
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 07 October 2021
Sec. Multiple Sclerosis and Neuroimmunology
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.716548
This article is part of the Research Topic Reassessing the Immune System Contribution in Multiple Sclerosis: Therapeutic Target, Biomarkers of Disease and Immune Pathogenesis View all 19 articles
 Jose M. Serra López-Matencio1
Jose M. Serra López-Matencio1 Yaiza Pérez García2
Yaiza Pérez García2 Virginia Meca-Lallana3
Virginia Meca-Lallana3 Raquel Juárez-Sánchez2Angeles Ursa2Lorena Vega-Piris4Dora Pascual-Salcedo2Annick de Vries5
Raquel Juárez-Sánchez2Angeles Ursa2Lorena Vega-Piris4Dora Pascual-Salcedo2Annick de Vries5 Theo Rispens5
Theo Rispens5 Cecilia Muñoz-Calleja2,6*
Cecilia Muñoz-Calleja2,6*Background: Plasma concentration of natalizumab falls above the therapeutic threshold in many patients who, therefore, receive more natalizumab than necessary and have higher risk of progressive multifocal leukoencephalopathy.
Objective: To assess in a single study the individual and treatment characteristics that influence the pharmacokinetics and pharmacodynamics of natalizumab in multiple sclerosis (MS) patients in the real-world practice.
Methods: Prospective observational study to analyse the impact of body weight, height, body surface area, body mass index, gender, age, treatment duration, and dosage scheme on natalizumab concentrations and the occupancy of α4-integrin receptor (RO) by natalizumab.
Results: Natalizumab concentrations ranged from 0.72 to 67 μg/ml, and RO from 26 to 100%. Body mass index inversely associated with natalizumab concentration (beta = −1.78; p ≤ 0.001), as it did body weight (beta = −0.34; p = 0.001), but not height, body surface area, age or gender Extended vs. standard dose scheme, but not treatment duration, was inversely associated with natalizumab concentration (beta = −7.92; p = 0.016). Similar to natalizumab concentration, body mass index (beta = −1.39; p = 0.001) and weight (beta = −0.31; p = 0.001) inversely impacted RO. Finally, there was a strong direct linear correlation between serum concentrations and RO until 9 μg/ml (rho = 0.71; p = 0.003). Nevertheless, most patients had higher concentrations of natalizumab resulting in the saturation of the integrin.
Conclusions: Body mass index and dosing interval are the main variables found to influence the pharmacology of natalizumab. Plasma concentration of natalizumab and/or RO are wide variable among patients and should be routinely measured to personalize treatment and, therefore, avoid either over and underdosing.
Natalizumab is a recombinant humanized anti-α4-integrin antibody against the α subunit (CD49d) of α4 integrins [α4β1 (VLA-4) and α4β7], that prevents the extravasation of inflammatory leukocytes across the blood-brain barrier into the central nervous system (1, 2). Natalizumab is currently indicated as a single disease modifying therapy in highly active relapsing remitting multiple sclerosis (RRMS) (3–5). The drug reduces multiple sclerosis relapses very effectively; nevertheless, it is associated with progressive multifocal leukoencephalopathy (PML), a potentially fatal complication caused by the reactivation of latent John Cunningham virus (JCV). Established risk factors for PML include: the level of anti JCV antibodies in serum as assessed by an anti-JCV antibody index; the use of immunosuppressant therapy before natalizumab initiation; and the duration of natalizumab treatment (6, 7).
The mechanisms underlying the development of PML associated with natalizumab are not completely understood but in all likelihood include, among others, the inhibition of the trafficking of immune cells like antigen presenting cells and anti-viral Th1 lymphocytes to the central nervous system (8, 9), therefore hampering the elimination of the JVC. The magnitude of this extravasation blockade is almost certainly related to the degree of saturation of the α4-integrin. Since demonstrating the presence of a concentration-dependent increase of α4-integrin saturation (10, 11), the PML risk seems to be linked to natalizumab serum concentrations (12–14).
Natalizumab is approved at a fixed dose of 300 mg IV every 4 weeks for the treatment of RRMS in adult patients, allowing natalizumab concentrations to be maintained at levels which ensure continuous maximal α4β1 integrin receptor saturation (15). However, many monoclonal antibodies are dosed on an individual basis (16, 17).
Whereas in the AFFIRM trial the average concentration on the steady state ranged between 23 and 29 μg/ml (11). It is known that plasma concentrations of natalizumab between 1 and 2 μg/ml are enough for most patients to reach saturation of α4-integrin [>80% of receptor occupancy (RO)]. Also that receptor desaturation (saturation <50%) only happens when natalizumab serum concentrations fall below 1 μg/mL (18). This suggests that most patients are overdosed by following the approved guidelines. In addition, considerable variation in natalizumab levels was found among patients in several studies (5, 10, 11, 19) despite administering the same dosage. As a consequence, many clinicians throughout the world now utilize alternative dosing schedules, mainly the extended interval dose (EID), to the standard interval dose (SID) (20–22).
We believe that optimizing natalizumab doses for individual patients is necessary to avoid either relapses or side-effects of the drug. To achieve this, it is necessary to know the impact of different parameters, including: body weight, height, body surface area, body mass index (BMI), age, gender, treatment duration and dosing intervals which influence the pharmacology of natalizumab. However, very few studies (19) have considered, in the real-world practice, both the personal and treatment characteristics altogether in the pharmacokinetics (PK) and pharmacodynamics (PD) of this therapeutic antibody.
This study is a prospective, observational, nonrandomized, open-label study performed at La Princesa Hospital (Madrid, Spain). For the study were enrolled 32 patients receiving natalizumab for relapsing into various forms of RRMS between 2014 and 2019. The eligibility criteria were: a diagnosis of RRMS according to the applicable panel criteria (23), age of 18 years or older and receiving natalizumab treatment with a minimum of six consecutive infusions. Exclusion criteria were: patients who did not give their informed consent in writing to take part in the study, patients who did not follow the treatment and patients who did not meet the above criteria.
Blood samples were collected immediately prior to the next natalizumab infusion. For some analyses, patients were divided into two groups based on the time interval since the previous natalizumab infusion: SID (26–33 days) or EID (34–41 days). These ranges were chosen after considering the bibliography, in which an interval of 3.5–4.5 weeks was considered standard, and an interval of more than 5 weeks was considered as extended (19–21). Body surface area was calculated with the Du Bois formula (24) and BMI was calculated as body-weight/height2 (25). At least two serum samples and a maximum of four were drawn from each patient with a difference between samples of 1–5 months. Twenty three patients contributed with two samples, eight with three and one with four.
All samples were obtained at least 7 months after the first dose of natalizumab, therefore the drug had reached the steady state in all patients (10, 26). The longest time from the beginning of the treatment to the extraction of the peripheral blood samples was 54 months. In the case of SID and EID, the interval between sample collection and start of treatment is comparable (30.8 months for SID and 35.61 for EID) according to a two-sample t-test with equal variances, p-value = 0.1789. In total, 74 samples were collected: 30 corresponded to the SID group (40.54%), and 44 to the EID one (59.45%).
The study was classified as a “Postauthorization-Observational Study with drugs” by the Spanish Drug Agency and approved by the ethics committee of La Princesa Hospital (2634A; AMB-NAT-2015-01) and written, informed consent was provided by all research participants. Expanded disability scale score (EDSS), annualized relapse rate (ARRR), age, gender, body weight, treatment duration, and other clinical parameters were obtained from the Hospital medical records.
Serum concentrations of natalizumab were measured at Sanquin Laboratories (Amsterdam) by an ELISA technique, previously described (27). Briefly, the technique requires specific polyclonal rabbit anti-natalizumab F (ab) 2 fragments as capture reagent and a mouse anti-human IgG4 (anti-hIgG4) monoclonal antibody for detection.
The RO was measured by flow cytometry with an anti-human IgG4-PE to reveal the binding of natalizumab to the surface of the lymphocytes. Three aliquots of whole peripheral blood were washed twice with phosphate-buffered saline to eliminate soluble IgG4 immunoglobulins present in the plasma of the patients to which anti-IgG4-PE could be bound. One of the aliquots was incubated with saturating natalizumab (10 μg/mL) for 1 h at 4°C temperature whereas the remaining two were kept in ice without natalizumab. After incubation, immunofluorescence was carried out against the following human molecules with the next panel of labeled antibodies: CD4-FITC, IgG4-PE, CD19-PerCP, CD3-V500, and CD8-APC-H7 (BD Biosciences, San José, CA). One of the tubes without natalizumab was used for fluorescence minus one (FMO)-PE control. The incubation was made in darkness for 30 min at 4°C. Then, red blood cells were lysed with FACS lysing solution (BD Biosciences, San José, CA) for 10 min and the remaining leukocytes were suspended with phosphate-buffered saline−1% fetal calf serum. The percentage of the different lymphoid subsets and the mean fluorescence intensity (MFI) of the PE signal were measured with a FACSCanto II flow cytometer (BD Biosciences, San José, CA) collecting 100,000 nucleated events. The percentage of natalizumab saturation was calculated from the MFI in each sample by the following formula: MFI – hIgG4-PE signal (without natalizumab)/MFI – hIgG4-PE signal (with natalizumab) × 100.
Sample size predetermination was focused on the association between RO and plasma levels. Assuming a minimum correlation = 0.50, an alpha risk of 0.05 and a beta risk of 0.20, we obtained a sample of 30 patients.
Variables analyzed included serum concentration of natalizumab, α4-integrin saturation (RO), weight, height, body surface area, BMI, age, gender, time to treatment start, and dose scheme [either as continuous or categoric variable (SID vs. EID)].
Descriptive analysis of the sample: quantitative variables were described by their measures of central tendency (mean) and dispersion (standard deviation); qualitative variables were described by their proportion and number of patient. Differences of mean were analyzed by t-test. Homoscedasticity was tested with Levened and since the t-test is a robust test (n ≥ 30), normality was not checked. Heteroscedasticity variables were analyzed with an unequal variance t-test. Spearman's correlation (rho) was used for association analysis of quantitative variables. A linear regression model was applied to control for possible confounding variables. A 95% CI was calculated for all estimates. A p < 0.05 was considered statistically significant. All analyses were performed using Stata version 13.
The 32 patients enrolled for the study experienced at least 1 relapse in the previous 12 months before being treated with natalizumab and their characteristics are summarized in Table 1.
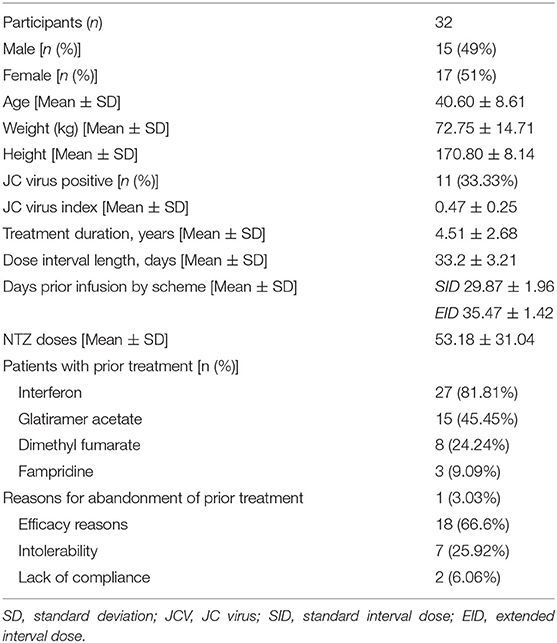
Table 1. Patient demographic and clinical characteristics.
According to the Expanded Disability Status Scale (EDSS) (23), 26 patients (81.25%) presented mild to moderate impairment (EDSS ≤ 4), while 6 (18.75%) patients presented mild to moderate disability (EDSS between 4 and 7): no patient exceeded (EDSS > 7) thus unable to walk beyond ~5 m. The mean (SD) EDSS score at the start of the study was 2.599 ± 1.520 while at the end it was 2.484 ± 1.486.
No participant missed a scheduled dose of natalizumab and all patients received the full 300 mg dose. There were no major adverse events that could have prevented the administration of a dose to a patient. All patients were radiologically stable and did not relapse during the study.
The serum concentration of natalizumab was highly varied, ranging from 0.72 to 67 μg/ml: the concentration was constant over time for the same patient and most individuals. A variation in concentration of more than 15 ug/ml was observed in four patients. The rest of the patients had quite a good concordance in serum concentrations amongst samples from the same individual. However, variation among serum natalizumab concentrations between one individual and another were high, ranging from 1–2 to 50 or more μg/ml.
In view of these observations, we analyzed individual factors which could affect the PK and PD of natalizumab, including body weight, height, body surface area, BMI, age, gender, dose scheme, and duration of treatment.
Among individual characteristics, we found a negative linear relationship between serum concentrations of natalizumab and patient body weight (rho = −0.404; p < 0.001; Figure 1A), body surface area (−0.3624; p = 0.0015; Figure 1B), and BMI (−0.4933; p = 0.0000; Figure 1C), when considered as continuous variables. Similarly, when we analyzed the correlation between serum concentration and the interval between doses in each sample we saw a slight negative correlation between post-infusion days and plasma concentration of natalizumab (rho = −0.2389; p = 0.0403; Figure 1D). This correlation between body weight and natalizumab concentrations was seen with similar strength in both treatment schemes (SID rho = −0.41 p < 0.04 vs. EID rho = −0.42 p < 0.002; data not shown).
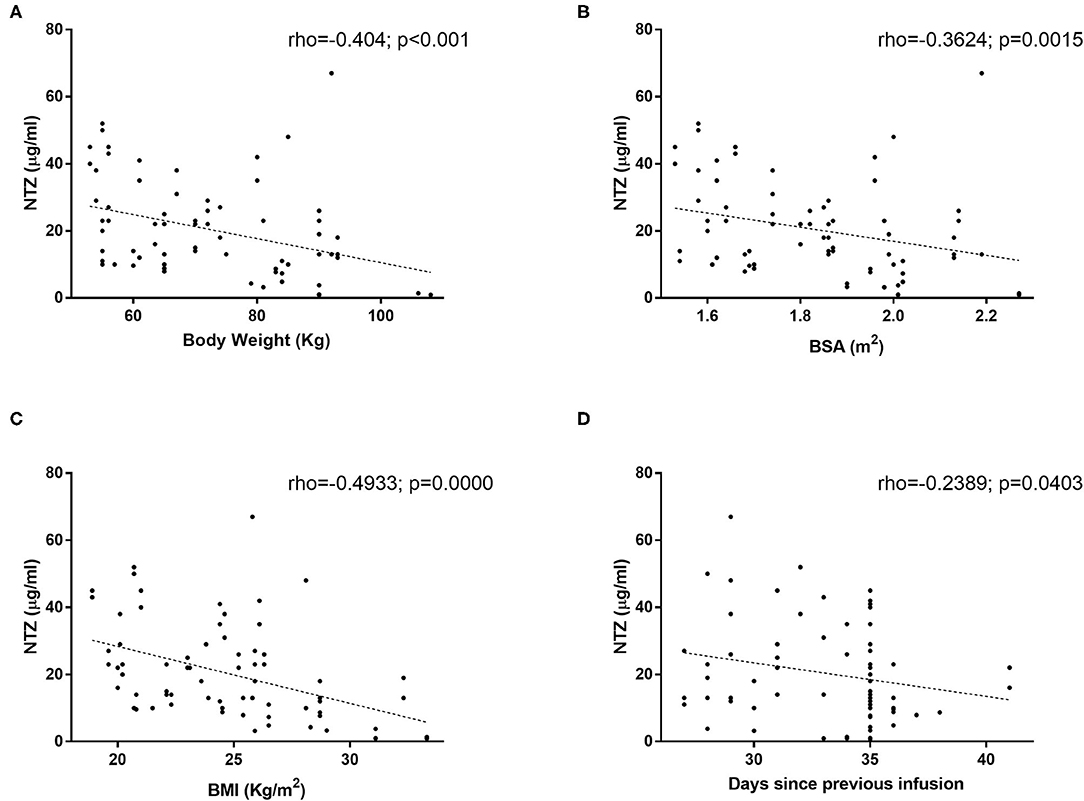
Figure 1. Natalizumab serum concentration correlation to (A) body weight, (B) Body Surface Area (BSA), (C) Body Mass Index (BMI), and (D) scheme doses. Natalizumab concentration was measured with ELISA as described by Rispens et al. in 74 samples from 32 patients. Spearman's correlation (rho) was used for association analysis of quantitative variables.
Multivariate analysis confirmed that body weight, BMI and dose interval influence the serum levels of natalizumab (Tables 2, 3).

Table 2. Multivariate analysis for drug serum levels and body weight (variables are considered as continuous).

Table 3. Multivariate analysis for drug serum levels and BMI (variables are considered as continuous).
Finally, we found a weak association between natalizumab serum concentration and patient age (p = 0.033; data not shown) while the duration of the treatment did not influence the serum levels of the drug (data not shown).
To evaluate the PD of natalizumab we measured the RO in the T-cells from the peripheral blood of patients by using flow cytometry. Just as with natalizumab concentrations we analyzed the impact of different individual characteristics as well as the scheme of treatment on the RO of natalizumab.
The evaluation of natalizumab occupancy of α4-integrin also revealed high variability among patients, ranging from 44 to 100% (data not shown). Natalizumab occupancy of α4-integrin was weakly inversely related to the body weight when the whole cohort was considered (rho = −0.28; p = 0.02; Figure 2A). Similar correlations were obtained with both body surface area and BMI (rho = −0.2885; p = 0.0127; rho = −0.2232; p = 0.0559; Figures 2B,C). When patients were divided on SID or EID scheme of treatment, natalizumab occupancy of α4-integrin was related to body weight only in those patients treated with the EID scheme (rho = −0.416, p = 0.003). Actually, most patients with values of RO below 70% were high weight individuals from the EID scheme. In addition, the treatment scheme did not influence the RO, either as a categorical (SID or EID: 88.41 vs. 85.67, p = 0.367) or continuous variable (rho = 0.02; p = 0.853; Figure 2D).
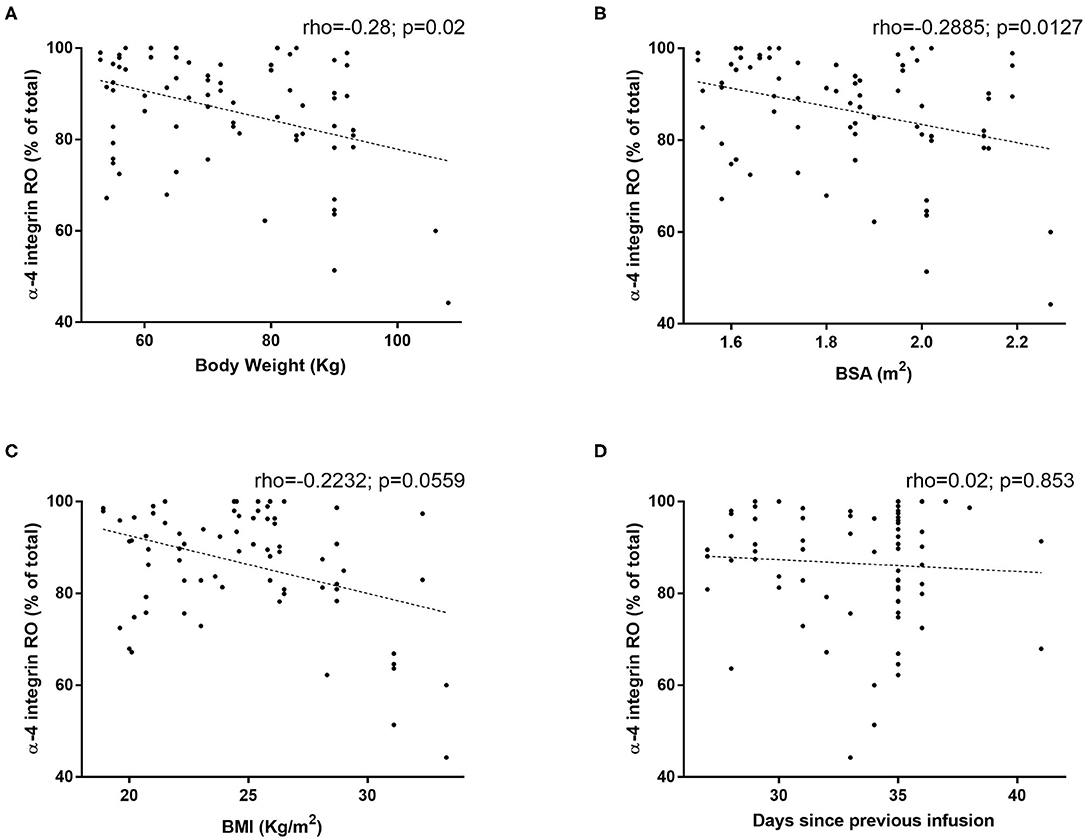
Figure 2. Correlation of receptor occupancy of α4-integrin by natalizumab to (A) body weight, (B) Body Surface Area (BSA), (C) Body Mass Index (BMI), and (D) scheme doses. The receptor occupancy of natalizumab was measured by flow cytometry, with an anti-human IgG4-PE, by revealing the binding of natalizumab to the surface of the lymphocytes in 74 samples from 32 patients. Spearman's correlation (rho) was used for association analysis of quantitative variables.
Similarly, the age, gender or treatment duration were not related to the RO neither considering patients as a whole cohort nor divided by the SID or EID scheme of treatment (data not shown). The multivariate analysis confirmed the inverse association between RO and body weight (beta = −0.31; p = 0.001) and BMI (beta = −1.39; p = 0.001; Tables 4, 5).

Table 4. Multivariate analysis for receptor occupancy of α4-integrin and body weight (variables are considered as continuous).

Table 5. Multivariate analysis for receptor occupancy of α4-integrin and BMI (variables are considered as continuous).
Finally, we wanted to confirm the dependence of the RO on the plasma concentration of natalizumab in our cohort of patients. A weak association was found between both parameters in the cohort of patients (rho = 0.256, p = 0.027; Figure 3); in the case for male patients (rho = 0.477, p = 0.019); in the group of patients above 40 years old (rho = 0.453, p = 0.04); and in the EID scheme (rho = 0.416, p = 0.003). A multivariate analysis confirmed that the higher the natalizumab concentration the higher the RO adjusted of gender, age and scheme of treatment (Table 6).
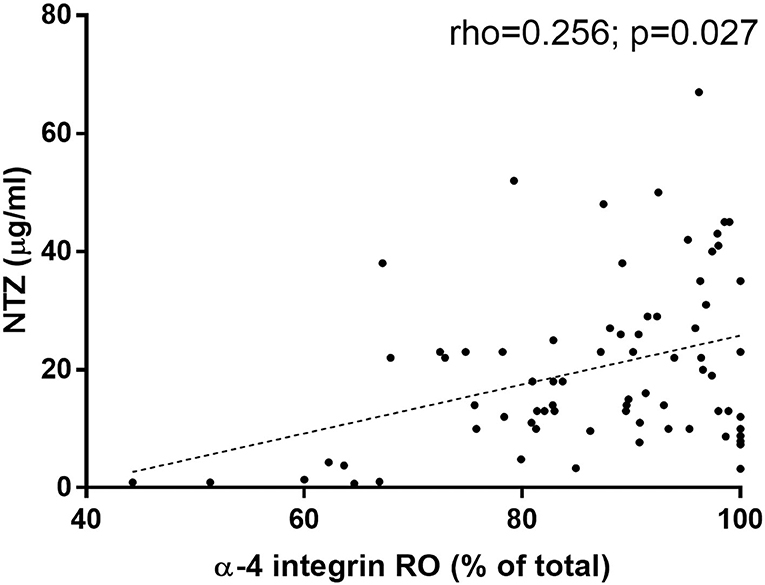
Figure 3. Receptor occupancy of α4-integrin by natalizumab correlates to natalizumab serum concentration. Natalizumab concentration was measured with ELISA as described by Rispens et al. The receptor occupancy of natalizumab was measured by flow cytometry with an anti-human IgG4-PE, by revealing the binding of natalizumab to the surface of the lymphocytes in 74 samples from 32 patients.

Table 6. Multivariate analysis confirming the relation between natalizumab concentration and receptor occupancy of α4-integrin.
The weak association between RO and plasma levels of natalizumab in the whole cohort was due to the fact that for over 10 μg/ml there was no correlation between RO and plasma concentration of natalizumab (Figure 3). In the light of this, correlations of up to 10 μg/ml and above 10 μg/ml were calculated separately: the values were for up to 10 μg/ml rho = 0.58 (p = 0.006) and above 10 μg/ml rho = 0.23 (p = 0.091). Moreover, the cut-off point with the highest statistic correlation between both parameters was 9 μg/ml (rho = 0.71; p = 0.003).
Our study adds insights on how the individual characteristics of the patients which mostly influence the PK (natalizumab serum concentration) and the PD (natalizumab RO) of natalizumab in 32 effectively treated RRMS patients for a long period of time with no major adverse reactions (data given in Table 1).
The long-standing experience reached with natalizumab in clinical trials and in observational studies offers strong evidence of its effectiveness in RRMS patients (3–5). However, there has been some concern for the patient safety since natalizumab was linked to some cases of PML (6, 7). Established risk factors for PML include the level of anti JCV antibodies in serum as assessed by anti-JCV antibody index, the use of immunosuppressant therapy before natalizumab initiation, and the duration of natalizumab treatment (6, 7). Moreover, it is more than likely that the EID scheme would develop this severe disease to a lesser extent and that this scheme could effectively control the RRMS in the same way. To confirm this possibility several studies were carried out by different authors (11, 18–22, 27–29). Currently, there are two clinical trials in this field, one assessing the effect of a planned 12-week dosing interruption on the drug PK (NCT04048577), and another to evaluate the impact of switching the patients from SID to EID on the effectiveness of natalizumab (NCT04580381).
The evaluation of natalizumab serum concentrations in our patients revealed a broad range (over 60-fold) of values, showing the pharmacological variability that exists among patients. The majority of patients had concentrations of 5 μg/ml or greater, including two patients with concentrations >50 μg/ml. This means that most patients were over-treated (19, 20), since concentrations higher than 5 μg/ml were related to complete saturation of the α4-integrin in most patients. This could increase the patient's risk of developing PML (29).
Our data demonstrate that serum concentration of natalizumab is inversely related with patient's weight, in agreement with previous studies (19, 30, 31), as well as with body surface area and BMI. Therefore, these parameters should be taken into consideration when deciding the scheme for natalizumab.
Similar to other studies the treatment scheme also impacted the plasma concentration of natalizumab, that was higher in the SID scheme (19, 21, 22). The selected patients from the SID group could, therefore, switch to the EID group since no patient relapsed during the study. Several studies after natalizumab discontinuation indicate that MS disease activity is suppressed for at least 6 weeks after the last administration of the drug (12, 14). Furthermore, 2 retrospective studies have suggested that natalizumab efficacy is not compromised by EID regimens (21, 22).
When stratified by gender, natalizumab serum concentrations were lower in men, both in the whole cohort and in the different dose schedules. However, no effect of gender was observed in the multivariate analysis, suggesting that those differences were actually related to weight differences between the sexes. Treatment duration did not influence the natalizumab serum concentrations, which is in line with other study (31). These findings reopen the discussion on whether a longer course of treatment could be supported without increasing the risk of PML (32, 33).
Regarding natalizumab RO, it has always been assumed that values between 70 and 80% were necessary for optimal drug efficacy. However, different studies show that much lower levels (around 20%) would be enough to keep the patient without significant disease activity (18, 34). This is supported by our study here where we found RO values under 70% and even some under 60% in stable patients.
In the individual characteristics that affect the RO, we found that occupancy of α4-integrin is weakly inversely related to the body weight and BMI when the whole cohort was considered. The fact that most patients were beyond saturation levels may explain the low significance, in accordance with a previous study (10). The relationship of RO and body weight found in the whole cohort was only maintained in the EID cohort, this may be due to the fact that many of our samples for EID were from heavier patients. There are no significant differences in RO values when dividing patients by the scheme of treatment, in contrast with other studies whereby those were greater in SID (19, 21). This may be a reflection of our study design, in which the EID samples were collected at ~5 weeks post infusion (Table 1), while in these other studies the time was longer, around 6 weeks. This would mean that the treatment could be extended at least 1 week without significant changes in RO.
Finally, in our cohort of patients we confirmed and characterized the correlation between the RO and the plasma concentration of natalizumab. In fact, we have described that a concentration of natalizumab of 9 μg/ ml is the cut-off point where the strongest correlation between these variables: when the natalizumab concentration increases, the α4ß1-integrin saturation increases rapidly from ~40% to 80%, but the curve flattens beyond this value. In other studies this cut-off was established at 10 μg/ml (10). It appears that physicians should avoid concentrations higher than 9 μg/ml because there is no PD advantage or clinical benefits. Furthermore, we should seek lower concentrations to obtain even lower RO values since RO values below 50% have been sufficient to keep patients without radiological and clinical disease activity, either in our study or others (18, 34). Nevertheless, we are conscious that stability on MRI and lack of clinical relapses in the short term of observation are unequivocally not identical to lack of clinical progression, neurodegeneration, and axonal loss over the longer term.
In summary, with the current approved fixed dose, there is a wide pharmacological variability between patients that prescribing clinicians should be aware and take into account. Among the individual characteristics, body weight, BMI, and the treatment scheme, had a significant impact on the pharmacology of natalizumab. In addition, RO strongly depends on natalizumab serum concentrations up to ~9 μg/ml while higher concentrations result in the saturation of the integrin in most patients. As a consequence, the majority of our patients were overtreated. Conversely, testing levels may be extremely useful to prevent inadvertent underdosing of patients, specifically those in whom extended dosing is exhibited. The possibility of underdosing should dominate clinical concerns in this group of patients. To pursue these possible outcomes larger studies will be necessary.
In summary, the authors strong argue that either the RO and/or the serum concentration of natalizumab should be routinely measured in every patient, with the aim of personalizing treatment without loss of efficacy.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of La Princesa Hospital. The patients/participants provided their written informed consent to participate in this study.
JMSL-M and CM-C: conception, data collection, analysis, and writing. YP: data collection and sample analysis. VM-L: conception, data collection, and critical revision. RJ-S: sample analysis. LV-P: analysis and critical revision. DP-S: critical revision. AV: sample analysis and critical revision. TR: sample analysis and critical revision. All authors contributed to the article and approved the submitted version.
This work was supported by a grant PI018/01163 from the Fondo de Investigaciones Sanitarias, Instituto de Investigación Carlos III, Ministerio de Sanidad y Consumo, Spain, to CM-C who also was cofinanced by FEDER funds.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Lawrence Baron for linguistic and grammatical editing of the manuscript and Ana Marcos Jiménez for editing of the figures.
1. Yednock TA, Cannon C, Fritz LC, Sanchez-Madrid F, Steinman L, Karin N. Prevention of experimental autoimmune encephalomyelitis by antibodies against alpha 4 beta 1 integrin. Nature. (1992) 356:63–6. doi: 10.1038/356063a0
2. Léger OJ, Yednock TA, Tanner L, Horner HC, Hines DK, Keen S, et al. Humanization of a mouse antibody against human alpha-4 integrin: a potential therapeutic for the treatment of multiple sclerosis. Hum Antibodies. (1997) 8:3–16. doi: 10.3233/HAB-1997-8102
3. European Commission (2006). Renewing and Amending the Marketing Authorisation for the Medicinal Product for Human Use and Quot; Tysabri - Natalizumab and Quot; granted by Decision C. Available online at: http://ec.europa.eu/health/documents/community-register/2016/20160418134501/dec_134501_en.pdf (accessed March 1, 2017).
4. Rudick R, Polman C, Clifford D, Miller D, Steinman L. Natalizumab: bench to bedside and beyond. JAMA Neurol. (2013) 70:172–82. doi: 10.1001/jamaneurol.2013.598
5. Polman CH, O'Connor PW, Havrdova E, Hutchinson M, Kappos L, Miller DH, et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. (2006) 354:899–910. doi: 10.1056/NEJMoa044397
6. Langer-Gould A, Atlas SW, Green AJ, Bollen AW, Pelletier D. Progressive multifocal leukoencephalopathy in a patient treated with natalizumab. N Engl J Med. (2005) 353:375–81. doi: 10.1056/NEJMoa051847
7. Kleinschmidt-DeMasters BK, Tyler KL. Progressive multifocal leukoencephalopathy complicating treatment with natalizumab and interferon beta-1a for multiple sclerosis. N Engl J Med. (2005) 353:369–74. doi: 10.1056/NEJMoa051782
8. Del Pilar Martin M, Cravens PD, Winger R, Frohman EM, Racke MK, Eagar TN. Decrease in the numbers of dendritic cells and CD4+ T cells in cerebral perivascular spaces due to natalizumab. Arch Neurol. (2008) 65:1596–603. doi: 10.1001/archneur.65.12.noc80051
9. Paroni M, Maltese V, De Simone M, Ranzani V, Larghi P, Fenoglio C, et al. Recognition of viral and self-antigens by TH1 and TH1/TH17 central memory cells in patients with multiple sclerosis reveals distinct roles in immune surveillance and relapses. J Allergy Clin Immunol. (2017) 140:797–808. doi: 10.1016/j.jaci.2016.11.045
10. Muralidharan KK, Kuesters G, Plavina T, Subramanyam M, Mikol DD, Gopal S, et al. Population pharmacokinetics and target engagement of natalizumab in patients with multiple sclerosis. J Clin Pharmacol. (2017) 57:1017–30. doi: 10.1002/jcph.894
11. Fox RJ, Cree BA, De Seze J, Gold R, Hartung H-P, Jeffery D, et al. MS disease activity in RESTORE: a randomized 24-week natalizumab treatment interruption study. Neurology. (2014) 82:1491–8. doi: 10.1212/WNL.0000000000000355
12. Frohman EM, Monaco MC, Remington G, Ryschkewitsch C, Jensen PN, Johnson K, et al. JC virus in CD34+ and CD19+ cells in patients with multiple sclerosis treated with natalizumab. JAMA Neurol. (2014) 71:596–602. doi: 10.1001/jamaneurol.2014.63
13. Major EO, Frohman EM, Douek D. JC viremia in natalizumab treated patients with multiple sclerosis. N Engl J Med. (2013) 368:2240–1. doi: 10.1056/NEJMc1214233
14. Berkovich R, Togasaki DM, Cen SY, Steinman L. CD4 cell response to interval therapy with natalizumab. Ann Clin Transl Neurol. (2015) 2:570–4. doi: 10.1002/acn3.190
15. European Medicine Agency (EMA) (2020). Natalizumab: Summary of Product Characteristics. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000603/WC500044686.pdf (accessed March 1, 2020).
16. European Medicine Agency (EMA). Tocilizumab: Summary of Product Characteristics. (2020). Available online at: https://www.ema.europa.eu/en/medicines/human/EPAR/roactemra (accessed March 1, 2020).
17. European Medicine Agency (EMA). Rituximab: Summary of Product Characteristics. (2020). Available online at: https://www.ema.europa.eu/en/documents/productinformation/mabthera-epar-product-information_en.pdf (accessed March 1, 2020).
18. Khatri BO, Man S, Giovannoni G, Koo AP, Lee JC, Tucky B, et al. Effect of plasma exchange in accelerating natalizumab clearance and restoring leukocyte function. Neurology. (2009) 72:402–9. doi: 10.1212/01.wnl.0000341766.59028.9d
19. Foley JF, Goelz S, Hoyt T, Christensen A, Metzger RR. Evaluation of natalizumab pharmacokinetics and pharmacodynamics with standard and extended interval dosing. Mult Scler Relat Disord. (2019) 31:65–71. doi: 10.1016/j.msard.2019.03.017
20. Yamout BI, Sahraian MA, Ayoubi NE, Tamim H, Nicolas J, Khoury SJ, et al. Efficacy and safety of natalizumab extended interval dosing. Mult Scler Relat Disord. (2018) 24:113–6. doi: 10.1016/j.msard.2018.06.015
21. Bomprezzi R, Pawate S. Extended interval dosing of natalizumab: a two-center, 7-year experience. Ther Adv Neurol Disord. (2014) 7:227–31. doi: 10.1177/1756285614540224
22. Zhovtis RL, Frohman TC, Foley J, Kister I, Weinstock-Guttman B, Tornatore C, et al. Extended interval dosing of natalizumab in multiple sclerosis. J Neurol Neurosurg Psychiatry. (2016) 87:885–9. doi: 10.1136/jnnp-2015-312940
23. Thompson A, Banwell B, Barkoff F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald Criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/S1474-4422(17)30470-2
24. Du Bois D, Du Bois EF. A formula to estimate the approximate surface area if height and weight be known. Arch of Int Med. (1916) 17:863–71. doi: 10.1001/archinte.1916.00080130010002
25. Deurenberg P, Weststrate JA, Seidell JC. Body mass index as a measure of body fatness: age- and sex-specific prediction formulas. Br J Nutr. (1991) 65:105. doi: 10.1079/BJN19910073
26. Calabresi PA, Giovannoni G, Confavreux C, Galetta SL, Havrdova E, Hutchinson M, et al. The incidence and significance of anti-natalizumab antibodies: results from AFFIRM and SENTINEL. Neurology. (2007) 69:1391–403. doi: 10.1212/01.wnl.0000277457.17420.b5
27. Rispens T, Leeuwen A, Vennegoor A, Killestein J, Aalberse RC, Wolbink GJ, et al. Measurement of serum levels of natalizumab, an immunoglobulin G4 therapeutic monoclonal antibody. Anal Biochem. (2011) 411:271–6. doi: 10.1016/j.ab.2011.01.001
28. Sehr T, Proschmann U, Thomas K, Marggraf M, Straube E, Reichmann H, et al. New insights into the pharmacokinetics and pharmacodynamics of natalizumab treatment for patients with multiple sclerosis, obtained from clinical and in vitro studies. J Neuroinflammation. (2016) 13:164. doi: 10.1186/s12974-016-0635-2
29. Van Kempen ZL, Leurs CE, Witte BI, de Vries A, Wattjes MP, Rispens T, et al. The majority of natalizumab-treated MS patients have high natalizumab concentrations at time of re-dosing. Mult Scler. (2017) 24:805–10. doi: 10.1177/1352458517708464
30. Zhovtis RL, Foley JF, Chang I, Kister I, Cutter G, Metzger RR, et al. Risk of natalizumab-associated PML in patients with MS is reduced with extended interval dosing. Neurology. (2019) 93:e1452–62.
31. van Kempen ZLE, Hoogervorst ELJ, Wattjes MP, Kalkers NF, Mostert JP, Lissenberg-Witte BI, et al. Personalized extended interval dosing of natalizumab in MS - a prospective multicenter trial. Neurology. (2020) 95:e745–54. doi: 10.1212/WNL.0000000000009995
32. Bloomgren G, Richman S, Hotermans C, Subramanyam M, Goelz S, Natarajan A, et al. Risk of natalizumab-associated progressive multifocal leukoencephalopathy. N Engl J Med. (2012) 366:1870–80. doi: 10.1056/NEJMoa1107829
33. Ho PR, Koendgen H, Campbell N, et al. Risk of natalizumab-associated progressive multifocal leukoencephalopathy in patients with multiple sclerosis: a retrospective analysis of data from four clinical studies. Lancet Neurol. (2017) 16:925–33. doi: 10.1016/S1474-4422(17)30282-X
Keywords: natalizumab, pharmacokinetics, pharmacodynamics, multiple sclerosis, α4-integrin, dose scheme, efficacy, progressive multifocal leukoencephalopathy PML
Citation: Serra López-Matencio JM, Pérez García Y, Meca-Lallana V, Juárez-Sánchez R, Ursa A, Vega-Piris L, Pascual-Salcedo D, de Vries A, Rispens T and Muñoz-Calleja C (2021) Evaluation of Natalizumab Pharmacokinetics and Pharmacodynamics: Toward Individualized Doses. Front. Neurol. 12:716548. doi: 10.3389/fneur.2021.716548
Received: 07 June 2021; Accepted: 07 September 2021;
Published: 07 October 2021.
Edited by:
Luisa María Villar, Ramón y Cajal University Hospital, SpainReviewed by:
Allan G. Kermode, University of Western Australia, AustraliaCopyright © 2021 Serra López-Matencio, Pérez García, Meca-Lallana, Juárez-Sánchez, Ursa, Vega-Piris, Pascual-Salcedo, de Vries, Rispens and Muñoz-Calleja. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cecilia Muñoz-Calleja, bXVub3pjYWxsZWphY2VjaWxpYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.