 Tianye Hu
Tianye Hu Hantong Hu
Hantong Hu Feng Chen1*
Feng Chen1*
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Neurol. , 15 July 2021
Sec. Headache and Neurogenic Pain
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.709803
Introduction: With a high incidence rate and low diagnosis rate, vestibular migraine (VM) can seriously affect the quality of life of patients, but it remains difficult to manage by current treatment options. Acupuncture may be a potential treatment option for VM prophylaxis, but the currently available evidence is still uncertain. Therefore, this trial aims to evaluate the efficacy and safety of acupuncture for VM prophylaxis.
Methods: This is a 28-week parallel, randomized, controlled clinical trial including 4 weeks of baseline, 8 weeks of treatment, and 16 weeks of follow-up. A total of 72 participants will be randomly assigned to two groups. The participants will receive acupuncture in the experimental group, while the participants in the control group will be treated with venlafaxine. The primary outcome measures are change in vertigo/migraine days and vertigo/migraine attacks, vertigo severity, and migraine intensity per 4 weeks from baseline. The secondary outcome measures are change in doses of rescue medication, anxiety level, depression level, and quality of life per 4 weeks from baseline. Adverse events will be recorded for safety evaluation.
Discussion: This study will investigate the efficacy and safety of acupuncture for VM prophylaxis. The results will contribute to determining whether acupuncture can serve as an optional treatment strategy for treating VM.
Clinical Trial Registration: www.ClinicalTrials.gov, identifier: NCT0464088.
Vestibular migraine (VM) is the most common cause of recurrent spontaneous attacks of vertigo, except for benign paroxysmal positional vertigo, which is causally related to migraine (1). Its typical clinical features consist of recurrent episodic vestibular symptoms and migrainous symptoms. Vestibular symptoms can present as vertigo/dizziness, unsteadiness, oscillopsia, and intolerance of head movement, while migrainous symptoms can be characterized by migrainous headache, photophobia, phonophobia, and visual or other neurologic auras (1).
VM can occur at any age, but it is more prevalent in women and in the age group of 30-40 years (2, 3). Epidemiological data of outpatient service show that VM accounts for about 9% of patients in migraine clinics (1), 11% of patients in dizziness clinics (4), and 4.2–29.3% of patients in otolaryngology clinics (5, 6). Despite its high incidence rate, the diagnosed rate of VM is low. As shown in a previous study, referring doctors had suspected only 1.8% of patients to have VM in a tertiary vertigo center, but a diagnosis was finally reached in 20.2% (7). Moreover, VM often leads to some common comorbidities, such as Meniere's disease and psychological disorders (especially anxiety and depression), which contribute to an increasing global burden (8–10). Nevertheless, till now, the pathogenesis of VM has been inconclusive, and further research are urgently warranted. Consequently, there is not any widely acknowledged therapy for treating VM.
At present, the treatment of VM mainly includes rescue treatment and prophylaxis, both of which are mainly pharmacological-based therapies and often lead to a series of unavoidable side effects, such as dizziness, paresthesia, dyspepsia, dry mouth, nausea, somnolence, and chest discomfort (11). Moreover, frequent VM attacks can seriously affect the daily life of patients. Therefore, prophylaxis treatment is very important for VM patients. As a consensus among expert proponents in China, it is vital for VM patients to receive prophylaxis treatment assuming that the frequency of vertigo/migraine episodes is at least three times per month in the past 3 months or the response to rescue therapies is poor in the acute phase of VM (12). Thus, there is a great need to identify alternative preventive treatments for VM.
As one of the major treatment modalities of traditional Chinese medicine (TCM), acupuncture has gained an important role as a non-pharmaceutical therapy for treating a variety of diseases or conditions, thereby receiving increasing worldwide acceptance. Acupuncture may be a potential treatment option for VM prophylaxis, the rationales of which include two major considerations. First, previous studies have reported encouraging results favoring acupuncture for treating vertigo/dizziness (13) and migraine (14, 15), which are major clinical symptoms of VM. Meanwhile, there are several reports indicating that acupuncture is beneficial to psychological disorders such as anxiety and depression (16, 17), which are common comorbidities of VM. Second, emerging studies have revealed that the pathogenesis of VM is related to the dysfunction of the connection between the trigeminal–vestibular–vagus nerves (18, 19). As a form of stimulation, cumulative evidence demonstrates that acupuncture can relieve the symptoms of patients via mediating neural plasticity (20). In this scenario, acupuncture can be considered as a potential treatment option for patients with VM, but the current evidence remains inconclusive (21).
In recent years, VM has increasingly attracted the attention of clinicians and researchers; however, there is yet a great lack of randomized controlled trials (RCTs) investigating acupuncture for VM prophylaxis. Therefore, the present study protocol of a RCT aims to investigate the efficacy and safety of acupuncture for VM prophylaxis, which will provide evidence and guide clinicians in this field.
The design of this trial is based on the Standards for Reporting Interventions in Clinical Trials of Acupuncture (22) and the Standard Protocol Items: Recommendations for Interventional Trials (23) reporting guidelines.
This randomized, controlled, single-center clinical trial will comprise two parallel groups. The participants will be randomly assigned in a 1:1 ratio to either the acupuncture group or the control group. The flowchart of the trial is presented in Figure 1, and the schedule of enrolment, interventions, and outcome assessments are presented in Table 1.
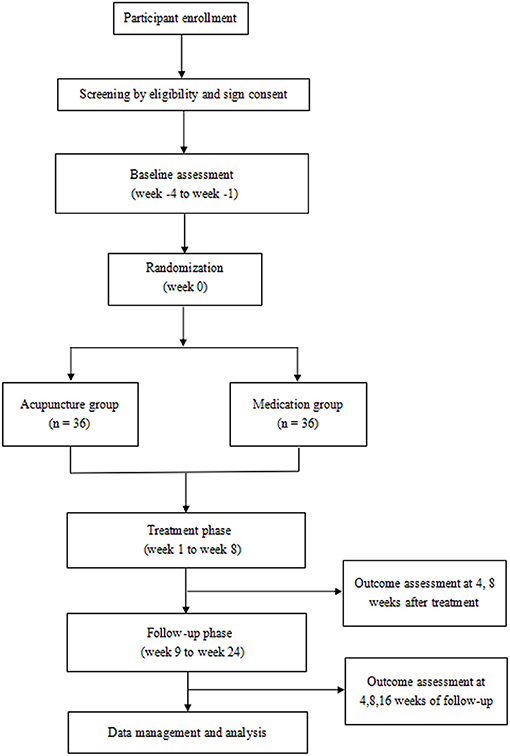
Figure 1. Flow diagram of the study procedure.
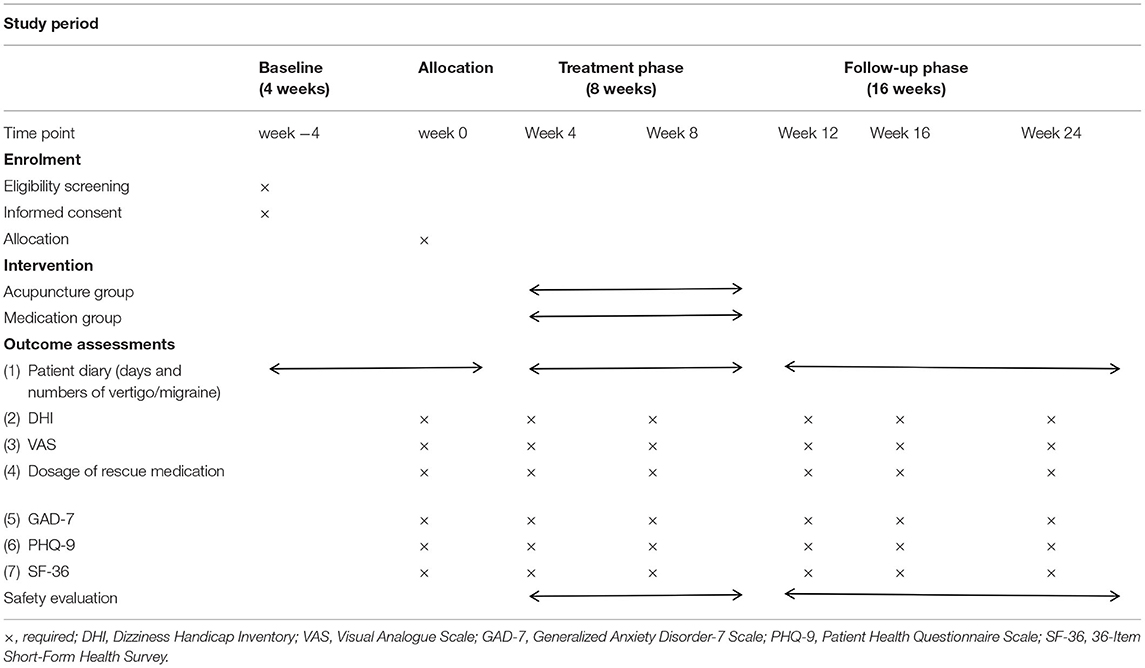
Table 1. Schedule of enrolment, interventions, and outcome assessments.
This trial is conducted in accordance with the principles of the Declaration of Helsinki and has been approved by the Ethical Committee of The First Affiliated Hospital of Jiaxing University (approval number: LS2020-259). Each participant will be notified regarding the details of the study protocol.
The study protocol has been registered in the clinicaltrials registry, with the identification number NCT0464088.
All participants will be given enough time to decide whether to engage in this trial. Patients who participate in this trial will be entitled to the right to achieve all relevant information of the trial, including the benefits or potential risk, and they will be allowed to drop out according to their consent or to discontinue their participation at any point of the study. The confidentiality of all the participant records will be protected. All participants should provide written informed consents if they are included in the trial.
The duration of the trial will include three study phases, including a 4-week screening and baseline phase (week −4 to week 0), an 8-week treatment phase (weeks 1-8), and a 16-week follow-up phase (weeks 9-24).
If the participants have an interest to take part in this trial, the researchers will interview their medical history in a screening form. For potentially eligible subjects, they will be instructed to continually keep a patient diary for 4 weeks, which is mainly designed to record details including the number and days of vertigo/migraine attacks, duration, frequency, vertigo severity, migraine intensity, and dose of rescue medication. Subsequently, they will be invited to attend an eligibility assessment to determine whether they can be included in the trial by the study investigators.
A target sample of 72 participants will be recruited in the acupuncture clinic and neurology clinic at The First Affiliated Hospital of Jiaxing University. The trial will be started from January 2021 to December 2023. Two major strategies will be used to recruit participants with VM. One is to recruit participants in outpatient clinics from the hospital mentioned above. The other is to show recruitment advertisements outside the clinics and through official media platform, which include roll-up banners, WeChat official accounts, and newspapers. The advertisements will contain brief introductions about the inclusion criteria, the population needed to be involved, and the contact information of the researcher.
(1) The age is between 18 and 80, and gender is not limited.
(2) Patients meet the VM diagnostic criteria proposed by the collaboration of Barany Society and the International Headache Society in 2012 (24).
(3) Vertigo/migraine attacks are at least three times per month in the last 3 months or vertigo/migraine days are at least 4 days per month.
(4) Patients have an unsatisfactory response to rescue treatments and seek for preventive treatments.
(5) Patients can fully understand the study protocol and agree to sign written informed consent forms.
(1) The vertigo and headache of patients are caused by other diseases, such as vestibular neuritis, Meniere's disease, tension headache, and other cerebrovascular diseases.
(2) Patients have a prophylactic headache treatment with drugs in the past 3 months.
(3) Patients are receiving adjunctive therapy that is not widely accepted for treating VM, such as Chinese herbs.
(4) Patients have severe complications in cardiovascular, cerebrovascular, liver, kidney, hematopoietic, and other systems that are not controlled significantly.
(5) Patients are pregnant and lactating female.
(6) Patients have a mental illness that affects cognitive function.
(1) Subjects have serious adverse reactions throughout the study and researchers determine it is not safe to continue participating in the trial.
(2) Subjects have serious complications or deteriorating conditions throughout the study and emergency measures are urgently needed.
(3) Subjects request to withdraw from the trial halfway due to any personal reasons.
(4) Subjects have poor compliance and fail to comply with the trial protocol.
(5) Subjects receive adjunctive treatments without permission, which will affect the efficacy assessment of current treatment schemes.
Eligible participants will be assigned randomly into the acupuncture group or the control group according to a table of random numbers, which is generated using Statistical Product and Service Solutions software V25.0 (SPSS V25.0).
To guarantee allocation concealment, random sequence will be created and kept secure by a specially designated coordinator who will not participate in other procedures of the trial. The randomization list will only be seen by this specially designated coordinator and will be concealed from other researchers. Grouping information will be hidden using sequentially numbered, opaque, and sealed envelopes. The researchers need to contact the designated coordinator by telephone to obtain the corresponding random number and grouping information for each included participant.
Owing to the complete difference between the two therapies in the two groups (i.e., acupuncture vs. pharmaceutical therapy), the participants will not be blinded in our study. Meanwhile, it is also impractical to blind the acupuncture operators due to the nature of the acupuncture procedure.
Nevertheless, the goal of blinding is to eliminate the influence of subjective factors from study subjects and researchers on the study results. With the attempt to minimize the subjective influence, the treatment, outcome assessment, and statistical analysis will be performed by independent researchers in our study. Statisticians and data managers who collect data and assess outcomes will be blinded to the grouping information by third-party independent personnel.
This group will include 36 VM patients. The participants in this group will receive acupuncture treatment for 8 weeks. The participants in the treatment group are not allowed to take prophylactic medications, but in case of intolerable acute VM attacks, the participants in the acupuncture group will be instructed to take triptans as rescue medication, and the dosage of medication will be documented in detail in the medical diary by the patient.
The rationales for the acupoint selection are based on consensus with experienced acupuncture experts, which target at alleviating major symptoms (i.e., migraine and vertigo/dizziness) and common comorbidities (i.e., emotional disorders) in VM patients. The acupoint selection of our study is highly overlapping with that in previously published trials involving acupuncture for treating migraine (14, 15), vertigo/dizziness (13, 25), and emotional disorders (16). As shown in Table 2, the selected acupoints include Baihui (DU20), Qianding (DU21), Yintang (EX-HN3), Fengchi (GB20), Shuaigu (GB8), Hegu (LI4), Neiguan (PC6), Shenmen (HT7), Fenglong (ST40), and Taichong (LR3). The location standard of the acupoints is based on the WHO standard for acupuncture point location (26).
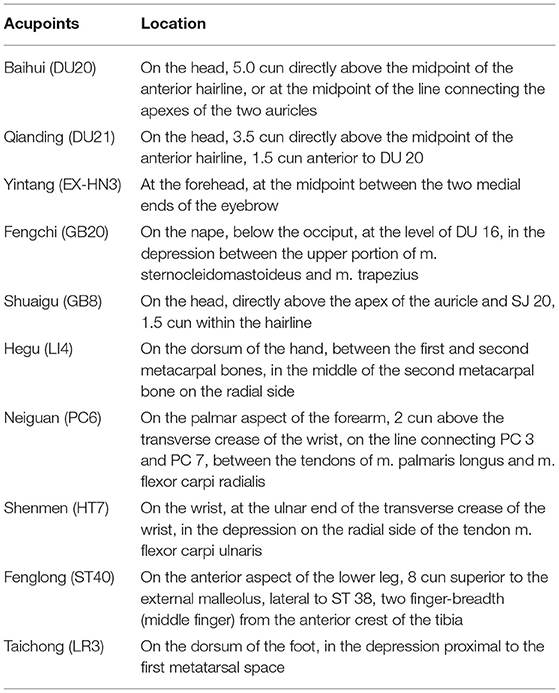
Table 2. Locations of the selected acupoints for treating vestibular migraine.
The acupuncturist will insert sterile, single-use filiform acupuncture needles (length, 40 mm; diameter, 0.30 mm) after disinfecting the skin. The needles used are Hwato needles (Suzhou Hwato Medical Instruments Co., China). Insertion will be followed by the classical needle stimulation methods of lifting/thrusting and twirling/rotating to produce a sensation known as Deqi (a compositional sensation including soreness, numbness, distention, and heaviness). Some acupoints, such as DU20 and DU21, are located beneath the scalp, which could be needled followed by the stimulation methods of pulling and pushing to reinforce a Deqi sensation.
The patients in this group will receive acupuncture once every other day (3 days per week) over an 8-week period (a total of 24 sessions). In each session, the needles will be retained for 30 min.
This group will include 36 VM patients. The participants in this group will receive an oral administration of venlafaxine at 50 mg once a day for 8 weeks. The reasons for selecting the dose of 50 mg in this study are based on clinical experience and results from a previous study, which revealed that a lower dose (e.g., 37.5 mg) of venlafaxine had a favorable therapeutic effect in the prophylaxis of VM (27). Additionally, a lower dose is likely to have less serious side effects when compared with a higher dose. In case of intolerable acute VM attacks, the participants will be instructed to take triptans as rescue medication, and the dosage of medication will be documented in detail in the medical diary by the patient.
All outcomes will be assessed at baseline (4 weeks before randomization), at 4 and 8 weeks after intervention, and at 4, 8, and 16 weeks of follow-up.
(1) Change in the number of vertigo/migraine days and vertigo/migraine attacks per 4 weeks from baseline: All participants will be instructed to keep a medical diary to record the number of vertigo/migraine days and vertigo/migraine attacks.
(2) Change in vertigo severity per 4 weeks from baseline: Vertigo severity will be measured by the Dizziness Handicap Inventory (DHI). DHI is a well-accepted questionnaire with 25 items and developed to assess the maiming and handicapping impact of dizziness (28). The total DHI index ranges from 0 to 100 (best to worst) to measure the overall severity of vertigo, which include physical, emotional, and functional three dimensions, and the higher the score, the greater effect to the patients.
(3) Change in migraine intensity per 4 weeks from baseline: Migraine intensity will be measured by a 10-point Visual Analog Scale (VAS). VAS is the most widely used scale for estimating subjective symptoms, including migraine intensity. The study subjects will use 0–10 (0: no symptoms, 10: most severe symptoms) to rate the intensity of migraine (29, 30).
(1) Change in doses of rescue medication: Doses of rescue medication (i.e., triptans) will be documented by patients in the medical diary.
(2) Change in anxiety level per 4 weeks from baseline: Anxiety level will be measured by Generalized Anxiety Disorder-7 (GAD-7) scale. The GAD-7 is a valid and reliable tool to measure general anxiety symptoms over the past 2 weeks across varied settings and populations (31). A total of seven questions, with frequencies of 0–3, are adopted to assess the presence and severity of anxiety based on the patient's condition, with 0–4 being no GAD, 5–9 being mild GAD, 10–14 being moderate GAD, and 15–21 being severe GAD (32).
(3) Change in depression level per 4 weeks from baseline: Depression level will be measured by Patient Health Questionnaire (PHQ-9) scale. The PHQ-9 is generally used to measure depression symptoms over the past 2 weeks with well-established validity and reliability (33). It includes a total of nine questions—the higher the score, the more depressed (34).
(4) Change in quality of life per 4 weeks from baseline: Quality of life will be measured by the 36-item Short-Form Health Survey (SF-36). The SF-36 is a tool to evaluate general health-based analysis of life condition in three aspects (functional ability, wellbeing, and overall health) over the past 4 weeks (35). The validity and reliability of SF-36 for measuring quality of life have been proven (36).
Safety evaluation will be performed based on the number of adverse events (AEs). The participants will report any AE that they experience during the study phase, including acupuncture-related AEs (e.g., discomfort or bruising at the site of needle insertion, vertigo/dizziness, nausea, feeling faint after each treatment, etc.) and drug-related AEs (e.g., dyspepsia, paresthesia, dry mouth, nausea, and somnolence).
We will take multiple measures to enhance quality control throughout the entire trial process. Prior to the study, we will organize an intensive trial training to ensure that all researchers fully understand the trial protocol, standard operating procedures, and their corresponding roles—for example, all outcome assessors will be trained to perform outcome assessments and fill in the case report forms (CRFs) uniformly. All involved licensed acupuncturists are required to have at least 10 years of clinical experience and will be trained in acupuncture procedure to reduce operation bias as much as possible, especially in positioning of acupoints and acupuncture manipulations.
During the study, we will periodically inspect the implementation of the trial to minimize the occurrence of AEs or complications as much as possible. The reason for dropout or withdrawal will be documented in CRFs. A third-party data safety monitoring committee will be employed to monitor the reliability of the data. They have the right to verify the authenticity and consistency between raw data and recorded data. Meanwhile, all major investigators will organize periodical meetings to discuss issues that will arise during the trial and figure out the best solutions. Moreover, in order to promote patient enrollment, all acupuncture treatment costs will be free for the included participants.
At follow-up visits, economic compensation and health education will be adopted to improve patient compliance and reduce dropouts during a long period of 16-week follow-ups.
Power Analysis and Sample Size for Windows (NCSS, Kaysville, Utah, USA; PASS version 15.0) software is used to calculate the required sample size. Owing to the lack of previously published relevant RCTs, the sample size calculation is estimated based on the results of our pilot study. The participants will be divided into two groups in a 1:1 ratio. It is assumed that the mean of the number of vertigo days at 8 weeks after intervention will be 2.2 in the acupuncture group and 3.3 in the control groups, with a pooled standard deviation of 1.54. Given a difference in vertigo days of 1.1 between the two groups and a statistical power of 0.8 to reject a null effect at the 0.05 significance level, the required sample size of each group is 31. Considering an estimated attrition rate of 15%, each group will include 36 initial participants; thereby, a total of 72 participants are needed.
Statistical software package SPSS19.0 (SPSS Inc., Chicago, IL, USA) will be adopted to conduct the statistical analysis. The statistical analysis will be conducted based on the intention-to-treat principle by third-party statisticians who are blinded to the group allocation and intervention process. Missing data will be imputed by the last-observation-carried-forward method.
Regarding categorical data, these will be displayed as counts and percentages. Numeric data with normal distribution will be expressed as mean ± standard deviations, while data with non-normal distribution will be expressed as median with 95% confidence intervals. For the data in normal distribution, repeated-measures analysis of variance (ANOVA) will be used to perform within-group and between-group comparison by assessing change in continuous variables before and after intervention at different time points, while non-parametric test will be adopted to conduct within-group and between-group comparison for data in on-normal distribution. All hypothesis tests will be bilateral, with p-value <0.05 considered statistically significant.
To date, there has not been a universally approved treatment for VM treatment, and VM remains difficult to manage by current treatment options (37). Thus, it is critical to seek an effective and safe non-pharmacological therapy for VM prophylaxis, which can improve the quality of life of VM patients and reduce the side effects of pharmacotherapies and medical expense. On one hand, increasing the trials has favored the therapeutic effect of acupuncture for treating the major symptoms [i.e., vertigo/dizziness (13, 25) and migraine (14, 15)] and common comorbidities [e.g., anxiety (16) and depression (17)] of VM. On the other hand, although the pathogenesis of VM remains inconclusive, it is not only related to the central system but also a kind of recurrent peripheral vestibular disorders (9, 38). Emerging studies (18, 19) have also revealed that VM is related to the dysfunction of the connection between the trigeminal–vestibular–vagus nerves, and cumulative evidence demonstrates that acupuncture can relieve the symptoms of patients via mediating neural plasticity (20). In this scenario, acupuncture may be a potential treatment option for VM prophylaxis, but current evidence remains insufficient. Therefore, the present protocol of a RCT aims to investigate the efficacy and safety of acupuncture in the prophylactic treatment of VM patients, which is the first RCT in the acupuncture field.
Given that the acupoint selection has a close correlation with the efficacy maximization of acupuncture, the acupoint prescription of our study is carefully schemed. The rationales for the acupoint prescription are mainly based on consensus with experienced acupuncture experts, which are highly overlapping with those adopted in previously published trials involving acupuncture for treating migraine (15), vertigo/dizziness (13), and emotional disorders (16, 17). The acupoint selection in our study targets at alleviating major symptoms (i.e., migraine and vertigo/dizziness) and common comorbidities (i.e., emotional disorders) in VM patients, given that VM affects both the central and peripheral parts of the nervous system and previous studies revealed that Du meridian plays a vital role in treating various nervous system diseases (39, 40), including vertigo and headache. Accordingly, one important part of our acupoint prescription is to select acupoints of Du meridian [i.e., Baihui (DU20), Qianding (DU21)]. Meanwhile, migraine is one of the major symptoms of VM, and according to the theory of TCM, migraine belongs to shaoyang headache, which is corresponding to the gallbladder meridian. Thus, acupoints located in the gallbladder meridian [i.e., Fengchi (GB20), Shuaigu (GB8)] are another important part of our acupoint prescription. Moreover, a great number of experimental and clinical trials reveal the therapeutic effect of acupoints on Du meridian and gallbladder meridian, such as Baihui (DU20) (41) and Fengchi (GB20) (42), for relieving vertigo and migraine, which are two major symptoms in VM patients. In addition, the remaining acupoints [e.g., Yintang (EX-HN3), Neiguan (PC6), Shenmen (HT7), and Taichong (LR3)] are selected to treat clinical symptoms related to psychological disorders, which are common comorbidities in VM patients.
As the controlled arm, venlafaxine is a drug classified as serotonin and norepinephrine reuptake inhibitors, which is widely used to treat depression (43). In recent years, the results of increasing RCTs have favored the efficacy of venlafaxine in the prophylaxis of VM (44). Therefore, we compare the efficacy and safety of acupuncture with venlafaxine, which is chosen as a standard drug therapy in the control group.
It is noteworthy that, owing to two major considerations, sham acupuncture is not selected as the control arm in our study. First, given that acupuncture is very popular and widely used in the hospital that recruited the participants, the overwhelming majority of the study subjects have accumulated a rich experience of acupuncture, which makes successful participant blinding very difficult even if a sham acupuncture group is adopted. Second, despite the fact that sham acupuncture remains to be identified as the method of controlling acupuncture to blind the study subjects and control the non-specific placebo effects, distinguishing between the specific and non-specific effects of acupuncture via sham control seems to be impossible. Until now, mimicking acupuncture without any physiological activity is still impractical. Many studies indicate that all currently available modalities of sham acupuncture (regarding penetrating or non-penetrating) are not absolutely inert and have positive treatment effects (45–47). In this case, the overall therapeutic effect of acupuncture may be greatly underestimated if it is compared with sham acupuncture, especially in trials that aim to evaluate the effect of acupuncture for treating pain conditions (48). Therefore, some scholars debate that the complex and multi-element characteristics of acupuncture doom the design of sham acupuncture and that the great effort to control the psychological (non-specific) factors through currently available modalities of sham acupuncture might be unnecessary and unsuccessful (49). In this scenario, we do not set up a sham acupuncture group as the control in our study.
There are several limitations of our study. First, with a lack of objective measurement indicators, till now the diagnostic criteria of VM have been relatively subjective. Meanwhile, its major clinical feature of vertigo is a very subjective symptom; a lot of patients cannot describe it clearly, especially old people, thereby making it difficult to diagnose and judge a therapeutic effect. These factors will have an impact on participant inclusion and outcome assessments. Second, given that there is great lack of previously published relevant RCTs, our sample size is estimated according to our pilot study. Nevertheless, our trial will provide effect size data for sample size calculations of future large-scale RCTs. Third, although sham acupuncture is not adopted as the control, owing to the aforementioned considerations, the psychological (non-specific) effect of acupuncture in treating VM cannot be completely eliminated, owing to the lack of sham acupuncture. Thus, when the trial is finished and the results are interpreted, particular considerations should be given to the psychological (non-specific) effects of acupuncture that may influence the treatment effect.
The first participant was included in January 2021, and it is expected to complete in December 2023.
The studies involving human participants were reviewed and approved by The First Affiliated Hospital of Jiaxing University. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
TH is responsible for this study. TH and JH designed the trial protocol and drafted the manuscript. HH, FC, and JH revised the manuscript. BJ and FS planned a data analysis solution. YS and MY participated in the recruitment. All authors have read, revised, and approved this version of the manuscript.
The trial is financially supported by the Project of Zhejiang Administration of Traditional Chinese Medicine (grant no. 2021ZQ084), Key Discipline of Traditional Chinese Medicine of Jiaxing (grant no. 2019XK-B01), 13th Five-Year Key Specialty of Traditional Chinese Medicine of Zhejiang Province, and the Project of Jiaxing Science and Technology Bureau (grant no. 2019AD32180). The funders do not participate in the design, execution, and writing of the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.709803/full#supplementary-material
1. Sohn JH. Recent advances in the understanding of vestibular migraine. Behav Neurol. (2016) 2016:1–9. doi: 10.1155/2016/1801845
2. Cass SP, Ankerstjerne JKP, Yetiser S, Furman J, Balaban C, Aydogan B. Migraine-related vestibulopathy. Ann Otol Rhinol Laryngol. (1997) 106:182–9. doi: 10.1177/000348949710600302
3. Neuhauser H, Leopold M, von Brevern M, Arnold G, Lempert T. The interrelations of migraine, vertigo, and migrainous vertigo. Neurology. (2001) 56:436–41. doi: 10.1212/WNL.56.4.436
4. Lempert T, Olesen J, Furman J, Waterston J, Seemungal B, Carey J, et al. Vestibular migraine: diagnostic criteria: consensus document of the Bárány Society and the International Headache Society. Der Nervenarzt. (2013) 84:51–16. doi: 10.1007/s00115-013-3768-x
5. Van Ombergen A, Van Rompaey V, Van de Heyning P, Wuyts F. Vestibular migraine in an otolaryngology clinic: prevalence, associated symptoms, and prophylactic medication effectiveness. Otol Neurotol. (2015) 36:133–8. doi: 10.1097/MAO.0000000000000596
6. Tungvachirakul V, Lisnichuk H, O'Leary SJ. Epidemiology of vestibular vertigo in a neuro-otology clinic population in Thailand. J Laryngol Otol. (2014) 128(Suppl 2):S31–8. doi: 10.1017/S0022215113003484
7. Dieterich M, Obermann M, Celebisoy N. Vestibular migraine: the most frequent entity of episodic vertigo. J Neurol. (2016) 263:82–9. doi: 10.1007/s00415-015-7905-2
8. Shin CH, Kim Y, Yoo MH, Kim TS, Park JW, Kang BC, et al. Management of ménière's disease: how does the coexistence of vestibular migraine affect outcomes? Otol Neurotol. (2019) 40:666–73. doi: 10.1097/MAO.0000000000002176
9. Yuan Q, Yu L, Shi D, Ke XX, Zhang H. Anxiety and depression among patients with different types of vestibular peripheral vertigo. Medicine. (2015) 94:e453. doi: 10.1097/MD.0000000000000453
10. Kim SK, Kim YB, Park IS, Hong SJ, Kim H, Hong SM. Clinical analysis of dizzy patients with high levels of depression and anxiety. J Audiol Otol. (2016) 20:174–8. doi: 10.7874/jao.2016.20.3.174
11. Law S, Derry S, Moore RA. Sumatriptan plus naproxen for the treatment of acute migraine attacks in adults. Cochrane Database Syst Rev. (2016) 4:Cd008541. doi: 10.1002/14651858.CD008541.pub3
12. Yu SY, Wan Q, Wang WQ, Liu B, Li MX, Wu ZM, et al. Expert consensus on the diagnosis and treatment of vestibular migraine of China (2018). Chinese J Pain Med. (2018) 24:481–8. doi: 10.3969/j.issn.1006-9852.2018.07.001
13. Jiao JH, Li YJ, Peng TQ, Xia MX, Chen HD. Acupuncture points stimulation for Meniere's disease/syndrome: a promising therapeutic approach. Evid Based Complement Alternat Med. (2016) 2016:6404197. doi: 10.1155/2016/6404197
14. Wang LP, Zhang XZ, Guo J, Liu HL, Zhang Y, Liu CZ, et al. Efficacy of acupuncture for acute migraine attack: a multicenter single blinded, randomized controlled trial. Pain Med. (2012) 13:623–30. doi: 10.1111/j.1526-4637.2012.01376.x
15. Ling Z, Jiao C, Ying L, Sun X, Chang XR, Zheng H, et al. The long-term effect of acupuncture for migraine prophylaxis a randomized clinical trial. JAMA Intern Med. (2017) 177:508–15. doi: 10.1001/jamainternmed.2016.9378
16. Amorim D, Amado J, Brito I, Fiuza SM, Amorim N, Costeira C, et al. Acupuncture and electroacupuncture for anxiety disorders: a systematic review of the clinical research (2018). Complement Ther Clin Pract. (2018) 31:31–7. doi: 10.1016/j.ctcp.2018.01.008
17. Armour M, Smith CA, Wang LQ, Naidoo D, Yang GY, MacPherson H, et al. Acupuncture for depression: a systematic review and meta-analysis. J Clin Med. (2019) 8:1140. doi: 10.3390/jcm8081140
18. Beh SC, Friedman DI. Acute vestibular migraine treatment with noninvasive vagus nerve stimulation. Neurology. (2019) 93:e1715–9. doi: 10.1212/WNL.0000000000008388
19. Beh SC. Nystagmus and vertigo in acute vestibular migraine attacks: response to non-invasive vagus nerve stimulation. Otol Neurotol. (2021) 42:e233–6. doi: 10.1097/MAO.0000000000002892
20. Xiao L, Wang X, Ye Y, Yang JW, Cao Y, Ma SM, et al. Applications of acupuncture therapy in modulating plasticity of central nervous system. Neuromodulation. (2018) 21:762–76. doi: 10.1111/ner.12724
21. Hu TY, Zhang AJ, Jiang B, Shen FF, Hu J. Is acupuncture effective and safe for prophylaxis of vestibular migraine? A protocol for systematic review and meta-analysis. Medicine. (2020) 99:e23533. doi: 10.1097/MD.0000000000023533
22. Svenkerud S, MacPherson H. The impact of STRICTA and CONSORT on reporting of randomised control trials of acupuncture: a systematic methodological evaluation. Acupunct Med. (2018) 36:349–57. doi: 10.1136/acupmed-2017-011519
23. Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, KrleŽa-Jerić K, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. (2013) 158:200–7. doi: 10.7326/0003-4819-158-3-201302050-00583
24. Lempert T, Olesen J, Furman J, Waterston J, Seemungal B, Carey J, et al. Vestibular migraine: diagnostic criteria. J Vestib Res. (2012) 22:167–72. doi: 10.3233/VES-2012-0453
25. Hou ZZ, Xu SB, Li QL, Cai LB, Wu WG, Yu HD, et al. The efficacy of acupuncture for the treatment of cervical vertigo: a systematic review and meta-analysis. Evid Based Complement Alternat Med. (2017) 2017:7597363. doi: 10.1155/2017/7597363
26. Lim S. WHO standard acupuncture point locations. Evid Based Complement Alternat Med. (2010) 7:167–8. doi: 10.1093/ecam/nep006
27. Liu F, Ma T, Che X, Wang Q, Yu S. The efficacy of venlafaxine, flunarizine, and valproic acid in the prophylaxis of vestibular migraine. Front Neurol. (2017) 8:524. doi: 10.3389/fneur.2017.00524
28. Wyngaerde K, Lee MK, Jacobson GP, Pasupathy K, Romero-Brufau S, McCaslin DL, et al. The component structure of the dizziness handicap inventory (DHI): a reappraisal. Otol Neurotol. (2019) 40:1217–23. doi: 10.1097/MAO.0000000000002365
29. Heller GZ, Manuguerra M, Chow R. How to analyze the visual analogue scale: myths, truths and clinical relevance. Scand J Pain. (2016) 13:67–75. doi: 10.1016/j.sjpain.2016.06.012
30. Lee JJ, Lee MK, Kim JE, Kim HZ, Park SH, Tae JH, et al. Pain relief scale is more highly correlated with numerical rating scale than with visual analogue scale in chronic pain patients. Pain Physician. (2015) 18:e195–200. doi: 10.36076/ppj/2015.18.E195
31. Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzoget W, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. (2008) 46:266–74. doi: 10.1097/MLR.0b013e318160d093
32. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
33. Martin A, Rief W, Klaiberg A, Breahler E. Validity of the Brief Patient Health Questionnaire Mood Scale (PHQ-9) in the general population. Gen Hosp Psychiatry. (2006) 28:71–7. doi: 10.1016/j.genhosppsych.2005.07.003
34. Levis B, Benedetti A, Thombs BD, DEPRESsion Screening Data (DEPRESSD) Collaboration. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. (2019) 365:l1476. doi: 10.1136/bmj.l1476
35. Patel AA, Donegan D, Albert T. The 36-item short form. J Am Acad Orthop Surg. (2007) 15:126–34. doi: 10.5435/00124635-200702000-00007
36. Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: scoping review. SAGE Open Med. (2016) 4:2050312116671725. doi: 10.1177/2050312116671725
37. Nowaczewska M. Vestibular migraine - an underdiagnosed cause of vertigo. Diagnosis and treatment. Neurol Neurochir Pol. (2020) 54:106–15. doi: 10.5603/PJNNS.a2020.0031
38. Strupp M, Dlugaiczyk J, Ertl-Wagner BB, Rujescu D, Westhofen M, Dieterich M. Vestibular disorders. Dtsch Arztebl Int. (2020) 117:300–10. doi: 10.3238/arztebl.2020.0300
39. Su X, Wu Z, Mai F, Fan ZY, Du SJ, Qian H, et al. Governor vessel-unblocking and mind-regulating acupuncture therapy ameliorates cognitive dysfunction in a rat model of middle cerebral artery occlusion. Int J Mol Med. (2019) 43:221–32. doi: 10.3892/ijmm.2018.3981
40. Xia KP, Pang J, Li SL, Zhang M, Li HL, Wang YJ. Effect of electroacupuncture at governor vessel on learning-memory ability and serum level of APP, Aβ1-42 in patients with Alzheimer's disease. Chin Acupunct Moxibuction. (2020) 40:375–8. doi: 10.13703/j.0255-2930.20190728-0003
41. Zhao L, Ren YL, Liang FR. Analysis of characteristics of meridians and acupoints selected for training migraine in past dynasties based on date excavation. Chin Acupunct Moxibuction. (2009) 29:467–2. doi: 10.13703/CNKI:SUN:ZGZE.0.2009-06-023
42. Li SF, Huang JH, Lin ZP, Chen XZ, Lin DN, Lu P, et al. Infraoccipital needle-knife for cervical vertigo. Chin Acupunct Moxibuction. (2017) 37:297–300. doi: 10.13703/j.0255.2930.2017.03.021
43. Barbui C, Butler R, Cipriani A, Geddes J, Hatcher S. Depression in adults: drug and physical treatments. BMJ Clin Evid. (2007) 2007:1003. doi: 10.1016/j.aim.2008.01.011
44. Feng ZW, Jiao QW, Yu MC, Xu ZX. Serotonin–norepinephrine reuptake inhibitors for the prevention of migraine and vestibular migraine: a systematic review and meta-analysis. Reg Anesth Pain Med. (2020) 45:323–30. doi: 10.1136/rapm-2019-101207
45. Koog YH. Effect of placebo acupuncture over no-treatment: a simple model incorporating the placebo and nocebo effects. Complement Ther Med. (2016) 24:69–72. doi: 10.1016/j.ctim.2015.12.007
46. Chae Y, Lee YS, Enck P. How placebo needles differ from placebo pills? Front Psychiatry. (2018) 9:243. doi: 10.3389/fpsyt.2018.00243
47. Lee YS, Chae Y. Powerful effects of placebo needles. Acupunct Med. (2018) 36:197–8. doi: 10.1136/acupmed-2017-011516
48. Hu HT, Hu TY, Han DX, Gao H. Establishment of appropriate sham acupuncture and successful patient blinding. Acupunct Med. (2021) 39:159–60. doi: 10.1177/0964528420924035
Keywords: vestibular migraine, acupuncture, prophylaxis, randomized controlled trial, protocol
Citation: Hu T, Hu H, Chen F, Jiang B, Shen F, Su Y, Yang M and Hu J (2021) The Efficacy and Safety of Acupuncture for Prophylaxis of Vestibular Migraine: A Study Protocol for a Randomized Controlled Trial. Front. Neurol. 12:709803. doi: 10.3389/fneur.2021.709803
Received: 14 May 2021; Accepted: 07 June 2021;
Published: 15 July 2021.
Edited by:
Aynur Özge, Mersin University, TurkeyReviewed by:
Pinar Yalinay Dikmen, Acibadem University, TurkeyCopyright © 2021 Hu, Hu, Chen, Jiang, Shen, Su, Yang and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Feng Chen, bWFyZ2FyZXRfaHR5QGZveG1haWwuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.