 Ana Simon-Gozalbo1*
Ana Simon-Gozalbo1* Carmen Rodriguez-Blazquez2
Carmen Rodriguez-Blazquez2 Maria J. Forjaz2
Maria J. Forjaz2 Pablo Martinez-Martin2 on behalf of Cog-PD Study1
Pablo Martinez-Martin2 on behalf of Cog-PD Study1- 1Doctorate Program in Health Sciences, University of Alcala, Alcala de Henares, Spain
- 2National Center of Epidemiology and CIBERNED, Carlos III Institute of Health, Madrid, Spain
Background: Cognitive impairment is one of the most frequent and disabling non-motor symptoms in Parkinson disease (PD) and encompasses a continuum from mild cognitive impairment (PD-MCI) to dementia (PDD). The risk factors associated with them are not completely elucidated.
Objective: To characterize the presence and clinical presentation of PD-MCI and PDD in patients with idiopathic PD, examining motor and non-motor features and determining factors associated with cognitive impairment.
Methods: Multicenter, cross-sectional study in 298 PD patients who underwent clinical [Hoehn and Yahr (HY) staging and Clinical Impression of Severity Index for Parkinson Disease], neurological [Scales for Outcomes in Parkinson's Disease (SCOPA)-Motor], neuropsychological (Mini Mental State Examination, SCOPA-Cognition, Frontal Assessment Battery and Clinical Dementia Rating Scale), neuropsychiatric [SCOPA-Psychiatric complications, SCOPA-Psychosocial (SCOPA-PS), and Hospital Anxiety and Depression Scale (HADS)], and health-related quality of life [Parkinson Disease Questionnaire for quality of life (PDQ-8)] assessment. Movement Disorders Society criteria were applied to classify patients as normal cognition (NC), PD-MCI, and PDD. The association between variables was explored using multivariate binary and multinomial logistic regression models.
Results: Seventy-two patients (24.2%) were classified as NC, 82 (27.5%) as PD-MCI, and 144 (48.3%) as PDD. These last two groups reported more psychosocial problems related with the disease (mean SCOPA-PS, 16.27 and 10.39, respectively), compared with NC (7.28) and lower quality-of-life outcomes (PDQ-8 48.98 and 28.42, respectively) compared to NC (19.05). The logistic regression analysis showed that both cognitive impaired groups had a more severe stage of PD measured by HY [odds ratio (OR) for MCI-PD, 2.45; 95% confidence interval (CI), 1.22–4.90; OR for PDD 2.64; 95% CI, 1.17–5.98]. Specifically, age (OR, 1.30; 95% CI, 1.16–1.47), years of education (OR, 0.91; 95% CI, 0.83–0.99), disease duration (OR, 1.19; 95% CI, 1.07–1.32), HADS-D (OR, 1.20; 95% CI, 1.06–1.35), and hallucinations (OR, 2.98; 95% CI, 1.16–7.69) were related to PDD.
Conclusions: Cognitive impairment in PD is associated with more severe disease stage, resulting in a global, neuropsychiatric, psychosocial, and quality-of-life deterioration. This study provides a better understanding of the great impact that cognitive impairment has within the natural history of PD and its relationship with the rest of motor and non-motor symptoms in the disease.
Background
Idiopathic Parkinson disease (PD) is a common, chronic, and neurodegenerative disorder characterized by the presence of motor manifestations such as tremor, rigidity, bradykinesia, or instability. However, there are also non-motor features including cognitive dysfunction, sleep disorders, neuropsychiatric symptoms, autonomic dysfunction, pain, fatigue, and olfactory disorders that may be present since the earliest stages of PD or even prior to its diagnosis, generating a great impact on patients and caregivers (1, 2). In conjunction with this fact, the latest evidence from clinical, genetic, neuropathological, and imaging studies suggests the initiation of PD-specific pathology prior to the initial presentation of the classical motor clinical features by years (preclinical and prodromal stages of PD). The existence of these “premotor biomarkers” opens up the possibility to new therapies that would help prevent the onset of the disease or retard the progression (3). One of the most recent neuroprotective substances would be the cystatin C, which seems to play a significant role in neural and vascular cell function in neurodegenerative diseases (4, 5). Another new biomarker related to PD progression could be the decreased serum levels of mitochondrial creatine kinase. However, no significant relationship was found between this levels and the Hoehn and Yahr (HY) stage or non-motor symptoms scales (6).
With regard to cognition, the heterogeneous presentations encompass a continuum from cognitively intact patients to subjective cognitive decline, mild cognitive impairment (PD-MCI), and, finally, PD dementia (PDD), with a progressive severity gradient (7). Cognitive decline is one of the most frequent clinical manifestations of PD, being a prognostic variable of institutionalization and mortality (8). Prevalence of PD-MCI is estimated between 15 and 40% of PD patients according to recent studies and ~40% of patients with PD-MCI decline to PDD over 3 years (9). In 2007 and 2012, the Movement Disorder Society (MDS) published the diagnostic criteria PDD and PD-MCI, respectively. For both disorders, MDS established two levels of diagnostic certainty: level I, using a brief neuropsychological evaluation; and level II, which includes a much more extensive battery of tests (10, 11).
Several sociodemographic and disease-related features have been identified as potential risk factors that increase the progression of cognitive decline in PD, such as old age, low educational level, severity of disease, high age at onset, disease duration, high doses of levodopa, or use of anticholinergic medication (12, 13). Other clinical manifestations, such as neuropsychiatric symptoms, hallucinations, or rapid eye movement–sleep behavior disorder (RBD), have also been investigated and even considered as prodromal markers of PD (3, 14). The pathophysiological mechanisms underlying RBD and its relation with PDD include a major cholinergic denervation, a higher burden of cerebrovascular disease, and a more advanced deposition of synaptic nucleoprotein in brain areas (15). With regard to the link between depression symptoms and different types of dementia, some animal models have been developed, showing that exposure to several exogenous factors (economic status, education, family support, and social environment) and endogenous factors (such as aging, cerebral small vessel disease, brain circuits, neuroendocrine activity, neurochemistry, neurotransmitters, and inflammatory cytokines) could contribute to the pathogenesis of depression. Overall, non-motor symptoms in PD patients have been associated with dysfunction of the microbiota–gut–brain axis (16). Specifically, PDD has been associated to certain biomarkers such as low cerebrospinal fluid levels of β-amyloid 42, low serum uric acid levels, low serum Trefoil factor 3 levels, low serum cholinesterase activity, and high serum levels of homocysteine (17). In addition, some proinflammatory substances such as lipoprotein-associated phospholipase A2, superoxide dismutase, and high-sensitivity C-reactive protein are linked to neuroinflammation and therefore to progression of disease and cognitive impairment (18–20).
Concerning PD-MCI status, there are only a few studies on associated risk factors, and they suggest that older age, late age at onset, male gender, depression, and more advanced motor impairment have been associated with PD-MCI (9, 21). However, when reviewing the existing literature, the results are still conflicting regarding some of these factors. For example, contradictory findings have been reported for gender, education, age at onset, disease duration, HY stage, depression, and levodopa dose (12, 13, 22, 23). It is suggested that the reason for this is due to differences in populations, differences in methodology, outcome measures, and lack of robust studies with large sample size (24). In neuroimaging studies, PD-MCI patients showed more severe atrophy in the right entorhinal cortex, compared to PD patients without cognitive impairment, suggesting this brain area as a neuroanatomical biomarker in PD-MCI (25).
In the last decades, studies have tried to achieve a better understanding of the clinical heterogeneity in PD by defining different subtypes within the disease via cluster analysis, which could predict disease course, underlie neuropathological mechanisms, and lead to more efficient, personalized, therapeutic strategies (26, 27). The traditional subtyping systems were based on motor symptoms and motor complications, such as tremor-dominant PD (TD) vs. postural instability and gait difficulty (PIGD) with an akinetic-rigid predominance (28, 29). The TD motor phenotype was considered to have a more favorable prognosis than the PIGD phenotype, whereas the latter is associated to a more rapid and greater progression of the disease, including cognitive impairment (30, 31). Several studies have defined subtypes in relation to demographic and disease-related factors, such as the age at onset, claiming that patients with young-onset PD had a slower progression of disease than those with late-onset PD, concluding that age at onset was a major determinant of the course of disease (32). In recent years, the increasing importance of non-motor symptoms in PD has led to non-motor symptoms based subtypes, such as cognitive PD phenotypes (33, 34). However, the clinical, neuropsychological, and neuropathological boundaries between PDD and dementia with Lewy bodies (DLBs) have challenged the concept of different clinical entities. Conventionally, the diagnosis of PDD is usually made when dementia develops within the context of an established PD, whereas DLBs might be more appropriate when dementia precedes or coincides within 1 year of Parkinsonism onset (35). The so-called “Park cognitive” subtype is characterized by developing cognitive impairment even at an early stage, progressing rapidly to dementia (36). In other cognitive models graded by severity of cognitive impairment, cognitively intact patients were significantly younger and had received more years of formal education, whereas patients in the more cognitive impaired clusters had more severe motor symptoms, longer disease duration, and more axial signs (7).
Finally, the latest cluster analysis includes clinical, neuropsychological, neuroimaging, biospecimen, and genetic information to develop criteria to assign patients to a PD subtype (30, 37). The so-called “diffuse malignant” phenotype, in which three critical non-motor features (MCI, RBD, and orthostatic hypotension) at baseline identified the most rapidly progressive subtype, showed more severe motor and non-motor symptoms, more atrophy in substantia nigra–connected areas, more dopaminergic deficit on SPECT, reduced β-amyloid in cerebrospinal fluid, and shorter survival rates (38). Moreover, this subtype had greater decline in cognition and in dopamine functional neuroimaging after an average of 2.7 years (30).
However, subtyping PD has been challenging, because of inconsistent reliability and possibility of confusion between subtypes and different stages of disease progression (27). Therefore, there is currently no clear way to define and divide subtypes in PD.
The aim of the present study is to examine and compare the sociodemographic, disease-related, and clinical characteristics in a sample of PD patients with different degrees of cognitive impairment determined using the MDS diagnostic criteria. Additionally, a detailed analysis of the relationship between cognitive decline in PD and other manifestations of the disease will be carried out. The aforementioned aspects are not fully understood and are key to the management and well-being promotion of these patients. Moreover, these clinical markers have still potential to be used alongside with other biological and neuroimaging biomarkers as indicators of cognitive impairment (39).
Methods
This study used data from a previous international, multicenter, cross-sectional study (40). Patients 30 years or older and diagnosed with idiopathic PD according to the UK Parkinson's Disease Society Brain Bank Criteria were included (41). To obtain an adequate sample size of at least 100 patients with PDD, patients with cognitive impairment were specifically overrecruited. Exclusion criteria were as follows: (1) parkinsonism other than idiopathic PD; (2) acute or chronic concomitant disease that could interfere in the evaluation of PD; and (3) any type of disability that could interfere with answering the questionnaires, with the exception of cognitive impairment. In cognitive impaired patients, information pertaining to self-administered and patient-reported outcome (PRO) scales was obtained from clinical interview to the caregiver.
Patients were recruited from movement disorder clinics in Brazil (n = 76), Ecuador (n = 95), and Romania (n = 127). A neurologist with expertise in movement disorders collected sociodemographic and disease-related data. In addition, a neurological, neuropsychological, neuropsychiatric, functional, and quality-of-life assessment was carried out, applying different rating scales: the global severity of PD was defined according to the HY staging (42) and the Clinical Impression of Severity Index (CISI-PD) (43); functional status was assessed through the Barthel Index (44); the motor manifestations were evaluated by the Scales for Outcomes in Parkinson's Disease-Motor (SCOPA-Motor) (45); the assessment of cognitive status included the Mini-Mental State Examination (MMSE) (46), the SCOPA-Cognition (SCOPA-Cog) (47), the Frontal Assessment Battery (FAB) (48, 49), and the Clinical Dementia Rating Scale (CDR) (50); the neuropsychiatric symptoms were collected through the SCOPA-Psychiatric (SCOPA-PC) (51). Finally, each patient completed the following self-administered questionnaires: the Hospital Anxiety and Depression Scale (HADS), with two subscales, HADS-A and HADS-D, respectively (52); the 8-item Parkinson Disease Questionnaire for quality of life (PDQ-8) (53); and the SCOPA-Psychosocial (SCOPA-PS) for psychosocial consequences of PD (54). For all instruments except cognitive tests (MMSE, SCOPA-Cog, and FAB) and the Barthel Index, higher scores reflect poorer functioning. A cutoff of ≥11 in the HADS-A and HADS-D was used as indicative of presence of anxiety and depression (52). All evaluations were performed during “on” state. The culturally adapted and validated versions were used in each country.
Neurologists evaluated the severity of cognitive impairment using the neuropsychological examination and the clinical interview with patient and caregiver, CDR scale scores, the presence or absence of dementia according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria, and item 3 of the CISI-PD scale, which refers to the patient's cognitive status. Cognitive symptoms started at least 1 year after the onset of PD in all participants.
Subsequently and independently, patients were classified by the research team into three groups, namely, normal cognition (NC), PD-MCI, and PDD, using criteria based on those proposed by the MDS (level I) and literature review [Table 1; (10, 11, 40, 55)].
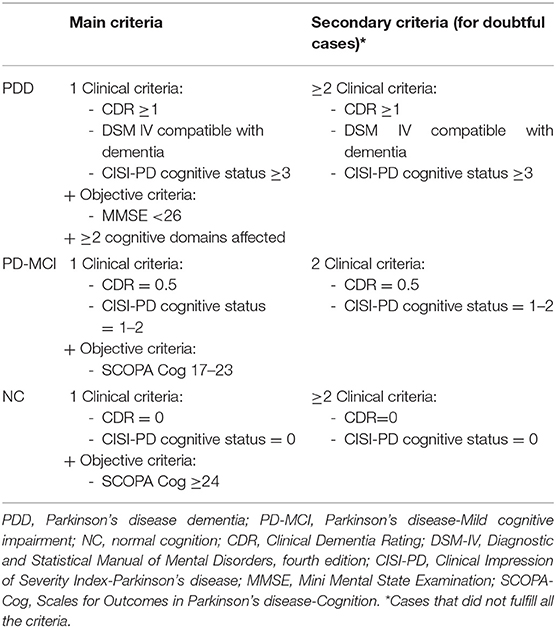
Table 1. Classification criteria based on MDS criteria and literature review.
The study was formally approved by the local institutional review boards. Written informed consent was obtained from all patients prior to participating in the study. In those with severe dementia, informed consent was signed by the main caregiver.
Statistical Analysis
In addition to descriptive statistics, tests for determining the differences between the 3 groups of patients were used. For data not fitting the normal distribution, non-parametric tests were applied. Chi-square χ2-tests were used for comparing categorical variables, whereas the Kruskal–Wallis test was applied in continuous variables that were not normally distributed.
Two multivariate binary logistic regression models were subsequently performed: one with the presence of any degree of cognitive impairment (NC vs. MCI-PD/PDD) and the other one with the presence of dementia (NC/MCI-PD vs. PDD), as dependent variables. The independent variables were motor and non-motor symptoms variables and time since diagnosis in years. Moreover, a multinomial logistic regression model was undertaken, with the same independent variables and using the three diagnostic groups as the outcome variable. Variables with p < 0.10 from the univariate analysis and those that were considered clinically relevant were selected for inclusion in the multivariate analyses. Age, sex, and education were controlled. Odds ratio (OR) with 95% confidence intervals (CIs) was used to assess the significance of associations. The binary logistic regression models were carried out to help clarifying the interpretation of data in the two stages of cognitive decline (MCI-PD and PDD) and, at the same time, adding more information to the topic, contrasting and completing the data provided by the multinomial logistic regression model.
In the logistic regression models, the cognitive assessment tests were not included because they had been used for the classification of the diagnostic groups and therefore could interfere in the results of the analysis. To analyze the relationship between the different variables, Spearman correlation coefficients were determined. Coefficients of ≥0.60 were considered as collinearity. According to this test, the CISI-PD was not included, because of collinearity with the SCOPA-Motor scale and the HY. Likewise, the SCOPA-PC was not introduced in the models, as it may have interactions with hallucinations (an item from the scale) and HADS. Finally, because the age at onset is dependent on the patient's baseline age and the disease duration, it was also excluded.
Statistical calculations were performed with the Statistical Package for the Social Sciences version 22.0 IBM (Armonk, New York).
Results
Sociodemographic and Disease-Related Characteristics
The sample was composed of 298 patients (186 men and 112 women). Applying the MDS criteria, 72 participants (24.2%) were classified as NC, 82 (27.5%) as PD-MCI, and 144 (48.3%) as PDD (Table 2).
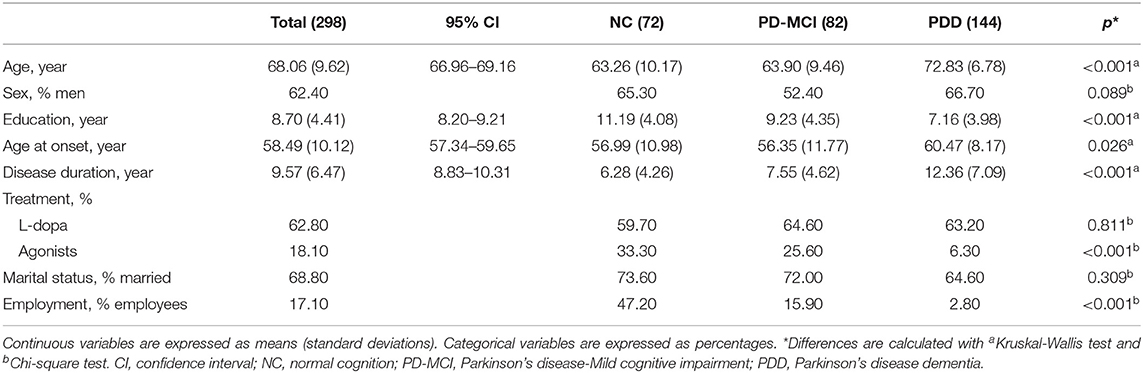
Table 2. Sociodemographic and disease-related features of study groups.
The mean age of the total sample was 68.06 [standard deviation (SD) = 9.62] years with 8.7 (SD = 4.41) years of education. Parkinson disease MCI and PDD patients were significantly older and presented a lower education level than NC patients. No differences by sex were found between the three cognition groups. Overall, age at onset was 58.49 (SD = 10.12) years, with a statistically significantly higher age at onset in the PDD group than the other groups. The average duration of the disease at the time of data collection was 9.57 (SD = 6.47) years, being significantly higher in the cognitive impaired groups (12.36 for PDD vs. 6.28 years for NC). Dopamine agonists were more frequently taken in NC patients (33.3% in the intact vs. 6.3% in the PDD group, p < 0.05), and there were no significant differences regarding L-dopa treatment between the groups.
Motor and Non-motor Symptoms
Parkinson disease MCI and PDD patients presented a more severe stage of disease (according to HY), as well as a worse clinical, motor, and functional status (measured by the CISI-PD, SCOPA-Motor, and Barthel index, respectively) than NC patients. Regarding the cognitive sphere, as expected, all cognitive test scores were worse in the cognitively impaired groups, with the lowest scores for PDD patients. The latter also obtained the highest average score on the neuropsychiatric symptom scale (SCOPA-PC). Specifically, 43.8% of PDD patients exceeded the cutoff point for anxiety, and 55.6% surpassed it for depression. One-third of PDD patients (34%) had hallucinations, compared to only 8 and 5% in PD-MCI and NC, respectively. There were lower quality-of-life and more psychosocial consequences in the cognitively impaired groups. All tests showed significant differences (p < 0.05) between the three study groups (Table 3).
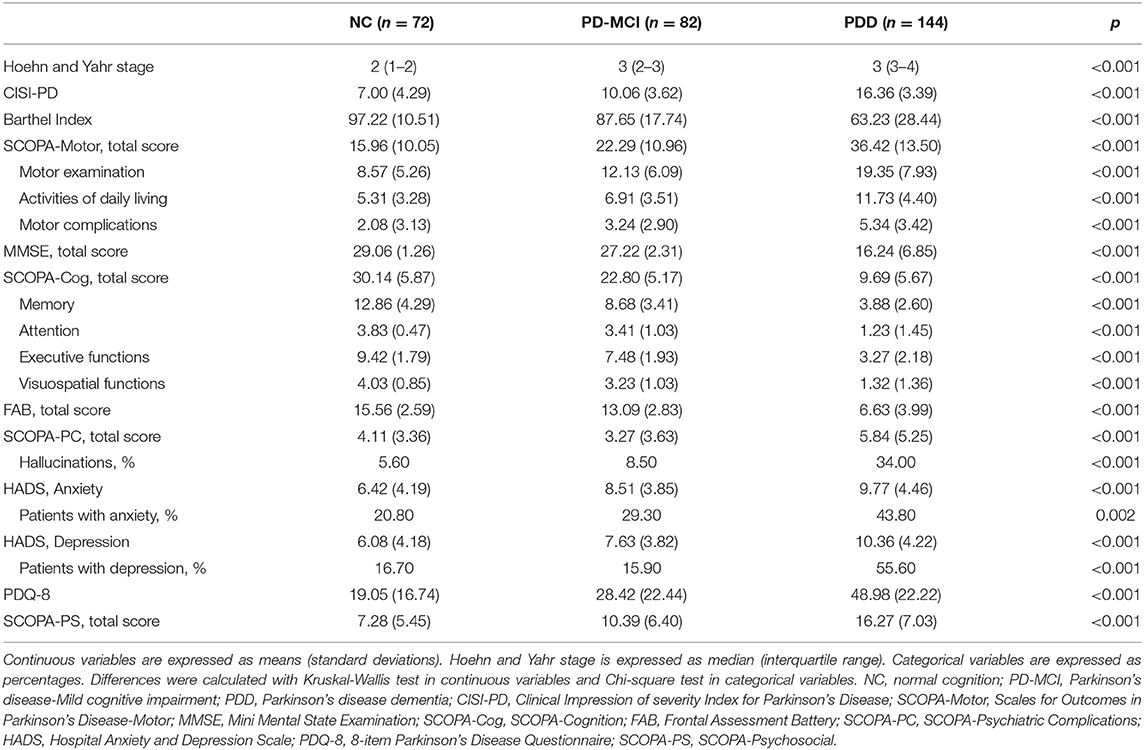
Table 3. Motor and non-motor symptoms in study groups.
Association Between Cognitive Impairment and Motor and Non-motor Symptoms
In the first regression model (Table 4), with cognitive impairment (PD-MCI or PDD) as dependent variable, two variables were found to be significant. Hoehn and Yahr stage (OR, 2.06; 95% CI, 1.10–3.85) and the motor exploration subscale in SCOPA-Motor scale (OR, 1.11; 95% CI, 1.01–1.21) showed a positive association with cognitive dysfunction. This model explained 49.0% of the variance.
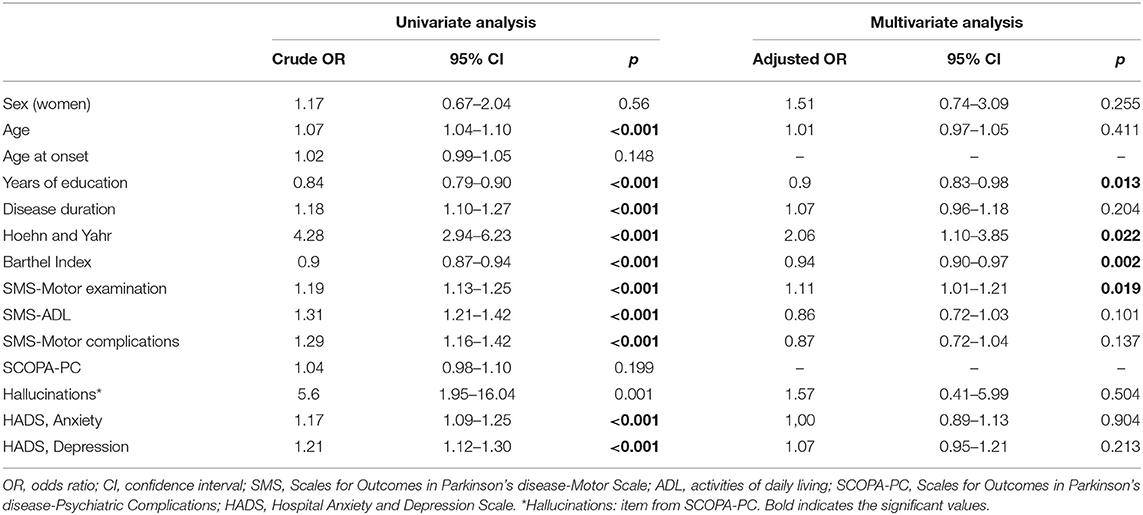
Table 4. Binary logistic regression model for normal cognition vs. cognitive impairment (PD-MCI/PDD).
The second regression model (Table 5), with dementia as dependent variable, showed that dementia was positively associated with higher age (OR, 1.30; 95% CI, 1.16–1.47) and disease duration (OR, 1.19; 95% CI, 1.07–1.32), an increased score in HADS-D (OR, 1.20; 95% CI, 1.06–1.35), and more hallucination symptoms (OR, 2.98; 95% CI, 1.16–7.69). The motor complications SCOPA-Motor subscale (OR, 0.82; 95% CI, 0.69–0.98) was negatively associated with the presence of dementia. This model explained 63.5% of the variance.
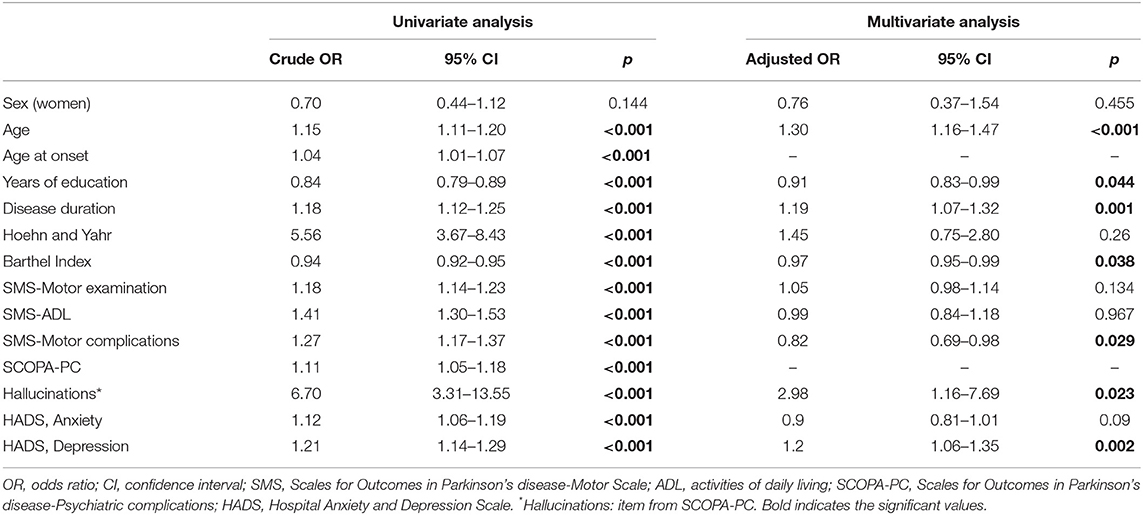
Table 5. Binary logistic regression model for dementia vs. no dementia (NC/PD-MCI).
Finally, in the multinomial model (Table 6), there was a positive association between the presence of PD-MCI and HY stage (OR, 2.45; 95% CI, 1.22–4.90). On the other hand, age (OR, 1.24; 95% CI, 1.07–1.44), HY stage (OR, 2.64; 95% CI, 1.17–5.98), and the depression HADS subscale (OR, 1.19; 95% CI, 1.02–1.37) were positively associated with the PDD group, whereas years of education (OR, 0.87; 95% CI, 0.78–0.97) was negatively associated. This model explained 61.6% of the variance.
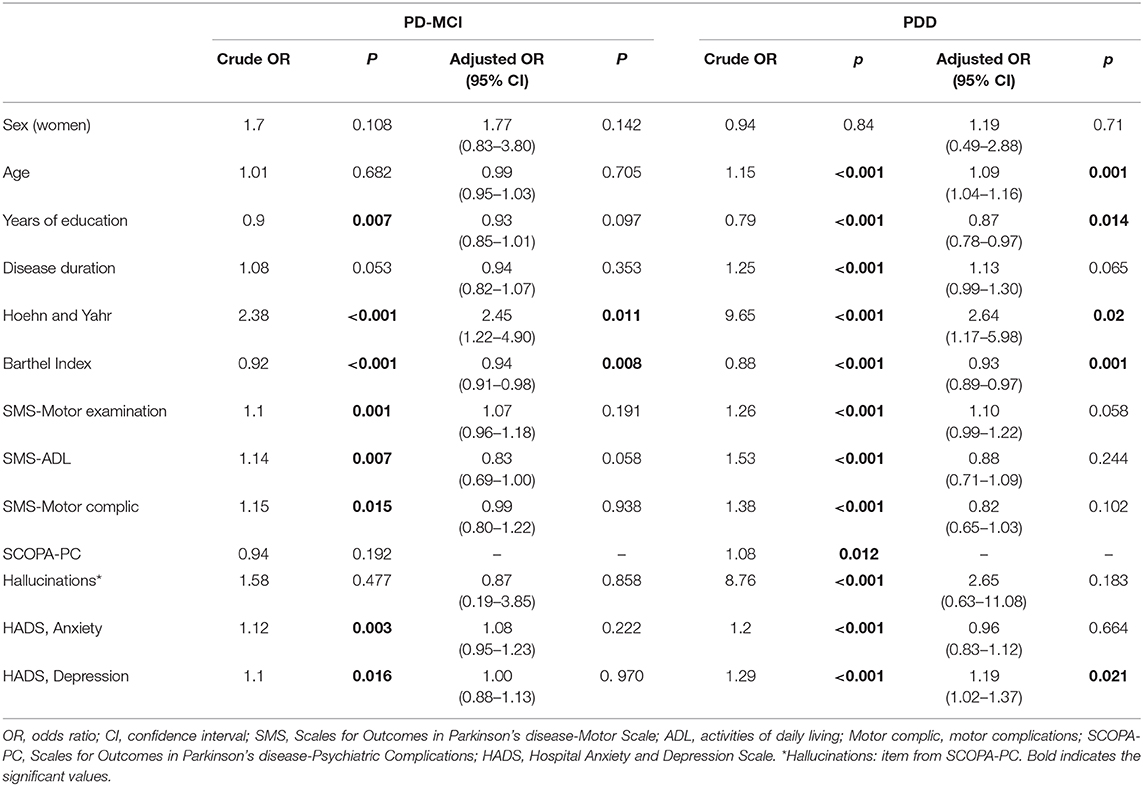
Table 6. Multinomial logistic regression model (NC vs. PD-MCI vs. PDD).
Discussion
This study applied the level I diagnostic criteria proposed by the MDS to analyze the differences between groups of PD patients according to their cognitive status. We found significant differences in sociodemographic, disease-related, and clinical variables depending on the severity of cognitive impairment, suggesting the usefulness of these criteria to classify PD-MCI and PDD patients according to their cognitive status. Recent studies reveal that levels I and II MCIs in PD classification have similar discriminative ability to predict the hazard of PDD (56). Nevertheless, previous studies suggest that level I criteria could be too broad and have a poor sensibility to classify PD patients; therefore, results should be interpreted carefully (57–59).
Participants with cognitive impairment (PD-MCI or PDD) were older and less educated than cognitively intact patients. In addition, they presented longer duration of PD, worse clinical and functional situation, higher levels of anxiety, depression, and greater presence of hallucinations than patients cognitively intact. Participants with cognitive impairment also had a worse quality of life and a more severe psychosocial impact of their disease, even in the early stages of cognitive decline (PD-MCI). Our findings are in line with other cross-sectional (24, 60, 61) and follow-up (24, 62) studies and highlight the importance of assessing these risk factors in the clinical setting. Moreover, non-motor symptoms have also been reported to affect the quality of life of PD patients to a greater extent than motor features, and this negative impact would appear from the very beginning of the disease (63).
Parkinson disease MCI and PDD patients were found to be more globally impaired than NC PD patients, with higher deterioration of both motor and non-motor symptoms, especially axial motor symptoms, depression, hallucinations, and cognitive performance measured by neuropsychological tests (64–66). All these features, considered even more disabling than the classic motor symptoms of PD, lead to a significant reduction in the quality of life of cognitive impaired patients.
A significant, although inverse, relationship between the degree of functionality (measured by the Barthel Index) and the presence of cognitive impairment was also found. This association, meaning that the less level of disability (corresponding to higher scores in Barthel index) is negatively associated with PD-MCI and PDD, compared to NC, is the only that consistently appeared in the binary and multinomial regression models. Multiple studies have already pointed out that dementia in PD results in a functional decline, and it has even been seen that the instrumental activities of daily life are also affected from the stage of MCI-PD (67). This relationship could be considered valid in both directions, because not only does cognitive impairment lead to greater disability, but also greater disability and physical frailty can eventually lead to “cognitive frailty,” meaning more decline in cognitive functions. As a matter of fact, these two conditions could share similar pathophysiological mechanisms, such as chronic inflammation, impaired hypothalamic–pituitary axis stress response, imbalanced energy metabolism, mitochondrial dysfunction, oxidative stress, and neuroendocrine dysfunction (68). A previous study has highlighted the important role of preserving cognitive functions to prevent disability and functional impairment (69).
The global severity of PD, measured by HY stage, and motor symptoms in PD were strongly associated with the presence of any type of cognitive impairment. Previous studies and reviews have shown that motor impairment is related to the overall presence of cognitive impairment (70, 71) and specifically to PD-MCI (72) and PDD (73, 74). In line with these previous studies, we found that the presence of cognitive impairment was associated with a more severe HY stage of PD. Conversely, the inverse association between motor complications and the presence of dementia that was found in one of our logistic regression models is not consistent with the reviewing literature that report motor complications as a risk factor for the development of PDD (24, 75). However, there is limited evidence on this topic, and the short length of the subscale that we have used (only four items, two for dyskinesias, and two for motor fluctuations) in combination with the lack of information on patient's treatment could explain a negative association between dementia and motor complications. Moreover, one study found that dyskinesias, but not motor fluctuations, were significantly related to dementia (24).
Our findings suggest that PD-MCI and PDD patients showed more neuropsychiatric symptoms than the NC patients. In the vast majority of studies, with different rating scales, neuropsychiatric symptoms seem to be related to cognitive impairment (74). Moreover, these disruptions could independently affect to disease progression by means of damaging frontal–subcortical pathways (76). Our study has found that behavior disorders are highly common in PD, and as suggested in previous studies, there may be a certain overlap between this symptomatology and cognitive symptoms (77).
We found a high prevalence of anxiety, depression, and hallucinations in PDD patients. Studies have shown that these features occur in ~30% of PD patients, often in the early stage of the disease (3). In binary logistic regression models, a statistical association between the last two and the presence of PDD was also found, in agreement with previous studies (12, 66). Visual hallucinations have been proposed as predictors of future development of dementia in patients with PD (12, 22). With the presence of cognitive dysfunction emerges the possibility of a higher frequency of hallucinations and depressive symptomatology. Studies indicate that both dementia and visual hallucinations share the same limbic system networks (24). Moreover, depression in PD has been associated to decreased white matter in the fornix, as well as cognitive impairment and apathy (78), and differences in brain circuitry appear since mild stages of depression (79).
Higher age and low educational level are well-known risk factors in the general population for developing cognitive impairment and dementia (24, 71), and the same is true for PDD (30, 36, 41, 49), as shown in our study. According to some authors, advanced age in PD is associated with a much higher risk of dementia than the effect of age alone (24), suggesting some kind of interaction effect between age and severity of PD in the risk of dementia (60). On the other hand, the relationship between age, educational level, and PD-MCI is not completely clear (72) but higher educational level seems to be a protective factor in recent studies, in line with our trends (80, 81).
Our results did not find association between gender and cognitive impairment, in agreement with previous studies (66, 72). As women are older than men when they start with the symptoms, they have a shorter disease duration, compared with men of the same age. Therefore, men with PD would have a more advanced disease stage than women of the same age, increasing their risk of PDD (71). However, there are also studies that have found an association between male sex and PDD/MCI-PD after controlling for age and disease duration (21, 65, 82), so the significance of this risk factor remains unclear.
Regarding the disease-related risk factors, a positive relationship between PD duration and PDD was found. However, age is also related to the duration of the disease, and for that reason, it is difficult to unravel the effects of each one on the risk of dementia. Furthermore, a very recent cross-sectional study assessing dementia in long-term PD patients did not find any significant differences between age, age at onset, or disease duration between PD patients with and without dementia (83).
Several limitations of this study should be acknowledged. Although we carried out the assessment during “on” state, cognitive fluctuations are always possible in PD. Because we performed a single evaluation over time, and PRO scales (HADS, SCOPA-PS and PDQ-8) in cognitive impairment patients were completed by caregivers (proxy evaluations), the results have to be taken with caution and should not be interpreted as causal. In addition, we do not know the premorbid performance or cognitive reserve of the participating patients, and the results of cognitive scales could have been affected by these factors.
Our study, designed for a broader goal, did not allow applying a completely exhaustive neuropsychological evaluation. Therefore, only the “possible” PD-MCI and PDD status could be achieved. However, all the applied tests have been widely validated in the literature, and in particular, the screening test used, SCOPA-Cog, was proposed by the MDS as a scale of global cognitive abilities validated for use in PD, whose clinimetric characteristics are satisfactory (84). This fact increases the reliability of the finding results.
At last, we would like to remark that we did not carry out a cluster analysis in this study, as there is no widely accepted consensus of how best to group patients (85). Yet, the criteria to identify subtypes and predict individual prognosis remain unclear and therefore lack clinical applicability and reproducibility (30). Moreover, differences in inclusion criteria from datasets, variable selection, and methodology between studies using cluster analysis have made it difficult to compare the subtypes, and the features describing them can be confusing and overlapping (86). Most of studies are cross-sectional, with a short follow-up, so they are often considered of limited utility (87). Finally, the division of PD into major subtypes has been criticized because it could be a simplification of the heterogeneous reality in the disease (36).
In this study, cognitive decline was associated with a worse disease stage at a global, psychiatric, and psychosocial level and therefore with an impairment of quality of life. We also observed that the patients with greater physical disability had worse cognitive functioning, so it seems important to identify the progression of disease to prevent cognitive impairment.
Some patient characteristics, such as age and lower educational level, were independently associated with dementia, as reported in previous studies. These data could help to understand the deeply impact that cognitive decline has on PD prognosis and highlight the importance of design and deliver integrated care for PD patients and their families. The greater knowledge on non-motor features would undoubtedly lead to a more accurate PD diagnosis and better treatments. As a result, the quality of life of these patients and the living conditions of their caregivers and family members would also improve. We strongly recommend assessing cognitive status at the time of PD diagnosis; exploring premorbid cognitive status, appearance, and type of deficits; and monitoring changes in disease severity over time. It is also relevant to pay special attention to neuropsychiatric symptoms, mainly depression and presence of hallucinations, as they seem to be strongly associated with cognitive impairment. Nevertheless, further research is required to understand the underlying pathophysiological mechanisms that link cognitive impairment with the remaining non-motor symptoms in PD.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements, as all datasets were fully anonymized prior to transfer and processing. Our paper is a retrospective (secondary) study, not requiring review and approval.
Author Contributions
PM-M initiated and designed the study, and collected the data within the Cog-PD study. AS-G, CR-B, and MF conducted the data analysis and wrote the main manuscript text. All authors reviewed the manuscript.
Funding
This study was partially funded by the QASP research project (Institute of Health Carlos III, Intramural Strategical Action in Health AESI 2018, Ref: PI18CIII/00046).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
To all patients and caregivers that made this study possible. To the researchers that conducted the Cog-PD study, from which the data were collected:
- C. Falup-Pecurariu, from Department of Neurology, University Hospital, Faculty of Medicine, Transilvania University, Braṣov, Romania.
- M. Serrano-Dueñas, from Movement Disorder and Biostatistic Units and Neurological Service, in Carlos Andrade Marín Hospital and Medicine Faculty, Pontifical Catholic University of Ecuador, Quito, Ecuador.
- F. J. Carod Artal, from Department of Neurology, Virgen de la Luz Hospital, Cuenca, Spain.
- J. M. Rojo, Department of Statistics, Centre of Human and Social Sciences, Spanish Council for Scientific Research, Madrid, Spain.
- D. Aarsland, Department of Old Age Psychiatry, Institute of Psychiatry, Psychology & Neuroscience, King's College London, England.
This manuscript was partly presented as conference paper at the 2019 International Congress of Parkinson's Disease and Movement Disorders organized by International Parkinson and Movement Disorder Society (MDS), September 2019, Nice, France.
References
1. Xu Y, Yang J, Shang H. Meta-analysis of risk factors for Parkinson's disease dementia. Transl Neurodegener. (2016) 5:11. doi: 10.1186/s40035-016-0058-0
2. Pont-Sunyer C, Hotter A, Gaig C, Seppi K, Compta Y, Katzenschlager R, et al. The onset of nonmotor symptoms in Parkinson's disease (the ONSET PD study). Mov Disord. (2015) 30:229–37. doi: 10.1002/mds.26077
3. Xie F, Gao X, Yang W, Chang Z, Yang X, Wei X, et al. Advances in the research of risk factors and prodromal biomarkers of Parkinson's disease. ACS Chem Neurosci. (2019) 10:973–90. doi: 10.1021/acschemneuro.8b00520
4. Zou J, Chen Z, Wei X, Chen Z, Fu Y, Yang X, et al. Cystatin C as a potential therapeutic mediator against Parkinson's disease via VEGF-induced angiogenesis and enhanced neuronal autophagy in neurovascular units. Cell Death Dis. (2017) 8:e2854. doi: 10.1038/cddis.2017.240
5. Weng R, Wei X, Yu B, Zhu S, Yang X, Xie F, et al. Combined measurement of plasma cystatin C and low-density lipoprotein cholesterol: a valuable tool for evaluating progressive supranuclear palsy. Parkinsonism Relat Disord. (2018) 52:37–42. doi: 10.1016/j.parkreldis.2018.03.014
6. Xu J, Fu X, Pan M, Zhou X, Chen Z, Wang D, et al. Mitochondrial creatine kinase is decreased in the serum of idiopathic Parkinson's disease patients. Aging Dis. (2019) 10:601-10. doi: 10.14336/AD.2018.0615
7. Dujardin K, Leentjens AFG, Langlois C, Moonen AJH, Duits AA, Carette A-S, et al. The spectrum of cognitive disorders in Parkinson's disease: a data-driven approach. Mov Disord. (2013) 28:183–9. doi: 10.1002/mds.25311
8. de Lau LML, Verbaan D, Marinus J, van Hilten JJ. Survival in Parkinson's disease. Relation with motor and non-motor features. Parkinsonism Relat Disord. (2014) 20:613–6. doi: 10.1016/j.parkreldis.2014.02.030
9. Weintraub D, Tröster AI, Marras C, Stebbins G. Initial cognitive changes in Parkinson's disease. Mov Disord. (2018) 33:511–9. doi: 10.1002/mds.27330
10. Litvan I, Goldman JG, Tröster AI, Schmand BA, Weintraub D, Petersen RC, et al. Diagnostic criteria for mild cognitive impairment in Parkinson's disease: movement disorder society task force guidelines. Mov Disord. (2012) 27:349–56. doi: 10.1002/mds.24893
11. Dubois B, Burn D, Goetz C, Aarsland D, Brown RG, Broe GA, et al. Diagnostic procedures for Parkinson's disease dementia: recommendations from the movement disorder society task force. Mov Disord. (2007) 22:2314–24. doi: 10.1002/mds.21844
12. Aarsland D, Andersen K, Larsen JP, Lolk A, Kragh-Sørensen P. Prevalence and characteristics of dementia in Parkinson disease: an 8-year prospective study. Arch Neurol. (2003) 60:387–92. doi: 10.1001/archneur.60.3.387
13. Hughes TA, Ross HF, Musa S, Bhattacherjee S, Nathan RN, Mindham RH, et al. A 10-year study of the incidence of and factors predicting dementia in Parkinson's disease. Neurology. (2000) 54:1596–602. doi: 10.1212/WNL.54.8.1596
14. Postuma RB, Bertrand J-A, Montplaisir J, Desjardins C, Vendette M, Rios Romenets S, et al. Rapid eye movement sleep behavior disorder and risk of dementia in Parkinson's disease: a prospective study. Mov Disord. (2012) 27:720–6. doi: 10.1002/mds.24939
15. Zhang F, Niu L, Liu X, Liu Y, Li S, Yu H, et al. Rapid eye movement sleep behavior disorder and neurodegenerative diseases: an update. Aging Dis. (2020) 11:315–26. doi: 10.14336/AD.2019.0324
16. Zheng W, He R, Yan Z, Huang Y, Huang W, Cai Z, et al. Regulation of immune-driven pathogenesis in Parkinson's disease by gut microbiota. Brain Behav Immun. (2020) 87:890–7. doi: 10.1016/j.bbi.2020.01.009
17. Zou J, Chen Z, Liang C, Fu Y, Wei X, Lu J, et al. Trefoil factor 3, cholinesterase and homocysteine: potential predictors for Parkinson's disease dementia and vascular Parkinsonism dementia in advanced stage. Aging Dis. (2018) 9:51–65. doi: 10.14336/AD.2017.0416
18. Tao X, Yang W, Zhu S, Que R, Liu C, Fan T, et al. Models of poststroke depression and assessments of core depressive symptoms in rodents: How to choose? Exp Neurol. (2019) 322:113060. doi: 10.1016/j.expneurol.2019.113060
19. Zhu S, Wei X, Yang X, Huang Z, Chang Z, Xie F, et al. Plasma lipoprotein-associated phospholipase A2 and superoxide dismutase are independent predicators of cognitive impairment in cerebral small vessel disease patients: diagnosis and assessment. Aging Dis. (2019) 10:834–46. doi: 10.14336/AD.2019.0304
20. Yang W, Chang Z, Que R, Weng G, Deng B, Wang T, et al. Contra-directional expression of plasma superoxide dismutase with lipoprotein cholesterol and high-sensitivity c-reactive protein as important markers of parkinson's disease severity. Front Aging Neurosci. (2020) 12:53. doi: 10.3389/fnagi.2020.00053
21. Aarsland D, Bronnick K, Williams-Gray C, Weintraub D, Marder K, Kulisevsky J, et al. Mild cognitive impairment in Parkinson disease: a multicenter pooled analysis. Neurology. (2010) 75:1062–9. doi: 10.1212/WNL.0b013e3181f39d0e
22. Aarsland D, Andersen K, Larsen JP, Lolk A, Nielsen H, Kragh-Sørensen P. Risk of dementia in Parkinson's disease: a community-based, prospective study. Neurology. (2001) 56:730–6. doi: 10.1212/WNL.56.6.730
23. Mahieux F, Fénelon G, Flahault A, Manifacier MJ, Michelet D, Boller F. Neuropsychological prediction of dementia in Parkinson's disease. J Neurol Neurosurg Psychiatry. (1998) 64:178–83. doi: 10.1136/jnnp.64.2.178
24. Zhu K, van Hilten JJ, Marinus J. Predictors of dementia in Parkinson's disease; findings from a 5-year prospective study using the SCOPA-COG. Parkinsonism Relat Disord. (2014) 20:980–5. doi: 10.1016/j.parkreldis.2014.06.006
25. Jia X, Wang Z, Yang T, Li Y, Gao S, Wu G, et al. Entorhinal cortex atrophy in early, drug-naive Parkinson's disease with mild cognitive impairment. Aging Dis. (2019) 10:1221–32. doi: 10.14336/AD.2018.1116
26. Fereshtehnejad S-M, Romenets SR, Anang JBM, Latreille V, Gagnon J-F, Postuma RB. New clinical subtypes of Parkinson disease and their longitudinal progression: a prospective cohort comparison with other phenotypes. JAMA Neurol. (2015) 72:863–73. doi: 10.1001/jamaneurol.2015.0703
27. Qian E, Huang Y. Subtyping of Parkinson's disease - where are we up to? Aging Dis. (2019) 10:1130–9. doi: 10.14336/AD.2019.0112
28. Jankovic J, McDermott M, Carter J, Gauthier S, Goetz C, Golbe L, et al. Variable expression of Parkinson's disease: a base-line analysis of the DATATOP cohort. The Parkinson Study Group. Neurology. (1990) 40:1529–34. doi: 10.1212/WNL.40.10.1529
29. Stebbins GT, Goetz CG, Burn DJ, Jankovic J, Khoo TK, Tilley BC. How to identify tremor dominant and postural instability/gait difficulty groups with the movement disorder society unified Parkinson's disease rating scale: comparison with the unified Parkinson's disease rating scale. Mov Disord. (2013) 28:668–70. doi: 10.1002/mds.25383
30. Fereshtehnejad S-M, Zeighami Y, Dagher A, Postuma RB. Clinical criteria for subtyping Parkinson's disease: biomarkers and longitudinal progression. Brain J Neurol. (2017) 140:1959–76. doi: 10.1093/brain/awx118
31. Marras C, Chaudhuri KR. Nonmotor features of Parkinson's disease subtypes. Mov Disord. (2016) 31:1095–102. doi: 10.1002/mds.26510
32. Thenganatt MA, Jankovic J. Parkinson disease subtypes. JAMA Neurol. (2014) 71:499–504. doi: 10.1001/jamaneurol.2013.6233
33. Lawton M, Ben-Shlomo Y, May MT, Baig F, Barber TR, Klein JC, et al. Developing and validating Parkinson's disease subtypes and their motor and cognitive progression. J Neurol Neurosurg Psychiatry. (2018) 89:1279–87. doi: 10.1136/jnnp-2018-318337
34. van Rooden SM, Colas F, Martínez-Martín P, Visser M, Verbaan D, Marinus J, et al. Clinical subtypes of Parkinson's disease. Mov Disord. (2011) 26:51–8. doi: 10.1002/mds.23346
35. Sauerbier A, Rosa-Grilo M, Qamar MA, Chaudhuri KR. Nonmotor Subtyping in Parkinson's Disease. Int Rev Neurobiol. (2017) 133:447–78. doi: 10.1016/bs.irn.2017.05.011
36. Sauerbier A, Jenner P, Todorova A, Chaudhuri KR. Non motor subtypes and Parkinson's disease. Parkinsonism Relat Disord. (2016) 22(Suppl. 1):S41–6. doi: 10.1016/j.parkreldis.2015.09.027
37. Uribe C, Segura B, Baggio HC, Abos A, Garcia-Diaz AI, Campabadal A, et al. Progression of Parkinson's disease patients' subtypes based on cortical thinning: 4-year follow-up. Parkinsonism Relat Disord. (2019) 64:286–92. doi: 10.1016/j.parkreldis.2019.05.012
38. de Pablo-Fernández E, Lees AJ, Holton JL, Warner TT. Prognosis and neuropathologic correlation of clinical subtypes of Parkinson disease. JAMA Neurol. (2019) 76:470–9. doi: 10.1001/jamaneurol.2018.4377
39. Martin GP, McDonald KR, Allsop D, Diggle PJ, Leroi I. Apathy as a behavioural marker of cognitive impairment in Parkinson's disease: a longitudinal analysis. J Neurol. (2020) 267:214–27. doi: 10.1007/s00415-019-09538-z
40. Martinez-Martin P, Falup-Pecurariu C, Rodriguez-Blazquez C, Serrano-Dueñas M, Carod Artal FJ, Rojo Abuin JM, et al. Dementia associated with Parkinson's disease: applying the movement disorder society task force criteria. Parkinsonism Relat Disord. (2011) 17:621–4. doi: 10.1016/j.parkreldis.2011.05.017
41. Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's disease. J Neurol Neurosurg Psychiatry. (1988) 51:745–52. doi: 10.1136/jnnp.51.6.745
42. Hoehn MM, Yahr MD. Parkinsonism: onset, progression, and mortality. Neurology. (2001) 57(10 Suppl. 3):S11–26. doi: 10.1212/wnl.17.5.427
43. Martínez-Martín P, Rodríguez-Blázquez C, Forjaz MJ, de Pedro J, Spanish-American Longitudinal PD Patient Study Group. The clinical impression of severity index for Parkinson's disease: international validation study. Mov Disord. (2009) 24:211–7. doi: 10.1002/mds.22320
44. Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. (1965) 14:61–5. doi: 10.1037/t02366-000
45. Marinus J, Visser M, Stiggelbout A, Rabey J, Martinez-Martin P, Bonuccelli U, et al. A short scale for the assessment of motor impairments disabilities in Parkinson's disease: the SPES/SCOPA. J Neurol Neurosurg Psychiatry. (2004) 75:388–95. doi: 10.1136/jnnp.2003.017509
46. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
47. Marinus J, Visser M, Verwey NA, Verhey FRJ, Middelkoop HAM, Stiggelbout AM, et al. Assessment of cognition in Parkinson's disease. Neurology. (2003) 61:1222–8. doi: 10.1212/01.WNL.0000091864.39702.1C
48. Dubois B, Slachevsky A, Litvan I, Pillon B. The FAB: a Frontal Assessment Battery at bedside. Neurology. (2000) 55:1621–6. doi: 10.1212/WNL.55.11.1621
49. Hurtado-Pomares M, Terol-Cantero MC, Sánchez-Pérez A, Leiva-Santana C, Peral-Gómez P, Valera-Gran D, et al. Measuring executive dysfunction in Parkinson's disease: reliability and validity of the Spanish version of Frontal Assessment Battery (FAB-E). PLoS ONE. (2018) 13:e0207698. doi: 10.1371/journal.pone.0207698
50. Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL. A new clinical scale for the staging of dementia. Br J Psychiatry J Ment Sci. (1982) 140:566–72. doi: 10.1192/bjp.140.6.566
51. Visser M, Verbaan D, van Rooden SM, Stiggelbout AM, Marinus J, van Hilten JJ. Assessment of psychiatric complications in Parkinson's disease: The SCOPA-PC. Mov Disord. (2007) 22:2221–8. doi: 10.1002/mds.21696
52. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
53. Peto V, Jenkinson C, Fitzpatrick R. PDQ-39: a review of the development, validation and application of a Parkinson's disease quality of life questionnaire and its associated measures. J Neurol. (1998) 245(Suppl. 1):S10–4. doi: 10.1007/PL00007730
54. Marinus J, Visser M, Martínez-Martín P, van Hilten JJ, Stiggelbout AM. A short psychosocial questionnaire for patients with Parkinson's disease: the SCOPA-PS. J Clin Epidemiol. (2003) 56:61–7. doi: 10.1016/S0895-4356(02)00569-3
55. Isella V, Mapelli C, Morielli N, Siri C, de Gaspari D, Pezzoli G, et al. Diagnosis of possible mild cognitive impairment in Parkinson's disease: validity of the SCOPA-Cog. Parkinsonism Relat Disord. (2013) 19:1160–3. doi: 10.1016/j.parkreldis.2013.08.008
56. Hoogland J, Boel JA, de Bie RMA, Schmand BA, Geskus RB, Dalrymple-Alford JC, et al. Risk of Parkinson's disease dementia related to level I MDS PD-MCI. Mov Disord. (2019) 34:430–5. doi: 10.1002/mds.27617
57. Szeto JYY, Mowszowski L, Gilat M, Walton CC, Naismith SL, Lewis SJG. Assessing the utility of the movement disorder society task force level 1 diagnostic criteria for mild cognitive impairment in Parkinson's disease. Parkinsonism Relat Disord. (2015) 21:31–5. doi: 10.1016/j.parkreldis.2014.10.020
58. Barton B, Grabli D, Bernard B, Czernecki V, Goldman JG, Stebbins G, et al. Clinical validation of movement disorder society-recommended diagnostic criteria for Parkinson's disease with dementia. Mov Disord. (2012) 27:248–53. doi: 10.1002/mds.24059
59. Uysal-Cantürk P, Hanagasi HA, Bilgiç B, Gürvit H, Emre M. An assessment of movement disorder society task force diagnostic criteria for mild cognitive impairment in Parkinson's disease. Eur J Neurol. (2018) 25:148–53. doi: 10.1111/ene.13467
60. Cholerton BA, Zabetian CP, Quinn JF, Chung KA, Peterson A, Espay AJ, et al. Pacific Northwest Udall Center of excellence clinical consortium: study design and baseline cohort characteristics. J Park Dis. (2013) 3:205–14. doi: 10.3233/JPD-130189
61. Campos LS, Guimarães RP, Piovesana LG, de Azevedo PC, Santos LMB, D'Abreu A. Clinical predictors of cognitive impairment and psychiatric complications in Parkinson's disease. Arq Neuropsiquiatr. (2015) 73:390–5. doi: 10.1590/0004-282X20150016
62. Broeders M, de Bie RMA, Velseboer DC, Speelman JD, Muslimovic D, Schmand B. Evolution of mild cognitive impairment in Parkinson disease. Neurology. (2013) 81:346–52. doi: 10.1212/WNL.0b013e31829c5c86
63. Müller B, Assmus J, Herlofson K, Larsen JP, Tysnes O-B. Importance of motor vs. non-motor symptoms for health-related quality of life in early Parkinson's disease. Parkinsonism Relat Disord. (2013) 19:1027–32. doi: 10.1016/j.parkreldis.2013.07.010
64. Aarsland D, Andersen K, Larsen JP, Perry R, Wentzel-Larsen T, Lolk A, et al. The rate of cognitive decline in Parkinson disease. Arch Neurol. (2004) 61:1906–11. doi: 10.1001/archneur.61.12.1906
65. Pigott K, Rick J, Xie SX, Hurtig H, Chen-Plotkin A, Duda JE, et al. Longitudinal study of normal cognition in Parkinson disease. Neurology. (2015) 85:1276–82. doi: 10.1212/WNL.0000000000002001
66. Schrag A, Siddiqui UF, Anastasiou Z, Weintraub D, Schott JM. Clinical variables and biomarkers in prediction of cognitive impairment in patients with newly diagnosed Parkinson's disease: a cohort study. Lancet Neurol. (2017) 16:66–75. doi: 10.1016/S1474-4422(16)30328-3
67. Pirogovsky E, Schiehser DM, Obtera KM, Burke MM, Lessig SL, Song DD, et al. Instrumental activities of daily living are impaired in Parkinson's disease patients with mild cognitive impairment. Neuropsychology. (2014) 28:229–37. doi: 10.1037/neu0000045
68. Ma L, Chan P. Understanding the physiological links between physical frailty and cognitive decline. Aging Dis. (2020) 11:405–18. doi: 10.14336/AD.2019.0521
69. Wang CY, Chan L, Wu D, Chi W-C, Yen C-F, Liao H-F, et al. Effect of cognitive disability and ambulation status on functioning in moderate-to-advanced Parkinson disease. Front Neurol. (2019) 10:1360. doi: 10.3389/fneur.2019.01360
70. Aarsland D, Creese B, Politis M, Chaudhuri KR, Ffytche DH, Weintraub D, et al. Cognitive decline in Parkinson disease. Nat Rev Neurol. (2017) 13:217–31. doi: 10.1038/nrneurol.2017.27
71. Marinus J, Zhu K, Marras C, Aarsland D, van Hilten JJ. Risk factors for non-motor symptoms in Parkinson's disease. Lancet Neurol. (2018) 17:559–68. doi: 10.1016/S1474-4422(18)30127-3
72. Monastero R, Cicero CE, Baschi R, Davì M, Luca A, Restivo V, et al. Mild cognitive impairment in Parkinson's disease: the Parkinson's disease cognitive study (PACOS). J Neurol. (2018) 265:1050–8. doi: 10.1007/s00415-018-8800-4
73. Hoogland J, Boel JA, de Bie RMA, Geskus RB, Schmand BA, Dalrymple-Alford JC, et al. Mild cognitive impairment as a risk factor for Parkinson's disease dementia. Mov Disord. (2017) 32:1056–65. doi: 10.1002/mds.27002
74. Wang Q, Zhang Z, Li L, Wen H, Xu Q. Assessment of cognitive impairment in patients with Parkinson's disease: prevalence and risk factors. Clin Interv Aging. (2014) 9:275–81. doi: 10.2147/CIA.S47367
75. Solla P, Cannas A, Floris GL, Orofino G, Costantino E, Boi A, et al. Behavioral, neuropsychiatric and cognitive disorders in Parkinson's disease patients with and without motor complications. Prog Neuropsychopharmacol Biol Psychiatry. (2011) 35:1009–13. doi: 10.1016/j.pnpbp.2011.02.002
76. Kulisevsky J, Pagonabarraga J, Pascual-Sedano B, García-Sánchez C, Gironell A, Trapecio Group Study. Prevalence and correlates of neuropsychiatric symptoms in Parkinson's disease without dementia. Mov Disord. (2008) 23:1889–96. doi: 10.1002/mds.22246
77. McDermott KL, Fisher N, Bradford S, Camicioli R. Parkinson's disease mild cognitive impairment classifications and neurobehavioral symptoms. Int Psychogeriatr. (2018) 30:253–60. doi: 10.1017/S1041610217002265
78. Hollocks MJ, Lawrence AJ, Brookes RL, Barrick TR, Morris RG, Husain M, et al. Differential relationships between apathy and depression with white matter microstructural changes and functional outcomes. Brain J Neurol. (2015) 138(Pt 12):3803–15. doi: 10.1093/brain/awv304
79. Dobkin RD, Interian A. Improved understanding, detection, and management of neuropsychiatric complications: essential components to the optimal treatment of Parkinson's disease. Int Psychogeriatr. (2019) 31:1–4. doi: 10.1017/S1041610219000048
80. Nie K, Gao Y, Mei M, Guo M, Huang Z, Wang L, et al. The clinical characteristics and cognitive features of mild cognitive impairment in Parkinson's disease and the analysis of relevant factors. J Clin Neurosci. (2019) 63:142–8. doi: 10.1016/j.jocn.2019.01.021
81. Nicoletti A, Luca A, Baschi R, Cicero CE, Mostile G, Davì M, et al. Incidence of mild cognitive impairment and dementia in Parkinson's disease: the Parkinson's disease cognitive impairment study. Front Aging Neurosci. (2019) 11:21. doi: 10.3389/fnagi.2019.00021
82. Levy G, Tang MX, Cote LJ, Louis ED, Alfaro B, Mejia H, et al. Motor impairment in PD: relationship to incident dementia and age. Neurology. (2000) 55:539–44. doi: 10.1212/WNL.55.4.539
83. Szeto JYY, Walton CC, Rizos A, Martinez-Martin P, Halliday GM, Naismith SL, et al. Dementia in long-term Parkinson's disease patients: a multicentre retrospective study. NPJ Park Dis. (2020) 6:2. doi: 10.1038/s41531-019-0106-4
84. Martínez-Martín P, Frades-Payo B, Rodríguez-Blázquez C, Forjaz MJ, de Pedro-Cuesta J, Grupo Estudio Longitudinal de Pacientes con Enfermedad de Parkinson. Psychometric attributes of scales for outcomes in Parkinson's disease-cognition (SCOPA-Cog), Castilian language. Rev Neurol. (2008) 47:337–43. doi: 10.33588/rn.4707.2008430
85. Lawton M, Baig F, Rolinski M, Ruffman C, Nithi K, May MT, et al. Parkinson's disease subtypes in the Oxford Parkinson Disease Centre (OPDC) discovery cohort. J Park Dis. (2015) 5:269–79. doi: 10.3233/JPD-140523
86. Fereshtehnejad S-M, Postuma RB. Subtypes of Parkinson's disease: what do they tell us about disease progression? Curr Neurol Neurosci Rep. (2017) 17:34. doi: 10.1007/s11910-017-0738-x
Keywords: cognitive dysfunction, Parkinson's disease, motor and non-motor symptoms, dementia, mild cognitive impairment, clinical characteristics
Citation: Simon-Gozalbo A, Rodriguez-Blazquez C, Forjaz MJ and Martinez-Martin P (2020) Clinical Characterization of Parkinson's Disease Patients With Cognitive Impairment. Front. Neurol. 11:731. doi: 10.3389/fneur.2020.00731
Received: 11 April 2020; Accepted: 15 June 2020;
Published: 04 August 2020.
Edited by:
Emilia Mabel Gatto, Sanatorio de la Trinidad Mitre, ArgentinaReviewed by:
Pedro Chana-Cuevas, University of Santiago, ChileDennis Qing Wang, Southern Medical University, China
Copyright © 2020 Simon-Gozalbo, Rodriguez-Blazquez, Forjaz and Martinez-Martin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Simon-Gozalbo, YXNpZ284M0BnbWFpbC5jb20=