
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 10 October 2022
Sec. Sleep Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fneur.2022.1009907
This article is part of the Research Topic Neuroimaging Findings in Chronic diseases, Volume 2 View all 8 articles
 Chaofan Geng1
Chaofan Geng1 Hongju Zhang1,2*
Hongju Zhang1,2*Idiopathic rapid eye movement sleep behavior disorder (iRBD) is an important non-motor complication of Parkinson's disease. At the same time, iRBD is considered to be the prodromal stage of α-synucleinopathy. This high risk of conversion suggests that iRBD becomes a nerve It is a window for early research on degenerative diseases and is the best candidate for neuroprotection trials. A wide range of neuroimaging techniques has improved our understanding of iRBD as a prodromal stage of the disease. In addition, neuroimaging of abnormal iRBD is expected to be a potential biomarker for predicting clinical phenotypic transformation. This article reviews the research progress of neuromolecular imaging in patients with iRBD from the perspective of iRBD transforming synucleinopathies.
Idiopathic rapid eye movement (REM) sleep behavior disorder (iRBD) is a parasomnia mainly characterized by the loss of muscular atonia and dream enacting behaviors during REM sleep (1, 2). The pathogenesis is related to the dysfunction of the locus coeruleus and the ventral nucleus of the medulla oblongata, which have a role in regulating muscle tone during the REM period (3). Longitudinal studies have reported that 80% of clinically diagnosed iRBD patients can develop neurodegenerative disorders after 10-year follow-up, especially α-synucleinopathies, such as Parkinson's disease (PD), dementia with Lewy bodies, and multiple system atrophy (MSA) (1, 4, 5). Accordingly, iRBD is considered to be a powerful prodromal state of α-synucleinopathies (6) and has become the most important clinical symptom for predicting neurodegenerative diseases (7). However, the time course of iRBD conversion to α-synucleinopathy is highly variable (8), and the search for early biomarkers of iRBD conversion becomes a preferred problem (9), which could contribute to delaying disease progression in its earliest stages.
Currently, more and more studies are looking for early neuroimaging evidence of iRBD transformation in order to detect structural and functional abnormalities in the iRBD brain earlier (10). Among neuroimaging markers, radionuclide imaging is a widely used molecular imaging technique because of its precise localization and specific labeling (11), mainly including Positron emission tomography (PET), Single photon emission computed tomography (SPECT), and 123Iodine-metaiodobenzylguanidine (123I-MIBG) cardiac imaging.
Considering all these factors, we review the latest research on molecular imaging between iRBD and α-synucleinopathies. The molecular neuroimaging markers that predict the early transformation of iRBD were the place we pay the closest attention to in this article. A comprehensive understanding and review of neuroimaging techniques to explore phenotypic conversion in iRBD will be able to guide future research in this field and further facilitate the clinical management of this disease.
The exact pathophysiology of iRBD is not fully established. Animal models of RBD with damage to the sublaterodorsal tegmental nucleus (SLD) showed behavioral abnormalities during REM sleep similar to those of human RBD (12). Previous studies have confirmed that the SLD is the key brain structure that triggers muscle retardation in REM sleep and that selective blockade of glutamatergic transmission in the SLD leads to REM sleep without atonia (RSWA) (13). During REM sleep, SLD inhibits skeletal muscle movement and dystonia during REM sleep by activating direct and indirect inhibitory pathways (13). SLD neurons act on interneurons via a direct pathway. Intermediate neurons in turn inhibit glycinergic and gamma-aminobutyric acidergic neurons via spinal anterior horn motor neurons, resulting in skeletal during REM sleep skeletal muscle movements being inhibited during REM sleep (14). In addition, glutamatergic neurons in the SLD can also activate the ventral medial reticular formation (VMD) of the medulla oblongata through an indirect pathway, leading to a relaxation of skeletal muscle tone (15). Under normal waking conditions, direct stimulation of the VMM can effectively trigger REM sleep and lead to motor inhibition during REM sleep. SLD and VMM together form a complete brainstem circuit, and damage to any part of this circuit may lead to RBD (16).
[18F] fluorodeoxyglucose (FDG) positron emission tomography (PET) is an assay targeting glucose metabolism visualization in the brain, with higher metabolic rates presenting high signal changes (17), reflecting the metabolic activity of neurons in the brain. The first 18F-FDG-PET scan was performed on nine patients with iRBD, and four patients were found to have decreased glucose metabolism in the occipital cortex, especially in the primary visual cortex (PVC), which is the priority area for patients with MSA. In contrast, the other five patients showed hypermetabolic changes in the left cingulate gyrus, right frontal lobe and right temporal lobe, which are the preferentially affected regions of PD patients (18). The differences in metabolic profiles between regions suggest heterogeneity of clinical conversion in patients with iRBD. Another study reported that 63. 6% of people with decreased occipital cortex glucose metabolism converted to iRBD after an average of 3 years (19), suggesting that decreased occipital glucose metabolism is an early intracerebral change in iRBD. iRBD patients also have increased glucose metabolism in the hippocampus, cingulate gyrus, pons and posterior cerebellum, while decreased glucose metabolism in the lingual gyrus (20), and iRBD with significant decreased occipital cortex glucose metabolism is often associated with mild cognitive impairment (19). Hypermetabolism in the pontine region of the brain in patients with iRBD may be an early alteration in the dystonia regulatory area, and hypermetabolism in the cingulate and hippocampal regions may be due to abnormal neuronal generation and an early alteration in the conversion of iRBD to α-synucleinopathy (21–23). A previous longitudinal study found that all patients with iRBD developed cognitive impairment after 6.4 years, and there was a significant correlation with decreased glucose metabolism in the PVC region, suggesting that decreased metabolism in the PVC region may be responsible for their cognitive impairment (24).
The iRBD metabolic pattern (RBD-related pattern, RBDRP) was determined using 18F-FDG-PET and was characterized by increased metabolic activity in the pons, cerebellum, thalamus, hippocampus, medial frontal area, superior limbic gyrus, and inferior temporal gyrus, while decreased metabolic activity in the occipital and superior temporal gyrus. This pattern was significantly expressed in the early stages of PD and correlated with the severity of PD (25). Expression of both PDRP and iRBDRP was higher in patients with a more severe form of PD (PD-MCI), which indicates that expression of the 2 patterns increases with disease severity (26). Therefore, it can predict the future regression of patients with iRBD and has clinical applications.
Single photon emission computed tomography is a neuroimaging tool to measure regional cerebral blood flow (rCBF) (27). Using SPECT, it was demonstrated that patients with iRBD had decreased perfusion in the bilaterally frontal, temporal, and parietal lobes, while increased perfusion in the hippocampus, putamen, and pons (28), and the extent of this cerebral perfusion change was more pronounced in patients with iRBD with cognitive impairment (22). However, no correlation was found between changes in local cerebral blood flow and the duration of RBD symptoms in patients (28). Another study found that the cerebral perfusion in the parietal occipital and parietal temporal regions was decreased in patients with iRBD, and this decreased level of perfusion could be used to predict the conversion of iRBD to α-synucleinopathy (29). A longitudinal study found that increased frontal and occipital temporal perfusion returned to normal control levels as the duration of iRBD patients progressed (30), suggesting that compensation may have occurred. We hypothesized that this change in brain perfusion pattern is an intermediate link between iRBD and neurological symptoms and that longitudinal exploration of local cerebral blood flow levels in different brain regions with iRBD can help to understand the pathophysiological mechanisms underlying the transformation to α-synucleinopathy.
The main pathological alteration in PD is degeneration of the substantial nigra-striatal dopaminergic pathway (31). Striatal dopamine levels can be reflected by selective binding of dopamine transporter (DAT) using specific tracers. Several studies have shown that patients with iRBD have abnormal DAT imaging (8, 32–34), and are at high risk for short-term conversion to α-synucleinopathy (35, 36). However, a meta-analysis noted that while abnormal DAT imaging supports the conversion to α-synucleinopathy, there was high heterogeneity among neuroimaging methods and multicenter studies were needed to determine the diagnostic validity of DAT-SPECT (37). The results of a multicenter study that included 1,280 patients with iRBD suggested a 1.98-fold risk of conversion to α-synuclein in patients with iRBD with abnormal DAT imaging at baseline (38), with a low effect size. We speculated that the value of DAT imaging as a predictive marker may have been severely underestimated because only some patients in the study underwent DAT imaging and the imaging methods were not uniform. Notably, multiple predictors identified by the study were non-specific (36), for which the results of the quantitative DAT-SPECT study suggest that reduction of FP-CIT uptake in putamen greater than 25% can predict synucleinopathy during an average follow-up of 3 years (35). A growing body of evidence had demonstrated that abnormal DAT binding can predict the future short-term risk of clinically-defined α-synucleinopathy diagnosis (34). Previous studies showed that iRBD patients with mild cognitive impairment (MCI) who had abnormal DAT manifestations had a higher transformation to α-synucleinopathy risk was higher in iRBD patients with abnormal DAT imaging (HR = 25.05) (39). Therefore, the presence of abnormal DAT imaging in patients with iRBD suggests that patients have developed pathological changes of neurodegenerative disease and their neuronal loss has not yet reached the clinical diagnostic threshold. Therefore, abnormal DAT imaging may be used as a predictor of conversion to α-synucleinopathy.
Previous studies have confirmed the involvement of the mesencephalic 5-hydroxytryptaminergic and norepinephrinergic systems of the locus coeruleus in the pathophysiology of α-synucleinopathy (40). Thalamic monoaminergic dysfunction was found in patients with iRBD (41), reflecting abnormalities in the terminals of neurons originating from the raphe nucleus and locus coeruleus projections. Although 5-hydroxytryptaminergic reuptake inhibitors can induce RBD symptoms (42), no imaging evidence of impaired an 5-hydroxytryptaminergic system in patients with iRBD has been found (37, 42–44). It was found that the norepinephrine-rich blue spot nuclei in the brainstem of PD patients were abnormally visualized and preceded by dopaminergic (45), which confirms the Braak staging theory of PD, a bottom-up pathological damage process (46). In vivo study of noradrenergic changes in 17 patients with iRBD using 11C-MeNER as a tracer revealed that tracer uptake levels were decreased in the locus coeruleus to the thalamus and red nucleus regions in patients with iRBD compared to normal controls (47). Compared with PD patients, the uptake level of 11C-MeNER tracer in the hypothalamus, red nucleus, and locus coeruleus of PD patients with RBD decreased. Moreover, the abnormal noradrenergic level of PD patients with RBD was positively correlated with abnormal muscle activity during REM sleep (48). Therefore, it was suggested that norepinephrine plays an important role in the pathogenesis of iRBD. A recent study found that the uptake level of 11C-MeNER in the primary sensorimotor cortex of iRBD patients decreased (49), and it was speculated that there was nerve fiber projection damage from the locus coeruleus to the primary sensorimotor cortex. These evidences indicated that the norepinephrine system in locus coeruleus may become the target of early intervention of iRBD, but there was still a lack of longitudinal research to prove the application value of norepinephrine.
Microglia are widely distributed immune cells in the central nervous system and are closely associated with neuronal inflammatory responses, and long-term activation of microglia may be involved in the development and progression of neurodegenerative diseases (50). Previous studies had demonstrated that peripheral immunity contributes to PD development (51). Several studies have shown microglial activation in patients with α-synucleinopathy, suggesting that neuroinflammation may be a causal mechanism for α-synucleinopathy (52). Controlling microglia activation in the early stages of the disease could provide a potential therapeutic strategy to slow down disease progression. Using 11C-PK11195 as a tracer, an in vivo study of 20 patients with iRBD revealed that microglia activation was elevated in the nigrostriatal region and higher than in the striatal region in patients with iRBD compared to normal controls (53), and that elevated levels of 11C-PK11195 uptake in the nigrostriatal region correlated with decreased levels of 18F-DOPA uptake in the striatum, and that caudate nucleus involvement was consistent with impairment of Lewy body dementia (54), suggesting that synaptic dysfunction of striatal dopamine neurons in patients with iRBD is accompanied by an inflammatory response in the substantia nigra. The observation of microglia activation in the striatal region revealed a significantly higher level of activation than in the substantia nigra (52), probably due to the size of the tissue structure in both regions. Recent studies have found significantly higher levels of microglia activation in the occipital lobe of patients with iRBD (41), suggesting that neuroinflammation in the occipital lobe is involved in the pathogenesis of iRBD. However, whether the level of microglia activation in iRBD can be used as a biomarker for conversion to α-synucleinopathy needs to be further investigated and demonstrated due to the lack of relevant studies.
An increasing number of clinical studies have focused on the evaluation of cardiac sympathetic nerve function in iRBD. [123I] metaiodobenzylguanidine (123I-MIBG) cardiac imaging is a commonly used imaging technique to diagnose cardiac sympathetic function (55). It was found that 123I-MIBG uptake levels were decreased in the heart of PD patients (56), and more significantly in PD patients with RBD (57). Studies have shown that patients with iRBD also have decreased 123I-MIBG uptake levels (58, 59), and are similar to Lewy body dementia. Previous studies had found that cardiac sympathetic function was linked with the severity of REM in iRBD patients (60). Furthermore, some studies have shown that abnormal 123I-MIBG manifestations can precede the dopaminergic system in patients with iRBD (61, 62). However, a longitudinal study of iRBD patients followed for 2.8 years found no significant changes in the level of 123I-MIBG uptake by the patient's heart, possibly related to the course of the disease (57), which was contrary to the findings of other studies (63). Despite the high sensitivity and specificity of early autonomic damage in PD to cardiac sympathetic imaging, whether 123I-MIBG can be a neurobiological marker to predict disease progression in patients with iRBD needs to be further validated (64).
Neuroimaging reveals the presence of structural and functional alterations in iRBD that precede α-synucleinopathy (Table 1). The use of molecular imaging techniques may contribute to what may be a sensitive screening tool for exploring iRBD-transformed α-synucleinopathy, with a wide range of clinical applications. Compared to other risk factors for α-synucleinopathy, such as cognitive deficits, olfactory impairment and dopamine transporter protein (DAT-SPECT) abnormalities are at much higher predicted risk in the conversion of iRBD to α-synucleinopathy. Therefore, a single imaging modality for iRBD does not yet fully reflect the underlying pathophysiological changes in iRBD or the different clinical features. Therefore, adopting multiple complementary neuroimaging examinations and conducting prospective studies to validate the search for sensitive and effective biomarkers of iRBD conversion to α-synucleinopathy will help to accurately identify the clinical conversion of iRBD.
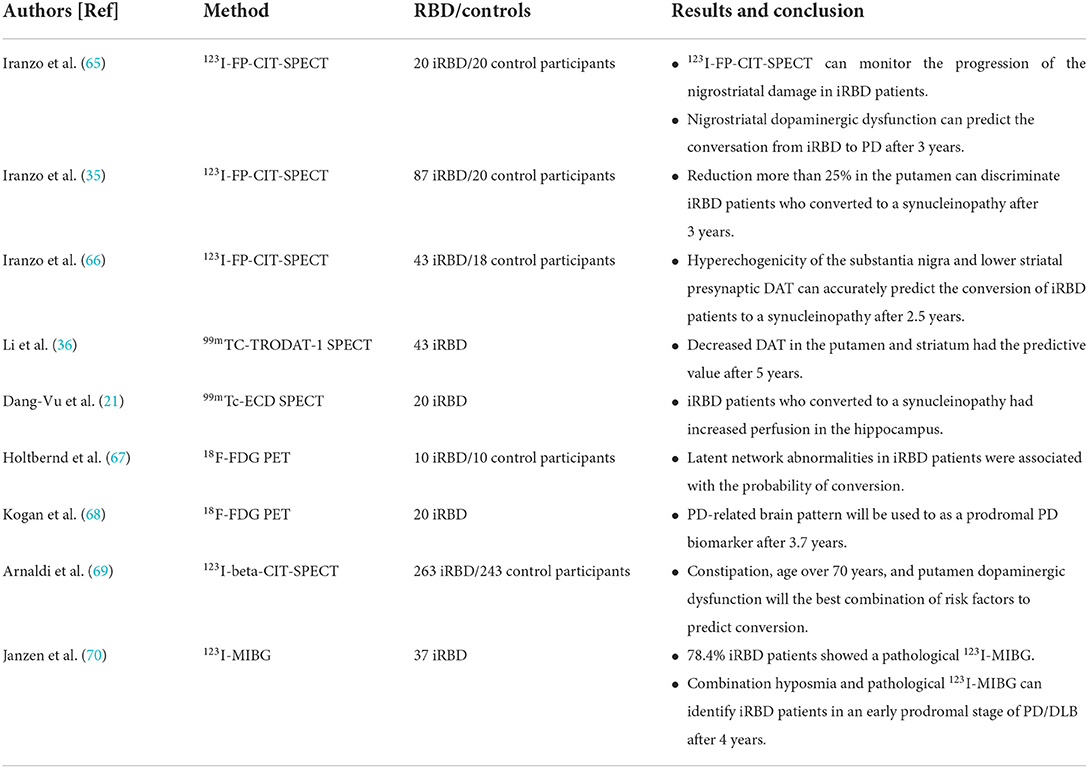
Table 1. Main findings of each neuromolecular imaging studies in iRBD patients.
CG: wrote first draft. HZ: conceptualization and resources. All authors approved the submitted version.
This work was supported by the Henan Medical Science and Technology Research Program (No. 202102310082), and Henan Province Medical Science and Technology Tackling Provincial Ministry Key Projects (SBGJ202102033).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Iranzo A, Santamaria J, Tolosa E. Idiopathic rapid eye movement sleep behavior disorder: diagnosis, management, and the need for neuroprotective interventions. Lancet Neurol. (2016) 15:405–19. doi: 10.1016/S1474-4422(16)00057-0
2. Sun J, Lai Z, Ma J, Gao L, Chen M, Chen J, et al. Quantitative evaluation of iron content in idiopathic rapid eye movement sleep behavior disorder. Mov Disord. (2020) 35:478–85. doi: 10.1002/mds.27929
3. Iranzo A. The REM sleep circuit and how its impairment leads to REM sleep behavior disorder. Cell Tissue Res. (2018) 373:245–66. doi: 10.1007/s00441-018-2852-8
4. Schenck CH, Boeve BF, Mahowald MW. Delayed emergence of a Parkinsonian disorder or dementia in 81% of older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder: a 16-year update on a previously reported series. Sleep Med. (2013) 14:744–8. doi: 10.1016/j.sleep.2012.10.009
5. Postuma RB, Iranzo A, Hogl B, Arnulf I, Ferini-Strambi L, Manni R, et al. Risk factors for neurodegeneration in idiopathic rapid eye movement sleep behavior disorder: a multicenter study. Ann Neurol. (2015) 77:830–9. doi: 10.1002/ana.24385
6. Kim R, Jun JS, Kim HJ, Jung KY, Shin YW, Yang TW, et al. Peripheral blood inflammatory cytokines in idiopathic REM sleep behavior disorder. Mov Disord. (2019) 34:1739–44. doi: 10.1002/mds.27841
7. Ehgoetz MK, Matar E, Hall JM, Phillips J, Szeto JYY, Gouelle A, et al. Subtle gait and balance impairments occur in idiopathic rapid eye movement sleep behavior disorder. Mov Disord. (2019) 34:1374–80. doi: 10.1002/mds.27780
8. Huang Z, Jiang C, Li L, Xu Q, Ge J, Li M, et al. Correlations between dopaminergic dysfunction and abnormal metabolic network activity in REM sleep behavior disorder. J Cereb Blood Flow Metab. (2020) 40:552–62. doi: 10.1177/0271678X19828916
9. Salat D, Noyce A J, Schrag A, Tolosa E. Challenges of modifying disease progression in prediagnostic Parkinson's disease. Lancet Neurol. (2016) 15:637–48. doi: 10.1016/S1474-4422(16)00060-0
10. Heller J, Brcina N, Dogan I, Holtbernd F, Romanzetti S, Schulz JB, et al. Brain imaging findings in idiopathic REM sleep behavior disorder (RBD)—a systematic review on potential biomarkers for neurodegeneration. Sleep Med Rev. (2017) 34:23–33. doi: 10.1016/j.smrv.2016.06.006
11. Campabadal A, Segura B, Junque C, Iranzo A. Structural and functional magnetic resonance imaging in isolated REM sleep behavior disorder: a systematic review of studies using neuroimaging software. Sleep Med Rev. (2021) 59:101495. doi: 10.1016/j.smrv.2021.101495
12. George R, Haslett WL, Jenden DJ. A cholinergic mechanism in the brainstem reticular formation: induction of paradoxical sleep. Int J Neuropharmacol. (1964) 3:541–52. doi: 10.1016/0028-3908(64)90076-0
13. Valencia GS, Libourel PA, Lazarus M, Grassi D, Luppi PH, Fort P. Genetic inactivation of glutamate neurons in the rat sublaterodorsal tegmental nucleus recapitulates REM sleep behavior disorder. Brain. (2017) 140:414–28. doi: 10.1093/brain/aww310
14. Rodriguez CL, Jaimchariyatam N, Budur K. Rapid eye movement sleep behavior disorder: a review of the literature and update on current concepts. Chest. (2017) 152:650–62. doi: 10.1016/j.chest.2017.03.015
15. Zhang F, Niu L, Liu X, Liu Y, Li S, Yu H, et al. Rapid eye movement sleep behavior disorder and neurodegenerative diseases: an update. Aging Dis. (2020) 11:315–26. doi: 10.14336/AD.2019.0324
16. Iranzo A, Tolosa E, Gelpi E, Molinuevo JL, Valldeoriola F, Serradell M, et al. Neurodegenerative disease status and post-mortem pathology in idiopathic rapid-eye-movement sleep behavior disorder: an observational cohort study. Lancet Neurol. (2013) 12:443–53. doi: 10.1016/S1474-4422(13)70056-5
17. Meles SK, Teune LK, de Jong BM, Dierckx RA, Leenders KL. Metabolic imaging in Parkinson disease. J Nucl Med. (2017) 58:23–28. doi: 10.2967/jnumed.116.183152
18. Fujishiro H, Iseki E, Murayama N, Yamamoto R, Higashi S, Kasanuki K, et al. Diffuse occipital hypometabolism on [18 F]-FDG PET scans in patients with idiopathic REM sleep behavior disorder: prodromal dementia with Lewy bodies? Psychogeriatrics. (2010) 10:144–52. doi: 10.1111/j.1479-8301.2010.00325.x
19. Eskildsen SF, Coupe P, Garcia-Lorenzo D, Fonov V, Pruessner JC, Collins DL, et al. Prediction of Alzheimer's disease in subjects with mild cognitive impairment from the ADNI cohort using patterns of cortical thinning. Neuroimage. (2013) 65:511–21. doi: 10.1016/j.neuroimage.2012.09.058
20. Ge J, Wu P, Peng S, Yu H, Zhang H, Guan Y, et al. Assessing cerebral glucose metabolism in patients with idiopathic rapid eye movement sleep behavior disorder. J Cereb Blood Flow Metab. (2015) 35:2062–9. doi: 10.1038/jcbfm.2015.173
21. Dang-Vu TT, Gagnon JF, Vendette M, Soucy JP, Postuma RB, Montplaisir J. Hippocampal perfusion predicts impending neurodegeneration in REM sleep behavior disorder. Neurology. (2012) 79:2302–6. doi: 10.1212/WNL.0b013e318278b658
22. Vendette M, Gagnon JF, Soucy JP, Gosselin N, Postuma RB, Tuineag M, et al. Brain perfusion and markers of neurodegeneration in rapid eye movement sleep behavior disorder. Mov Disord. (2011) 26:1717–24. doi: 10.1002/mds.23721
23. Chen M, Li Y, Chen J, Gao L, Sun J, Gu Z, et al. Structural and functional brain alterations in patients with idiopathic rapid eye movement sleep behavior disorder. J Neuroradiol. (2020) 49:66–72. doi: 10.1016/j.neurad.2020.04.007
24. Ota K, Fujishiro H, Kasanuki K, Kondo D, Chiba Y, Murayama N, et al. Prediction of later clinical course by a specific glucose metabolic pattern in non-demented patients with probable REM sleep behavior disorder admitted to a memory clinic: a case study. Psychiatry Res Neuroimaging. (2016) 248:151–8. doi: 10.1016/j.pscychresns.2015.12.004
25. Wu P, Yu H, Peng S, Dauvilliers Y, Wang J, Ge J, et al. Consistent abnormalities in metabolic network activity in idiopathic rapid eye movement sleep behavior disorder. Brain. (2014) 137(Pt 12):3122–8. doi: 10.1093/brain/awu290
26. Meles SK, Renken RJ, Janzen A, Vadasz D, Pagani M, Arnaldi D, et al. The metabolic pattern of idiopathic REM sleep behavior disorder reflects early-stage Parkinson disease. J Nucl Med. (2018) 59:1437–44. doi: 10.2967/jnumed.117.202242
27. Takahashi M, Tada T, Nakamura T, Koyama K, Momose T. Efficacy and limitations of rCBF-SPECT in the diagnosis of Alzheimer's disease with amyloid-PET. Am J Alzheimer's Dis Other Demen. (2019) 34:314–21. doi: 10.1177/1533317519841192
28. Hanyu H, Inoue Y, Sakurai H, Kanetaka H, Nakamura M, Miyamoto T, et al. Regional cerebral blood flow changes in patients with idiopathic REM sleep behavior disorder. Eur J Neurol. (2011) 18:784–8. doi: 10.1111/j.1468-1331.2010.03283.x
29. Sakurai H, Hanyu H, Inoue Y, Kanetaka H, Nakamura M, Miyamoto T, et al. Longitudinal study of regional cerebral blood flow in elderly patients with idiopathic rapid eye movement sleep behavior disorder. Geriatr Gerontol Int. (2014) 14:115–20. doi: 10.1111/ggi.12068
30. Baril AA, Gagnon JF, Pelletier A, Soucy JP, Gosselin N, Postuma RB, et al. Changes in regional cerebral perfusion over time in idiopathic REM sleep behavior disorder. Mov Disord. (2020) 35:1475–81. doi: 10.1002/mds.28092
31. Bloem BR, Okun MS, Klein C. Parkinson's disease. Lancet. (2021) 397:2284–303. doi: 10.1016/S0140-6736(21)00218-X
32. Miyamoto T, Miyamoto M, Numahata K, Onoue H, Akaiwa Y, Sairenchi T. Reduced dopamine transporter binding predicts early transition to Lewy body disease in Japanese patients with idiopathic rapid eye movement sleep behavior disorder. J Neurol Sci. (2020) 414:116821. doi: 10.1016/j.jns.2020.116821
33. Cao R, Chen X, Xie C, Hu P, Wang K. Serial dopamine transporter imaging of nigrostriatal function in Parkinson's disease with probable REM sleep behavior disorder. Front Neurosci. (2020) 14:349. doi: 10.3389/fnins.2020.00349
34. Chahine LM, Brumm MC, Caspell-Garcia C, Oertel W, Mollenhauer B, Amara A, et al. Dopamine transporter imaging predicts clinically-defined alpha-synucleinopathy in REM sleep behavior disorder. Ann Clin Transl Neurol. (2021) 8:201–12. doi: 10.1002/acn3.51269
35. Iranzo A, Santamaria J, Valldeoriola F, Serradell M, Salamero M, Gaig C, et al. Dopamine transporter imaging deficit predicts early transition to synucleinopathy in idiopathic rapid eye movement sleep behavior disorder. Ann Neurol. (2017) 82:419–28. doi: 10.1002/ana.25026
36. Li Y, Kang W, Yang Q, Zhang L, Zhang L, Dong F, et al. Predictive markers for early conversion of iRBD to neurodegenerative synucleinopathy diseases. Neurology. (2017) 88:1493–500. doi: 10.1212/WNL.0000000000003838
37. Bauckneht M, Chincarini A, De Carli F, Terzaghi M, Morbelli S, Nobili F, et al. Presynaptic dopaminergic neuroimaging in REM sleep behavior disorder: a systematic review and meta-analysis. Sleep Med Rev. (2018) 41:266–74. doi: 10.1016/j.smrv.2018.04.001
38. Postuma RB, Iranzo A, Hu M, Högl B, Boeve BF, Manni R, et al. Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behavior disorder: a multicentre study. Brain. (2019) 142:744–59. doi: 10.1093/brain/awz030
39. Arnaldi D, Chincarini A, De Carli F, Famà F, Girtler N, Brugnolo A, et al. The fate of patients with REM sleep behavior disorder and mild cognitive impairment. Sleep Med. (2021) 79:205–10. doi: 10.1016/j.sleep.2020.02.011
40. Eskildsen SF, Iranzo A, Stokholm MG, Stær K, Østergaard K, Serradell M, et al. Impaired cerebral microcirculation in isolated REM sleep behavior disorder. Brain. (2021) 144:1498–508. doi: 10.1093/brain/awab054
41. Stokholm MG, Iranzo A, Ostergaard K, Serradell M, Otto M, Bacher Svendsen K, et al. Extrastriatal monoaminergic dysfunction and enhanced microglial activation in idiopathic rapid eye movement sleep behavior disorder. Neurobiol Dis. (2018) 115:9–16. doi: 10.1016/j.nbd.2018.02.017
42. Arnaldi D, Fama F, De Carli F, Morbelli S, Ferrara M, Picco A, et al. The role of the serotonergic system in REM sleep behavior disorder. Sleep. (2015) 38:1505–9. doi: 10.5665/sleep.5000
43. Qamhawi Z, Towey D, Shah B, Pagano G, Seibyl J, Marek K, et al. Clinical correlates of raphe serotonergic dysfunction in early Parkinson's disease. Brain. (2015) 138(Pt 10):2964–73. doi: 10.1093/brain/awv215
44. Kotagal V, Albin RL, Muller ML, Koeppe RA, Chervin RD, Frey KA, et al. Symptoms of rapid eye movement sleep behavior disorder are associated with cholinergic denervation in Parkinson disease. Ann Neurol. (2012) 71:560–8. doi: 10.1002/ana.22691
45. McMillan PJ, White SS, Franklin A, Greenup JL, Leverenz JB, Raskind MA, et al. Differential response of the central noradrenergic nervous system to the loss of locus coeruleus neurons in Parkinson's disease and Alzheimer's disease. Brain Res. (2011) 1373:240–52. doi: 10.1016/j.brainres.2010.12.015
46. Mariotti P, Quaranta D, Di Giacopo R, Bentivoglio AR, Mazza M, Martini A, et al. Rapid eye movement sleep behavior disorder: a window on the emotional world of Parkinson disease. Sleep. (2015) 38:287–94. doi: 10.5665/sleep.4416
47. Knudsen K, Fedorova TD, Hansen AK, Sommerauer M, Otto M, Svendsen KB, et al. In-vivo staging of pathology in REM sleep behavior disorder: a multimodality imaging case-control study. Lancet Neurol. (2018) 17:618–28. doi: 10.1016/S1474-4422(18)30162-5
48. Sommerauer M, Fedorova TD, Hansen AK, Knudsen K, Otto M, Jeppesen J, et al. Evaluation of the noradrenergic system in Parkinson's disease: an 11C-MeNER PET and neuromelanin MRI study. Brain. (2018) 141:496–504. doi: 10.1093/brain/awx348
49. Andersen KB, Hansen AK, Sommerauer M, Fedorova TD, Knudsen K, Vang K, et al. Altered sensorimotor cortex noradrenergic function in idiopathic REM sleep behavior disorder—a PET study. Parkinsonism Relat Disord. (2020) 75:63–9. doi: 10.1016/j.parkreldis.2020.05.013
50. Smith JA, Das A, Ray SK, Banik NL. Role of pro-inflammatory cytokines released from microglia in neurodegenerative diseases. Brain Res Bull. (2012) 87:10–20. doi: 10.1016/j.brainresbull.2011.10.004
51. De Francesco E, Terzaghi M, Storelli E, Magistrelli L, Comi C, Legnaro M, et al. CD4+ T-cell transcription factors in idiopathic REM sleep behavior disorder and Parkinson's disease. Mov Disord. (2021) 36:225–9. doi: 10.1002/mds.28137
52. Iannaccone S, Cerami C, Alessio M, Garibotto V, Panzacchi A, Olivieri S, et al. In vivo microglia activation in very early dementia with Lewy bodies, comparison with Parkinson's disease. Parkinsonism Relat Disord. (2013) 19:47–52. doi: 10.1016/j.parkreldis.2012.07.002
53. Stokholm MG, Iranzo A, Ostergaard K, Serradell M, Otto M, Svendsen KB, et al. Assessment of neuroinflammation in patients with idiopathic rapid-eye-movement sleep behavior disorder: a case-control study. Lancet Neurol. (2017) 16:789–96. doi: 10.1016/S1474-4422(17)30173-4
54. Walker Z, Costa DC, Walker RW, Lee L, Livingston G, Jaros E, et al. Striatal dopamine transporter in dementia with Lewy bodies and Parkinson disease: a comparison. Neurology. (2004) 62:1568–72. doi: 10.1212/01.WNL.0000123248.39847.1D
55. Orimo S, Suzuki M, Inaba A, Mizusawa H. 123I-MIBG myocardial scintigraphy for differentiating Parkinson's disease from other neurodegenerative parkinsonism: a systematic review and meta-analysis. Parkinsonism Relat Disord. (2012) 18:494–500. doi: 10.1016/j.parkreldis.2012.01.009
56. Treglia G, Stefanelli A, Cason E, Cocciolillo F, Di Giuda D, Giordano A. Diagnostic performance of iodine-123-metaiodobenzylguanidine scintigraphy in differential diagnosis between Parkinson's disease and multiple-system atrophy: a systematic review and a meta-analysis. Clin Neurol Neurosurg. (2011) 113:823–9. doi: 10.1016/j.clineuro.2011.09.004
57. Miyamoto T, Miyamoto M, Iwanami M, Hirata K. Follow-up study of cardiac 123I-MIBG scintigraphy in idiopathic REM sleep behavior disorder. Eur J Neurol. (2011) 18:1275–8. doi: 10.1111/j.1468-1331.2011.03392.x
58. Tsukita K, Tachibana N, Hamano T. Appropriate assessment method of 123I-MIBG myocardial scintigraphy for the diagnosis of Lewy body diseases and idiopathic REM sleep behavior disorder. J Neurol. (2020) 267:3248–57. doi: 10.1007/s00415-020-09992-0
59. Kashihara K, Imamura T, Shinya T. Cardiac 123I-MIBG uptake is reduced more markedly in patients with REM sleep behavior disorder than in those with early stage Parkinson's disease. Parkinsonism Relat Disord. (2010) 16:252–5. doi: 10.1016/j.parkreldis.2009.12.010
60. You S, Won KS, Kim KT, Lee HW, Cho YW. Cardiac autonomic dysfunction is associated with severity of REM sleep without atonia in isolated REM sleep behavior disorder. J Clin Med. (2021) 10:5414. doi: 10.3390/jcm10225414
61. Paglionico S, Labate A, Salsone M, Morelli M, Novellino F, Cascini G, et al. Involvement of cardiac sympathetic nerve endings in a patient with idiopathic RBD and intact nigrostriatal pathway. Parkinsonism Relat Disord. (2009) 15:789–91. doi: 10.1016/j.parkreldis.2009.03.008
62. Labate A, Salsone M, Novellino F, Morelli M, Sturniolo M, Gambardella A, et al. Combined use of cardiac m-i123-iodobenzylguanidine scintigraphy and 123I-fp-cit single photon emission computed tomography in older adults with rapid eye movement sleep behavior disorder. J Am Geriatr Soc. (2011) 59:928–9. doi: 10.1111/j.1532-5415.2011.03379.x
63. Fedorova TD, Knudsen K, Andersen KB, Horsager J, Skjærbæk C, Beier CP, et al. Imaging progressive peripheral and central dysfunction in isolated REM sleep behavior disorder after 3 years of follow-up. Parkinsonism Relat Disord. (2022) 101:99–104. doi: 10.1016/j.parkreldis.2022.07.005
64. Iranzo A, Fernandez-Arcos A, Tolosa E, Serradell M, Molinuevo JL, Valldeoriola F, et al. Neurodegenerative disorder risk in idiopathic REM sleep behavior disorder: study in 174 patients. PLoS ONE. (2014) 9:e89741. doi: 10.1371/journal.pone.0089741
65. Iranzo A, Valldeoriola F, Lomena F, Molinuevo JL, Serradell M, Salamero M, et al. Serial dopamine transporter imaging of nigrostriatal function in patients with idiopathic rapid-eye-movement sleep behavior disorder: a prospective study. Lancet Neurol. (2011) 10:797–805. doi: 10.1016/S1474-4422(11)70152-1
66. Iranzo A, Lomena F, Stockner H, Valldeoriola F, Vilaseca I, Salamero M, et al. Decreased striatal dopamine transporter uptake and substantia nigra hyperechogenicity as risk markers of synucleinopathy in patients with idiopathic rapid-eye-movement sleep behavior disorder: a prospective study [corrected]. Lancet Neurol. (2010) 9:1070–7. doi: 10.1016/S1474-4422(10)70216-7
67. Holtbernd F, Gagnon JF, Postuma RB, Ma Y, Tang CC, Feigin A, et al. Abnormal metabolic network activity in REM sleep behavior disorder. Neurology. (2014) 82:620–7. doi: 10.1212/WNL.0000000000000130
68. Kogan RV, Janzen A, Meles SK, Sittig E, Renken RJ, Geibl FF, et al. Four-year follow-up of [(18) F]fluorodeoxyglucose positron emission tomography-based Parkinson's disease-related pattern expression in 20 patients with isolated rapid eye movement sleep behavior disorder shows prodromal progression. Mov Disord. (2021) 36:230–5. doi: 10.1002/mds.28260
69. Arnaldi D, Chincarini A, Hu MT, Sonka K, Boeve B, Miyamoto T, et al. Dopaminergic imaging and clinical predictors for phenoconversion of REM sleep behavior disorder. Brain. (2021) 144:278–87. doi: 10.1093/brain/awaa365
Keywords: idiopathic rapid eye movement sleep behavior disorder (iRBD), neuromolecular imaging, alpha-synuclein, conversion, sleep
Citation: Geng C and Zhang H (2022) Research progress on neuromolecular imaging of REM sleep behavior disorder. Front. Neurol. 13:1009907. doi: 10.3389/fneur.2022.1009907
Received: 02 August 2022; Accepted: 21 September 2022;
Published: 10 October 2022.
Edited by:
Dario Arnaldi, University of Genoa, ItalyReviewed by:
Maurizio Versino, Humanitas Mater Domini, ItalyCopyright © 2022 Geng and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hongju Zhang, aG9uZ2p1ekBzaW5hLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.