 Keiko Niimi
Keiko Niimi Ayataka Fujimoto
Ayataka Fujimoto Hideo Enoki
Hideo Enoki
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Neurol. , 04 May 2021
Sec. Epilepsy
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.677828
This article is part of the Research Topic The Comorbid Anxiety and Depression Disorder in Patients with Epilepsy: Diagnosis, Prevention and Treatment View all 15 articles
Introduction: Our hypothesis in this study was that differences might exist between patients with epilepsy (PWE) who underwent epilepsy surgery before and within the period of the coronavirus disease 2019 (COVID-19) pandemic. The purpose of this study was to compare results of the Zung Self-Rating Depression Scale (SDS) between PWE who underwent epilepsy surgery before and during the pandemic period.
Methods: Participants were PWE who underwent open cranial epilepsy surgery between February 2019 and February 2021 in our hospital. Patients who underwent surgery in the first half of this period, between February 2019 and January 2020, were defined as the pre-pandemic period group (pre-Group) and those treated in the second half, between February 2020 and February 2021, were categorized as the pandemic period group (within-Group). All patients completed the SDS before surgery, and scores were compared between groups.
Results: SDS score was significantly higher in the pre-Group than in the within-Group (p = 0.037). Other factors, including age (p = 0.51), sex (p = 0.558), epilepsy duration from onset to SDS score evaluation (p = 0.190), seizure frequency (p = 0.794), number of anti-seizure medications (p = 0.787), and intelligence quotient (p = 0.871) did not differ significantly between groups.
Conclusion: SDS score was higher in the pre-pandemic group than in the within-pandemic group, which may indicate that PWE with less-positive outlooks may be less likely to seek medical attention during stressful periods.
- PWE who underwent surgery during the pandemic period showed less depressive symptoms.
- PWE with depressive tendencies might be at risk during stressful periods.
- Technology might offer hope for PWE showing depressive tendencies.
The coronavirus disease 2019 (COVID-19) pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) started in 2019, and has shown three peaks in Japan since the beginning of 2020.
Previously, as pandemics in the 20th century, we experienced the Spanish flu, acquired immunodeficiency syndrome (AIDS) and highly pathogenic avian influenza viruses (1–4). However, in the 21st century, the frequency of epidemics seems to have increased markedly (5–9). Regardless of the cause, the possibility of pandemics occurring more frequently in the near future must naturally be considered.
Patients with epilepsy (PWE) are known to have been suffering during the calamity of COVID-19 due to anxiety and depression (10). In particular, PWE with surgically remediable epilepsy are known to be vulnerable to psychiatric disturbance before and after surgery, even when societal calamities are not present. Since the adequate treatment of psychiatric comorbidities increases the likelihood of seizure freedom and optimizes the psychosocial benefits afforded by epilepsy surgery (11), provision of psychological care to PWE must be a priority. At the same time, continuity of treatment for PWE is also necessary. The idea of continuing business functions in society has already been described in 2012 by the International Organization for Standardization (ISO) as ISO22301 (https://www.iso.org/standard/75106.html). This ISO standard describes how to continually manage business in an organization to protect against the occurrence of disruptive incidents. These underlying principles are also applicable to healthcare businesses and our hospital follows this standard.
We have already described a retrospective study showing the importance of local interdisciplinary care for PWE (12). We have also shown that SARS-CoV-2 did not influence the volume of epilepsy surgeries in our facility (13). From these efforts, approaches to the calamity from the healthcare perspective might improve such negative situations for PWE. However, in the real world, worsening of seizure frequency and postponement of medical examinations are commonplace experiences for many PWE during the COVID-19 pandemic (14). If many PWE postponed adequate medical treatments during the pandemic, psychological differences might exist between PWE who did not postpone treatments and underwent epilepsy surgery during the pandemic and PWE who underwent epilepsy surgery before the pandemic.
Our hypothesis for the present study was thus that psychological differences might exist between PWE who underwent epilepsy surgery before and during the COVID-19 pandemic. The purpose of this study was to compare results from a depression scale among PWE who underwent epilepsy surgery before and during the COVID-19 pandemic.
The ethics committee at Seirei Hamamatsu General Hospital, Japan, approved the protocol for this retrospective study (approval no. 3578), which was performed in accordance with the principles of the Declaration of Helsinki. Subjects in this study were identified from a review of the electronic medical records for patients who had undergone epilepsy surgery between February 2019 and February 2021 in the Comprehensive Epilepsy Center at Seirei Hamamatsu General Hospital.
We collected information from patients who underwent epilepsy surgery between February 2019 and February 2021, as the first half of this period between February 2019 and January 2020 was pre-pandemic and the second half between February 2020 and February 2021 was just within the pandemic period in Japan. Patient age was recorded at the time of depression scale evaluation.
Data were obtained from all 32 patients who underwent open cranial epilepsy surgery for medically intractable epilepsy between February 2019 and February 2021 in our hospital. Among this population, inclusion criteria were: (1) age ≥18 years at evaluation, as the depression scale used was the Zung Self-Rating Depression Scale [SDS], which is adapted for individuals ≥18 years old (15); and (2) full intelligence quotient (IQ) ≥60. Among this population, exclusion criteria were: (1) patients who had undergone vagus nerve stimulation (VNS) therapy; and (2) patients who exhibited psychogenic non-epileptic seizures (PNES) (16) or other non-stereotypical activities.
As intellectual disorder and depression are sometime difficult to differentiate, such as in depressive cognitive disorders (17), patients with more than moderate intellectual disorder were allowed to enroll in this study. As VNS therapy has antidepressant effects (18), patients with VNS devices were excluded. All patients underwent long-term video electroencephalography and stereotypical epileptic seizures were captured. Based on the stereotypical seizure semiology, PWE who had experienced non-stereotypical activities were excluded because these non-stereotypical activities were regarded as possible PNES or non-epileptic events.
The SDS test is a 20-item self-reported questionnaire in common use as a screening tool, covering affective, psychological, and somatic symptoms associated with depression. The questionnaire takes 5–10 min to complete, and items are framed in terms of positive and negative statements. The total score is derived as the sum of scores for the individual item scores, ranging from 20 to 80. Patients who undergo epilepsy surgery in our institution undergo SDS before the surgery. We divided the enrolled patients into two groups: those who underwent surgery in the first half of the period, categorized as during the pre-pandemic period group between February 2019 and January 2020 (pre-Group); and those who underwent surgery in the second half of the period, categorized as during the pandemic period between February 2020 and February 2021 (within-Group). We compared SDS scores between these two groups.
We also compared seizure frequency, duration from onset to SDS score evaluation, and number of anti-seizure medications (ASMs) between the pre-Group and within-Group. Seizure frequency was classified as: (1) daily; (2) weekly; (3) monthly; or (4) yearly. These secondary outcomes were chosen as factors potentially related to anxiety or depressive disorders (19).
The Mann-Whitney U-test and Student's t-test were used in this study, as appropriate. Statistical significance was set at the level of p < 0.05. Analyses were conducted using Sigma plot (Systat Software, San Jose, CA, USA).
Clinical information and results of the SDS are shown in Table 1.
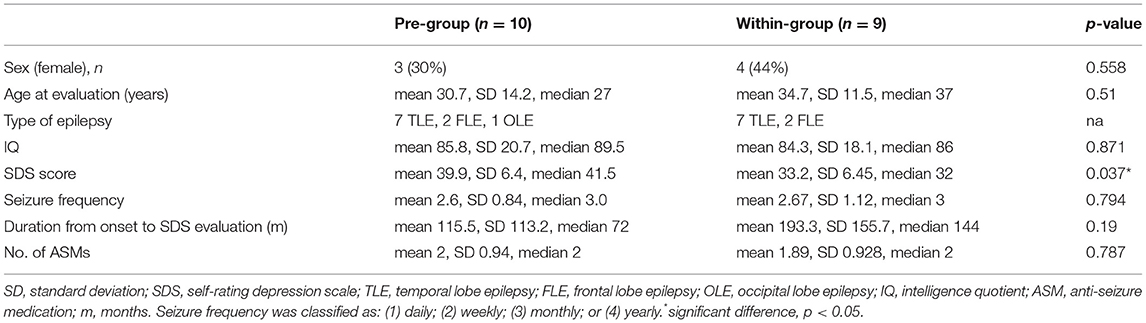
Table 1. Clinical information and SDS scores.
Seven female PWE and 12 male PWE (mean age at evaluation, 32.6 years; median age, 35.0 years; range, 18–59 years; standard deviation, 12.8 years; confidence interval of the mean, 6.16 years) fulfilled the inclusion criteria. None of the patients exhibited PNES. Table 2 shows the ASMs used by the patients.

Table 2. Use of ASMs.
SDS scale score was significantly higher in the pre-Group than in the within-Group (p = 0.037). No other factors, including age (p = 0.51), sex (p = 0.558), or IQ (p = 0.871), showed significant differences between groups (Table 1).
Epilepsy duration from onset to SDS score evaluation (p = 0.190), seizure frequency (p = 0.794), and number of ASMs (p = 0.787) all showed no significance differences between groups (Table 1).
SDS scale score was significantly higher in the pre-Group than in the within-Group. Even though scores were not within the diagnostic range for depression, the pre-Group was relatively closer to the range for depressive symptoms than the within-Group. This might be because PWE with a more positive outlook were less likely to put off epilepsy surgery even during the pandemic period.
Rayner and Wilson (11) reported that a less compromised psychiatric profile may contribute to better outcomes of epilepsy surgery. Even though we did not provide special treatments for psychiatric comorbidities for enrolled PWE, the fact that PWE with a less negative outlook underwent epilepsy surgery during the pandemic in this study might partially support this theory by Rayner and Wilson. Given the disaster-preparedness measures taken by our facility, the continuity plan might have worked. As Japan experiences relatively frequent disasters, such as earthquakes, typhoons, and floods, many facilities in Japan might prepare for such disruptive events. The other effort was that as our local interdisciplinary system for epilepsy treatment became established (13), the flow cycle for PWE among local general physicians and our epilepsy center was able to be maintained. Based on these approaches to the calamity that might be decreasing psychological stresses among surgical candidates, thereby improving such negative situations for PWE, epileptologists might not hesitate to perform epilepsy surgery even during a pandemic.
Conversely, about 30% of PWE are considered to have depressive symptoms (20). Many of these patients might be more strongly influenced by psychological factors than by the epilepsy itself (21). From our results and those of previous reports, the possibility should be considered that some PWE might neglect beneficial advanced medical care such as epilepsy surgery under disruptive situations.
As interventions in medical treatments, including for epilepsy, have a certain order of priority (22), some PWE might be classified as having non-urgent disorders (23), despite they might have severe conditions such as COVID-19-related status epilepticus (24). However, using advanced technologies such as telemetry (10, 25), home-video recordings (26) and tele-neuropsychology tests (27) should be implemented to maximize efficient provision of appropriate medical interventions.
A key limitation of this study was the small number of PWE in each group. However, the suggestion that some PWE might be neglected under various circumstances is important and worth exploring further in future work.
SDS scores obtained from multiple centers before and during the pandemic and other societal circumstances should be analyzed in future investigations.
SDS score was higher in the pre-pandemic group than in the within-pandemic group, which may indicate that PWE with less-positive outlooks may be less likely to seek medical attention during periods of societal or personal stress.
The original contributions generated for this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by The ethics committee of Seirei Hamamatsu General Hospital. The patients/participants provided their written informed consent to participate in this study.
KN, AF, HE, KS, and TO: acquisition of data. AF, TO, and HE: analysis and interpretation of data. AF: epilepsy surgery. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Landesman SH, Ginzburg HM, Weiss SH. The AIDS epidemic. N Engl J Med. (1985) 312:521–5. doi: 10.1056/NEJM198502213120829
2. Trilla A, Trilla G, Daer C. The 1918 “Spanish flu” in Spain. Clin Infect Dis. (2008) 47:668–73. doi: 10.1086/590567
3. Lai S, Qin Y, Cowling BJ, Ren X, Wardrop NA, Gilbert M, et al. Global epidemiology of avian influenza A H5N1 virus infection in humans, 1997–2015: a systematic review of individual case data. Lancet Infect Dis. (2016) 16:e108–18. doi: 10.1016/S1473-3099(16)00153-5
4. Aassve A, Alfani G, Gandolfi F, Le Moglie M. Epidemics and trust: the case of the spanish flu. Health Econ. (2021) 30:840–57. doi: 10.1002/hec4218
5. Dye C, Gay N. Modeling the SARS epidemic. Science. (2003) 300:1884–5. doi: 10.1126/science1086925
6. Fineberg HV. Preparing for avian influenza: lessons from the “swine flu affair”. J Infect Dis. (2008) 197:S14–8. doi: 10.1086/524989
7. Fung IC-H, Tse ZTH, Cheung C-N, Miu AS, Fu K-W. Ebola and the social media. Lancet. (2014) 384:2207. doi: 10.1016/S0140-6736(14)62418-1
8. Lowe R, Rodo X, Barcellos C, Carvalho MS, Coelho CA, Bailey TC, et al. Dengue Epidemic Early Warning System for Brazil. UNISDR Scientific and Technical Advisory Group. (2015).
10. Assenza G, Lanzone J, Brigo F, Coppola A, Di Gennaro G, Di Lazzaro V, et al. Epilepsy care in the time of COVID-19 pandemic in Italy: risk factors for seizure worsening. Front Neurol. (2020) 11:737. doi: 10.3389/fneur.202000737
11. Rayner G, Wilson SJ. Psychiatric care in epilepsy surgery: who needs it? Epilepsy Curr. (2012) 12:46–50. doi: 10.5698/1535-7511-12.246
12. Fujimoto A, Ichikawa N, Sato K, Nishimura M, Enoki H, Okanishi T. Inclusion of general physicians in the multidisciplinary treatment team for epilepsy may lead to an economic benefit. Epilepsy Behav. (2019) 95:56–60. doi: 10.1016/j.yebeh.2019.03041
13. Fujimoto A, Sato K, Enoki H. Change in patient flow in the epilepsy care network due to novel coronavirus infection: an opportunity to strengthen local interdisciplinary epilepsy care with general physicians. Front Neurol. (2020) 11:1467. doi: 10.3389/fneur.2020591423
14. Grande E, Tufo T, Ciavarro M, Di Muccio I, Fuggetta F, Silvestri M, et al. The impact of COVID-19 lockdown on people with epilepsy and vagal nerve stimulation. Front Neurol.. (2021) 12:181. doi: 10.3389/fneur.2021640581
15. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. (1965) 12:63–70. doi: 10.1001/archpsyc.196501720310065008
16. Anzellotti F, Dono F, Evangelista G, Di Pietro M, Carrarini C, Russo M, et al. Psychogenic non-epileptic seizures and pseudo-refractory epilepsy, a management challenge. Front Neurol. (2020) 11:461. doi: 10.3389/fneur.202000461
17. Sekhon S, Marwaha R. Depressive cognitive disorders. In: StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2021, StatPearls Publishing LLC. (2021).
18. Assenza G, Tombini M, Lanzone J, Ricci L, Di Lazzaro V, Casciato S, et al. Antidepressant effect of vagal nerve stimulation in epilepsy patients: a systematic review. Neurol Sci. (2020) 41:3075–84. doi: 10.1007/s10072-020-04479-2
19. Dehn LB, Pfäfflin M, Brückner S, Lutz MT, Steinhoff BJ, Mayer T, et al. Relationships of depression and anxiety symptoms with seizure frequency: Results from a multicenter follow-up study. Seizure. (2017) 53:103–9. doi: 10.1016/j.seizure.2017.11008
20. Tombini M, Assenza G, Quintiliani L, Ricci L, Lanzone J, Ulivi M, et al. Depressive symptoms and difficulties in emotion regulation in adult patients with epilepsy: Association with quality of life and stigma. Epilepsy Behav. (2020) 107:107073. doi: 10.1016/j.yebeh.2020107073
21. Tombini M, Assenza G, Quintiliani L, Ricci L, Lanzone J, Di Lazzaro V. Epilepsy and quality of life: what does really matter? Neurol Sci. (2021). doi: 10.1007/s10072-020-04990-6
22. Grippo A, Assenza G, Scarpino M, Broglia L, Cilea R, Galimberti CA, et al. Electroencephalography during SARS-CoV-2 outbreak: practical recommendations from the task force of the Italian Society of Neurophysiology (SINC), the Italian League Against Epilepsy (LICE), and the Italian Association of Neurophysiology Technologists (AITN). Neurol Sci. (2020) 41:2345–51. doi: 10.1007/s10072-020-04585-1
23. Abokalawa F, Ahmad SF, Al-Hashel J, Hassan AM, Arabi M. The effects of coronavirus disease 2019 (COVID-19) pandemic on people with epilepsy (PwE): an online survey-based study. Acta Neurol Belg. (2021) 1–8. doi: 10.1007/s13760-021-01609-1
24. Dono F, Nucera B, Lanzone J, Evangelista G, Rinaldi F, Speranza R, et al. Status epilepticus and COVID-19: a systematic review. Epilepsy Behav. (2021) 118:107887. doi: 10.1016/j.yebeh.2021107887
25. Kuchenbuch M, D'Onofrio G, Wirrell E, Jiang Y, Dupont S, Grinspan ZM, et al. An accelerated shift in the use of remote systems in epilepsy due to the COVID-19 pandemic. Epilepsy Behav. (2020) 112:107376. doi: 10.1016/j.yebeh.2020107376
26. Ricci L, Boscarino M, Assenza G, Tombini M, Lanzone J, Di Lazzaro V, et al. Clinical utility of home videos for diagnosing epileptic seizures: a systematic review and practical recommendations for optimal and safe recording. Neurol Sci. (2021) 42:1301–9. doi: 10.1007/s10072-021-05040-5
Keywords: Zung self-rating depression scale, pandemic, epilepsy surgery, COVID-19, SARS-CoV-2
Citation: Niimi K, Fujimoto A, Sato K, Enoki H and Okanishi T (2021) Patients With Epilepsy Who Underwent Epilepsy Surgery During the COVID-19 Pandemic Showed Less Depressive Tendencies. Front. Neurol. 12:677828. doi: 10.3389/fneur.2021.677828
Received: 08 March 2021; Accepted: 09 April 2021;
Published: 04 May 2021.
Edited by:
Giovanni Assenza, Campus Bio-Medico University, ItalyReviewed by:
Jacopo Lanzone, Sant'Isidoro Hospital Ferb Onlus Trescore Balneario, ItalyCopyright © 2021 Niimi, Fujimoto, Sato, Enoki and Okanishi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ayataka Fujimoto, YWZ1amltb3Rvc2NpZW5jZWFjYWRlbXlAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.