 Aline Gauchat1,2
Aline Gauchat1,2 Antonio Zadra2
Antonio Zadra2 Mira El-Hourani2,3
Mira El-Hourani2,3 Sophie Parent4Richard E. Tremblay2,3,5,6
Sophie Parent4Richard E. Tremblay2,3,5,6 Jean R. Séguin3,7*
Jean R. Séguin3,7*- 1Clinique de Consultation Conjugale et Familiale Poitras-Wright, Côté, Longueuil, QC, Canada
- 2Department of Psychology, Université de Montréal, Montreal, QC, Canada
- 3CHU Ste-Justine Research Center, Montreal, QC, Canada
- 4School of Psychoeducation, Université de Montréal, Montreal, QC, Canada
- 5Department of Pediatrics, Université de Montréal, Montreal, QC, Canada
- 6School of Public Health, University College Dublin, Dublin, Ireland
- 7Department of Psychiatry and Addictology, Université de Montréal, Montreal, QC, Canada
Although frequent disturbing dreams, including bad dreams and nightmares, have been repeatedly associated with poor psychological well-being in adults, considerably less information exists on their psychosocial correlates in children. Recent empirical and theoretical contributions suggest that the association between disturbing dream frequency and psychosocial adaptation in children may differ as a function of children's negative emotionality. The current study assessed the moderating effect of very early negative emotionality (17 months of age) in the relation between disturbing dream frequency and psychosocial maladjustment (i.e., externalizing + internalizing behaviors) in a sample of 173 11-year-old children. Mixed-model analyses revealed that disturbing dream frequency was associated with some internalizing behaviors but that the association between disturbing dream frequency and most externalizing behaviors was moderated by early negative emotionality. The latter result indicates that the relation between disturbing dream frequency and externalizing behaviors was significant in 11-year-old children showing moderate negative emotionality early in life, but particularly strong in those children with high early negative emotionality. Whereas, a moderating effect of early negative emotionality was not found between disturbing dream frequency and internalizing behaviors, the findings highlight the more specific role of early emotional negativity as a developmental moderator for the link between disturbing dreams and externalizing behaviors in children. The results are discussed in light of recent models of disturbed dreaming production.
Introduction
Up to 20% of children experience psychosocial adjustment difficulties (1, 2) which are typically divided between externalizing and internalizing problems (3, 4), although both categories evince common and unique risk factors (5). Studies show that while good sleep quality is associated with optimal behavior development, poor sleep is related to both externalizing and internalizing problems (6–17). Even after controlling for other risk factors, sleep problems appear to explain a small but significant proportion of the variance in both externalizing and internalizing behaviors (15, 18). However, different sleep problems appear to be associated with different externalizing or internalizing problems (6, 19).
Among these sleep problems, disturbing dreams (DDs; vivid dreams marked by intense negative emotions such as fear, anxiety, and anger) are frequently experienced by children (20–24). DDs may be associated with a wide range of psychosocial difficulties as they may signal problems with emotional regulation processes that normally occur during sleep as well as in dreams (for more details about this hypothesis, see (22, 25–28). While frequent DDs, including bad dreams and nightmares, have been repeatedly associated with poor psychological well-being and increased psychopathology in clinical and non-clinical adult populations (27), considerably less information exists on their psychosocial maladjustment correlates in children.
A recent review of the literature suggests that the occurrence of frequent DDs during childhood and adolescence is associated with a range of difficulties (21). First, DD frequency is associated with other sleep-related problems including insomnia, sleepwalking, bruxism, sleep talking, sleep terrors, nighttime awakenings, and unwillingness to go to bed (29–37). Second, DDs have also been linked to a range of specific mental health symptoms and psychosocial problems, including low prosociality (37, 38), academic problems (33), emotional excitability and being easily emotionally hurt (39), emotional symptoms (37, 38, 40), psychotic experiences (41, 42), borderline personality disorder (40), other mental health disorders (43), as well as suicidal ideation and suicide attempts (44–46). A prospective study found that DD frequency at 12 years of age was related to symptoms of psychosis during adulthood (47).
Moreover, DD frequency has been associated with internalizing problems in childhood and adolescence and repeatedly linked to anxiety (6, 48–54). Prospective studies of adolescents and late teenagers have similarly revealed links between parent-rated DDs at 10–19 years of age and later symptoms of anxiety and depression at 18–32 years of age (55). Moreover, DD frequency has also been linked to externalizing problems. Indeed, some studies of children show that DDs are associated with conduct disorders (37), rule-breaking, aggression, impulsivity (56), and hyperactivity (37, 57, 58). However, other studies did not find these associations (38, 59). Some studies also reported significant associations between DD frequency and attention deficit hyperactivity disorder (ADHD) (60) as well as with ADHD subtypes (61, 62), and one prospective study found that parent-rated DDs at 10–19 years of age predicted symptoms of inattention and direct/indirect aggression at 18–32 years of age (55).
Finally, some studies reviewed above combine sleep-related difficulties into one construct, thus not taking into account the differential relations of each sleep problem with unique measures of daytime functioning (16, 63, 64). Thus, whether or not DDs are related equally across internalizing and externalizing problems remains to be determined.
To further clarify inconsistencies in the literature, the construct of “affect distress,” defined as a trait-like disposition to react to emotional stressors with heightened negative affect and distress (27, 65) should be taken into account as it may play a role in the association between DDs and psychosocial adjustment difficulties. First, Levin and Nielsen's (27) model of DD production proposes that DDs occur out of an interaction between “affect load,” or day-to-day variations in emotional stress, and the aforementioned construct of affect distress, which can be viewed as a temperament subtype. Affect distress would fall under the negative emotionality dimension of temperament (66, 67). In the developmental literature, negative emotionality encompasses individual differences in typical reactions to negative emotional experiences, which can be readily observed from birth (68, 69). In fact, negative emotionality was found to be stable from early childhood to early adolescence (70) and was found to have a moderate continuity 17 years later (3–20 years old) (71).
Second, negative emotionality or difficultness, which refers to the tendency to experience negative emotions (fear, anger, sadness, discomfort) and high emotional distress when confronted to novel, ambiguous, and intense situations (66), has been related to psychosocial maladjustment throughout infancy and childhood (72–74). Recently, it is its moderating effect that has been mainly reported in the literature. Indeed, difficultness is already known to moderate relations between a variety of risk factors and children's behavior, such as the associations between cumulative contextual risk and children's externalizing, internalizing, and sleep problems (75–78). Some early temperamental characteristics may indeed predispose children to develop later behavior problems, particularly when other risk factors are present (79–82).
Taken together, Nielsen and Levin's (22) model of DD production and developmental literature on temperament suggests that the link between the frequency of DDs and psychosocial adaptation may differ as a function of a child's negative emotionality. This hypothesized moderator effect of negative emotionality has never been empirically tested. Furthermore, there is a lack of data on the relation between DDs and externalizing problems, and most studies of DDs in children suffer from one of the following three methodological limitations. First, DD frequency in children is often assessed through parent reports, despite the fact that this method has been shown to underestimate DD frequency and distress in comparison to child self-reports (37, 48, 50, 83). Second, many studies did not include any adjustment for possible confounding factors, such as risk factors common to both psychopathology and DDs (e.g., socio-economic status or comorbid sleep problems), despite the fact that taking such factors into account has been shown to attenuate observed associations (84). Third, and finally, although it is important to measure children's psychosocial maladjustment through multiple informants due to differences in child behavior across contexts (58, 85), multiple informants have rarely been used in the reviewed studies (21).
The goal of the present study was to first investigate the relationship between DD frequency and psychosocial maladjustment in children across a wide range of internalizing and externalizing behaviors and, second, to take into account the possible moderator effect of early emotional negativity. Methodological shortcomings characteristic of many studies in the field were also addressed: (a) measures of DD frequency were obtained from the children themselves, (b) socio-economic status and co-morbid sleep disorders were taken into account in the analyses, and (c) children's psychosocial maladjustment was assessed through multiple informants.
Two main and complementary predictions were tested: (1) DD frequency will be positively associated with psychosocial maladjustment across several internalizing and externalizing behavioral domains; and (2) negative emotionality will moderate this relation between measures of DD frequency and psychosocial maladjustment across several internalizing and externalizing behavioral domains. Specifically, we tested the hypothesis that the association between DD frequency and internalizing and externalizing problems would be strengthened with increasing levels of negative emotionality. These hypotheses will be tested separately for each internalizing (anxiety, social withdrawal, and emotional problems) and externalizing (opposition, physical aggression, reactive, proactive aggression, indirect aggression, and ADHD) symptoms.
Materials and Methods
Participants
Participants were part of a longitudinal study focusing on the social, psychological, and cognitive development of children from urban socio-economic backgrounds in the province of Québec, Canada. At the study's inception, 1,000 families were randomly selected from the Québec 1996–1997 birth register (86). Of these, 572 consented to participate in the original study and were then assessed annually in French (~82%) or English (Canada's two official languages) from the age of 5 months. Due to annual attrition, variability in the participants' year to year availability for data collection, and funding constraints which limited the capacity to follow-up all families, a total of 173 children (comprised equally of boys and girls) completed the present study (mean age = 11.4 years, SD = 0.1). These 173 children did not differ from the remainder of the original 572 5-month-old children in terms of their socio-economic level, including family income (p = 0.68), family type (single parent or not; p = 0.57), maternal level of education (p = 0.33), or negative emotionality at 17 months of age (p = 0.54). They did not differ on other behavioral measures at 17 months in term of hyperactivity (p = 0.73); inattention (p = 0.89); emotional troubles (p = 0.77); anxiety (p = 0.74); physical aggression (p = 0.71), except for opposition with children in the current sample being a little less oppositional (M = 3.2; SD = 1) than the remainder of the sample (M = 3.5; SD = 1.1); t = 2.8; p < 0.05.
Measures
Assessment of Disturbing Dreams
Participants from this longitudinal sample self-reported about their DDs for the first time at 11 years of age. The instructions to children referred to DDs using the expression “bad dreams” (defined as very disturbing dreams) because the term DD was too unfamiliar to them given their age. Children were required to answer the question: “On average, how frequently do you have bad dreams?” using the following choices: “Never,” “Sometimes,” “Often,” “Always,” or “Don't know.” Participants reporting bad dreams were also asked to estimate the number of bad dreams experienced over the past month. For children who reported “never” in the previous question, the number of bad dreams was coded as 0 while maximum frequency was set at 30 (i.e., 1 DD/day) to limit the impact of potential outliers. Thus, values for monthly DD frequency ranged between 0 and 30. A 1-month retrospective frequency estimate was used instead of a 1-year estimate as it has been shown to correspond more closely to prospectively collected log-based frequency measures of DDs from the same individuals (87, 88).
Measures of Psychosocial Maladjustment
Psychosocial maladjustment was measured using a battery of validated scales (89–91) drawn from various instruments. Some scales from the Preschool Behavior Questionnaire (92), the Child Behavior Checklist (93), and the Reactive and Proactive Aggression Questionnaire (94) were used to create the questionaire. The scales (and mean Cronbach alpha across informants) included measures of both internalizing problems: anxiety (4 items, Mα = 0.72, e.g., being nervous, high-strung or tense), social withdrawal (3 items, Mα = 0.68, e.g., prefers to play alone rather than with other children), and emotional problems (3 items, Mα = 0.69, e.g., has trouble enjoying him or herself); and externalizing problems: opposition (3 items, Mα = 0.51, e.g., punishment doesn't change the child's behavior), physical aggression (4 items, Mα = 0.75, e.g., physically aggresses people), reactive aggression (4 items, Mα = 0.75, e.g., reacts aggressively when someone takes a personal belonging, for example by hitting, pushing, or slapping another child), proactive aggression (3 items, Mα = 0.55, e.g., scares other children to get what is wanted), indirect aggression (3 items, Mα = 0.69, e.g., when angry at someone, tries to get others to dislike the other person), and ADHD symptoms (7 items, Mα = 0.86, e.g., cannot settle on anything for more than a few moments; is impulsive/acts without thinking; is inattentive). These validated scales (89, 91) have been shown to be sensitive to various environmental, familial, and perinatal risk and protective factors (95–99) as well as to early sleep patterns (100). The instrument was completed by the participants themselves at 11 years of age as well as by each child's father and teacher in order to get a complete description of their difficulties across the social context. Questions for the child version were read to them by the research assistant but they could record answers confidentially.
Covariables
Socio-Economic Status
Three variables were used to evaluate each family's socio-economic status: family income (continuous variable), level of maternal education (dichotomous variable, with a high level being defined as having a secondary school diploma or higher), and whether or not the child was in a single-parent family (dichotomous variable).
Sleep
Two sleep-related variables were included: sleepwalking, since this sleep disorder has been repeatedly associated with DDs (29, 33, 34, 39, 57) and daytime somnolence because poor sleep quality (which usually leads to daytime somnolence) is associated with poor mood and behaviors (6, 100, 101). Two questions to the mother were “Does your child sleepwalk in his/her sleep?” and “In general, is your child sleepy during the day?” Both could be answered with “Never,” “Sometimes,” “Often,” or “Always.”
Negative Emotionality
Negative emotionality was assessed at 17 months using a shortened scale developed by Vitaro and colleagues (102) of the original fussy/difficult temperament scale developed by Bates and colleagues (103) (example of item: intensity of the child's protest). This seven-item scale was completed by the mother, in order to avoid a shared-method variance problem with the informants who completed the psychosocial adjustment measures for our analyses (102). The measure of negative emotionality used in the present study showed good internal consistency with a Cronbach alpha of 0.71.
Procedure
Each parent, or legal guardian responsible for the child, and teacher received an invitation by mail to participate in the study. Consent was obtained from parents or legal guardians and assent was obtained from the child. The study was approved by the Research Ethics Committee of the CHU Ste-Justine Research Center, and the study protocol also complied with the ethical guidelines of the American Psychological Association (“Ethical Principles of Psychologists and Code of Conduct,” 2017).
Analyses
Model used: Mixed-effects model analyses were estimated using the “Statistical Package for the Social Sciences” (Version 18) (104) to investigate relationships between DDs and dimensions of psychosocial maladjustment. Nine models were tested, one for each measure of psychosocial maladjustment, three for internalizing problems, and six for externalizing problems. Specifically, responses provided by the three informants (child, teacher, and father) were included for each psychosocial maladjustment scale within the mixed-effects models where each of the informants represents a repeated component. A mixed-effects model as opposed to a traditional repeated-measure ANOVA allows for an unbalanced design. This model is also adapted for situations with unequal covariance as it does not assume equal correlations across informants. In a mixed-effects model, if one or two informants are missing, the other informants are still included in the analyses, whereas traditional repeated-measures ANOVA requires data from all three informants for each participant entered in the analyses. Thus, the mixed-effect model actually uses all the available information for parameter estimation (105). Responses were available from all three informants for 78 participants (42.6%)—from the child and teacher for 38 participants (22%), from the child and father for 32 participants (18.6%), and only from the child in 32 cases (18.6%). There was no systematic pattern of missing responses related to child behavior outcomes.
Preliminary Analyses
Sex differences on DD frequency measures were assessed with T-tests. Potential a priori covariates were selected for inclusion in the analyses on an empirical basis in order to enter only meaningful variables and avoid loss of power (106) as it has been done in other studies (81). This was done by first computing correlations or ANOVAs between potential control variables (socioeconomic status; SES, sleepwalking, somnolence) and outcome variables to determine which control variables should be entered as fixed effects for which outcome measures. If a potential control variable was related to an outcome variable (at p ≤ 0.05) assessed by at least one of the informants, it was entered in the analysis. Maternal level of education was thus entered in the analyses for anxiety, physical aggression, ADHD symptoms, and opposition, whereas family income was entered in the analyses for anxiety, ADHD symptoms, and opposition (for all those variables, a higher socio-economic status was linked to less psychosocial maladjustment). The family type and sleep disorder variables were not related to any of the psychosocial maladjustment measures. Whenever interactions between two variables were not significant, the interaction term was removed from the analytical model and only the main effect was tested.
Our two overarching hypotheses were tested using the mixed-effects model for each psychosocial maladjustment problem within internalizing and externalizing problems. Informant source and child sex were always entered as fixed effects. Interactions between DD measures and child sex or informant source were tested since children's behaviors can be perceived differently at school vs. at home and because behavioral difficulties differ between boys and girls (85, 107, 108), resulting in differences in observed associations between DDs and behavioral difficulties as a function of context and sex.
Interactions between DDs and early negative emotionality were investigated to test the second hypothesis which proposed that early negative emotionality moderates the relationship between DD frequency and psychosocial maladjustment. DD frequency and early negative emotionality were centered.
Results
Descriptive Statistics
Of the 173 children that completed the questionnaires, 129 (82.7%) reported experiencing at least one DD per month. The mean frequency of DDs reported per month by the entire sample was 3.6 (SD = 5.3), with 12% of the sample having 10 or more DD per month. A significantly greater proportion of girls (88.7%) reported having at least one DD in the last month than did boys (76.3%), χ2 = 4.21, p < 0.05. However, there were no significant sex differences in the actual number of DDs experienced in the past month. Using the MIXED models, none of the DDs by informant interactions were significant, and early negative emotionality was not correlated to DDs (r = 0.04; p = 0.58). Correlations between each informant for a given variable vary between r = 0.03 for opposition and r = 0.28 for anxiety with a mean of Mr = 0.17.
Before testing the moderating effect of early negative emotionality on each childhood-dependent variable, we examined its correlation with DDs to determine if it met the criteria for moderation analysis. DDs and early negative emotionality were not correlated (r = 0.04; p = 0.58). We also examined associations between early negative emotionality and dependent variables. Correlations ranged from r = 0.03 to r = 0.07 with a mean of Mr = 0.05 for internalizing behaviors, and they ranged from r = 0.05 to r = 0.20 with a mean of Mr = 0.09 for externalizing behaviors. None of those correlations were significant except the one between early emotional negativity and physical aggression (r = 0.19; p ≤ 0.05).
Associations Between DD Frequency and Internalizing Behaviors
When considering internalizing behaviors, none of the interactions between DDs and temperament were significant (all ps > 0.50). They were therefore removed from the models. Table 1 shows main effects and effect sizes for the association between DD frequency and internalizing problems once control variables were included in the statistical models. DD frequency was positively related to 2 of the 3 measures of internalizing behaviors (social withdrawal and emotional problems), with Cohen's d statistics of effect size for continuous variables in the small to medium range (109). This only partially supports the first hypothesis, as no moderating effect of early negative emotionality was found.
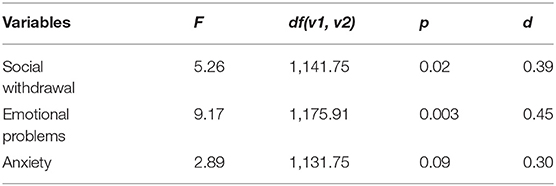
Table 1. Main effects of DD frequency on internalizing problems.
Associations Between DD Frequency and Externalizing Behaviors
The interaction term between early emotional negativity and DDs was kept in all models examining externalizing behaviors because p-values were consistently below 0.13 (ranging from 0.001 for proactive aggression and 0.13 for opposition), suggesting that this pattern was not random. Table 2 presents results of the analyses of main effects and interactions for each externalizing behavior. Figure 1 plots these interactions using the method proposed by Aiken and West (110) by showing the strength of the association between DD frequency and each dimension of externalizing behaviors plotted as a function of early negative emotionality level [low (−1 SD), average or high (+1 SD)]. As can be seen in Figure 1, the pattern of interactions was highly consistent across dimensions of externalizing behaviors, where associations between frequency of DDs and externalizing behaviors were systematically positive and significant for children with moderate to high levels of early negative emotionality. For these children, effect sizes were medium to large, ranging from d = 0.41 to d = 0.85 (109). This pattern of interactions and absence of main effects only partially supports the second hypothesis.
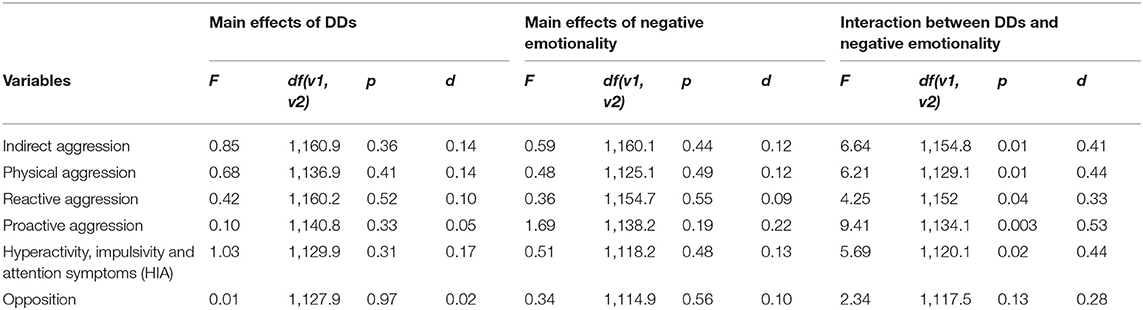
Table 2. Main effects of DD frequency and interactions with early negative emotionality for each externalizing behavior problem.
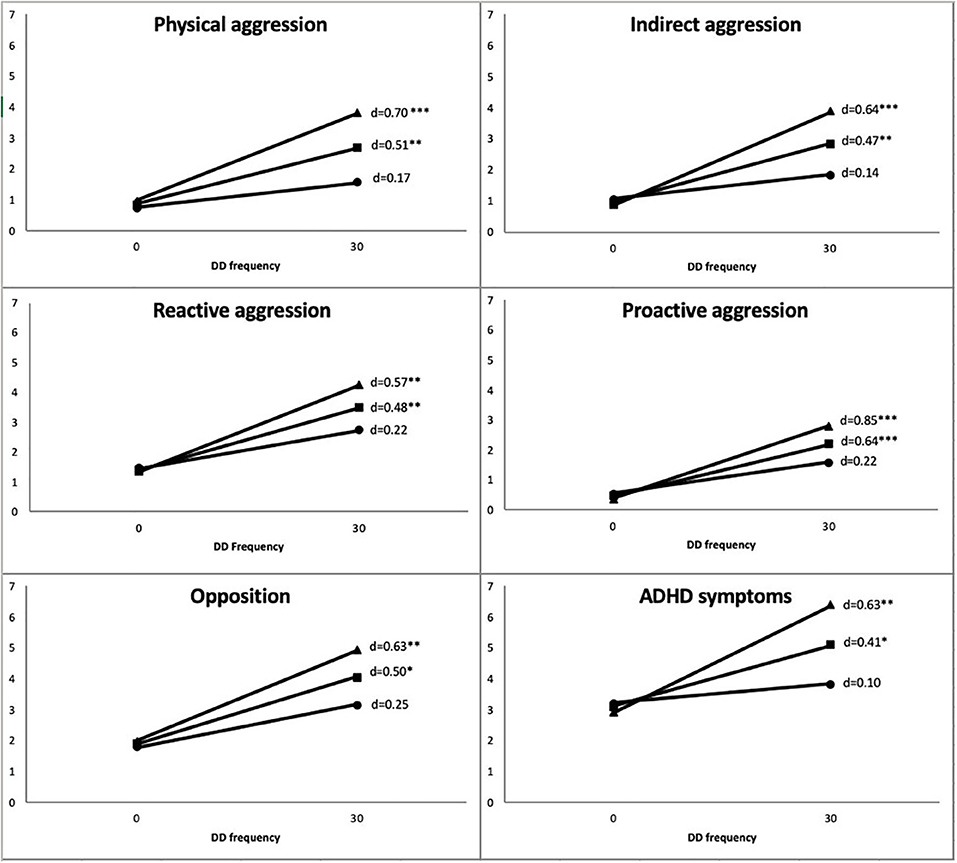
Figure 1. Strength of association between monthly DD frequency (x-axis) and externalizing behaviors (y-axis) as a function of averaged negative emotionality and ± 1 SD. *p < 0.05; **p < 0.01; ***p < 0.001. Externalizing behaviors were standardized across a range from 0 to 7. Monthly DD frequency ranged from 0 to 30.
Discussion
The results of the present study partially support our predictions that DD frequency would be positively associated with psychosocial maladjustment in children and that early emotional negativity would moderate this relationship. In line with previous adult and childhood literature, DD frequency was positively related to psychosocial maladjustment of the internalizing type: across informants, children with higher DD frequency scored higher on two of the three measures of internalizing problems (i.e., emotional problems and social withdrawal) without moderation by early emotional negativity. For psychosocial maladjustment of the externalizing type, there was a moderation effect of early emotional negativity: the association between DDs and externalizing difficulties was stronger with increasing levels of early emotional negativity.
The associations between DD frequency and internalizing behaviors remained significant even after adjusting for socio-economic and sleep-related variables. That DDs in children were associated with a range of internalizing problems (e.g., emotional problems and social withdrawal) is consistent with findings reported in children and adult populations (21, 27, 40, 56). However, unlike some reports, DD frequency in the present study was not significantly related to anxiety. The effect size for this relation (d = 0.30) was too small to reach statistical significance given our sample size. By comparison, effect sizes in previous studies have ranged between 0.20 and 0.72 (Md = 0.53) (49, 51, 53). Differences in measures of anxiety themselves (e.g., source of informant, symptoms scale vs. clinical diagnosis) may also partially account for this. The fact that none of the interactions with informants were significant shows that despite contextual differences in behaviors, the association between DDs and psychosocial maladjustment is robust and did not differ as a function of informant source.
The absence of the hypothesized moderator effect of early emotional negativity on internalizing problems may have been related to the measure used in the present study. Specifically, our measure of early emotional negativity at 17 months may not have been sensitive to the complete spectrum of manifestations of affect distress. For example, in contrast to observations in infants, studies have shown that toddlers high in emotional reactivity are more likely to manifest their reactivity through inhibition or withdrawal (111–114). These behavioral manifestations have been associated with later proneness to internalizing difficulties (79, 115–117). By contrast, our measure did not include items specifically formulated to detect these behavioral manifestations of early emotional reactivity, which might explain why it did not correlate with, or moderate, later internalizing difficulties. Thus, our measure may be more sensitive to behavioral manifestations of toddlers' “affect distress,” like aggression, that are linked to later externalizing problems than to subsequent internalizing problems.
The finding that early negative emotionality specifically moderated the relationship between DDs and externalizing behaviors is new. In fact, this is the first study to document that DDs in children with early moderate to high early emotional negativity are strongly associated with externalizing behaviors (with corresponding ds ranging between 0.60 and 0.90). The consistency of results across externalizing problems may be due to a common underlying factor (3, 118). How the relation between frequent DDs and externalizing behaviors in children with a history of moderate to elevated negative early emotionality evolves over time remains to be clarified. However, some studies have shown that early emotional negativity may moderate other associations implicating later externalizing behaviors, such as the relation between early child care and externalizing behaviors during adolescence (119). Another study (76) found that low early negative emotionality at 18 months emerged as a protective factor in children experiencing a cumulative risk of developing internalizing and sleep problems at 24 months. Consequently, and in the absence of a concurrent measure of negative emotionality, this long-term effect noted across several studies also supports the hypothesis that negative emotionality is a relatively stable developmental characteristic.
The correlational nature of our study does not allow us to draw conclusions about the direction of the link between DDs and psychosocial adjustment. On the one hand, it is possible that DDs have an impact on psychosocial adjustment as it has been shown that DDs could influence the dreamer's mood the following day (120). Frequent DDs in children could similarly result in negative emotions and distress during wakefulness much like the nightmare-related distress documented in adults (27, 121–123). Thus, it is possible that repeated and negative experiencing of DDs elicits negative reactive emotions during wakefulness.
On the other hand, it is also possible that psychosocial adjustment problems and related perceived stress may have an impact on the frequency of DDs (27, 124, 125). In this case, DDs would reflect issues and concerns experienced during wakefulness. Alternatively, it is possible that a third variable explains the relation between DDs and psychosocial adjustment. This would be consistent with suggestions that DDs represent a failure in the emotional regulation function believed to occur during normal dreaming (126–128). Psychosocial maladjustment problems are also known to be related to problems in emotional regulation (74, 129–131). As discussed earlier, this interpretation would be consistent with the hypothesis of a moderator effect of emotional negativity and DDs on psychosocial adjustment. While our study has some key strengths including the use of an early measure of negative emotionality, control variables, and multiple informants for the assessment of psychosocial maladjustment, it also has some shortcomings. With the exception of the children's early emotional negativity measure, this was essentially a cross-sectional correlational study, and as such, it cannot address the developmental sequence with regard to DDs and psychosocial maladjustment.
Longitudinal studies are needed to clarify the nature and time course of DDs in relation to psychosocial maladjustment. Also, as has been done in adults, the inclusion of measures of potentially more severe forms of maladjustment such as suicidality (which emerges in early adolescence) may be helpful as suicidal ideation has been linked to both internal distress and externalizing behaviors such as impulsivity and conduct disorders (132–134). In fact, one review found that impulsivity and emotional dysregulation could explain the link between sleep disturbances and suicidality (135). More studies should investigate these associations specifically with DDs. In addition, the study of other moderator variables could further our understanding of these complex developmental issues. Disorganized attachment, for instance, is a promising candidate as it has been related to both externalizing behaviors and DDs and could play a moderator role in these relations (136–139).
In sum, the present study highlights the role of early emotional negativity as a developmental moderator for the link between DDs and externalizing behaviors in children and points to the need to consider temperamental traits when investigating associations between DDs and internalizing and externalizing problems from a developmental perspective.
Data Availability Statement
Data may be available by completing a request on our website http://gripinfo.ca/grip/public/www/etudes/en/dadprocedures.asp?langue=en. All data requests are subject to current privacy laws guiding their ethical use in Québec, Canada, and examined by the CHU Ste-Justine Research Ethics committee.
Ethics Statement
The studies involving human participants were reviewed and approved by Research Ethics Committee of the CHU Ste-Justine Research Center. Written informed consent to participate in this study was provided by the adult informants themselves, the study participants' parents or legal guardian, and assent was provided by the children themselves.
Author Contributions
AG contributed to study design, analyzed the results, and wrote the manuscript draft. AZ obtained supporting grants, supervised the study, contributed to the statistical analyses, and reviewed the manuscript. ME-H reviewed the data collection and reviewed the manuscript. RT obtained supporting grants and contributed to the study design, data collection, and reviewed the manuscript. SP and JS obtained supporting grants, designed and supervised the study, contributed to the statistical analyses and their interpretation, and reviewed the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Canadian Institutes for Health Research via grant MOP 44072 to JS, grant MOP-97910 to JS and SP, and grant MOP 97865 to AZ; the Fonds de Recherche en Santé du Québec via the Réseau Santé Mentale du Québec (Québec Mental Health Network), fellowships to JS and grant 981055 to JS and RT, and grant 991027 to JS; the Social Sciences and Humanities Research Council of Canada, grants 839-2000-1008 to RT and JS and 410-2007-1957 to AZ; and the Fonds de Recherche du Québec – Société et Culture infrastructure grants 2002-RS-79238 (RT, JS, and SP), # 2009-RG-124779 and #2015-RG-178735 (both to RT and JS). ME-H was supported by the Fonds Maria et Georginia Daoussis and AG and JS were supported by the Fonds Monique Gaumond pour la recherche en maladies affectives.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This article was adapted from a study contained in the first author's doctoral thesis entitled Rêves dysphoriques et rêves récurrents chez les enfants et les adolescents: investigations cliniques et corrélats psychosociaux. The authors are grateful to Charles-Édouard Giguère for data management and statistical analyses, and to our partner, the Institut de la Statistique du Québec. We thank all the parents and children for their generous participation in the study.
References
1. Essex MJ, Kraemer HC, Slattery MJ, Burk LR, Boyce W, Woodward HR, et al. Screening for childhood mental health problems: outcomes and early identification. J Child Psychol Psychiatry. (2009) 50:562–70. doi: 10.1111/j.1469-7610.2008.02015.x
2. Fechete GL, Susa-Erdogan G, Benga O. Internalizing problems in a sample of Romanian preschool children. Contributions of both child and maternal temperament along with family functioning. Early Child Dev Care. (2018) 188:46–61. doi: 10.1080/03004430.2016.1266485
3. Castellanos-Ryan N, Brière FN, O'Leary-Barrett M, Banaschewski T, Bokde A, Bromberg U, et al. The structure of psychopathology in adolescence and its common personality and cognitive correlates. J Abnormal Psychol. (2016) 125:1039. doi: 10.1037/abn0000193
4. Cicchetti D, Toth LT (eds.). Internalizing and Externalizing Expressions of Dysfunction, Vol. 2. Hillsdale, NJ: Lawrence Erlbaum and Associates (1991).
5. Bayer JK, Ukoumunne OC, Lucas N, Wake M, Scalzo K, Nicholson JM. Risk factors for childhood mental health symptoms: National Longitudinal Study of Australian Children. Pediatrics. (2011) 128:e865–79. doi: 10.1542/peds.2011-0491
6. Alfano CA, Gamble AL. The role of sleep in childhood psychiatric disorders. Child Youth Care Forum. (2009) 38:327–40. doi: 10.1007/s10566-009-9081-y
7. Alfano CA, Ginsburg GS, Kingery JN. Sleep-related problems among children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry. (2007) 46:224–32. doi: 10.1097/01.chi.0000242233.06011.8e
8. Aronen ET, Paavonen E, Fjallberg M, Soininen M, Torronen J. Sleep and psychiatric symptoms in school-age children. J Am Acad Child Adolesc Psychiatry. (2000) 39:502–8. doi: 10.1097/00004583-200004000-00020
9. Becker SP, Luebbe AM, Langberg JM. Attention-deficit/hyperactivity disorder dimensions and sluggish cognitive tempo symptoms in relation to college students' sleep functioning. Child Psychiatry Hum Dev. (2014) 45:675–85. doi: 10.1007/s10578-014-0436-8
10. El-Sheikh M, Saini EK, Gillis BT, Kelly RJ. Interactions between sleep duration and quality as predictors of adolescents' adjustment. Sleep Health. (2019) 5:180–6. doi: 10.1016/j.sleh.2018.11.004
11. Gregory AM, Caspi A, Eley TC, Moffitt TE, O'Connor TG, Poulton R. Prospective longitudinal associations between persistent sleep problems in childhood and anxiety and depression disorders in adulthood. J Abnormal Child Psychol. (2005) 33:157–63. doi: 10.1007/s10802-005-1824-0
12. Gregory AM, O'Connor TG. Sleep problems in childhood: A longitudinal study of developmental change and association with behavioral problems. J Am Acad Child Adolesc Psychiatry. (2002) 41:964–71. doi: 10.1097/00004583-200208000-00015
13. Gregory AM, Rijsdijk F, Lau JY, Dahl RE, Eley TC. The direction of longitudinal associations between sleep problems and depression symptoms: a study of twins aged 8 and 10 years. Sleep. (2009) 32:189–99. doi: 10.1093/sleep/32.2.189
14. Huhdanpää H, Klenberg L, Westerinen H, Fontell T, Aronen ET. Sleep and psychiatric symptoms in young child psychiatric outpatients. Clin Child Psychol Psychiatry. (2018) 23:77–95. doi: 10.1177/1359104517718366
15. Pieters S, Burk WJ, Van der Vorst H, Dahl RE, Wiers RW, Engels RC. Prospective relationships between sleep problems and substance use, internalizing and externalizing problems. J Youth Adolesc. (2015) 44:379–88. doi: 10.1007/s10964-014-0213-9
16. Quach JL, Nguyen CD, Williams KE, Sciberras E. Bidirectional associations between child sleep problems and internalizing and externalizing difficulties from preschool to early adolescence. JAMA Pediatrics. (2018) 172:e174363. doi: 10.1001/jamapediatrics.2017.4363
17. Rubens SL, Evans SC, Becker SP, Fite PJ, Tountas AM. Self-reported time in bed and sleep quality in association with internalizing and externalizing symptoms in school-age youth. Child Psychiatry Hum Dev. (2017) 48:455–67. doi: 10.1007/s10578-016-0672-1
18. Reid GJ, Hong RY, Wade TJ. The relation between common sleep problems and emotional and behavioral problems among 2-and 3-year-olds in the context of known risk factors for psychopathology. J Sleep Res. (2009) 18:49–59. doi: 10.1111/j.1365-2869.2008.00692.x
19. Gauchat A. Rêves dysphoriques et rêves récurrents chez les enfants et les adolescents: corrélats psychosociaux et implications cliniques (Doctoral dissertation), Université de Montréal. (2015). Available online at: https://papyrus.bib.umontreal.ca/xmlui/bitstream/handle/1866/11592/Aline_Gauchat_2014_these.pdf?sequence=2&isAllowed=y
20. Abdel-Khalek AM. Nightmares: prevalence, age and gender differences among kuwaiti children and adolescents. Sleep Hypnosis. (2006) 8:33–40. Available online at: http://www.sleepandhypnosis.org/ing/archivelist.aspx?SayiID=29
21. Gauchat A, Séguin JR, Zadra A. Prevalence and correlates of disturbed dreaming in children. Pathol Biol. (2014) 62:311–8. doi: 10.1016/j.patbio.2014.05.016
22. Nielsen T, Levin R. Nightmares: a new neurocognitive model. Sleep Med Rev. (2007) 11:295–310. doi: 10.1016/j.smrv.2007.03.004
23. Ophoff D, Slaats M, Boudewyns A, Glazemakers I, Van Hoorenbeeck K, Verhulst S. Sleep disorders during childhood: a practical review. Eur J Pediatrics. (2018) 177:641–8. doi: 10.1007/s00431-018-3116-z
24. Schredl M, Biemelt J, Roos K, Dunkel T, Harris N. Nightmares and stress in children. Sleep Hypnosis. (2008) 10:19–25. Available online at: https://www.sleepandhypnosis.org/ing/archivelist.aspx?SayiID=37
25. Ennis CR, Short NA, Moltisanti AJ, Smith CE, Joiner TE, Taylor J. Nightmares and nonsuicidal self-injury: the mediating role of emotional dysregulation. Comprehens Psychiatry. (2017) 76:104–12. doi: 10.1016/j.comppsych.2017.04.003
26. Kramer M. The selective mood regulatory function of dreaming: an update and revision. In: Moffitt A, Kramer M, Hoffmann R, editors. The Functions of Dreaming. Albany, NY: State University of New York Press. (1993). p. 139–95.
27. Levin R, Nielsen T. Disturbed dreaming, posttraumatic stress disorder, and affect distress: a review and neurocognitive model. Psycholo Bull. (2007) 133:482–528. doi: 10.1037/0033-2909.133.3.482
28. Nielsen T. The stress acceleration hypothesis of nightmares. Front Neurol. (2017) 8:201. doi: 10.3389/fneur.2017.00201
29. Hawkins C, Williams TI. Nigthmares, life events and behavior problems in preschool-children. Child Care Health Dev. (1992) 18:117–28. doi: 10.1111/j.1365-2214.1992.tb00346.x
30. Lebowitz ER, Shimshoni Y, Silverman WK. Family accommodation mediates nightmares and sleep-related problems in anxious children. J Anxiety Disord. (2019) 62:94–9. doi: 10.1016/j.janxdis.2019.01.004
31. Russell K, Rasmussen S, Hunter SC. Insomnia and nightmares as markers of risk for suicidal ideation in young people: investigating the role of defeat and entrapment. J Clin Sleep Med. (2018) 14:775–84. doi: 10.5664/jcsm.7104
32. Salzarulo P, Chevalier A. Sleep pronlems in children and their relationship with early disturbances of the waking-sleep rythms. Sleep. (1983) 6:47–51. doi: 10.1093/sleep/6.1.47
33. Schredl M, Blomeyer D, Görlinger M. Nigthmares in children: influencing factors. Somnologie. (2000) 4:145–9. doi: 10.1007/s11818-000-0007-z
34. Shang CY, Gau SSF, Soong WT. Association between childhood sleep problems and perinatal factors, parental mental distress and behavioral problems. J Sleep Res. (2006) 15:63–73. doi: 10.1111/j.1365-2869.2006.00492.x
35. Simonds JF, Parraga H. Prevalence of sleep disorders and sleep behaviors in children and adolescents. J Am Acad Child Adolesc Psychiatry. (1982) 21:383–8. doi: 10.1016/S0002-7138(09)60942-0
36. Stein MA, Mendelsohn J, Obermeyer WH, Amromin J, Benca R. Sleep and behavior problems in school-aged children. Pediatrics. (2001) 107:e60. doi: 10.1542/peds.107.4.e60
37. Schredl M, Fricke-Oerkermann L, Mitschke A, Wiater A, Lehmkuhl G. Longitudinal study of nightmares in children: stability and effect of emotional symptoms. Child Psychiatry Hum Dev. (2009) 40:439–49. doi: 10.1007/s10578-009-0136-y
38. Smedje H, Broman J, Hetta J. Associations between disturbed sleep and behavioural difficulties in 635 children aged six to eight years: a study based on parents' perceptions. opean Child Adolesc Psychiatry. (2001) 10:1–9. doi: 10.1007/s007870170041
39. Fisher BE, Wilson AE. Selected sleep disturbances in schoolchildren reported by parents - prevalence, interrlatonships, behavioral-correlates and parental attributions. Perceptual Motor Skills. (1987) 64:1147–57. doi: 10.2466/pms.1987.64.3c.1147
40. Lereya ST, Winsper C, Tang NK, Wolke D. Sleep problems in childhood and borderline personality disorder symptoms in early adolescence. J Abnormal Child Psychol. (2017) 45:193–206. doi: 10.1007/s10802-016-0158-4
41. Fisher HL, Lereya ST, Thompson A, Lewis G, Zammit S, Wolke D. Childhood parasomnias and psychotic experiences at age 12 years in a United Kingdom birth cohort. Sleep. (2014) 37:475–82. doi: 10.5665/sleep.3478
42. Koopman-Verhoeff ME, Bolhuis K, Cecil CA, Kocevska D, Hudziak JJ, Hillegers MH, et al. During day and night: Childhood psychotic experiences and objective and subjective sleep problems. Schizophrenia Res. (2019) 206:127–34. doi: 10.1016/j.schres.2018.12.002
43. Lemyre A, Bastien C, Vallières A. Nightmares in mental disorders: a review. Dreaming. (2019) 29:144. doi: 10.1037/drm0000103
44. Liu X. Sleep and adolescent suicidal behavior. Sleep. (2004) 27:1351–8. doi: 10.1093/sleep/27.7.1351
45. Pigeon WR, Pinquart M, Conner K. Meta-analysis of sleep disturbance and suicidal thoughts and behaviors. J Clin Psychiatry. (2012) 73:e1160–7. doi: 10.4088/JCP.11r07586
46. Roberts J, Lennings C. Personality, psychopathology and nightmares in young people. Personal Individual Differ. (2006) 41:733–44. doi: 10.1016/j.paid.2006.03.010
47. Thompson A, Lereya S, Lewis G, Zammit S, Fisher H, Wolke D. Childhood sleep disturbance and risk of psychotic experiences at 18: UK birth cohort. Br J Psychiatry. (2015) 207:23–9. doi: 10.1192/bjp.bp.113.144089
48. Floress MT, Kuhn BR, Bernas RS, Dandurand M. Nightmare prevalence, distress, and anxiety among young children. Dreaming. (2016) 26:280. doi: 10.1037/drm0000034
49. Gregory AM, Eley TC. Sleep problems, anxiety and cognitive style in school-aged children. Infant Child Dev. (2005) 14:435–44. doi: 10.1002/icd.409
50. Mindell JA, Barrett KM. Nightmares and anxiety in elementary-aged children: is there a relationship? Child Care Health Dev. (2002) 28:317–22. doi: 10.1046/j.1365-2214.2002.00274.x
51. Nielsen TA, Laberge L, Paquet J, Tremblay RE, Vitaro F, Montplaisir J. Development of disturbing dreams during adolescence and their relation to anxiety symptoms. Sleep. (2000) 23:727–36. doi: 10.1093/sleep/23.6.1
52. Reynolds KC, Alfano CA. Things that go bump in the night: frequency and predictors of nightmares in anxious and nonanxious children. Behav Sleep Med. (2016) 14:442–56. doi: 10.1080/15402002.2015.1017099
53. Schredl M, Pallmer R, Montasser A. Anxiety dreams in school-aged children. Dreaming. (1996) 6:265–70. doi: 10.1037/h0094461
54. Simard V, Nielsen TA, Tremblay RE, Boivin M, Montplaisir JY. Longitudinal study of bad dreams in preschool-aged children: prevalence, demographic correlates, risk and protective factors. Sleep. (2008) 31:62–70. doi: 10.1093/sleep/31.1.62
55. Gregory AM, Van der Ende J, Willis TA, Verhulst FC. Parent-reported sleep problems during development and self-reported anxiety/depression, attention problems, and aggressive behavior later in life. Arch Pediatrics Adolesc Med. (2008) 162:330–5. doi: 10.1001/archpedi.162.4.330
56. Wong MM, Brower KJ, Conroy DA, Lachance KA, Craun EA. Sleep characteristics and behavioral problems among children of alcoholics and controls. Alcohol Clin Exp Res. (2018) 42:603–12. doi: 10.1111/acer.13585
57. Li SX, Yu MWM, Lam SP, Zhang J, Li AM, Lai KYC, et al. Frequent nightmares in children: Familial aggregation and associations with parent-reported behavioral and mood problems. Sleep. (2011) 34:487–93. doi: 10.1093/sleep/34.4.487
58. Muratori P, Menicucci D, Lai E, Battaglia F, Bontempelli L, Chericoni N, et al. Linking sleep to externalizing behavioral difficulties: a longitudinal psychometric survey in a cohort of Italian school-age children. J Primary Prev. (2019) 40:231–41. doi: 10.1007/s10935-019-00547-2
59. Tsai F-J, Chiang H-L, Lee C-M, Gau SS-F, Lee W-T, Fan P-C, et al. Sleep problems in children with autism, attention-deficit hyperactivity disorder, and epilepsy. Res Autism Spectrum Disord. (2012) 6:413–21. doi: 10.1016/j.rasd.2011.07.002
60. Grünwald J, Schlarb AA. Relationship between subtypes and symptoms of ADHD. insomnia, and nightmares in connection with quality of life in children. Neuropsychiatr Dis Treat. (2017) 13:2341. doi: 10.2147/NDT.S118076
61. Chiang HL, Gau SSF, Ni HC, Chiu YN, Shang CY, Wu YY, et al. Association between symptoms and subtypes of attention-deficit hyperactivity disorder and sleep problems/disorders. J Sleep Res. (2010) 19:535–45. doi: 10.1111/j.1365-2869.2010.00832.x
62. Mayes SD, Calhoun SL, Bixler EO, Vgontzas AN, Mahr F, Hillwig-Garcia J, et al. ADHD subtypes and comorbid anxiety, depression, and oppositional-defiant disorder: differences in sleep problems. J Pediatr Psychol. (2008) 34:328–37. doi: 10.1093/jpepsy/jsn083
63. Wang B, Eastwood PR, Becker A, Isensee C, Wong JW, Huang R-C, et al. Concurrent developmental course of sleep problems and emotional/behavioral problems in childhood and adolescence as reflected by the dysregulation profile. Sleep. (2019) 42:zsy243. doi: 10.1093/sleep/zsy243
64. Zhang J, Xu Z, Zhao K, Chen T, Ye X, Shen Z, et al. Sleep habits, sleep problems, sleep hygiene, and their associations with mental health problems among adolescents. J Am Psychiatr Nurses Assoc. (2018) 24:223–34. doi: 10.1177/1078390317715315
65. Gieselmann A, Ait Aoudia M, Carr M, Germain A, Gorzka R, Holzinger B, et al. (2019) Aetiology and treatment of nightmare disorder: state of the art and future perspectives. J Sleep Res. 28:e12820. doi: 10.1111/jsr.12820
66. Rothbart MK, Ahadi SA, Hersey KL, Fisher P. Investigations of temperament at three to seven years: the children's behavior questionnaire. Child Dev. (2001) 72:1394–408. doi: 10.1111/1467-8624.00355
67. Rothbart MK, Jones LB. Temperament, self-regulation and education. Sch Psychol Rev. (1998) 27:479–91.
68. Gartstein MA, Rothbart MK. Studying infant temperament via the revised infant behavior questionnaire. Infant Behav Dev. (2003) 26:64–86. doi: 10.1016/S0163-6383(02)00169-8
69. Sanson A, Hemphill SA, Smart D. Connections between temperament and social development: a review. Social Dev. (2004) 13:142–70. doi: 10.1046/j.1467-9507.2004.00261.x
70. Kopala-Sibley DC, Olino T, Durbin E, Dyson MW, Klein DN. The stability of temperament from early childhood to early adolescence: a multi-method, multi-informant examination. Eur J Personal. (2018) 32:128–45. doi: 10.1002/per.2151
71. Pesonen A-K, Räikkönen K, Keskivaara P, Keltikangas-Järvinen L. Difficult temperament in childhood and adulthood: continuity from maternal perceptions to self-ratings over 17 years. Personal Individual Differ. (2003) 34:19–31. doi: 10.1016/S0191-8869(02)00021-1
72. Clark LA, Watson D, Mineka S. Temperament, personality, and the mood and anxiety disorders. J Abnormal Psychol. (1994) 103:103–16. doi: 10.1037/0021-843X.103.1.103
73. Rhee SH, Lahey BB, Waldman ID. Comorbidity among dimensions of childhood psychopathology: converging evidence from behavior genetics. Child Dev Perspect. (2015) 9:26–31. doi: 10.1111/cdep.12102
74. Uhl K, Halpern LF, Tam C, Fox JK, Ryan JL. Relations of emotion regulation, negative and positive affect to anxiety and depression in middle childhood. J Child Family Stud. (2019) 28:2988–99. doi: 10.1007/s10826-019-01474-w
75. Bush NR, Lengua LJ, Colder CR. Temperament as a moderator of the relation between neighborhood and children's adjustment. J Appl Dev Psychol. (2010) 31:351–61. doi: 10.1016/j.appdev.2010.06.004
76. Northerner LM, Trentacosta CJ, McLear CM. Negative affectivity moderates associations between cumulative risk and at-risk toddlers' behavior problems. J Child Family Stud. (2016) 25:691–9. doi: 10.1007/s10826-015-0248-x
77. Pluess M, Belsky J. Children's differential susceptibility to effects of parenting. Family Sci. (2010) 1:14–25. doi: 10.1080/19424620903388554
78. Veenstra R, Oldehinkel AJ, De Winter AF, Lindenberg S, Ormel J. Temperament, environment, and antisocial behavior in a population sample of preadolescent boys and girls. Int J Behav Dev. (2006) 30:422–32. doi: 10.1177/0165025406071490
79. Davis S, Votruba-Drzal E, Silk JS. Trajectories of internalizing symptoms from early childhood to adolescence: associations with temperament and parenting. Social Dev. (2015) 24:501–20. doi: 10.1111/sode.12105
80. Edwards RC, Hans SL. Infant risk factors associated with internalizing, externalizing, and co-occurring behavior problems in young children. Dev Psychol. (2015) 51:489. doi: 10.1037/a0038800
81. Jessee A, Mangelsdorf SC, Shigeto A, Wong MS. Temperament as a moderator of the effects of parental depressive symptoms on child behavior problems. Social Dev. (2012) 21:610–27. doi: 10.1111/j.1467-9507.2011.00639.x
82. Karreman A, van Tuijl C, van Aken MAG, Dekovic M. Predicting young children's externalizing problems interactions among effortful control, parenting, child gender. Merrill Palmer Q J Dev Psychol. (2009) 55:111–34. doi: 10.1353/mpq.0.0020
83. Schredl M, Fricke-Oerkermann L, Mitschke A, Wiater A, Lehmkuhl G. Factors affecting nightmares in children: parents' vs. children's ratings. Eur Child Adolesc Psychiatry. (2009) 18:20–5. doi: 10.1007/s00787-008-0697-5
84. Coulombe J, Reid GJ, Boyle MH, Racine Y. Concurrent associations among sleep problems, indicators of inadequate sleep, psychopathology, and shared risk factors in a population-based sample of healthy Ontario children. J Pediatr Psychol. (2010) 35:790–9. doi: 10.1093/jpepsy/jsp097
85. van der Ende J, Verhulst FC, Tiemeier H. Agreement of informants on emotional and behavioral problems from childhood to adulthood. Psychol Assessment. (2012) 24:293–300. doi: 10.1037/a0025500
86. Santé Québec JM, Desrosiers H, Tremblay RE. “En 2001. J'aurai 5 ans”, Enquête auprès des bébés de 5 mois: Rapport préliminaire de l'Étude longitudinale du développement des enfants du Québec (ÉLDEQ) [translation: “In 2001. I'll be 5 years old” Survey of 5 months old infants: Preliminary report from the Québec Longitudinal Study of Childhood Development (QLSCD)]. Montréal, QC: Ministère de la Santé et des Services sociaux, Gouvernement du Québec (1997).
87. Robert G, Zadra A. Measuring nightmare and bad dream frequency: impact of retrospective and prospective instruments. J Sleep Res. (2008) 17:132–9. doi: 10.1111/j.1365-2869.2008.00649.x
88. Zadra A, Donderi D. Nightmares and bad dreams: their prevalence and relationship to well-being. J Abnormal Psychol. (2000) 109:273–81. doi: 10.1037/0021-843X.109.2.273
89. Baillargeon RH, Normand CL, Séguin JR, Zoccolillo M, Japel C, Pérusse D, et al. The evolution of problem and social competence behaviors during toddlerhood: a prospective population-based cohort survey. Infant Mental Health J. (2007) 28:12–38. doi: 10.1002/imhj.20120
90. Gauchat A, Zadra A, Tremblay RE, Zelazo PD, Séguin JR. Recurrent dreams and psychosocial adjustment in preteenaged children. Dreaming. (2009) 19:75–84. doi: 10.1037/a0016549
91. Vaillancourt T, Miller JL, Fagbemi J, Côté S, Tremblay RE. Trajectories and predictors of indirect aggression: results from a nationally representative longitudinal study of Canadian children aged 2-10. Aggress Behav. (2007) 33:314–26. doi: 10.1002/ab.20202
92. Tremblay RE, Vitaro F, Gagnon C, Piché C, Royer N. A prosocial scale for the preschool behaviour questionnaire: concurrent and predictive correlates. Int J Behav Dev. (1992) 15:227–45. doi: 10.1177/016502549201500204
93. Achenbach TM. The Child Behavior Checklist and Related Instruments. Mahwah, NJ: Lawrence Erlbaum Associates Publishers (1999).
94. Dodge KA, Coie JD. Social-information-processing factors in reactive and proactive aggression in children's peer groups. J Personal Social Psychol. (1987) 53:1146–58. doi: 10.1037/0022-3514.53.6.1146
95. Charrois J, Côté SM, Paquin S, Séguin JR, Japel C, Vitaro F, et al. Maternal depression in early childhood and child emotional and behavioral outcomes at school age: examining the roles of preschool childcare quality and current maternal depression symptomatology. Eur Child Adolesc Psychiatry. (2019) 29:637–48. doi: 10.1007/s00787-019-01385-7
96. Huijbregts SCJ, Seguin JR, Zoccolillo M, Boivin M, Tremblay RE. Maternal prenatal smoking, parental antisocial behavior, and early childhood physical aggression. Dev Psychopathol. (2008) 20:437–53. doi: 10.1017/S0954579408000217
97. La Buissonnière-Ariza V, Séguin JR, Nassim M, Boivin M, Pine DS, Lepore F, et al. Chronic harsh parenting and anxiety associations with fear circuitry function in healthy adolescents: a preliminary study. Biol Psychol. (2019) 145:198–210. doi: 10.1016/j.biopsycho.2019.03.019
98. Paquin C, Castellanos-Ryan N, Vitaro F, Côté SM, Tremblay RE, Séguin JR, et al. Maternal depression symptoms, child behavior problems, and their transactional relations: Probing the role of formal childcare. Dev Psychopathol. (2019). doi: 10.1017/S0954579419000956. [Epub ahead of print].
99. Rioux C, Murray J, Castellanos-Ryan N, Séguin JR, Tremblay RE, Parent S. Moderation of parenting by inhibitory control in the prediction of the common and unique variance of hyperactivity-impulsivity and inattention. Dev Psychopathol. (2019). doi: 10.1017/S0954579419000774. [Epub ahead of print].
100. Touchette E, Petit D, Seguin JR, Boivin M, Tremblay RE, Montplaisir JY. Associations between sleep duration patterns and behavioral/cognitive functioning at school entry. Sleep. (2007) 30:1213–9. doi: 10.1093/sleep/30.9.1213
101. Touchette E, Petit D, Tremblay RE, Montplaisir JY. Risk factors and consequences of early childhood dyssomnias: New perspectives. Sleep Med Rev. (2009) 13:355–61. doi: 10.1016/j.smrv.2008.12.001
102. Vitaro F, Barker ED, Boivin M, Brendgen M, Tremblay RE. Do early difficult temperament and harsh parenting differentially predict reactive and proactive aggression? J Abnormal Child Psychol. (2006) 34:685–95. doi: 10.1007/s10802-006-9055-6
103. Bates JE, Freeland CA, Lounsbur ML. Measures of infant difficultness. Child Dev. (1979) 50:794–803. doi: 10.2307/1128946
105. Harrison XA, Donaldson L, Correa-Cano ME, Evans J, Fisher DN, Goodwin CED, et al. A brief introduction to mixed effects modelling and multi-model inference in ecology. PeerJ. (2018) 6:e4794. doi: 10.7717/peerj.4794
106. Tabachnick BG, Fidell LS. Using Multivariate Statistics. 6th ed. Boston, MA: Pearson Education (2013).
107. Carneiro A, Dias P, Soares I. Risk factors for internalizing and externalizing problems in the preschool years: systematic literature review based on the child behavior checklist 1−5. J Child Family Stud. (2016) 25:2941–53. doi: 10.1007/s10826-016-0456-z
108. Costello E, Mustillo S, Erkanli A, Keeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch General Psychiatry. (2003) 60:837–44. doi: 10.1001/archpsyc.60.8.837
110. Aiken LS, West SG. Multiple Regression: Testing and Interpreting Interactions. Thousand Oaks, CA: Sage Publications, Inc; US (1991).
111. Kagan J, Snidman N. Infant predictors of inhibited and uninhibited profiles. Psychol Sci. (1991) 2:40–44. doi: 10.1111/j.1467-9280.1991.tb00094.x
112. Kagan J, Snidman N. Temperamental factors in human development. Am Psychol. (1991) 46:856–62. doi: 10.1037/0003-066X.46.8.856
113. Kagan J, Snidman N. The Long Shadow of Temperament. Cambridge; London: Belknap; Harvard Press (2004).
114. Putnam SP, Stifter CA. Behavioral approach–inhibition in toddlers: prediction from infancy, positive and negative affective components, and relations with behavior problems. Child Dev. (2005) 76:212–26. doi: 10.1111/j.1467-8624.2005.00840.x
115. Chronis-Tuscano A, Degnan KA, Pine DS, Perez-Edgar K, Henderson HA, Diaz Y, et al. Stable early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. J Am Acad Child Adolesc Psychiatry. (2009) 48:928–35. doi: 10.1097/CHI.0b013e3181ae09df
116. Fox NA, Henderson HA, Rubin KH, Calkins SD, Schmidt LA. Continuity and discontinuity of behavioral inhibition and exuberance: psychophysiological and behavioral influences across the first four years of life. Child Dev. (2001) 72:1–21. doi: 10.1111/1467-8624.00262
117. Prior M, Smart D, Sanson A, Oberklaid F. Does shy-inhibited temperament in childhood lead to anxiety problems in adolescence? J Am Acad Child Adolesc Psychiatry. (2000) 39:461–8. doi: 10.1097/00004583-200004000-00015
118. Krueger RF, Hicks BM, Patrick CJ, Carlson SR, Iacono WG, McGue M. Etiologic connections among substance dependence, antisocial behavior, and personality: modeling the externalizing spectrum. J Abnormal Psychol. (2002) 111:411–24. doi: 10.1037/0021-843X.111.3.411
119. Belsky J, Pluess M. Differential susceptibility to long-term effects of quality of child care on externalizing behavior in adolescence? Int J Behav Dev. (2012) 36:2–10. doi: 10.1177/0165025411406855
120. Lancee J, Schrijnemaekers NC. The association between nightmares and daily distress. Sleep Biol Rhythms. (2013) 11:14–9. doi: 10.1111/j.1479-8425.2012.00586.x
121. Belicki K. Nightmare frequency versus nightmare distress: relations to psychopathology and cognitive style. J Abnormal Psychol. (1992) 101:592–7. doi: 10.1037/0021-843X.101.3.592
122. Blagrove M, Farmer L, Williams E. The relationship of nightmare frequency and nightmare distress to well-being. J Sleep Res. (2004) 13:129–36. doi: 10.1111/j.1365-2869.2004.00394.x
123. Lee R, Suh S. Nightmare distress as a mediator between nightmare frequency and suicidal ideation. Dreaming. (2016) 26:308. doi: 10.1037/drm0000039
124. Kelly WE. Pathological and nonpathological worry: their relationships with nightmare frequency. Psychiatry Behav Sci. (2018) 8:1–6. doi: 10.5455/jmood.20180204033253
125. Secrist ME, Dalenberg CJ, Gevirtz R. Contributing factors predicting nightmares in children: trauma, anxiety, dissociation, emotion regulation. Psychol Trauma Theory Res Pract Policy. (2019) 11:114. doi: 10.1037/tra0000387
126. Cartwright R, Agargun MY, Kirkby J, Friedman JK. Relation of dreams to waking concerns. Psychiatry Res. (2006) 141:261–70. doi: 10.1016/j.psychres.2005.05.013
127. Hartmann E. The Nature and Functions of Dreaming. New York, NY: Oxford University Press (2010).
128. Scarpelli S, Bartolacci C, D'Atri A, Gorgoni M, De Gennaro L. The functional role of dreaming in emotional processes. Front Psychol. (2019) 10:459. doi: 10.3389/fpsyg.2019.00459
129. Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin Psychol Rev. (2010) 30:217–37. doi: 10.1016/j.cpr.2009.11.004
130. Eisenberg N, Cumberland A, Spinrad TL, Fabes RA, Shepard SA, Reiser M, et al. The relations of regulation and emotionality to children's externalizing and internalizing problem behavior. Child Dev. (2001) 72:1112–34. doi: 10.1111/1467-8624.00337
131. Kim-Spoon J, Cicchetti D, Rogosch FA. A longitudinal study of emotion regulation, emotion lability-negativity, and internalizing symptomatology in maltreated and nonmaltreated children. Child Dev. (2013) 84:512–27. doi: 10.1111/j.1467-8624.2012.01857.x
132. Dougherty DM, Mathias CW, Marsh DM, Papageorgiou T, Swann AC, Moeller F. Laboratory measured behavioral impulsivity relates to suicide attempt history. Suicide Life Threat Behav. (2004) 34:374–85. doi: 10.1521/suli.34.4.374.53738
133. Gould MS, Greenberg T, Velting DM, Shaffer D. Youth suicide risk and preventive interventions: a review of the past 10 years. J Am Acad Child Adolesc Psychiatry. (2003) 42:386–405. doi: 10.1097/01.CHI.0000046821.95464.CF
134. Simon TR, Swann AC, Powell KE, Potter LB, Kresnow M-j, O'Carroll PW. Characteristics of impulsive suicide attempts and attempters. Suicide Life Threat Behav. (2001) 32:49–59. doi: 10.1521/suli.32.1.5.49.24212
135. Winsper C, Tang NKY. Linkages between insomnia and suicidality: prospective associations, high-risk subgroups and possible psychological mechanisms. Int Rev Psychiatry. (2014) 26:189–204. doi: 10.3109/09540261.2014.881330
136. Belfiore LA, Pietrowsky R. Attachment styles and nightmares in adults. Dreaming. (2017) 27:59. doi: 10.1037/drm0000045
137. Csoka S, Simor P, Szabo G, Kopp MS, Bodizs R. Early maternal separation, nightmares, and bad dreams: results from the hungarostudy epidemiological panel. Attach Hum Dev. (2011) 13:125–40. doi: 10.1080/14616734.2011.553991
138. van Ijzendoorn MH, Schuengel C, Bakermans-Kranenburg MJ. Disorganized attachment in early childhood: Meta-analysis of precursors, concomitants, and sequelae. Dev Psychopathol. (1999) 11:225–49. doi: 10.1017/S0954579499002035
Keywords: disturbing dreams, nightmares, bad dreams, dreaming, psychosocial maladjustment, temperament, negative emotionality
Citation: Gauchat A, Zadra A, El-Hourani M, Parent S, Tremblay RE and Séguin JR (2020) Disturbing Dreams and Psychosocial Maladjustment in Children: A Prospective Study of the Moderating Role of Early Negative Emotionality. Front. Neurol. 11:762. doi: 10.3389/fneur.2020.00762
Received: 11 December 2019; Accepted: 19 June 2020;
Published: 07 August 2020.
Edited by:
S. R. Pandi-Perumal, Somnogen Canada Inc., CanadaReviewed by:
Kevin P. Grace, Beth Israel Deaconess Medical Center, Harvard Medical School, United StatesMark Blagrove, Swansea University, United Kingdom
Copyright © 2020 Gauchat, Zadra, El-Hourani, Parent, Tremblay and Séguin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jean R. Séguin, amVhbi5zZWd1aW5AdW1vbnRyZWFsLmNh