 Carla Piano1
Carla Piano1 Francesco Bove1,2*
Francesco Bove1,2* Tommaso Tufo3
Tommaso Tufo3 Isabella Imbimbo1,4Danilo Genovese1,2
Isabella Imbimbo1,4Danilo Genovese1,2 Alessandro Stefani5
Alessandro Stefani5 Massimo Marano6
Massimo Marano6 Antonella Peppe7Livia Brusa8
Antonella Peppe7Livia Brusa8 Rocco Cerroni5
Rocco Cerroni5 Francesco Motolese6
Francesco Motolese6 Enrico Di Stasio9,10
Enrico Di Stasio9,10 Marianna Mazza11
Marianna Mazza11 Antonio Daniele1,2Alessandro Olivi2,3
Antonio Daniele1,2Alessandro Olivi2,3 Paolo Calabresi1,2Anna Rita Bentivoglio1,2 and Lazio DBS Study Group
Paolo Calabresi1,2Anna Rita Bentivoglio1,2 and Lazio DBS Study Group- 1Neurology Unit, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
- 2Department of Neurosciences, Università Cattolica del Sacro Cuore, Rome, Italy
- 3Neurosurgery Unit, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
- 4Fondazione Don Carlo Gnocchi Onlus, Milan, Italy
- 5Department of System Medicine, Unità Operativa Semplice Dipartimentale (UOSD) Parkinson, University of Rome Tor Vergata, Rome, Italy
- 6Neurology, Neurophysiology and Neurobiology Unit, Department of Medicine, Università Campus Bio-Medico di Roma, Rome, Italy
- 7IRCCS Santa Lucia Foundation, Rome, Italy
- 8Neurology Unit, S. Eugenio Hospital, Rome, Italy
- 9Unit of Chemistry, Biochemistry and Clinical Molecular Biology, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
- 10Institute of Biochemistry and Clinical Biochemistry, Università Cattolica del Sacro Cuore, Rome, Italy
- 11Department of Geriatrics, Neuroscience and Orthopedics, Institute of Psychiatry and Psychology, Fondazione Policlinico Universitario A. Gemelli IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy
Background: The containment measures taken by Italian government authorities during the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic caused the interruption of neurological activities of outpatient clinics. Vulnerable patients, as Parkinson's disease (PD) and dystonic patients with deep brain stimulation (DBS), may have an increased risk of chronic stress related to social restriction measures and may show a potential worsening of motor and psychiatric symptoms.
Methods: This cross-sectional multicenter study was carried out during the SARS-CoV-2 pandemic and was based on a structured survey administered during a telephone call. The questionnaire was designed to gather motor and/or psychiatric effects of the lockdown and coronavirus disease 2019 (COVID-19) epidemiologic information in PD and dystonic patients with a functioning DBS implant.
Results: One hundred four patients were included in the study, 90 affected by PD and 14 by dystonia. Forty-nine patients reported a subjective perception of worsening of global neurological symptoms (motor and/or psychiatric) related to the containment measures. In the multivariate analysis, having problems with the DBS device was the only independent predictor of motor worsening [odds ratio (OR) = 3.10 (1.22–7.91), p = 0.018]. Independent predictors of psychiatric worsening were instrumental activities of daily living (IADL) score [OR = 0.78 (0.64–0.95), p = 0.012] and problems with DBS [OR = 5.69 (1.95–16.62), p = 0.001]. Only one patient underwent nasopharyngeal swabs, both negative, and no patient received a diagnosis of COVID-19.
Conclusions: Lockdown restriction measures were associated with subjective worsening of motor and psychiatric symptoms in PD and dystonic patients treated with DBS, and they may have exacerbated the burden of neurological disease and increased the chronic stress related to the DBS management.
Introduction
In early 2020, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection has spread worldwide, becoming a pandemic. Coronavirus disease 2019 (COVID-19) commonly presents with fever, cough, and dyspnea; the most severe complication of the infection is the acute respiratory distress syndrome (1). Many government authorities took emergency containment measures to reduce viral transmission (2). In Italy, according to Prime Minister Decree of March 11, 2020, the containment measures recommended a reduction of routine hospital activities: activities of outpatient clinics were stopped, and admittance of patients affected by neurological disorders was allowed only for emergency conditions. Elderly individuals with preexisting comorbidities, including movement disorders, are fragile patients due to their higher risk of infections and poor outcome of disease management (3). Deep brain stimulation (DBS) is a well-established second-level treatment for patients with severe Parkinson's disease (PD) and dystonia who show poor response to pharmacological treatment (4). These patients are routinely monitored with close follow-up, given the need for periodic adjustments of stimulation parameters to optimize motor control and for periodic checks of implantable pulse generator (IPG) functionality and battery status in order to reduce the risk of device-related complications (5, 6). In addition, PD and dystonic patients treated with DBS often need a close follow-up of possible psychiatric symptoms (depression, anxiety, apathy, impulse control disorders, psychosis, disorders of sleep, and wakefulness) (7). For the aforementioned reasons, patients with movement disorders are exposed to an increased risk of chronic stress related to social restriction measures and may show a potential worsening of motor and psychiatric symptoms (8–10). Aim of the present study was to analyze the effects of the lockdown on this vulnerable category of patients affected by PD and dystonia treated with DBS and, secondarily, to investigate the prevalence of COVID-19 suggestive symptoms in this population.
Patients and Methods
This cross-sectional multicenter study was carried out during the SARS-CoV-2 pandemic and was promoted by the Neurology Clinic of the Fondazione Policlinico Universitario A. Gemelli IRCCS in Rome (Italy), in collaboration with other neurology clinics based in Lazio region with good expertise on the management of DBS for movement disorders.
Study Population
Inclusion Criteria
PD and dystonic patients who received a DBS implant, which was functioning during the COVID-19 lockdown, and followed in the DBS centers of Lazio region were asked to participate in a telephone survey. Patients were included regardless of the DBS target, the hospital, and the year in which implantation of the neurostimulator was carried out.
Exclusion Criteria
Patients were excluded if they were unable to provide informed and valid consent at the time of the interview, if they show cognitive decline, and if they did not speak Italian fluently.
Survey Design and Testing
The study was based on a structured survey administered during a telephone call carried out as part of the close follow-up scheduled for the included patients. Surveys started on April 28, 2020, and ended on May 12, 2020. A questionnaire was employed, aimed at gathering the following data:
- demographic and clinical data related to PD and dystonia (age, sex, age at disease onset, disease duration, presence of psychiatric symptoms prior to the lockdown, preexisting hyposmia, PD phenotype, current treatment of the neurological disorder)
- information about DBS (target, years from the DBS surgery)
- assumption of medications potentially interfering with SARS-CoV-2 infection
- concomitant diseases and disability measures [activities of daily living (ADL) and instrumental activities of daily living (IADL) scales (11, 12), Hoehn and Yahr (H&Y) scale for PD patients (13), Clinical Global Impression (CGI) Severity scale (14)]
- COVID-19-related questions [including a history of COVID-19-suggestive symptoms in the last 4 months (fever, cough, dyspnea, diarrhea, abdominal pain, pharyngodynia, worsening of hyposmia, hearing loss) and additional information related to SARS-CoV-2 pandemic (testing by nasopharyngeal swabs, COVID-19 diagnosis, contact with COVID-19+ subjects, presence in endemic areas for COVID-19, presence in residential care home, respect of social restriction measures according to Prime Minister Decree of March 11, 2020, flu vaccination)]
- effects of the lockdown (all of the following were yes/no answer questions) [discontinuation of outpatient neurological visits or physiotherapy (motor physical therapy), difficulties in finding medications, need of urgent outpatient neurological visit, difficulties in the management of the DBS device (rechargeable systems and/or patients with handheld controller to turn the DBS system on and off), feeling of insecurity about the DBS device, worsening of the relationship with own body, subjective perception of worsening of global neurological symptoms (motor and/or psychiatric), sleep disorders, depression, panic attacks, persecutory delusions, visual hallucinations, suicidal ideation, impulsive–compulsive behaviors, increased consumption of coffee and tea]
- changes on CGI Improvement scale (14) related to the lockdown period
For patients who complained one or both “difficulties in the management of the DBS device” and “feeling of insecurity about the DBS device,” the cumulative variable “problems with the DBS device” was considered.
The variables related to the effects of the lockdown were assessed to detect emergent symptoms and/or changes of preexisting symptoms after March 11, 2020.
Statistical Analysis
All statistical analyses were carried out using the Statistical Package for Social Science (SPSS) program, version 25.0 (IBM Co., Armonk, NY). Data were analyzed for normality of distribution using the Kolmogorov–Smirnov test of normality and were expressed as mean [±standard deviation (SD)] for continuous variables or as frequencies (n, %) for categorical variables according to a neurological diagnosis. The Mann–Whitney rank sum test was used to compare continuous variables between diagnostic subgroups (PD and dystonia) and between patients with or without subjective perception of worsening of neurological symptoms. The χ2 test or Fisher's exact test was used for categorical variables. Phi coefficients were calculated to estimate correlation strengths between motor/psychiatric worsening and the other binomial variables evaluating the effects of the lockdown. Finally, multivariate binary logistic analysis was performed to evaluate the relationship between the worsening of motor or psychiatric symptoms and clinical findings. The coefficients obtained from the logistic regression were expressed in terms of odds ratio (OR) with 95% confidence intervals. All statistical tests were two-tailed; statistical significance was defined as p value < 0.05, and the effect size was also reported.
Standard Protocol Approvals, Registration, and Patient Consent
The study and the survey questions were reviewed and approved by local ethical committee. Because of the biological risks related to the pandemic, after receiving a copy of written informed consent by mail or fax, patients were asked to carefully read, sign, and send it by mail or fax to the referral hospital.
Data Availability
Anonymized data will be shared with qualified external researchers after approval of their requests.
Results
One hundred four patients treated with DBS were asked to participate in the survey. Since all agreed to participate, met the inclusion criteria, and no one had exclusion criteria, all 104 patients were included in the study. Ninety patients were affected by PD and 14 patients by dystonia (including 10 patients with idiopathic dystonia and four patients with secondary dystonia). In the total sample, the male/female ratio was 64/40, the mean age was 61 years (SD ±12), and the mean disease duration was 19 years (SD ±8). All dystonic patients underwent globus pallidus internus (GPi) DBS, while the DBS target was different among PD patients: 85 patients were implanted in the subthalamic nucleus (STN), three patients in the GPi, and two patients in the thalamic ventral intermediate nucleus (Vim).
For each diagnostic group, demographic and disease clinical data, disability scales, concomitant medical conditions, and neurological medications are reported in Table 1. When the subgroups of PD and dystonic patients were compared for demographic and disease clinical features, significant differences were found for age (62 ± 10 vs. 53 ± 16 years, p = 0.038, effect size = 0.82–large), age at disease onset (44 ± 9 vs. 29 ± 19 years, p = 0.007, effect size = 1.39–large), disease duration (18 ± 7 vs. 24 ± 10 years, p = 0.020, effect size = 0.81–large), scores on ADL (4.8 ± 1.8 vs. 5.9 ± 0.5, p = 0.012, effect size = 0.65–medium), IADL (4.4 ± 3.0 vs. 7.1 ± 2.1, p = 0.001, effect size = 0.93–large), and CGI Severity scale (4.0 ± 1.3 vs. 2.9 ± 1.6, p = 0.016, effect size = 0.82–large).
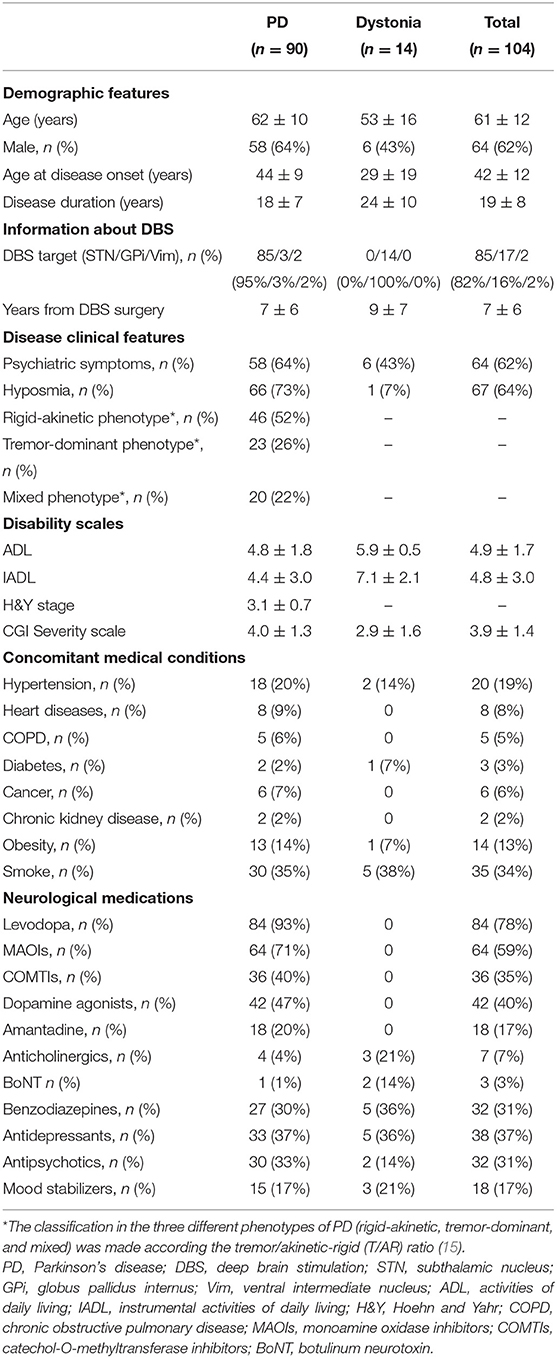
Table 1. Demographic and disease clinical data, disability scales, concomitant medical conditions, and specific neurological medications for each diagnostic group.
Coronavirus Disease 2019-Related Questions
Distribution of symptoms suggestive of COVID-19 in the last 4 months, epidemiologic data, and medications potentially interfering with the SARS-CoV-2 infection are reported in Table 2. Twenty-six patients reported one or more symptoms suggestive of COVID-19, while only five of them referred three or more of these symptoms. The most frequent symptom was cough, reported by 17 patients. Only one patient underwent (twice) nasopharyngeal swabs, both negative, and no patient received a diagnosis of COVID-19. In our sample, there was no correlation between symptoms suggestive of SARS-CoV-2 infection and assumption of angiotensin-converting enzyme (ACE) inhibitors, nonsteroidal anti-inflammatory drugs (NSAIDs), or immunosuppressant therapy.
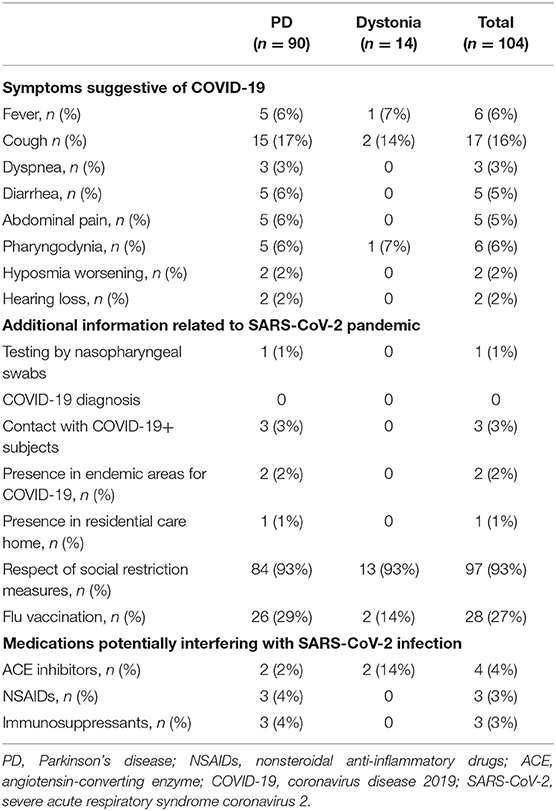
Table 2. Symptoms suggestive of COVID-19 in the last 4 months, epidemiologic data, and medications potentially interfering with SARS-CoV-2 infection for each diagnostic group.
No significant differences were found between the two diagnostic subgroups (PD and dystonia) as to COVID-19-suggestive symptoms or additional information related to SARS-CoV-2 pandemic.
Effects of the Lockdown on Disease Burden
Information related to the impact of the lockdown on disease burden is reported in Table 3. Forty-nine patients out of 104 (47%) reported a subjective perception of worsening of global neurological symptoms related to the containment measures: 20 patients (19%) reported a worsening of motor symptoms; five patients (5%), a worsening of psychiatric symptoms; 24 patients (23%), a worsening of both motor and psychiatric symptoms. The overall worsening of the health status was also confirmed by the mean score on the CGI Improvement scale (4.6 ± 1.3). Ninety-two patients (88%) lost the scheduled follow-up visit, 60 (58%) discontinued physiotherapy, and 18 (17%) needed urgent outpatient neurological visit. Eighteen patients (17%) reported difficulties in the management of the DBS device, 26 (25%) reported feeling of insecurity about the DBS device, while 28 (27%) reported a worsening in the relationship with their own body as compared to the period immediately preceding the lockdown. Thirty-four patients (33%) complained of sleep disorders, 39 (37%) depression, 13 (12%) panic attacks, nine (9%) persecutory delusions, 13 (12%) visual hallucinations, and eight (8%) suicidal ideation. Moreover, 21 patients (20%) reported impulsive–compulsive behaviors as increase of shopping online, video game playing, and punding. Thirty-five patients (34%) reported an increased coffee and tea consumption. Among the 21 patients who complained worsening of impulsive–compulsive behaviors, 10 were on treatment with dopamine agonists. The proportion of patients on treatment with dopamine agonists was not significantly higher in the subgroup with worsening of impulsive–compulsive behaviors than in the other subgroup of patients (48 vs. 39%, respectively, p = 0.6).
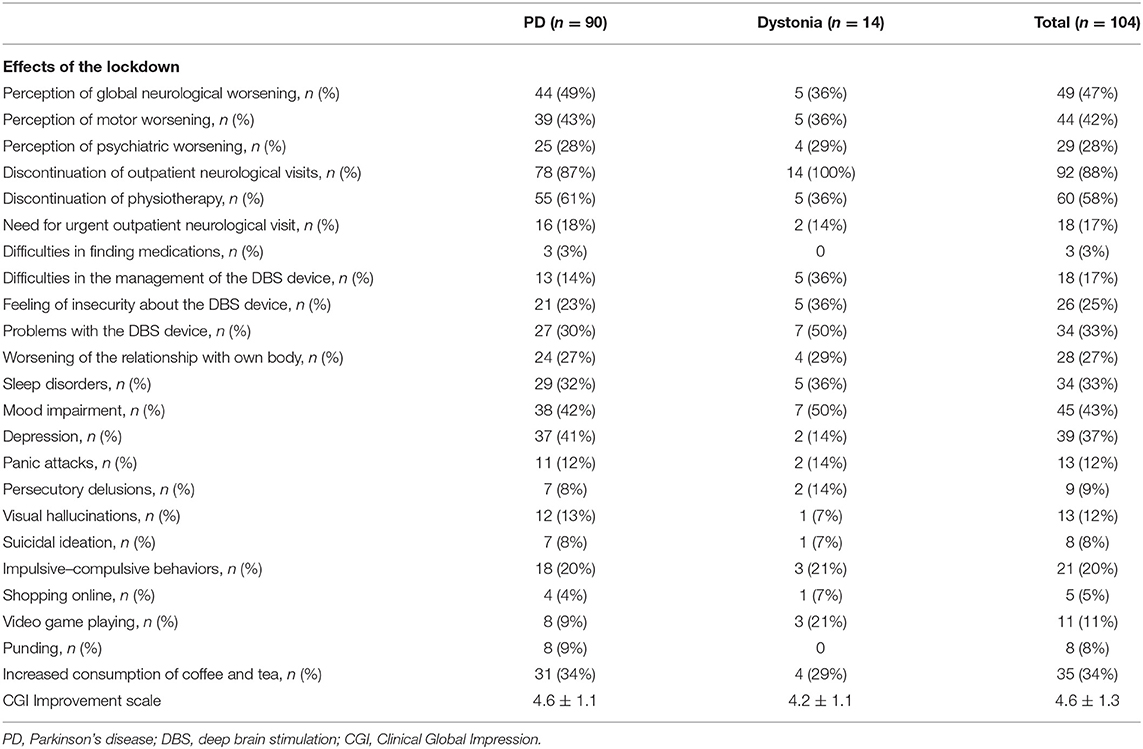
Table 3. Effects of the lockdown on disease burden for each diagnostic group.
No significant differences were found between the two diagnostic subgroups (PD vs. dystonic patients) as to the effects of the lockdown.
Considering the subgroup of 26 patients reporting one or more symptoms suggestive of COVID-19 and comparing this one with the subgroup of patients without symptoms suggestive of COVID-19, no significant differences were found in worsening of motor or psychiatric symptoms.
Significant correlations were found between motor worsening and discontinuation of physiotherapy (phi coefficient = 0.22, p = 0.024, effect size = 0.45–small) and between worsening of psychiatric symptoms and chronic benzodiazepine intake (phi coefficient = 0.28, p = 0.004, effect size = 0.59–medium). Significant correlations were also observed between both motor and psychiatric worsening and need for urgent outpatient neurological visit (phi coefficient = 0.38, p < 0.001, effect size = 1.06–large and phi coefficient = 0.40, p < 0.001, effect size = 0.99–large, respectively), difficulties in the management of the DBS device (phi coefficient = 0.23, p = 0.021, effect size = 0.60–medium and phi coefficient = 0.23, p = 0.021, effect size = 0.60–medium, respectively), feeling of insecurity about the DBS device (phi coefficient = 0.27, p = 0.006, effect size = 0.63–medium and phi coefficient = 0.28, p = 0.004, effect size = 0.63–medium, respectively), worsening of the relationship with own body (phi coefficient = 0.45, p < 0.001, effect size = 1.04–large and phi coefficient = 0.40, p < 0.001, effect size = 0.86–large, respectively), sleep disorders (phi coefficient = 0.27, p = 0.005, effect size = 0.59–medium and phi coefficient = 0.44, p < 0.001, effect size = 0.91–large, respectively), depression (phi coefficient = 0.22, p = 0.024, effect size = 0.46–small and phi coefficient = 0.45, p < 0.001, effect size = 0.99–large, respectively).
No difference was found on disability scales between the subgroups of patients with and without worsening of motor symptoms. By contrast, the subgroup with worsening of psychiatric symptoms, as compared to the subgroup without psychiatric worsening, presented significantly lower scores on IADL (3.7 ± 3.0 vs. 5.2 ± 2.9, p = 0.0436, effect size = 0.50–small) and higher scores on CGI Severity scale (4.5 ± 1.0 vs. 3.7 ± 1.4, p = 0.0081, effect size = 0.71–medium).
In the reduced models of multivariate logistic regression analysis, having problems with the DBS device (difficulties in the management of the DBS device or feeling of insecurity about the DBS device) was the only independent predictor of motor worsening [OR = 3.10 (1.22–7.91), p = 0.018]. Independent predictors of psychiatric worsening were IADL score [OR = 0.78 (0.64–0.95), p = 0.012] and problems with DBS [OR = 5.69 (1.95–16.62), p = 0.001]. Other variables included in the models were age, sex, diagnosis (PD or dystonia), and disease duration (Table 4).
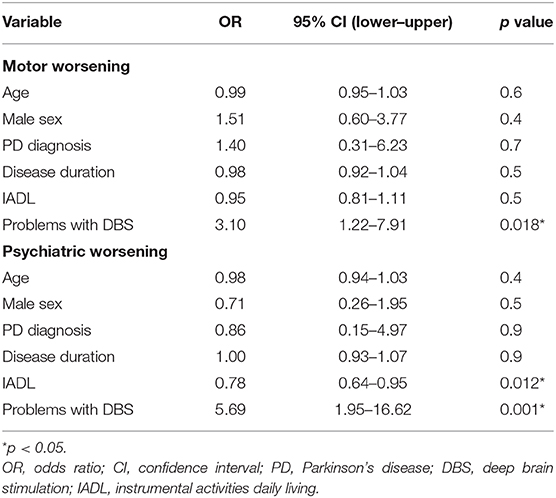
Table 4. Multivariate logistic regression models of factors predicting motor and psychiatric worsening during the lockdown.
Discussion
The study, based on a telephone survey administered by neurologists of the DBS movement disorders network in Lazio region, attempted to investigate the consequences of the COVID-19 lockdown on the perception of neurological status (motor and psychiatric symptoms) in patients affected by PD and dystonia treated with DBS.
The demographic and clinical characteristics between the two diagnostic subgroups differed significantly: as compared to PD patients, dystonic patients showed an earlier age at onset, a longer disease duration, and a milder disability.
Although patients with neurological disorders, especially in late disease stages, might be particularly at risk for COVID-19 complications (16–18), in our sample, only ¼ of patients reported symptoms suggestive of SARS-CoV-2 infection. One patient underwent nasopharyngeal swabs, and none received a diagnosis of COVID-19. No patient with symptoms suggestive of COVID-19 needed specific treatments, hospitalization, or respiratory assistance.
Half of the patients in our sample reported a subjective perception of global neurological worsening, which required urgent outpatient neurological visit in 18 cases. A mean CGI Improvement score >4 after the lockdown period confirmed these data. In most patients, worsening of health status seemed to result from discontinuation of neurological visits and physiotherapy, as reported for patients with chronic neurological diseases (19, 20). A significant number of patients presented a worsening of sleep quality, mood, and behavioral disturbances, including onset or worsening of impulsive–compulsive behaviors. As well as worsening of impulsive–compulsive behaviors was not related to treatment with dopamine agonists, it may be a consequence of restriction measures more than an adverse effect induced by dopamine agonists. Indeed, 13 patients reported visual hallucinations during the weeks of social isolation probably induced by a home “hospitalization” phenomenon (21) and exacerbated by sleep disturbances (22).
No significant differences were found between the two diagnostic subgroups (PD vs. dystonic patients) as to the effects of the lockdown. Furthermore, in the multivariate analysis, the specific neurological disease was not an independent predictor of motor or psychiatric worsening during the lockdown.
No significant differences were found in worsening of motor or psychiatric symptoms comparing the subgroup of patients with and without symptoms suggestive of COVID-19.
Significant correlations were found between the subjective perception of motor worsening and discontinuation of physiotherapy treatment, although with a small effect size, and between worsening of psychiatric symptoms and chronic intake of benzodiazepines, with a medium effect size. These findings point out the beneficial effects of physiotherapy in patients with movement disorders and the importance of strategies focused on remote rehabilitation treatment (23). Indeed, a closer psychiatric follow-up would be recommended for patients with chronic use of benzodiazepines, who have an increased risk of developing depressive symptoms (24).
In our study, problems with the DBS device (difficulties in the management of the DBS device and feeling of insecurity about the DBS device) were independent predictors of motor and psychiatric worsening. Such difficulties may be chronic stressful factors that induce depression, anxiety, and insomnia (25). Therefore, DBS played an important role in impairing motor and psychiatric symptoms during the lockdown, independently from the underlying neurological disease. Greater disability (lower IADL score) due to the chronic neurological disease was another independent predictor of psychiatric worsening. On the other hand, demographic factors, disease duration, and neurological diagnosis (PD or dystonia) did not contribute to the global worsening during the lockdown.
These findings suggest that the effects of social restriction measures seriously impact on patients with chronic neurological disease and, in particular, in carriers of a DBS stimulator with greater disability. They also highlight the importance of management programs in the post-epidemic phase with the implementation of telemedicine, remote rehabilitation treatment, and technologies for remote DBS monitoring and programming (9, 26, 27).
Limitations
This study has several limits. First, since data collection was carried out by means of telephone contacts and not by a face-to-face assessment, the results of the survey might have been influenced by uncontrolled biases. Second, the effects of the lockdown were only assessed by subjective perception and not by validated scales for motor and psychiatric symptoms because of the lack of specific evaluation just before the lockdown. Furthermore, subjective perception of motor and/or psychiatric worsening may be influenced by depressive mood, which had a high prevalence in our sample and is typical of the pandemic situation. In fact, there is a positive correlation between depression and subjective perception of motor and/or psychiatric worsening, thus the patients might have overestimated the real worsening during the pandemic. Another limitation of the study is the small sample size for dystonic patients. Finally, although the multivariate analysis showed that DBS played an independent role in motor and psychiatric worsening, future comparative studies between carriers and noncarriers of DBS should be made.
Conclusions
Our findings suggest that lockdown restriction measures were associated with subjective worsening of motor and psychiatric symptoms in PD and dystonic patients treated with DBS, and that such measures may have exacerbated the burden of neurological disease and increased the chronic stress related to the DBS management.
Lazio DBS Study Group
Maria Concetta Altavista, Neurology Unit, San Filippo Neri Hospital ASL Roma 1, Roma, Italy
Marco Ciavarro, IRCCS Neuromed, Pozzilli, Italy
Francesca Cortese, Neurology Unit, San Filippo Neri Hospital ASL Roma 1, Roma, Italy
Manuela D'Ercole, Neurosurgery, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
Lazzaro Di Biase, Unit of Neurology, Neurophysiology and Neurobiology, Department of Medicine, Campus Bio-Medico of Rome University, Rome, Italy
Maria Francesca De Pandis, Institute for Research and Medical Care IRCCS San Raffaele Cassino, Cassino, Italy
Daniela Di Giuda, Nuclear Medicine, Fondazione Policlinico Universitario A. Gemelli IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy
Giovanni Fabbrini, Department of Human Neurosciences, Sapienza University of Rome, Italy; IRCCS Neuromed Institute, Pozzilli, Italy
Alessandro Izzo, Neurosurgery, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
Rosa Liperoti, Geriatrics, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
Giuseppe Marano, Institute of Psychiatry and Psychology, Department of Geriatrics, Neuroscience and Orthopedics, Fondazione Policlinico Universitario A. Gemelli IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy
Nicola Modugno, IRCCS Neuromed, Pozzilli, Italy
Michela Orsini, Clinical Psychology, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
Michele Paradiso, Department of Neurology, St John the Baptist Hospital, ACISMOM, Rome, Italy
Mariangela Pierantozzi, Neurology Unit, University Hospital “Tor Vergata”, Rome, Italy; Department of Systems Medicine, University of Rome Tor Vergata, Rome, Italy
Camilla Rocchi, Department of Systems Medicine, University of Rome Tor Vergata, Rome, Italy
Antonio Suppa, Department of Human Neurosciences, Sapienza University of Rome, Italy; IRCCS Neuromed Institute, Pozzilli, Italy
Laura Vacca, University and Institute for Research and Medical Care IRCCS San Raffaele, Rome, Italy
Rita Vadalà, NeuroRadiology, IRCCS Fondazione S Lucia, Rome, Italy
Michela Orsini, Neurology, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy
Fabio Viselli, Department of Neurology, St John the Baptist Hospital, ACISMOM, Rome, Italy.
Data Availability Statement
The original contributions generated in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Fondazione Policlinico Universitario A. Gemelli IRCCS ethics committee. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CP, FB, and ARB designed and conceptualized the study, interpreted the data, and drafted the manuscript. EDS analyzed the data and revised the manuscript for intellectual content. TT, II, DG, AS, MMar, AP, LB, RC, FM, MMaz, AD, AO, PC, and Lazio DBS Study Group collected the data and revised the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. (2020) 180:934–43. doi: 10.1001/jamainternmed.2020.0994
2. Harapan H, Itoh N, Yufika A, Winardi W, Keam S, Te H, et al. Coronavirus disease 2019 (COVID-19): A literature review. J Infect Public Health. (2020) 13:667–73. doi: 10.1016/j.jiph.2020.03.019
3. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. (2013) 381:752–62. doi: 10.1016/S0140-6736(12)62167-9
4. Larson PS. Deep brain stimulation for movement disorders. Neurotherapeutics. (2014) 11:465–74. doi: 10.1007/s13311-014-0274-1
5. Deuschl G, Herzog J, Kleiner-Fisman G, Kubu C, Lozano AM, Lyons KE, et al. Deep brain stimulation: postoperative issues. Mov Disord. (2006) 21 (Suppl. 14):S219–37. doi: 10.1002/mds.20957
6. Holla VV, Neeraja K, Surisetti BK, Prasad S, Kamble N, Srinivas D, et al. Deep brain stimulation battery exhaustion during the COVID-19 pandemic: crisis within a crisis. J Mov Disord. (2020) 13:218–22. doi: 10.14802/jmd.20073
7. Lauterbach EC, Freeman A, Vogel RL. Differential DSM-III psychiatric disorder prevalence profiles in dystonia and Parkinson's disease. J Neuropsychiatry Clin Neurosci. (2004) 16:29–36. doi: 10.1176/jnp.16.1.29
8. Helmich RC, Bloem BR. The impact of the COVID-19 pandemic on Parkinson's disease: hidden sorrows and emerging opportunities. J Parkinsons Dis. (2020) 10:351–4. doi: 10.3233/JPD-202038
9. Bhidayasiri R, Virameteekul S, Kim JM, Pal PK, Chung SJ. COVID-19: an early review of its global impact and considerations for Parkinson's disease patient care. J Mov Disord. (2020) 13:105–14. doi: 10.14802/jmd.20042
10. Salari M, Zali A, Ashrafi F, Etemadifar M, Sharma S, Hajizadeh N, et al. Incidence of anxiety in Parkinson's disease during coronavirus disease (COVID-19) pandemic. Mov Disord. (2020) 35:1095–6. doi: 10.1016/j.yebeh.2020.107442
11. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of Adl: A standardized measure of biological and psychosocial function. JAMA. (1963) 185:914–9. doi: 10.1001/jama.1963.03060120024016
12. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. (1969) 9:179–86. doi: 10.1093/geront/9.3_Part_1.179
13. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology. (1967) 17:427–42. doi: 10.1212/WNL.17.5.427
14. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry. (2007) 4:28–37.
15. Schiess MC, Zheng H, Soukup VM, Bonnen JG, Nauta HJ. Parkinson's disease subtypes: clinical classification and ventricular cerebrospinal fluid analysis. Parkinsonism Relat Disord. (2000) 6:69–76. doi: 10.1016/S1353-8020(99)00051-6
16. Antonini A, Leta V, Teo J, Chaudhuri KR. Outcome of Parkinson's disease patients affected by COVID-19. Mov Disord. (2020) 35:905–8. doi: 10.1002/mds.28104
17. Schirinzi T, Cerroni R, Di Lazzaro G, Liguori C, Scalise S, Bovenzi R, et al. Self-reported needs of patients with Parkinson's disease during COVID-19 emergency in Italy. Neurol Sci. (2020) 41:1373–5. doi: 10.1007/s10072-020-04442-1
18. Fasano A, Cereda E, Barichella M, Cassani E, Ferri V, Zecchinelli AL, et al. COVID-19 in Parkinson's disease patients living in Lombardy, Italy. Mov Disord. (2020) 35:1089–93. doi: 10.1002/mds.28176
19. Piano C, Di Stasio E, Primiano G, Janiri D, Luigetti M, Frisullo G, et al. An Italian neurology outpatient clinic facing SARS-CoV-2 pandemic: data from 2,167 patients. Front Neurol. (2020) 11:564. doi: 10.3389/fneur.2020.00564
20. Prasad S, Holla VV, Neeraja K, Surisetti BK, Kamble N, Yadav R, et al. Impact of prolonged lockdown due to COVID-19 in patients with Parkinson's disease. Neurol India. (2020) 68:792–5. doi: 10.4103/0028-3886.293472
21. Michalska Da Rocha B, Rhodes S, Vasilopoulou E, Hutton P. Loneliness in psychosis: a Meta-analytical review. Schizophr Bull. (2018) 44:114–25. doi: 10.1093/schbul/sbx036
22. Sheaves B, Bebbington PE, Goodwin GM, Harrison PJ, Espie CA, Foster RG, et al. Insomnia and hallucinations in the general population: findings from the 2000 and 2007 British Psychiatric Morbidity Surveys. Psychiatry Res. (2016) 241:141–6. doi: 10.1016/j.psychres.2016.03.055
23. Leocani L, Diserens K, Moccia M, Caltagirone C. Disability through COVID-19 pandemic: neurorehabilitation cannot wait. Eur J Neurol. (2020) 27:e50–1. doi: 10.1111/ene.14320
24. Quello SB, Brady KT, Sonne SC. Mood disorders and substance use disorder: a complex comorbidity. Sci Pract Perspect. (2005) 3:13–21. doi: 10.1151/spp053113
25. Fasano A, Antonini A, Katzenschlager R, Krack P, Odin P, Evans AH, et al. Management of advanced therapies in Parkinson's disease patients in times of humanitarian crisis: The COVID-19 experience. Mov Disord Clin Pract. (2020) 7:361–72. doi: 10.1002/mdc3.12965
26. Miocinovic S, Ostrem JL, Okun MS, Bullinger KL, Riva-Posse P, Gross RE, et al. Recommendations for deep brain stimulation device management during a pandemic. J Parkinsons Dis. (2020) 10:903–10. doi: 10.3233/JPD-202072
Keywords: COVID-19, SARS-CoV-2, deep brain stimulation, Parkinson's disease, dystonia
Citation: Piano C, Bove F, Tufo T, Imbimbo I, Genovese D, Stefani A, Marano M, Peppe A, Brusa L, Cerroni R, Motolese F, Di Stasio E, Mazza M, Daniele A, Olivi A, Calabresi P, Bentivoglio AR and Lazio DBS Study Group (2020) Effects of COVID-19 Lockdown on Movement Disorders Patients With Deep Brain Stimulation: A Multicenter Survey. Front. Neurol. 11:616550. doi: 10.3389/fneur.2020.616550
Received: 12 October 2020; Accepted: 16 November 2020;
Published: 16 December 2020.
Edited by:
Jordi A. Matias-Guiu, Hospital Clínico San Carlos, SpainReviewed by:
Pedro Chana-Cuevas, University of Santiago, ChileMariana H. G. Monje, Centro Integral en Neurociencias A.C. HM CINAC, Spain
Copyright © 2020 Piano, Bove, Tufo, Imbimbo, Genovese, Stefani, Marano, Peppe, Brusa, Cerroni, Motolese, Di Stasio, Mazza, Daniele, Olivi, Calabresi, Bentivoglio and Lazio DBS Study Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Bove, ZnJhbmNlc2NvYm92ZTg2QGdtYWlsLmNvbQ==