
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 21 January 2021
Sec. Endovascular and Interventional Neurology
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.615094
This article is part of the Research Topic Intracranial Atherosclerotic Disease: Epidemiology, Imaging, Treatment and Prognosis View all 17 articles
 Rajbeer S. Sangha1*
Rajbeer S. Sangha1* Shyam Prabhakaran2
Shyam Prabhakaran2 Edward Feldmann3Tristan Honda4Azhar Nizam5George A. Cotsonis5
Edward Feldmann3Tristan Honda4Azhar Nizam5George A. Cotsonis5 Iszet Campo-Bustillo6
Iszet Campo-Bustillo6 Jose G. Romano6
Jose G. Romano6 David S. Liebeskind4 on behalf of the MyRIAD Investigators
David S. Liebeskind4 on behalf of the MyRIAD InvestigatorsIntroduction: While much is known about recurrent clinical events in patients with intracranial atherosclerotic disease (ICAD), there is limited data on characteristics of recurrent infarcts.
Methods: The NIH-funded MyRIAD prospective, observational study was designed to identify mechanisms of ischemia and predictors of recurrence in ICAD. Recurrent infarction was assessed on MRI at 6–8 weeks. We reviewed the DWI/ADC and FLAIR sequences in patients with recurrent stroke and characterized the number of infarcts, infarct location, size, and patterns based on whether they were borderzone (BZ), perforator (SC/P), cortical or territorial (C/T), and mixed. Temporal characteristics were delineated by ADC/FLAIR correlation.
Results: Of the 89 patients with 6–8 weeks MRI, 22 (24.7%) had recurrent infarcts in the territory of the symptomatic artery. Recurrent infarcts were evident on DWI in 63.6% and single infarcts in 54.5%. The median recurrent infarct volume was 2.0 cm3 compared to median index infarct volumes of 2.5 cm3. A mixed infarct pattern was most common (40.9%), followed by borderzone (22.7%), cortical or territorial (27.3%), while only 9.1% were in a perforator artery distribution. Amongst those with a mixed pattern, 8/9 had a borderzone distribution infarct as part of their mixed infarct pattern.
Conclusion: These findings provide novel data on the characteristics of early recurrent infarcts in patients with symptomatic ICAD.
Intracranial atherosclerotic disease (ICAD) is the most common cause of ischemic stroke globally and carries the highest risk of stroke recurrence with an estimated 1 year rate of ~12% despite aggressive medical therapy (1–3). The Mechanisms of Early Recurrence in Intracranial Atherosclerotic Disease (MyRIAD) Study (NIH/NINDS) aimed to determine the mechanisms of ischemic stroke in ICAD using imaging biomarkers and determine the rate of early recurrent infarction (4).
Recurrent infarct characteristics may provide valuable information regarding the mechanisms of ischemic recurrence. Previous studies have investigated the correlations between mechanisms of ischemic stroke and infarct patterns on brain imaging in patients with ICAD (5–7). Analysis of infarct patterns in patients with ICAD have demonstrated a correlation between borderzone infarcts and poor distal perfusion (8). In this secondary analysis of MyRIAD, we aimed to describe recurrent infarct characteristics patients enrolled in MyRIAD.
The MyRIAD study design has been previously described (4). Eligible patients had a recent (<21 days) ischemic stroke or a transient ischemic attack (TIA) caused by ICAD of the intracranial carotid artery, middle cerebral artery M1 segment, basilar artery, or vertebral artery V4 segment, with 50–99% stenosis, in the absence of proximal cervical arterial stenosis >50% or a cardioembolic source. Ischemic stroke required symptoms lasting >24 h with imaging confirmation of an infarct; TIA had either diffusion weighted imaging (DWI) abnormality or two or more stereotypical events with unequivocally ischemic symptoms. The degree of stenosis was calculated by established methods (9) on digital subtraction angiography (n = 23), CT angiography (n = 69) or MR angiography (n = 26); a flow gap on MR angiography was considered eligible. Eligibility for vascular imaging was reviewed centrally. Eligible patients were >30 years of age, but those of age 30–49 years had either established atherosclerosis in another vascular bed or 2 or more vascular risk factors, and signed informed consent. We excluded those with contraindications to MRI, MR contrast agents, including allergy, creatinine >1.5 mg/dL or GFR <30 mL/min/1.73 m2, and those with planned endovascular treatment for ICAD. All enrolled patients were treated with aggressive medical therapy based on the Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial medical regimen (10). The primary outcome in the MyRIAD study was to assess the incidence of ischemic stroke in the territory of the stenotic artery; secondary outcomes included recurrent TIA and new infarct on MRI at 6–8 weeks.
We recorded demographic and clinical characteristics, medications, laboratory tests at the time of the index event, and collected all eligibility brain parenchymal and vascular imaging. A brain MRI with FLAIR and DWI/ADC sequences was obtained at 6–8 weeks. Clinical follow-up occurred at 6–8 weeks, 3 months + 15 days, 6 months + 15 days, and 12 months + 21 days to determine if an endpoint had occurred and to record treatment adherence.
The baseline study imaging was evaluated by central readers. Patterns of recurrent infarcts were analyzed by reviewing the MRI FLAIR and DWI sequences by two central adjudicators (R.S.S and D.L). We classified recurrent infarct patterns using a methodology used prior studies of ICAD (5) as follows: (1) Perforator (Figure 1)—single subcortical lesions that result from perforating vessels originating at the site of the stenosis; (2) Borderzone (Figure 2)—lesions that occur in the corona radiata or centrum semiovale and or between cortical borderzone territories, such as between the middle cerebral artery and anterior cerebral artery or the middle cerebral artery and the posterior cerebral artery; (3) Cortical/Territorial (Figure 3)—lesions that occur distal to the region of stenosis but are located in the region supplied by the corresponding intracranial artery; and (4) Mixed (Figure 4)—a combination of cortical and subcortical lesions.
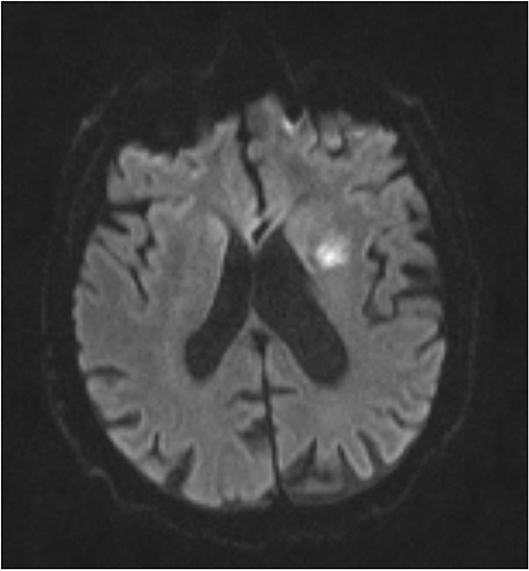
Figure 1. MRI DWI sequence of Perforator Infarct.
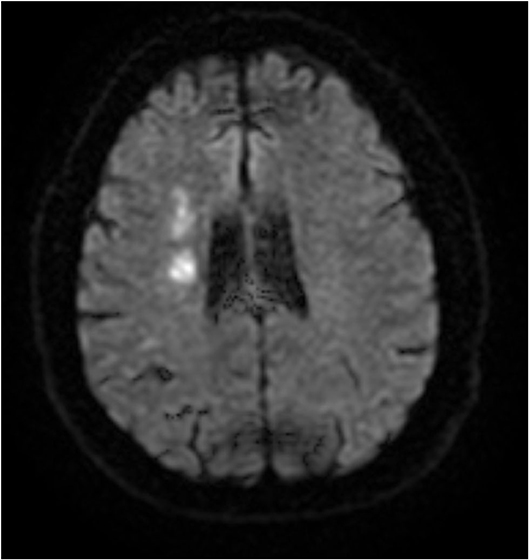
Figure 2. MRI DWI sequence of Borderzone Infarct.
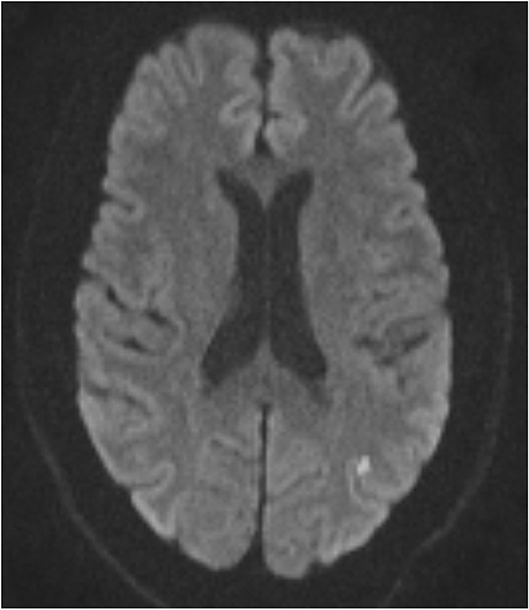
Figure 3. MRI DWI sequence of Cortical/Territorial Infarct.
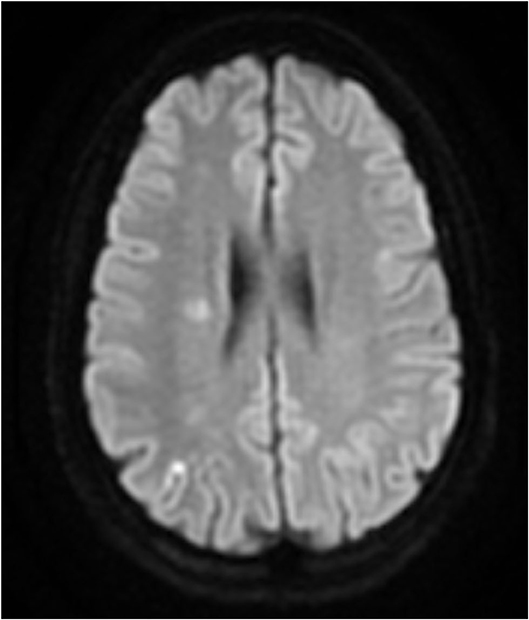
Figure 4. MRI DWI sequence of Mixed Infarct.
Recurrent infarcts were considered when new DWI/ADC or FLAIR sequence lesion developed compared to the baseline MRI ascertained by 2 independent experienced vascular neurologists (EF, RSS) who reviewed clinical data and imaging studies, including that obtained at baseline, 6–8 weeks, and at the time of a clinical endpoint. Recurrent infarcts were also analyzed for volume of infarcts by comparing the original volume of infarct measured on FLAIR (cm3) as well as the volume of FLAIR and DWI lesions at 6–8 weeks MRI or clinical endpoint MRI. Oleasphere 3.0 was used to co-register the baseline and 6–8 weeks MRI FLAIR sequences. Volumes of new infarction were calculated from the subtraction maps after visual verification to remove any artifacts.
Continuous measurements are summarized as mean ± standard deviation, or median ± interquartile range for attributes with skewed distributions.
MyRIAD is supported through a grant by the NIH/NINDS (R01 NS084288). The institutional review board/ethics committee at each participating institution approved this study, which is registered at ClinicalTrials.gov (NCT02121028).
Of 89 patients with 6–8 weeks MRI, 22 (24.7%) had recurrent infarcts in the territory of the symptomatic artery. The mean age was 57.7 ± 12.2 (mean, SD) years with 14/22 (64%) male, 13/22 (59%) White, 8/22 (36%) African American, 1/22 (5%) Asian, and 4/22 (18%) Hispanic. The location of stenosis was the middle cerebral artery in 14 (63.6%), intracranial carotid artery in 4 (18.2%) and basilar artery in 3 (13.6%). The mean degree of stenosis was 83% (±9%) in 21 cases while 1 had a flow gap on MRA.
The recurrent infarct was evident on DWI in 14 of the 22 (63.6%) patients while in 8 of 22 (36.4%) they were apparent only on FLAIR. Only 5/22 (22.7%) patients had symptomatic presentations in this time period. Recurrent ischemic lesions were single in 12/22 (54.5%) and multiple in 10/22 (45.5%) patients. The median volume of infarcted tissue was 2.0 cm3 with interquartile range 5.3 cm3 (minimum and maximum volumes 0 and 25.2 cm3, respectively). Index infarct volumes were median 2.5 cm3 with interquartile range 7 cm3 (minimum and maximum 0 and 30.3 cm3).
The infarct patterns are exemplified in Table 1. We found a mixed pattern in 9/22 (40.9%), borderzone distribution in 5 (22.7%), cortical or territorial in 6 (27.3%), while only 2 (9.1%) were in a perforator artery distribution. Amongst those with a mixed pattern, 8/9 had a borderzone distribution infarct as part of their mixed infarct pattern.
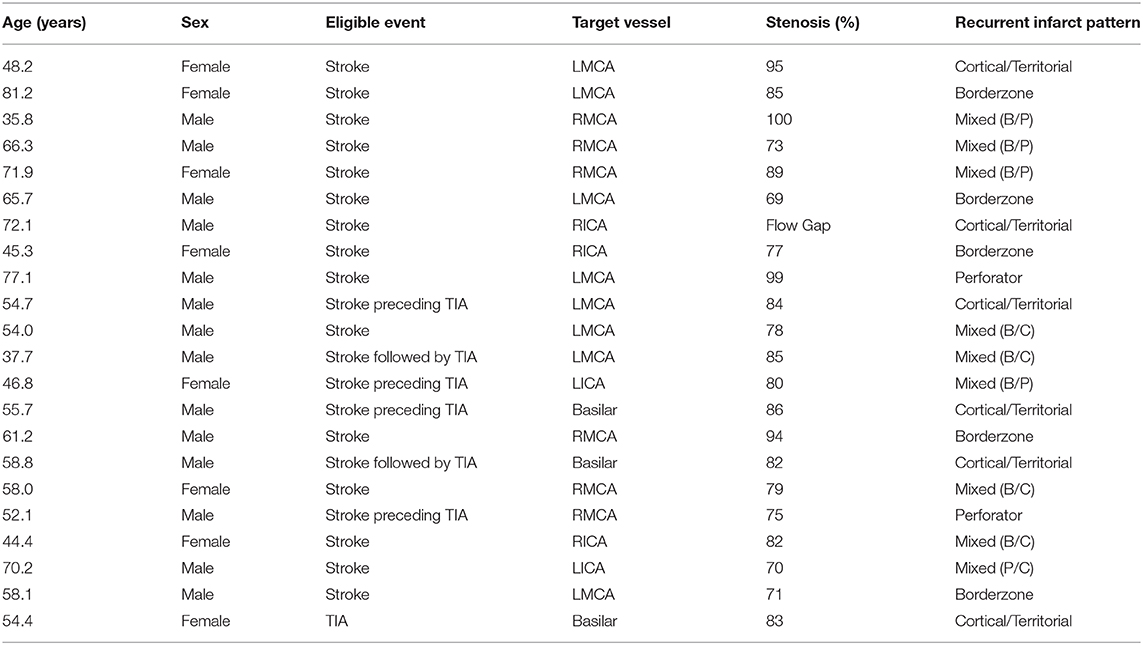
Table 1. Characteristics of patients with recurrent infarct in the MyRIAD cohort.
In this secondary analysis of the MyRIAD study, we describe characteristics of recurrent infarcts, with interesting observations. First, patients were noted to have recurrent infarcts that were similar in size to the original index event. Both the index event and recurrent events had lesion volumes of 2–2.5 cm3. These data suggest that that a quarter of patients with ICAD will accrue infarcts within 8 weeks with similar volumetric impact on the brain as the index infarct. These cumulative effects of overt and covert infarcts may lead to long-term cognitive and other neurologic consequences and requires further study. Previous studies have shown that infarct size is a predictor of poor outcome in ischemic stroke patients (11). It should be noted that while infarct size and outcome has been reported in lacunar strokes (12), this is the first study to report the size of recurrent infarcts in patients with ICAD. Further studies should focus on determination of patient functional and cognitive outcomes with temporal relation to changes in infarct size.
Second, nearly two thirds of recurrent infarcts had restricted diffusion, indicating that the infarcts were acute and not merely evolution and extensions of the original infarcts. A prior study suggested that while early lesion recurrence may be secondary to a progression of the initial ischemic event, delayed occurrence is a more accurate reflection of a recurrent ischemic event (13). Given that only five of the 22 cases had a clinical stroke recurrence, MRI-defined ischemic lesion recurrence could be a more sensitive and objective marker for stroke recurrence and should be considered in future clinical trials of ICAD (13). It is possible that earlier small recurrent infarcts within areas of baseline FLAIR/T2 signal abnormality could go undetected at the time frame of repeat imaging as the DWI signal abnormality may have normalized. The time course of early infarction recurrence should be evaluated in future studies with earlier repeat imaging. Furthermore, it is difficult to ascertain the effects of silent ischemic lesions (SIL) without clinical manifestations on patient outcomes; further analysis is required to assess changes in patient cognition, physical phenotypes, and quality of life to fully understand whether SIL's will require further changes in medical therapy or medical approaches for patients with symptomatic ICAD.
Finally, the majority of patients with recurrent infarcts had had a borderzone distribution infarct, either alone or in combination with other patterns, at the index event. This suggests that hypoperfusion is a significant mechanism for recurrent events. Similar patterns have been seen in previous analysis of ICAD patients and recurrent patterns of infarcts (5). Patients with a perforator pattern of infarct were less common. This is different from other studies (5) and may be explained by the small sample size.
There are limitations to this study. With a small sample size, it is difficult to draw definitive conclusions regarding the mechanisms of recurrent infarcts. This analysis was also completed post-hoc with attendant biases. This study also has some important strengths, including volumetric analysis of recurrent infarct volume and careful ascertainment of infarct recurrence in a meticulously analyzed ICAD cohort.
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the institutional ethics review board at each participating institution approved to participate in MyRIAD. The patients/participants provided their written informed consent to participate in this study.
RS, SP, JR, and DL: formulation of research question, data collection, data review, writing manuscript, and editing of manuscript. EF, TH, GC, and IC-B: data collection. AN: statistical analysis, data collection, and editing of manuscript. All authors contributed to the article and approved the submitted version.
MyRIAD was an investigator-initiated study funded by the NIH/NINDS (R01 NS084288). VasSol Inc. (River Forest, IL) provided the NOVA software for QMRA at no cost. In addition to its 10 recruiting sites, MyRIAD has various core facilities: central coordinating and TCD core (U Miami), PWI and neuroimaging core (UCLA), QMRA core (U Chicago), eligibility and endpoint adjudication (Baystate), and statistical and data management core (Emory). It was registered in ClinicalTrials.gov: NCT02121028.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Gorelick PB, Wong KS, Bae HJ, Pandey DK. Large artery intracranial occlusive disease: a large worldwide burden but a relatively neglected frontier. Stroke. (2008) 39:2396–9. doi: 10.1161/STROKEAHA.107.505776
2. Chimowitz MI, Lynn MJ, Howlett-Smith H, Stern BJ, Hertzberg VS, Frankel MR, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. (2005) 352:1305–16. doi: 10.1056/NEJMoa043033
3. Derdeyn CP, Chimowitz MI, Lynn MJ, Fiorella D, Turan TN, Janis LS, et al. Aggressive medical treatment with or without stenting in high-risk patients with intracranial artery stenosis (SAMMPRIS): the final results of a randomised trial. Lancet. (2014) 383:333–41. doi: 10.1016/S0140-6736(13)62038-3
4. Liebeskind DS, Prabhakaran S, Azhar N, Feldmann E, Campo-Bustillo I, Sangha R, et al. Mechanisms of early recurrence in intracranial atherosclerotic disease (MyRIAD): rationale and design. J Stroke Cerebrovasc Dis. (2020) 29:105051. doi: 10.1016/j.jstrokecerebrovasdis.2020.105051
5. López-Cancio E, Matheus MG, Romano JG, Liebeskind DS, Prabhakaran S, Turan TN, et al. Infarct patterns, collaterals and likely causative mechanisms of stroke in symptomatic intracranial atherosclerosis. Cerebrovasc Dis. (2014) 37:417–22. doi: 10.1159/000362922
6. Jung JM, Kang DW, Yu KH, Koo JS, Lee JH, Park JM, et al. Predictors of recurrent stroke in patients with symptomatic intracranial arterial stenosis. Stroke. (2012) 43:2785–7. doi: 10.1161/STROKEAHA.112.659185
7. Wessels T, Wessels C, Ellsiepen A, Reuter I, Trittmacher S, Stolz E, et al. Contribution of diffusion-weighted imaging in determination of stroke etiology. Am J Neuroradiol. (2006) 27:35–9.
8. Yaghi S, Grory BM, Prabhakaran S, Yeatts SD, Cutting S, Jayaraman M, et al. Infarct pattern, perfusion mismatch thresholds, and recurrent cerebrovascular events in symptomatic intracranial stenosis. J Neuroimaging. (2019) 29:640–4. doi: 10.1111/jon.12630
9. Samuels OB, Joseph GJ, Lynn MJ, Smith HA, Chimowitz MI. A standardized method for measuring intracranial arterial stenosis. Am J Neuroradiol. (2000) 21:643–6.
10. Turan TN, Lynn MJ, Nizam A, Lane B, Egan BM, Le NA, et al. Rationale, design, and implementation of aggressive risk factor management in the stenting and aggressive medical management for prevention of recurrent stroke in intracranial stenosis (SAMMPRIS) trial. Circ Cardiovasc Qual Outcomes. (2012) 5:e51–60. doi: 10.1161/CIRCOUTCOMES.112.966911
11. Vogt G, Laage R, Shuaib A, Schneider A, VISTA Collaboration. Initial lesion volume is an independent predictor of clinical stroke outcome at day 90: an analysis of the virtual international stroke trials archive (VISTA) database. Stroke. (2012) 43:1266–72. doi: 10.1161/STROKEAHA.111.646570
12. Asdaghi N, Pearce LA, Nakajima M, Field TS, Bazan C, Cermeno F, et al. Clinical correlates of infarct shape and volume in lacunar strokes: the secondary prevention of small subcortical strokes trial. Stroke. (2014) 45:2952–8. doi: 10.1161/STROKEAHA.114.005211
Keywords: ischemic stroke, intracranial atherosclerosis, stroke mechanisms, recurrent infarction pattern, infarct size
Citation: Sangha RS, Prabhakaran S, Feldmann E, Honda T, Nizam A, Cotsonis GA, Campo-Bustillo I, Romano JG and Liebeskind DS (2021) Imaging Patterns of Recurrent Infarction in the Mechanisms of Early Recurrence in Intracranial Atherosclerotic Disease (MyRIAD) Study. Front. Neurol. 11:615094. doi: 10.3389/fneur.2020.615094
Received: 08 October 2020; Accepted: 29 December 2020;
Published: 21 January 2021.
Edited by:
Gustavo J. Rodriguez, Texas Tech University Health Sciences Center El Paso, United StatesReviewed by:
Alberto Maud, Texas Tech University Health Sciences Center El Paso, United StatesCopyright © 2021 Sangha, Prabhakaran, Feldmann, Honda, Nizam, Cotsonis, Campo-Bustillo, Romano and Liebeskind. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rajbeer S. Sangha, cnNzYW5naGFAdWFibWMuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.