 Lingxin Cai
Lingxin Cai Hanhai Zeng†
Hanhai Zeng† Cong Qian
Cong Qian
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol., 03 June 2021
Sec. Stroke
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.671098
Aneurysmal subarachnoid hemorrhage (aSAH) is an important type of stroke with the highest rates of mortality and disability. Recent evidence indicates that neuroinflammation plays a critical role in both early brain injury and delayed neural deterioration after aSAH, contributing to unfavorable outcomes. The neutrophil-to-lymphocyte ratio (NLR) is a peripheral biomarker that conveys information about the inflammatory burden in terms of both innate and adaptive immunity. This review summarizes relevant studies that associate the NLR with aSAH to evaluate whether the NLR can predict outcomes and serve as an effective biomarker for clinical management. We found that increased NLR is valuable in predicting the clinical outcome of aSAH patients and is related to the risk of complications such as delayed cerebral ischemia (DCI) or rebleeding. Combined with other indicators, the NLR provides improved accuracy for predicting prognosis to stratify patients into different risk categories. The underlying pathophysiology is highlighted to identify new potential targets for neuroprotection and to develop novel therapeutic strategies.
Aneurysmal subarachnoid hemorrhage (aSAH) is the leading cause of death in stroke patients, with a mortality rate of ~40–50% (1, 2). More than 30% of survivors may develop severe disability and delayed neurological dysfunction due to complications such as delayed cerebral ischemia (DCI) and rebleeding (3). The progression of aSAH is individualized and rapid, so accurate risk stratification and prognosis prediction is challenging (4). A growing body of research has found that neuroinflammation and immune disorders after aSAH may play an important role in both early brain injury (EBI) and delayed neurological injury (5). Neutrophils and lymphocytes are vital inflammatory cells and participate in many pathogenic processes (6), such as endothelial injury, blood–brain barrier (BBB) destruction, microcirculation disturbance, and vasospasm (7). The dynamics of inflammatory cells and cytokines in the periphery can also contribute to systemic inflammatory response syndrome (SIRS) (8) and immunosuppression (9), which can perhaps increase the risk of infection (10).
The neutrophils-to-lymphocyte ratio (NLR) is a parameter that reflects inflammation and is regarded as a predictor of cardiovascular disease, pancreatitis, tumors, and other diseases (11). At present, several studies have shown that an increase in the NLR can predict adverse outcomes in patients with intracerebral hemorrhage (ICH) (12, 13). Because aSAH has a disease model similar to that of intracranial hemorrhage (14), the NLR may have the potential to assist in the prediction of the prognosis of aSAH.
The purpose of this review is to summarize existing evidence on the relationship between the NLR and aSAH and evaluate whether the NLR can be used to predict outcomes and as an effective biomarker for clinical management. We will also provide important insights into the underlying pathophysiological mechanisms and discuss the limitations of the current studies to make recommendations for future research.
After aneurysm rupture, the blood enters the subarachnoid space and spreads to the brain through the cerebrospinal fluid (CSF). Erythrocytes degrade and release many bioactive and potentially toxic molecules (15), destroying blood vessels and initiating an inflammatory cascade reaction (16). Inflammation regulated by complex pathways plays a pivotal role in both neurological impairment and destruction (17). Microglia are resident immune cells in the central nervous system (CNS) and react rapidly to inflammation-associated neurological injuries (18). When activated by toll-like receptor 4 (TLR4), microglia switch to a pro-inflammatory phenotype (M1) and secrete a large number of pro-inflammatory chemokines and cytokines, such as interleukin-6 (IL-6), interleukin-1β (IL-1β) (19), tumor necrosis factor-alpha (TNF-α), and nitric oxide (NO) (20). These inflammatory factors can increase the expression of specific cell adhesion molecules (CAMs) on the luminal surface of endothelial cells (ECs), recruit macrophages and neutrophils to bind ECs, and enter the CNS (21). After migrating to the subarachnoid space, neutrophils are essential in clearing extravascular hemoglobin through the Hp–Hgb complex, and this process is a response to hemorrhage that promotes neural stability and recovery (22, 23).
The acute neuroinflammatory response influences delayed events such as rebleeding and DCI after aSAH (24, 25). The recruitment of neutrophils and lymphocytes damages the blood vessel wall, resulting in the thinning of the aneurysm wall and coagulation dysfunction (26, 27). Recent studies have highlighted the role of the neuroinflammation of the microvasculature in DCI (28). Inflammation disrupts the balance between endogenous vasodilators and vasoconstrictors, especially the production of NO and endothelin-1 (29). This imbalance can increase lipid peroxidation of the cell membrane and direct oxidative stress in smooth muscle cells (30), causing microperfusion disorders and cerebral ischemic infarction (31). The interaction of neutrophils with platelets and vascular endothelium has also been demonstrated (32). Some clinical evidence shows that the increase of neutrophils in CSF indicates vascular injury and may be an independent predictor of vasospasm, indicating the risk of DCI (33, 34). Further studies have found additional pathogenic mechanisms, such as EBI and apoptosis, destruction of the BBB (35), micro thromboembolism (36), and cortical diffuse depolarization (37), which are more or less linked to inflammation.
Neutrophils migrate to the damaged brain tissue at the earliest stage and reach a peak in the early stage (24–48 h) (38). Neutrophils interact with activated ECs and play an important role in aggravating the inflammatory response, leading to the destruction of the BBB, brain edema, hypoperfusion, and nerve cell injury (39). Targeting neutrophil function could mitigate cerebral hypoperfusion (40, 41), and inhibition of neutrophil–endothelial interactions markedly decreased neuronal cell death and reduced secondary brain injury (42). The mechanism pathway involves inflammatory factors released by neutrophils, such as reactive oxygen species, cathepsin (43), matrix metalloproteinase-9 (MMP-9), and myeloperoxidase (MPO) (44). Neutrophils show significant procoagulant effects and aggravate the disturbance of the microcirculation (45).
The activation of inflammation and an increase in neutrophils also occur in the peripheral immune system (46, 47). The interruption of the BBB or the CSF drainage system may serve as a communication channel for inflammatory factors (48, 49). The peripheral activation of innate immune cells after aSAH is regulated by the sympathetic nervous system (SNS) and the hypothalamic–pituitary–adrenal (HPA) axis (50, 51). These changes in the peripheral inflammatory status and the resulting symptoms may manifest as SIRS (52). The occurrence of SIRS with common characteristics, like body temperature, heart rate, blood pressure, leukocytosis, and platelet activation, usually leads to continuous tissue hypoperfusion and damage to microcirculatory blood flow (53, 54). In return, systemic hyperinflammation provoked by maladaptive innate immunity may activate innate immune signaling pathways in the CNS, increasing BBB destruction (55).
Adaptive immunity is active in both the CSF and periphery after aSAH (56). Lymphocytes are found in the CNS after aSAH and are mainly involved in the protective mechanism against brain injury (57). Tregs play a key role in the elimination of inflammation and are the main brain-protective immunomodulator (58, 59). Tregs can reduce the inflammatory response by blocking the activation of the TLR4/nuclear factor-kappa B (NF-κB) signaling pathway, inducing the transformation of microglia toward a more favorable M2-like phenotype inhibiting the effect of neutrophil-derived MMP-9 to protect the integrity of the BBB and EC function (60, 61). The potent homeostatic function of Tregs in the peripheral immune system involves the inhibition of early immune overactivation that may result in an exhausted immune phenotype (62). In contrast, Th17 cells promote the inflammatory response (63) and are an important source of pro-inflammatory cytokines to aggravate brain injury (64).
A decrease in the total number of lymphocytes, especially Tregs, is found in aSAH patients (65). The profound loss of lymphocytes and the reduction of their activation are defined as pathophysiological immunosuppression, which is a long-lasting state that can last for several weeks and has a complex mechanism. The autonomic nervous system (ANS) and the SNS affect immune responses in the periphery and play a major role in immunosuppression (66). The stress response induced by injury activates the HPA axis and also leads to deficiency in the early activation of lymphocytes (67). Neutrophils release arginase 1 (ARG1), resulting in T-lymphocyte suppression in peripheral blood (68). Immunosuppression is also associated with changes in related cytokines released by lymphocytes, such as decreases in interferon-gamma (INF-γ) and interleukin-10 (IL-10) (69, 70). Lymphocytes are crucial for host defense against pathogens, and apparently, concomitant immunosuppression can increase vulnerability to systemic infection (71).
We reviewed relevant studies that associate NLR with aSAH to evaluate whether the NLR could serve as a biomarker to predict outcomes and be used as an effective biomarker for clinical management. A total of 11 studies assessed short- or long-term clinical outcomes according to the Modified Rankin Scale (mRS), early neurological deterioration, mortality, the occurrence of DCI, and other parameters. The synopses of the studies include the primary endpoint, inclusion criteria, and exclusion criteria, which are summarized in Table 1. The main characteristics of the patients enrolled in the studies are summarized in Table 2. The main conclusions are summarized in Table 3.
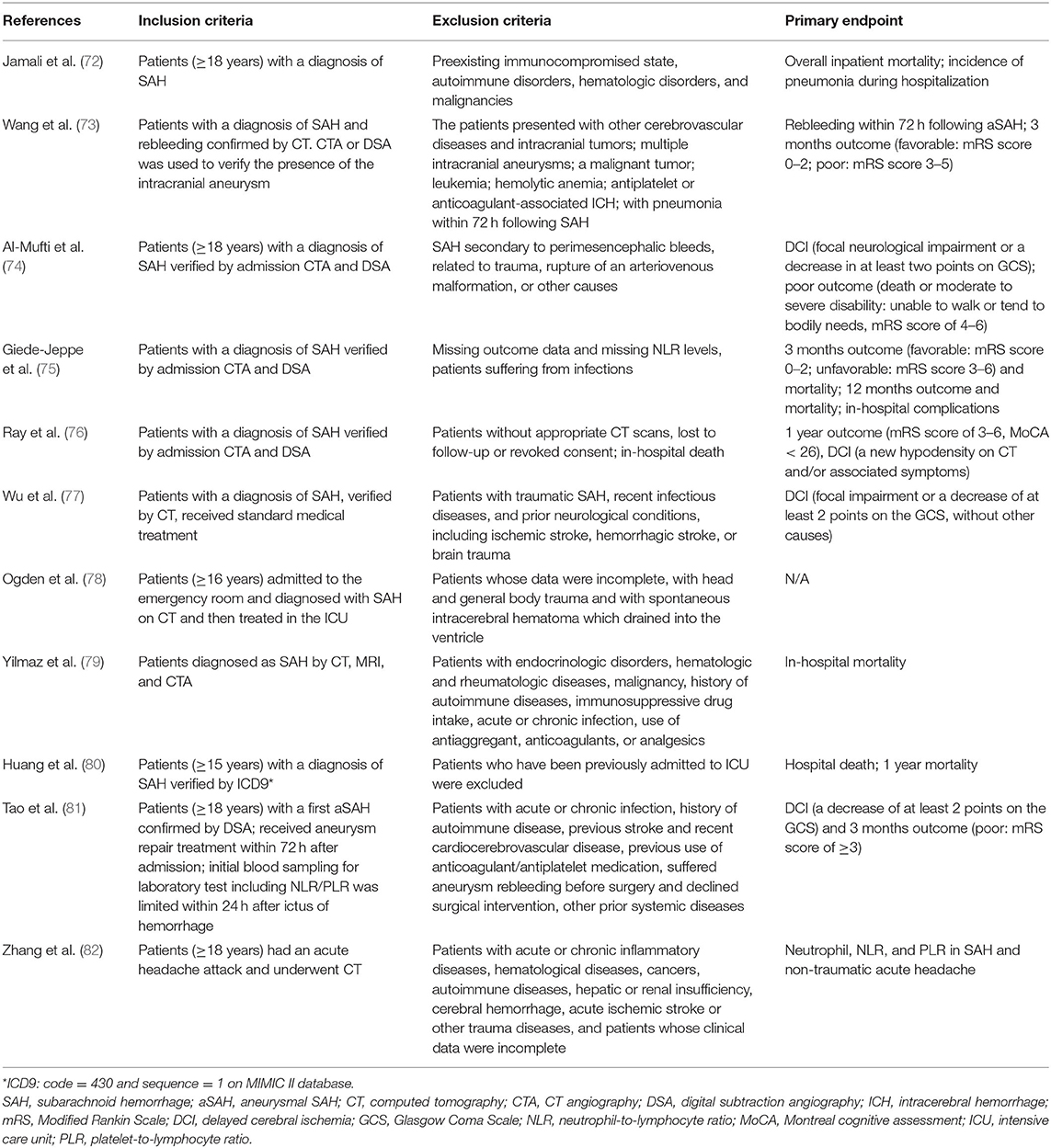
Table 1. Synopsis of the studies.
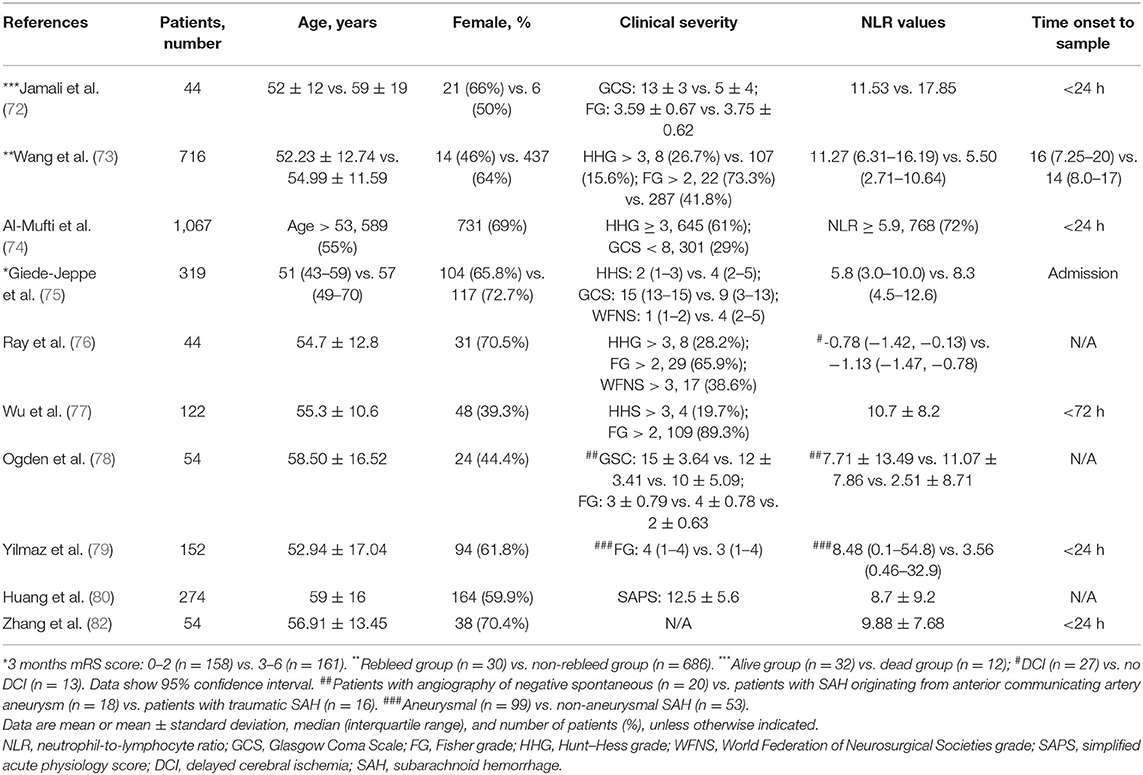
Table 2. Characteristics of the included patients.

Table 3. Synthesis of the main findings.
The relationship between the NLR and unfavorable clinical outcomes was investigated in a retrospective cohort study. Giede-Jeppe et al. described 319 patients in a tertiary inpatient center in Germany and recorded the mRS score at 3 and 12 months. It was found that the NLR value of patients with an unfavorable prognosis was significantly increased. After adjustment, the NLR remained an important factor in predicting unfavorable outcomes in patients. Through receiver operating characteristic (ROC) analysis, an NLR ≥7.05 was determined as the best cutoff value to predict unfavorable outcomes, which indicated an mRS score of 3–6 after 3 months (75). Wang et al. also found that there was a positive correlation between the NLR and the Hunt–Hess grade and that the NLR could predict the adverse outcomes of patients with an mRS score of 3–5 after 3 months (73). In a study that included 247 patients, the NLR was proven to be an independent predictor of adverse outcomes after 3 months, with a sensitivity of 74.5% and a specificity of 69.3% (81).
The NLR was also an independent marker of mortality in patients with aSAH. Huang et al. found that the increase in the NLR in intensive care unit (ICU) patients was significantly associated with hospital mortality and 1-year mortality (80). Jamali et al. found that the NLR value of patients who died in the hospital was significantly higher than that of surviving patients, and the in-hospital mortality rate of patients with an NLR ≥12.5 increased significantly. In this study, the effects of the absolute neutrophil count and absolute lymphocyte count on mortality were compared separately, and the results showed that there was no difference (72). Yilmaz et al. also found that the NLR was associated with the Fisher score and mortality and was a simple indicator of aSAH patient severity and short-term mortality (79).
The main complications of aSAH are DCI and rebleeding, which are common clinically and cause severe disability and delayed neurological dysfunction. A single-center, prospective, observational cohort study of 1,067 patients at Columbia University Medical Center demonstrated that the NLR on admission could predict the occurrence of DCI. They found that in the multivariate model, an increased NLR was associated with a poor Hess grade on admission, Caucasian race, the location of the anterior aneurysm, loss of consciousness at onset, and an increased bleeding volume (Fisher ≥ 3). After controlling for known predictors such as age, poor clinical grade on admission, bleeding volume, and mean arterial pressure on admission, the admission NLR could predict the occurrence of DCI, and an NLR ≥5.9 on admission predicted a 2-fold increase in the risk of DCI (74).
Wu et al. also found that the NLR may be a practical index to predict the occurrence of DCI in aSAH patients. They studied 122 patients, and 43 of them developed DCI during hospitalization and had an increased white blood cell count, neutrophil count, and NLR and a lower lymphocyte count. The NLR value was the most predictive variable among the four variables, and the best predictive value was 11.47. The sensitivity and specificity were 58.1 and 82.3%, respectively (77). The findings of Tao et al. also supported these results, as they found that an increased NLR was an independent factor that predicted the occurrence of DCI, with a sensitivity of 87.3% and a specificity of 48.4% (81). Ray et al. carried out further studies on the dynamics of the NLR and found that NLR trends showed a significant initial decline followed by a gradual rise among those without DCI, whereas the NLR was persistently low in those patients that developed DCI in an early immune-depressed state after aSAH (76).
The relationship between the NLR and rebleeding was proven as well. In a study that included 716 patients with aSAH, rebleeding occurred in 4.19% of patients. Univariate analysis showed that the NLR in patients with rebleeding was significantly higher than that in patients without rebleeding. In the multivariate analysis, the NLR and Fisher grade were risk factors for rebleeding. An increased NLR predicted the occurrence of rebleeding and poor prognosis after aSAH. In addition, a model combining the NLR and the Fisher grade was more valuable for predicting rebleeding than a single NLR or Fisher rating model, with a specificity of 100% (73).
The mortality rate of aSAH is quite high, and survivors are typically left with prolonged functional impairments, but accurate estimation of the prognosis of aSAH patients has been challenging (83). At present, the most important prognostic determinants for the aSAH outcome are the neurological grade on initial examination, radiographic results, and age (84, 85). However, subjective differences are inevitable in using the grading scales (86), and the sensitivity of the radiograph depends on the time interval between symptom occurrence and image acquisition (87). Researchers are hard-pressed to find new, feasible, and accurate evaluation and prediction methods.
Severe subarachnoid hemorrhage is associated with the strong early inflammatory response (88), and the most direct and easily observed result is the change in peripheral inflammatory biomarkers, such as the neutrophil and lymphocyte counts (89, 90). In general, an increase in neutrophils in peripheral blood is a manifestation of inflammation in the CNS and may be related to the development of extracerebral organ immune dysfunction. And SIRS associated with neutrophils is also related to poor clinical grade and independently predicts poor outcomes (91). A decrease in lymphocytes suggests the loss of neuroprotection and the impairment of native immunity with immunosuppression in the periphery (92). Therefore, NLR is a peripheral biomarker that conveys information about the inflammatory burden in terms of both innate and adaptive immunity and may fill the current lack of prognosis prediction.
It is understood that NLR is easy to utilize clinically without additional costs. As a ratio, the NLR remains more reliable and stable than a single blood parameter and is not affected by factors such as dehydration, overhydration, and blood sample treatment (93, 94). In addition, the NLR is more specific, multidimensional, and sensitive when slight changes in the inflammatory status of patients are difficult to detect (95). In conjunction with imaging results and the neurological grade, the NLR is of great value for the risk stratification process and the guidance of early prevention (96).
The complications of aSAH include rebleeding, DCI, hydrocephalus, increased intracranial pressure, and seizures (97). Previous studies have highlighted rebleeding and DCI, which contribute to high rates of disability and neurological dysfunction in survivors and are independent predictors of unfavorable outcomes (98). Rebleeding events are defined as a new hemorrhage apparent on repeat computed tomography (CT) with or without new symptoms and are viewed as the cerebrovascular equivalent of a second hit (99, 100). One of the causes of adverse clinical outcomes is the delayed diagnosis and treatment of rebleeding (101, 102). There is no sensitive and facile prediction method for prioritizing early treatment, such as early or ultra-early aneurysm repair and the use of antifibrinolytic drugs (103, 104). The NLR has been shown to predict the occurrence of rebleeding, which may be explained by the mechanism that neutrophil recruitment changes the stability of the ruptured aneurysm wall (73, 105). The present study on the NLR and rebleeding is limited but indicates potential predictors and new strategies for addressing neuroinflammation in rebleeding.
DCI generally occurs within 2 weeks after subarachnoid hemorrhage and is caused by cerebral perfusion defects (106), resulting in the deterioration of neurological function and a dramatically decreased quality of life in most survivors (107). The challenge is how to predict the occurrence of DCI and then formulate effective preventive strategies to reverse the development of DCI in advance (108). At present, four clinical studies have proven that the NLR is an independent prognostic factor for the occurrence of DCI with strong sensitivity and specificity (74, 76, 77, 81). This implies that the NLR is promising as a new predictor for DCI to help classify patients and direct preventive treatment to those who are most likely to benefit.
Increasing evidence shows that immune system disorders after aSAH and the risk of infection are increased (109). Immunosuppression induced by a significant decrease in peripheral lymphocytes is perhaps the vital reason for the increased risk of infection, especially in critically ill patients (110). Patients with SIRS also tend to become infected (111). Within 24 h after aSAH, an increase in the NLR may indicate the occurrence of intense early inflammation, which could develop into a strong late inflammatory response (112). Patients with a high NLR are more likely to develop pneumonia during hospitalization (113), and an NLR ≥5.9 is associated with pulmonary edema and high fever (74). The average number of neutrophils in patients with pneumonia is significantly increased (72). In particular, patients with DCI have a higher NLR and are more likely to be infected at a later stage (76). The NLR is an accessible indicator to evaluate immunity status and infection risk and can help adjust treatment strategies for preventing postoperative infectious complications (114).
Further study could focus on the comparison of the role of neutrophils and lymphocytes in different neurological diseases. Current studies have shown that NLR is associated with a variety of diseases, such as ischemic stroke, other ICH (115), and traumatic brain injury. A number of studies have shown that NLR was predictive of short-term functional outcome in acute ischemic stroke (AIS) (116). A high NLR was also found to be an independent predictor for the complications following AIS including cerebral edema (117), hemorrhagic transformation after ischemia (118), and the development of ICH after endovascular treatment (119).
Neuroinflammation is prevalent in these conditions and plays with similar mechanisms. In the early stage of both SAH and AIS, the activation of microglia by neutrophil is vital for following cascade of inflammation, with similar inflammatory mediators and pathways (120). Moreover, Tregs also play a major role in immunomodulatory function and neuroprotection after AIS (121). Valuable findings and breakthroughs may occur through comparing the similarities and differences of pathophysiological mechanisms about neuroinflammation among these medical conditions.
Furthermore, systematic and quantitative analyses of relevant clinical studies are needed to explore different levels and trends of NLR in multiple diseases, which could develop potential and guiding clinical applications. Ogden et al. studied patients in the neonatal intensive care unit (NICU) and found that the NLR was higher in aSAH than in traumatic subarachnoid hemorrhage (78). Eryigit et al. also found that the NLR can be used in distinguishing aSAH and migraine, with different levels and changes of NLR (122). The different cutoff values may be useful in specific classifications for etiologies.
NLR is proven to be a useful and potential tool in distinguishing between aSAH and SAH of other etiologies (82). The potential mechanism may be that neuroinflammation plays a significant role during the formation and rupture of cerebral aneurysms (123). Neutrophil infiltration and pro-inflammatory cytokine overexpression cause thinning of the aneurysm wall and coagulation dysfunction (124, 125). However, the hypothesis that the NLR may be used as an early warning index before aneurysm rupture requires more exploration regarding the pathology of aneurysm progression and neuroinflammation.
It is encouraging that combining the NLR with other indicators can enhance the predictive value. The combined NLR–Fisher score model significantly improves the ability to predict the outcome of aSAH with higher sensitivity and specificity (74). Combining the NLR with the platelet-to-lymphocyte ratio (PLR) is more sensitive for aSAH than either indicator alone (81, 126). The prognosis of neurological diseases is affected by a number of factors, and combining NLR with other potential indicators may be a potential way to improve the prediction accuracy and clinical value of NLR. Lattanzi et al. found that the accuracy of outcome prediction in acute ICH would increase when NLR combined with the modified ICH score (127). NLR combined with patient characteristics like gender, a history of hypertension, diabetes mellitus, and smoking could present high diagnostic accuracy in ischemic stroke (128, 129). NLR combined with PLR was also found to be more meaningful in the early clinical detection of post-stroke depression than either alone (130).
Further studies may focus on the application of the NLR as a new potential target for developing novel therapeutic strategies (131). Neutrophils and lymphocytes show the potential to have substantial beneficial effects. Preclinical studies have shown that selective limitation of neutrophil activity can reduce neuroinflammation and neuronal apoptosis, eventually protecting the microcirculation and improving prognosis (132). Therapeutic strategies for T lymphocytes, such as the use of cyclosporine, have also been shown to be effective in some studies (133, 134). Many studies have evaluated drugs aimed at inhibiting inflammation, but the results have been mixed and not as obvious as originally hoped (135). It is not advisable to inhibit overall inflammation, and immunomodulatory methods should aim to block harmful effects selectively rather than functioning as an extensive, non-selective anti-inflammatory therapy (136, 137). Future treatment strategies should focus on subtle regulation of the immune response, which requires the precise assessment of inflammation, and the NLR may be a promising index for this.
There are many areas of uncertainty regarding the evaluation of the NLR as a prognostic marker in aSAH and new therapeutic targets. To some extent, the conclusions of clinical studies may overestimate the causality and clinical correlation between the NLR and aSAH, for the existence of confounding factors is inevitable (138). In addition, the admission criteria of studies are not harmonized or standardized, and some are not strict enough. Moreover, the sampling time of all studies is at the time of admission, which ignores the fact that the NLR is a dynamic index (23, 139). The current research can only prove the predictive role of the NLR on admission; a further prospective study is needed to provide time trend data to explore the overall dynamic changes.
Undoubtedly, further multicenter, large-sample, prospective, standardized evaluation studies are needed to confirm the detailed mechanisms and causal link between the NLR and aSAH. Additionally, all candidate biomarkers and molecules in the upstream pathways should be further explored for the detection of target antigens that link central and peripheral inflammation and to help identify other new targets (140).
Present studies have demonstrated that NLR may be useful for predicting clinical outcome and the risk of complications in patients with aSAH. And the underlying pathophysiology mechanism of neuroinflammation is highlighted to further support this conclusion. However, NLR may present an insufficient specificity when it plays a predictive role in a variety of medical conditions. Combining NLR with other relevant prognosis factors may be a potential way to improve the predictive ability and clinical value of NLR. Despite the complexities of neuroinflammation and deficiency of present studies, modulating levels of neutrophils and lymphocytes and relevant signal transduction pathways could be a clinical therapeutic intervention in aSAH.
LC and HZ wrote and revised the manuscript. XW and XT helped in finding references. All authors contributed to the article and approved the submitted version.
This work was supported by the National Natural Science Foundation of China (Grant No. 81701152).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
aSAH, aneurysmal subarachnoid hemorrhage; NLR, neutrophil-to-lymphocyte ratio; EBI, early brain injury; DCI, delayed cerebral ischemia; BBB, blood–brain barrier; SIRS, systemic inflammatory response syndrome; CSF, cerebrospinal fluid; CNS, central nervous system; TLR4, toll-like receptor 4; IL-6, interleukin-6; IL-1β, interleukin-1β; TNF-α, tumor necrosis factor-alpha; NO, nitric oxide; CAMs, cell adhesion molecules; MMP-9, matrix metalloproteinase-9; PSGL-1, P-selectin glycoprotein ligand-1; MPO, myeloperoxidase; mRS, Modified Rankin Scale; ANS, autonomic nervous system; SNS, sympathetic nervous system; HPA, hypothalamic–pituitary–adrenal.
1. van Gijn J, Rinkel GJE. Subarachnoid haemorrhage: diagnosis, causes and management. Brain. (2001) 124:249–78. doi: 10.1093/brain/124.2.249
2. van Gijn J, Kerr R, Rinkel G. Subarachnoid haemorrhage. Lancet. (2007) 369:306–18. doi: 10.1016/S0140-6736(07)60153-6
3. Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. Lancet. (2017) 389:655–66. doi: 10.1016/S0140-6736(16)30668-7
4. Ois A, Vivas E, Figueras-Aguirre G, Guimaraens L, Cuadrado-Godia E, Avellaneda C, et al. Misdiagnosis worsens prognosis in subarachnoid hemorrhage with good hunt and hess score. Stroke. (2019) 50:3072–6. doi: 10.1161/STROKEAHA.119.025520
5. Khey K, Huard A, Mahmoud S. Inflammatory pathways following subarachnoid hemorrhage. Cell Mol Neurobiol. (2020) 40:675–93. doi: 10.1007/s10571-019-00767-4
6. Friedrich V, Flores R, Muller A, Bi W, Peerschke E, Sehba F. Reduction of neutrophil activity decreases early microvascular injury after subarachnoid haemorrhage. J Neuroinflamm. (2011) 8:103. doi: 10.1186/1742-2094-8-103
7. Zhou C, Xie G, Wang C, Zhang Z, Chen Q, Zhang L, et al. Decreased progranulin levels in patients and rats with subarachnoid hemorrhage: a potential role in inhibiting inflammation by suppressing neutrophil recruitment. J Neuroinflamm. (2015) 12:200. doi: 10.1186/s12974-015-0415-4
8. Savarraj J, Parsha K, Hergenroeder G, Ahn S, Chang T, Kim D, et al. Early brain injury associated with systemic inflammation after subarachnoid hemorrhage. Neurocritical Care. (2018) 28:203–11. doi: 10.1007/s12028-017-0471-y
9. Sarrafzadeh A, Schlenk F, Meisel A, Dreier J, Vajkoczy P, Meisel C. Immunodepression after aneurysmal subarachnoid hemorrhage. Stroke. (2011) 42:53–8. doi: 10.1161/STROKEAHA.110.594705
10. Nam K, Kim T, Lee J, Kwon H, Lee Y, Ko S, et al. High neutrophil-to-lymphocyte ratio predicts stroke-associated pneumonia. Stroke. (2018) 49:1886–92. doi: 10.1161/STROKEAHA.118.021228
11. Kim S, Eliot M, Koestler D, Wu W, Kelsey K. Association of neutrophil-to-lymphocyte ratio with mortality and cardiovascular disease in the jackson heart study and modification by the duffy antigen variant. JAMA Cardiol. (2018) 3:455–62. doi: 10.1001/jamacardio.2018.1042
12. Tschoe C, Bushnell C, Duncan P, Alexander-Miller M, Wolfe S. Neuroinflammation after intracerebral hemorrhage and potential therapeutic targets. J Stroke. (2020) 22:29–46. doi: 10.5853/jos.2019.02236
13. Brooks S, Spears C, Cummings C, VanGilder R, Stinehart K, Gutmann L, et al. Admission neutrophil-lymphocyte ratio predicts 90 day outcome after endovascular stroke therapy. J Neurointervent Surg. (2014) 6:578–83. doi: 10.1136/neurintsurg-2013-010780
14. Lux D, Alakbarzade V, Bridge L, Clark C, Clarke B, Zhang L, et al. The association of neutrophil-lymphocyte ratio and lymphocyte-monocyte ratio with 3-month clinical outcome after mechanical thrombectomy following stroke. J Neuroinflamm. (2020) 17:60. doi: 10.1186/s12974-020-01739-y
15. Buehler P, Humar R, Schaer D. Haptoglobin therapeutics and compartmentalization of cell-free hemoglobin toxicity. Trends Mol Med. (2020) 26:683–97. doi: 10.1016/j.molmed.2020.02.004
16. Chen J, Wang L, Xu H, Xing L, Zhuang Z, Zheng Y, et al. Meningeal lymphatics clear erythrocytes that arise from subarachnoid hemorrhage. Nat Commun. (2020) 11:3159. doi: 10.1038/s41467-020-16851-z
17. Lucke-Wold B, Logsdon A, Manoranjan B, Turner R, McConnell E, Vates G, et al. Aneurysmal subarachnoid hemorrhage and neuroinflammation: a comprehensive review. Int J Mol Sci. (2016) 17:497. doi: 10.3390/ijms17040497
18. Lan X, Han X, Li Q, Yang Q, Wang J. Modulators of microglial activation and polarization after intracerebral haemorrhage. Neurology. (2017) 13:420–33. doi: 10.1038/nrneurol.2017.69
19. Zheng Z, Lyu H, Lam S, Lam P, Poon W, Wong G. The dynamics of microglial polarization reveal the resident neuroinflammatory responses after subarachnoid hemorrhage. Transl Stroke Res. (2020) 11:433–49. doi: 10.1007/s12975-019-00728-5
20. Liu L, Liu J, Bao J, Bai Q, Wang G. Interaction of microglia and astrocytes in the neurovascular unit. Front Immunol. (2020) 11:1024. doi: 10.3389/fimmu.2020.01024
21. Chen X, Jiang M, Li H, Wang Y, Shen H, Li X, et al. CX3CL1/CX3CR1 axis attenuates early brain injury via promoting the delivery of exosomal microRNA-124 from neuron to microglia after subarachnoid hemorrhage. J Neuroinflamm. (2020) 17:209. doi: 10.1186/s12974-020-01882-6
22. Amantea D, Micieli G, Tassorelli C, Cuartero M, Ballesteros I, Certo M, et al. Rational modulation of the innate immune system for neuroprotection in ischemic stroke. Front Neurosci. (2015) 9:147. doi: 10.3389/fnins.2015.00147
23. Coulibaly A, Provencio J. Aneurysmal subarachnoid hemorrhage: an overview of inflammation-induced cellular changes. Neurotherapeutics. (2020) 17:436–45. doi: 10.1007/s13311-019-00829-x
24. Ahn S, Savarraj J, Parsha K, Hergenroeder G, Chang T, Kim D, et al. Inflammation in delayed ischemia and functional outcomes after subarachnoid hemorrhage. J Neuroinflamm. (2019) 16:213. doi: 10.1186/s12974-019-1578-1
25. Schneider U, Xu R, Vajkoczy P. Inflammatory events following subarachnoid hemorrhage (SAH). Curr Neuropharmacol. (2018) 16:1385–95. doi: 10.2174/1570159X16666180412110919
26. Hosaka K, Hoh B. Inflammation and cerebral aneurysms. Transl Stroke Res. (2014) 5:190–8. doi: 10.1007/s12975-013-0313-y
27. Mao L, Li P, Zhu W, Cai W, Liu Z, Wang Y, et al. Regulatory T cells ameliorate tissue plasminogen activator-induced brain haemorrhage after stroke. Brain. (2017) 140:1914–31. doi: 10.1093/brain/awx111
28. Geraghty J, Testai F. Delayed cerebral ischemia after subarachnoid hemorrhage: beyond vasospasm and towards a multifactorial pathophysiology. Curr Atheroscl Rep. (2017) 19:50. doi: 10.1007/s11883-017-0690-x
29. Huang C, Wang L, Shan Y, Pan C, Tsai K. Memantine attenuates delayed vasospasm after experimental subarachnoid hemorrhage via modulating endothelial nitric oxide synthase. Int J Mol Sci. (2015) 16:14171–80. doi: 10.3390/ijms160614171
30. Shimamura N, Ohkuma H. Phenotypic transformation of smooth muscle in vasospasm after aneurysmal subarachnoid hemorrhage. Transl Stroke Res. (2014) 5:357–64. doi: 10.1007/s12975-013-0310-1
31. Serrone JC, Maekawa H, Tjahjadi M, Hernesniemi J. Aneurysmal subarachnoid hemorrhage: pathobiology, current treatment and future directions. Expert Rev Neurotherapeutics. (2015) 15:367–80. doi: 10.1586/14737175.2015.1018892
32. Freedman J, Loscalzo J. Platelet-monocyte aggregates: bridging thrombosis and inflammation. Circulation. (2002) 105:2130–2. doi: 10.1161/01.CIR.0000017140.26466.F5
33. Yang T, Lin Y, Tsai N, Lin W, Ho J, Chang W, et al. The prognostic value of serial leukocyte adhesion molecules in post-aneurysmal subarachnoid hemorrhage. Clin Chim Acta Int J Clin Chem. (2012) 413:411–6. doi: 10.1016/j.cca.2011.10.007
34. Srinivasan A, Aggarwal A, Gaudihalli S, Mohanty M, Dhandapani M, Singh H, et al. Impact of early leukocytosis and elevated high-sensitivity C-reactive protein on delayed cerebral ischemia and neurologic outcome after subarachnoid hemorrhage. World Neurosurg. (2016) 90:91–5. doi: 10.1016/j.wneu.2016.02.049
35. Budohoski K, Guilfoyle M, Helmy A, Huuskonen T, Czosnyka M, Kirollos R, et al. The pathophysiology and treatment of delayed cerebral ischaemia following subarachnoid haemorrhage. J Neurol Neurosurg Psaychiatry. (2014) 85:1343–53. doi: 10.1136/jnnp-2014-307711
36. Clarke J, Suggs J, Diwan D, Lee J, Lipsey K, Vellimana A, et al. Microvascular platelet aggregation and thrombosis after subarachnoid hemorrhage: a review and synthesis. J Cerebral Blood Flow Metab. (2020) 40:1565–75. doi: 10.1177/0271678X20921974
37. Sugimoto K, Chung D. Spreading depolarizations and subarachnoid hemorrhage. Neurotherapeutics. (2020) 17:497–510. doi: 10.1007/s13311-020-00850-5
38. Geraghty JR, Davis JL, Testai FD. Neuroinflammation and microvascular dysfunction after experimental subarachnoid hemorrhage: emerging components of early brain injury related to outcome. Neurocrit Care. (2019) 31:373–89. doi: 10.1007/s12028-019-00710-x
39. Maestrini I, Tagzirt M, Gautier S, Dupont A, Mendyk A, Susen S, et al. Analysis of the association of MPO and MMP-9 with stroke severity and outcome: Cohort study. Neurology. (2020) 95:e97–108. doi: 10.1212/WNL.0000000000009179
40. Neulen A, Pantel T, Kosterhon M, Kramer A, Kunath S, Petermeyer M, et al. Neutrophils mediate early cerebral cortical hypoperfusion in a murine model of subarachnoid haemorrhage. Sci Rep. (2019) 9:8460. doi: 10.1038/s41598-019-44906-9
41. Deddens L, van Tilborg G, van der Marel K, Hunt H, van der Toorn A, Viergever M, et al. In vivo molecular MRI of ICAM-1 expression on endothelium and leukocytes from subacute to chronic stages after experimental stroke. Transl Stroke Res. (2017) 8:440–8. doi: 10.1007/s12975-017-0536-4
42. Atangana E, Schneider U, Blecharz K, Magrini S, Wagner J, Nieminen-Kelhä M, et al. Intravascular inflammation triggers intracerebral activated microglia and contributes to secondary brain injury after experimental subarachnoid hemorrhage (eSAH). Transl Stroke Res. (2017) 8:144–56. doi: 10.1007/s12975-016-0485-3
43. Yang C, Hsiao L, Tseng H, Kuo C, Yang C. Pristimerin inhibits MMP-9 expression and cell migration through attenuating NOX/ROS-dependent NF-κB activation in rat brain astrocytes challenged with LPS. J Inflamm Res. (2020) 13:325–41. doi: 10.2147/JIR.S252659
44. Chu Y, Wilson K, Gu H, Wegman-Points L, Dooley S, Pierce G, et al. Myeloperoxidase is increased in human cerebral aneurysms and increases formation and rupture of cerebral aneurysms in mice. Stroke. (2015) 46:1651–6. doi: 10.1161/STROKEAHA.114.008589
45. Morotti A, Phuah C, Anderson C, Jessel M, Schwab K, Ayres A, et al. Leukocyte count and intracerebral hemorrhage expansion. Stroke. (2016) 47:1473–8. doi: 10.1161/STROKEAHA.116.013176
46. Gris T, Laplante P, Thebault P, Cayrol R, Najjar A, Joannette-Pilon B, et al. Innate immunity activation in the early brain injury period following subarachnoid hemorrhage. J Neuroinflamm. (2019) 16:253. doi: 10.1186/s12974-019-1629-7
47. Blecharz-Lang K, Wagner J, Fries A, Nieminen-Kelhä M, Rösner J, Schneider U, et al. Interleukin 6-mediated endothelial barrier disturbances can be attenuated by blockade of the IL6 receptor expressed in brain microvascular endothelial cells. Transl Stroke Res. (2018) 9:631–42. doi: 10.1007/s12975-018-0614-2
48. van der Bilt I, Vendeville J, van de Hoef T, Begieneman M, Lagrand W, Kros J, et al. Myocarditis in patients with subarachnoid hemorrhage: a histopathologic study. J Critical Care. (2016) 32:196–200. doi: 10.1016/j.jcrc.2015.12.005
49. Li R, Yuan Q, Su Y, Chopp M, Yan T, Chen J. Immune response mediates the cardiac damage after subarachnoid hemorrhage. Exp Neurol. (2020) 323:113093. doi: 10.1016/j.expneurol.2019.113093
50. Schiller M, Ben-Shaanan T, Rolls A. Neuronal regulation of immunity: why, how and where? Nat Rev Immunol. (2020) 21:20–36. doi: 10.1038/s41577-020-0387-1
51. Hu D, Al-Shalan H, Shi Z, Wang P, Wu Y, Nicholls P, et al. Distribution of nerve fibers and nerve-immune cell association in mouse spleen revealed by immunofluorescent staining. Sci Rep. (2020) 10:9850. doi: 10.1038/s41598-020-66619-0
52. Guterman E, Kamel H, Azran C, Shah M, Claude Hemphill J, Smith W, et al. Time from onset of SIRS to antibiotic administration and outcomes after subarachnoid hemorrhage. Neurocritical Care. (2014) 21:85–90. doi: 10.1007/s12028-013-9846-x
53. Shim R, Wen S, Wanrooy B, Rank M, Thirugnanachandran T, Ho L, et al. Stroke severity, and not cerebral infarct location, increases the risk of infection. Transl Stroke Res. (2020) 11:387–401. doi: 10.1007/s12975-019-00738-3
54. Zera K, Buckwalter M. The local and peripheral immune responses to stroke: implications for therapeutic development. Neurotherapeutics. (2020) 17:414–35. doi: 10.1007/s13311-020-00844-3
55. Najjar S, Najjar A, Chong D, Pramanik B, Kirsch C, Kuzniecky R, et al. Central nervous system complications associated with SARS-CoV-2 infection: integrative concepts of pathophysiology and case reports. J Neuroinflamm. (2020) 17:231. doi: 10.1186/s12974-020-01896-0
56. Engelhardt B, Vajkoczy P, Weller R. The movers and shapers in immune privilege of the CNS. Nat Immunol. (2017) 18:123–31. doi: 10.1038/ni.3666
57. Mrdjen D, Pavlovic A, Hartmann F, Schreiner B, Utz S, Leung B, et al. High-dimensional single-cell mapping of central nervous system immune cells reveals distinct myeloid subsets in health, aging, and disease. Immunity. (2018) 48:380–95.e6. doi: 10.1016/j.immuni.2018.01.011
58. Evans F, Dittmer M, de la Fuente A, Fitzgerald DC. Protective and regenerative roles of T cells in central nervous system disorders. Front Immunol. (2019) 10:2171. doi: 10.3389/fimmu.2019.02171
59. Mundt S, Mrdjen D, Utz S, Greter M, Schreiner B, Becher B. Conventional DCs sample and present myelin antigens in the healthy CNS and allow parenchymal T cell entry to initiate neuroinflammation. Sci Immunol. (2019) 4:1–11. doi: 10.1126/sciimmunol.aau8380
60. Liu G, Tao T, Wang H, Zhou Y, Gao X, Gao Y, et al. Functions of resolvin D1-ALX/FPR2 receptor interaction in the hemoglobin-induced microglial inflammatory response and neuronal injury. J Neuroinflamm. (2020) 17:239. doi: 10.1186/s12974-020-01918-x
61. Li P, Gan Y, Sun B, Zhang F, Lu B, Gao Y, et al. Adoptive regulatory T-cell therapy protects against cerebral ischemia. Ann Neurol. (2013) 74:458–71. doi: 10.1002/ana.23815
62. Liesz A, Kleinschnitz C. Regulatory T cells in post-stroke immune homeostasis. Transl Stroke Res. (2016) 7:313–21. doi: 10.1007/s12975-016-0465-7
63. Noster R, de Koning H, Maier E, Prelog M, Lainka E, Zielinski C. Dysregulation of proinflammatory versus anti-inflammatory human T17 cell functionalities in the autoinflammatory Schnitzler syndrome. J Allergy Clin Immunol. (2016) 138:1161–9.e6. doi: 10.1016/j.jaci.2015.12.1338
64. Roa J, Sarkar D, Zanaty M, Ishii D, Lu Y, Karandikar N, et al. Preliminary results in the analysis of the immune response after aneurysmal subarachnoid hemorrhage. Sci Rep. (2020) 10:11809. doi: 10.1038/s41598-020-68861-y
65. Klein R, Hunter C. Protective and pathological immunity during central nervous system infections. Immunity. (2017) 46:891–909. doi: 10.1016/j.immuni.2017.06.012
66. Chen A, Sun X, Wang W, Liu J, Zeng X, Qiu J, et al. Activation of the hypothalamic-pituitary-adrenal (HPA) axis contributes to the immunosuppression of mice infected with Angiostrongylus cantonensis. J Neuroinflamm. (2016) 13:266. doi: 10.1186/s12974-016-0743-z
67. Liesz A, Hu X, Kleinschnitz C, Offner H. Functional role of regulatory lymphocytes in stroke: facts and controversies. Stroke. (2015) 46:1422–30. doi: 10.1161/STROKEAHA.114.008608
68. Asano S, Chantler PD, Barr TL. Gene expression profiling in stroke: relevance of blood-brain interaction. Curr Opin Pharmacol. (2016) 26:80–6. doi: 10.1016/j.coph.2015.10.004
69. Chaudhry S, Kahlert U, Kinfe T, Lamprecht A, Niemelä M, Hänggi D, et al. Elevated systemic IL-10 levels indicate immunodepression leading to nosocomial infections after aneurysmal Subarachnoid hemorrhage (SAH) in patients. Int J Mol Sci. (2020) 21:1569. doi: 10.3390/ijms21051569
70. Mittal S, Cho K, Ishido S, Roche P. Interleukin 10 (IL-10)-mediated immunosuppression: MARCH-I induction regulates antigen presentation by macrophages but not dendritic cells. J Biol Chem. (2015) 290:27158–67. doi: 10.1074/jbc.M115.682708
71. Tsokos G, Terhorst C. T lymphocytes cash their value in clinical medicine. Trends Mol Med. (2020) 26:800–2. doi: 10.1016/j.molmed.2020.06.003
72. Jamali SA, Turnbull MT, Kanekiyo T, Vishnu P, Zubair AC, Raper CC, et al. Elevated neutrophil-lymphocyte ratio is predictive of poor outcomes following aneurysmal subarachnoid hemorrhage. J Stroke Cerebrovasc Dis. (2020) 29:104631. doi: 10.1016/j.jstrokecerebrovasdis.2019.104631
73. Wang J-Y, Zhang X-T, Wang J-Q, Wang C-Y, Zheng W-L, Pan Z-M, et al. Admission neutrophil–lymphocyte ratio predicts rebleeding following aneurismal subarachnoid hemorrhage. World Neurosurgery. (2020) 138:e317–22. doi: 10.1016/j.wneu.2020.02.112
74. Al-Mufti F, Amuluru K, Damodara N, Dodson V, Roh D, Agarwal S, et al. Admission neutrophil–lymphocyte ratio predicts delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage. J NeuroIntervent Surg. (2019) 11:1135–40. doi: 10.1136/neurintsurg-2019-014759
75. Giede-Jeppe A, Reichl J, Sprügel MI, Lücking H, Hoelter P, Eyüpoglu IY, et al. Neutrophil-to-lymphocyte ratio as an independent predictor for unfavorable functional outcome in aneurysmal subarachnoid hemorrhage. J Neurosurg. (2020) 132:400–7. doi: 10.3171/2018.9.JNS181975
76. Ray B, Ross SR, Danala G, Aghaei F, Nouh CD, Ford L, et al. Systemic response of coated-platelet and peripheral blood inflammatory cell indices after aneurysmal subarachnoid hemorrhage and long-term clinical outcome. J Crit Care. (2019) 52:1–9. doi: 10.1016/j.jcrc.2019.03.003
77. Wu Y, He Q, Wei Y, Zhu J, He Z, Zhang X, et al. The association of neutrophil-to-lymphocyte ratio and delayed cerebral ischemia in patients with aneurysmal subarachnoid hemorrhage: possible involvement of cerebral blood perfusion. Neuropsychiatric Dis Treat. (2019) 15:1001–7. doi: 10.2147/NDT.S190477
78. Ogden M, Bakar B, Karagedik M, Bulut I, Cetin C, Aydin G, et al. Analysis of biochemical laboratory values to determine etiology and prognosis in patients with subarachnoid hemorrhage: a clinical study. Neurol Res. (2019) 41:156–67. doi: 10.1080/01616412.2018.1545414
79. Yilmaz A, Ozkul A. Admission neutrophil to lymphocyte and platelet to lymphocyte ratio as a predictor of mortality in patients with subarachnoid hemorrhage. Turkish J Cerebrovasc Dis. (2018) 24:19–25. doi: 10.5505/tbdhd.2018.57338
80. Huang Y, Han Z, Hu Z. Red blood cell distribution width and neutrophil to lymphocyte ratio are associated with outcomes of adult subarachnoid haemorrhage patients admitted to intensive care unit. Ann Clin Biochem. (2017) 54:696–701. doi: 10.1177/0004563216686623
81. Tao C, Wang J, Hu X, Ma J, Li H, You C. Clinical value of neutrophil to lymphocyte and platelet to lymphocyte ratio after aneurysmal subarachnoid hemorrhage. Neurocritical Care. (2017) 26:393–401. doi: 10.1007/s12028-016-0332-0
82. Zhang Y, Yang P, Gu B, Wang J. Comparison of the diagnostic values of neutrophil, neutrophil to lymphocyte ratio, and platelet to lymphocyte ratio in distinguishing spontaneous subarachnoid hemorrhage from nontraumatic acute headache. Clin Lab. (2019) 65:246–53. doi: 10.7754/Clin.Lab.2019.190301
83. Roquer J, Cuadrado-Godia E, Guimaraens L, Conesa G, Rodríguez-Campello A, Capellades J, et al. Short and long-term outcome of aneurysmal subarachnoid hemorrhage patients. Neurology. (2020) 95:e1819–29. doi: 10.1212/WNL.0000000000010618
84. Mascitelli J, Cole T, Yoon S, Nakaji P, Albuquerque F, McDougall C, et al. External validation of the subarachnoid hemorrhage international trialists (SAHIT) predictive model using the barrow ruptured aneurysm trial (BRAT) Cohort. Neurosurgery. (2020) 86:101–6. doi: 10.1093/neuros/nyy600
85. Dong Y, Guo Z, Li Q, Ni W, Gu H, Gu Y, et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of spontaneous subarachnoid haemorrhage. Stroke. (2019) 4:176–81. doi: 10.1136/svn-2019-000296
86. Dengler N, Sommerfeld J, Diesing D, Vajkoczy P, Wolf S. Prediction of cerebral infarction and patient outcome in aneurysmal subarachnoid hemorrhage: comparison of new and established radiographic, clinical and combined scores. Euro J Neurol. (2018) 25:111–9. doi: 10.1111/ene.13471
87. Jaja B, Saposnik G, Lingsma H, Macdonald E, Thorpe K, Mamdani M, et al. Development and validation of outcome prediction models for aneurysmal subarachnoid haemorrhage: the SAHIT multinational cohort study. BMJ. (2018) 360:j5745. doi: 10.1136/bmj.k4079
88. Duris K, Lipkova J, Splichal Z, Madaraszova T, Jurajda M. Early inflammatory response in the brain and anesthesia recovery time evaluation after experimental subarachnoid hemorrhage. Transl Stroke Res. (2018) 87:1–11. doi: 10.1007/s12975-018-0641-z
89. Bevers M, Wolcott Z, Bache S, Hansen C, Sastre C, Mylvaganam R, et al. Soluble ST2 links inflammation to outcome after subarachnoid hemorrhage. Ann Neurol. (2019) 86:384–94. doi: 10.1002/ana.25545
90. Muroi C, Hugelshofer M, Seule M, Tastan I, Fujioka M, Mishima K, et al. Correlation among systemic inflammatory parameter, occurrence of delayed neurological deficits, and outcome after aneurysmal subarachnoid hemorrhage. Neurosurgery. (2013) 72:367–75; discussion: 75. doi: 10.1227/NEU.0b013e31828048ce
91. Rass V, Gaasch M, Kofler M, Schiefecker A, Ianosi B, Rhomberg P, et al. Systemic inflammatory response syndrome as predictor of poor outcome in nontraumatic subarachnoid hemorrhage patients. Crit Care Med. (2018) 46:e1152–9. doi: 10.1097/CCM.0000000000003429
92. Li G, Wang X, Huang L, Wang Y, Hao J, Ge X, et al. Cytotoxic function of CD8+ T lymphocytes isolated from patients with acute severe cerebral infarction: an assessment of stroke-induced immunosuppression. BMC immunology. (2013) 14:1. doi: 10.1186/1471-2172-14-1
93. Fest J, Ruiter T, Groot Koerkamp B, Rizopoulos D, Ikram M, van Eijck C, et al. The neutrophil-to-lymphocyte ratio is associated with mortality in the general population: the Rotterdam study. Euro J Epidemiol. (2019) 34:463–70. doi: 10.1007/s10654-018-0472-y
94. Fang Y, Tong M, Sung P, Chen Y, Chen C, Tsai N, et al. Higher neutrophil counts and neutrophil-to-lymphocyte ratio predict prognostic outcomes in patients after non-atrial fibrillation-caused ischemic stroke. Biomed J. (2017) 40:154–62. doi: 10.1016/j.bj.2017.03.002
95. Grenader T, Waddell T, Peckitt C, Oates J, Starling N, Cunningham D, et al. Prognostic value of neutrophil-to-lymphocyte ratio in advanced oesophago-gastric cancer: exploratory analysis of the REAL-2 trial. Ann Oncol. (2016) 27:687–92. doi: 10.1093/annonc/mdw012
96. Gusdon A, Gialdini G, Kone G, Baradaran H, Merkler A, Mangat H, et al. Neutrophil-lymphocyte ratio and perihematomal edema growth in intracerebral hemorrhage. Stroke. (2017) 48:2589–92. doi: 10.1161/STROKEAHA.117.018120
97. Stienen M, Germans M, Burkhardt J, Neidert M, Fung C, Bervini D, et al. Predictors of in-hospital death after aneurysmal subarachnoid hemorrhage: analysis of a nationwide database (Swiss SOS [Swiss Study on Aneurysmal Subarachnoid Hemorrhage]). Stroke. (2018) 49:333–40. doi: 10.1161/STR.0000000000000169
98. Hostettler I, Sebök M, Ambler G, Muroi C, Prömmel P, Neidert M, et al. Validation and optimization of barrow neurological institute score in prediction of adverse events and functional outcome after subarachnoid hemorrhage-creation of the HATCH (hemorrhage, age, treatment, clinical state, hydrocephalus) score. Neurosurgery. (2020) 88:96–105. doi: 10.1093/neuros/nyaa316
99. Horie N, Sato S, Kaminogo M, Morofuji Y, Izumo T, Anda T, et al. Impact of perioperative aneurysm rebleeding after subarachnoid hemorrhage. J Neurosurg. (2019) 133:1–10. doi: 10.3171/2019.6.JNS19704
100. Lu V, Graffeo C, Perry A, Carlstrom L, Rangel-Castilla L, Lanzino G, et al. Rebleeding drives poor outcome in aneurysmal subarachnoid hemorrhage independent of delayed cerebral ischemia: a propensity-score matched cohort study. J Neurosurg. (2019) 133:1–9. doi: 10.3171/2019.4.JNS19779
101. Zhao B, Fan Y, Xiong Y, Yin R, Zheng K, Li Z, et al. Aneurysm rebleeding after poor-grade aneurysmal subarachnoid hemorrhage: predictors and impact on clinical outcomes. J Neurol Sci. (2016) 371:62–6. doi: 10.1016/j.jns.2016.10.020
102. Linzey J, Williamson C, Rajajee V, Sheehan K, Thompson B, Pandey A. Twenty-four-hour emergency intervention versus early intervention in aneurysmal subarachnoid hemorrhage. J Neurosurg. (2018) 128:1297–303. doi: 10.3171/2017.2.JNS163017
103. Francoeur C, Roh D, Schmidt J, Mayer S, Falo M, Agarwal S, et al. Desmopressin administration and rebleeding in subarachnoid hemorrhage: analysis of an observational prospective database. J Neurosurg. (2018) 130:1–7. doi: 10.3171/2017.7.JNS17990
104. Germans M, Coert B, Vandertop W, Verbaan D. Time intervals from subarachnoid hemorrhage to rebleed. J Neurol. (2014) 261:1425–31. doi: 10.1007/s00415-014-7365-0
105. van Donkelaar C, Bakker N, Veeger N, Uyttenboogaart M, Metzemaekers J, Luijckx G, et al. Predictive factors for rebleeding after aneurysmal subarachnoid hemorrhage: rebleeding aneurysmal subarachnoid hemorrhage study. Stroke. (2015) 46:2100–6. doi: 10.1161/STROKEAHA.115.010037
106. Citerio G, Gaini S, Tomei G, Stocchetti N. Management of 350 aneurysmal subarachnoid hemorrhages in 22 Italian neurosurgical centers. Intensive Care Med. (2007) 33:1580–6. doi: 10.1007/s00134-007-0700-5
107. Kim Y, Zipfel G, Ogilvy C, Pricola K, Welch B, Shakir N, et al. Preconditioning effect on cerebral vasospasm in patients with aneurysmal subarachnoid hemorrhage. Neurosurgery. (2014) 74:351–8; discussion: 8–9. doi: 10.1227/NEU.0000000000000282
108. de Oliveira Manoel A, Jaja B, Germans M, Yan H, Qian W, Kouzmina E, et al. The VASOGRADE: a simple grading scale for prediction of delayed cerebral ischemia after subarachnoid hemorrhage. Stroke. (2015) 46:1826–31. doi: 10.1161/STROKEAHA.115.008728
109. Radolf S, Smoll N, Drenckhahn C, Dreier J, Vajkoczy P, Sarrafzadeh A. Cerebral lactate correlates with early onset pneumonia after aneurysmal SAH. Transl Stroke Res. (2014) 5:278–85. doi: 10.1007/s12975-013-0292-z
110. Saand A, Yu F, Chen J, Chou S. Systemic inflammation in hemorrhagic strokes - a novel neurological sign and therapeutic target? J Cerebral Blood Flow Metab. (2019) 39:959–88. doi: 10.1177/0271678X19841443
111. Chaudhry S, Stoffel-Wagner B, Kinfe T, Güresir E, Vatter H, Dietrich D, et al. Elevated systemic IL-6 levels in patients with aneurysmal subarachnoid hemorrhage is an unspecific marker for post-SAH complications. Int J Mol Sci. (2017) 18:2580. doi: 10.3390/ijms18122580
112. Salciccioli J, Marshall D, Pimentel M, Santos M, Pollard T, Celi L, et al. The association between the neutrophil-to-lymphocyte ratio and mortality in critical illness: an observational cohort study. Critical Care Med. (2015) 19:13. doi: 10.1186/s13054-014-0731-6
113. Yan J, Greer J, Etherington K, Cadigan G, Cavanagh H, Henderson R, et al. Immune activation in the peripheral blood of patients with acute ischemic stroke. J Neuroimmunol. (2009) 206:112–7. doi: 10.1016/j.jneuroim.2008.11.001
114. Laban K, Rinkel G, Vergouwen M. Nosocomial infections after aneurysmal subarachnoid hemorrhage: time course and causative pathogens. Int J Stroke. (2015) 10:763–6. doi: 10.1111/ijs.12494
115. Guo R, Wu Y, Chen R, Yu Z, You C, Ma L, et al. Clinical value of neutrophil-to-lymphocyte ratio in primary intraventricular hemorrhage. World Neurosurg. (2019) 127:e1051–6. doi: 10.1016/j.wneu.2019.04.040
116. Yu S, Arima H, Bertmar C, Clarke S, Herkes G, Krause M. Neutrophil to lymphocyte ratio and early clinical outcomes in patients with acute ischemic stroke. J Neurol Sci. (2018) 387:115–8. doi: 10.1016/j.jns.2018.02.002
117. Ferro D, Matias M, Neto J, Dias R, Moreira G, Petersen N, et al. Neutrophil-to-lymphocyte ratio predicts cerebral edema and clinical worsening early after reperfusion therapy in stroke. Stroke. (2021) 52:859–67. doi: 10.1161/STROKEAHA.120.032130
118. Switońska M, Piekuś-Słomka N, Słomka A, Sokal P, Zekanowska E, Lattanzi S. Neutrophil-to-lymphocyte ratio and symptomatic hemorrhagic transformation in ischemic stroke patients undergoing revascularization. Brain Sci. (2020) 10:771. doi: 10.3390/brainsci10110771
119. Pikija S, Sztriha L, Killer-Oberpfalzer M, Weymayr F, Hecker C, Ramesmayer C, et al. Neutrophil to lymphocyte ratio predicts intracranial hemorrhage after endovascular thrombectomy in acute ischemic stroke. J Neuroinflamm. (2018) 15:319. doi: 10.1186/s12974-018-1359-2
120. Li T, Zhao J, Xie W, Yuan W, Guo J, Pang S, et al. Specific depletion of resident microglia in the early stage of stroke reduces cerebral ischemic damage. J Neuroinflamm. (2021) 18:81. doi: 10.1186/s12974-021-02127-w
121. Nakajima S, Tanaka R, Yamashiro K, Chiba A, Noto D, Inaba T, et al. Mucosal-associated invariant t cells are involved in acute ischemic stroke by regulating neuroinflammation. J Am Heart Assoc. (2021) 10:e018803. doi: 10.1161/JAHA.120.018803
122. Eryigit U, Altunayoglu Cakmak V, Sahin A, Tatli O, Pasli S, Gazioglu G, et al. The diagnostic value of the neutrophil-lymphocyte ratio in distinguishing between subarachnoid hemorrhage and migraine. Am J Emerg Med. (2017) 35:1276–80. doi: 10.1016/j.ajem.2017.03.063
123. Ramesh S, Christopher R, Indira Devi B, Bhat D. The vascular protective role of oestradiol: a focus on postmenopausal oestradiol deficiency and aneurysmal subarachnoid haemorrhage. Biol Rev Cambridge Philos Soc. (2019) 94:1897–917. doi: 10.1111/brv.12541
124. Chalouhi N, Ali M, Starke R, Jabbour P, Tjoumakaris S, Gonzalez L, et al. Cigarette smoke and inflammation: role in cerebral aneurysm formation and rupture. Mediators Inflamm. (2012) 2012:271582. doi: 10.1155/2012/271582
125. Makino H, Tada Y, Wada K, Liang E, Chang M, Mobashery S, et al. Pharmacological stabilization of intracranial aneurysms in mice: a feasibility study. Stroke. (2012) 43:2450–6. doi: 10.1161/STROKEAHA.112.659821
126. Chen L, Zhang Q. Predictive value of mean platelet volume for aneurysm recurrence in patients with aneurysmal subarachnoid hemorrhage after endovascular treatment. World Neurosurg. (2020) 145:e32–7. doi: 10.1016/j.wneu.2020.09.003
127. Lattanzi S, Cagnetti C, Rinaldi C, Angelocola S, Provinciali L, Silvestrini M. Neutrophil-to-lymphocyte ratio improves outcome prediction of acute intracerebral hemorrhage. J Neurol Sci. (2018) 387:98–102. doi: 10.1016/j.jns.2018.01.038
128. Wang M, Yu M, Li W, Li Y. Application of neutrophil to lymphocyte ratio to identify CT-negative cerebral infarction with nonfocal symptoms. Ann Transl Med. (2020) 8:1359. doi: 10.21037/atm-20-1640
129. Cheng Y, Ying A, Lin Y, Yu J, Luo J, Zeng Y, et al. Neutrophil-to-lymphocyte ratio, hyperglycemia, and outcomes in ischemic stroke patients treated with intravenous thrombolysis. Brain Behav. (2020) 10:e01741. doi: 10.1002/brb3.1741
130. Hu J, Zhou W, Zhou Z, Han J, Dong W. Elevated neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios predict post-stroke depression with acute ischemic stroke. Exp Ther Med. (2020) 19:2497–504. doi: 10.3892/etm.2020.8514
131. Vandenbark A, Meza-Romero R, Benedek G, Offner H. A novel neurotherapeutic for multiple sclerosis, ischemic injury, methamphetamine addiction, and traumatic brain injury. J Neuroinflamm. (2019) 16:14. doi: 10.1186/s12974-018-1393-0
132. Moraes L, Grille S, Morelli P, Mila R, Trias N, Brugnini A, et al. Immune cells subpopulations in cerebrospinal fluid and peripheral blood of patients with Aneurysmal Subarachnoid Hemorrhage. SpringerPlus. (2015) 4:195. doi: 10.1186/s40064-015-0970-2
133. Palzur E, Sharon A, Shehadeh M, Soustiel J. Investigation of the mechanisms of neuroprotection mediated by Ro5-4864 in brain injury. Neuroscience. (2016) 329:162–70. doi: 10.1016/j.neuroscience.2016.05.014
134. Yadav S, Pawar G, Kulkarni P, Ferris C, Amiji M. CNS delivery and anti-inflammatory effects of intranasally administered cyclosporine-A in cationic nanoformulations. J Pharmacol Exp Ther. (2019) 370:843–54. doi: 10.1124/jpet.118.254672
135. Shekhar S, Cunningham MW, Pabbidi MR, Wang S, Booz GW, Fan F. Targeting vascular inflammation in ischemic stroke: recent developments on novel immunomodulatory approaches. Euro J Pharmacol. (2018) 833:531–44. doi: 10.1016/j.ejphar.2018.06.028
136. Galea J, Ogungbenro K, Hulme S, Patel H, Scarth S, Hoadley M, et al. Reduction of inflammation after administration of interleukin-1 receptor antagonist following aneurysmal subarachnoid hemorrhage: results of the Subcutaneous Interleukin-1Ra in SAH (SCIL-SAH) study. J Neurosurg. (2018) 128:515–23. doi: 10.3171/2016.9.JNS16615
137. Kipnis J. Multifaceted interactions between adaptive immunity and the central nervous system. Science. (2016) 353:766–71. doi: 10.1126/science.aag2638
138. van Donkelaar CE, Bakker NA, Birks J, Clarke A, Sneade M, Kerr RSC, et al. Impact of treatment delay on outcome in the international subarachnoid aneurysm trial. Stroke. (2020) 51:1600–3. doi: 10.1161/STROKEAHA.120.028993
139. Guo Z, Yu S, Xiao L, Chen X, Ye R, Zheng P, et al. Dynamic change of neutrophil to lymphocyte ratio and hemorrhagic transformation after thrombolysis in stroke. J Neuroinflamm. (2016) 13:199. doi: 10.1186/s12974-016-0680-x
Keywords: aneurysmal subarachnoid hemorrhage, neutrophil to lymphocyte ratio, neuroinflammation, cerebrovascular disease, immune response, biomarkers
Citation: Cai L, Zeng H, Tan X, Wu X, Qian C and Chen G (2021) The Role of the Blood Neutrophil-to-Lymphocyte Ratio in Aneurysmal Subarachnoid Hemorrhage. Front. Neurol. 12:671098. doi: 10.3389/fneur.2021.671098
Received: 23 February 2021; Accepted: 13 April 2021;
Published: 03 June 2021.
Edited by:
Anna Rosell, Vall d'Hebron Research Institute (VHIR), SpainReviewed by:
Simona Lattanzi, Marche Polytechnic University, ItalyCopyright © 2021 Cai, Zeng, Tan, Wu, Qian and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cong Qian, Y29uZ3FpYW5Aemp1LmVkdS5jbg==; Gao Chen, ZC1jaGVuZ2FvQHpqdS5lZHUuY24=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.