
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol., 23 March 2021
Sec. Neurorehabilitation
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.638904
 Auwal Abdullahi1,2*
Auwal Abdullahi1,2* Steven Truijen2Naima A. Umar3
Steven Truijen2Naima A. Umar3 Ushotanefe Useh4Victor A. Egwuonwu5
Ushotanefe Useh4Victor A. Egwuonwu5 Tamaya Van Criekinge2Wim Saeys2
Tamaya Van Criekinge2Wim Saeys2Background: Constraint induced movement therapy (CIMT) is effective at improving upper limb outcomes after stroke.
Aim: The aim of this study was to carry out a systematic review and meta-analysis of the effects of lower limb CIMT studies of any design in people with stroke.
Materials/ Method: PubMED, PEDro, OTSeeker, CENTRAL, and Web of Science were searched from their earliest dates to February 2021. Lower limbs CIMT studies that measured outcomes at baseline and post-intervention were selected. Sample size, mean, and standard deviation on the outcomes of interest and the protocols of both the experimental and control groups were extracted. McMaster Critical Review Form was used to assess the methodological quality of the studies.
Result: Sixteen studies with different designs were included in this review. The result showed that lower limb CIMT improves functional, physiological and person's reported outcomes including motor function, balance, mobility, gait speed, oxygen uptake, exertion before and after commencement of activities, knee extensor spasticity, weight bearing, lower limb kinematics and quality of life in people with stroke post intervention. However, there were only significant differences in quality of life in favor of CIMT post-intervention [mean difference (MD) = 16.20, 95% CI = 3.30–29.10, p = 0.01]; and at follow-up [mean difference (MD) = 14.10, 95% CI = 2.07–26.13, p = 0.02] between CIMT and the control group. Even for the quality of life, there was significant heterogeneity in the studies post intervention (I2 = 84%, p = 0.01).
Conclusion: Lower limb CIMT improves motor function, balance, functional mobility, gait speed, oxygen uptake, weigh bearing, lower limb kinematics, and quality of life. However, it is only superior to the control at improving quality of life after stroke based on the current literature.
Constraint Induced Movement Therapy (CIMT) is a translational motor rehabilitation technique following injury of the Central Nervous System (CNS). The technique originated many decades ago from use in primates; and was translated to humans following stroke and other neurological conditions (1). The original concept involved constraint of the unaffected limb and forced use of the affected one (2). Subsequent studies in humans involved voluntary massed tasks or shaping practices with the affected limb. Consequently, CIMT has been reported to be effective at improving real world arm use, motor function, and kinematic outcomes by inducing changes in the functions and structures of the brain (3–7). However, there have been many modifications over the years of the original protocol of CIMT, including but not limited to the length of time for the tasks practice, the constraint, and the use of a transfer package (7–9).
The effects of CIMT on the recovery of motor function of the upper limb have been well-investigated (7, 10). The practicability of the protocol for upper limbs could be because of the unilateral nature of the use of these limbs in most of our activities of daily living (ADL). For the lower limbs, this may seem difficult since humans are bipedal, and this requires them to use the two limbs simultaneously for ADL especially during walking. However, the positive results in the recovery of motor function of the upper limb following CIMT persuaded the neuroscientific community to consider translating the technique to the lower limbs. Consequently, a lower limb CIMT protocol was designed to comprise mainly of intensive practice with the affected limb, shaping activities, transfer package, and encouraging the increased use of the affected limb (11). So far, there are several small sample size studies that have investigated the effects of lower limb CIMT on gait parameters, balance, and motor function using different study designs such as case reports, experimental studies, quasi-experimental studies, and randomized controlled trials (RCTs) (12). These studies reported that lower limbs CIMT improved gait speed, step length, motor function, functional mobility, balance, and kinematic outcomes. However, small sample size studies may overestimate the effect of an intervention (13–15). Second, the only difference in the protocols of the CIMT and control groups was the use of a constraint in the CIMT group, with no difference in the types of tasks used in most of these studies, including the intensity. According to Abdullahi, task practice is the most important component of CIMT (16, 17). Therefore, it is possible that the effects of lower limb CIMT reported in those studies were overestimated.
In addition, in upper limb CIMT constraint is used to immobilize the unaffected limb to prevent movement at joints essential for the functioning of the limb. This is to done to maximize the use of the affected limb, and to help recover function. However, for lower limb CIMT, the types of constraints used include encouraging weight bearing on the affected limb, the use of an insole in the affected limb, the use of knee braces or a splint, and attaching weight to the ankle of the affected limb (12). Constraining one of the limbs may cause asymmetry which could negatively affect normal functions such as walking, especially since humans are bipedal. The aim of this study was to therefore carry out a systematic review and meta-analysis on the effects of lower limb CIMT on outcomes after stroke such as gait parameters, balance, motor function, functional mobility, and quality of life. This review sought to answer this question: What are the effects of lower limb CIMT on this information is important as, to date, there does not seem to be any review and/ or meta-analysis on the effects of lower limb CIMT following stroke.
The systematic review and meta-analysis were registered with PROSPERO (CRD42017083886).
A systematic literature search was carried out in PubMED, PEDro, OT Seeker, CENTRAL, and Web of Science from their earliest dates to February 2021. Similarly, the reference lists of the included studies and a review article were also manually searched for relevant studies. The search terms used were; constraint induced movement therapy, constraint induced therapy, forced use, stroke and lower limbs. The search terms were combined using appropriate Boolean operators such as AND and/or OR where appropriate. The search was also limited to studies published in English only, and those that were carried out in humans. The search was carried out by AA and TVC independently; TVC also removed duplicate studies using Endnote software. The search strategy is available in Appendix 1. Studies of any type of design that included stroke patients who were ≥18 years of age with motor impairment of the lower limbs, and assessed outcomes such as motor function, walking speed, and balance were included in the review. For RCT designs, the studies were included if they compared CIMT with any control interventions. Details of the inclusion and exclusion criteria for the eligibility of the studies are summarized in Table 1.
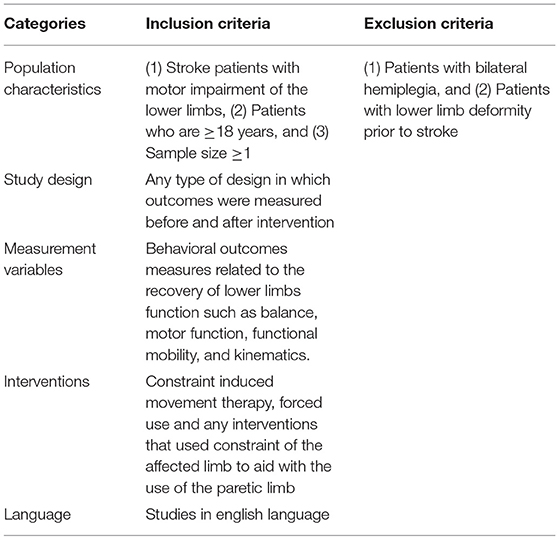
Table 1. Inclusion and exclusion criteria.
The study selection was carried out by AA and NAU independently using Rayyan software (18). At first, the abstracts and titles of the studies were assessed, and in the absence of sufficient information to either include or exclude a study, full texts of the articles were read. Disputes on whether to include or exclude studies were resolved through consensus discussions between AA and NUM or through consulting another author (VAE). Data extraction was carried out by AA and the data included were study designs, sample size, stage of stroke, participants' mean age, interventions for both experimental and control groups, including intensity and duration, and outcomes assessed (mean scores and standard deviation).
Methodological quality of the included studies was assessed using the Modified McMaster Critical Review Form for Quantitative Studies (19, 20). This form is used to assess: (1) whether the purpose of the study was clearly stated, (2) whether the relevant literature was reviewed, (3) the extent to which the sample of the study was described, (4) whether the sample size in the study was justified, (5) randomization, (6) whether the procedure for the randomization was appropriate, (7) how reliable the method used to establish diagnosis of the condition is, (8) how valid the outcome measures used are, (9) how reliable the outcome measures used are, (10) whether the intervention used was described in detail, (11) avoidance of contamination, (12) whether co-intervention was avoided, (13) whether statistical significance was reported, (14) whether the method of analysis used was appropriate, (15) whether clinical significance or importance was reported, (16) whether drop-outs were reported, and (17) whether the conclusion was drawn appropriately in accordance with the study methods and results. The scores for each item ranges from zero to one. A score of zero is awarded when the answer to the question is no or is not addressed; whereas a score of one is awarded when the answer to the question is yes. However, when a question is not applicable to a particular design such as studies that are not RCTs, the answer is indicated as not applicable (NA). In addition, the Cochrane risk of bias table was used to further assess the risk of bias of the included RCTs, and the results of this are presented in a risk of bias graph. The assessment was carried out by two of the authors (AA & NAU) and any disputes were resolved through discussions and contacting a third reviewer (VAE). The level of evidence of the included studies was determined using the National Health and Medical Research Council's (NHMRC) evidence hierarchy (21).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) was used to report the results of this systematic review and meta-analysis. RevMan (version 5.3) was used to create the PRISMA flow chart of the study and the graph for the risk of bias of the included RCTs. In addition, the mean and standard deviation of the scores on the outcomes of interest post intervention and at follow up; and the study sample size (for both the experimental and the control groups) were pooled using RevMan (version 5.3). When studies used the same outcome measures, the data was analyzed using fixed effect model. However, when studies used different outcome measures, the data was analyzed using the random effect model. Heterogeneity between studies was considered substantial only when I2 (which measures whether the percentage of variation across studies is caused by heterogeneity rather than chance) value is ≥50%. Furthermore, a level of significance, p < 0.05 was considered to be significant. For interpretation of the findings and their implication for clinical practice, the NHMRC form methodology was used (21).
A total of 16 studies were included in the study (22–37). The search of the databases and the reference list of the relevant studies yielded 1,023 hits in which 17 hits were provided from the reference list of the relevant studies. Subsequently, full texts of 46 articles were read and 30 articles were excluded for not fulfilling the study inclusion criteria. See Figure 1 for the study flowchart.
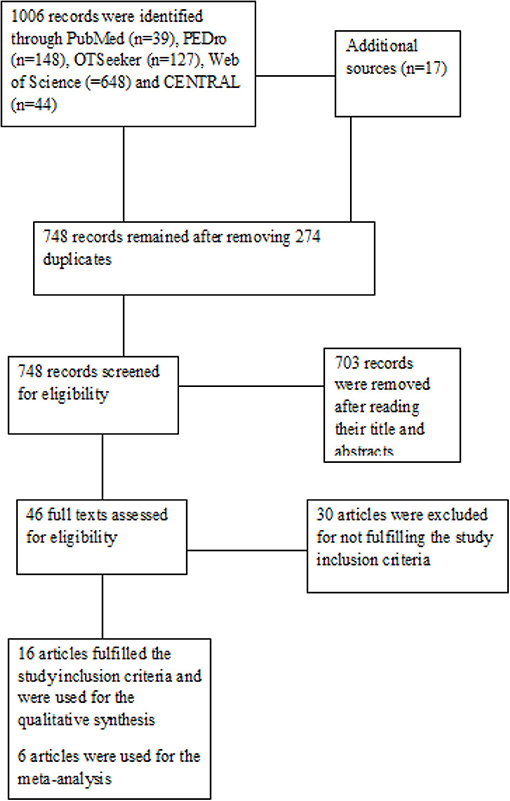
Figure 1. The Study flowchart.
The total number of participants in the included studies was 304, out of which 169 and 135 were men and women, respectively. The range for the sample size in the studies was between one and 58 participants. However, only four studies reported how the sample size was calculated (22–24, 37). The studies were published between 2005 and 2021. Out of the 16 included studies, 10 are RCTs (22, 24–31, 37), and two studies each are either single subject experimental AB designs (32, 33); pre-test- post-test experimental designs (23, 34); and case reports (35, 36), respectively.
Eight studies included chronic stroke patients (23, 24, 26, 31–34, 36). Three studies included subacute stroke patients (25, 29, 35). Two studies included subacute and chronic stroke patients (22, 28). Three studies included acute, subacute, and chronic stroke patients (27, 30, 37). Overall, the range of time since the stroke was 1 week to 6 years. Eleven out of the 16 studies included participants who could independently walk several meters or more (23, 25–28, 30, 32–34, 36, 37). One study included participants who could rise from a chair without using the arm or stand independently (24). Four studies included participants who were within Brunnstrom stages of recovery, 3 to 4 (22, 28, 29, 36).
In addition, 12 studies included participants with no significant cognitive impairment (22, 24, 26–32, 34, 36, 37). One study included participants who had significant walking speed deficits of ≤0.8 m/s (30). Only 11 studies provided information on the types of stroke the participants suffered, 176 ischaemic and 44 haemorrhagic (22, 23, 25, 27, 28, 30, 31, 34–37). Eight studies used participants with ischaemic and haemorrhagic stroke (22, 23, 27, 28, 30, 31, 34, 37). Two studies used participants with only ischaemic stroke (25, 35). This information is important since the type of stroke may provide information on the prognosis (38). Furthermore, most of the studies excluded participants who had serious medical conditions such as unstable hypertension, musculoskeletal deformities, and cardiopulmonary conditions that could hinder participation in the studies.
The studies used different forms of task practice and constraints in the intervention. For the constraint, one study used a weight attached to the participants' ankles (30). Four studies emphasized that participants bear weight on the affected limb during training (23, 24, 27, 34). Two studies used shoe insoles (26, 28). Three studies used knee braces or a splint (25, 31, 35). Two studies used whole leg orthosis (32, 33). One study used whole leg orthosis and a shoe insert (22). One study asked participants not to make use of the unaffected during training as much as possible (37). However, in one study, no constraint was used (36). For the affected side, only one study with 38 participants did not provide information on the affected side (30). Therefore, excluding this study, 143 and 123 participants had right and left sided hemiplegia, respectively. The affected side is an important prognostic indicator after stroke (39). In addition, some of the outcome measures used in the studies include electromyography for muscle activity (motor function), lower limb Fugl-Meyer for motor function, lower extremity motor activity log (LE-MAL) for real world use of the lower limb, Berg balance scale (BBS) for balance, the stroke specific quality of life questionnaire (SSQOL), and the stroke impact scale (SIS) for quality of life, the 10 m walk test (10MWT) for walking speed, the 6 min walk test (6MWT) for walking endurance, the motion analysis system for gait analysis, the timed up and go test (TUG) and Rivermead mobility index (RMI) for functional mobility, and the hard activity chart for exertion. Motor function is the ability to have voluntary control of movement patterns (40). Functional mobility ‘is a person's physiological ability to move independently and safely in a variety of environments to accomplish functional activities or tasks and to participate in the activities of daily living, at home, work and in the community’ (41). See Table 2 for the details of the characteristics of the included studies.
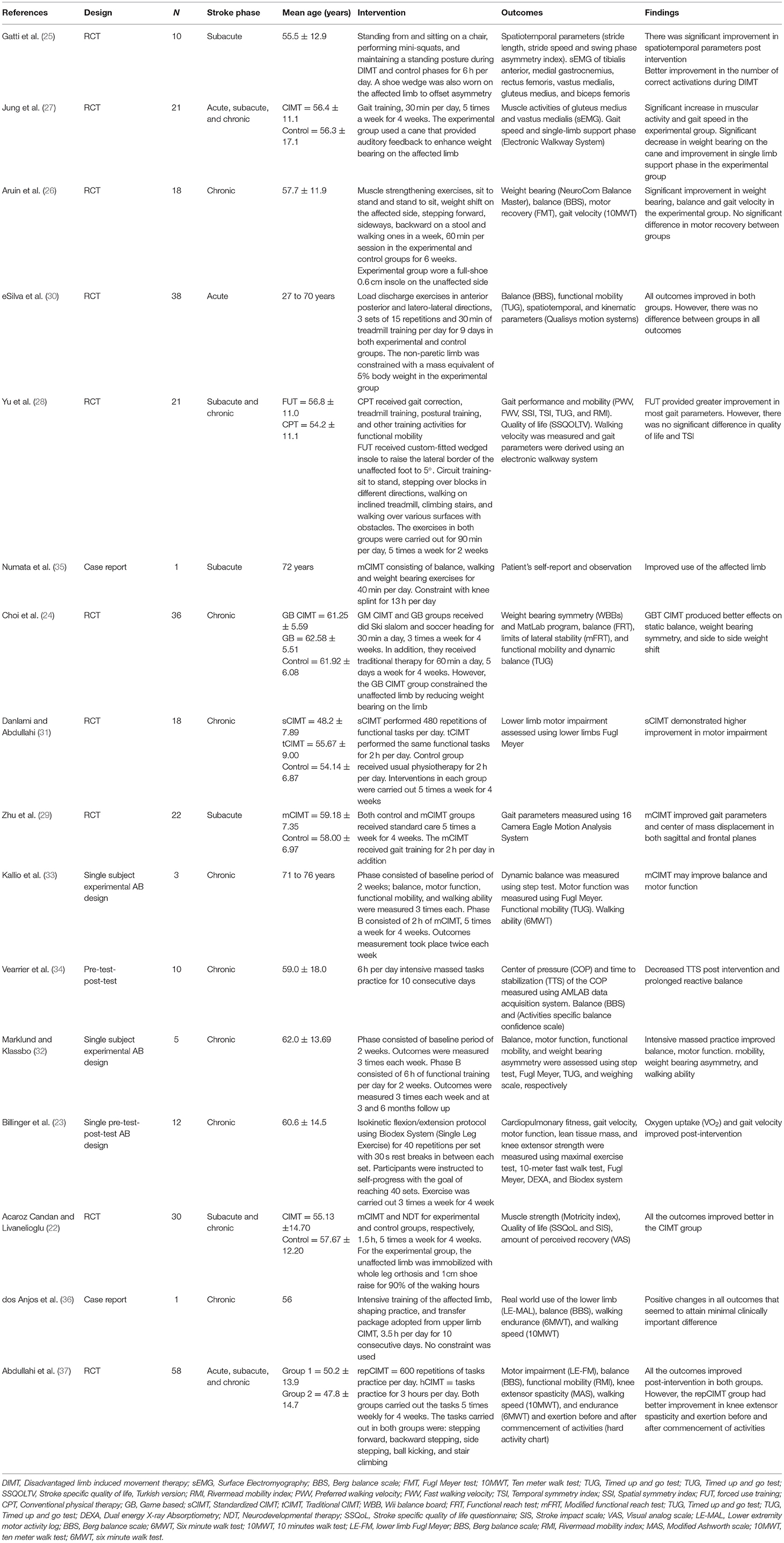
Table 2. Characteristics of the studies.
A total of six RCTs were included in the meta-analysis (22, 24, 26, 28, 30). One study has one experimental and two control groups (24). Four RCTs were excluded from the meta-analysis (25, 29, 31, 37). Two of the RCTs were excluded because they did not provide sufficient information to enable a meta-analysis (25, 29); while the remaining two were excluded because they compared two different modes of CIMT with one as a control to the other (31, 37).
For motor function, there was no significant difference between CIMT and the control [standardized mean difference (SMD) = 0.34, 95% CI = −0.30–0.97, p = 0.30]. In addition, there was no significant heterogeneity in the studies (I2 = 0%, p = 0.89). See Figure 2 for the forest plot.

Figure 2. Motor function post-intervention.
For balance post intervention and at follow-up, there was no significant difference between CIMT and the control (SMD = 0.62, 95% CI = −0.54–1.78, p = 0.30) and (SMD = 0.94, 95% CI = −0.65–2.52, p = 0.25), respectively. However, there was a significant heterogeneity in the studies, (I2 = 82%, p = 0.004) and (I2 = 83%, p = 0.001), respectively. See Figures 3A,B for the forest plots of balance post intervention and at follow up, respectively.
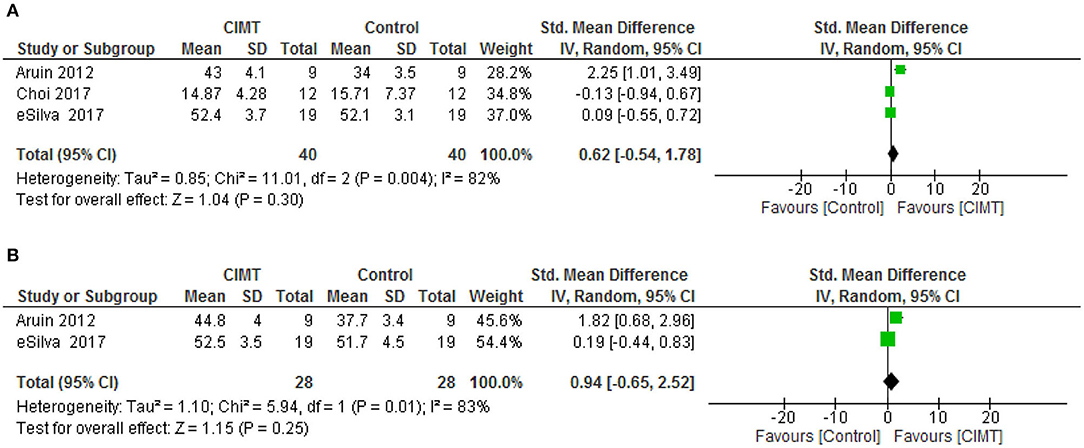
Figure 3. (A) Balance post-intervention. (B) Balance at follow up.
For functional mobility, there was no significant difference between CIMT and the control at both post intervention [mean difference (MD) = −0.53, 95% CI = −3.61–2.52, p = 0.74] and follow-up [MD = −3.16, 95% CI = −6.96–0.64, p = 0.10). However, there was no significant heterogeneity in the studies, (I2 = 30%, p = 0.24) and (I2 = 0%, p = 0.92), respectively. See Figures 4A,B for the forest plots of functional mobility post intervention and at follow up, respectively.
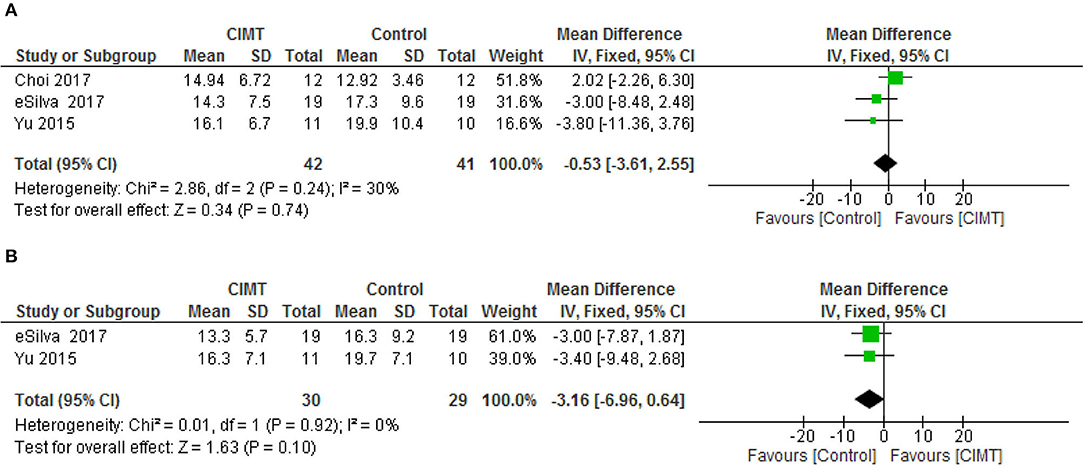
Figure 4. (A) Functional mobility post-intervention. (B) Functional mobility follow up.
For gait speed, there was no significant difference between CIMT and the control post intervention (SMD = 0.57, 95% CI= −0.22–1.37, p = 0.16) and at follow-up (SMD = 0.20, 95% CI = −0.26–0.66, p = 0.09). However, there was no significant heterogeneity in the studies, (I2 = 33%, p = 0.22) and (I2 = 65%, p = 0.09), respectively. See Figures 5A,B for the forest plots of gait speed post intervention and at follow up, respectively.
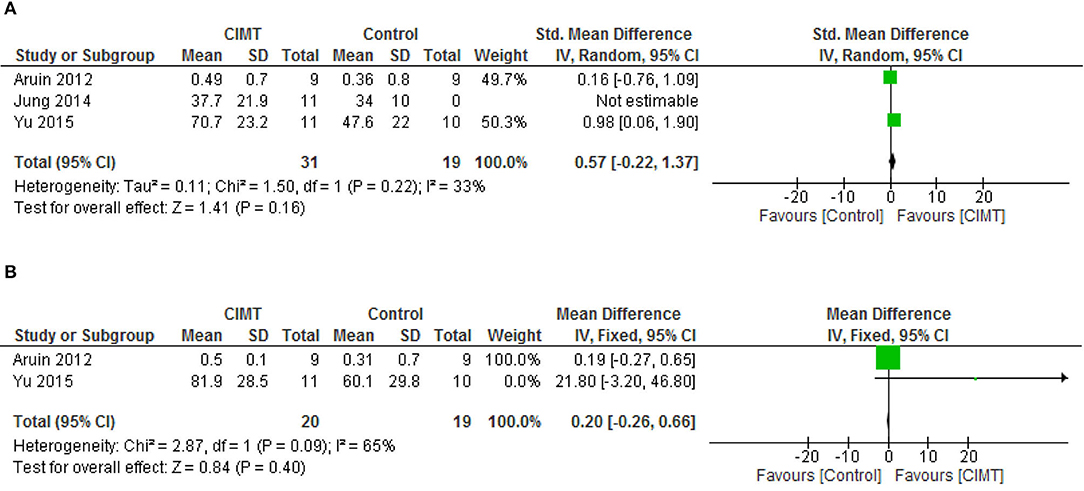
Figure 5. (A) Gait speed post-intervention. (B) Gait speed at follow up.
For quality of life, there was significant difference between CIMT and the control post intervention (MD = 16.20, 95% CI = 3.30–29.10, p = 0.01) and at follow-up (MD = 14.10, 95% CI = 2.07–26.13, p = 0.02) in favor of CIMT. However, there was significant heterogeneity in the studies post intervention (I2 = 84%, p = 0.01). See Figures 6A,B for the forest plots of quality-of-life post intervention and at follow up, respectively.
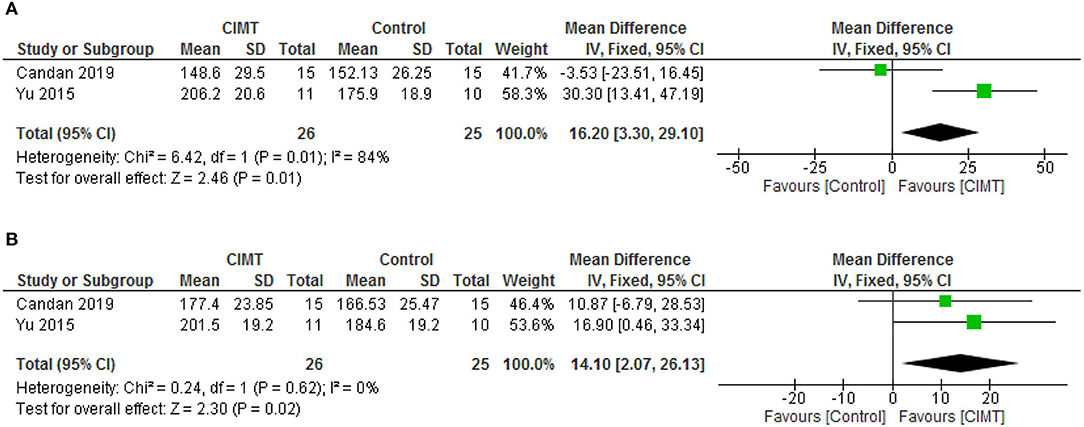
Figure 6. (A) Quality of life post-intervention. (B) Quality of life at follow up.
Ten studies were rated as Level II evidence (22, 24–31, 37). One study was rated as Level III-2 evidence (34). Three studies were rated as level III-3 evidence (23, 32, 33). Two studies were rated as level IV evidence (35, 36). The main methodological concerns in the included studies are a lack of justification for the sample size as only four studies performed a power calculation (22, 24, 27, 37); only six studies provided information on the reliability (24–27, 34, 36); only four studies provided information on validity (26, 34, 36, 37); and lack of reporting clinical significance as only three studies provided information on this (22, 23, 36). In addition, only three studies reported adverse events, tiredness, and stiff and aching muscles; physical and mental stress; and mild low back pain and calf muscle pain, respectively (33, 35, 37). See Table 3 for the details of the methodological quality and level of evidence of the included studies and Figure 7 for the risk of bias graph of the included RCTs. Considering the results of the review, the evidence was interpreted in Table 4 using NHMRC form (42).
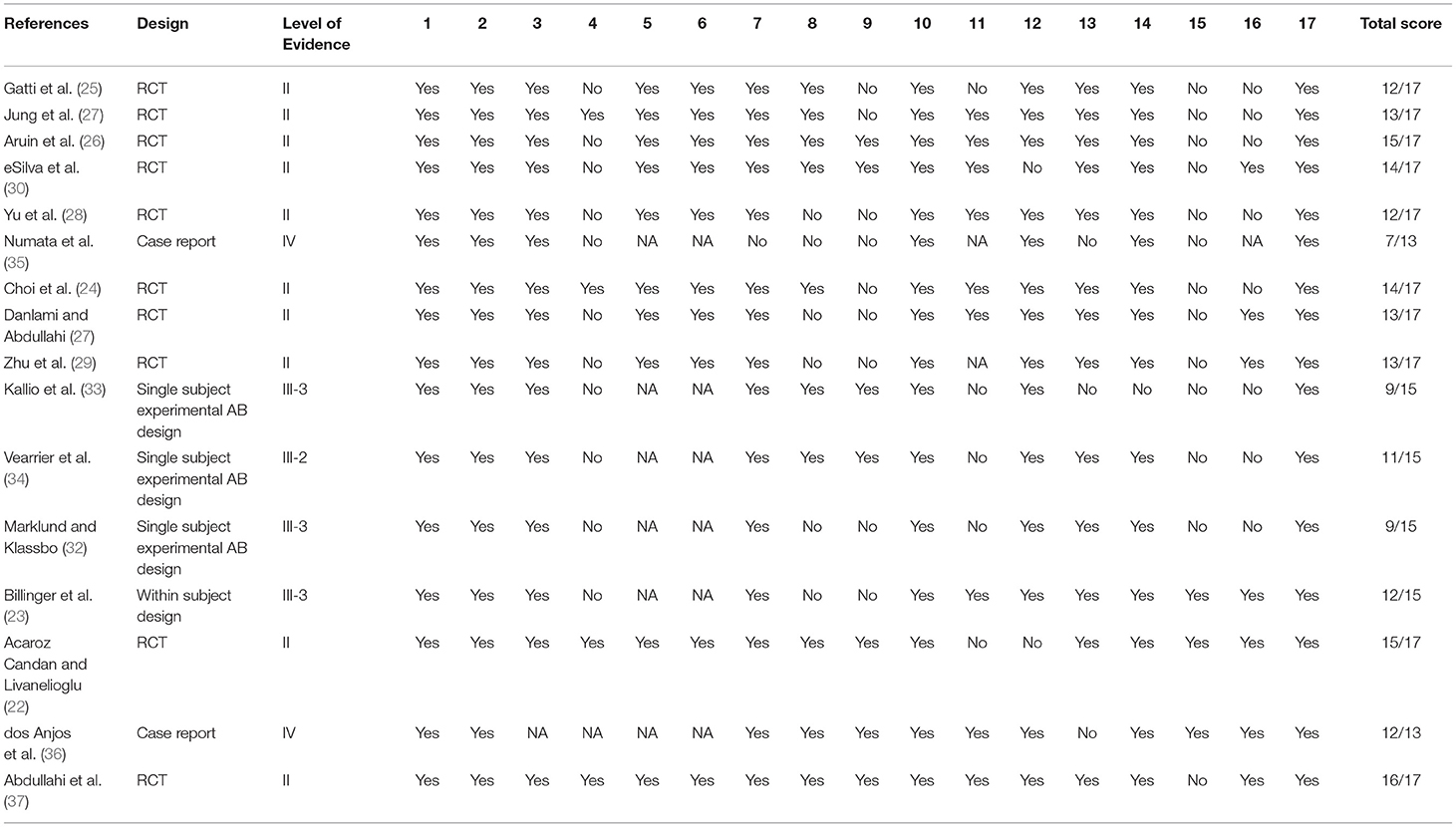
Table 3. Levels of evidence and methodological quality of the included studies.
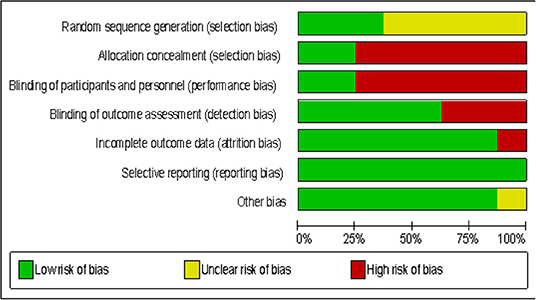
Figure 7. Risk of bias of the included RCTs.
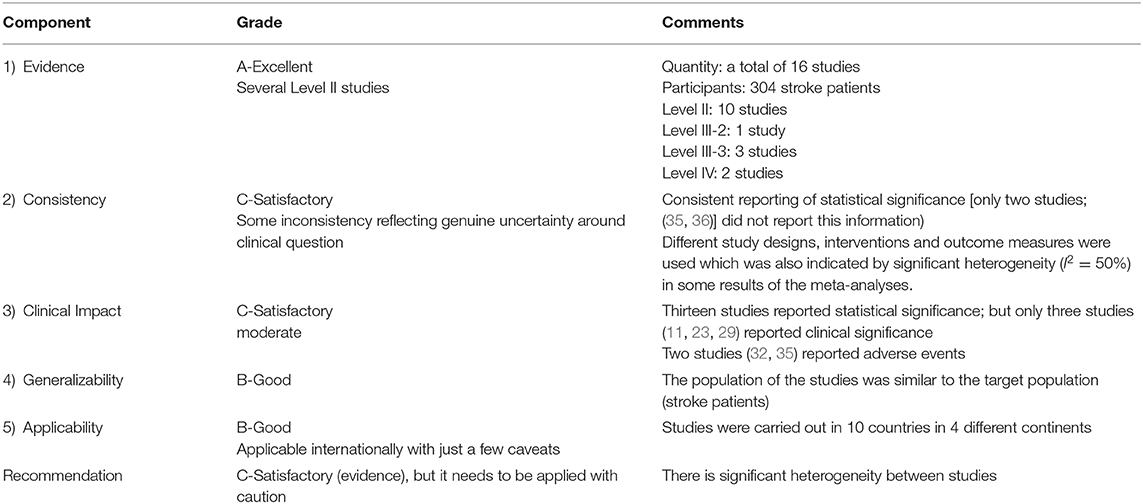
Table 4. NHMRC form framework.
The aim of this systematic review and meta-analysis was to find out what effects of lower limbs CIMT have on outcomes after stroke. The results showed that, 16 studies with levels of evidence ranging from level IV to level II were eligible for the study. The studies were carried out in 10 different countries and four different continents. In addition, the studies showed that, lower limb CIMT improves motor function, balance, functional mobility, walking speed, oxygen uptake, weight bearing, knee extensor spasticity, exertion before and after commencement of activities, quality of life, and kinematic outcomes. However, a meta-analysis involving 6 level II studies showed that there was only a significant difference between the experimental and control groups in quality of life at both post intervention and follow-up, in favor of CIMT. These findings can be explained by many factors. First, the participants in the RCTs included in the meta-analysis were mainly in the chronic stage of stroke, a stage in which the functional recovery process is usually very slow (43). Therefore, during this stage, many patients might have learned to compensate for their deficits, especially since humans are bipedal. To achieve recovery of function during the chronic stage of stroke, motor rehabilitation techniques such as CIMT may need to be combined with sensorimotor stimulation techniques such as transcortical direct stimulation (tCDs) and trans-magnetic stimulation (TMS) (44). This may help in recruiting more areas of the brain that will help in controlling motor function. Coincidently, none of the included studies combined CIMT with any sensorimotor stimulation techniques.
Second, there is heterogeneity in the included studies, especially in the protocols of CIMT and the outcome measures used. Heterogeneity can affect outcomes in terms of either overestimating or underestimating them (45). For instance, types of constraints (shoe raise, weight bearing on the affected limb, splints/orthosis, weight attached to the participants' ankles, and whole leg orthosis) used in the studies differ significantly. Use of constraints such as a shoe raise or insole during lower limb CIMT could alter the lower limbs' biomechanics and hinder recovery of function. Therefore, considering, the potential of the use of constraints such as the shoe raise in altering lower limb biomechanics, it can be argued that use of a constraint during lower limb CIMT may not be necessary. Rather, patients can be instructed to make sure they maximize the use of the affected limb, while minimizing the use of the unaffected limb as much as possible. Similarly, half of the six RCTs included in the meta-analysis are underpowered as only four studies calculated the sample size. Small sample studies may overestimate or underestimate effects (13–15). Furthermore, in most of the studies, there does not seem to be much difference in terms of the types, or the intensity of tasks practiced between the experimental and the control groups. According to the results of previous studies, intensity of task practice (how much a task is practiced or repeated) is an integral requirement for recovery of function (46–48). However, in some of the studies included in this review, intervention was provided for just a short period of time which may not allow for the high intensity training required for neuroplasticity to take place and therefore, the subsequent improvement in functions. Neuroplasticity is usually achieved when there is a high repetition of tasks of about 300 times per day which is usually performed within 1 h on average (46, 47). High repetitions of task practice may only be achieved within a short period when technological aids are used. In a recent systematic review and meta-analysis, task repetitions of 800 to 1,000 were achieved in 30 min in patients with severe motor impairment using exoskeleton robot-assisted gait training (48). Therefore, studies of lower limbs CIMT should be very clear on the types of tasks practiced in both the experimental and the control groups. Equally, the use of the number of repetitions of task practice as the measure of intensity of practice during lower limb CIMT should be encouraged. This is because this type of protocol provides a clear instruction on the intensity of the practice as opposed to the use of number of hours of practice (16, 49). Fortunately, some of the reviewed studies also used this type of protocol (23, 30, 31, 37).
In addition, most of the exercises used in the studies did not target balance directly but were aimed at improving motor function and functional mobility. Balance control goes beyond motor ability (50). However, even though there was no significant difference in motor function and balance between groups, careful observation of the forest plots revealed that the combined effect sizes for these two outcomes were in favor of the experimental group. This indicates that, there was a trend toward better improvement in balance in the experimental group compared with the control group. Similarly, CIMT showed better improvement in quality of life which is an important outcome for people with stroke. The reason for this could be because quality of life is a subjective outcome which may depend on many factors including time since stroke (51). Interestingly, most of the participants in the included studies were within the chronic stage of stroke, a time when patients might have learned to cope with their condition or disability. Consequently, their disabilities may not seriously or negatively impact their quality of life.
Nevertheless, the overall findings have implications for both research and practice. For research, more studies are needed to compare the effects of lower limb CIMT and control intervention on outcomes after stroke. For practice, since the number of repetitions of task practice required for recovery of motor function following stroke is known, lower limbs CIMT should focus on the use of this number of repetitions in their protocols. This type of protocol has been advocated and used for upper limb CIMT with success (16, 17, 46, 47). In addition, use of constraints such as a shoe raise or insole during lower limb CIMT, which could alter the lower limb's biomechanics and subsequently the limb's function, should be discouraged. Furthermore, the neurophysiological underpinnings of lower limb CIMT should also be investigated to help elucidate more robust evidence for it. This is because, for upper limb CIMT, many neurophysiological changes such as an increased cortical map size, decreased intracallosal inhibition, and the upregulation of growth associated protein 43 (GAP-43) have been reported (5, 52, 53).
Lower limb CIMT is effective at improving outcomes such balance, functional mobility, motor function, gait speed, oxygen uptake, exertion before and after commencement of activities, knee extensor spasticity, weight bearing, lower limb kinematic, and quality of life following a stroke. However, based on the current evidence, it is only superior to the control at improving quality of life. Therefore, more studies, especially RCTs, with adequate power are needed to determine the effects of lower limb CIMT on outcomes after stroke compared with the control. The studies should also include qualitative methodology to help gain more insights from the participants on how lower limb CIMT improves their functions.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
AA and NU conceived the study. AA, ST, NU, UU, VE, TV, and WS designed the study. AA, NU, TV, and VE in the data collection. AA did the qualitative and quantitative analysis and writing up of the manuscript. ST and WS cross checked the analyses and the interpretations. ST, NU, UU, VE, TV, and WS critically reviewed the manuscript. All authors approved the manuscript for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.638904/full#supplementary-material
1. Ostendorf CG, Wolf SL. Effect of forced use of the upper extremity of a hemiplegic patient on changes in function. A single-case design. Phys Ther. (1981) 61:1022–8. doi: 10.1093/ptj/61.7.1022
2. Taub E, Berman AJ. Avoidance conditioning in the absence of relevant proprioceptive and exteroceptive feedback. J Comp Physiol Psychol. (1963) 56:1012–6. doi: 10.1037/h0048315
3. Gauthier LV, Taub E, Perkins C, Ortmann M, Mark VW, Uswatte G. Remodeling the brain: plastic structural brain changes produced by different motor therapies after stroke. Stroke. (2008) 39:1520–25. doi: 10.1161/STROKEAHA.107.502229
4. Massie C, Malcolm MP, Greene D, Thaut M. The effects of constraint-induced therapy on kinematic outcomes and compensatory movement patterns: an exploratory study. Arch Phys Med Rehabil. (2009) 90:571–9. doi: 10.1016/j.apmr.2008.09.574
5. Cunningham DA, Varnerin N, Machado A, Bonnetta C, Janini D, Roelle S. Stimulation targeting higher motor areas in stroke rehabilitation: a proof-of-concept, randomized, double-blinded placebo-controlled study of effectiveness and underlying mechanisms. Restor Neurol Neurosci. (2015) 33:911–26. doi: 10.3233/RNN-150574
6. El-Helow MR, Zamzam ML, Fathalla MM, El-Badawy MA, El-Nahhas N, Awad MR, et al. Efficacy of modified constraint-induced movement therapy in acute stroke. Eur J Phys Rehabil Med. (2015) 51:371–379.
7. Etoom M, Hawamdeh M, Hawamdeh Z. Constraint-induced movement therapy as a rehabilitation intervention for upper extremity in stroke patients: systematic review and metaanalysis. Int J Rehabil Res. (2016) 39:197–210. doi: 10.1097/MRR.0000000000000169
8. Page SJ, Levine P, Leonard AC. Modified constraintinduced therapy in acute stroke: a randomized controlled pilot study. Neurorehabil Neural Repair. (2005) 19:27–32. doi: 10.1177/1545968304272701
9. Brogårdh C, Vestling M, Sjölund BH. Shortened constrained induced movement therapyin subacute stroke-no effect of using a restraint: a randomized controlled study with independent observers. J Rehabil Med. (2009) 41:231–6. doi: 10.2340/16501977-0312
10. Nijland R, Kwakkel G, Bakers J, van Wegen E. Constraint-induced movement therapy for the upper paretic limb in acute or sub-acute stroke: a systematic review. Int J Stroke. (2011) 6:425–33. doi: 10.1111/j.1747-4949.2011.00646.x
11. dos Anjos S, Morris D, Taub E. Constraint-induced movement therapy for lower extremity function: describing the LE-CIMT protocol. Phys Ther. (2020) 100:698–707. doi: 10.1093/ptj/pzz191
12. Ribeiro TS, Oliveira DA, Ferreira LGLM, Costa MFP, Lacerda MO, Lindquist ARR. Constraint- induced movement therapy for the paretic lower limb in acute and sub-acute stroke. Austin J Cerebrovasc Dis Stroke. (2014) 1:1029.
13. Button KS, Ioannidis JP, Mokrysz C, Nosek BA, Flint J, Robinson ESJ, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. (2013) 14:365–76. doi: 10.1038/nrn3475
14. Colquhoun D. An investigation of the false discovery rate and the misinterpretation of p-values. R Soc Open Sci. (2014) 1:140216. doi: 10.1098/rsos.140216
15. Forstmeier W, Wagenmakers EJ, Parker TH. Detecting and avoiding likely false-positive findings – a practical guide. Biol Rev Camb Philos Soc. (2017) 92:1941–68. doi: 10.1111/brv.12315
16. Abdullahi A. Is time spent using constraint induced movement therapy an appropriate measure of dose? A critical literature review. Int J Therap Rehabil. (2014) 21:140–6. doi: 10.12968/ijtr.2014.21.3.140
17. Abdullahi A. Effects of number of repetitions and number of hours of shaping practice during constraint-induced movement therapy: a randomized controlled trial. Neurol Res Int. (2018) 2018:5496408. doi: 10.1155/2018/5496408
18. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan- a web and mobile application for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
19. Law M, Stewart C, Pollock N, Letts L, Bosch J, Westmorland M. McMaster Critical Review Form±Quantitative Studies. Hamilton, ON: McMaster University Occupational Therapy Evidence-Based Practice Research Group (1998).
20. Law M, Stewart D, Pollock N, Letts L, Bosch J, Westmorland M. Guidelines for Critical Review Formð* Quantitative Studies. Hamilton, ON: McMaster University Occupational Evidence-based Practice Research Group (1998).
21. Council-NHaMR. NHMRC Levels of Evidence and Grades for Recommendations for Guideline Developers. Canberra, ACT: National Health and Medical Research Council (2009).
22. Acaröz Candan S, Livanelioglu A. Efficacy of modified constraint-induced movement therapy for lower extremity in patients with stroke: strength and quality of life outcomes. Turkish J Physiother Rehabil. (2019) 30:23–32. doi: 10.21653/tfrd.406349
23. Billinger SA, Guo LX, Pohl PS, Kluding PM. Single limb exercise: pilot study of physiological and functional responses to forced use of the hemiparetic lower extremity. Top Stroke Rehabil. (2010) 17:128–39. doi: 10.1310/tsr1702-128
24. Choi HS, Shin WS, Bang DH, Choi SJ. Effects of game-based constraint-induced movement therapy on balance in patients with stroke. A single-blind randomized controlled trial. Am J Phys Med Rehabil. (2017) 96:184–90. doi: 10.1097/PHM.0000000000000567
25. Gatti A, Tettamanti A, Sirtori V, Comola N. Disadvantage of the healthy lower limb in subacute poststroke subject: a pilot study. Physiotherapy. (2011) 1:107–14.
26. Aruin AS, Rao N, Sharma A, Chaudhuri G. Compelled body-weight shift approach in rehabilitation of individuals with chronic stroke. Top Stroke Rehabil. (2012) 19:556–63. doi: 10.1310/tsr1906-556
27. Jung K, Kim Y, Cha Y, In TS, Hur YG, Chung Y. Effects of gait training with a cane and an augmented pressure sensor for enhancement of weight bearing over the affected lower limb in patients with stroke: a randomized controlled pilot study. Clinical Rehabil. (2014) 29:135–42. doi: 10.1177/0269215514540923
28. Yu WH, Liu WY, Wong Alice MK, Wang TC, Li YC, Lien HY. Effect of forced use of the lower extremity on gait performance and mobility of post-acute stroke patients. J Phys Ther Sci. (2015) 27:421–425. doi: 10.1589/jpts.27.421
29. Zhu Y, Zhou C, Liu Y, Liu J, Jin J, Zhang S, et al. Effects of modified constraintinduced movement therapy on the lower extremities in patients with stroke: a pilot study. Disabil Rehabil. (2016) 38:1893–9. doi: 10.3109/09638288.2015.1107775
30. eSilva EMGS, Ribeiro TS, da Silva TCC, Costa MFP, Cavalcanti FADC, Lindquist ARR. Effects of constraint-induced movement therapy for lower limbs on measurements of functional mobility and postural balance in subjects with stroke: a randomized controlled trial. Top Stroke Rehabil. (2017) 24:555–61. doi: 10.1080/10749357.2017.1366011
31. Danlami KA, Abdullahi A. Remodelling the protocol of lower limb constraint induced movement therapy: a randomized controlled trial. Arch Physiother Glob Res. (2017) 21:21–7.
32. Marklund I, Klässbo M. Effects of lower limb intensive mass practice in poststroke patients: single-subject experimental design with long-term follow-up. Clin Rehabil. (2006) 20:568–76. doi: 10.1191/0269215506cr973oa
33. Kallio K, Nilsson-Wikmar L, Thorsén AM. Modified constraint-induced therapy for the lower extremity in elderly persons with chronic stroke: single-subject experimental design study. Top Stroke Rehabil. (2014) 21:111–9. doi: 10.1310/tsr2102-111
34. Vearrier LA, Langan J, Shumway-Cook A, Woollacott M. An intensive massed practice approach to retraining balance post-stroke. Gait Posture. (2005) 22:154–6. doi: 10.1016/j.gaitpost.2004.09.001
35. Numata K, Murayama T, Takasugi J, Oga M. Effect of modified constraint-induced movement therapy on lower extremity hemiplegia due to a higher-motor area lesion. Brain Injury. (2008) 22:898–904. doi: 10.1080/02699050802425436
36. dos Anjos S, Morris DM, Taub E. Constraint-induced movement therapy for improving motor function of the paretic lower extremity after stroke. Am J Phys Med Rehabil. (2020) 99:e75–8. doi: 10.1097/PHM.0000000000001249
37. Abdullahi A, Umar NA, Ushotanefe U, Abba MA, Akindele MO, Truijen S, et al. Effects of two different modes of tasks practice during lower limbs constraint-induced movement therapy in people with stroke: a randomized clinical trial. Neural Plast. (2020) 2021:6664058. doi: 10.1155/2021/6664058
38. Vermeer SE, Algra A, Franke CL, Koudstaal PJ, Rinkel GJE. Long-term prognosis after recovery from primary intracerebral hemorrhage. Neurology. (2002) 59:205–9. doi: 10.1212/WNL.59.2.205
39. Bindawas SM, Mawajdeh HM, Vennu VS, Alhaidary HM. Functional recovery differences after stroke rehabilitation in patients with uni- or bilateral hemiparesis. Neurosciences. (2017) 22:186–91. doi: 10.17712/nsj.2017.3.20170010
40. Shumway-Cook A, Woollacott MH. Motor Control: Theory and Practical Applications. Philadelphia: Lippincott Williams & Wilkins (2001).
41. Bouça-Machado R, Maetzler W, Ferreira JJ. What is functional mobility applied to parkinson's disease? J Parkinsons Dis. (2018) 8:121–30. doi: 10.3233/JPD-171233
42. Hillier S, Grimmer-Somers K, Merlin T, Middleton P, Salisbury J, Tooher R. FORM: an Australian method for formulating and grading recommendations in evidence-based clinical guidelines. BMC Medical Res Methodol. (2011) 11:23. doi: 10.1186/1471-2288-11-23
43. Duncan PW, Lai SM. Stroke recovery. Topics Stroke Rehabil. (1997) 4:51–8 doi: 10.1310/KYD7-HN2K-VGYG-8C98
44. Abdullahi A, Truijen S, Saeys W. Neurobiology of recovery of motor function after stroke: the central nervous system (CNS) biomarkers of effects of constraint induced movement therapy. Neural Plasticit. (2020) 2020:9484298. doi: 10.1155/2020/9484298
45. Cochrane Methods. Assessing Risk of Bias in Included Studies. London: The Cochrane Collaboration (2017). Available online at: https://tinyurl.com/yc9gmpzh
46. Birkenmeier RL, Prager EM, Lang CE. Translating animal doses of task-specific training to people with chronic stroke in one hour therapy sessions: a proof-of-concept study. Neurorehabil Neural Repair. (2010) 24:620–35. doi: 10.1177/1545968310361957
47. Waddell KJ, Birkenmeier RL, Moore JL, George Hornby TG, Lang CE. Feasibility of high-repetition, task-specific training for individuals with upper-extremity paresis. Am J Occup Ther. (2014) 68:444–53. doi: 10.5014/ajot.2014.011619
48. Schröder J, Truijen S, Van Criekinge T, Wim Saeys W. Feasibility and effectiveness of repetitive gait training early after stroke: a systematic review and meta-analysis. J Rehabil Med. (2019) 51:78–88. doi: 10.2340/16501977-2505
49. Kaplon RT, Prettyman MG, Kushi CLCJ. Six hours in the laboratory: quantification of practice time during constraint induced therapy. ClinRehabil. (2007) 21:950–8. doi: 10.1177/0269215507078333
50. Reimann H, Fettrow T, Thompson ED, Jeka JJ. Neural control of balance during walking. Front Physiol. (2018) 9:1271. doi: 10.3389/fphys.2018.01271
51. Huang YH, Wu CY, Lin KC, Hsieh YW, Snow WM, Wang TN. Determinants of change in stroke-specific quality of life after distributed constraint-induced therapy. Am J Occup Ther. (2013) 67:54–63. doi: 10.5014/ajot.2013.004820
52. Ro T, Noser E, Boake C, Johnson R, Gaber M, Speroni A, et al. Functional reorganization and recovery after constraint-induced movement therapy in subacute stroke: case reports. Neurocase. (2006) 12:50–60. doi: 10.1080/13554790500493415
53. Zhao S, Zhao M, Xiao T, Jolkkonen J, Zhao C. Constraint- induced movement therapy overcomes the intrinsic axonal growth-inhibitory signals in stroke rats. Stroke. (2013) 44:1698–705. doi: 10.1161/STROKEAHA.111.000361
The search strategy used in PubMED and CENTRAL.
1) Constraint induced movement therapy
2) Constraint induced therapy
3) Forced use
4) 1 OR 2 OR 3
5) Stroke
6) 4 AND 5
7) Lower limbs
8) 6 AND 7
Keywords: stroke, lower extremity, constraint induced movement therapy, activities of daily living, quality of life
Citation: Abdullahi A, Truijen S, Umar NA, Useh U, Egwuonwu VA, Van Criekinge T and Saeys W (2021) Effects of Lower Limb Constraint Induced Movement Therapy in People With Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 12:638904. doi: 10.3389/fneur.2021.638904
Received: 07 December 2020; Accepted: 22 February 2021;
Published: 23 March 2021.
Edited by:
Nam-Jong Paik, Seoul National University, South KoreaReviewed by:
Fan Gao, University of Kentucky, United StatesCopyright © 2021 Abdullahi, Truijen, Umar, Useh, Egwuonwu, Van Criekinge and Saeys. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Auwal Abdullahi, YWFiZHVsbGFoaS5wdGhAYnVrLmVkdS5uZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.