 Stefanie Danielle Piña-Escudero1,2,3*
Stefanie Danielle Piña-Escudero1,2,3* Gloria Annette Aguirre1,3
Gloria Annette Aguirre1,3 Shireen Javandel1,3
Shireen Javandel1,3 Erika Mariana Longoria-Ibarrola1,4
Erika Mariana Longoria-Ibarrola1,4- 1The Global Brain Health Institute, University of California, San Francisco, San Francisco, CA, United States and Trinity College, Dublin, Ireland
- 2Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
- 3Department of Neurology, Memory and Aging Center, University of California, San Francisco, San Francisco, CA, United States
- 4Instituto Nacional de Neurología y Neurocirugía José Velazco Suárez, Mexico City, Mexico
Latin America is a vast heterogeneous territory where chronic diseases such as mild cognitive impairment or dementia are becoming higher. Frontotemporal dementia (FTD) prevalence in this region is estimated to be around 12–18 cases per thousand persons. However, this prevalence is underestimated given the lack of awareness of FTD even among healthcare professionals. Family members are responsible for the care of patients with FTD at home. These caregivers deliver care despite being ill-equipped and living in the context of austerity policies and social inequities. They often face unsurmountable financial and social burdens that are specific to the region. The most important step to support caregivers in Latin America is to increase awareness of the disease at all levels. Healthcare diplomacy is fundamental to create joint efforts that push policies forward to protect caregivers of FTD patients.
Introduction
In Latin America, dementia numbers are rapidly rising (1). The incidence of dementia diagnosis has been estimated between 9.10 and 13.8 per 1,000 people/year (2, 3). The global dementia prevalence in Latin American among older adults is 11% with Alzheimer's Disease being the most frequent type (4). In Latin American middle-income countries, the mortality risk is 1.56–5.69 times higher than in individuals without dementia (5). FTD is a term used to encompass the clinical syndromes that result from frontotemporal lobar degeneration pathology. These clinical syndromes include the behavioral variant of FTD (bvFTD), semantic and non-fluent variants of primary progressive aphasia (PPA), and the overlap syndromes with amyotrophic lateral sclerosis (FTD-ALS) or with other parkinsonian syndromes (i.e., corticobasal syndrome, progressive supranuclear palsy) (6). There is little information about the prevalence of FTD in Latin America, but it is estimated to be around 12 to 18 cases per thousand persons in community-dwelling settings (7), which is in line with estimates in other countries (10.84/100,000) (8, 9). In high-income countries, studies of FTD have increased considerably over the last decade and FTD is now considered the second leading cause of dementia for those under 65 years (10), thanks to the many advances in neuropathology, biochemistry, and genetics that clarified correlations between molecular profiles and clinical phenotypes (11).
In contrast, in Latin America, these resources are extremely limited and most healthcare professionals, even specialists, are unaware of FTD and lack the training to diagnose it (12, 13). The model of memory clinics that is commonly found in developed countries is extremely limited in Latin America and constrained mostly to big cities (14). In rural settings, economic and geographical barriers limit access to specialized healthcare even more (15). Scarce financial and social resources, limited knowledge about the disease, and competing health and social needs challenge caregivers around the world, however, in low-income countries, inequality has substantially affected capacity building for diagnosis and follow-up care in FTD. In Latin America, informal employment is the source of income of more than half of the households, resulting in limited access to medical services, disability insurance, and other benefits associated with formal employment (16, 17). The few public services that ensure continuity of care for patients such as in-home care, long-term care, and palliative care cover only a very small sector of the population (18). Additionally, few private resources are available and are accessible only for patients who have financial resources to cover the high costs (19). In high-income countries, the estimated annual cost for care for patients with FTD can be over $100,000 (twice the cost of care for a patient with Alzheimer's disease) (20). In Latin America, FTD care represents an insurmountable financial burden.
Caregiving for FTD Patients in LAC
Since research in FTD is a niche science in Latin America with only a few published manuscripts, research on caregiving in FTD is practically non-existent in the region. In fact, we conducted a literature search of the published literature on PubMed, EMBASE, and Web of Science databases up to April 2021. The search strategy that retrieved the majority of the studies used the keywords “caregiver burden” AND “frontotemporal dementia.” From the 268 retrieved articles, just two of them were conducted in Latin America and just one covered the relationship between caregivers and patients with FTD. Due to the scarcity of published work around this topic, our effort was focused on contextualizing the challenges and lived experiences of caregivers of patients with FTD in Latin America, setting the stage for future avenues of research on this topic.
In Latin America, most of the caregivers for patients with FTD are family members. They compensate for the lack of formal governmental support and insufficient financial resources by taking care of patients with FTD at home. This responsibility can consume more than 8 h a day (21). Often influenced by cultural factors, caregiver roles are mainly fulfilled by females (22, 23). These women oftentimes have low education and live in multigenerational households where taking care of the patient is not their main role (21, 22). Female caregivers have to play multiple roles such as wives, daughters, mothers, or employees, and more often than is the case with men, women's caregiving roles interfere with other life activities, which may ultimately lead to “role-captivity” (caregiver feelings of being “trapped” in their role) (24). Caregivers frequently take care of patients at home, setting an example for their children about family obligation and intergenerational reciprocity (25). In the context of FTD, it is important to account that genetic variants of the disease such as mutations in C9ORF72, MAPT, GRN, TARDBP, etc. have been described to affect large families in Latin America and a caregiver may be in charge of the care of multiple sick members of a family (26).
Challenges for Caregivers of Patients With bvFTD
The trajectory of perceived caregiver burden depends largely on the clinical phenotype of the patient and the practical daily issues that derive from each syndrome (27). bvFTD is characterized by behavioral disinhibition, apathy, loss of empathy, perseverative, stereotyped, or compulsive/ ritualistic behaviors, binge eating behavior, and dietary changes (28). Common behaviors include inappropriate sexual conduct, shoplifting, aggression, loss of manners, and tactlessness. The study of Lima Silva et al. showed that, compared to Alzheimer's disease, Brazilian participants with FTD presented more agitation/aggression (0.001), apathy (<0.001), disinhibition (<0.001), euphoria (0.021), and irritability (0.003) (29). All of these behavioral symptoms place a heavy toll on caregivers from the beginning of the patient's disease. Brazilian caregivers of participants with FTD doubled the distress scores of their counterparts caring for participants with Alzheimer's disease measured by the Caregiver Distress Scale part of the Neuropsychiatric Inventory obtaining 13.22 (±7.94) vs. 6.13 (±4.67) points respectively with a p < 0.001. The participant's symptoms that generated the statistically significant differences in caregivers' distress were apathy, disinhibition, irritability, and aggression (29). It can be particularly emotionally taxing when caregivers do not understand these behaviors to be symptoms of dementia because of cultural views or because it is difficult to obtain a diagnosis from a healthcare provider.
Since behavioral symptoms often present in patients before the age of 65 without other neurological and/or cognitive complaints (28), they are frequently not interpreted as pathological by physicians. The study conducted by Gleichgerrcht et al. showed that <30% of general practitioners in Latin America have heard of bvFTD during their medical training (12). Coping with a patient presenting misunderstood behavioral symptoms can lead to emotions of shame, irritation, guilt, exhaustion, and fear in the caregivers. These negative emotions can affect their interpersonal relationships with the patients and even lead to mistreatment (30, 31). In Latin America, there is also a strong culture of unconditional respect for the patriarch. Women and young family members caring for an older male may find it uncomfortable to redirect inappropriate behaviors, not wishing to be seen as lacking respect (32, 33). Further complicating matters, caregivers may be less likely to seek professional help if the presenting behavioral symptoms consist of inappropriate sexual comments, excessive drinking, and/or aggressivity, as these actions are often dismissed or even accepted within Latin American cultures. As a result of this sociocultural setting, caregivers themselves may see the behaviors as intentional, not recognizing them as symptoms of bvFTD (33), potentially delaying interventions of benefit to the patient. On the positive side, since pathological behaviors are within the accepted social norms, caregivers might experience less burden when caring for these patients. This could be a possible explanation for the unexpected findings of Lima-Silva et al. that reported that in a predominantly masculine cohort in Brazil, caring for participants with FTD with behavioral symptoms, even when more distressful, was not more burdensome than caring for patients with Alzheimer's disease measured by the Zarit Burden Inventory (p = 0.150) (29). If these same behaviors are present in women with FTD, particularly impulsivity related to sexual behaviors, caregivers may feel shame and isolate themselves and the patients from society to avoid public embarrassment (34, 35). The CUIDEME Study reported that in a predominantly female cohort with dementia in Chile, a higher number of neuropsychiatric symptoms in the Neuropsychiatric Inventory correlated with a higher caregiver burden (p < 0.001) (23). Chronic stress from constant aggression and social isolation increase burden and the caregiver's risk for physical and mental illness (36).
There can also be a substantial financial burden of caring for patients with bvFTD, even when families are not paying for formal care. Symptoms like apathy, impulsivity, inability to engage in complex activities can result in loss of employment early in the course of the disease. With a relatively young age of onset, many families of patients with bvFTD are still reliant on the patient's income and this loss can represent a considerable financial strain as the family will need to take care of the patient while establishing a new primary source of income. Furthermore, family members who become caregivers have less opportunity to advance their own careers or to support the educational or career advancement of their children (21). The COVID-19 pandemic has been especially challenging for the caregivers of patients with bvFTD as behavioral and cognitive symptoms make these patients less likely to follow the safety recommendations, putting themselves and their caregivers at a higher risk of contracting the virus.
Limited public healthcare resources and the high cost of private care can also increase the burden that caregivers of patients with bvFTD experience. Patients with bvFTD are usually referred for a psychiatric evaluation as behavioral symptoms progress (37). For many caregivers, getting the patient to specialized medical care represents a huge challenge. Mental health services in general hospitals are very limited. Outside of Argentina and Uruguay, Latin American countries have fewer than 10 psychiatrists per 100,000 citizens (38). Therefore, families who do not live in urban areas often need to travel long distances to receive this specialized care and they must cover those expenses out of pocket, which can present a high financial burden. Additionally, the proportion of psychiatrists in Latin America who answered affirmatively to whether they diagnose dementia went from (yes to no ratio) 6:1 to 1.49:1 when asked if they make the differential diagnosis of bvFTD (12). Therefore, since few psychiatric specialists are trained to identify bvFTD, diagnosis may be delayed, further referrals could be requested, or the patient could be misdiagnosed with a psychiatric disorder (31). Misdiagnosis or delay in correct diagnosis reduces the caregiver's ability to understand the patient's symptoms and seek any supportive resources that could exist locally, further increasing the burden of care (39). Fortunately, some countries including Mexico, Costa Rica, Colombia, and Chile, have begun incorporating psychiatrists in their memory clinics, which is slowly increasing awareness of bvFTD in the field.
In terms of services for caregivers that could mitigate the burden, only a handful of specialized support groups for patients with bvFTD can be found and exist mainly in big cities in Brazil,1 Argentina,2 and Colombia.3 Most of these groups are focused on creating printed materials and informative sessions to support caregivers. The content of these sessions is mostly focused on decreasing the burden of care by offering techniques to manage difficult behavioral symptoms of patients. Unfortunately, there are still places like Nicaragua where, due to the lack of appropriate FTD diagnosis, the creation of services and resources has been stymied. Frequently, family caregivers who have already lost income to provide care, face the additional expense of hiring outside caregivers to further assist (21). In Uruguay, the government subsidizes costs for in-home care assistance for people with disabilities. However, in this system, the priority is given to people under 30 years of age and over 80 in a situation of severe dependency, and people over 65 in a situation of mild and moderate dependency so, it is not ideal for bvFTD where symptom onset occurs between those ages (40). Frequently, family caregivers who have already lost income to provide care, face the additional expense of hiring outside caregivers to further assist (21).
For many caregivers of patients with bvFTD, as the disease progresses, the burden becomes greater, and the social network becomes more limited. In this situation, institutionalization may be considered as the last resource (25). There are a limited number of long-term care institutions in Latin America. Governmental support is extremely limited and private markets are not regulated, allowing private facilities to charge more to care for people with behavioral symptoms. Most families willing to access these services would need to pay high out-of-pocket costs that are not possible for most middle- and low-income families (41, 42). Caregivers must also contend with the reluctance of patients with bvFTD to be institutionalized and a sense of guilt in the context of cultures that view institutionalization as a form of disrespect or betrayal (43). Since most of these institutions are designed to care for older patients, individuals with bvFTD may lack a sense of belonging. Frequently, patients with bvFTD end up in psychiatric institutions. Brazil and Chile, the countries with the highest number of psychiatric beds in public long-term care facilities, provide only 0.3 beds per 100,000 population and they are not exclusive or specifically equipped to care for patients with bvFTD (38).
Challenges for Caregivers of Patients With Other Forms of FTD
In contrast to bvFTD where caregiver burden is higher earlier in the course of the disease, in PPA and ALS, caregiver burden tends to increase over time (27). Semantic (sv) and non-fluent variants of PPA are typically characterized by language impairments when they affect the left side of the brain (44). Although not a Latin American example, a study conducted by Koyama et al. in Japan, compared the Zarit Burden Interview score from caregivers of participants mostly in mild stages of right svPPA, left svPPA, and bvFTD. Caregivers of participants with bvFTD reported the highest Zarit Burden Interview scores (0.002). No significant differences in ZBI scores were found in the right vs. left svPPA (p = 0.166). However, the effect size was large (d = 0.89) (45). These results aside, behavioral symptoms do emerge with disease progression and they can be somewhat unexpected for the caregivers. When behavioral symptoms emerge, caregivers might experience a greater sense of burden since they will no longer be caring for a family member with only a language difficulty (27). Individuals with right-sided predominant semantic variant PPA exhibit prosopagnosia and early behavioral changes similar to those seen in bvFTD, such as social awkwardness, job loss, loss of insight, and difficulty with personal identification (46). Their caregivers will experience similar challenges to those experienced by caregivers of patients with bvFTD. In the study conducted by Hsieh et al. in an Australian population, the authors showed an increase in behavioral symptoms and the Zarit Burden Interview score (p < 0.001) over a 3-year follow-up period in participants with svPPA compared to their caregivers of bvFTD participants counterparts whose Zarit Burden Interview score remained high throughout the follow-up (27).
As with bvFTD, caregivers of patients with PPA face difficulties in getting an early and accurate diagnosis. Aphasia might be incorrectly attributed to stroke or trauma, especially in rural settings where brain imaging is not available (12, 47). Importantly, the svPPA diagnostic criteria were developed for English speakers, and challenges with applying these criteria in patients who speak Portuguese, Spanish or indigenous languages can delay diagnosis (48, 49).
In Latin America, the family unit is the central part of society and an essential element of well-being and it is considered necessary to provide optimal care to the members who need it. Tight family bonds are built through communication between its members. Breakdowns in communication resulting from language deficits could lead to a loss of the sense of family and result in social isolation among caregivers and patients (50, 51). As the patient loses the ability to communicate, family roles need to change, especially in those circumstances in which the patient lost his or her job as a consequence of aphasia (51). This is especially important for very traditional Latin American families with very pre-determined gender roles in which spouses are not equipped with the skills to fulfill their partner's role. Fulfilling opposite gender roles might lead to frustration, stress, anxiety, and embarrassment that importantly increase caregiver burden (52). For Latin American indigenous families, language plays a critical role in sustaining the ancient culture. Oral tradition represents an important part of the inheritance from one generation to the next. Caregivers who are children of people with PPA are unable to receive that knowledge and can experience additional frustration and guilt for not being able to carry and transmit the heritage of their family line (53, 54).
Speech therapy can ameliorate the burden of the disease for patients while also providing indirect relief to caregivers. Brazil has made an important effort to increase the number of phonoaudiologists and language therapists and to raise awareness of PPA among this group. While speech rehabilitation services can be effective at addressing symptoms, they are limited in Latin America (55, 56). Other barriers to access include financial constraints, caregiver availability and transportation limitations. As improvements will be short-term in the context of a disease that will inevitably result in language deterioration, the costs for caregivers in participating in these programs may outweigh the benefits (57, 58). Notably, some online programs have emerged during the COVID-19 pandemic that may provide solutions for geographical issues (see text footnote 2, 3).
Patients with FTD-ALS experience the shortest mean and median survival of the FTD subtypes (59). Each patient displays a unique set of symptoms that come with the motor manifestations such as changes in behavior, personality, and language skills. As pointed out by Hsieh et al., caregivers of participants with FTD-ALS can experience a steeper caregiver burden increase compared to patients with svPPA and bvFTD over a 3-year follow up. High Zarit Burden Interview (p < 0.001) and Motor Neuron Disease Behavioral Scale (p < 0.001) scores at baseline showed to be the best predictors of caregiver burden over time (27). Aside from the challenge that their behavioral and language impairment may present for caregivers, these patients require significant physical help with basic activities of daily living as the disease progresses (60). Caregivers are often ill-equipped to offer the type of care required to cope with the patient's motor and respiratory impairments and since it is physically demanding work, it is less likely that people within the caregiver's social network will help them with caregiving duties (61, 62). Worsening of symptoms and physical concerns may lead to increased stress, anxiety, and depression for caregivers, diminishing energy for leisure activities and time to fulfill their own needs (60). Caregivers who experience feelings of depression may find it even more challenging to cope with the caregiving demands placed on them and can neglect the patients (30, 62).
All types of FTD will follow a progressive fatal trajectory. Medical, financial, and end-of-life decisions need to be considered by caregivers, particularly in FTD-ALS where the disease progresses most rapidly (27). From diagnosis, all patients with FTD should receive information about advance care planning and caregiver assistance with understanding and consideration of the patient's wishes (63). Unfortunately, the training of specialists in palliative care is still insufficient, even in developed countries (64). Lack of planning can bring avoidable distress to caregivers since the ethical and emotional responsibilities to make such complex decisions are great (e.g., artificial nutrition/hydration, antibiotics, etc.). This is particularly true for caregivers with low education, greater financial burden, and limited access to providers and support services (65). In Latin America, these decisions are usually made through family consensus, sometimes even involving the extended family or respected members of the community (66). The role of religion is important in Latin American societies, and caregivers might seek a religious leader to also support their decisions (67). The absence of the support network formed by family and sometimes religious leaders when these decisions need to be made in emergency contexts can leave important emotional sequelae in the caregivers (68). It is important to note that only six countries in Latin America (Argentina, Brazil, Colombia, Mexico, Panama, and Uruguay) have specific legislation regarding an advance directive document and the requirements to create one, therefore, the family's discussion of these topics early in the course of these diseases is fundamental to avoid adverse outcomes in the caregiver (67).
Next Steps in Supporting Caregiving for Patients With FTD in Latin America
Awareness of FTD in Latin America is scarce (7). Therefore, the first and most important point moving forward is to increase awareness of the disease at all levels, informing members of community-dwelling populations and healthcare providers alike. Generating awareness is fundamental to reducing stigma (69). Awareness should also be paired with the education of all sectors of the population to help caregivers to be informed about the disease (70). Table 1 highlights literature that included reportable outcomes following FTD caregiver interventions in different parts of the world. From this table we identified that caregivers of individuals with FTD benefitted from support groups, and education programs which addressed their specific needs with participants reporting improved knowledge and understanding of the disease, and valuing mutual support and sharing of coping strategies (73–77) The limitations for most of these interventions to be applied in Latin America is the lack of specialized providers, specialized resources and the inability to leverage technology that could include caregivers living in remote areas. On a large scale, two institutions, the Global Brain Health Institute4 as an international organization and the BrainLat Institute5 as a Latin American organization are taking some steps forward in training Latin American multidisciplinary professionals on FTD. The hope is to get a multi-directional effect in which they educate and raise awareness among other professionals, general population and policy makers and increase the creation of dementia resources in Latin America.
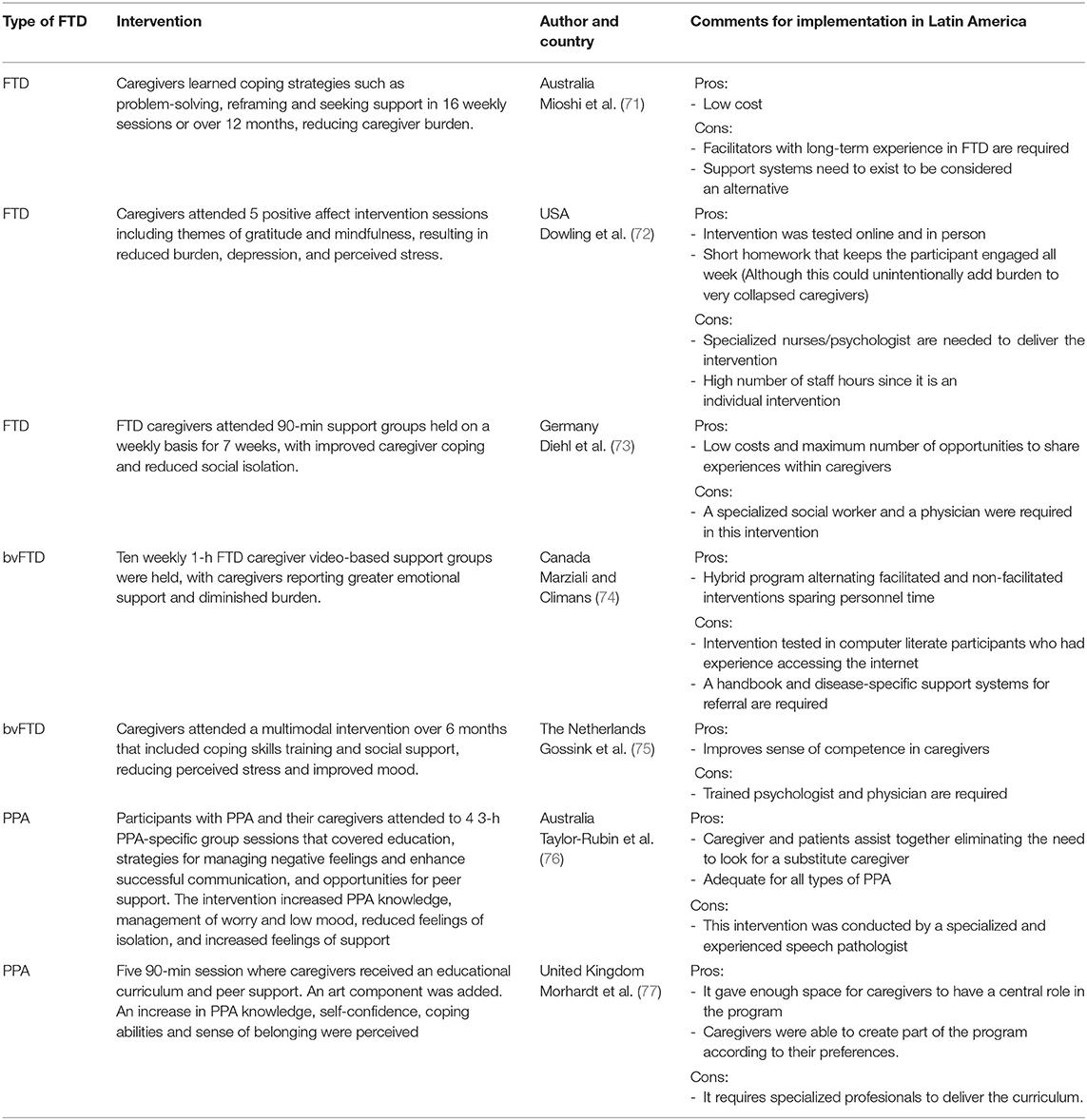
Table 1. Interventions for caregivers and implementation observations in Latin America.
Specialized caregiver support groups and psychoeducational programs need to be subsidized to be available on a larger scale for caregivers and their funding should contemplate providing technological resources and support to people in remote areas in order to increase access. In the United States, the Association for Frontotemporal Degeneration6 formed by healthcare providers and caregivers represents a model that provides caregivers support resources and educational materials. In Spain, the Frontotemporal Dementia Association7 is a similar model that also provides resources to caregivers. These examples could be adapted to local needs in Latin America if the appropriate resources existed. The Alzheimer's Associations and the local groups (see text footnote 1–3) have taken the lead in supporting caregivers of patients with FTD on a smaller scale. These Associations must join efforts with caregivers, healthcare providers, and policymakers from all Latin America to advance FTD care in Latin America.
It is important to highlight the scarcity of literature on the caregiving for FTD patients in Latin America. Researchers' associations like the International Society for Frontotemporal Dementias8 and the Latin America and the Caribbean Consortium on Dementia9 keep raising awareness on this gap among their members and promote increasing research on this topic. Since FTD diagnosis is low in the region at this moment, even small group caregiver intervention strategies like the ones being put in place in different places in Latin America (see text footnote 1–3) are valuable, can inform the literature and provide guidelines to health providers in the region.
Health policies and infrastructure are fundamental to provide support to caregivers of persons with FTD. Even when national dementia plans from Costa Rica (78), Argentina (79), Uruguay (80), Chile (81), Perú, and Mexico (82) include caregiver support for dementia patients, in reality, more services and infrastructure are needed to fulfill the needs of caregivers, particularly in rural areas. The Uruguayan model of caregiver support functions as a first example to inform the region how policies on this topic can be made, implemented and improved over time to provide social, economic, and legal support to caregivers. It also provides a telehealth model that can benefit the sector of the population that has access to internet services and can be used as proof that such services need to be widely available for caregivers (40). Healthcare diplomacy is fundamental to create joint efforts that push policies forward to protect caregivers of patients with FTD in which all the aforementioned organization can act as stakeholders.
Finally, we must consider that despite the many barriers to care patients with FTD face in Latin America, there are also strengths inherent to its cultures and traditions. For instance, there is more emphasis on aging in the community and within the family, where it may be easier to find solidarity and tolerance even if the disease is not well-understood. Leveraging this as an advantage, it is very likely that in future circumstances, once better education and infrastructure exist, new models of care will emerge. Blending the resourcefulness that exists within the region while implementing broad changes that benefit patients with FTD and their caregivers. The goals are that patients and caregivers get the tools they need to seek care in the early stages of the disease, primary care providers become able to identify the disease and make an early referral, and specialists become able to provide a timely diagnosis that will help patients and caregivers obtain appropriate resources and plan for the future including palliative care. Ideally, services with adequately trained personnel become available and help reduce the burden of care for caregivers and the society becomes more educated and tolerant with patients with FTD reducing the stress of caregivers in social interaction situations.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
SP-E conceived of the presented idea. All authors reviewed the existent literature, developed the idea, and contributed to the final manuscript.
Funding
This work was supported by the Multi-Partner Consortium to Expand Dementia Research in Latin America (ReDLat), supported by the National Institutes of Aging of the National Institutes of Health under award number R01AG057234, Alzheimer's Association Grant (SG-20-725707-ReDLat), the Rainwater Foundation, and the Global Brain Health Institute.
Disclaimer
The content is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health, Alzheimer's Association, Rainwater Charitable Foundation, or Global Brain Health Institute.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the members of the Multi-Partner Consortium to Expand Dementia Research in Latin America (ReDLat) and the Global Brain Health Institute for providing regional context for the construction of the manuscript.
Footnotes
2. ^https://www.ineco.org.ar/patologias/demencia-frontotemporal-dft/
3. ^https://www.fundacionudea.com/sitio/neurociencias/
4. ^www.ghi.og
References
1. Custodio N, Wheelock A, Thumala D, Slachevsky A. Dementia in Latin America: epidemiological evidence and implications for public policy. Front Aging Neurosci. (2017) 9:00221. doi: 10.3389/fnagi.2017.00221
2. Maestre G, Mena L, Pino-Ramirez G, Melgarejo J, Urribarri M, Pacheco C, et al. Incidence of dementia in the maracaibo aging study. Alzheimers Dement. (2011) 7:S356–7. doi: 10.1016/j.jalz.2011.05.1032
3. Nitrini R, Caramelli P, Herrera EJ, Bahia VS, Caixeta LF, Radanovic M, et al. Incidence of dementia in a community-dwelling Brazilian population. Alzheimer Dis Assoc Disord. (2004) 18:241–6.
4. Zurique Sánchez C, Cadena Sanabria MO, Zurique Sánchez M, Camacho López PA, Sánche Sanabriaz M, Hernández Hernández S, et al. Prevalencia de demencia en adultos mayores de América Latina: revisión sistemática. Rev Española Geriatr Gerontol. (2019) 54:346–55. doi: 10.1016/j.regg.2018.12.007
5. Nitrini R, Caramelli P, Herrera E, de Castro I, Bahia VS, et al. Mortality from dementia in a community-dwelling Brazilian population. Int J Geriatr Psychiatry. (2005) 20:247–53. doi: 10.1002/gps.1274
6. Olney NT, Spina S, Miller BL. Frontotemporal Dementia. Neurol Clin. (2017) 35:339. doi: 10.1016/j.ncl.2017.01.008
7. Custodio N, Herrera-Perez E, Lira D, Montesinos R, Bendezu L. Prevalence of frontotemporal dementia in community-based studies in Latin America: a systematic review. Dement Neuropsychol. (2013) 7:27–32. doi: 10.1590/S1980-57642013DN70100005
8. Onyike CU, Diehl-Schmid J. The epidemiology of frontotemporal dementia. Int Rev Psychiatry (Abingdon, England). (2013) 25:130–7. doi: 10.3109/09540261.2013.776523
9. Coyle-Gilchrist ITS, Dick KM, Patterson K, Vázquez Rodríquez P, Wehmann E, Wilcox A, et al. Prevalence, characteristics, and survival of frontotemporal lobar degeneration syndromes. Neurology. (2016) 86:1736–43. doi: 10.1212/WNL.0000000000002638
10. Knopman DS, Roberts RO. Estimating the number of persons with frontotemporal lobar degeneration in the US population. J Mol Neurosci : MN. (2011) 45:330–5. doi: 10.1007/s12031-011-9538-y
11. Bang J, Spina S, Miller B. Frontotemporal dementia. Lancet. (2015) 386:1672–82. doi: 10.1016/S0140-6736(15)00461-4
12. Gleichgerrcht E, Flichtentrei D, Manes F. How much do physicians in Latin America know about behavioral variant frontotemporal dementia? J Mol Neurosci. (2011) 45:609–17. doi: 10.1007/s12031-011-9556-9
13. Ibanez A, Flichtentrei D, Hesse E, Dottori M, Tomio A, Slachevsky A, et al. The power of knowledge about dementia in Latin America across health professionals working on aging. Alzheimers Demen (Amsterdam, Netherlands). (2020) 12:e12117. doi: 10.1002/dad2.12117
14. Baez S, Ibáñez A. Dementia in Latin America: an emergent silent tsunami. Front Aging Neurosci. (2016) 8:e00253. doi: 10.3389/fnagi.2016.00253
15. Brea JA. Population Dynamics in Latin America. Population Reference Bureau. (2003). Available online at: https://www.prb.org/populationdynamicsinlatinamericapdf318kbx/ (accessed May 20, 2021).
16. International Labor Organization. Panorama Laboral 2019. America Latina y El Caribe (pp. 1-152). Organización Internacional del Trabaajo/Oficina Regional para América Latina y el Caribe, 2019. (2019). p. 152. Available online at: https://www.ilo.org/wcmsp5/groups/public/—americas/—ro-lima/documents/publication/wcms_732198.pdf (accessed May 20, 2021).
17. Rojas G, Bartoloni L, Dillon C, Serrano CM, Iturry M, Allegri RF. Clinical and economic characteristics associated with direct costs of Alzheimer's, frontotemporal and vascular dementia in Argentina. Int Psychogeriatr. (2011) 23:554–61. doi: 10.1017/S1041610210002012
18. Gonzalez FJ, Gaona C, Quintero M, Chavez CA, Selga J, Maestre GE. Building capacity for dementia care in Latin America and the Caribbean. Demen Neuropsychol. (2014) 8:310–6. doi: 10.1590/S1980-57642014DN84000002
19. Gomez D, Power C, Gill MJ, Koenig N, Vega R, Fujiwara E. Empiric neurocognitive performance profile discovery and interpretation in HIV infection. J Neurovirol. (2019) 25:72–84. doi: 10.1007/s13365-018-0685-6
20. Galvin JE, Howard DH, Denny SS, Dickinson S, Tatton N. The social and economic burden of frontotemporal degeneration. Neurology. (2017) 89:2049–56. doi: 10.1212/WNL.0000000000004614
21. Prince M, 10/66 Dementia Research Group. Care arrangements for people with dementia in developing countries. Int J Geriatr Psychiatry. (2004) 19:170–7. doi: 10.1002/gps.1046
22. Lloyd-Sherlock P, Mayston R, Acosta A, Gallardo S, Guerra M, Sosa AL, et al. Allocating family responsibilities for dependent older people in Mexico and Peru. J Dev Stud. (2018) 54:682–701. doi: 10.1080/00220388.2017.1308489
23. Slachevsky A, Budinich M, Miranda-Castillo C, Núñez-Huasaf J, Silva JR, Muñoz-Neira C, et al. The CUIDEME Study: determinants of burden in chilean primary caregivers of patients with dementia. J Alzheimers Dis. (2013) 35:297–306. doi: 10.3233/JAD-122086
24. Parkman S. Role captivity: a concept of constraining dimensions in dementia care. Nurs Forum. (2020) 55:128–35. doi: 10.1111/nuf.12406
25. Neary SR, Mahoney DF. Dementia caregiving: the experiences of Hispanic/Latino caregivers. J Transcult Nurs. (2005) 16:163–70. doi: 10.1177/1043659604273547
26. Ramos C, Aguillon D, Cordano C, Lopera F. Genetics of dementia: insights from Latin America. Demen Neuropsychol. (2020) 14:223–36. doi: 10.1590/1980-57642020dn14-030004
27. Hsieh S, Leyton CE, Caga J, Flanagan E, Kaizik C, O'Connor CM, et al. The evolution of caregiver burden in frontotemporal dementia with and without amyotrophic lateral sclerosis. J Alzheimers Dis. (2016) 49:875–85. doi: 10.3233/JAD-150475
28. Harris JM, Gall C, Thompson JC, Richardson AMT, Neary D, du Plessis D, et al. Sensitivity and specificity of FTDC criteria for behavioral variant frontotemporal dementia. Neurology. (2013) 80:1881–7. doi: 10.1212/WNL.0b013e318292a342
29. Lima-Silva TB, Bahia VS, Carvalho VA, Guimarães HC, Caramelli P, Balthazar ML, et al. Neuropsychiatric symptoms, caregiver burden and distress in behavioral-variant frontotemporal dementia and Alzheimer's disease. Demen Geriatr Cogn Disord. (2015) 40:268–75. doi: 10.1159/000437351
30. Piña-Escudero SD, Weinstein CA, Ritchie C. Contextualizing mistreatment in cognitive impairment in Latin America. J Elder Abuse Neglect. (2019) 31:255–61. doi: 10.1080/08946566.2019.1584070
31. Rasmussen H, Hellzen O, Stordal E, Enmarker I. Family caregivers experiences of the pre-diagnostic stage in frontotemporal dementia. Geriatr Nurs (New York, NY). (2019) 40:246–51. doi: 10.1016/j.gerinurse.2018.10.006
32. Galanti G-A. The hispanic family and male-female relationships: an overview. J Transcult Nurs. (2003) 14:180–5. doi: 10.1177/1043659603014003004
33. Rascovsky K, Matallana DL. Frontotemporal dementia. In: International Neurology. Hoboken, NJ: John Wiley and Sons, Ltd. (2016). p. 153–6.
34. Bott S, Guedes A, Goodwin M, Mendoza JA. Violence Against Women in Latin America and the Caribbean: A Comparative Analysis of Population-Based Data from 12 Countries. Panamerican Health Organization. Washington, DC: Centers for Disease Control and Prevention of the United States (2014).
35. González-Cosio M. Sexuality and Dementia. Instituto Nacional de Geriatría and Asociación Mexicana de Alzheimer y Enfermedades Similares (2017). Available online at: http://www.geriatria.salud.gob.mx/descargas/publicaciones/sexualidad-y-demencia.pdf (accessed May 20, 2021).
36. Kovaleva M, Spangler S, Clevenger C, Hepburn K. Chronic stress, social isolation, and perceived loneliness in dementia caregivers. J Psychosoc Nurs Mental Health Serv. (2018) 56:36–43. doi: 10.3928/02793695-20180329-04
37. Lanata SC, Miller BL. The behavioural variant frontotemporal dementia (bvFTD) syndrome in psychiatry. J Neurol Neurosurg Psychiatry. (2016) 87:501–11. doi: 10.1136/jnnp-2015-310697
38. Panamerican Health Organization. WHO-AIMS Regional Report on Mental Health Systems in Latin America and the Caribbean. PAHO (2013). Available online at: https://www.paho.org/hq/dmdocuments/2013/ENG-WHOAIMSREG-(For-Web-Apr-2013).pdf (accessed May 20, 2021).
39. Merrilees J, Ketelle R. Advanced practice nursing: meeting the caregiving challenges for families of persons with frontotemporal dementia. Clin Nurse Spec. (2010) 24:245–51. doi: 10.1097/NUR.0b013e3181ecdc32
40. Aranco N, Sorio R. Envejecimiento y atención a la dependencia en Uruguay | Publications (IDB - TN - 1615, pp. 1-66) [Technical Report]. Interamerican Developmental Bank (2019). Available online at: https://publications.iadb.org/publications/spanish/document/Envejecimiento_y_atenci%C3%B3n_a_la_dependencia_en_Uruguay_es.pdf (accessed May 20, 2021).
41. Caruso Bloeck M, Galiani S, Ibarrarán P. Long-Term Care in Latin America and the Caribbean?: Theory and Policy Considerations | Publications (IDB WORKING PAPER IDB-WP-834). Inter-American Development Bank (2017). Available online at: https://publications.iadb.org/publications/english/document/Long-Term-Care-in-Latin-America-and-the-Caribbean-Theory-and-Policy-Considerations.pdf (accessed May 20, 2021).
42. Ibáñez A, Pina-Escudero SD, Possin KL, Quiroz YT, Peres FA, Slachevsky A, et al. Dementia caregiving across Latin America and the Caribbean and brain health diplomacy. Lancet Healthy Longevity. (2021) 2:e222–31. doi: 10.1016/S2666-7568(21)00031-3
43. Arias EM, Herrera BS, González GMC. Apoyo al cuidador familiar en el proceso de institucionalizar a un ser querido con demencia. Rev Cubana de Enferm (2015) 31. http://www.revenfermeria.sld.cu/index.php/enf/article/view/544
44. Gorno-Tempini ML, Hillis AE, Weintraub S, Kertesz A, Mendez M, Cappa SF, et al. Classification of primary progressive aphasia and its variants. Neurology. (2011) 76:1006–14. doi: 10.1212/WNL.0b013e31821103e6
45. Koyama A, Hashimoto M, Fukuhara R, Ichimi N, Takasaki A, Matsushita M, et al. Caregiver burden in semantic dementia with right- and left-sided predominant cerebral atrophy and in behavioral-variant frontotemporal dementia. Demen Geriatr Cogn Disord Extra. (2018) 8:128–37. doi: 10.1159/000487851
46. Thompson SA, Patterson K, Hodges JR. Left/right asymmetry of atrophy in semantic dementia: behavioral-cognitive implications. Neurology. (2003) 61:1196–203. doi: 10.1212/01.WNL.0000091868.28557.B8
47. Khayum B, Wieneke C, Rogalski E, Robinson J, O'Hara M. Thinking outside the stroke: treating primary progressive aphasia (PPA). Perspect Gerontol. (2012) 17:37–49. doi: 10.1044/gero17.2.37
48. Wilson MA, Martínez-Cuitiño M. Semantic dementia without surface dyslexia in Spanish: unimpaired reading with impaired semantics. Behav Neurol. (2012) 25:273–84. doi: 10.1155/2012/258685
49. Defior S, Martos F, Cary L. Differences in reading acquisition development in two shallow orthographies: Portuguese and Spanish. Appl Psycholinguist. (2002) 23:135–48. doi: 10.1017/S0142716402000073
50. Tatsumi H, Nakaaki S, Satoh M, Yamamoto M, Chino N, Hadano K. Relationships among communication self-efficacy, communication burden, and the mental health of the families of persons with aphasia. J Stroke Cerebrovasc Dis. (2016) 25:197–205. doi: 10.1016/j.jstrokecerebrovasdis.2015.09.018
51. Jacquet-Andrieu A. The aphasic patient: vulnerability and/or exclusion. Cult Med Psychiatry. (2014) 38:60–76. doi: 10.1007/s11013-014-9363-1
52. Saldívar Garduño A, Díaz Loving R, Reyes Ruiz NE, Armenta Hurtarte C, López Rosales F, Moreno López M, et al. Roles de Género y Diversidad: validación de una Escala en Varios Contextos Culturales1. Acta de Investigación Psicológica. (2015) 5:2124–47. doi: 10.1016/S2007-4719(16)30005-9
53. Ramirez Poloche N. La importancia de la tradición oral: El grupo Coyaima-Colombia. Revista Científica Guillermo de Ockham. (2012) 10:129–43.
54. Riascos J. Ancient and indigenous stories: their ethics and power reflected in Latin American storytelling movements. Marvels Tales. (2007) 21:253–267. doi: 10.1353/mat.0.0031
55. Sousa M, de FS, de Nascimento CMB, do Sousa F, de OS, Lima MLLLT, et al. Evolution of speech-language pathologists supply in Unified Health System (SUS) and in primary healthcare in Brazil. Revista CEFAC. (2017) 19:213–20. doi: 10.1590/1982-0216201719215816
56. Beber BC, Brandão L, Chaves MLF, Beber BC, Brandão L, Chaves MLF. Alerta à comunidade fonoaudiológica brasileira sobre a importância da atuação científica e clínica na afasia progressiva primária. CoDAS. (2015) 27:505–8. doi: 10.1590/2317-1782/20152015081
57. Henry ML, Hubbard HI, Grasso SM, Mandelli ML, Wilson SM, Sathishkumar MT, et al. Retraining speech production and fluency in non-fluent/agrammatic primary progressive aphasia. Brain. (2018) 141:1799–814. doi: 10.1093/brain/awy101
58. Dorze GL, Signori F-H. Needs, barriers and facilitators experienced by spouses of people with aphasia. Disabil Rehabil. (2010) 32:1073–87. doi: 10.3109/09638280903374121
59. Kansal K, Mareddy M, Sloane KL, Minc AA, Rabins PV, McGready JB, et al. Survival in frontotemporal dementia phenotypes: a meta-analysis. Demen Geriatr Cogn Disord. (2016) 41:109–22. doi: 10.1159/000443205
60. Chiò A, Gauthier A, Vignola A, Calvo A, Ghiglione P, Cavallo E, et al. Caregiver time use in ALS. Neurology. (2006) 67:902–4. doi: 10.1212/01.wnl.0000233840.41688.df
61. Weisser FB, Bristowe K, Jackson D. Experiences of burden, needs, rewards and resilience in family caregivers of people living with Motor Neurone Disease/Amyotrophic Lateral Sclerosis: A secondary thematic analysis of qualitative interviews. Palliat Med. (2015) 29:737–45. doi: 10.1177/0269216315575851
62. de Wit J, Bakker LA, van Groenestijn AC, van den Berg LH, Schröder CD, Visser-Meily JM, et al. Caregiver burden in amyotrophic lateral sclerosis: a systematic review. Palliat Med. (2018) 32:231–45. doi: 10.1177/0269216317709965
63. Boersma I, Miyasaki J, Kutner J, Kluger B. Palliative care and neurology. Neurology. (2014) 83:561–7. doi: 10.1212/WNL.0000000000000674
64. Creutzfeldt CJ, Gooley T, Walker M. Are neurology residents prepared to deal with dying patients? Arch Neurol. (2009) 66:1427–8. doi: 10.1001/archneurol.2009.241
65. Xie B, Berkley AS, Kwak J, Fleischmann KR, Champion JD, Koltai KS. End-of-life decision making by family caregivers of persons with advanced dementia: a literature review of decision aids. SAGE Open Med. (2018) 6:205031211877751. doi: 10.1177/2050312118777517
66. Born W, Greiner KA, Sylvia E, Butler J, Ahluwalia JS. Knowledge, attitudes, and beliefs about end-of-life care among inner-city African Americans and Latinos. J Palliat Med. (2004) 7:247–56. doi: 10.1089/109662104773709369
67. Soto-Perez-de-Celis E, Chavarri-Guerra Y, Pastrana T, Ruiz-Mendoza R, Bukowski A, Goss PE. End-of-life care in Latin America. J Global Oncol. (2016) 3:261–70. doi: 10.1200/JGO.2016.005579
68. Braun UK, Beyth RJ, Ford ME, McCullough LB. Voices of African American, Caucasian, and Hispanic surrogates on the burdens of end-of-life decision making. J Gen Intern Med. (2008) 23:267–74. doi: 10.1007/s11606-007-0487-7
69. Fletcher JR. Destigmatising dementia: the dangers of felt stigma and benevolent othering. Dementia. (2019) 20:1471301219884821. doi: 10.1177/1471301219884821
70. Kim S, Werner P, Richardson A, Anstey KJ. Dementia Stigma Reduction (DESeRvE): Study Protocol for a Randomized Controlled Trial of an Online Intervention Program to Reduce Dementia-Related Public Stigma. Contemporary Clinical Trials Communications, 14 (Kim S.,c2FyYW5nLmtpbUB1dGFzLmVkdS5hdQ==) Centre for Research on Ageing, HealthandWellbeing, Research School of Population Health, Australian National University, Canberra, Australia). Embase. (2019).
,+sarang.kim@utas.edu.au)+Centre+for+Research+on+Ageing,+HealthandWellbeing,+Research+School+of+Population+Health,+Australian+National+University,+Canberra,+Australia)" target="_blank">Google Scholar
71. Mioshi E, McKinnon C, Savage S, O'Connor CM, Hodges JR. Improving burden and coping skills in frontotemporal dementia caregivers: a pilot study. Alzheimer Dis Assoc Disord. (2013) 27:84–6. doi: 10.1097/WAD.0b013e31824a7f5b (accessed May 20, 2021).
72. Dowling GA, Merrilees J, Mastick J, Chang VY, Hubbard E, Moskowitz JT. Life enhancing activities for family caregivers of people with frontotemporal dementia. Alzheimer Dis Assoc Disord. (2014) 28:175–81. doi: 10.1097/WAD.0b013e3182a6b905
73. Diehl J, Mayer T, Förstl H, Kurz A. A Support Group for caregivers of patients with frontotemporal dementia. Dementia. (2003) 2:151–61. doi: 10.1177/1471301203002002002
74. Marziali E, Climans R. New technology to connect frontotemporal dementia spousal caregivers online. Can Rev Alzheimers Dis Other Demen. (2009) 12:23–6.
75. Gossink F, Pijnenburg Y, Scheltens P, Pera A, Kleverwal R, Korten N, et al. An intervention programme for caregivers of dementia patients with frontal behavioural changes: an explorative study with controlled effect on sense of competence. Psychogeriatrics. (2018) 18:451–9. doi: 10.1111/psyg.12351
76. Taylor-Rubin C, Azizi L, Croot K, Nickels L. Primary progressive aphasia education and support groups: a clinical evaluation. Am J Alzheimers Dis Other Demen. (2020) 35:1533317519895638. doi: 10.1177/1533317519895638
77. Morhardt DJ, O'Hara MC, Zachrich K, Wieneke C, Rogalski EJ. Development of a psycho-educational support program for individuals with primary progressive aphasia and their care-partners. Dementia (London, England). (2019) 18:1310–27. doi: 10.1177/1471301217699675
78. Román Garita N. Plan Nacional para la Enfermedad de Alzheimer y Demencias Relacionadas Esfuerzos Compartidos 2014-2024. Presidencia de La República de Costa Rica, ASCADA, AIA, COMCAEDA, ADI (2014). Available online at: https://www.conapam.go.cr/mantenimiento/Plan%20Nacional%20Alzheimer.pdf (accessed May 20, 2021).
79. Manes F, Zamora R, Bustin J, Triskier F, Abudulhamid P, Aguirre F, et al. Plan Estratégico Nacional PAMI para un cerebro saludable, enfermedad de Alzheimer y otras demencias. Programa de Atención Médica Integral (2016). Available online at: https://www.ceafa.es/files/2017/05/ARGENTINA.pdf (accessed May 20, 2021).
80. Acosta L, Alberti R, Acosta MG. (2016). Plan Nacional de Demencias Para Larepública Oriental del Uruguay. Asociación Uruguaya de Alzheimer y Similares. p. 1–25. Available online at: https://www.audas.org.uy/06_Informacion/AUDAS_Plan_Nacional_Demencias-Presentacion_Publica.pdf (accessed May 20, 2021).
81. Abusleme Lama MT, Arenas Massa Á, Budinich Villouta M, Gajardo Jauregui J, Gálvez Pérez MJ, Larrain Salas A, et al. Plan Nacional de Demencia. Ministerio de Salud, Gobierno de Chile (2017). Available online at: https://www.minsal.cl/wp-content/uploads/2017/11/PLAN-DE-DEMENCIA.pdf (accessed May 20, 2021).
82. Gutierrez Robledo LM, Arrieta Cruz I, Ávila Fermatt F, Corona Vazquez T, Sosa Ortiz AL, Trujillo de los Santos Z, et al. Plan de Acción Alzheimer y otras demencias, México 2014 (pp. 7-71). Instituto Nacional de Geriatría (2014). Available online at: https://bpo.sep.gob.mx/#/recurso/3456/document/1 (accessed May 20, 2021).
Keywords: caregivers, frontotemporal dementia, Latin America, caregiver burden, dementia
Citation: Piña-Escudero SD, Aguirre GA, Javandel S and Longoria-Ibarrola EM (2021) Caregiving for Patients With Frontotemporal Dementia in Latin America. Front. Neurol. 12:665694. doi: 10.3389/fneur.2021.665694
Received: 08 February 2021; Accepted: 24 May 2021;
Published: 07 July 2021.
Edited by:
Andrea Slachevsky, University of Chile, ChileReviewed by:
Akitoshi Takeda, Osaka City University, JapanGang Wang, Shanghai Jiao Tong University, China
Copyright © 2021 Piña-Escudero, Aguirre, Javandel and Longoria-Ibarrola. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: PStefanie Danielle Piña-Escudero, c3RlZmFuaWUucGluYS1lc2N1ZGVyb0BnYmhpLm9yZw==