
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol. , 10 November 2021
Sec. Neurotrauma
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.751736
 Sonja Stojanovski1,2
Sonja Stojanovski1,2 Shannon E. Scratch3,4,5
Shannon E. Scratch3,4,5 Benjamin T. Dunkley1,6,7
Benjamin T. Dunkley1,6,7 Russell Schachar1,8
Russell Schachar1,8 Anne L. Wheeler1,2*
Anne L. Wheeler1,2*Objective: To summarize existing knowledge about the characteristics of attention problems secondary to traumatic brain injuries (TBI) of all severities in children.
Methods: Computerized databases PubMed and PsychINFO and gray literature sources were used to identify relevant studies. Search terms were selected to identify original research examining new ADHD diagnosis or attention problems after TBI in children. Studies were included if they investigated any severity of TBI, assessed attention or ADHD after brain injury, investigated children as a primary or sub-analysis, and controlled for or excluded participants with preinjury ADHD or attention problems.
Results: Thirty-nine studies were included in the review. Studies examined the prevalence of and risk factors for new attention problems and ADHD following TBI in children as well as behavioral and neuropsychological factors associated with these attention problems. Studies report a wide range of prevalence rates of new ADHD diagnosis or attention problems after TBI. Evidence indicates that more severe injury, injury in early childhood, or preinjury adaptive functioning problems, increases the risk for new ADHD and attention problems after TBI and both sexes appear to be equally vulnerable. Further, literature suggests that cases of new ADHD often co-occurs with neuropsychiatric impairment in other domains. Identified gaps in our understanding of new attention problems and ADHD include if mild TBI, the most common type of injury, increases risk and what brain abnormalities are associated with the emergence of these problems.
Conclusion: This scoping review describes existing studies of new attention problems and ADHD following TBI in children and highlights important risk factors and comorbidities. Important future research directions are identified that will inform the extent of this outcome across TBI severities, its neural basis and points of intervention to minimize its impact.
Traumatic brain injury (TBI) is a major cause of acquired disability in children (1), and altogether accounts for over 700,000 emergency room visits annually in the United States (2). Importantly, emergency room visits underreport the true incidence of TBI as the majority of injuries are at the mild end of the spectrum (referred to as mild TBI or concussion) and children with mild injuries may seek medical attention from family doctors, other medical professions or not at all. The high prevalence of mild injuries is supported by surveys of high school students in which one in five adolescents report a lifetime history of concussion (3, 4).
TBI in children is associated with many different types of adverse outcomes as TBI to the developing brain impacts ongoing developmental processes (5). These include behavioral (6) and social problems (7), difficulties with academic achievement (8), and persistent cognitive deficits (9) that can occur across the spectrum of severities. The literature suggests a dose-response relationship between severity and outcome. Children with mild TBI typically recover within a month of injury (10) and the poorest outcomes, which may worsen over time, are seen in severe TBI (11, 12). Attention problems in particular are thought to be a common sequela of TBI (13). Attention supports higher cognitive thinking, learning, and problem-solving, and attention problems can negatively impact social interactions and the ability to function well at home and in school (14, 15). Attention problems that arise along with hyperactivity and impulsivity after TBI may contribute to new diagnoses of attention deficit hyperactivity disorder (ADHD) (16). The onset of ADHD symptoms (inattention, hyperactivity, and impulsivity) after an injury will hereafter referred to as secondary ADHD (SADHD) to be consistent with the majority of the existing literature. Importantly, the similarities and differences between primary and SADHD in youth are not fully understood and may represent very different disorders. This scoping review endeavors to begin to shed light on these differences by better characterizing SADHD which may inform the need for updated nomenclature. Studies have estimated that the rates of SADHD diagnoses may be as high as 46% in children hospitalized for TBI (17). Importantly, ADHD is also a risk factor for TBI (16), as children with ADHD are more likely to be injured, so disentangling preexisting ADHD from SADHD is important for understanding the etiology of attention problems and ADHD in children with TBI.
We identified six existing systematic reviews that included examinations of ADHD or attention problems after pediatric TBI (18–23). Generally, these reviews report that attention problems are among the most commonly reported problems in individuals with a history of brain injury. However, none of the existing reviews sought to explicitly characterize new attention problems or SADHD by accounting for preinjury attention problems or ADHD before the injury. Since the etiology of pre-existing ADHD and SADHD are likely to be different, assessing the existing literature that addresses SADHD specifically is necessary to guide future research that aims to determine its causes and provide treatment. A recent meta-analysis took the crucial step of controlling for or eliminating preinjury ADHD, but exclusively investigates whether there is an association between diagnosed ADHD and TBI (24). Given the dearth of synthesized literature capturing new attention problems, defined broadly, this review sought to formally assess what research evidence has been presented on the topic of attention problems that emerge after TBI in the literature to date. Systematic reviews and meta-analyses are important tools for addressing questions of prevalence or risk factors, however they have a narrow scope. Conversely, a scoping review framework was deemed most appropriate to achieve the goal of charting the data according to key general themes to identify knowledge gaps to guide focused research questions moving forward.
Here we review and synthesize the literature on attention problems acquired after TBI in children to summarize the existing knowledge base, as well as to identify areas requiring further research. We consider studies that examine attention problems specifically as well as those that assess SADHD diagnosis, though acknowledge that ADHD is a complex disorder that also includes problems with impulsivity and hyperactivity. Given the volume and scope of literature unearthed, extracted data was organized into categories which summarized: the prevalence of new attention problems and SADHD, injury and non-injury factors associated with risk for developing new attention problems as well as the behavioral presentation and associated neuropsychological impairments.
The approach for this scoping review was guided by a protocol drafted using the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension for scoping reviews (PRISMA-ScR) (25). The protocol which is available via the Open Science Framework (https://bit.ly/2YcIMYr) was submitted for registration in December 2020 to ensure transparency. To be included in the review, sources needed to formally assess symptoms of ADHD or measure attention problems following TBI in children (age 0–18 years).
We conducted a scoping review of scholarly and gray literature. To identify potentially relevant scholarly studies, PubMed and PsycINFO were searched from inception to June 2021. The final search strategy used the following search terms to search in title and abstract text in scholarly literature: “ADHD” or “attention deficit disorder” or “attention deficit hyperactivity” and “secondary” or “after” or “following” and “concussion” or “concussions” or “concussive” or “TBI” or “TBIs” or “mTBI” or “mTBIs” or “brain injury” or “brain injuries” or “brain damage” or “head impacts” (see Appendix S1 for the search strategy applied to PubMed). The study design filter was set to select only peer-reviewed journal articles in the PsycINFO search. The literature search was performed by SS, in consultation with AW. The final search results were exported into Zotero, before being imported into Covidence where duplicates were removed.
Additionally, gray literature, via vital statistics data, government surveillance data and reports, Centers for Disease Control and Prevention data, population censuses and surveys (i.e., national or provincial health survey data) and disease association websites were sought to decrease publication bias, and introduce alternative perspectives (26). Following the identification of relevant authorities these sources were searched through targeted website searching. Where targeted website searching turned up no sources advanced searching was applied to search the websites of the relevant authorities. The gray literature search applied the same search terms utilized for the scholarly literature search.
The literature search was performed by SSt and AW. To ensure consistency of screening 10 titles and abstracts were selected at random, independently screened and results were discussed to amend the screening protocol. All titles and abstracts were subsequently evaluated. Literature was retained for full-text search if it was: written in English, involved human participants, presented primary research, investigated any severity of TBI, assessed attention or ADHD after brain injury, and investigated children as a primary or sub-analysis. We required that studies controlled for or excluded participants with preinjury ADHD or attention problems to isolate attention outcomes secondary to TBI. Full texts of publications identified by the search and screening were independently assessed and retained for extraction if they contained the same features as were considered for the title and abstract screening. Disagreements on study selection were resolved by discussion if needed.
A data charting form was jointly developed by SSt and AW to determine which variables to extract and piloted on five randomly selected papers that passed full text screening. The two reviewers then iteratively updated the data-charting form to be applied to all eligible studies. Data charting was performed by SSt and verified by AW for accuracy, and inconsistencies were resolved through discussion. Specifically, data was abstracted on the following study characteristics: study design, study population, sample sizes, control groups, brain injury characteristics, and contextual factors (i.e., injury severity, age at injury, time since injury), how preinjury attention was controlled for, and how attention was assessed. Additionally, we abstracted data related to the following domains: prevalence, risk factors, behavioral features (including comorbidities), and neuropsychological characteristics associated with secondary attention problems and ADHD. Attention problems were defined according to thresholds for clinical significance in the individual scales used in each publication. We then grouped studies by the domain(s) of interest that they assessed and summarized the results of those analyses within each study.
After duplicates were removed, a total of 557 citations were identified from searches of electronic databases. Additionally, 675 citations were identified from searches of gray literature. Based on title and abstract, 1,158 were excluded and 101 full-text articles were retrieved and assessed for eligibility. Of these 13 were excluded for having no estimate of preinjury attention, 15 did not assess attention or ADHD, eight did not investigate children, seven studies included children but did not report results in children, six were not original research articles, seven did not control or exclude for preinjury attention or ADHD, three were excluded for assessing no fields of interest (prevalence, risk factor, behavioral features, or neuropsychological impairment), two did not investigate TBI, and three were excluded for being a duplicate. The remaining 39 studies were included in this review (Figure 1).
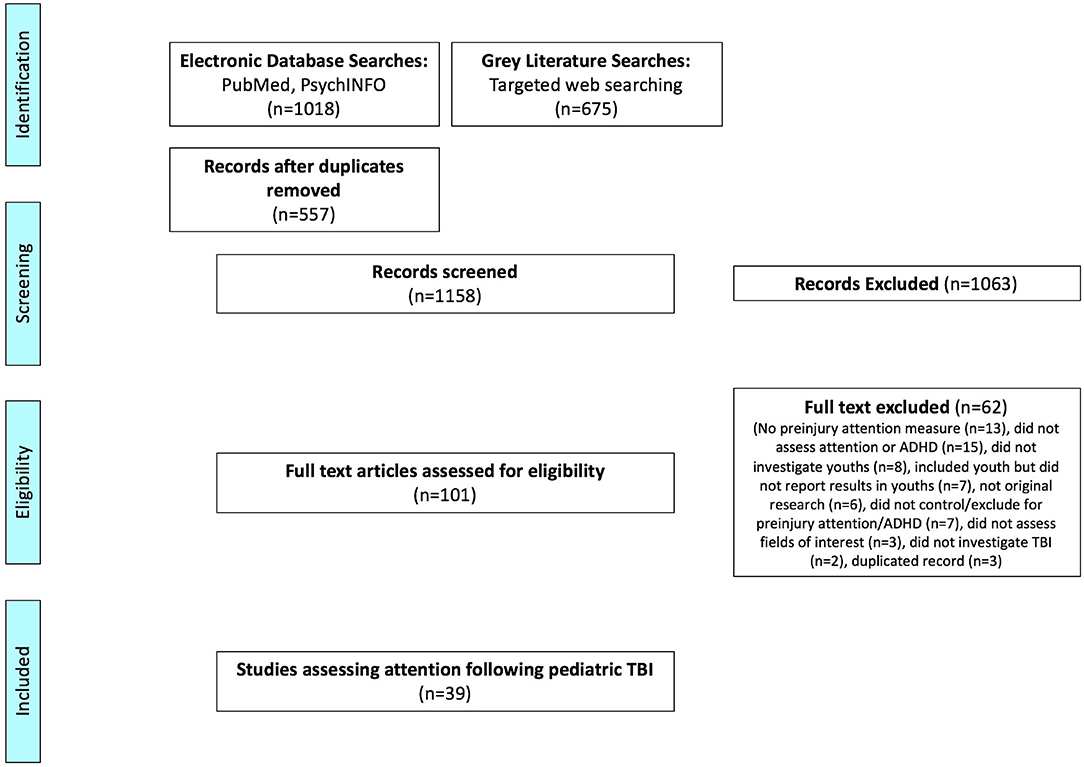
Figure 1. Flowchart article selection procedure.
An overview of the characteristics of each of the 39 studies is provided in Table 1. All 39 studies were derived from scholarly literature while no material from the gray literature search survived abstract and full text screening. Of the 39 studies more than half, 24, were prospective cohort studies of which two were birth cohorts. Twelve of the studies were retrospective studies, eight were cross-sectional, two were population cohorts, and two were chart reviews. Two studies combined prospective and retrospective cohorts. The majority of the studies (25) examined youth across the spectrum of TBI severity: mild, moderate, and severe TBI. Of these studies, five restricted the mild cases in their sample to those that were classified as “complicated mild,” meaning that there were positive findings on clinical neuroimaging assessments. Six studies included only moderate and severe cases of TBI, two included only severe TBI, and six included only mild TBI, including one that was a sample of children with a concussion. Nineteen studies included only youth with TBI whereas 20 studies also had a non-TBI comparison group, 10 were orthopedic injury controls and 10 had comparison groups that did not have a TBI. The range in age of injury of the subjects in each sample varied with more representation of older children and adolescents than younger children; only six studies included children injured in the first 3 years of life whereas 10 studies included older adolescents, age 16–18. The longest post-injury assessment time points in the studies ranged from 3 months to 20 years with six studies assessing youth less than a year after their injury, nine between 1 and 2 years, 11 between 2 and 5 years, nine between 5 and 10 years, and four longer than 10 years post-injury. The majority of study samples were hospitalized youth (27), whereas one study recruited only youth who visited the emergency department, three were recruited from TBI clinics and five studies included youth recruited from a combination of these settings. Only three studies examined population-based samples. Approximately half of the studies (20) assessed ADHD diagnosis as the attention outcome, whereas eight studies used an attention problem scale, and five studies used an attention task. Six studies used a combination of diagnosis, symptoms, scales, and tasks to assess attention. As this review includes only studies that assessed ADHD that is secondary to a TBI, studies used different approaches to account for preinjury attention. The majority of the studies (22) excluded youth with pre-injury (i.e., primary) diagnoses of ADHD. Eleven studies controlled for preinjury attention by including a retrospective assessment as a covariate in their statistical models, four studies examined youth with primary ADHD separately and two studies were birth cohorts which allowed them to establish the emergence of attention problems after injury in early childhood.
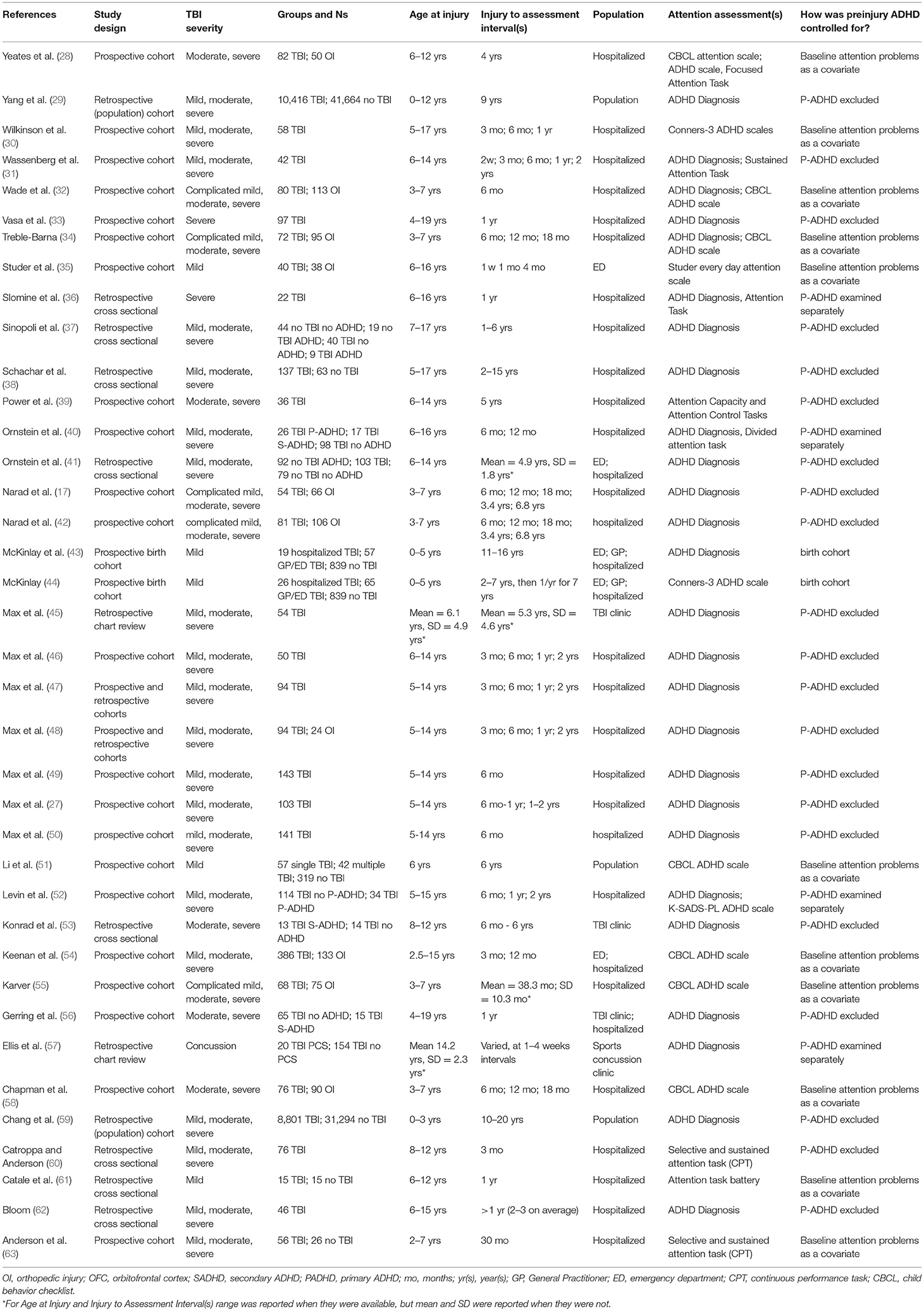
Table 1. Characteristics of included studies.
We consider studies that examine attention problems specifically as well as those that assess SADHD. Eighteen studies reported the prevalence of SADHD after TBI and these are reported at the longest measured timepoint for each study in Table 2. Two studies reported the prevalence of new attention problems after TBI and these are reported hereafter.
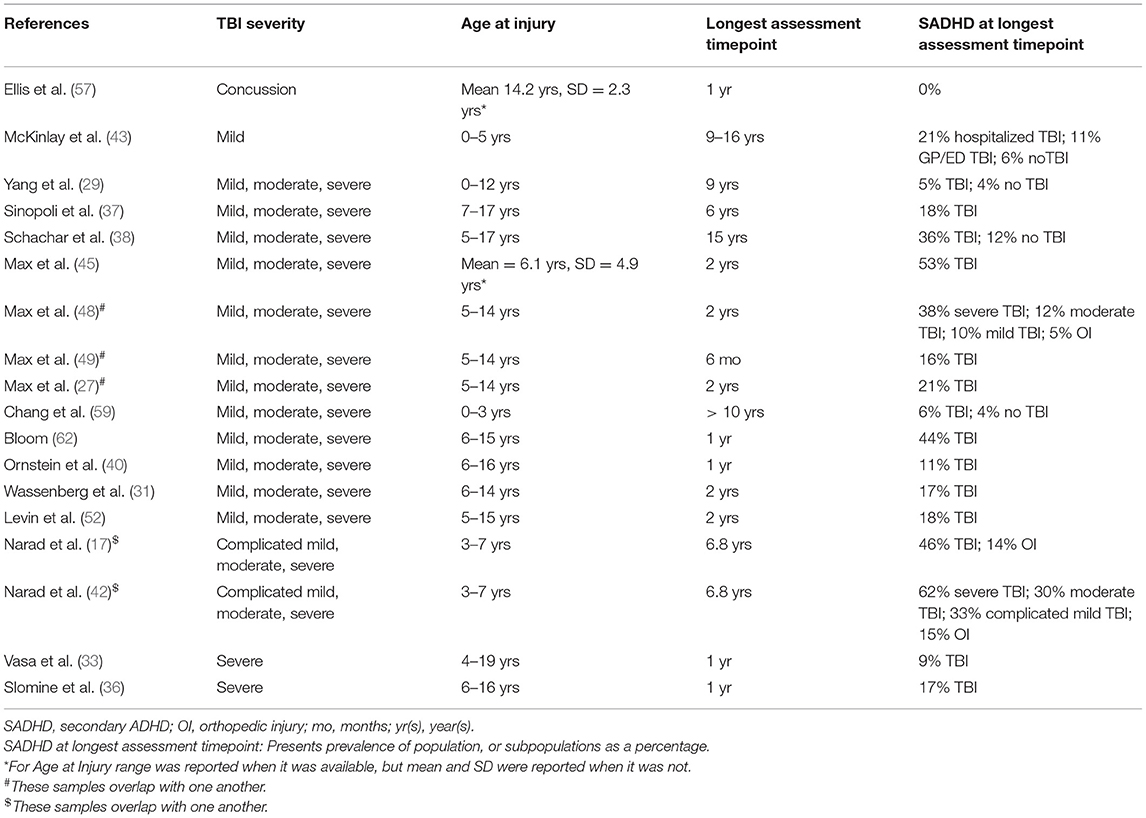
Table 2. Studies of prevalence.
Two of these studies reported prevalence at different time points post-injury from an overlapping sample (27, 49) and two studies reported a breakdown of prevalence by injury severity (42, 48) in samples that overlapped with samples from studies where they reported the prevalence for all severities (17, 27, 49). Nine studies included a control comparison group that allowed for statistical comparisons. In studies that examined the full range of TBI severity the prevalence of ADHD diagnosis after TBI ranged from 5 to 53%. Prevalence was lowest in population-based studies (29, 59), though notably, these rates were statistically higher than controls in those studies. Prevalence was highest in the one study that recruited from a TBI clinic, 53% (45). Prevalence ranged from 11 to 46% in hospitalized samples. Four studies examined either mild TBI only or reported prevalence in mild TBI specifically. A study in a concussion sample reported no new ADHD post injury (57), whereas, a prospective birth cohort of children who had sustained a mild injury in early childhood, reported that 11% of children who had been outpatients and 21% of children who had been inpatients at the time of injury were diagnosed with ADHD by mid-adolescence compared to 6% of children with no TBI (43). A mixed retrospective and prospective study reported that 10% of subjects with mild TBI developed ADHD compared to 5% of subjects with orthopedic injury (48) whereas a study in younger children reported 33% of subjects with complicated mild TBI developed ADHD compared to 15% of subjects with orthopedic injury (42). The same two studies reported prevalence of moderate TBI as 12% and severe TBI as 38% compared to 5% in orthopedic injury (48) in the first study, and 30% in moderate TBI and 62% in severe TBI compared to 15% in orthopedic injury (42) in the second study. Two studies examined severe TBI exclusively reporting 9% (33) and 17% (36) prevalence. Where statistical comparisons were possible the prevalence of SADHD after severe TBI was always significantly higher than the controls (28, 42, 48, 58), whereas this was not always the case for mild and moderate TBI (42, 48). Studies by Chapman et al. (58) and Yeates et al. (28) examined youth with moderate and severe TBI and reported clinically significant attention problems after severe injury (32 and 46%, respectively) compared to orthopedic injury controls (7 and 26%, respectively).
Twenty-five studies examined risk factors associated with children developing ADHD or new attention problems after TBI. We separated risk factors into injury-related and non-injury related and have summarized the significant and non-significant factors in Table 3.
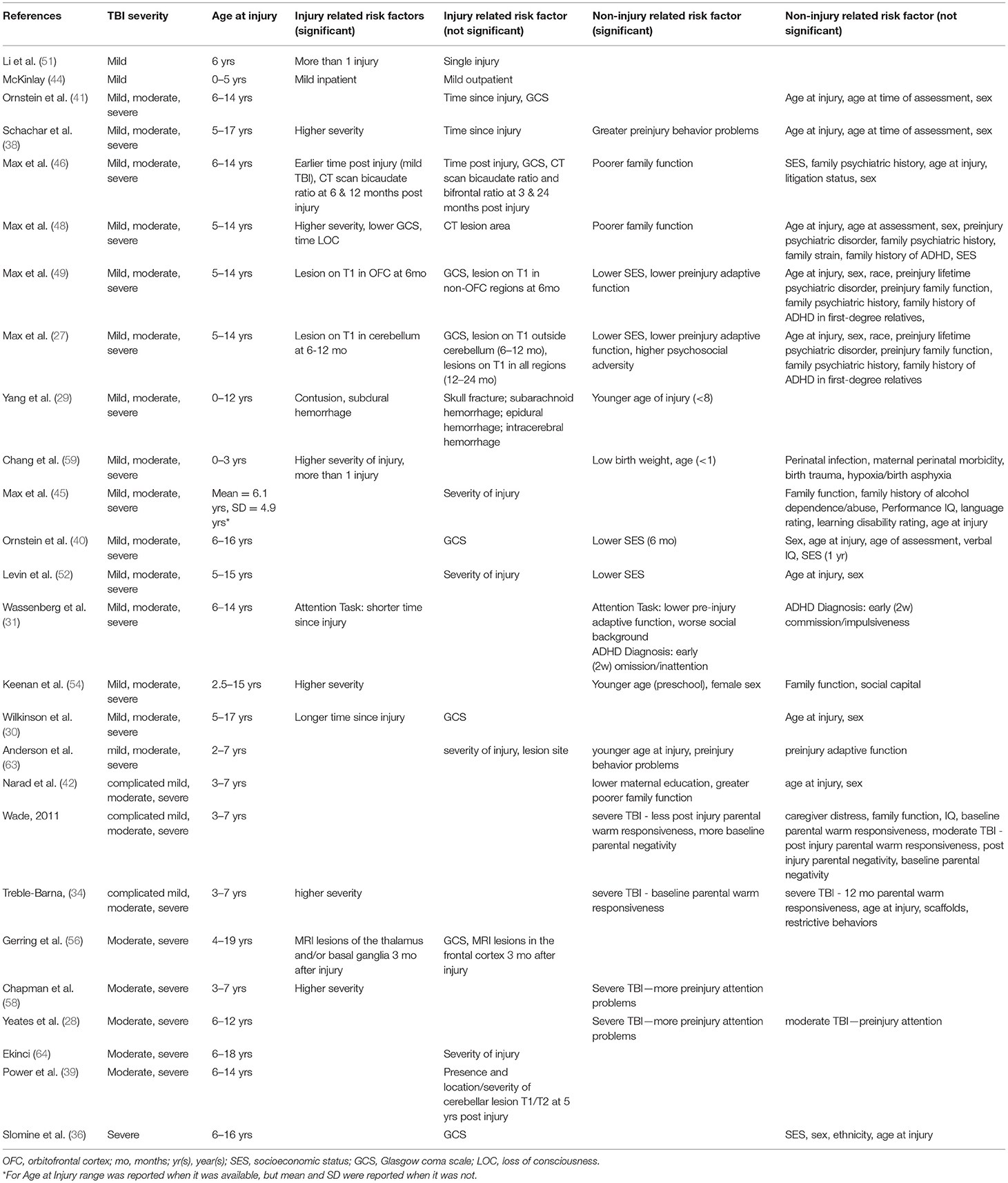
Table 3. Studies of risk factors.
As suggested by the prevalence rates grouped by severity, studies that examined severity as a moderating factor sometimes reported that increased severity based on grouping (mild, moderate, and severe) or Glasgow Coma Score (GCS), an index of severity based on the level of consciousness after an injury, was associated with higher rates of ADHD diagnosis or attention problems. However, an equal number of studies found that severity/GCS was not associated with SADHD or attention problems. Two studies examined the impact of having more than one injury and reported that this was associated with increased attention problems or SADHD diagnosis (51, 59). Only one study examined the loss of consciousness, reporting that increased time spent unconscious after the injury was associated with developing ADHD (48). Two prospective cohort studies with similar design reported an association between time since injury and attention problems, however with opposite directions of effect (30, 31). Two retrospective studies that assessed children many years after injury reported no effect of time since injury suggesting that attention problems do not get worse or improve over time after injury (38, 41).
The ability of neuroimaging to predict risk for subsequent new attention problems was investigated in several studies. Acute imaging with computerized tomography (CT) is common after injury and in their population study. Yang et al. (29) found that contusion and subdural hemorrhage, but not other types of hemorrhage or skull fracture were associated with subsequent ADHD diagnosis. A study by Max et al. (45) measured 2 frontal ratios and reported that bicaudate ratio, indicative of ventricular compression, was associated with attention problems when measured 6 and 12 months after injury but not at 3 months and 2 years post-injury. Another prospective cohort study by Max and colleagues employed magnetic resonance imaging (MRI) and demonstrated that lesions in the orbital frontal cortex 6 months after injury and the cerebellum 6–12 months after injury were associated with SADHD. However, these findings did not hold for the other time points examined and there were no relationships between lesions in other regions and SADHD (27). Another MRI study by Gerring et al. (56) found an association between lesions in the thalamus and basal ganglia 3 months after injury and SADHD, but no association with lesions in the frontal cortex. Power et al. (39) examined MRIs 5 years after injury and noted no relationship between cerebellar lesions or the location and severity of cerebral lesions and performance on attention tasks. Similarly, Anderson et al. (63) noted that there were no significant relationships between lesion site and attentional impairment after injury in a preschool-aged sample.
Most studies reported the influence of the age at the time of injury on the subsequent diagnosis of ADHD or new attention problems. For the most part, these studies did not report significant effects, however, the four studies that did report that younger children were at increased risk of attention problems were those that included the youngest children in their samples (29, 54, 59, 63). Of the 12 studies that examined sex as a possible risk factor all but one reported that there was no increased risk for attention problems for males or females (27, 30, 36, 38, 40–42, 46, 48, 49, 52). The study that did report an effect found that female sex increased the risk for attention problems (54). An equal number of studies found that socioeconomic status was a significant (27, 49, 52) or non-significant (36, 40, 45, 48) risk factor for new ADHD or attention problems. Worse family functioning was sometime (42, 45, 48) but not always (27, 32, 46, 49, 54) shown to be associated with ADHD or more attention problems. Wade et al. (32), assessed aspects of family function and reported that in severe but not moderate TBI more baseline parental negativity and less parental warmth and responsiveness were associated with more attention problems. The population study by Chang et al. (59) found that low birth weight but no other perinatal or birth factors increased the risk of developing ADHD after TBI. Studies that examined family psychiatric history (27, 45, 48, 49) or baseline IQ (32, 40, 46) did not find associations with subsequent attention problems following TBI. Lower preinjury adaptive functioning was reported as a significant factor in 3 out of 4 studies that assessed it (27, 31, 49, 63). Greater preinjury behavior problems (38, 63), as well as preinjury attention problems (28, 58) specifically in severe TBI, were consistently associated with secondary attention problems.
Thirteen studies reported behavioral features of SADHD, though five of these studies examined overlapping samples. These behavioral features are summarized in Table 4. All studies were prospective cohort studies of hospitalized samples. Two studies described inattention as the predominant feature of SADHD. One study noted that the inattention but not hyperactivity/impulsivity subscales of the Conners-3 ADHD scale increased pre to post injury (30) and another reported the inattentive ADHD subtype was the most common while hyperactive symptoms declined over time in children with SADHD (52). Children with SADHD were reported to have reduced communication skills and socialization skills compared to children that did not develop SADHD as well as children with primary ADHD. However, ratings of daily living skills were not significantly different between groups (40). In line with this study, another study also found that SADHD was associated with reduced adaptive functioning as well as intellectual function relative to children who did not develop ADHD after injury (48). Another study found that SADHD was associated with worse functional impairment and behavioral regulation but not metacognition in comparison with children with TBI that do not develop ADHD, as well as children with an orthopedic injury that develop SADHD (17). The emergence of SADHD has also been associated with co-occurring novel psychiatric problems including oppositional defiant disorder and conduct disorder (27, 45, 49), and affective lability (27, 33, 47–50). In the same sample, SADHD did not co-occur with new-onset anxiety disorders but did co-occur with new-onset depressive disorders at a 1 yr but not 6 mo or 2 years post injury (27, 49).
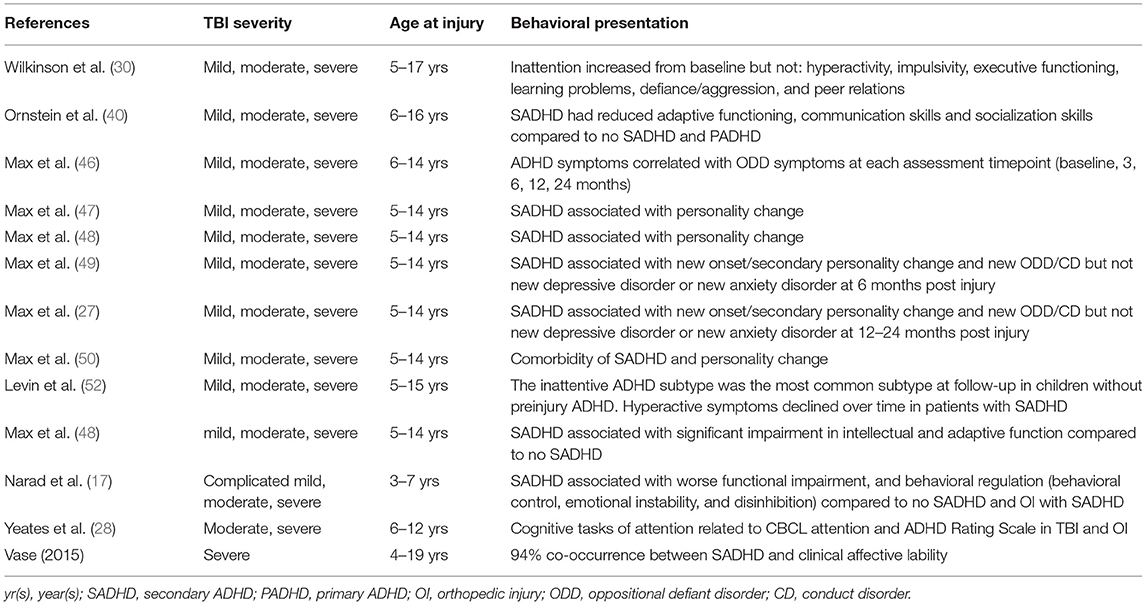
Table 4. Studies of associated behavioral features.
Unsurprisingly tests of attention revealed impaired function after TBI. One study found impaired selective attention after mild TBI (61), another found impaired focused attention after severe but not moderate TBI compared to controls (28) and two studies found that children with severe TBI perform more poorly than mild to moderate groups on a sustained attention task (60, 63). Children with SADHD performed worse on a divided attention task compared to children who did not develop ADHD after an injury as well as those that had primary ADHD (40). Though children with TBI were found to have deficits in inhibitory control processing in the stop-task similar to children with primary ADHD (53), there is mixed evidence as to if children with SADHD are especially impaired (37, 38, 40, 41, 53). New post-injury attention problems in children were associated with poorer verbal learning (35), short term memory (36), and working memory as well as planning ability (40). These neuropsychological impairments are summarized in Table 5.
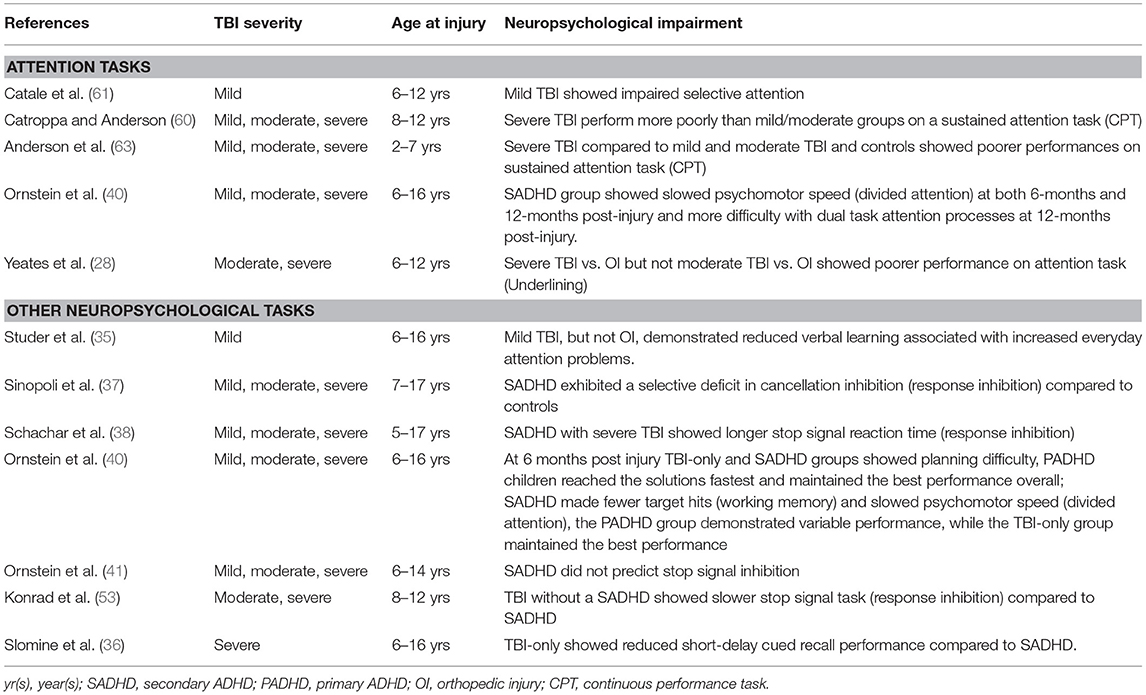
Table 5. Studies of associated neuropsychological impairments.
This scoping review summarized the state of the literature that assesses new-onset ADHD and attention problems that emerge after TBI in children and adolescents. Identified literature was organized into the following conceptual domains: prevalence, risk factors (divided into injury-related and non-injury related factors), associated behavioral features, and neuropsychological impairments.
The findings from the scoping review supports the increased prevalence of new clinically significant attention problems and SADHD following injury in severe TBI (28, 42, 48, 58), consistent with a recent meta-analysis of SADHD (24). The review also supports that there is a higher risk of new attention problems and SADHD in children and youth with low preinjury adaptive functioning (27, 31, 49, 63), and when the injury occurs in early childhood (<7 years of age at time of injury) (29, 42, 54, 59, 63). Evidence suggests that both sexes are equally vulnerable (27, 30, 36, 38, 40–42, 46, 48, 49, 52), and poor family functioning was sometimes (42, 45, 48) but not always (27, 32, 46, 49, 54) a risk factor for SADHD and new attention problems. These conclusions are supported by a recent review that specifically examined biopsychosocial factors associated with attention problems in youth with TBI (23). Due to the lack of topical limitation of a scoping review framework the current review also found evidence to support that commonly concurrent neuropsychological characteristics and behavioral presentation include: (1) co-occurring novel psychiatric problems including ODD, CD (27, 45, 49), and affective lability (27, 33, 47–50), (2) and reductions in daily functioning (communication, socialization, and adaptive functioning) (17, 40, 48). Furthermore, this scoping review identified mixed evidence as to: (1) the prevalence of new attention problems in mild TBI, (2) if children with SADHD are especially neuropsychologically impaired (37, 38, 40, 41, 53), (3) the predominant class of attentional impairment in youth with TBI due to inconsistent outcome measures (28, 60, 63), and (4) the role of brain lesions in attention problems after injury.
A wide range of prevalences were reported for SADHD and new attention problems after TBI which is likely influenced by the presence of identified risk factors in different study samples. Evidence from identified studies suggests that new attention problems and ADHD diagnoses may be more common when the injury occurs in early childhood (29, 42, 54, 59, 63). Children injured in early childhood may be most vulnerable to developing new attention problems after injury. This may be due to damage to brain circuitry that is responsible for basic attentional processes in early development or injury that prevents the future proper development of later maturing attentional processes (65, 66). Experiencing multiple injuries was associated with elevated risk for attention problems in the two reviewed studies that examined this and it should be an area for further study given that repeat injuries are common in children who play sports.
Though the prevalence of primary (i.e., developmental) ADHD is higher in males than females [3:1 (67)] this does not appear to be the case for ADHD secondary to TBI as the majority of studies reported no influence of sex. There is a need for additional research to determine the circumstances when mild TBI is a risk factor for secondary attention problems and ADHD as prevalence reported in these subjects was particularly varied. The majority of the reviewed studies included hospitalized children suggesting that they included more severe forms of mild TBI or children who suffered from other extensive injuries. This points to an underrepresentation of mild cases that are representative of typical mild cases of TBI that are seen in an emergency room, assessed by their general practitioner, or who receive no initial medical attention.
Studies that examined whether specific types of brain pathology detected with brain imaging are associated with new attention problems are difficult to synthesize due to their varied methodology. Specifically, the ability to meaningfully consider risk factors identified through neuroimaging is confounded by differing imaging modalities, time since injury, the severity of the injury, and population type in the identified studies. Some evidence supports the usefulness of imaging performed acutely after injury to inform the child's outcome including attention problems (27, 49, 56). However, one study reported acute imaging as a non-significant risk factor (48) and all positive studies were in hospitalized youth which brings into question the generalizability to those with mild injury. Currently, CT is most often performed to assess hematomas, brain swelling, and skull fracture though it is not recommended for mild injury to avoid unnecessary radiation exposure in children. MRI, which does not involve radiation, is more sensitive to certain types of pathology such as microhemorrhage, contusion, and gliosis, as well as axonal injury. MRI may be a more sensitive tool for prognosis through the detection of brain changes after TBI. However, there is currently no agreed-upon schema for coding of MRI findings used in clinical practice. It may be the case that diffuse axonal injury (68, 69), known to result from TBI, disrupts the functional integrity of widely distributed neural pathways that are involved in attention processes (70) and is associated with new attention problems, but this has not been assessed. Advanced MRI methods such as diffusion-weighted imaging that is sensitive to microscopic injury in the brain would be suitable diffuse axonal injury in attention circuits in future studies. Similarly, we did not identify any existing studies that use functional imaging (EEG, MEG, or fMRI) to examine circuit functional alterations that may predict new attention problems after injury.
Some studies include a comparison group with primary ADHD which could be informative for distinguishing related factors and may have implications for how the ADHD is managed. Whether SADHD mimics the primary ADHD endophenotype or not may inform whether these are separate disorders with different underlying mechanisms. The studies reviewed here demonstrated no associations between risk for secondary attention problems and family psychiatric history, unlike primary ADHD (71). This is consistent with a lack of a genetic association seen between genetic risk variants associated with primary ADHD and ADHD associated with TBI (72). The reviewed studies suggest that SADHD is associated with more debilitating outcomes (i.e., comorbid disorders, behavioral and functional impairments, and cognitive impairment) in some cases compared to primary ADHD. Of note treatment studies reviewed elsewhere suggest that treatment approaches that are beneficial for primary ADHD in children, methylphenidate, in particular, are also beneficial for treating SADHD (21, 22). Together these studies suggest that although attention problems that emerge after TBI may have separate underlying mechanisms than those that result from primary ADHD, existing treatment may be able to relieve symptoms through common overriding mechanisms.
This review has several important limitations. In general, there was a large amount of variability in the measures to assess similar study variables and outcomes which supports calls for the collection of TBI common data elements across all methodologies to more easily compare studies and draw conclusions (73). In this review, attention was assessed via diagnosis of ADHD as well as measures of attention (questionnaire and objective). The criteria for diagnosis are discrete, while measurements of self or parent-reported attention problems are heterogeneous in terms of their interpretation and reliability. This imposes limitations on the ability to characterize attention problems following TBI since the threshold on labeling behaviors as pathological is likely inconsistent. Another important source of methodological heterogeneity was that only half of the studies examined included a non-TBI comparison group, and half of these were an orthopedic injury group. The selection of an appropriate non-TBI comparison group controls for factors that predispose children to injury and are associated with the injury and recovery process. These factors are important to consider as they may influence the detection of the emergence of attention problems after TBI in children. Importantly, this review sought to explicitly examine new attention problems and SADHD however retrospective recall of preinjury functioning is potentially confounded. Recall can be heavily influenced by retrospective biases (26). Additionally, as per scoping review methodology, the quality of the included studies was not assessed. Therefore, there is a potential risk of bias inherent from included studies with potentially low-quality methodological design which limits the interpretations that can be made from this review. Finally, due to the large age range included in the majority of identified studies we were not able to break down the results by restricted age cohorts in order to identify age as a moderating factor between studies.
In summary, this scoping review synthesized a sizable body of evidence about the effects of TBI in childhood and adolescence on the emergence of new ADHD and attention problems. The results suggest that children that experience TBI are at increased risk for SADHD and new attention problems and that several injury and non-injury factors such as severity, the number of injuries, and age at injury may predict this risk. However, the evidence in some areas is lacking. This review identified that younger age of injury was a risk factor for new attention problems or SADHD within studies that included the youngest children (<7 years), however most studies included children across a large age range. Future studies should examine new attention problems in more restricted age cohorts that are expected to differ in their recovery from TBI due to many important neurodevelopmental changes take place across childhood. At the severe end of the TBI spectrum where the association with an increased risk for attention problems and SADHD is noted in this review and elsewhere (24) future clinical intervention studies can consider exploring psychosocial factors identified in this review. For example, interventions focused on family functioning and parental style, which have been associated with more attention problems (42, 45, 48), may prevent or attenuate the development of attention problems following injury. As even subclinical attention problems can affect learning and socializing in children the field would benefit from large studies of representative mild and moderate cases of TBI that measure attention problems dimensionally. These future studies should control for dimensional measures of preinjury attention problems and include appropriate control groups to understand the true risk for new attention problems following mild TBI. Further, longitudinal studies of representative cases will allow for the investigation of prevalence at various timepoints following injury to establish how often and in whom this type of impairment persists. Across severities a deeper understanding of the etiology of new attention problems and SADHD following brain injury can be achieved from the integration of advanced brain imaging. Functional and structural neuroimaging studies can shed light on the specific circuits that are disrupted by injury and cause attention problems. In addition to determining if or when mild TBI promotes new attention problems in children, these studies will be able to inform the mechanism by which these attention difficulties emerge and potentially distinguish them from the large existing body of literature on primary ADHD (74, 75). Evidence for prevalence, risk factors and characteristics of attention problems that develop after pediatric TBI is of interest to scientists as further understanding of the unique etiology of secondary attention problems will lead to knowledge of the mechanisms of symptom generation. This information may eventually be relevant to clinicians who treat these patients as this knowledge can aid the detection of attention problems and inform its management.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
SS, AW, and RS contributed to conception and design of the study. SS and AW performed data screening and extraction and wrote the first draft of the manuscript. All authors contributed to the interpretation of the data, manuscript revision, read, and approved the submitted version.
SS was supported by a Restracomp Scholarship from the Hospital for Sick Children and the Ontario Graduate Scholarship. AW was supported by the Scottish Rite Charitable Foundation of Canada.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.751736/full#supplementary-material
1. Shi J, Xiang H, Wheeler K, Smith GA, Stallones L, Groner J, et al. Costs, mortality likelihood and outcomes of hospitalized US children with traumatic brain injuries. Brain Inj. (2009) 23:602–11. doi: 10.1080/02699050903014907
2. Taylor CA, Bell JM, Breiding MJ, Xu L. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths—United States, 2007 and 2013. MMWR Surveill Summ. (2017) 66:1–16. doi: 10.15585/mmwr.ss6609a1
3. Veliz P, McCabe SE, Eckner JT, Schulenberg JE. Prevalence of concussion among US adolescents and correlated factors. J Am Med Assoc. (2017) 318:1180–2. doi: 10.1001/jama.2017.9087
4. Ilie G, Boak A, Adlaf EM, Asbridge M, Cusimano MD. Prevalence and correlates of traumatic brain injuries among adolescents. J Am Med Assoc. (2013) 309:2550–2. doi: 10.1001/jama.2013.6750
5. Choe MC, Babikian T, DiFiori J, Hovda DA, Giza CC. A pediatric perspective on concussion pathophysiology. Curr Opin Pediatr. (2012) 24:689–95. doi: 10.1097/MOP.0b013e32835a1a44
6. Blennow K, Hardy J, Zetterberg H. The neuropathology and neurobiology of traumatic brain injury. Neuron. (2012) 76:886–99. doi: 10.1016/j.neuron.2012.11.021
7. Ganesalingam K, Yeates KO, Sanson A, Anderson V. Social problem-solving skills following childhood traumatic brain injury and its association with self-regulation and social and behavioural functioning. J Neuropsychol. (2007) 1:149–70. doi: 10.1348/174866407X185300
8. Catroppa C, Anderson VA, Muscara F, Morse SA, Haritou F, Rosenfeld JV, et al. Educational skills: long-term outcome and predictors following paediatric traumatic brain injury. Neuropsychol Rehabil. (2009) 19:716–32. doi: 10.1080/09602010902732868
9. Beauchamp MH, Anderson V. Cognitive and psychopathological sequelae of pediatric traumatic brain injury. Handb Clin Neurol. (2013) 112:913–20. doi: 10.1016/B978-0-444-52910-7.00013-1
10. Zemek R, Barrowman N, Freedman SB, Gravel J, Gagnon I, McGahern C, et al. Clinical risk score for persistent postconcussion symptoms among children with acute concussion in the ED. J Am Med Assoc. (2016) 315:1014–25. doi: 10.1001/jama.2016.1203
11. Catroppa C, Anderson VA, Morse SA, Haritou F, Rosenfeld JV. Outcome and predictors of functional recovery 5 years following pediatric traumatic brain injury (TBI). J Pediatr Psychol. (2008) 33:707–18. doi: 10.1093/jpepsy/jsn006
12. Schrieff-Elson LE, Steenkamp N, Hendricks MIK, Thomas GF, Rohlwink UK. Local and global challenges in pediatric traumatic brain injury outcome and rehabilitation assessment. Childs Nerv Syst. (2017) 33:1775–84. doi: 10.1007/s00381-017-3527-6
13. Kaufmann PM, Fletcher JM, Levin HS, Miner ME, Ewing-Cobbs L. Attentional disturbance after pediatric closed head injury. J Child Neurol. (1993) 8:348–53. doi: 10.1177/088307389300800410
14. Gioia GA, Isquith PK. Ecological assessment of executive function in traumatic brain injury. Dev Neuropsychol. (2004) 25:135–58. doi: 10.1207/s15326942dn2501&2_8
15. Levin HS, Hanten G. Executive functions after traumatic brain injury in children. Pediatr Neurol. (2005) 33:79–93. doi: 10.1016/j.pediatrneurol.2005.02.002
16. Schachar RJ, Park LS, Dennis M. Mental health implications of traumatic brain injury (TBI) in children and youth. J Can Acad Child Adolesc Psychiatry. (2015) 24:100–8.
17. Narad ME, Riemersma J, Wade SL, Smith-Paine J, Morrison P, Taylor HG, et al. Impact of secondary ADHD on long-term outcomes after early childhood traumatic brain injury. J Head Trauma Rehabil. (2020) 35:E271–9. doi: 10.1097/HTR.0000000000000550
18. Li L, Liu J. The effect of pediatric traumatic brain injury on behavioral outcomes: a systematic review. Dev Med Child Neurol. (2013) 55:37–45. doi: 10.1111/j.1469-8749.2012.04414.x
19. Emery CA, Barlow KM, Brooks BL, Max JE, Villavicencio-Requis A, Gnanakumar V, et al. A systematic review of psychiatric, psychological, and behavioural outcomes following mild traumatic brain injury in children and adolescents. Can J Psychiatry. (2016) 61:259–69. doi: 10.1177/0706743716643741
20. Adeyemo BO, Biederman J, Zafonte R, Kagan E, Spencer TJ, Uchida M, et al. Mild traumatic brain injury and ADHD: a systematic review of the literature and meta-analysis. J Atten Disord. (2014) 18:576–84. doi: 10.1177/1087054714543371
21. Backeljauw B, Kurowski BG. Interventions for attention problems after pediatric traumatic brain injury: what is the evidence? PM R. (2014) 6:814–24. doi: 10.1016/j.pmrj.2014.04.004
22. Jin C, Schachar R. Methylphenidate treatment of attention-deficit/hyperactivity disorder secondary to traumatic brain injury: a critical appraisal of treatment studies. CNS Spectr. (2004) 9:217–26. doi: 10.1017/S1092852900009019
23. Bolikal PD, Narad M, Raj S, Kennelly M, Kurowski BG. Biopsychosocial factors associated with attention problems in children after traumatic brain injury: a systematic review. Am J Phys Med Rehabil. (2021) 100:215–28. doi: 10.1097/PHM.0000000000001643
24. Asarnow RF, Newman N, Weiss RE, Su E. Association of attention-deficit/hyperactivity disorder diagnoses with pediatric traumatic brain injury: a meta-analysis. J Am Med Assoc Pediatr. (2021) 175:1009–16. doi: 10.1001/jamapediatrics.2021.2033
25. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
26. Brooks BL, Kadoura B, Turley B, Crawford S, Mikrogianakis A, Barlow KM. Perception of recovery after pediatric mild traumatic brain injury is influenced by the “good old days” bias: tangible implications for clinical practice and outcomes research. Arch Clin Neuropsychol. (2014) 29:186–93. doi: 10.1093/arclin/act083
27. Max JE, Schachar RJ, Levin HS, Ewing-Cobbs L, Chapman SB, Dennis M, et al. Predictors of attention-deficit/hyperactivity disorder within 6 months after pediatric traumatic brain injury. J Am Acad Child Adolesc Psychiatry. (2005) 44:1032–40. doi: 10.1097/01.chi.0000173293.05817.b1
28. Yeates KO, Armstrong K, Janusz J, Taylor HG, Wade S, Stancin T, et al. Long-term attention problems in children with traumatic brain injury. J Am Acad Child Adolesc Psychiatry. (2005) 44:574–84. doi: 10.1097/01.chi.0000159947.50523.64
29. Yang L, Huang C, Chiu W, Huang L, Lo W, Wang J. Association of traumatic brain injury in childhood and attention-deficit/hyperactivity disorder: a population-based study. Pediatr Res. (2016) 80:356–62. doi: 10.1038/pr.2016.85
30. Wilkinson AA, Simic N, Frndova H, Taylor MJ, Choong K, Fraser D, et al. Serum biomarkers help predict attention problems in critically ill children with traumatic brain injury. Pediatr Crit Care Med. (2016) 17:638–48. doi: 10.1097/PCC.0000000000000752
31. Wassenberg R, Max JE, Lindgren SD, Schatz A. Sustained attention in children and adolescents after traumatic brain injury: relation to severity of injury, adaptive functioning, ADHD and social background. Brain Inj. (2004) 18:751–64. doi: 10.1080/02699050410001671775
32. Wade SL, Cassedy A, Walz NC, Taylor HG, Stancin T, Yeates KO. The relationship of parental warm responsiveness and negativity to emerging behavior problems following traumatic brain injury in young children. Dev Psychol. (2011) 47:119–33. doi: 10.1037/a0021028
33. Vasa RA, Suskauer SJ, Thorn JM, Kalb L, Grados MA, Slomine BS, et al. Prevalence and predictors of affective lability after pediatric traumatic brain injury. In: Brain Inj. (2015) 8:309–19. doi: 10.3109/02699052.2015.1005670
34. Treble-Barna A, Zang H, Zhang N, Taylor HG, Stancin T, Yeates KO, et al. Observed parent behaviors as time-varying moderators of problem behaviors following traumatic brain injury in young children. Dev Psychol. (2016) 52:1777–92. doi: 10.1037/dev0000208
35. Studer M, Goeggel Simonetti B, Joeris A, Margelisch K, Steinlin M, Roebers CM, et al. Post-concussive symptoms and neuropsychological performance in the post-acute period following pediatric mild traumatic brain injury. J Int Neuropsychol Soc. (2014) 20:982–93. doi: 10.1017/S1355617714000927
36. Slomine BS, Salorio CF, Grados MA, Vasa RA, Christensen JR, Gerring JP. Differences in attention, executive functioning, and memory in children with and without ADHD after severe traumatic brain injury. J Int Neuropsychol Soc. (2005) 11:645–53. doi: 10.1017/S1355617705050769
37. Sinopoli K, Schachar R, Dennis M. Traumatic brain injury and secondary attention-deficit/ hyperactivity disorder in children and adolescents: the effect of reward on inhibitory control. J Clin Exp Neuropsychol. (2011) 33:805–19. doi: 10.1080/13803395.2011.562864
38. Schachar R, Levin HS, Max JE, Purvis K, Chen S. Attention deficit hyperactivity disorder symptoms and response inhibition after closed head injury in children: do preinjury behavior and injury severity predict outcome? Dev Neuropsychol. (2004) 25:179–98. doi: 10.1207/s15326942dn2501&2_10
39. Power T, Catroppa C, Coleman L, Ditchfield M, Anderson V. Do lesion site and severity predict deficits in attentional control after preschool traumatic brain injury (TBI)? Brain Inj. (2007) 21:279–92. doi: 10.1080/02699050701253095
40. Ornstein TJ, Sagar S, Schachar RJ, Ewing-Cobbs L, Chapman SB, Dennis M, et al. Neuropsychological performance of youth with secondary attention-deficit/hyperactivity disorder 6- and 12-months after traumatic brain injury. J Int Neuropsychol Soc. (2014) 20:971–81. doi: 10.1017/S1355617714000903
41. Ornstein TJ, Max JE, Schachar R, Dennis M, Barnes M, Ewing-Cobbs L, et al. Response inhibition in children with and without ADHD after traumatic brain injury. J Neuropsychol. (2013) 7:1–11. doi: 10.1111/j.1748-6653.2012.02027.x
42. Narad ME, Kennelly M, Zhang N, Wade SL, Yeates KO, Taylor HG, et al. Secondary attention-deficit/hyperactivity disorder in children and adolescents 5 to 10 years after traumatic brain injury. J Am Med Assoc Pediatr. (2018) 172:437–43. doi: 10.1001/jamapediatrics.2017.5746
43. McKinlay A, Grace R, Horwood J, Fergusson D, MacFarlane M. Adolescent psychiatric symptoms following preschool childhood mild traumatic brain injury: evidence from a birth cohort. J Head Trauma Rehabil. (2009) 24:221–7. doi: 10.1097/HTR.0b013e3181a40590
44. McKinlay A, Grace RC, Horwood LJ, Fergusson DM, MacFarlane MR. Long-term behavioural outcomes of pre-school mild traumatic brain injury. Child Care Health Dev. (2010) 36:22–30. doi: 10.1111/j.1365-2214.2009.00947.x
45. Max JE, Arndt S, Castillo CS, Bokura H, Robin DA, Lindgren SD, et al. Attention-deficit hyperactivity symptomatology after traumatic brain injury: a prospective study. J Am Acad Child Adolesc Psychiatry. (1998) 37:841–7. doi: 10.1097/00004583-199808000-00014
46. Max JE, Lindgren SD, Knutson C, Pearson CS, Ihrig D, Welborn A. Child and adolescent traumatic brain injury: correlates of disruptive behaviour disorders. Brain Inj. (1998) 12:41–52. doi: 10.1080/026990598122845
47. Max JE, Koele SL, Castillo CC, Lindgren SD, Arndt S, Bokura H, et al. Personality change disorder in children and adolescents following traumatic brain injury. J Int Neuropsychol Soc. (2000) 6:279–89. doi: 10.1017/S1355617700633039
48. Max JE, Lansing AE, Koele SL, Castillo CS, Bokura H, Schachar R, et al. Attention deficit hyperactivity disorder in children and adolescents following traumatic brain injury. Dev Neuropsychol. (2004) 25:159–77. doi: 10.1207/s15326942dn2501&2_9
49. Max JE, Schachar RJ, Levin HS, Ewing-Cobbs L, Chapman SB, Dennis M, et al. Predictors of secondary attention-deficit/hyperactivity disorder in children and adolescents 6 to 24 months after traumatic brain injury. J Am Acad Child Adolesc Psychiatry. (2005) 44:1041–9. doi: 10.1097/01.chi.0000173292.05817.f8
50. Max JE, Wilde EA, Bigler ED, Hanten G, Dennis M, Schachar RJ, et al. Personality change due to traumatic brain injury in children and adolescents: neurocognitive correlates. J Neuropsychiatry Clin Neurosci. (2015) 27:272–9. doi: 10.1176/appi.neuropsych.15030073
51. Li L, Li Y, McDonald C, Liu J. Parent-reported mild head injury history in children: long-term effects on attention-deficit hyperactivity disorder. Glob Pediatr Health. (2018) 5:2333794X18756465. doi: 10.1177/2333794X18756465
52. Levin H, Hanten G, Max J, Li X, Swank P, Ewing-Cobbs L, et al. Symptoms of attention-deficit/hyperactivity disorder following traumatic brain injury in children. J Dev Behav Pediatr. (2007) 28:108–18. doi: 10.1097/01.DBP.0000267559.26576.cd
53. Konrad K, Guaggel S, Scholl M. Inhibitory control in children with traumatic brain injury (TBI) and children with attention deficit/ hyperactivity disorder (ADHD). Brain Inj. (2000) 10:859–75. doi: 10.1080/026990500445691
54. Keenan HT, Clark AE, Holubkov R, Cox CS, Ewing-Cobbs L. Psychosocial and executive function recovery trajectories one year after pediatric traumatic brain injury: the influence of age and injury severity. J Neurotrauma. (2018) 35:286–96. doi: 10.1089/neu.2017.5265
55. Karver CL, Wade SL, Cassedy A, Taylor HG, Stancin T, Yeates KO, et al. Age at injury and long-term behavior problems after traumatic brain injury in young children. Rehabil Psychol. (2012) 57:256–65. doi: 10.1037/a0029522
56. Gerring J, Brady K, Chen A, Quinn C, Herskovits E, Bandeen-Roche K, et al. Neuroimaging variables related to development of Secondary Attention Deficit Hyperactivity Disorder after closed head injury in children and adolescents. Brain Inj. (2000) 14:205–18. doi: 10.1080/026990500120682
57. Ellis MJ, Ritchie LJ, Koltek M, Hosain S, Cordingley D, Chu S, et al. Psychiatric outcomes after pediatric sports-related concussion. J Neurosurg Pediatr. (2015) 16:709–18. doi: 10.3171/2015.5.PEDS15220
58. Chapman LA, Wade SL, Walz NC, Taylor HG, Stancin T, Yeates KO. Clinically significant behavior problems during the initial 18 months following early childhood traumatic brain injury. Rehabil Psychol. (2010) 55:48–57. doi: 10.1037/a0018418
59. Chang HK, Hsu JW, Wu JC, Huang KL, Chang HC, Bai YM, et al. Traumatic brain injury in early childhood and risk of attention-deficit/hyperactivity disorder and autism spectrum disorder: a nationwide longitudinal study. J Clin Psychiatry. (2018) 79:11857. doi: 10.4088/JCP.17m11857
60. Catroppa C, Anderson V. Attentional skills in the acute phase following pediatric traumatic brain injury. Child Neuropsychol. (1999) 5:251–64. doi: 10.1076/0929-7049(199912)05:04;1-R;FT251
61. Catale C, Marique P, Closset A, Meulemans T. Attentional and executive functioning following mild traumatic brain injury in children using the Test for Attentional Performance (TAP) battery. J Clin Exp Neuropsychol. (2009) 31:331–8. doi: 10.1080/13803390802134616
62. Bloom DR, Levin HS, Ewing-Cobbs L, Saunders AE, Song J, Fletcher JM, et al. Lifetime and novel psychiatric disorders after pediatric traumatic brain injury. J Am Acad Child Adolesc Psychiatry (2001) 40:572–9. doi: 10.1097/00004583-200105000-00017
63. Anderson V, Catroppa C, Morse S, Haritou F, Rosenfeld J. Attentional and processing skills following traumatic brain injury in early childhood. Brain Inj. (2005) 19:699–710. doi: 10.1080/02699050400025281
64. Ekinci O, Direk M7, Gunes S, Teke H, Ekinci N, Y?ld?r?m F, et al. Short-term efficacy and tolerability of methylphenidate in children with traumatic brain injury and attention problems. Brain Dev. (2017) 39:327–36. doi: 10.1016/j.braindev.2016.11.005
65. Klenberg L, Korkman M, Lahti-Nuuttila P. Differential development of attention and executive functions in 3- to 12-year-old Finnish children. Dev Neuropsychol. (2001) 20:407–28. doi: 10.1207/S15326942DN2001_6
66. Ewing-Cobbs L, Prasad MR, Landry SH, Kramer L, DeLeon R. Executive functions following traumatic brain injury in young children: a preliminary analysis. Dev Neuropsychol. (2004) 26:487–512. doi: 10.1207/s15326942dn2601_7
67. Willcutt EG. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics. (2012) 9:490–9. doi: 10.1007/s13311-012-0135-8
68. Povlishock JT, Christman CW. The pathobiology of traumatically induced axonal injury in animals and humans: a review of current thoughts. J Neurotrauma. (1995) 12:555–64. doi: 10.1089/neu.1995.12.555
69. Bigler ED. Distinguished neuropsychologist award lecture 1999. The lesion(s) in traumatic brain injury: implications for clinical neuropsychology. Arch Clin Neuropsychol. (2001) 16:95–131. doi: 10.1016/S0887-6177(00)00095-0
70. Gao Y, Shuai D, Bu X, Hu X, Tang S, Zhang L, et al. Impairments of large-scale functional networks in attention-deficit/hyperactivity disorder: a meta-analysis of resting-state functional connectivity. Psychol Med. (2019) 49:2475–85. doi: 10.1017/S003329171900237X
71. Faraone SV, Perlis RH, Doyle AE, Smoller JW, Goralnick JJ, Holmgren MA, et al. Molecular genetics of attention-deficit/hyperactivity disorder. Biol Psychiatry. (2005) 57:1313–23. doi: 10.1016/j.biopsych.2004.11.024
72. Stojanovski S, Felsky D, Viviano JD, Shahab S, Bangali R, Burton CL, et al. Polygenic risk and neural substrates of attention-deficit/hyperactivity disorder symptoms in youths with a history of mild traumatic brain injury. Biol Psychiatry. (2019) 85:408–16. doi: 10.1016/j.biopsych.2018.06.024
73. Hicks R, Giacino J, Harrison-Felix C, Manley G, Valadka A, Wilde EA. Progress in developing common data elements for traumatic brain injury research: version two–the end of the beginning. J Neurotrauma. (2013) 30:1852–61. doi: 10.1089/neu.2013.2938
74. Hoogman M, Muetzel R, Guimaraes JP, Shumskaya E, Mennes M, Zwiers MP, et al. Brain imaging of the cortex in ADHD: a coordinated analysis of large-scale clinical and population-based samples. Am J Psychiatry. (2019) 176:531–42. doi: 10.1176/appi.ajp.2019.18091033
Keywords: ADHD, traumatic brain injury, attention, secondary ADHD, pediatric
Citation: Stojanovski S, Scratch SE, Dunkley BT, Schachar R and Wheeler AL (2021) A Systematic Scoping Review of New Attention Problems Following Traumatic Brain Injury in Children. Front. Neurol. 12:751736. doi: 10.3389/fneur.2021.751736
Received: 01 August 2021; Accepted: 04 October 2021;
Published: 10 November 2021.
Edited by:
Nicole Osier, University of Texas at Austin, United StatesReviewed by:
Nicholas Morris, University of Maryland, United StatesCopyright © 2021 Stojanovski, Scratch, Dunkley, Schachar and Wheeler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anne L. Wheeler, YW5uZS53aGVlbGVyQHNpY2traWRzLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.