions. J Am Med Dir Assoc. (2019) 20:382–383.e1. doi: 10.1016/j.jamda.2018.11.026
14. Villani A, McClure R, Barrett M, Scott D. Diagnostic differences and agreement between the original and revised European Working Group (EWGSOP) consensus definition for sarcopenia in community-dwelling older adults with type 2 diabetes mellitus. Arch Gerontol Geriatr. (2020) 89:104081. doi: 10.1016/j.archger.2020.104081
15. de Freitas MM, de Oliveira VLP, Grassi T, Valduga K, Miller MEP, Schuchmann RA, et al. Difference in sarcopenia prevalence and associated factors according to 2010 and 2018 European consensus (EWGSOP) in elderly patients with type 2 diabetes mellitus. Exp Gerontol. (2020) 132:110835. doi: 10.1016/j.exger.2020.110835
16. Nishikawa H, Asai A, Fukunishi S, Takeuchi T, Goto M, Ogura T, et al. Screening tools for sarcopenia. In Vivo. (2021) 35:3001–9. doi: 10.21873/invivo.12595
17. Hajaoui M, Locquet M, Beaudart C, Reginster J-Y, Petermans J, Bruyère O. Sarcopenia: performance of the SARC-F questionnaire according to the European consensus criteria, EWGSOP1 and EWGSOP2. J Am Med Dir Assoc. (2019) 20:1182–3. doi: 10.1016/j.jamda.2019.05.021
18. Wu T-Y, Liaw C-K, Chen F-C, Kuo K-L, Chie W-C, Yang R-S. Sarcopenia screened with SARC-F questionnaire is associated with quality of life and 4-year mortality. J Am Med Dir Assoc. (2016) 17:1129–35. doi: 10.1016/j.jamda.2016.07.029
19. Kemmler W, Sieber C, Freiberger E, von Stengel S. The SARC-F questionnaire: diagnostic overlap with established sarcopenia definitions in older German men with sarcopenia. Gerontology. (2017) 63:411–6. doi: 10.1159/000477935
20. Gade J, Quick AA, Beck AM, Rønholt F, Vinther A. SARC-F in hospitalized, geriatric medical patients—feasibility, prevalence of risk of sarcopenia, and characteristics of the risk group, including one-year follow-up. Clin Nutr ESPEN. (2020) 37:80–6. doi: 10.1016/j.clnesp.2020.03.016
21. Ishida Y, Maeda K, Nonogaki T, Shimizu A, Yamanaka Y, Matsuyama R, et al. As a screening tool for sarcopenia and possible sarcopenia proposed by AWGS 2019 in hospitalized older adults. J Nutr Health Aging. (2020) 24:1053–60. doi: 10.1007/s12603-020-1462-9
22. Bahat G, Oren MM, Yilmaz O, Kiliç C, Aydin K, Karan MA. Comparing SARC-F with SARC-CalF to screen sarcopenia in community living older adults. J Nutr Health Aging. (2018) 22:1034–8. doi: 10.1007/s12603-018-1072-y
23. Malmstrom TK, Miller DK, Simonsick EM, Ferrucci L, Morley JE. SARC-F a symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J Cachexia Sarcopenia Muscle. (2016) 7:28–36. doi: 10.1002/jcsm.12048
24. Woo J, Leung J, Morley JE. Validating the SARC-F: a suitable community screening tool for sarcopenia? J Am Med Dir Assoc. (2014) 15:630–4. doi: 10.1016/j.jamda.2014.04.021
25. Drey M, Hasmann SE, Krenovsky J-P, Hobert MA, Straub S, Elshehabi M, et al. Associations between early markers of Parkinson's disease and sarcopenia. Front Aging Neurosci. (2017) 9:1–5. doi: 10.3389/fnagi.2017.00053
26. Scalzo P, Kümmer A, Cardoso F, Teixeira AL. Serum levels of interleukin-6 are elevated in patients with Parkinson's disease and correlate with physical performance. Neurosci Lett. (2010) 468:56–8. doi: 10.1016/j.neulet.2009.10.062
27. Wu Y-N, Chen M-H, Chiang P-L, Lu C-H, Chen H-L, Yu C-C, et al. Associations between brain structural damage and core muscle loss in patients with Parkinson's disease. J Clin Med. (2020) 9:239. doi: 10.3390/jcm9010239
28. Caviness JN, Smith BE, Clarke Stevens J, Adler CH, Caselli RJ, Hentz JG, et al. Motor unit number estimates in idiopathic Parkinson's disease. Parkinsonism Relat Disord. (2002) 8:161–4. doi: 10.1016/S1353-8020(01)00007-4
29. Krenovsky J-P, Bötzel K, Ceballos-Baumann A, Fietzek UM, Schoser B, Maetzler W, et al. Interrelation between sarcopenia and the number of motor neurons in patients with Parkinsonian syndromes. Gerontology. (2020) 66:409–15. doi: 10.1159/000505590
30. Basualto-AlarcÃ3n C, Varela D, Duran J, Maass R, Estrada M. Sarcopenia and androgens: a link between pathology and treatment. Front Endocrinol. (2014) 5:1–11. doi: 10.3389/fendo.2014.00217
31. Cai Y, Feng F, Wei Q, Jiang Z, Ou R, Shang H. Sarcopenia in patients with Parkinson's disease: a systematic review and meta-analysis. Front Neurol. (2021) 12:1–11. doi: 10.3389/fneur.2021.598035
32. Postuma RB, Berg D, Stern M, Poewe W, Olanow CW, Oertel W, et al. MDS clinical diagnostic criteria for Parkinson's disease. Mov Disord. (2015) 30:1591–601. doi: 10.1002/mds.26424
33. Malmstrom TK, Morley JE. SARC-F a simple questionnaire to rapidly diagnose sarcopenia. J Am Med Dir Assoc. (2013) 14:531–2. doi: 10.1016/j.jamda.2013.05.018
34. Sergi G, De Rui M, Veronese N, Bolzetta F, Berton L, Carraro S, et al. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin Nutr. (2015) 34:667–73. doi: 10.1016/j.clnu.2014.07.010
35. da Luz MC, Pinho CP, de Araújo Bezerra GK, de Lemos MD, da Silva Diniz A, Cabral PC. SARC-F and SARC-CalF in screening for sarcopenia in older adults with Parkinson's disease. Exp Gerontol. (2021) 144:111183. doi: 10.1016/j.exger.2020.111183
36. Sacar DE, Kilic C, Karan MA, Bahat G. Ability of SARC-F to find probable sarcopenia cases in older adults. J Nutr Health Aging. (2021) 25:757–61. doi: 10.1007/s12603-021-1617-3
37. Barbosa-Silva TG, Menezes AMB, Bielemann RM, Malmstrom TK, Gonzalez MC. Enhancing SARC-F: improving sarcopenia screening in the clinical practice. J Am Med Dir Assoc. (2016) 17:1136–41. doi: 10.1016/j.jamda.2016.08.004
38. Barbosa-Silva TG, Bielemann RM, Gonzalez MC, Menezes AMB. Prevalence of sarcopenia among community-dwelling elderly of a medium-sized South American city: results of the COMO VAI? Study. J Cachexia Sarcopenia Muscle. (2016) 7:136–43. doi: 10.1002/jcsm.12049
39. Peball M, Mahlknecht P, Werkmann M, Marini K, Murr F, Herzmann H, et al. Prevalence and associated factors of sarcopenia and frailty in Parkinson's disease: a cross-sectional study. Gerontology. (2019) 65:216–28. doi: 10.1159/000492572
40. Barichella M, Pinelli G, Iorio L, Cassani E, Valentino A, Pusani C, et al. Sarcopenia and dynapenia in patients with Parkinsonism. J Am Med Dir Assoc. (2016) 17:640–6. doi: 10.1016/j.jamda.2016.03.016
41. Vetrano DL, Pisciotta MS, Laudisio A, Monaco MR, Onder G, Brandi V, et al. Sarcopenia in Parkinson disease: comparison of different criteria and association with disease severity. J Am Med Dir Assoc. (2018) 19:523–7. doi: 10.1016/j.jamda.2017.12.005
42. Ozer FF, Akin S, Gultekin M, Zararsiz GE. Sarcopenia, dynapenia, and body composition in Parkinson's disease: are they good predictors of disability?: a case–control study. Neurol Sci. (2020) 41:313–20. doi: 10.1007/s10072-019-04073-1
43. Yazar T, Yazar HO, Zayimoglu E, Çankaya S. Incidence of sarcopenia and dynapenia according to stage in patients with idiopathic Parkinson's disease. Neurol Sci. (2018) 39:1415–21. doi: 10.1007/s10072-018-3439-6
44. Ramirez E, Salas R, Bouzas C, Pastor R, Tur JA. Comparison between original and reviewed consensus of European working group on sarcopenia in older people: a probabilistic cross-sectional survey among community-dwelling older people. Gerontology. (2021) 68:869–76. doi: 10.1159/000519304
45. Rijk JM, Roos PRKM, Deckx L, van den Akker M, Buntinx F. Prognostic value of handgrip strength in people aged 60 years and older: a systematic review and meta-analysis. Geriatr Gerontol Int. (2016) 16:5–20. doi: 10.1111/ggi.12508
46. McLean RR, Shardell MD, Alley DE, Cawthon PM, Fragala MS, Harris TB, et al. Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: the foundation for the national institutes of health (FNIH) sarcopenia project. J Gerontol Ser A. (2014) 69:576–83. doi: 10.1093/gerona/glu012
47. Schaap LA, van Schoor NM, Lips P, Visser M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: the longitudinal aging study Amsterdam. J Gerontol Ser A. (2018) 73:1199–204. doi: 10.1093/gerona/glx245
48. Van Ancum JM, Alcazar J, Meskers CGM, Nielsen BR, Suetta C, Maier AB. Impact of using the updated EWGSOP2 definition in diagnosing sarcopenia: A clinical perspective. Arch Gerontol Geriatr. (2020) 90:104125. doi: 10.1016/j.archger.2020.104125
49. Baltadjieva R, Giladi N, Gruendlinger L, Peretz C, Hausdorff JM. Marked alterations in the gait timing and rhythmicity of patients with de novo Parkinson's disease. Eur J Neurosci. (2006) 24:1815–20. doi: 10.1111/j.1460-9568.2006.05033.x
50. Rahman S, Griffin HJ, Quinn NP, Jahanshahi M. On the nature of fear of falling in Parkinson's disease. Behav Neurol. (2011) 24:219–28. doi: 10.1155/2011/274539
Keywords: Parkinson's disease, sarcopenia, prevalence, screening tool, sensitivity, specificity
Citation: Valent D, Peball M, Krismer F, Lanbach A, Zemann S, Horlings C, Poewe W and Seppi K (2022) Different assessment tools to detect sarcopenia in patients with Parkinson's disease. Front. Neurol. 13:1014102. doi: 10.3389/fneur.2022.1014102
Received: 08 August 2022; Accepted: 07 November 2022;
Published: 28 November 2022.
Edited by:
Roberta Balestrino, San Raffaele Scientific Institute (IRCCS), ItalyReviewed by:
Marianna Amboni, University of Salerno, ItalyCopyright © 2022 Valent, Peball, Krismer, Lanbach, Zemann, Horlings, Poewe and Seppi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dora Valent, RG9yYS52YWxlbnRAdGlyb2wta2xpbmlrZW4uYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.