
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 22 February 2021
Sec. Applied Neuroimaging
Volume 12 - 2021 | https://doi.org/10.3389/fneur.2021.598336
 Vincent Huynh1,2*
Vincent Huynh1,2* Philipp Staempfli3,4
Philipp Staempfli3,4 Robin Luetolf2
Robin Luetolf2 Roger Luechinger5
Roger Luechinger5 Armin Curt1Spyros Kollias1
Armin Curt1Spyros Kollias1 Michèle Hubli2†
Michèle Hubli2† Lars Michels1†
Lars Michels1†Remote neurodegenerative changes in supraspinal white matter (WM) can manifest after central lesions such as spinal cord injury (SCI). The majority of diffusion tensor imaging (DTI) studies use traditional metrics such as fractional anisotropy (FA) and mean diffusivity (MD) to investigate microstructural changes in cerebral WM after SCI. However, interpretation of FA readouts is often challenged by inherent limitations of the tensor model. Recent developments in novel diffusion markers, such as fiber density (FD), allows more accurate depictions of WM pathways and has shown more reliable quantification of WM alterations compared to FA in recent studies of neurological diseases. This study investigated if FD provides useful characterization of supraspinal WM integrity after SCI in addition to the traditional DTI readouts. FA, MD, and FD maps were derived from diffusion datasets of 20 patients with chronic SCI and compared with 19 healthy controls (HC). Group differences were investigated across whole brain WM using tract-based spatial statistics and averaged diffusion values of the corticospinal tract (CST) and thalamic radiation (TR) were extracted for comparisons between HC and SCI subgroups. We also related diffusion readouts of the CST and TR with clinical scores of sensorimotor function. To investigate which diffusion markers of the CST and TR delineate HC and patients with SCI a receiver operating characteristic (ROC) analysis was performed. Overall, patients with an SCI showed decreased FA of the TR and CST. ROC analysis differentiated HC and SCI based on diffusion markers of large WM tracts including FD of the TR. Furthermore, patients' motor function was positively correlated with greater microstructural integrity of the CST. While FD showed the strongest correlation, motor function was also associated with FA and MD of the CST. In summary, microstructural changes of supraspinal WM in patients with SCI can be detected using FD as a complementary marker to traditional DTI readouts and correlates with their clinical characteristics. Future DTI studies may benefit from utilizing this novel marker to investigate complex large WM tracts in patient cohorts with varying presentations of SCI or neurodegenerative diseases.
Spinal cord injury (SCI) characteristically results in impairment of the central nervous system and presents with varying clinical characteristics, e.g., loss of motor and sensory function due to disruption of efferent and afferent pathways (1, 2). Traumatic SCI inevitably causes damage to white matter (WM) and mechanical destruction of glial cells and axons at the spinal cord level (1). However, beyond the immediate focal cord damage progressive degeneration in both antero- and retrograde directions of major WM tracts [e.g., the corticospinal (CST)] from the injury site and accompanying neuroplastic changes have been also revealed at supraspinal levels (3–5).
Recent neuroimaging studies including SCI patients have shown macrostructural alterations within the primary sensorimotor cortices, thalamus and frontal regions (3, 6, 7). In addition, current diffusion tensor imaging (DTI) studies have reported microstructural changes within the cerebellum, brainstem regions and large WM tracts (8–14). These DTI studies have provided insight on the impact of SCI in brain WM integrity, e.g., neurodegeneration, as indirectly measured and inferred by fractional anisotropy (FA) and mean diffusivity (MD), respectively (15–18). Whilst FA measures the preferential direction of water movement within tissue architecture, i.e., water molecules diffuse along the direction of tightly packed axons, MD measures the degree of water diffusion. In comparison to healthy controls (HC), SCI patients commonly show decreased FA and increased MD of large WM fibers, i.e., corpus callosum, anterior cingulum, superior and inferior longitudinal fasciculus (12, 19), regions of the CST and primary motor cortex (8, 20), as well as brainstem to midbrain regions (9). Furthermore, two cohorts of patients with a sensorimotor complete SCI and a poor recovery after a 6 months follow-up, showed decreased FA in the cerebellum (10) and primary motor cortex (11). In contrast, patients with an incomplete SCI and a favorable motor recovery at 6 months post-SCI showed similar WM integrity compared to healthy controls (HC) (10, 11). Accordingly, studies that investigated correlations between clinical characteristics and WM integrity reported that SCI patients with better sensory and motor function also showed higher FA values of the posterior thalamic radiations (TR) (13) and pathways of the CST (10), respectively.
However, DTI readouts, such as FA and MD, require careful interpretation when inferring the microstructural integrity of WM in patient cohorts (16). An inherent limitation of the tensor model is the inability to characterize complex fiber orientations, i.e., crossing or “kissing” fibers, which may confound the quantitative changes of FA (21). This problem is addressed with recent optimized methods such as spherical deconvolution (21, 22), which significantly improved the resolution of multiple fiber orientations within a voxel and the tractography method overall (22). Nevertheless, the extraction of reliable quantitative measures from diffusion weighted imaging remains challenging. Recent advances in tractography algorithms (23), microstructural diffusion models (24) and techniques for optimizing tractograms (25) have established a new parameter commonly referred as fiber density (FD). This marker is related to the volume of the intra-axonal compartment per unit of tissue volume, and is therefore sensitive to the volume of a fiber bundle (26, 27). According to the work by Daducci et al., and Smith et al., an optimal weight for each streamline is determined according to a biologically motivated forward model and the measured diffusion signal (25, 28). Assigning a weight of zero allows the elimination of false positive or improbable connections. In this work, we use the COMMIT framework of Daducci et al. (25). One of the results of the COMMIT optimization are intracellular compartment maps (IC maps), which are a direct measure of and correspond to the FD used in the present study. This measurement provides a better representation of the underlying WM tracts and may overcome limitations of traditional tensor derived measures [for DTI limitations see reviews (24, 29, 30)].
With regard to clinical application, FD has recently shown promise in evaluating cerebral WM integrity in neurological diseases such as amyotrophic lateral sclerosis (31) and schizophrenia (45). Specifically, longitudinal changes of FD were observed in commissural and association fiber tracts in amyotrophic lateral sclerosis patients (31) and correlations of positive symptoms with FD of the TR were reported in schizophrenia patients (45). In contrary, no significant results were observed with FA in these two studies, suggesting that FD could be more sensitive to microstructural WM changes in some clinical cohorts compared to FA.
Therefore, this study aims to investigate if FD provides useful characterization of supraspinal WM integrity after SCI in addition to traditional DTI readouts (FA and MD). Specifically, we explore differences between SCI patients and HC in the integrity of the entire WM and also of specific large WM tracts (e.g., CST). We further assess whether the clinical characteristics of SCI correlate with microstructural changes of WM, in particular major tracts involved in sensorimotor processing, i.e., CST and TR. This is performed by subgrouping the SCI cohort based on their severity, i.e., sensorimotor complete (AIS A) and motor incomplete (AIS C-D) lesions (32), and examining the relationship between sensorimotor function and the microstructural integrity of the CST and TR.
Based on previous studies, we hypothesize that patients with a more severe SCI will show decreased FA and FD, and increased MD of major cerebral WM tracts compared to less severely affected SCI patients and HC. Secondly, we hypothesize that SCI patients with better sensorimotor function will show greater WM integrity of the CST and TR.
Patients with a SCI were contacted and recruited via fllier advertisements and phone calls from the Spinal Cord Injury Center at Balgrist University Hospital and the Swiss Spinal Cord Injury Cohort Study. The inclusion criteria were: (i) Thoracic (T1-T12), traumatic SCI (paraplegics) and all levels of impairment as measured by the American Spinal Injury Association (ASIA) impairment scale (AIS A–D) (33); (ii) no contraindications for MRI; and (iii) no history or presence of other neurological conditions (e.g., traumatic brain injury). The inclusion criteria for HC were no history of neurological illness or other medical condition. All subjects provided written informed consent prior to the assessments and all procedures described below were in accordance with the Declaration of Helsinki. The study has been approved by the local ethics board “Kantonale Ethikkommission Zürich, KEK” (EK-04/2006, PB_2016-02051, clinicaltrial.gov number: NCT02138344).
Sensorimotor function was assessed using the sensory and motor scores from the International Standards for Neurological Classification of SCI (ISNCSCI) (33). Specifically, the sum of lateralised sensory scores (light touch and pin prick) and lower extremity motor scores (LEMS, left and right) were extracted to investigate correlations with lateralised WM fibers, i.e., right and left TR/CST. Upper extremity motor scores were omitted as all SCI subjects had intact motor function above the level of injury.
All subjects' MRI data were obtained using a 3.0 Tesla Philips Ingenia system (Philips Medical Systems, Best, the Netherlands) using a 32-channel Philips head coil. Diffusion weighted images were acquired with the following parameters: repetition time (TR), 12700.87 ms; echo time (TE), 79.9 ms; flip angle, 90°; number of slices, 52; slice thickness, 2.3 mm; field of view (FOV), 258 × 119.6 × 258 mm3; matrix, 112 × 110 and a scan time of 16:06 min. Diffusion acquisition was performed with a b-value of 1,500 s/mm2 along 62 directions after acquiring b0 images. 3D T1-weighted (T1w) structural images were acquired with a Turbo Field Echo sequence with the following parameters: TR, 8.083 ms; TE, 3.70 ms; flip angle, 8°; number of slices, 160; slice thickness, 1 mm; FOV, 240 × 240 × 160 mm3; matrix, 240 × 240 and isotropic voxel 0.97 × 0.98 × 1 mm3 and a scan time of 4:53 min.
The brain extraction tool in FSL 6.0 software (Oxford University Center for Functional Magnetic Resonance Imaging of the Brain, Oxford, UK; https://fsl.fmrib.ox.ac.uk/fsl/) (34, 35) was utilized to remove non-brain tissue from the diffusion data. Subsequently, the diffusion data was corrected for eddy current and head motion with the eddy tool (36). Diffusion tensor residuals were calculated for every acquired diffusion direction and the nine slices in the whole diffusion dataset with the highest residuals were identified for visual inspection. Furthermore, the MRtrix3 software package was applied to estimate the voxel-wise noise level using the residuals from a truncated spherical harmonics fit. Plots were generated depicting the 12 slices with the highest noise level, four in sagittal, four in axial, and four in coronal direction. In addition, mean signal intensity plots for every diffusion direction and the non-diffusion weighted image were derived and plotted slice by slice in sagittal, transverse, and coronal planes. Peaks in these signal courses often indicate head motion. Based on a subject-wise visual inspection of these signal courses and fitting residuals, a rating was performed on a Likert-type scale by a trained MR physicist (range 0–2; 0 = no motion, 2 = high motion). High motion data was omitted from analysis and data was also visually inspected for artifacts.
Pre-processing of the remaining diffusion weighted images was performed using FSL 6.0 software (Oxford University Center for Functional Magnetic Resonance Imaging of the Brain, Oxford, UK; https://fsl.fmrib.ox.ac.uk/fsl/) and MRtrix3 software package (Brain Research Institute, Melbourne, Australia, version 0.3.12) according to the procedure in Stämpfli et al. (31). Computation of FD maps within the same datasets were performed as follows: Fiber orientation distribution reconstruction and fiber tractography using the default iFOD2 probabilistic tracking algorithm was performed in MRtrix3 (37). Due to the dynamic seeding strategy within the whole WM, the distribution of streamlines is already approximating the apparent fiber density thereby reducing intrinsic tractography biases. A total of five million fibers were generated per subject. The resulting streamlines were optimized using the COMMIT framework (25) and parameters described previously by Sommer et al., to derive the FD for every subject (38). The derived intracellular compartment fraction corresponds to the FD. Full details were previously reported (31). FA and MD maps were calculated with the FSL package including non-linear co-registration, normalization, warping, and skeleton projection (35).
TBSS analysis of skeletonised FA, MD, and FD maps was performed with the randomize function in FSL. MD and FD images were analyzed using the “tbss_non_FA” command, this step is the standard algorithm of the TBSS framework for scalar diffusion maps other than FA maps. Thus, MD and FD images were analyzed with the same non-linear registration-, warping-, and skeleton projection operations used during the processing of the corresponding FA images (39). Non-parametric permutation test with 5,000 random permutations and a threshold-free cluster enhancement (TFCE) option was implemented and all statistical maps were corrected for multiple comparisons at p = 0.05. A one-way ANCOVA was performed to compare differences of whole brain WM between the SCI cohort and HC with age and sex as covariates of no interest.
Mean FA, MD, and FD values of the left and right TR and CST were exported into Statistical Package for the Social Sciences (SPSS) 24 for statistical analysis.
The anatomical regions of interest (ROIs) defining these major fiber tracts were obtained from a probabilistic tractography atlas (JHU white-matter tractography atlas) (40). In total, the JHU white-matter tractography atlas describes 20 major fiber bundles. The probability-weighted mean FD values were calculated for each of the fiber tracts by multiplying the probability-weighted maps of the individual tract with co-registered FD maps from the TBSS analysis. In other words, the probability tract maps served as ROIs to extract the FA, MD, and FD values within each of the fiber bundles. As opposed to the TBSS method, the ROI approach estimates the integrity of entire ROIs, rather than the central integrity of the tracts only and has the advantage of a higher regional sensitivity as compared to a whole brain, voxel-based method.
All statistical analyses were performed using SPSS (version 24) for Windows. Shapiro-Wilk test was used to test normality of subjects' demographics and independent t-test and Chi-squared tests were performed to assess differences in age and sex between the cohorts, respectively. Three separate (FD, FA, MD) one-way multivariate analyses of covariance (MANCOVA) were implemented to test differences of WM tracts between the whole SCI group and HC, alongside differences between SCI subgroups (AIS A and C-D) and HC. DTI values (FD, FA, MD) of the left and right TR and CST were set as dependent variables and grouping of the subjects (i.e., HC, whole SCI and SCI subgroups) were set as independent variables. Post-hoc pairwise comparisons were implemented only on WM tracts showing significant main effect of group (p < 0.05). Sex and age were added as covariates of no interest for all analyses. Post-hoc pairwise comparisons were corrected with Bonferroni correction at p < 0.05.
Partial correlations were implemented to assess the relationship between patients' lateralised sensory and motor scores with readouts of the TR and CST, respectively, correcting for age and sex. Only p-values that survived Bonferroni-Holm correction are reported (p < 0.05).
Furthermore, to identify which diffusion measure(s) of the CST and TR have the highest sensitivity and specificity for differentiating SCI patients from HC, we performed a receiver operating characteristic (ROC) curve analysis. Each diffusion marker of each tract (FA, MD, and FD) were selected as a test probability variable. A numeric grouping variable was selected to test the amount of sensitivity and specificity of each probability variable for delineating subjects into SCI and HC. The amount of sensitivity and specificity is provided by the area under the curve (AUC) and the range from 0.5 (no discrimination)−1 (perfect discrimination) (0.7–0.8 = acceptable; 0.8–0.9 = excellent; 0.9–1 = outstanding).
Fifty-four subjects were recruited: 25 HC and 29 SCI patients. Five HC and nine SCI patients were excluded due to motion artifacts. Therefore, 19 HC and 20 SCI patients were included in the analyses. Subject demographics are summarized in Table 1.
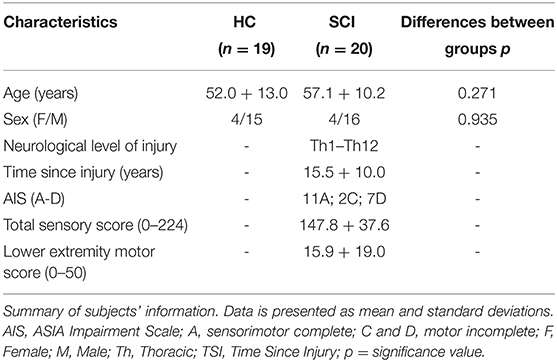
Table 1. Overview of subject demographics.
No significant differences of whole brain FA, MD, and FD maps were observed between the whole SCI cohort and HC (all p's > 0.05 TFCE). In addition, no significant differences of whole brain FA, MD, and FD maps were observed between SCI subgroups (AIS A; AIS C-D) and HC (all p's > 0.05 TFCE).
Comparing SCI and HC, between subject effects were observed in FA of the left TR [F(1, 38) = 8.36, p = 0.007], right TR [F(1, 38) = 6.45, p = 0.016], left CST [F(1, 38) = 5.84, p = 0.021], and right CST [F(1, 38) = 5.80, p = 0.022]. Patients presented with decreased FA of the left and right TR (p = 0.007 and 0.016, respectively), as well as left and right CST (p = 0.021 and 0.022, respectively) compared to HC (Table 2).
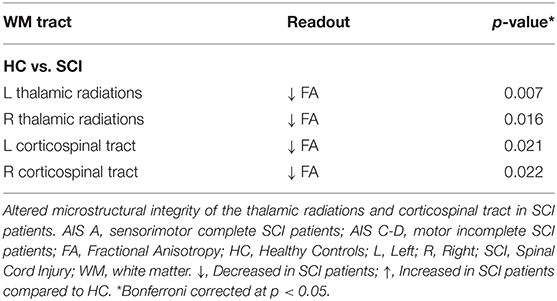
Table 2. Significant microstructural differences between HC and SCI patients.
Furthermore, between SCI subgroups and HC, between subject effects were only observed in FA of the left TR [F(1, 38) = 4.73, p = 0.015] and right TR [F(1, 38) = 3.84, p = 0.031]. Post-hoc pairwise comparisons showed that sensorimotor complete SCI patients (AIS A) present with decreased FA of the left and right TR (p = 0.015 and 0.029, respectively) compared to HC. No differences were observed between motor incomplete and sensorimotor complete SCI patients or HC (p > 0.05). Overall, FD and MD of the left and right TR and CST were not different between the groups (p > 0.05).
Significant correlations were observed between lateralised LEMS and contralateral TR and CST (Figure 1). Right LEMS correlated positively with FD (r = 0.557, p = 0.016), FA (r = 0.490, p = 0.039), and negatively with MD (r = −0.537, p = 0.022) of the left CST. No other correlations with LEMS were observed. In addition, lateralised sensory scores and microstructural readouts of the contralateral TR did not correlate (p > 0.05).
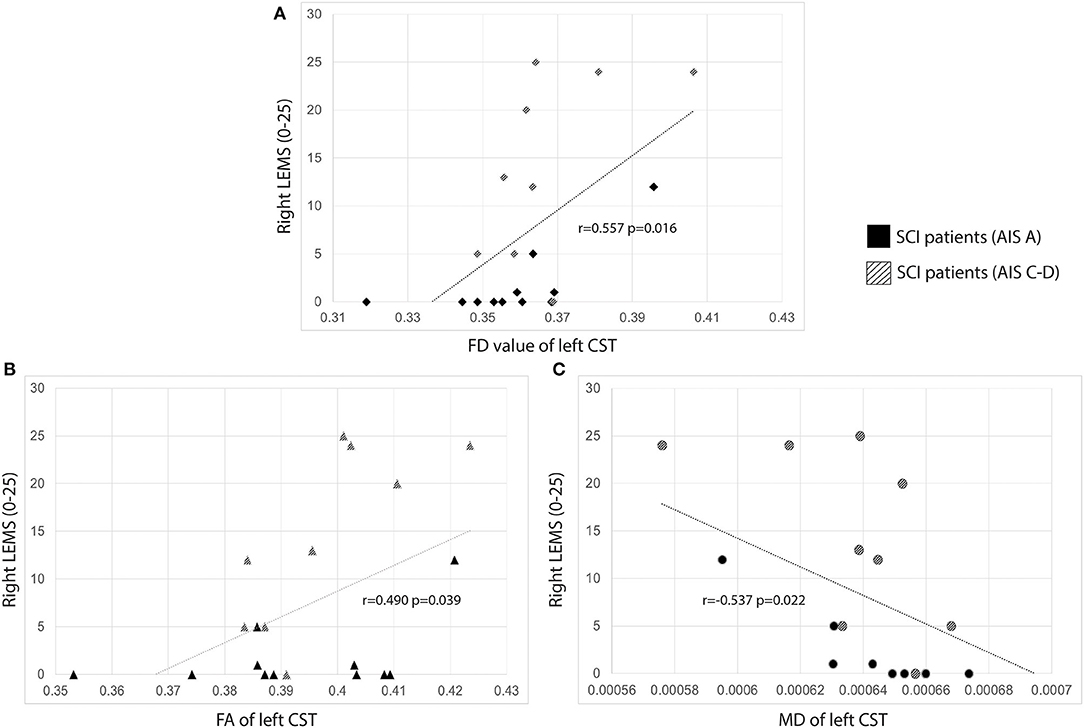
Figure 1. Scatter plots of lateralized LEMS and contralateral CST. Correlations between lateralised LEMS and microstructural readouts of the CST. SCI patients are color-coded based on impairment severity. (A) Correlations between lateralised LEMS and FD of contralateral CST; (B) correlations between lateralised LEMS and FA of contralateral CST; (C) correlations between lateralised LEMS and MD of contralateral CST. Subjects with an AIS A typically had a LEMS of 0. AIS, American Spinal Injury Association Impairment Scale; AIS A, sensorimotor complete; AIS C-D, motor incomplete; CST, corticospinal tract; FA, Fractional Anisotropy; FD, Fiber Density; LEMS, lower extreimity motor score; MD, Mean Diffusivity; SCI, Spinal Cord Injury.
The following WM tracts and diffusion measures showed the highest sensitivity for distinguishing subjects into HC and SCI: FA of the bilateral TR, CST, and FD of the bilateral TR (p < 0.05) (Supplementary Table 1).
This study explored whether FD, a novel diffusion marker, provides useful characterization of microstructural alterations of cerebral WM in patients with SCI. Although no group differences were observed with FD, FD correlates slightly stronger to the clinical outcome of SCI patients as compared to FA and MD, which could prove valuable in investigating complex WM pathways such as those involved with sensorimotor processing.
SCI patients showed significant decreases in FA of the TR and CST (Table 2). Also, our ROC curve analysis was able to differentiate between HC and SCI patients based on the FA and FD of the TR (Supplementary Table 1). Previous DTI studies have reported similar decreases in FA of the CST (8, 14, 20), cingulum (13, 19), SLF (12, 19), corpus callosum (13, 19), and TR (13) in various groups of patients with SCI, e.g., cervical vs. thoracic, complete vs. incomplete lesions. Some studies have also reported increases of MD of similar large WM tracts including the CST (8, 9, 13), corpus callosum, cingulum (13, 19), SLF (12, 13, 19), and TR (13). Furthermore, we also observed a significant negative correlation between MD of the CST and TR with patients' motor function. This could signify atrophy, i.e., decreased cell numbers of these remote sensorimotor pathways in patients with more impaired motor function. Whilst decreased FA and increased MD have been associated with impaired WM fiber integrity due to loss of coherent water movement or increased diffusion, careful interpretation is necessary and is dependent on the brain region, cellular composition and the clinical sample studied (16). In general, these DTI markers are sensitive (but non-specific) biomarkers of microstructural architecture and neuropathology (41–43). SCI causes immediate damage leading to inflammatory and degenerative processes, e.g., antero- and retrograde degeneration of WM pathways resulting in neurological dysfunction (1). Previous animal studies investigating microstructural changes at certain locations of the spine after SCI, i.e., epicenter of the injury, proximal and remote to the lesion site, suggest that axonal loss and demyelination occurs in both rostral and caudal directions [see review (44)]. Moreover, previous studies have observed correlations between clinical scores and DTI markers of WM integrity at the brain and spinal level, indicating that these markers are sensitive to the clinical characteristics of SCI patients. In particular, greater sensory scores were correlated with higher FA of the posterior TR (13) and better motor scores were correlated with higher FA within the CST pathway (centrum semiovale) (10) and cervical spinal cord (20).
Overall, our results are consistent with previous studies identifying microstructural abnormalities of cerebral WM fibers in patients with a chronic SCI. In addition, sensorimotor complete SCI patients showed abnormal microstructure of the TR whilst motor incomplete SCI patients showed no observable changes. We also found that patients with a less severe SCI (i.e., greater motor function) showed higher FA and decreased MD of the CST, indicating that a better (preserved) motor function below the level of injury is also associated with greater WM integrity of the major motor pathway (Figure 1).
A substantial benefit of FD is overcoming the limitations of classical DTI readouts, i.e., FA, which is unable to determine multiple fiber orientations within a voxel and therefore a precise anatomical representation of large WM tracts [see reviews (24, 29, 30)]. Better depiction of WM structures is particularly important for complex tracts such as the CST and corpus callosum, where crossing fibers of these two tracts at the centrum semiovale affects the diffusion measures within those voxels (22). FD may therefore be suitable for detecting changes in WM integrity of the CST. This is supported by our identification of a correlation between increased motor function and increased FD of the CST, which were weaker with FA and MD readouts (Figure 1). Furthermore, compared to FA, FD was recently shown to be more sensitive to detect microstructural changes of large WM tracts over a 6 months period in patients with amyotrophic lateral sclerosis (31), alongside WM alterations in patients with chronic schizophrenia (31). In patients with amyotrophic lateral sclerosis, whilst FA remain unchanged, decreases of FD was also observed in the CST, CC, and TR, alongside longitudinal decreases of FD in the CST, TR, corpus callosum, arcuate fasciculus, inferior and superior longitudinal fasciculus and uncinated fasciculus in the left hemisphere (31). In addition, a negative relationship between FD of the TR and higher positive symptoms was observed in patients with schizophrenia, indicating a relationship between clinical characteristics and WM integrity of core structures involved with information processing (45).
SCI patients with better motor function showed greater integrity of the CST with FD showing the strongest correlation compared to FA and MD (Figure 1). Although our ROC analysis was able to differentiate SCI patients and HC based on FD of the TR (Supplementary Table 1), we cannot conclude whether FD provides substantial value in characterizing WM changes as we primarily observed significant group differences of FA in our paraplegic cohort.
In this study, results were based off a relatively small number of patients (n = 20) and HC (n = 19). This may have decreased statistical power as we did not observe any microstructural changes between the SCI group and HC with whole-brain TBSS analysis. However, no changes in FA or MD have been previously observed in a cohort of sensorimotor complete paraplegics (n = 20) (46) and a group of acute patients (n = 15) with a heterogeneous SCI (level and severity of injury) (47) compared to HC. It is therefore feasible that widespread WM alterations in our particular cohort is not observable with a whole-brain approach. Nonetheless, with a ROIs approach we observed microstructural changes in sensorimotor WM pathways as observed in prior studies.
Future studies are needed to corroborate the validity of FD to identify WM changes following SCI. These studies may benefit by including larger cohorts and subgroups of patients, i.e., paraplegics and tetraplegics with varying severity. Studies that aim to: track neural plastic markers following rehabilitation training and/or therapeutic interventions, or to investigate WM integrity in neurodegenerative diseases, may benefit from utilizing FD to overcome certain limitations of classical DTI readouts. In general, both clinical and animal longitudinal studies are needed to determine whether microstructural abnormalities of cerebral WM coincide with the sequelae of SCI.
This is the first study to examine a novel diffusion marker (FD) in an SCI cohort. Although our ROC analysis was able to differentiate SCI patients and HC with FD of the TR, significant group differences could only be identified with classical DTI readouts. Importantly, greater microstructural integrity of the CST, as characterized by FD, correlated slightly stronger to the motor function in patients with SCI compared to FA and MD, making FD a potential complementary marker to the classical DTI readouts.
The datasets used and analyzed during the current study will be made available by the corresponding author upon reasonable request.
The studies involving human participants were reviewed and approved by Kantonale Ethikkommission Zürich, KEK. The patients/participants provided their written informed consent to participate in this study.
LM, MH, and VH designed the study and drafted the manuscripts. PS provided major technical contributions to the preprocessing of diffusion datasets. All authors read and revised drafts of manuscripts and approved the final version.
This project was funded by the Swiss National Science Foundation (320030_169250) and the Clinical Research Priority Program of the University of Zurich (CRPP Pain).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.598336/full#supplementary-material
1. Ahuja CS, Wilson JR, Nori S, Kotter MRN, Druschel C, Curt A, et al. Traumatic spinal cord injury. Nat Rev Dis Prim. (2017) 3:17018. doi: 10.1038/nrdp.2017.18
2. Alizadeh A, Dyck SM, Karimi-Abdolrezaee S. Traumatic spinal cord injury: an overview of pathophysiology, models and acute injury mechanisms. Front Neurol. (2019) 10:282. doi: 10.3389/fneur.2019.00282
3. Freund P, Weiskopf N, Ashburner J, Wolf K, Sutter R, Altmann DR, et al. MRI investigation of the sensorimotor cortex and the corticospinal tract after acute spinal cord injury: a prospective longitudinal study. Lancet Neurol. (2013) 12:873–81. doi: 10.1016/S1474-4422(13)70146-7
4. Freund P, Seif M, Weiskopf N, Friston K, Fehlings MG, Thompson AJ, et al. MRI in traumatic spinal cord injury: from clinical assessment to neuroimaging biomarkers. Lancet Neurol. (2019) 18:1123–35. doi: 10.1016/S1474-4422(19)30138-3
5. Grabher P, Callaghan MF, Ashburner J, Weiskopf N, Thompson AJ, Curt A, et al. Tracking sensory system atrophy and outcome prediction in spinal cord injury. Ann Neurol. (2015) 78:751–61. doi: 10.1002/ana.24508
6. Wrigley PJ, Press SR, Gustin SM, Macefield VG, Gandevia SC, Cousins MJ. Neuropathic pain and primary somatosensory cortex reorganization following spinal cord injury. Pain. (2009) 141:52–9. doi: 10.1016/j.pain.2008.10.007
7. Jutzeler CR, Huber E, Callaghan MF, Luechinger R, Curt A, Kramer JLK, et al. Association of pain and CNS structural changes after spinal cord injury. Sci Rep. (2016) 6:18534. doi: 10.1038/srep18534
8. Wrigley PJ, Gustin SM, Macey PM, Nash PG, Gandevia SC, Macefield VG, et al. Anatomical changes in human motor cortex and motor pathways following complete thoracic spinal cord injury. Cereb Cortex. (2009) 19:224–32. doi: 10.1093/cercor/bhn072
9. Guleria S, Gupta RK, Saksena S, Chandra A, Srivastava RN, Husain M, et al. Retrograde Wallerian degeneration of cranial corticospinal tracts in cervical spinal cord injury patients using diffusion tensor imaging. J Neurosci Res. (2008) 86:2271–80. doi: 10.1002/jnr.21664
10. Koskinen EA, Hakulinen U, Brander AE, Luoto TM, Ylinen A, Öhman JE. Clinical correlates of cerebral diffusion tensor imaging findings in chronic traumatic spinal cord injury. Spinal Cord. (2014) 52:202–8. doi: 10.1038/sc.2013.163
11. Hou J, Xiang Z, Yan R, Zhao M, Wu Y, Zhong J, et al. Motor recovery at 6 months after admission is related to structural and functional reorganization of the spine and brain in patients with spinal cord injury. Hum Brain Mapp. (2016) 37:2195–209. doi: 10.1002/hbm.23163
12. Zheng W, Chen Q, Chen X, Wan L, Qin W, Qi Z, et al. Brain white matter impairment in patients with spinal cord injury. Neural Plast. (2017) 2017:1–8. doi: 10.1155/2017/4671607
13. Guo Y, Gao F, Liu Y, Guo H, Yu W, Chen Z, et al. White matter microstructure alterations in patients with spinal cord injury assessed by diffusion tensor imaging. Front Hum Neurosci. (2019) 13:11. doi: 10.3389/fnhum.2019.00011
14. Freund P, Schneider T, Nagy Z, Hutton C, Weiskopf N, Friston K, et al. Degeneration of the injured cervical cord is associated with remote changes in corticospinal tract integrity and upper limb impairment. PLoS ONE. (2012) 7:e51729. doi: 10.1371/journal.pone.0051729
15. Johansen-Berg H, Behrens TEJ. Diffusion MRI: From Quantitative Measurement to in-vivo Neuroanatomy. Oxford: Academic Press (2009) 607–14. doi: 10.1016/B978-0-12-374709-9.00002-X
16. Soares JM, Marques P, Alves V, Sousa N. A hitchhiker's guide to diffusion tensor imaging. Front Neurosci. (2013) 7:31. doi: 10.3389/fnins.2013.00031
17. Pierpaoli C, Jezzard P, Basser PJ, Barnett A, Di Chiro G. Diffusion tensor MR imaging of the human brain. Radiology. (1996) 201:637–48. doi: 10.1148/radiology.201.3.8939209
18. Pierpaoli C, Barnett A, Pajevic S, Chen R, Penix L, Virta A, et al. Water diffusion changes in wallerian degeneration and their dependence on white matter architecture. Neuroimage. (2001) 13:1174–85. doi: 10.1006/nimg.2001.0765
19. Ilvesmäki T, Koskinen E, Brander A, Luoto T, Öhman J, Eskola H. Spinal cord injury induces widespread chronic changes in cerebral white matter. Hum Brain Mapp. (2017) 38:3637–47. doi: 10.1002/hbm.23619
20. Freund P, Wheeler-Kingshott CA, Nagy Z, Gorgoraptis N, Weiskopf N, Friston K, et al. Axonal integrity predicts cortical reorganisation following cervical injury. J Neurol Neurosurg Psychiatry. (2012) 83:629–37. doi: 10.1136/jnnp-2011-301875
21. Jeurissen B, Leemans A, Tournier JD, Jones DK, Sijbers J. Investigating the prevalence of complex fiber configurations in white matter tissue with diffusion magnetic resonance imaging. Hum Brain Mapp. (2013) 34:2747–66. doi: 10.1002/hbm.22099
22. Dell'Acqua F, Tournier JD. Modelling white matter with spherical deconvolution: How and why? NMR Biomed. (2019) 32:e3945. doi: 10.1002/nbm.3945
23. Smith RE, Tournier JD, Calamante F, Connelly A. Anatomically-constrained tractography: Improved diffusion MRI streamlines tractography through effective use of anatomical information. Neuroimage. (2012) 62:1924–38. doi: 10.1016/j.neuroimage.2012.06.005
24. Panagiotaki E, Schneider T, Siow B, Hall MG, Lythgoe MF, Alexander DC. Compartment models of the diffusion MR signal in brain white matter: A taxonomy and comparison. Neuroimage. (2012) 59:2241–54. doi: 10.1016/j.neuroimage.2011.09.081
25. Daducci A, Dal Palù A, Lemkaddem A, Thiran JP. COMMIT: Convex optimization modeling for microstructure informed tractography. IEEE Trans Med Imaging. (2015) 34:246–57. doi: 10.1109/TMI.2014.2352414
26. Calamante F, Smith RE, Tournier JD, Raffelt D, Connelly A. Quantification of voxel-wise total fibre density: Investigating the problems associated with track-count mapping. Neuroimage. (2015) 117:284–93. doi: 10.1016/j.neuroimage.2015.05.070
27. Raffelt DA, Tournier JD, Smith RE, Vaughan DN, Jackson G, Ridgway GR, et al. Investigating white matter fibre density and morphology using fixel-based analysis. Neuroimage. (2017) 144:58–73. doi: 10.1016/j.neuroimage.2016.09.029
28. Smith RE, Tournier JD, Calamante F, Connelly A. SIFT2: Enabling dense quantitative assessment of brain white matter connectivity using streamlines tractography. Neuroimage. (2015) 119:338–51. doi: 10.1016/j.neuroimage.2015.06.092
29. Jones DK. Challenges and limitations of quantifying brain connectivity in vivo with diffusion MRI. Imaging Med. (2010) 2:341–55. doi: 10.2217/iim.10.21
30. Winston GP. The physical biological basis of quantitative parameters derived from diffusion MRI. Q Imaging Med Surg. (2012) 2:254–65. doi: 10.3978/j.issn.2223-4292.2012.12.05
31. Stämpfli P, Sommer S, Czell D, Kozerke S, Neuwirth C, Weber M, et al. Investigation of neurodegenerative processes in amyotrophic lateral sclerosis using white matter fiber density. Clin Neuroradiol. (2019) 29:493–503. doi: 10.1007/s00062-018-0670-8
32. Kirshblum S, Biering-Sørensen F, Betz R, Burns S, Donovan W, Graves D, et al. International standards for neurological classification of spinal cord injury: cases with classification challenges. Top Spinal Cord Inj Rehabil. (2014) 20:81–9. doi: 10.1310/sci2002-81
33. Kirshblum S, Waring W. Updates for the international standards for neurological classification of Spinal Cord Injury. Phys Med Rehabil Clin N Am. (2014) 25:505–17. doi: 10.1016/j.pmr.2014.04.001
34. Smith SM. Fast robust automated brain extraction. Hum Brain Mapp. (2002) 17:143–55. doi: 10.1002/hbm.10062
35. Jenkinson M, Beckmann CF, Behrens TE, Woolrich MW, Smith SM. FSL 1. Neuroimage. (2012) 62:782–90. doi: 10.1016/j.neuroimage.2011.09.015
36. Andersson JLR, Sotiropoulos SN. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage. (2016) 125:1063–78. doi: 10.1016/j.neuroimage.2015.10.019
37. Tournier JD, Calamante F, Connelly A. MRtrix: diffusion tractography in crossing fiber regions. Int J Imaging Syst Technol. (2012) 22:53–66. doi: 10.1002/ima.22005
38. Sommer S, Kozerke S, Seifritz E, Staempfli P. Fiber up-sampling and quality assessment of tractograms – towards quantitative brain connectivity. Brain Behav. (2017) 7:e00588. doi: 10.1002/brb3.588
39. Smith SM, Jenkinson M, Johansen-Berg H, Rueckert D, Nichols TE, Mackay CE, et al. Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. Neuroimage. (2006) 31:1487–5052. doi: 10.1016/j.neuroimage.2006.02.024
40. Hua K, Zhang J, Wakana S, Jiang H, Li X, Reich DS, et al. Tract probability maps in stereotaxic spaces: analyses of white matter anatomy and tract-specific quantification. Neuroimage. (2008) 39:336–47. doi: 10.1016/j.neuroimage.2007.07.053
41. Alexander AL, Lee JE, Lazar M, Field AS. Diffusion tensor imaging of the brain. Neurotherapeutics. (2007) 4:316–29. doi: 10.1016/j.nurt.2007.05.011
42. Lerner A, Mogensen MA, Kim PE, Shiroishi MS, Hwang DH, Law M. Clinical applications of diffusion tensor imaging. World Neurosurg. (2014) 82:96–109. doi: 10.1016/j.wneu.2013.07.083
43. Tae WS, Ham BJ, Pyun SB, Kang SH, Kim BJ. Current clinical applications of diffusion-tensor imaging in neurological disorders. J Clin Neurol. (2018) 14:129–40. doi: 10.3988/jcn.2018.14.2.129
44. David G, Mohammadi S, Martin AR, Cohen-Adad J, Weiskopf N, Thompson A, et al. Traumatic and nontraumatic spinal cord injury: pathological insights from neuroimaging. Nat Rev Neurol. (2019) 15:718–31. doi: 10.1038/s41582-019-0270-5
45. Stämpfli P, Sommer S, Manoliu A, Burrer A, Schmidt A, Herdener M, et al. Subtle white matter alterations in schizophrenia identified with a new measure of fiber density. Sci Rep. (2019) 9:4636. doi: 10.1038/s41598-019-40070-2
46. Henderson LA, Gustin SM, Macey PM, Wrigley PJ, Siddall PJ. Functional reorganization of the brain in humans following spinal cord injury: evidence for underlying changes in cortical anatomy. J Neurosci. (2011) 31:2630–7. doi: 10.1523/JNEUROSCI.2717-10.2011
Keywords: spinal cord injury, diffusion weighted imaging, diffusion tensor imaging, fiber density, white matter pathways, sensorimotor function
Citation: Huynh V, Staempfli P, Luetolf R, Luechinger R, Curt A, Kollias S, Hubli M and Michels L (2021) Investigation of Cerebral White Matter Changes After Spinal Cord Injury With a Measure of Fiber Density. Front. Neurol. 12:598336. doi: 10.3389/fneur.2021.598336
Received: 26 August 2020; Accepted: 18 January 2021;
Published: 22 February 2021.
Edited by:
Volker Rasche, University of Ulm, GermanyReviewed by:
Ludovica Griffanti, University of Oxford, United KingdomCopyright © 2021 Huynh, Staempfli, Luetolf, Luechinger, Curt, Kollias, Hubli and Michels. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vincent Huynh, dmluY2VudC5odXluaEB1emguY2g=; dmluY2VudC5odXluaEBiYWxncmlzdC5jaA==
†These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.