
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Neurol. , 05 October 2021
Sec. Neurorehabilitation
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.667925
This article is part of the Research Topic COVID-19: The Neurorehabilitation Perspective View all 26 articles
 Abhishek Srivastava1
Abhishek Srivastava1 Aishwarya Swaminathan2
Aishwarya Swaminathan2 Manigandan Chockalingam3Murali K. Srinivasan4
Manigandan Chockalingam3Murali K. Srinivasan4 Nirmal Surya5*
Nirmal Surya5* Partha Ray6
Partha Ray6 Prasanna S. Hegde7
Prasanna S. Hegde7 Preetie Shetty Akkunje8
Preetie Shetty Akkunje8 Sanjivani Kamble9
Sanjivani Kamble9 Sonal Chitnis10
Sonal Chitnis10 Sureshkumar Kamalakannan11
Sureshkumar Kamalakannan11 Suvarna Ganvir12
Suvarna Ganvir12 Urvashi Shah13 and the Indian Federation of Neurorehabilitation (IFNR) Research Task Force
Urvashi Shah13 and the Indian Federation of Neurorehabilitation (IFNR) Research Task ForceThe importance of neurorehabilitation services for people with disabilities is getting well-recognized in low- and middle-income countries (LMICs) recently. However, accessibility to the same has remained the most significant challenge, in these contexts. This is especially because of the non-availability of trained specialists and the availability of neurorehabilitation centers only in urban cities owned predominantly by private healthcare organizations. In the current COVID-19 pandemic, the members of the Task Force for research at the Indian Federation of Neurorehabilitation (IFNR) reviewed the context for tele-neurorehabilitation (TNR) and have provided the contemporary implications for practicing TNR during COVID-19 for people with neurological disabilities (PWNDs) in LMICs. Neurorehabilitation is a science that is driven by rigorous research-based evidence. The current pandemic implies the need for systematically developed TNR interventions that is evaluated for its feasibility and acceptability and that is informed by available evidence from LMICs. Given the lack of organized systems in place for the provision of neurorehabilitation services in general, there needs to be sufficient budgetary allocations and a sector-wide approach to developing policies and systems for the provision of TNR services for PWNDs. The pandemic situation provides an opportunity to optimize the technological innovations in health and scale up these innovations to meet the growing burden of neurological disability in LMICs. Thus, this immense opportunity must be tapped to build capacity for safe and effective TNR services provision for PWNDs in these settings.
Neurological disorders are the leading causes of disability globally (1). During the past three decades, there is an absolute increase in people with neurological disability (PWND) by ~77.3% (2). A substantial proportion of this neurological disability burden are borne by low- and middle-income countries (LMICs) (3). Although there are several advances in the prevention and management of neurological disorders globally, factors such as demographic (increasing aging population) and epidemiological transitions (increasing non-communicable diseases) are consistently adding up to this burden (4).
The recent COVID-19 pandemic has tremendously halted most of the efforts toward combating the growing burden of neurological disorders, especially in LMICs (5). People with neurological disability (PWND) are unable to access neurorehabilitation services (5). Although access to such services was not available even during the pre-pandemic times, it is even harder to access during the COVID-19 pandemic (6). The shortage of specialists involved in neurorehabilitation, such as physiatrists, neurologists, rehabilitation nurses, physiotherapists, neuropsychologists, occupational therapists (OTs), speech and language pathologists, prosthetists and orthotists, and nutritionists, in LMICs has become even more acute in these settings (7). The neurorehabilitation specialists also experience an ambiguous situation during the pandemic due to the lack of specific guidelines to provide neurorehabilitation services for PWND (8).
Telerehabilitation has been perceived as a key innovation and an effective strategy to combat the existing pandemic situation and reduce the global burden of disability (9). Telecommunication technology has been a powerful tool to enhance the provision of health, education, and development services during the COVID-19 pandemic worldwide (10). It is also envisaged to be a game-changer in addressing the global burden of disability (9, 10). Even during the pre-pandemic times, these telecommunication technologies were substantially optimized to provide uninterrupted neurological rehabilitation services and care for PWNDs. They are popularly known as tele-neurorehabilitation (TNR) services (11). TNR is gaining considerable momentum globally in recent times (12). Though TNR services are well-organized and guided by good quality evidence in high-income countries (HICs), these services are yet to be systematically developed and tested for feasibility, acceptability, and effectiveness in LMICs (11, 13). In the current COVID-19 pandemic, the members of the Task Force for research at the Indian Federation of Neurorehabilitation (IFNR) reviewed the context for TNR and have provided the contemporary implications for practicing TNR during COVID-19 for PWNDs in LMICs. This critical reflection from the task force would potentially help to arrive at a policy or consensus for the provision of TNR services for PWNDs in LMICs.
With the largest number of internet users in Latin America, Brazil has introduced, accelerated emergency regulations for provision of tele-rehabilitation, and remotely delivered interventions to promote access to rehabilitation (14). A review of home-based tele-rehabilitation services in Southeast Asian countries found that the completion rates of interventions accessed by people with disabilities have been ~80% in China and South Korea (15). A recent survey from the sub-continent (India) had showed close to 80% of the rehabilitation facilities with basic tele-rehabilitation infrastructure (16). However, tele-health and rehabilitation services are not available and are poorly utilized by the government primary care systems in many countries in the region of Sub-Saharan Africa (17).
The practice of tele-health and rehabilitation had been an emerging science in improving access to healthcare and rehabilitation globally, even before the COVID-19 pandemic (18). The current pandemic has enabled its growth manifold by default worldwide. Tele-health and rehabilitation have become inevitable to meet the demands of those who need continued support globally (19). There have been a wide range of interventions and rationale for TNR. However, the experiences and evidence for organized provision of TNR services are very limited in LMICs.
Most types of TNR services in LMICs are used for two primary purposes: 1. clinical assessment and 2. therapeutic rehabilitation (20). The practice of neurorehabilitation has become more rewarding with the introduction/facilitation of TNR practice during COVID times. Guidelines for remote prescribing in several LMICs have also created access to medicines and strengthen primary care during the pandemic (21). A substantial amount of patient referrals are currently handled remotely through TNR (22). Tele-consultations are seen as equally effective and efficient as the face-to-face interaction with the added advantage of avoiding unnecessary exposure to infections (23). PWNDs are assessed and treated in their actual living environment, which is highly encouraging for the patients. It also reduces the service cost, and it cuts down the cost of traveling to access rehabilitation (23, 24). Therapeutic progress is currently being well-documented because of the auto-digitization features of telecommunication technology (23, 24). Overall, access to rehabilitation has improved with the introduction of TNR services. PWNDs who cannot travel due to their disability and the lockdown restrictions can still access rehabilitation and care without any access barriers and opportunity cost. Both providers of neurorehabilitation and the consumers are continuing to adapt to deliver and access services through TNR, respectively, in the current pandemic situation.
Overall, there are several implications to evaluate PWNDs and provide specialized, comprehensive multidisciplinary neurorehabilitation through TNR services in LMICs (8, 25). A key aspect to remember is that there must not be any compromise on the objectivity of the assessment or evaluation and therapeutic approaches for the management of the needs of PWNDs. Neurorehabilitation is a science that is driven by rigorous research-based evidence. Therefore, assessing and providing neurorehabilitation services, whether provided in-person or using telerehabilitation, must not have any compromise on its objectivity and evidence for evaluation and treatment. The current pandemic implies the need for systematically developed TNR interventions that is evaluated for its feasibility and acceptability and that is informed by available evidence from LMICs.
It is essential to understand the implications of TNR as this would enable identification of effective strategies for comprehensive assessment and treatment that can meet the needs of PWNDs. Though a potential opportunity, TNR cannot entirely replace the actual ways of delivering neurological rehabilitation (26). Neurologists can consult patients, provide treatment, and prescribe medications and referrals as appropriate. Optimizing TNR services for consultations had been proven feasible in HICs before and during the pandemic times (10, 18). However, available resources such as adequate internet bandwidth, devices with required configurations, and information management systems for implementing TNR services need to be in place. For instance, close to 1/3 of the Brazilian population lack access to internet (27). Although the providers have access to basic tele-rehabilitation infrastructure like in India, the consumers need to have internet access to avail such services (16).
From a physiatrist's perspective, continuity of treatment and care is something that TNR services could seamlessly support. PWNDs need continued care, and that can be enhanced through multidisciplinary neurorehabilitation team consultations led by the physiatrist virtually (28). Many South-Asian countries including India had come up with national guidelines on this (28, 29). Singapore's guidelines were considered comparatively comprehensive (29). Assessment of basic vital parameters, neurological status, pain, sleep, energy, spasticity, bladder and bowel, and mobility status; functionality of tracheostomy, feeding tube, and urinary catheters; patient and caregiver education; appropriate instructions for providing basic support; and interventions to prevent secondary complications are feasible with trained manpower keeping in mind the nature and course of the disease. However, to operationalize this, PWNDs and their caregivers must be thoroughly educated about these aspects of TNR. The literacy and understanding about tele-rehabilitation and use of tele-communication technologies for rehabilitation has been poor among those PWNDs even before the pandemic in many LMICs especially in Sub-Saharan Africa (29, 30). Considering these aspects will be crucial to enhance TNR services and enable service providers to achieve neurorehabilitation goals in a realistic way within their environment.
In this pandemic context, the neuropsychologist is expected to conduct neuropsychological evaluations and provide psychotherapy and cognitive rehabilitation for PWNDs through TNR (31, 32). However, it urges the understanding of its key implications. For instance, in Israel, the neuropsychological assessment services were postponed due to the pandemic with many people requiring such services put on a long waiting list. To combat this, the Israel government had developed remote solutions to meet the increasing demand for such services (33). Though these guidelines keep getting developed in many LMICs, some caveats need to be considered especially when it comes to administering standardized neuropsychological tests. There are significant differences between conducting a standardized neuropsychological evaluation in an ideal environment as compared to a virtual environment. Interpretation of the evaluations might differ and may not be the same while this is carried out virtually (33). Also, the neurorehabilitation team may have to rely substantially on the caregivers and patients to engage in the sessions proactively.
Given the high demand for physiotherapy services in LMICs, neuro-physiotherapists are accustomed to evaluate the range of motion, strength, muscle tone, and endurance of PWNDs through eye-balling sometimes. They are also competent to conduct a thorough neurological examination, including cranial nerve testing through performance-based assessments. Therefore, it is feasible to assess neurological disability remotely through TNR services (34, 35). However, the provision of actual therapy or intervention using specialized techniques must be carried out with utmost safety considerations. During the provision of TNR physiotherapy services, patients and caregivers may not comprehend the instructions as they do this in-person, leading to serious untoward incidences. Hence, many HICs like Australia and the UK recommend developing highly competent inter-professional rehabilitation services as well as a frameworks or guidelines to enhance the provision of physiotherapy services remotely using technology (36).
Speech–language pathologists (SLPs) are one of the key neurorehabilitation professionals who are not easily available and accessible in LMICs (37). It was estimated that there were only 2,500 SLPs in India, which is an acute shortage of such key neurorehabilitation professionals delivering care (38). However, it is commonly perceived that provision of assessment and rehabilitation for patients with neurological and neurosurgical disorders presenting with safe swallowing, speech, language, and cognitive-communication dysfunctions are some of the key aspects to include during tele-practice by SLPs across all age group in LMICs (39). Use of hybrid methods could also be a potential strategy in the management of neurodevelopmental and acquired communication disorders, dysarthria, oropharyngeal dysphagia, and cognitive-communication disorders experienced by patients reporting in outpatient as well as in-patient settings (40). There are examples from certain countries like the Indian Speech and Hearing Association that had published the tele-practice guidelines and specific resource material for speech–language pathology and audiology services in India (41). However, it is well-known that even during the pre-pandemic times, it was estimated that only 10%-12% of SLPs tend to use tele-practice as a strategy for providing SLP services in India (38). A similar survey recently in Croatia had also estimated that only 3% of those SLPs surveyed had completed a formal training related to tele-practice in SLP services. Several consumers in the survey expressed the lack of equipment and trust on the effectiveness of tele-practice as the reasons for non-utilization of such services (42). Hence, organizing TNR services provided for swallowing and cognitive communication requires careful planning and efficient strategies for implementation.
For OTs, it is critical to give utmost importance to performance than hospital-based rehabilitation, thus making TNR feasible for neuro-OTs (43). OTs are meant to assess and therapeutically manage the actual occupational performance of PWNDs like participation in activities of daily living (ADL), work, and leisure in their home/social environment (44). This strategy could help provide need-based, scientific, and therapeutically rigorous OT services using TNR framework in real-life contexts. Given that many occupational therapy assessments are based on function, it is also possible to incorporate real-life functional assessments for PWNDs. It would also provide immense opportunities for OTs to standardize these assessments for neurorehabilitation in the future in such contexts. Similar to the context of the SLPs, OTs are also scarce globally and especially in LMICs. The most frequently cited domains where OTs are scarce are directly related to conditions that predispose neurological disabilities. Therefore, it is of utmost importance that professional resources and expertise like OTs and SLPs must be protected and developed to address the needs of PWNDs through TNR during the COVID-19 pandemic.
Though there are several feasible aspects for implementing TNRs for PWNDs, it is also necessary to understand the barriers that need to be considered with caution. Not everything could be feasible, especially considering how rehabilitation services are organized for PWDs in general in LMICs. Therefore, it is highly pertinent to tease out the barriers for TNR services provided to PWNDs in LMICs.
Table 1 depicts the non-feasible aspects of TNR, especially in LMICs. The first and foremost aspect that may not be feasible while implementing TNR in LMICs is the comprehensive and intrinsically detailed neurological evaluation and treatment. This is especially because some of the evaluation and treatment require safe hands-on as well as moving and handling patients, and one cannot do this in TNR. Similarly, neurologists and physiatrists cannot prescribe certain drugs through TNR (45). There are also certain criteria for patient exclusion unless the TNR service is exclusively developed for the requirements. People with severe cognitive-perceptual, emotional, and behavioral issues, young children, and frail elderly patients with silent aspiration, visual, speech, and hearing impairment can most often be excluded from a comprehensive TNR service that may not be available to all in the LMIC context. PWNDs and their caregiver cooperation, privacy, and non-distractible environment are also some key aspects that could prove challenging and non-feasible while providing TNR services.
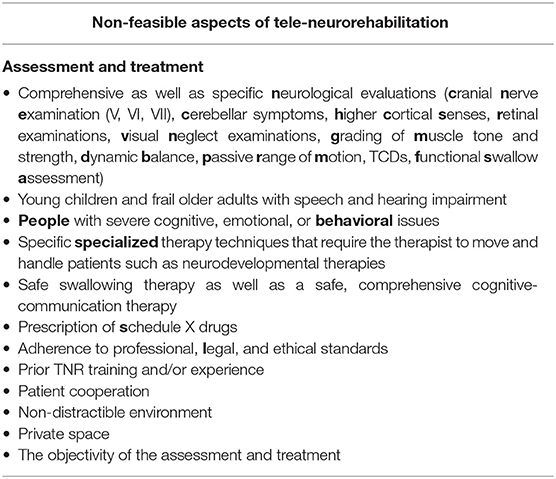
Table 1. Non-feasible aspects of tele-neurorehabilitation.
From the perspective of the TNR service providers, it is imperative that one needs prior training and sufficient experience in using TNR to deliver neurorehabilitation. This particular aspect is taken for granted since most providers assume that using a smartphone or computer can qualify them to deliver TNR services during the pandemic. It is also important that the neurorehabilitation providers do not lose objectivity of the evaluation and treatment while delivering TNR interventions since there is a high possibility for this to happen in the LMIC contexts. Despite the non-existence of any regulatory framework, the neurorehabilitation provider must maintain their highest legal, professional, and ethical standards to deliver safe and effective rehabilitation.
There are three kinds of clear-cut challenges to the implementation of TNR services for PWNDs in LMICs. They are the scientific, technological, and administrative aspects of implementing TNR. Table 2 provides more details of these aspects. From a scientific perspective, delivering TNR services requires specific competencies, and those competencies are not necessarily taught or achieved by neurorehabilitation professionals exclusively in the pre-pandemic times (46). However, competencies for delivering TNR services play a crucial role in making appropriate professional judgments and decisions for the patients. Lack of specific training and education to achieve such competencies within the curriculum of these professionals is a huge challenge (47). Similarly, striking a balance between patient autonomy and non-maleficence in decision making is very difficult when there is no evidence for such decisions in LMICs. TNR services are just emerging to bridge the gaps in access in LMICs and may not hold the same evidence for treatment delivered in person.
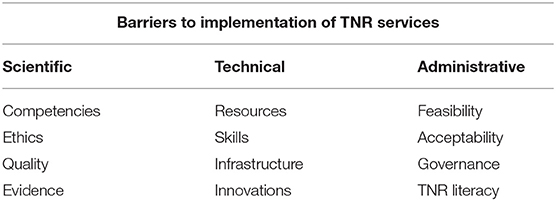
Table 2. Barriers to implementation of TNR services in LMICs.
Delivering TNR services has become a necessity in the pandemic situation. However, it must not compromise safe, effective, and good quality patient care that the patient may have received otherwise (36). Obtaining consent for the provision of therapeutic interventions through TNR services is not as easy as doing it in person. PWNDs and their primary caregivers must be thoroughly informed about the pros and cons of the decisions or choices available for treatment, enabling them to consent (48, 49). Given that neurorehabilitation professionals are accountable and responsible for their patients, due considerations must be provided to the scientific, professional, and ethical aspects of delivering TNR services for PWNDs.
There are several technological challenges in delivering TNR services. Aspects such as availability of telecommunication technologies such as computers, tablets, and smartphones; technological access features such as connectivity, bandwidth, data storage and management, server capacity, synchronization, and network; skilled workforce to synergistically support the implementation of TNR services; and the infrastructure for hosting and delivering TNR services for PWNDs must be ensured before embarking into service provision through TNR (50). These aspects require tremendous resources in terms of both funding and technology. It also requires skilled telecommunication experts to work with neurorehabilitation experts to innovate TNR interventions that are safe, effective, and of high public health value.
Additionally, from the perspective of the TNR service providers, it is imperative that one needs prior training and sufficient experience in using TNR to deliver neurorehabilitation. This particular aspect is taken for granted since most providers assume that using a smartphone or computer can qualify them to deliver TNR services during the pandemic. It is also important that the neurorehabilitation providers do not lose objectivity of the evaluation and treatment while delivering TNR interventions since there is a high possibility for this to happen in the LMIC contexts. Despite the non-existence of any regulatory framework, the neurorehabilitation provider must maintain their highest legal, professional, and ethical standards to deliver safe and effective rehabilitation.
Even if the scientific and technological challenges are addressed, administering TNR services is an immense strategic challenge. TNR service itself is an innovative intervention that must be feasible for implementation. In LMICs, much of the health and rehabilitation services is accessed through the private sector; hence, ensuring uniformity in the services and standards similar to the public run services may be challenging (51). Rehabilitation facilities can be small, with only an out-patient facility to a comprehensive in-patient facility. Similarly, the neurorehabilitation team can be a small team with a minimum of neurologists and physiotherapists to a comprehensive team with a physiatrist, OTs, SLPs, orthotist, and neuropsychologist in addition to the neurologist and physiotherapist (8). Therefore, implementation of TNR services within this wide range of service structure is highly challenging. It would certainly require a strong system of governance mechanisms to ensure the quality and safety of TNR services delivered in these facilities. To develop or strengthen the existing governance mechanisms, one must have TNR literacy. Without understanding the principles of neurorehabilitation and the application of telecommunication technology in it, it is not possible to govern TNR services in any context.
The same applies to the primary stakeholder of TNR services. PWNDs and caregivers must have TNR literacy or at least be technology literates to optimize TNR services (7). Without this literacy, patients and caregivers might not find value for their time and resources invested and potentially may not accept TNR services for themselves or their loved ones. It is also a crucial challenge to educate all the stakeholders, primarily the patients and their caregivers, about the benefits of TNR in LMICs.
Given the lack of organized systems in place for the provision of neurorehabilitation services in general, there needs to be sufficient budgetary allocations and a sector-wide approach to the development of policies and systems for the provision of TNR services for PWNDs. These allocations and actions must be from the Department of the Ministry of Health and all other ministries/departments, such as education, technology, telecommunications, and social justice, in a convergent manner (52). By default, the existing pandemic situation provided an opportunity to optimize the technological innovations in health and scale up these innovations to meet the growing burden of neurological disability in LMICs. Thus, this immense opportunity must be tapped to build capacity for safe and effective TNR services provision for PWNDs in these settings.
There have been several assumptions globally when attempting to understand the implications of TNR services. The primary assumption is that everyone has sufficient information and knowledge about both TNR and the COVID-19 pandemic. This assumption gives anyone the leverage to start TNR services. However, this could be detrimental if the science and standards for practice are not evidence-based. In the context of LMICs and the pandemic, the neurorehabilitation team can give due importance to the performance of the neurologically disabled rather than to sophisticated clinical procedures to ensure TNR becomes a reality in these settings. This can enable bridging the gaps in evidence with relevant science and rigor. This subsequently eludes the scientific community to the need for innovations that can connect people and professionals through technology in this pandemic and beyond. The future of neurorehabilitation could radically change, if we utilize these learning from the pandemic period to make TNR services accessible, affordable, and available (53, 54).
A potential link must be established between the remote TNR services and in-person neurological rehabilitation service provision. This could add value to the health and social care systems that were previously developed for serving the needs of PWND. The link must have due considerations to the needs of the PWNDs. It must also include the needs of the primary caregivers and family who provide continuous support to PWND before, during, and even in the post-pandemic situation. There is a definite implication that this link must strike a balance between access and availability of neurorehabilitation services. This is especially required in LMICs. There is also a need to make accessibility and availability of TNR services consistent across geography, disciplines, and conditions. This is potentially possible by reducing the variation and inconsistencies in terms of the intensity of rehabilitation measured by the dosage, duration, team expertise involved, and goals set and achieved for PWND in LMICs. An amalgamation of the existing system (pre-pandemic) with the innovative TNR systems to support PWND during the pandemic situation could be a feasible solution. This could serve as a potentially possible strategy, even in the future post-pandemic era.
This situation highlights the importance of two key aspects for immediate attention. The first is building the capacity of the patients, caregivers, and families with rigorous evidence-based training using simple protocols and culturally acceptable versions of optimizing TNR services. The training should also be provided to the providers of TNR services especially in terms of safe and effective use of telecommunication technology for neurological rehabilitation. Second, there is a need for immense government support to legitimately develop resources for TNR services such as guidelines and research evidence and address the growing burden of neurological disabilities in LMICs. The IFNR research task force has realized this opportunity to support the PWNDs in need and also the government. It had initiated the development of systematic action plans toward addressing the burden of neurological disabilities. As a first logical step, IFNR aims to develop a national guideline for the provision of TNR in India, and it recommends the same for all LMICs.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
On behalf of the IFNR Taskforce, all the authors contributed equally toward the development of this manuscript. All authors agree to be accountable for the content of the work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the Indian Federation of Neurorehabilitation and the World Federation of NeuroRehabilitation for their constant support toward the development of this manuscript. We also thank Mohamad Intan Sabrina from the Ministry of Health, Malaysia; Mazlina Binti Mazlan from the University of Malaysia; Hitav Someshwar from the World Federation for Neurorehabilitation (South Asia), Mumbai India; and Carl Froilan D Leochico from the University of the Philippines Manila, The Philippines for their critical inputs and support during the conceptualization of this work.
Abhishek Srivastava1, Neurorehab Specialist and Director, Centre for Physical Medicine and Rehabilitation, Kokilaben Dhirubhai Ambani Hospital and Medical Research Institute, Mumbai, India; Aishwarya Swaminathan2, School of Occupational Therapy, D. Y. Patil University, Navi Mumbai, India; Manigandan Chockalingam3, Lecturer in Occupational Therapy, National University of Ireland Galway, Galway, Ireland; Murali K. Srinivasan4, Faculty of Occupational Therapy, Meenakshi Academy of Higher Education and Research, Chennai, India; Nirmal Surya5, Chairman Surya Neuro Centre Mumbai, President Indian Federation of Neurorehabilitation (IFNR), Mumbai, India; Partha Ray6, Consultant Neurologist and Clinical Neurophysiologist National Health Services England, The Walton Centre Liverpool & National Professor of Neurology, Liverpool, United Kingdom; Prasanna S. Hegde7, Speech-Language Pathology, Program Director, Speech and Swallow Specialist, Deglutology and Speech-Language Pathology, HCG Hospital, Bangalore, India; Preetie Shetty Akkunje8, Senior Research Fellow, Department of Speech Pathology and Audiology, National Institute of Mental Health and Neurosciences, Bangalore, India; Sanjivani Kamble9, Dr. D. Y. Patil College of Physiotherapy, Dr. D. Y. Patil Vidyapeeth, Pune, India; Sonal Chitnis10, Assistant professor, Bharati Vidyapeeth (Deemed to be) University, School of Audiology Speech-Language Pathology, Pune, India; Sureshkumar Kamalakannan11, South Asia Centre for Disability Inclusive Development and Research (SACDIR), Public Health Foundation of India, The Indian Institute of Public Health Hyderabad, Hyderabad, India; Suvarna Ganvir12, Department of Neuro physiotherapy, Dr Vitalrao Vikhe Patil Foundation's College of Physiotherapy, Ahmednagar, India; Urvashi Shah13, Consultant Neuropsychologist, Department of Neurology, King Edward Memorial and Global Hospitals Mumbai, Mumbai, India.
1. Carroll WM. The global burden of neurological disorders. Lancet Neurol. (2019) 18:418–9. doi: 10.1016/S1474-4422(19)30029-8
2. Collins TR. Neurologic diseases were found to be the largest cause of disability worldwide. Neurol Today. (2020) 17:132–5. doi: 10.1097/01.NT.0000527316.80068.88
3. Group GBDNDC. Global, regional, and national burden of neurological disorders during 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet Neurol. (2017) 16:877–97. doi: 10.1016/S1474-4422(17)30299-5
4. Bawah A, Houle B, Alam N, Razzaque A, Streatfield PK, Debpuur C, et al. The evolving demographic and health transition in four low- and middle-income countries: evidence from four sites in the INDEPTH network of longitudinal health and demographic surveillance systems. PLoS ONE. (2016) 11:e0157281. doi: 10.1371/journal.pone.0157281
5. Kamalakannan S, Bhattacharjya S, Bogdanova Y, Papadimitriou C, Arango-Lasprilla JC, et al. Refugee empowerment task force, international networking group of the american congress of rehabilitation medicine. Health risks and consequences of a COVID-19 infection for people with disabilities: scoping review and descriptive thematic analysis. Int J Environ Res. Public Health. (2021) 18:4348. doi: 10.3390/ijerph18084348
6. Kim SY, Kumble S, Patel B, Pruski AD, Azola A, Tatini AL, et al. Managing the rehabilitation wave: rehabilitation services for COVID-19 survivors. Arch Phys Med Rehabil. (2020) 101:2243–9. doi: 10.1016/j.apmr.2020.09.372
7. Bright T, Wallace S, Kuper H. A systematic review of access to rehabilitation for people with disabilities in low- and middle-income countries. Int J Environ Res Public Health. (2018) 15:2165. doi: 10.3390/ijerph15102165
8. Platz T, Sandrini G. Specialty grand challenge for neurorehabilitation research. Front Neurol. (2020) 11:349. doi: 10.3389/fneur.2020.00349
9. Appleby E, Gill ST, Hayes LK, Walker TL, Walsh M, Kumar S. Effectiveness of telerehabilitation in the management of adults with stroke: a systematic review. PLoS ONE. (2019) 14:e0225150. doi: 10.1371/journal.pone.0225150
10. Cadilhac DA, Prvu Bettger J. Health policy and health services delivery in the era of COVID-19. Stroke. (2021) 52:2177–9. doi: 10.1161/STROKEAHA.121.033292
11. Khanna M, Gowda GS, Bagevadi VI, Gupta A, Kulkarni K, RP SS, et al. Feasibility and utility of tele-neurorehabilitation service in india: experience from a quaternary center. J Neurosci Rural Pract. (2018) 9:541–4. doi: 10.4103/jnrp.jnrp_104_18
12. Gowda GS, Manjunatha N, Kulkarni K, Bagewadi VI, Shyam RP, Basavaraju V, et al. A collaborative tele-neurology outpatient consultation service in Karnataka: seven years of experience from a tele-medicine center. Neurol India. (2020) 68:358–63. doi: 10.4103/0028-3886.280644
13. Sarfo FS, Adusei N, Ampofo M, Kpeme FK, Ovbiagele B. Pilot trial of a tele-rehab intervention to improve outcomes after stroke in Ghana: a feasibility and user satisfaction study. J Neurol Sci. (2018) 387:94–7. doi: 10.1016/j.jns.2018.01.039
14. Fioratti I, Fernandes LG, Reis FJ, Saragiotto BT. Strategies for a safe and assertive telerehabilitation practice. Braz J Phys Ther. (2021) 25:113–6. doi: 10.1016/j.bjpt.2020.07.009
15. Saito T, Izawa KP. Effectiveness and feasibility of home-based telerehabilitation for community-dwelling elderly people in Southeast Asian countries and regions: a systematic review. Aging Clin Exp Res. (2021). doi: 10.1007/s40520-021-01820-3. [Epub ahead of print].
16. Surya N, Srivastava A, Nagda T, Palande D, Someshwar H. Education, training, and practices of neurorehabilitation in India during the COVID-19 pandemic. Front. Neurol. (2021) 12:626399. doi: 10.3389/fneur.2021.626399
17. Dolapo B, Michael A, David AI. Telehealth during COVID-19: why Sub-Saharan Africa is yet to log-in to virtual healthcare?[J]. AIMS Med Sci. (2021) 8:46–55. doi: 10.3934/medsci.2021006
18. World Health Organization. mHealth New Horizons for Health Through Mobile Technologies Based on the Findings of the Second Global Survey on eHealth: Global Observatory For eHealth Series. Geneva (2011). p. 112.
19. Monaghesh E, Hajizadeh A. The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Health. (2020) 20:1193. doi: 10.1186/s12889-020-09301-4
20. Laver KE, Adey-Wakeling Z, Crotty M, Lannin NA, George S, Sherrington C. Telerehabilitation services for stroke. Cochrane Database Syst Rev. (2020) 1:CD010255. doi: 10.1002/14651858.CD010255.pub3
21. Peretti A, Amenta F, Tayebatig SK, Nittari G, Mahdi SS. Telerehabilitation: review of the state-of-the-art and areas of application. JMIR Rehabil Assist Technol. (2017) 4:e7. doi: 10.2196/rehab.7511
22. Hoffer-Hawlik MA, Moran AE, Burka D, Kaur P, Cai J, Frieden TR, et al. Leveraging telemedicine for chronic disease management in low- and middle-income countries during Covid-19. Glob Heart. (2020) 15:63. doi: 10.5334/gh.852
23. Nitkunan A, Paviour D, Nitkunan T. COVID-19: switching to remote neurology outpatient consultations. Pract Neurol. (2020) 20:222–4. doi: 10.1136/practneurol-2020-002571
24. Hwang NK, Park JS, Chang MY. Telehealth interventions to support self-management in stroke survivors: a systematic review. Healthcare. (2021) 9:472. doi: 10.3390/healthcare9040472
25. Brennan DM, Mawson S, Brownsell S. Telerehabilitation: enabling the remote delivery of healthcare, rehabilitation, and self-management. Stud Health Technol Inform. (2009) 145:231–48. doi: 10.3233/978-1-60750-018-6-231
26. Rollnik JD, Pohl M, Mokrusch T, Wallesch CW. Telerehabilitation cannot replace traditional neurological rehabilitation. Nervenarzt. (2017) 88:1192–3. doi: 10.1007/s00115-017-0420-1
27. Fernandes LG, Saragiotto BT. To what extent can telerehabilitation help patients in low-and middle-income countries? Braz J Phys Ther. (2020). doi: 10.1016/j.bjpt.2020.11.004. [Epub ahead of print].
28. Board of Governors in supersession of the Medical Council of India. Telemedicine practice guidelines. 1st ed. India BoG-MCI. New Delhi. India (2020).
29. Intan Sabrina M, Defi IR. Telemedicine guidelines in south east asia-a scoping review. Front Neurol. (2021) 11:581649. doi: 10.3389/fneur.2020.581649
30. Adebayo PB, Oluwole OJ, Taiwo FT. COVID-19 and teleneurology in sub-saharan Africa: leveraging the current exigency. Front Public Health. (2021) 8:574505. doi: 10.3389/fpubh.2020.574505
31. Taddei M, Bulgheroni S. Facing the real-time challenges of the COVID-19 emergency for child neuropsychology service in Milan. Res Dev Disabil. (2020) 107:103786. doi: 10.1016/j.ridd.2020.103786
32. Spreij LA, Visser-Meily JM, Sibbel J, Gosselt IK, Nijboer TC. Feasibility and user-experience of virtual reality in neuropsychological assessment following stroke. Neuropsychological Rehabil. (2020). doi: 10.1080/09602011.2020.1831935. [Epub ahead of print].
33. Bloch A, Maril S, Kavé G. How, when, and for whom: decisions regarding remote neuropsychological assessment during the 2020 COVID-19 pandemic. Isr J Health Policy Res. (2021) 10:31. doi: 10.1186/s13584-021-00465-x
34. Haines KJ, Berney S. Physiotherapists during COVID-19: usual business, in unusual times. J Physiother. (2020) 66:67–9. doi: 10.1016/j.jphys.2020.03.012
35. Aderonmu JA. Emerging challenges in meeting physiotherapy needs during COVID-19 through telerehabilitation. Bull Fac Phys Ther. (2020) 25:16. doi: 10.1186/s43161-020-00018-4
36. Prvu Bettger J, Resnik LJ. Telerehabilitation in the age of COVID-19: an opportunity for learning health system research. Phys Ther. (2020) 100:1913–6. doi: 10.1093/ptj/pzaa151
37. Karan A, Negandhi H, Hussain S, Zapata T, Mairembam D, De Graeve H, et al. Size, composition and distribution of health workforce in India: why, and where to invest? Hum Resour Health. (2021) 19:39. doi: 10.1186/s12960-021-00575-2
38. Mohan HS, Anjum A, Rao PK. A survey of telepractice in speech-language pathology and audiology in India. Int J Telerehabil. (2017) 9:69–80. doi: 10.5195/ijt.2017.6233
39. Wylie K, McAllister L, Davidson B, Marshall J. Communication rehabilitation in sub-Saharan Africa: the role of speech and language therapists. Afr J Disabil. (2018) 7:338. doi: 10.4102/ajod.v7i0.338
40. Dimer NA, Canto-Soares ND, Santos-Teixeira LD, Goulart BNG. The COVID-19 pandemic and the implementation of telehealth in speech-language and hearing therapy for patients at home: an experience report. Codas. (2020) 32:e20200144. doi: 10.1590/SciELOPreprints.610
41. Vrinda R, Reni PS. Telerehabilitation in the field of speech language pathology during pandemic COVID-19 outbreak-an analysis in Kerala. Biosc Biotech Res Comm. (2020) 13. doi: 10.21786/bbrc/13.4/99
42. Kuvac Kraljevic J, Matic A, Pavicic Dokoza K. Telepractice as a reaction to the COVID-19 crisis: insights from croatian SLP settings. Int J Telerehabil. (2020) 12:93–104. doi: 10.5195/ijt.2020.6325
43. Kamalakannan S, Chakraborty S. Occupational therapy: the key to unlocking locked-up occupations during the COVID-19 pandemic. Wellcome Open Res. (2020) 5:153. doi: 10.12688/wellcomeopenres.16089.1
44. World Federation of Occupational Therapists. Human Resources Project – Numerical. (2016). Available online at: http://www.wfot.org/ResourceCentre.aspx (accessed June 25, 2021).
45. Ministry of Health and Family Welfare. (2021). Available online at: https://www.mohfw.gov.in/pdf/Telemedicine.pdf (accessed February 13, 2021).
46. Kuper H, Banks LM, Bright T, Davey C, Shakespeare T. Disability-inclusive COVID-19 response: what it is, why it is important and what we can learn from the United Kingdom's response. Wellcome Open Res. (2020) 5:79. doi: 10.12688/wellcomeopenres.15833.1
47. Ganapathy K. Telemedicine and neurological practice in the COVID-19 Era. Neurol India. (2020) 68:555–9. doi: 10.4103/0028-3886.288994
48. Ozden F, Lembarki Y. The ethical necessities and principles in telerehabilitation. J Health Serv Educ. (2020) 3:35–7. doi: 10.35333/JOHSE.2020.130
49. Bali S. Barriers to development of telemedicine in developing countries. Intech Open. (2018). doi: 10.5772/intechopen.81723
50. Druetz T. Integrated primary health care in low- and middle-income countries: a double challenge. BMC Med Ethics. (2018) 19(Suppl. 1):48. doi: 10.1186/s12910-018-0288-z
51. Leochico CFD, Espiritu AI, Ignacio SD, Mojica JAP. Challenges to the emergence of telerehabilitation in a developing country: a systematic review. Front Neurol. (2020) 11:1007. doi: 10.3389/fneur.2020.01007
52. Nuara A, Fabbri-Destro M, Scalona E, Lenzi SE, Rizzolatti G, Avanzini P. Telerehabilitation in response to constrained physical distance: an opportunity to rethink neurorehabilitative routines. J Neurol. (2021) 1–12. doi: 10.1007/s00415-021-10397-w
53. Maresca G, Maggio MG, De Luca R, Manuli A, Tonin P, Pignolo L, et al. Tele-Neuro-Rehabilitation in Italy: state of the art and future perspectives. Front Neurol. (2020) 11:563375. doi: 10.3389/fneur.2020.563375
Keywords: neurorehabilitation, tele-rehabilitation system, neurological disability, COVID-19, pandemic (COVID-19), low- and middle-income countries
Citation: Srivastava A, Swaminathan A, Chockalingam M, Srinivasan MK, Surya N, Ray P, Hegde PS, Akkunje PS, Kamble S, Chitnis S, Kamalakannan S, Ganvir S, Shah U and the Indian Federation of Neurorehabilitation (IFNR) Research Task Force (2021) Tele-Neurorehabilitation During the COVID-19 Pandemic: Implications for Practice in Low- and Middle-Income Countries. Front. Neurol. 12:667925. doi: 10.3389/fneur.2021.667925
Received: 15 February 2021; Accepted: 23 August 2021;
Published: 05 October 2021.
Edited by:
Giorgio Sandrini, Fondazione Cirna Onlus, ItalyReviewed by:
Michelangelo Bartolo, Casa di Cura Habilita SpA, ItalyCopyright © 2021 Srivastava, Swaminathan, Chockalingam, Srinivasan, Surya, Ray, Hegde, Akkunje, Kamble, Chitnis, Kamalakannan, Ganvir, Shah and the Indian Federation of Neurorehabilitation (IFNR) Research Task Force. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nirmal Surya, bmlybWFsX3N1cnlhQHlhaG9vLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.