
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol., 15 December 2020
Sec. Headache and Neurogenic Pain
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.576272
 Carlo Maria Giovanardi1*
Carlo Maria Giovanardi1* Michela Cinquini2
Michela Cinquini2 Marco Aguggia3Gianni Allais4Manuela Campesato5
Marco Aguggia3Gianni Allais4Manuela Campesato5 Sabina Cevoli6Fabio Gentili7Annunzio Matrà8
Sabina Cevoli6Fabio Gentili7Annunzio Matrà8 Silvia Minozzi2
Silvia Minozzi2Introduction: Migraine is a chronic paroxymal neurological disorder characterized by attacks of moderate to severe headache and reversible neurological and systemic symptoms. Treatment of migraine includes acute therapies, that aim to reduce the intensity of pain of each attack, and preventive therapies that should decrease the frequency of headache recurrence. The objective of this systematic review was to assess the efficacy and safety of acupuncture for the prophylaxis of episodic or chronic migraine in adult patients compared to pharmacological treatment.
Methods: We included randomized-controlled trials published in western languages that compared any treatment involving needle insertion (with or without manual or electrical stimulation) at acupuncture points, pain points or trigger points, with any pharmacological prophylaxis in adult (≥18 years) with chronic or episodic migraine with or without aura according to the criteria of the International Headache Society.
Results: Nine randomized trials were included encompassing 1,484 patients. At the end of intervention we found a small reduction in favor of acupuncture for the number of days with migraine per month: (SMD: −0.37; 95% CI −1.64 to −0.11), and for response rate (RR: 1.46; 95% CI 1.16–1.84). We found a moderate effect in the reduction of pain intensity in favor of acupuncture (SMD: −0.36; 95% CI −0.60 to −0.13), and a large reduction in favor of acupuncture in both the dropout rate due to any reason (RR 0.39; 95% CI 0.18 to 0.84) and the dropout rate due to adverse event (RR 0.26; 95% CI 0.09 to 0.74). Quality of evidence was moderate for all these primary outcomes. Results at longest follow-up confirmed these effects.
Conclusions: Based on moderate certainty of evidence, we conclude that acupuncture is mildly more effective and much safer than medication for the prophylaxis of migraine.
Migraine is a chronic paroxymal neurological disease characterized by moderate to severe attacks of headache and reversible systemic and neurological symptoms. The typical state phase includes phonophobia, photophobia, gastrointestinal symptoms such as nausea, and vomit, and cutaneous allodynia (1).
Overall, migraine is a common form of disabling primary headache (1) (ref ICHD-3) and it is among the most prevalent disorder worldwide, affecting about 15% of adults in Western countries. Its prevalence is higher in the age group 35–39 years and among females. About 2.5% of subjects with episodic migraine progress to chronic migraine (CM) every year. CM, the most disabling form of migraine, currently affects up to 2% of the population worldwide.
Migraine is considered among the top five causes of disability by the Global Burden of Disease study with about one billion individuals affected worldwide. The GBD 2016 study reported that migraine is the first cause of years lived with disability (YLDs) both in males and females in the age group 15–49 years (2), afflicting people in the active period of their life, leading to a reduction of quality of life and relevant disability, with significant social consequences.
Migraine also leads to important use of health care resources, high direct and indirect costs, and work loss, with a significant societal impact.
A recent review on the burden of this disease highlighted that the total cost of migraine in USA was more than 2,500$ per year, and that the cost of CM was more than 8,200$ per year: according to this study, 60–64% of its costs were attributable to direct medical costs. In a recent European study the average direct cost of EM was estimated as 746€ per year, while those of CM were estimated as 2,427€ per year (3).
Treatment of migraine includes both therapies of the acute attacks, with the aim to reduce the intensity of pain of each migraineous attack, and prophylactic treatments, with the aim to reduce the frequency of headache recurrence. Considering both the evidence for efficacy and the risk of potential side effects, drugs with the most favorable profiles are amitriptyline, beta-blockers, candesartan, flunarizine, onabotulinumtoxinA (for CM), pizotifene, and topiramate. In addition, calcitonin gene-related peptide (CGRP) receptor monoclonal antibodies were recently approved for migraine prophylaxes (4).
Despite the progresses in drug treatment, patients are often still unsatisfied because of the insufficient control of pain or the disturbing adverse events that limit patients' compliance.
In the last decades, acupuncture has been suggested as a valid non-pharmacological alternative for migraine prophylaxis and its use in Western countries has increased considerably.
According to some authors, acupuncture carry out its analgesic effects by interacting with the hypothalamic-pituitary-adrenal axis and the endogenous opioid system, known to be important mediators of the stress response to pain (5). Several studies demonstrated that acupuncture activate the release of opioid in the central nervous system (6–10). Gao et al. (6) report that “Release of these peptides corresponds to long-lasting activation of ascending sensory tracks, thereby relieving an array of pain conditions.” Furthermore, using a migraine rat model, researchers observed that the expression of CGRP in the trigeminal ganglion, which is considered a migraine trigger factor (11), could be depressed by the electro-acupuncture treatment (12). In addition, acupuncture was demonstrated to restore the descending pain modulatory system, impaired in patients affected by migraine, by decreasing the resting state of functional connectivity between the rostral anterior cingulate cortex/medial prefrontal cortex and the periaqueductal gray, which is correlated with the intensity of pain during the attacks (13).
To understand the mechanisms of action of acupuncture, as well as its local, remote, and long-term effects, a key may be the reaction to needles insertion, called “de qi” and widely judged as an important factor affecting the therapeutic effect of acupuncture. “De qi” includes both a typical needling sensation, sensed by the patient, and a “needle grasp” noticed by the provider: the acupuncturist perceives tearing and augmented resistance to additional movement of the needle. Langevin hypothesized that “needle grasp is due to mechanical coupling between the needle and connective tissue with winding of tissue around the needle during needle rotation and needle manipulation transmits a mechanical signal to connective tissue cells via mechano-transduction” (14).
In conclusion, although the mechanism of action of acupuncture doesn't have yet a definite explanation, acupuncture has a scientific basis built on a series of studies that have been conducted over the last decades: there are neurobiological models that could elucidate how acupuncture obtain its therapeutic effect in several clinical settings.
The efficacy of acupuncture for migraine has been confirmed by several clinical trials and a series of systematic reviews, including a Cochrane Review (15, 16). Consequently, acupuncture is becoming a more accepted form of integrative medicine in the Western countries for the prevention and treatment of migraine (17) and is administered for migraine prophylaxis and chronic pain treatment all over the world (15, 18): migraine and other headaches were the primary indications for acupuncture treatment in 9.9% of US patients (17).
In 2009, a Cochrane review concluded that “there is consistent evidence that acupuncture provides additional benefit to treatment of acute migraine attacks only or to routine care. Available studies suggested that acupuncture is at least as effective as, or possibly more effective than, prophylactic drug treatment, and has fewer adverse effects” (15); after 7 years, the update of the same Cochrane review suggested the prevalence of headaches is reduced by combining acupuncture with usual care; it also suggested that there is an effect over sham and that acupuncture may be at least as effective as treatment with prophylactic drugs and it is associated with fewer adverse effects (16).
Since 2016, several new studies have appeared to support the efficacy of acupuncture in migraine prevention (16); acupuncture can be recognized as a valid treatment in Western countries if its specific effects are clearly understood.
The objective of this systematic review was to assess the efficacy and safety of acupuncture for the prophylaxis of episodic or chronic migraine in adult patients when compared to pharmacological treatment.
We performed this systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (19).
We included randomized-controlled trials published in western languages that compared any treatment involving needle insertion (with or without manual or electrical stimulation) at acupuncture points, pain points or trigger points, described as acupuncture with any pharmacological prophylaxis in adult (≥18 years) participants with chronic and episodic migraine with or without aura according to the criteria of the International Headache Society (1). Studies on patients with cluster headache or tension-type headache were excluded. We also excluded studies that evaluated acupuncture at specific “microsystems” (e.g., scalp or ear acupuncture), although we included trials using micro-system points in addition to body acupuncture; evaluated other methods of stimulating acupuncture points without needle insertion, for example, acupressure, laser stimulation, or transcutaneous electrical stimulation; injected fluids at acupuncture or trigger points.
Primary outcomes were:
• number of days with migraine per month
• response rate (≥50% frequency reduction documented in a headache diary)
• pain intensity as documented in a headache diary
• dropout from treatment for any reason
• drop out due to adverse event.
Secondary outcomes assessed were:
• quality of life as measured by validated scales (e.g., SF-36; SF-12) (20, 21)
• frequency of migraine attack per month
• disability due to migraine as measured by validated scale (e.g., MIDAS score; Pain disability index) (22, 23)
• use of rescue medication
• number of subjects with at least one adverse event AE.
Cochrane Database of Systematic Reviews (CENTRAL), Embase, MEDLINE, and ClinicalTrial.gov were searched for eligible studies. Literature search was performed using free text and Mesh terms from inception up to 14 May 2020 without language restriction. The detailed search strategy is reported in the Supplementary Material 1.
Two authors independently screened articles retrieved via the search strategy from the title and abstracts. Potentially relevant studies were acquired in full text and assessed for final inclusion independently by two authors. Any disagreement was discussed with a third author. Two review authors independently extracted data from the studies We extracted the following information: number and characteristics of participants: mean age, % female, duration of disease in years, chronic vs. episodic migraine; details of acupuncture treatments: number of sessions, number of acupoints, achievement of de-chi (an irradiating feeling considered to indicate effective needling), duration of treatment in weeks; type of drugs received by participant of the control group, length of follow-up after the end of treatment, types of outcomes assessed, country where the study was conducted.
Two authors independently assessed risk of bias according to the criteria set out in the Cochrane Handbook for Systematic Reviews of Interventions (24). The following criteria were considered: sequence generation and allocation concealment (selection bias), blinding of participants and providers (performance bias), blinding of outcome assessors (detection bias), incomplete outcome data (attrition bias), and selective outcome reporting (reporting bias). Disagreement between reviewers was resolved by discussion.
We analyzed dichotomous outcomes by calculating the risk ratio (RR) for each trial with the uncertainty in each result being expressed with a 95% confidence interval (CI). We analyzed continuous outcomes by calculating the mean difference (MD) with 95% CI when the studies used the same instrument for assessing the outcome. We used the standardized mean difference (SMD) when the studies used different instruments. We interpreted SMD values with the classification proposed by Cohen et al. (25) where an effect size of 0.2 means a small effect, 0.5 means a medium effect, 0.8 means a large effect.
As we supposed a certain degree of heterogeneity among studies, due to treatment schedules, way in assessing response criteria, risk of bias and other factors which may have affected direction and magnitude of treatment effect, we pooled data used the random effect model for each outcome.
Seeking statistical heterogeneity among studies, the Cochrane Q-test was performed, with a significant threshold of alpha = 0.1 and inconsistency among studies was quantified by the I-squared statistic (24); an I square >70% was judged a significant heterogeneity.
Results are depicted in all figures as conventional meta-analysis forest plots. RevMan 5.3 was used for producing forest plot figures (26).
We planned to use visual inspection of funnel plots (plots of the effect estimate from each study against the sample size or effect standard error) to indicate possible publication bias if there were at least 10 studies included in the meta-analysis.
Although the STRICTA (Standards for Reporting Interventions in Controlled Trials of Acupuncture) recommendations describe the components of acupuncture procedures (27) better outcomes appear to be associated with a greater numbers of needles and treatment sessions (28) and on the other hand, an insufficient dose of acupuncture may be an obstacle to good patient care (29).
When starting this study, the vast heterogeneity among the contributions available in the literature has soon become evident. The extremely different ways of administering acupuncture made it almost impossible to compare the outcomes of the trials. Consequently, we have decided to establish standard criteria for comparison of data. By introducing the concept of adequate dose of acupuncture already expressed by other authors (30), we have considered the following three parameters:
• number of points needled during each treatment
• de qi response
• number of treatment sessions.
The “de qi” response, that is to say the sensation from needling experienced by the patient, may be reported as numbness (A-beta fiber activation) or as aching, dull, heavy, and warm sensation (A-delta or C fiber activation) (31).
The concept of dose-intensity has thus been introduced and used to group the studies according to the intensity of acupuncture based on the following criteria:
• number of sessions (≥8 vs. <8)
• number of acupoints treated (≥10 vs. <10)
• achievement of de-qi (yes vs. no/not reported).
Acupuncture was judged as at low intensity of only one criterion was met; on medium intensity if two criteria were met; high intensity if all the three criteria were met. Subgroup analyses was performed for intensity of acupuncture.
We assessed the overall quality of the evidence for the primary outcomes using the five GRADE domains (study limitations, consistency of effect, imprecision, indirectness, and publication bias) according to the GRADE approach (32).
Based on the above domains, the GRADE system uses the following criteria to grade the evidence:
High: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Very low: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
The existing evidence was summarized in a “Summary of Findings” table that provides key information about the magnitudes of relative and absolute effects of the interventions, the amount of available evidence and the certainty of available evidence (33).
The database searches retrieved 115 records after duplicate were removed. Eighteen studies were judged as potentially relevant. For 6 records we were unable to retrieve the full text. Three articles were excluded because they did not meet the inclusion criteria (34–36). Nine randomized trials were finally included (31, 37–44) (Figure 1). These trials included 1,484 patients. Participants were recruited from outpatient departments in 6 studies (31, 38, 39, 41–43); they were partly respondents to a newspaper advertisement, partly referred from general practitioners in one study (40); methods of recruitment was not described in two studies (37, 44).
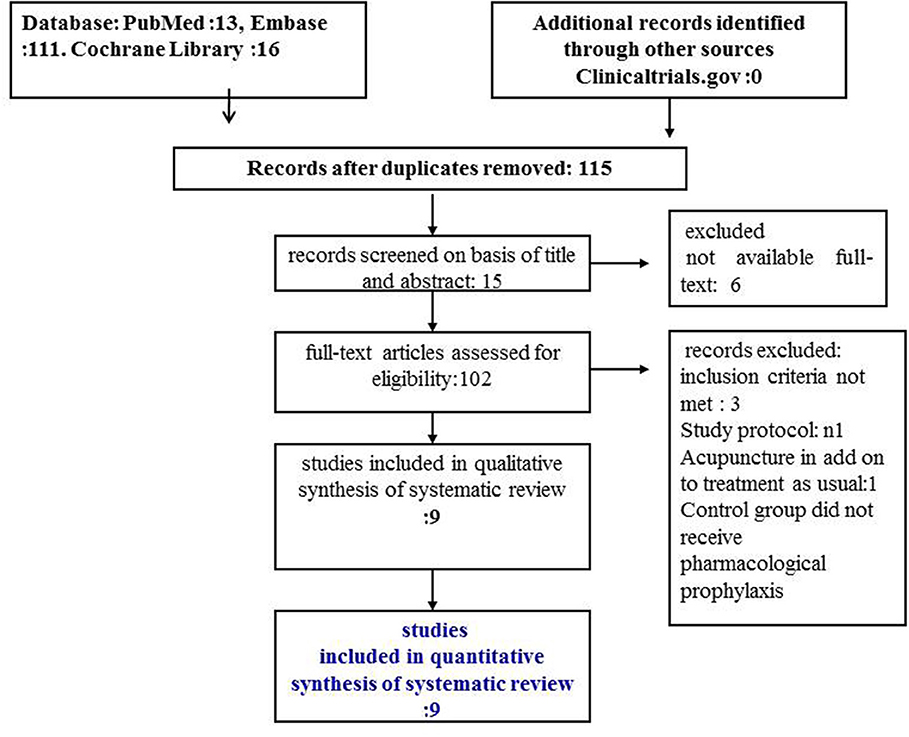
Figure 1. PRISMA flow diagram.
The mean age of participants was 39.5 year (range 36–47 years). Most participants were female (mean: 81% range: 81–100%). Mean duration of migraine was 13.9 (SD 6.12) years and the mean number of migraine days per month at baseline was 13.3 (SD 7.4), data available only from 5 studies.
The mean duration of acupuncture was 11 weeks (range 4–24 weeks). Acupuncture was judged of high intensity in 6 studies (32, 37–39, 41, 43), of medium intensity in one study (42), of low intensity in 2 studies (40, 44).
Drugs received by the control group were: flunarizine: 3 studies (37, 42, 44); valproate 2 studies (31, 39); metoprolol: 2 studies (40, 41); Topiramate: 1 study (43); either beta blockers, flunarizine or valproate: 1 study (37). One study (31) had a third arm which received botulinum toxin only once in 31 trigger zones over the facial and pericranial muscles, at the total dosage of 155 U. This arm was not considered in our meta-analysis as the total doses and the frequency of injections were judged insufficient to have a therapeutically effect. In fact, the study performed only one botulinum toxin A session while, according the protocol of the PREEMPT (36) and subsequent real-life studies, efficacy was higher after the second and third sessions.
The migraine days per months, the number of attacks per months, pain intensity and use of rescue medications were recorded in all the studies through a headache diary. We reported the results at the end of treatment period, which ranged from 4 to 24 weeks and at the longest available follow up, which ranged from 8 to 26 weeks.
Two studies were conducted in China (42, 44), two in Italy (37, 39) two in Germany (38, 41), one each in Taiwan (43), Iran (31), and Denmark (40). Table 1 summarizes the characteristics and results of each trial.
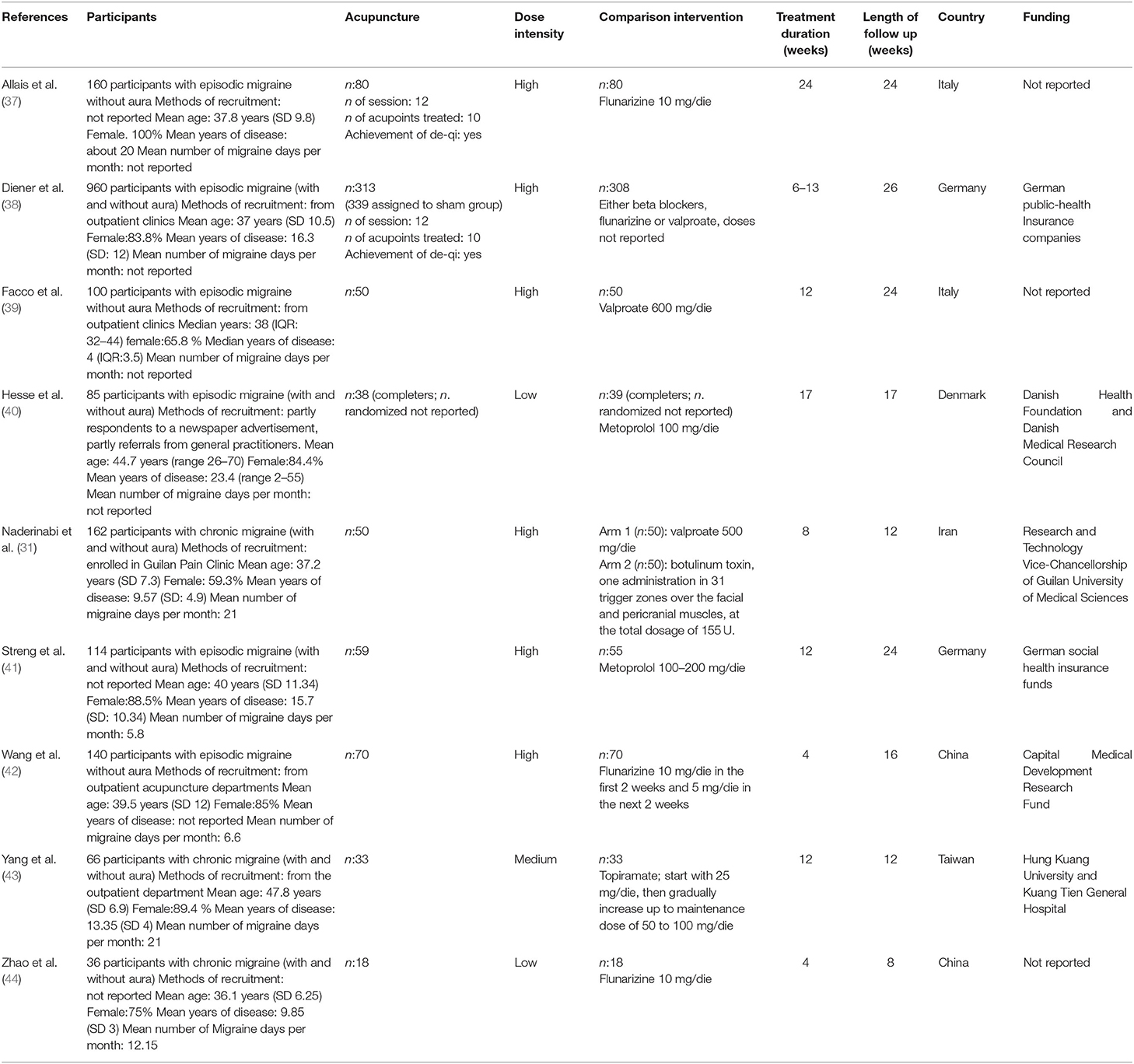
Table 1. Characteristics of included studies.
Six studies were judged at low risk of selection bias because both the methods for random sequence generation and allocation concealment was appropriate; one study (44) followed ad adequate method for random sequence generation but did not provide information about concealment of allocation. The remaining two studies (31, 40) were judged at unclear risk for selection bias because they did not provide any information about methods followed to generate the random sequence and to conceal the allocation. All but three studies were judged at high risk of both performance and detection bias because they were open label; Two studies (40, 42) used the double-blind double dummy approach and was judged at low risk for both the domains. Three studies were judged at high of attrition bias (38, 40, 41) because of the high number of subjects who dropped out from studies and no attempt to perform an intention to treat analysis. One study (31) did not provide information about subjects dropped out from each group. The study protocol was available only for two studies (31, 42) and the outcomes reported in the final publication coincided with the outcomes listed in the protocol; for all the remaining studies the protocol was not available and they were judged at unclear risk of selective outcome reporting (Figure 2).

Figure 2. Risk of bias assessment.
Number of days with migraine per month: we found a small but significant effect in favor of acupuncture (SMD: −0.37; 95% CI −0.64 to −0.11; I2 = 71%, 6 studies, 992 participants; Figure 3A).

Figure 3. Forest plot of primary outcomes—results at the end of the intervention. (A) Number of days with migraine per months; (B) Response rate to treatment; (C) Pain intensity.
Response rate: we found a small but significant reduction in favor of acupuncture (RR: 1.46; 95% CI 1.16 to 1.84; I2 = 58%, 5 studies, 956 participants; Figure 3B).
Pain intensity: we found a moderate effect in the reduction of pain in favor of acupuncture (SMD: −0.36; 95% CI −0.60 to −0.13; I2 = 49%, 3 studies, 730 participants; Figure 3C).
Dropout: we found a strong reduction in favor of acupuncture in both the dropout rate due to any reason (RR 0.39; 95% CI 0.18 to 0.84; I2 = 77%, 6 studies, 1,211 participants) and the dropout rate due to adverse event (RR 0.26; 95% CI 0.09 to 0.74; I2 = 0%, 6 studies, 646 participants; Figures 4A,B).
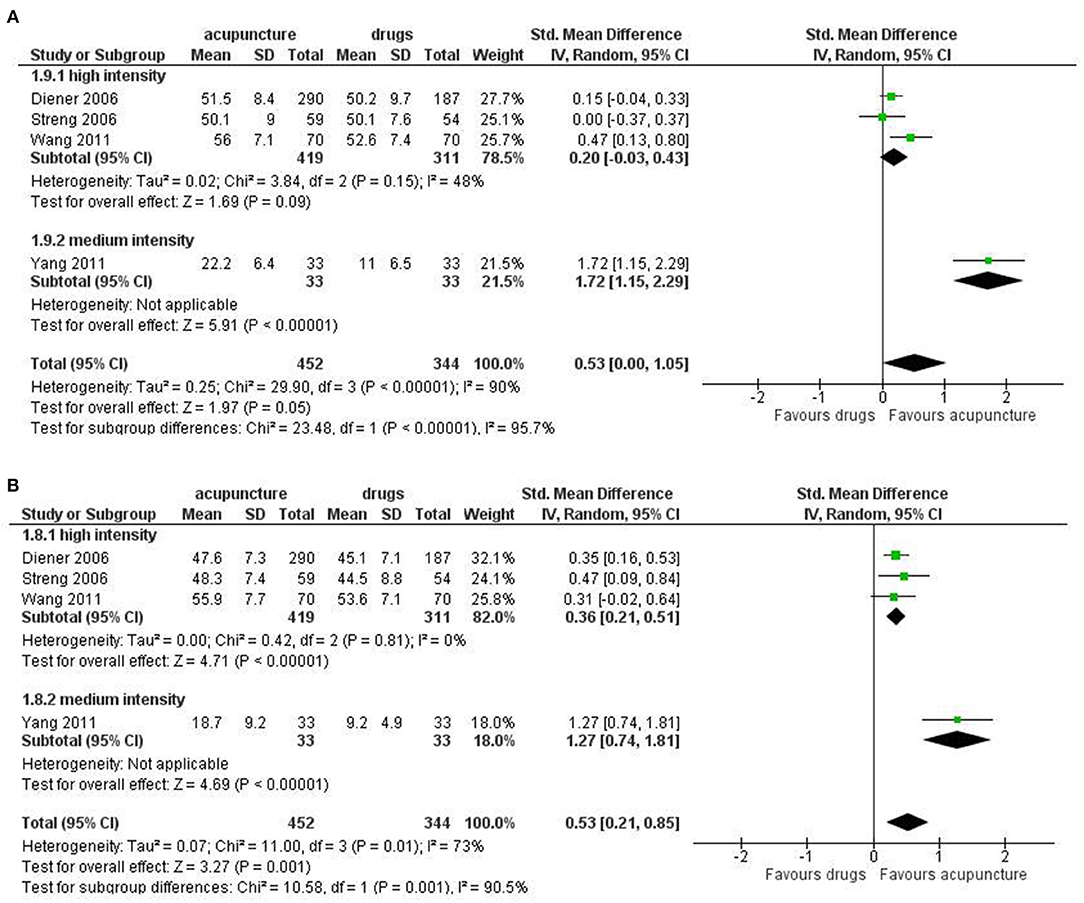
Figure 4. Forest plot of primary outcomes—results at the end of the intervention. (A) Dropout due to any events; (B) Dropout due to adverse events.
Quality of evidence was moderate for all the primary outcomes (Table 2).
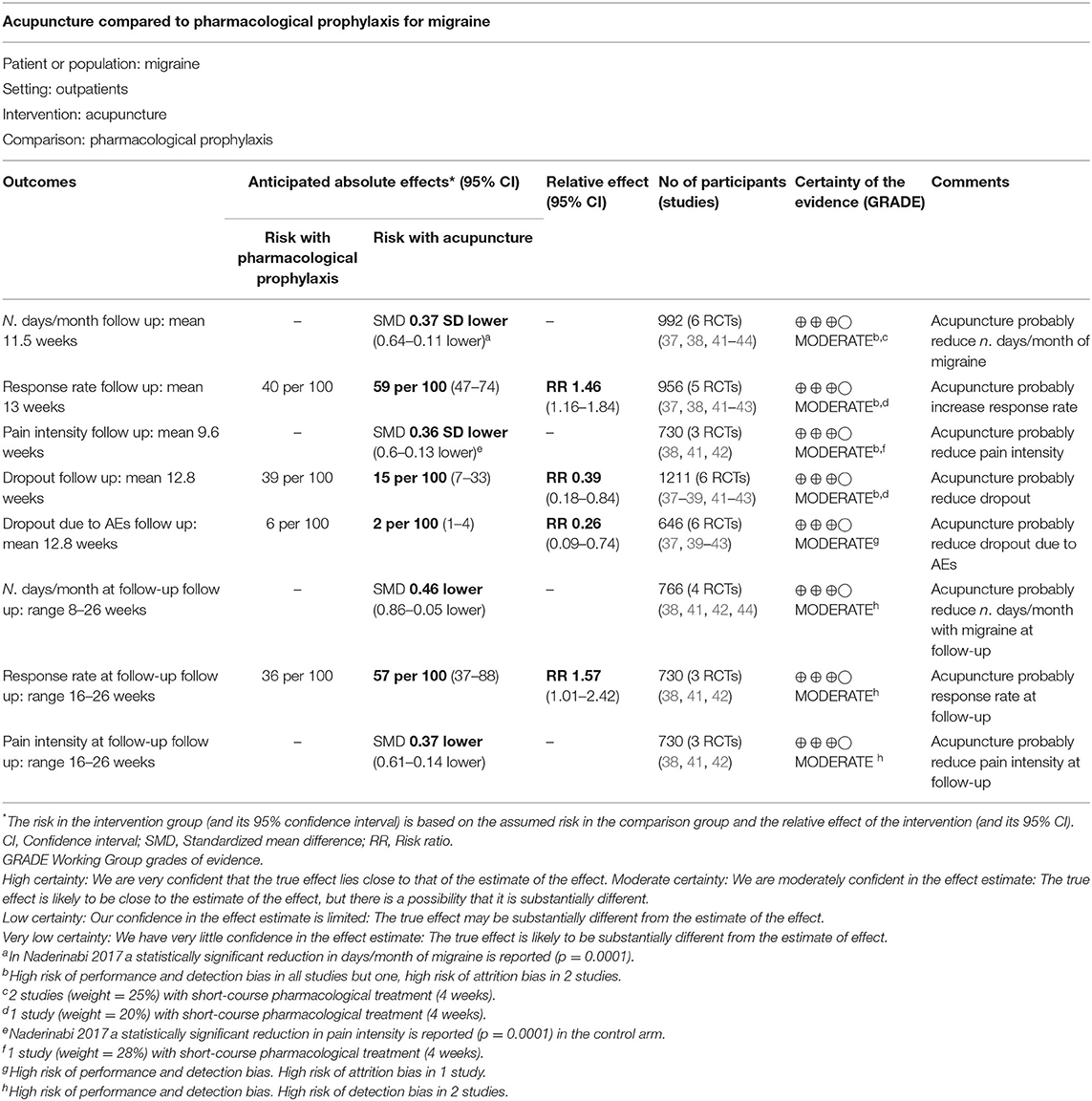
Table 2. Summary of findings.
For the secondary outcomes we did not find significant difference between treatments in the frequency of migraine attack per month (SMD: −0.15, 95% CI −0.39 to 0.08; I2 = 0%, 2 studies, 273 participant); disability (SMD: −0.33, 95% CI −0.89 to 0.22; I2 = 90%, 4 studies, 479 participants); use of rescue medication (SMD: −0.40, 95% CI −0.92 to 0.13; I2 = 89%, 5 studies, 532 participants); we found a significant difference in favor of acupuncture in the number of subjects with at least one adverse event (RR: 0.29, 95% CI 0.14 to 0.60; I2 = 82%, 7 studies, 1,153 participants; Figures 5A–D).
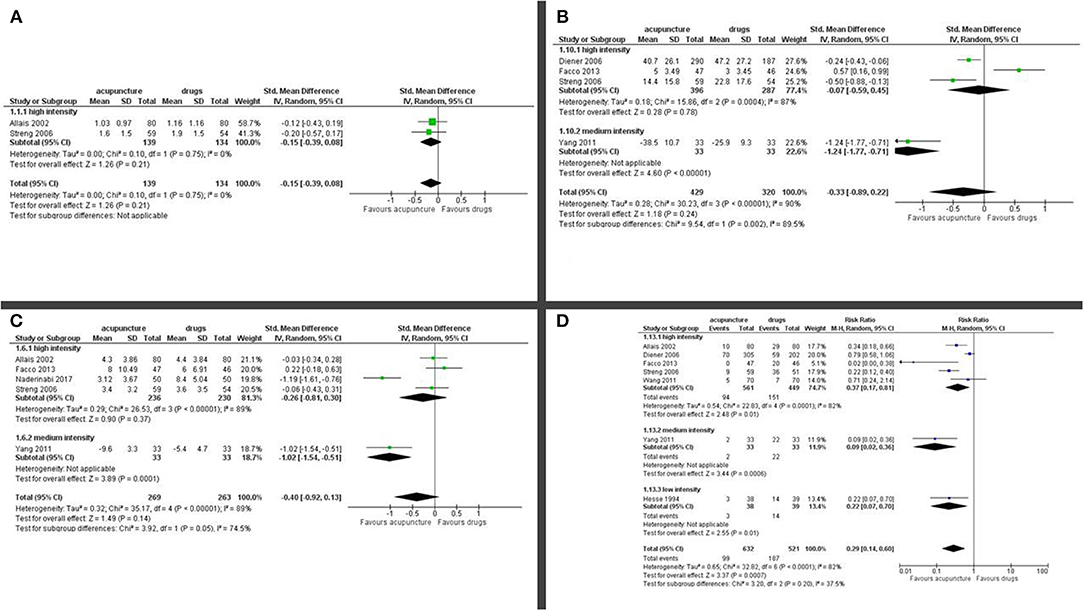
Figure 5. Forest plot of secondary outcomes—results at the end of the intervention. (A) Frequency of migraine attack per month; (B) Disability; (C) Use of rescue medication; (D) Number of subjects with at least one adverse event.
For Quality of life, we found a moderate effect in favor of acupuncture for both the mental health subdomain (SMD: 0.53; 95% CI 0.00 to 1.05; I2 = 90%, 4 studies, 796 participants) and physical health subdomains (SMD: 0.53; 95% CI 0.21 to 0.85; I2 = 73%, 4 studies, 796 participants; Figures 6A,B).
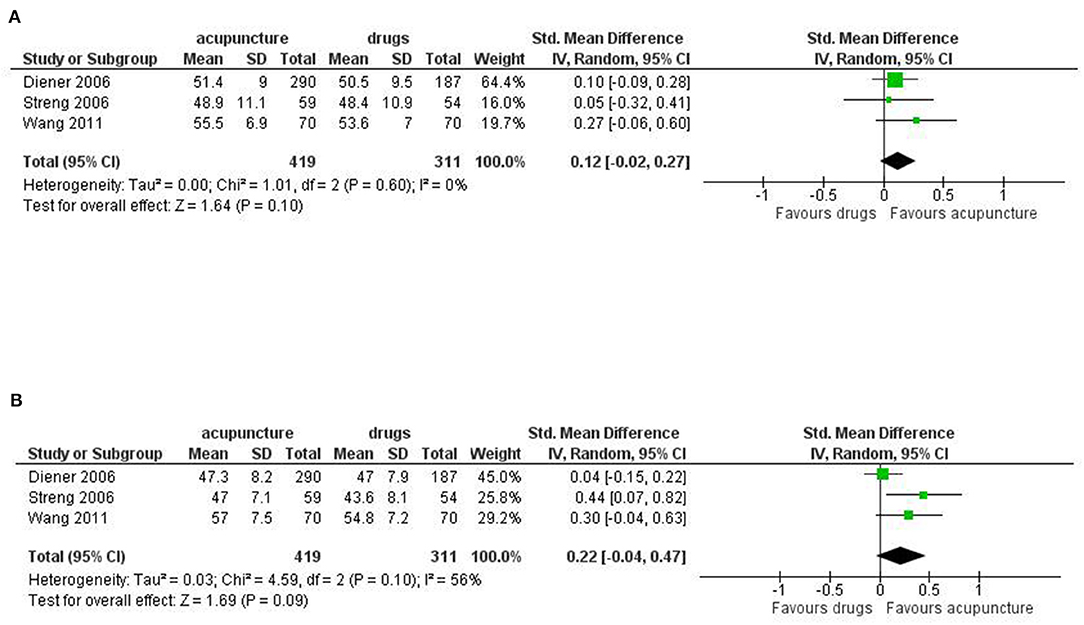
Figure 6. Forest plot of secondary outcomes—results at the end of the intervention. (A) Quality of Life: mental health; (B) Quality of Life: physical health.
Quality of evidence was moderate for number of subjects with at least one adverse event and quality of life and low for all the other secondary outcomes.
Subgroup analysis did not reveal important difference in all the primary outcomes between acupuncture of different intensity. However, there were too few studies in the subgroup to allow firm conclusion.
Results in favor of acupuncture were confirmed for the number of days with migraine per month (SMD: −0.46, 95% CI −0.86 to −0.05; I2 = 81%, 4 studies, 766 participants, moderate quality of evidence), response rate (RR: 1.57, 95% CI 1.01 to 2.42; I2 = 77%, 3 studies, 730 participants, moderate quality of evidence) pain intensity (SMD: −0.37, 95% CI −0.61 to −0.14; I2 = 48%, 3 studies, 730 participants, moderate quality of evidence; Figures 7A–C).
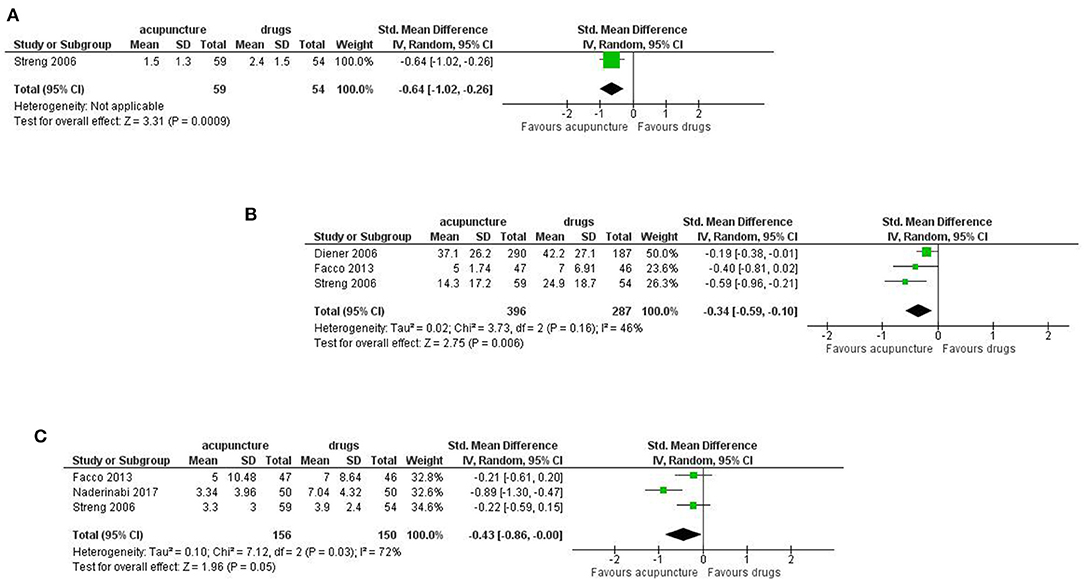
Figure 7. Forest plot of primary outcomes—results at longest available follow-up. (A) Number of days with migraine per months; (B) response rate to treatment; (C) Pain intensity.
For the secondary outcomes we found significant difference between treatments in the frequency of migraine attack per month (SMD: −0.64, 95% CI −1.02 to −0.26; 1 study, 113 participants); disability (SMD: −0.34, 95% CI −0.59 to −0.10; I2 = 46%, 3 studies, 683 participants); use of rescue medication (SMD: −0.43, 95% CI −0.86 to −0.00; I2 = 72%, 3 studies, 306 participants; Figures 8A–C).
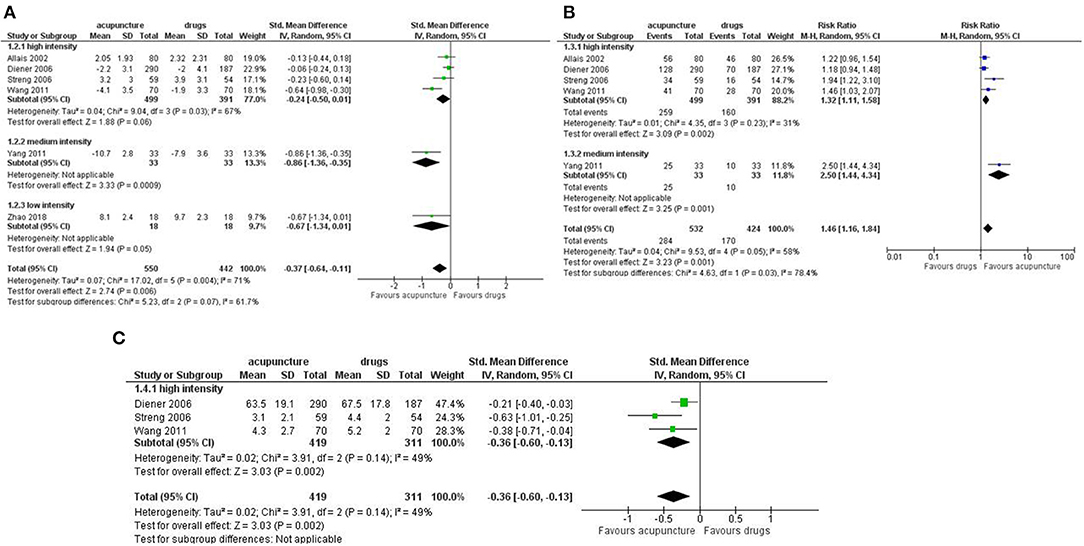
Figure 8. Forest plot of secondary outcomes—results at longest available follow up. (A) Frequency of migraine attack per month; (B) Disability; (C) Use of rescue medication.
At follow up no significant difference was found for Quality of Life, both the mental health subdomain (SMD: 0.12, 95% CI −0.02 to 0.27; I2 = 0%, 3 studies, 730 participants) and physical health subdomains (SMD: 0.22; 95% CI −0.04 to 0.47; I2 = 56%, 3 studies, 730 participants; Figures 9A,B).
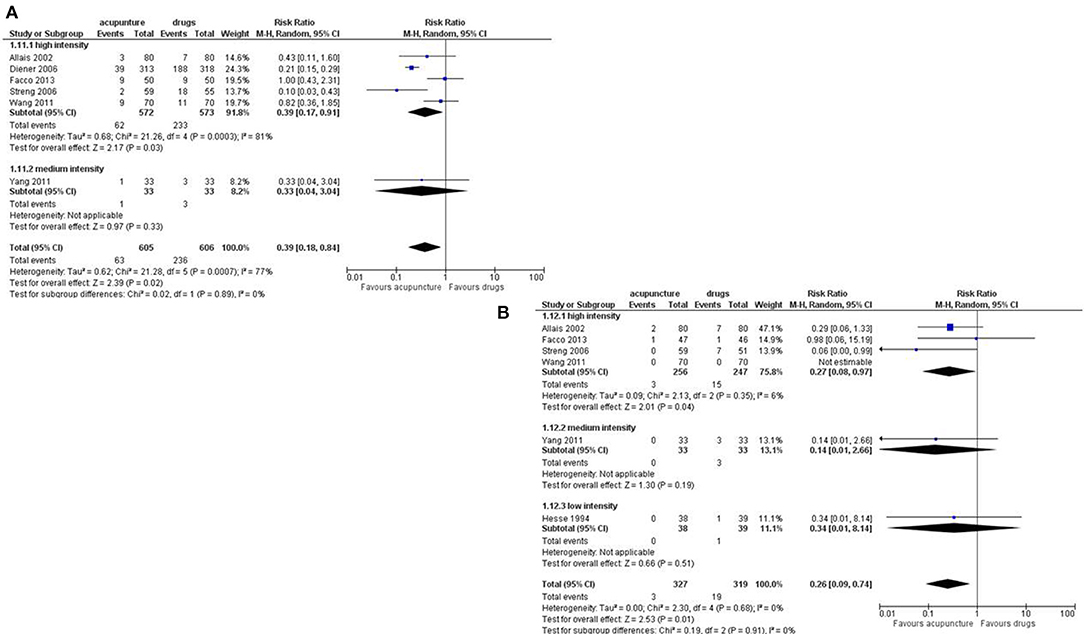
Figure 9. Forest plot of secondary outcomes—results at longest available follow up. (A) Quality of Life: mental health; (B) Quality of Life: physical health.
We included in our meta-analysis 9 studies, with a total of 1,484 participants that compared acupuncture with pharmacological prophylaxis for the prevention of migraine attacks in adults with chronic or episodic migraine. We found moderate quality of evidence that acupuncture is mildly more effective than any pharmacological prophylaxis in reducing the days with migraine per month, pain intensity, drop out from treatment, though the magnitude of the differences was small. We also found moderate quality of evidence that acupuncture is more effective than pharmacological prophylaxis in increasing the response rate to treatments and quality of life, but the magnitude of the differences was small. Conversely, we found moderate quality of evidence of a strong reduction in favor of acupuncture in both the dropout rate due to any and in the dropout rate due to adverse event.
Studies comparing true acupuncture vs. sham acupuncture in all its forms: superficial needling of “true” points (superficial needling of the acupoints for the treated condition), non-acupuncture' points (needling non-acupoints), “irrelevant” acupoints (needling of the acupoints not for the treated condition), “placebo needles” (devices that mimic acupuncture without skin penetration but pressing the skin) (45) have not been included, because sham acupuncture has already been proved not to be a placebo. Back in 2006, Lund et al. demonstrated that “the light touch of the skin stimulated mechanoreceptors coupled to slow conducting unmyelinated (C) afferents resulting in activity in the insular region, but not in the somatosensory cortex. Activity in these C tactile afferents was suggested to induce a ‘limbic touch’ response resulting in emotional and hormonal reactions” (46).
Many control procedures that were meant to be inert were likely to be activating these C tactile afferents and consequently resulted in the alleviation of the affective component of pain (46).
In the following years, numerous studies showed that sham acupuncture is just as effective as true acupuncture for the treatment of migraine (16); in addition, it may induce a wide range of peripheral, segmental, and central physiological responses to an unpredictable degree (43). Consequently, any intervention involving skin stimulation, whether it be penetration, pressure, or touch, cannot be considered an inert placebo (16, 31, 37, 38, 41, 43, 47).
Moreover, we chose to compare acupuncture against pharmacologic prophylaxis, instead of against sham acupuncture, to follow a more practical approach and provide a summary of the existing evidence that can be more useful in clinical practice as the pharmacologic prophylaxis is the most common treatment in usual care practice.
The most relevant flaws of the included studies were lack of blinding in all but two studies and the high risk of attrition bias in three studies. Overall, the certainty of evidence was judged moderate according to the GRADE approach for all the primary outcomes. A further limitation of some of the included studies is the short duration of treatment (4 weeks) and the short duration of follow up, as the effect of the medication might not be developed yet and acupuncture treatment usually last for several months. It should be noted that, in the studies with shorter follow-up the difference in treatment effect may be related to the faster mechanism of action of acupuncture compared to that of pharmacological prophylaxis. On the basis of the comparative studies currently in the literature, it was not possible to refer to very short windows of action, because these have not been considered by the authors. The exact onset of the prophylactic effect is not easily measurable and has not, however, been the subject of the studies we have considered in our review.
The two most recent SRs that addressed this topic were Linde et al. (16) and Zhang et al. (18).
Linde et al. is a Cochrane systematic review, well-conducted, but not updated since 2016, and Zhang et al. did not pool data across studies.
The strength of our review relies in a comprehensive bibliographic search on several databases without time restriction and in the rigor of the methodology that followed the highest standards as recommended by Cochrane (24).
Our review has some limitations. We limited our inclusion criteria to studies published in western languages due to our inability to translate studies published in Chinese or other eastern languages. Given the widespread use of acupuncture in Eastern countries and particularly in China, we probably missed some studies that made our comparison of interest. An overview of systematic reviews recently published described 14 systematic reviews that assess the efficacy of acupuncture against sham acupuncture or pharmacologic prophylaxis; we retrieved the full text of such reviews to look for trials which we could have missed. Unfortunately, eight of these reviews were written in Chinese and included primary studies written in Chinese as well so we were unable to evaluate the included studies.
Furthermore, a limitation of some of the included studies is the short duration of treatment (4 weeks) and the short duration of follow up, as the effect of the medication might not be developed yet and acupuncture treatment usually last for several months. Finally, we were unable to visually inspect funnel plot for the presence of possible publication bias because if <10 studies are included in meta-analysis, the funnel plot in considered uninformative (24).
The major flaws of most retrieved studies were the lack of blinding, that poses the efficacy results at high risk of performance and detection bias. Studies that adopt a double blind, double dummy design could provide unbiased estimates of efficacy results, though, due to the nature of the intervention, a double-blind trial is hard to be conducted.
Based on moderate certainty of evidence, we conclude that acupuncture is mildly more effective and much safer than medication for the prophylaxis of migraine.
The original contributions generated in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
SM and MC conceptualized and designed the study, screened studies from title and abstract, extracted data from included studies, assesses risk of bias, undertook data analysis, evaluated the certainty of evidence, and drafted the initial manuscript. CG, SC, and AM wrote the introduction and the discussion. All review authors contributed to writing and revising the final manuscript.
The project was funded by the Federazione Italiana delle Società di Agopuntura (FISA).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank Vanna Pistotti and Veronica Andrea Fittipaldo (Istituto di Ricerche Farmacologiche Mario Negri, Milan, Italy) for their support in literature search and reference formatting.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2020.576272/full#supplementary-material
Supplementary Material 1. Search strategy.
1. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. (2018) 38:1–211. doi: 10.1177/0333102417738202
2. GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2018) 17:954–76. doi: 10.1016/S1474-4422(18)30322-3
3. Leonardi M, Raggi A. A narrative review on the burden of migraine: when the burden is the impact on people's life. J Headache Pain. (2019) 20:41. doi: 10.1186/s10194-019-0993-0
4. Yuan H, Spare NM, Silberstein SD. Targeting CGRP for the prevention of migraine and cluster headache: a narrative review. Headache. (2019) 59:20–32. doi: 10.1111/head.13583
5. Li QQ, Shi GX, Xu Q, Wang J, Liu CZ, Wang LP. Acupuncture effect and central autonomic regulation. Evid Based Complement Alternat Med. (2013) 2013:267959. doi: 10.1155/2013/267959
6. Gao Z, Giovanardi CM, Li H, Hao C, Li Q, Zhang X, et al. Acupuncture for migraine: a protocol for a meta-analysis and meta-regression of randomised controlled trials. BMJ Open. (2019) 22:8. doi: 10.1136/bmjopen-2018-022998
7. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. (2008) 85: 355–75. doi: 10.1016/j.pneurobio.2008.05.004
8. Han JS. Acupuncture and endorphins. Neurosci Lett. (2004) 361: 258–61. doi: 10.1016/j.neulet.2003.12.019
9. Huang C, Wang Y, Han JS, Wang Y. Characteristics of electroacupuncture-induced analgesia in mice: variation with strain, frequency, intensity and opioid involvement. Brain Res. (2002) 945:20–5. doi: 10.1016/S0006-8993(02)02503-9
10. Goldman N, Chen M, Fujita T, Xu Q, Peng W, Liu W, et al. Adenosine A1 receptors mediate local anti-nociceptive effects of acupuncture. Nat Neurosci. (2010) 13:883–8. doi: 10.1038/nn.2562
11. Silberstein SD. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the quality standards subcommittee of the American academy of neurology. Neurology. (2000) 55:754–62. doi: 10.1212/wnl.55.6.754
12. Zhao LP, Liu L, Pei P, Qu ZY, Zhu YP, Wang LP. Electroacupuncture at Fengchi (GB20) inhibits calcitonin gene-related peptide expression in the trigeminovascular system of a rat model of migraine. Neural Regen Res. (2017) 12:804–11. doi: 10.4103/1673-5374.206652
13. Li Z, Liu M, Lan L, Zeng F, Makris N, Liang Y, et al. Altered periaqueductal gray resting state functional connectivity in migraine and the modulation effect of treatment. Sci Rep. (2016) 6:20298. doi: 10.1038/srep20298
14. Langevin HM, Churchill DL, Cipolla MJ. Mechanical signalling through connective tissue: a mechanism for the therapeutic effect of acupuncture. FASEB J. (2001) 15: 2275–82. doi: 10.1096/fj.01-0015hyp
15. Linde K, Allais G, Brinkhaus B, Fei Y, Mehring M, Vertosick EA, et al. Acupuncture for the prevention of episodic migraine. Cochrane Database Syst Rev. (2016) 6:CD001218. doi: 10.1002/14651858.CD001218.pub3
16. Linde K, Allais G, Brinkhaus B, Manheimer E, Vickers A, White AR. Acupuncture for migraine prophylaxis. Cochrane Database Syst Rev. (2009) 1:CD001218. doi: 10.1002/14651858.CD001218.pub2
17. Burke A, Upchurch DM, Dye C, Chyu L. Acupuncture use in the united states: findings from the national health interview survey. J Altern Complement Med. (2020) 12:7. doi: 10.1089/acm.2006.12.639
18. Zhang N, Houle T, Hindiyeh N, Aurora SK. Systematic review: acupuncture vs standard pharmacological therapy for migraine prevention. Headache. (2019) 60:309–17. doi: 10.1111/head.13723
19. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 21:e1000097. doi: 10.1371/journal.pmed.1000097
20. Hooker SA. SF-36. In: Gellman MD, Turner JR, editors. Encyclopedia of Behavioral Medicine. New York, NY: Springer (2013).
21. SF-12v2. In: Michalos AC, editor. Encyclopedia of Quality of Life and Well-Being Research. Dordrecht: Springer (2014).
22. Stewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN. Validity of the Migraine Disability Assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain. (2000) 88:41–52. doi: 10.1016/S0304-3959(00)00305-5
23. Soer R, Koke AJ, Vroomen PC, Stegeman P, Smeets RJ, Coppes MH, et al. Extensive validation of the pain disability index in 3 groups of patients with musculoskeletal pain. Spine (Phila Pa 1976). (2013) 38:E562–8. doi: 10.1097/BRS.0b013e31828af21f
24. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ. editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0. (2019). Available online at: https://training.cochrane.org/handbook#how-to-cite
25. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Earlbaum Associates (1988).
26. Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre; The Cochrane Collaboration (2014).
27. MacPherson H, White A, Cummings M, Jobst KA, Rose K, Niemtzow RC, et al. Standards for reporting interventions in controlled trials of acupuncture: the STRICTA recommendations. J Altern Complement Med. (2002) 8:85–9. doi: 10.1089/107555302753507212
28. White A, Cummings M, Barlas P, Cardini F, Filshie J, Foster NE, et al. Defining an adequate dose of acupuncture using a neurophysiological approach—a narrative review of the literature. Acupunct Med. (2008) 26:111–20. doi: 10.1136/aim.26.2.111
29. MacPherson H, Maschino AC, Lewith G, Foster NE, Witt CM, Vickers AJ, et al. Characteristics of acupuncture treatment associated with outcome: an individual patient meta-analysis of 17,922 patients with chronic pain in randomised controlled trials. PLoS ONE. (2013) 8:e77438. doi: 10.1371/journal.pone.0077438
30. Sun N, Tu JF, Lin LL, Li YT, Yang JW, Shi GX, et al. Correlation between acupuncture dose and effectiveness in the treatment of knee osteoarthritis: a systematic review. Acupunct Med. (2019) 37:261–7. doi: 10.1136/acupmed-2017-011608
31. Naderinabi B, Saberi A, Hashemi M, Haghighi M, Biazar G, Gharehdaghi F, et al. Acupuncture and botulinum toxin a injection in the treatment of chronic migraine: a randomized controlled study. Caspian J Intern Med. (2017) 8:196–204. doi: 10.22088/cjim.8.3.196
32. Schünemann H, Brozek J, Guyatt G, Oxman A editors. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. The GRADE Working Group (2013). Available online at: https://guidelinedevelopment.org/handbook
33. Schünemann H, Oxman A, Higgins J, Vist G, Glasziou P, Guyatt G. Chapter 11: presenting results and ‘Summary of findings’ tables. In: Higgins JP, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (2011). Available online at: https://handbook-5-1.cochrane.org/chapter_11/11_presenting_results_and_summary_of_findings_tables.htm
34. Facco E, Liguori A, Petti F, Zanette G, Coluzzi F, De Nardin M, et al. Traditional acupuncture in migraine: a controlled, randomized study. Headache. (2008) 48:398–407. doi: 10.1111/j.1526-4610.2007.00916.x
35. Jena S, Witt CM, Brinkhaus B, Wegscheider K, Willich SN. Acupuncture in patients with headache. Cephalalgia. (2008) 28:969–79. doi: 10.1111/j.1468-2982.2008.01640.x
36. Liu L, Zhao L, Zhang CS, Zeng L, Wang K, Zhao J, et al. Acupuncture as prophylaxis for chronic migraine: a protocol for a single-blinded, double-dummy randomised controlled trial. BMJ Open. (2018) 8:e020653. doi: 10.1136/bmjopen-2017-020653
37. Allais G, De Lorenzo C, Quirico PE, Airola G, Tolardo G, Mana O, et al. Acupuncture in the prophylactic treatment of migraine without aura: a comparison with flunarizine. Headache. (2002) 42:855–61. doi: 10.1046/j.1526-4610.2002.02203.x
38. Diener HC, Kronfeld K, Boewing G, Lungenhausen M, Maier C, Molsberger A, et al. Efficacy of acupuncture for the prophylaxis of migraine: a multicentre randomised controlled clinical trial. Lancet Neurol. (2006) 5:310–6. doi: 10.1016/S1474-4422(06)70382-9
39. Facco E, Liguori A, Petti F, Fauci AJ, Cavallin F, Zanette G. Acupuncture versus valproic acid in the prophilaxis of migraine without aura: a prospective controlled study. Minerva Anestesiol. (2013) 79:634–72.
40. Hesse J, Møgelvang B, Simonsen H. Acupuncture versus metoprolol in migraine prophylaxis: a randomized trial of trigger point inactivation. J Intern Med. (1994) 235: 451–6. doi: 10.1111/j.1365-2796.1994.tb01102.x
41. Streng A, Pfaffenrath V, Hammes M, Wagenpfeil S, et al. Effectiveness and tolerability of acupuncture compared with metoprolol in migraine prophylaxis. Headache. (2006) 46: 1492–502. doi: 10.1111/j.1526-4610.2006.00598.x
42. Wang LP, Zhang XZ, Guo J, Liu HL, Zhang Y, Liu CZ, et al. Efficacy of acupuncture for migraine prophylaxis: a single-blinded, double-dummy, randomized controlled trial. Pain. (2011) 152:1864–71. doi: 10.1016/j.pain.2011.04.006
43. Yang CP, Chang MH, Liu PE, Li TC, Hsieh CL, Hwang KL, et al. Acupuncture versus topiramate in chronic migraine prophylaxis: a randomized clinical trial. Cephalalgia. (2011) 31:1510–21. doi: 10.1177/0333102411420585
44. Zhao Z, Jia-hong SE, Guang SHI, Ning LI. The observation on different effectiveness between the embedding needle therapy and medication in the preventative treatment of chronic migraine. World J Acupunct Moxib. (2018) 25:242–5. doi: 10.1016/j.wjam.2018.12.006
45. Lund I, Näslund J, Lundeberg T. Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist's perspective. Chin Med. (2009) 4:1–9. doi: 10.1186/1749-8546-4-1
46. Lund I, Lundeberg T. Are minimal, superficial or sham acupuncture procedures acceptable as inert placebo controls? Acupunct Med. (2006) 24:13–5. doi: 10.1136/aim.24.1.13
Keywords: acupuncture—therapy, pharmacological prophylaxis, migraine, systematic review, RCTs
Citation: Giovanardi CM, Cinquini M, Aguggia M, Allais G, Campesato M, Cevoli S, Gentili F, Matrà A and Minozzi S (2020) Acupuncture vs. Pharmacological Prophylaxis of Migraine: A Systematic Review of Randomized Controlled Trials. Front. Neurol. 11:576272. doi: 10.3389/fneur.2020.576272
Received: 25 June 2020; Accepted: 06 November 2020;
Published: 15 December 2020.
Edited by:
Tim P. Jürgens, University Hospital Rostock, GermanyReviewed by:
Andreas Straube, Ludwig Maximilian University of Munich, GermanyCopyright © 2020 Giovanardi, Cinquini, Aguggia, Allais, Campesato, Cevoli, Gentili, Matrà and Minozzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlo Maria Giovanardi, Z2lvdmFuYXJkaWNhcmxvQGxpYmVyby5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.