
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol., 31 July 2020
Sec. Neuro-Oncology and Neurosurgical Oncology
Volume 11 - 2020 | https://doi.org/10.3389/fneur.2020.00723
 Jozef Buday*
Jozef Buday* Jakub Albrecht
Jakub Albrecht Tadeas Mareš
Tadeas Mareš Gabriela PodgornáKlara HoráčkováLucie KališováJiri RabochMartin Anders
Gabriela PodgornáKlara HoráčkováLucie KališováJiri RabochMartin AndersThe safety and efficacy of electroconvulsive therapy (ECT) in patients with a brain tumor have been debated in the past without a clear conclusion. In the last large review published by Maltbie et al. in 1980, it was concluded that the presence of an intracranial mass should be considered an absolute contraindication to ECT. In our updated review, we investigated a total of 33 published and indexed case reports, case report series, and reviews of 75 individual patients who underwent ECT in the presence of a brain tumor over the last 80 years. Mounting case reports after the original Maltbie et al. review show that it is feasible to apply this method safely in patients with benign or otherwise clinically insignificant lesions. Certain precautionary measures, such as dexamethasone or phenytoin application before ECT, could lead to a further minimalization or even absence of adverse effects, particularly in higher risk individuals.
The safety and efficacy of electroconvulsive therapy (ECT) in patients with a brain tumor were debated in the past without a clear conclusion. In the last large review published by Maltbie et al. (1) in 1980, it was deemed that the presence of an intracranial mass should be considered an absolute contraindication to ECT. In our updated review, we investigated a total of 33 published and indexed case reports, case report series, and reviews of 75 individual patients who underwent ECT in the presence of a brain tumor over the last 80 years.
The main aim of our review was to find out whether the original conclusion of Maltbie et al. (1) (the presence of a brain tumor should be considered an absolute contraindication to ECT) can be challenged by collecting and analyzing all case reports, case report series, or mini reviews that emerged on this topic since the publication of this review 40 years ago. Our secondary goal was to provide a comprehensive overview about the occurrence and severity of adverse effects (AEs) after ECT in patients with a brain tumor and find possible methods to increase the safety of this important treatment modality in current scientific literature.
We followed the PRISMA statement (2) as a guide for conducting our systematic review. We have searched the electronic databases of Cochrane, PubMed, Journal of ECT, Biological Psychiatry, and Brain Stimulation using combinations of terms “electroconvulsive therapy,” “brain tumor,” and “electroconvulsive therapy,” “intracranial mass,” and “ECT,” “brain tumor.” The search was last updated in May 2020. The electronic search returned 651 abstracts and titles. We screened these abstracts and excluded studies that were duplicates or not directly relevant to the topic of this review. Our inclusion criteria were all original studies—case reports, letters to the Editor, case report series, mini reviews, reviews, or book chapters that reported on patients who underwent ECT with a previously known presence of a brain tumor OR patients in which the brain tumor was discovered during/shortly after a course of ECT. We excluded papers that revolved around the application of ECT in patients after tumor resection, aneurysms, or other vascular malformations; patients with a severe disease or malformation of the central nervous system (hydrocephalus, encephalitis, etc.) (3); and patients with tumors that were outside the intracranial space. Only papers in English were considered for this review. Further details are provided in Figure 1.
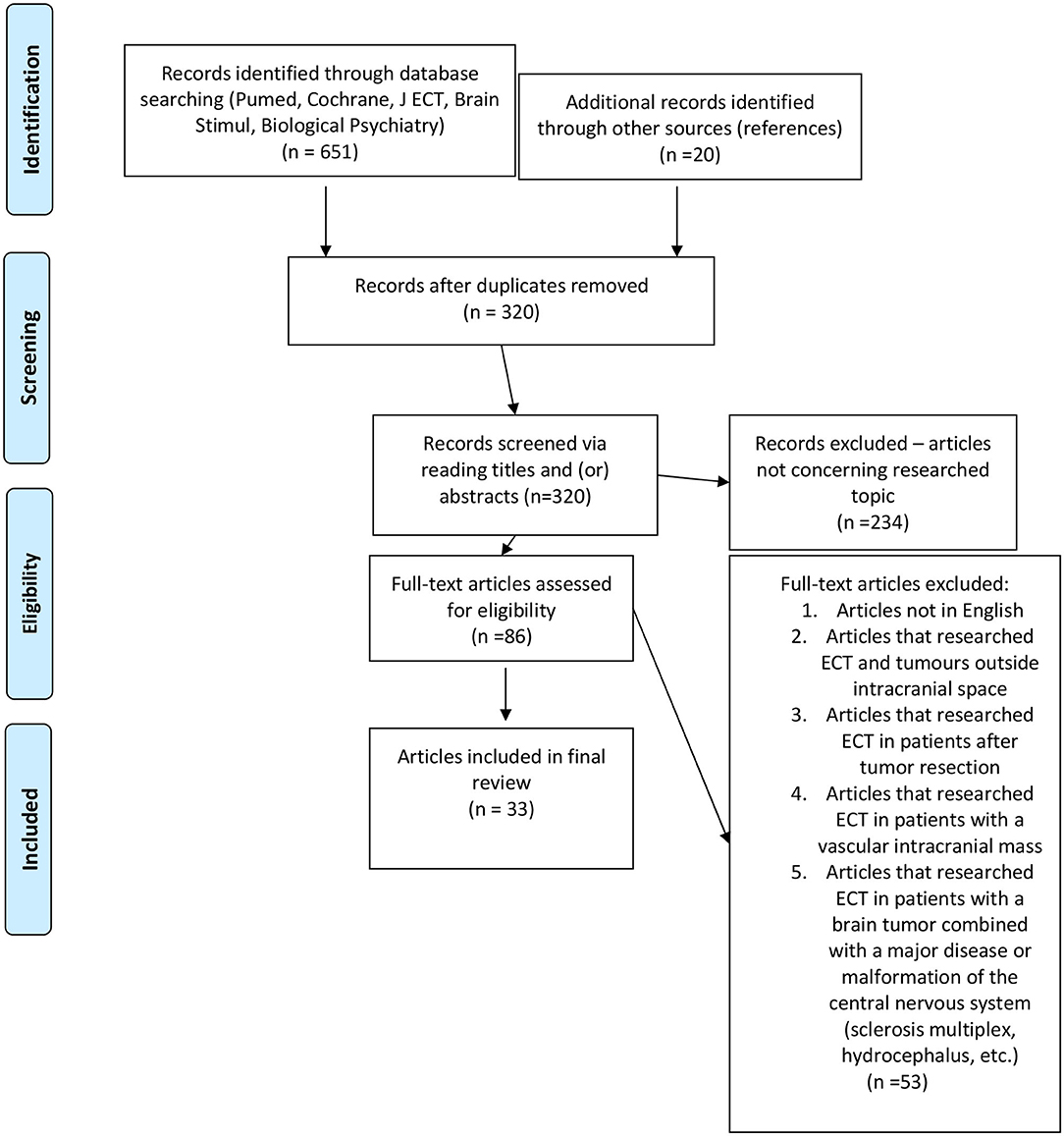
Figure 1. PRISMA flow chart of our search strategy. (“File:PRISMA flow chart for Wiki Journal of Medicine article.jpg” by Rwatson, 1955 is licensed under CC BY-SA 4.0/the template was used to draw a flow chart on the topic of our article).
The case reports up to 1980 were varied in the details provided—most of them lack the exact description of the type of ECT, stimulation parameters, device, and electrode placement (Table 1) and were already discussed in the Maltbie et al. (1) review. Nonetheless, we have summarized the available data from these individual case reports in Table 1. Because of the large variability in the quality of these articles up to 1980, we have focused our attention to summarize newer case reports, case report series, or mini reviews published between 1984 and 2020 (Table 2).
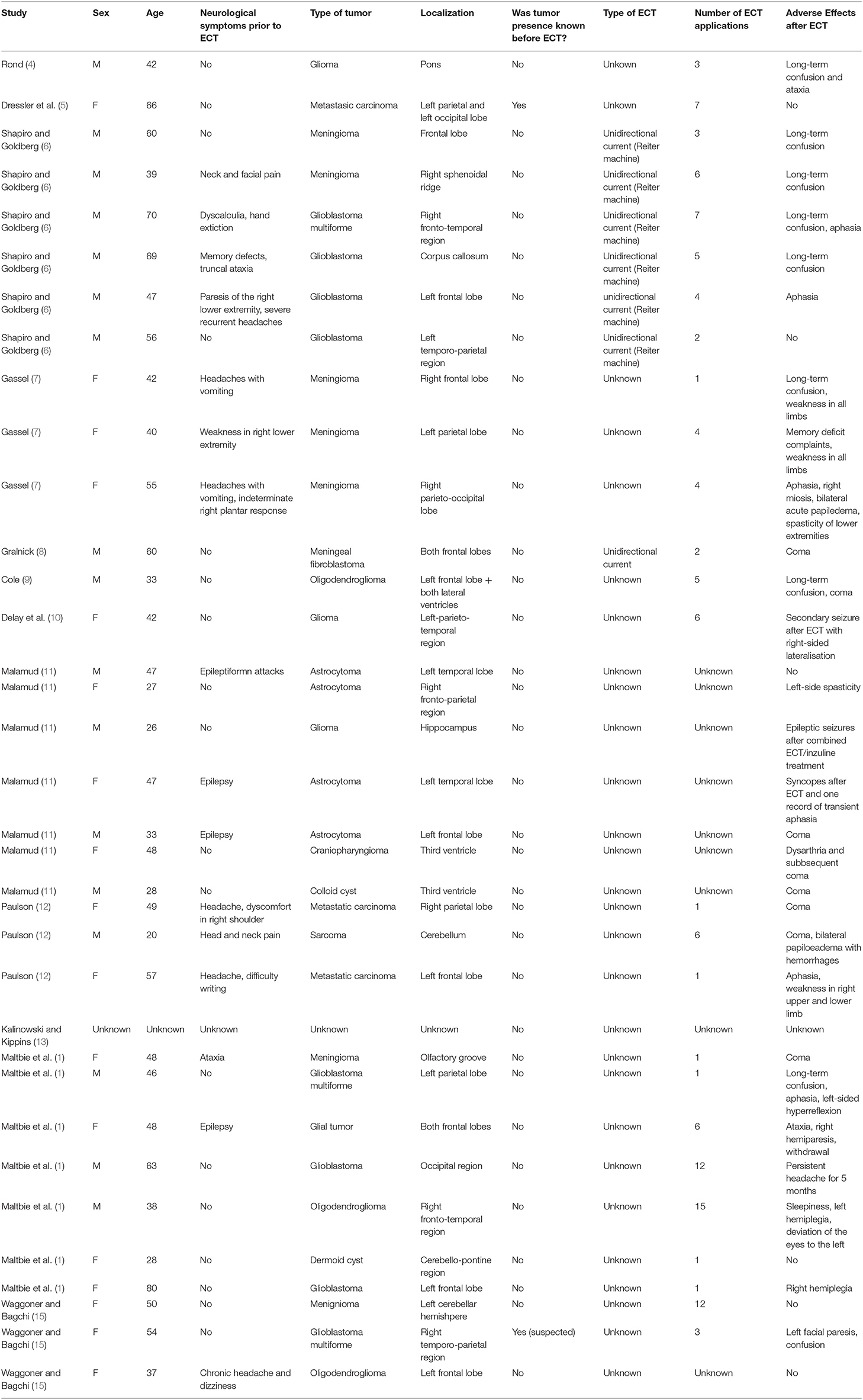
Table 1. ECT in patients with a brain tumor 1946–1980.
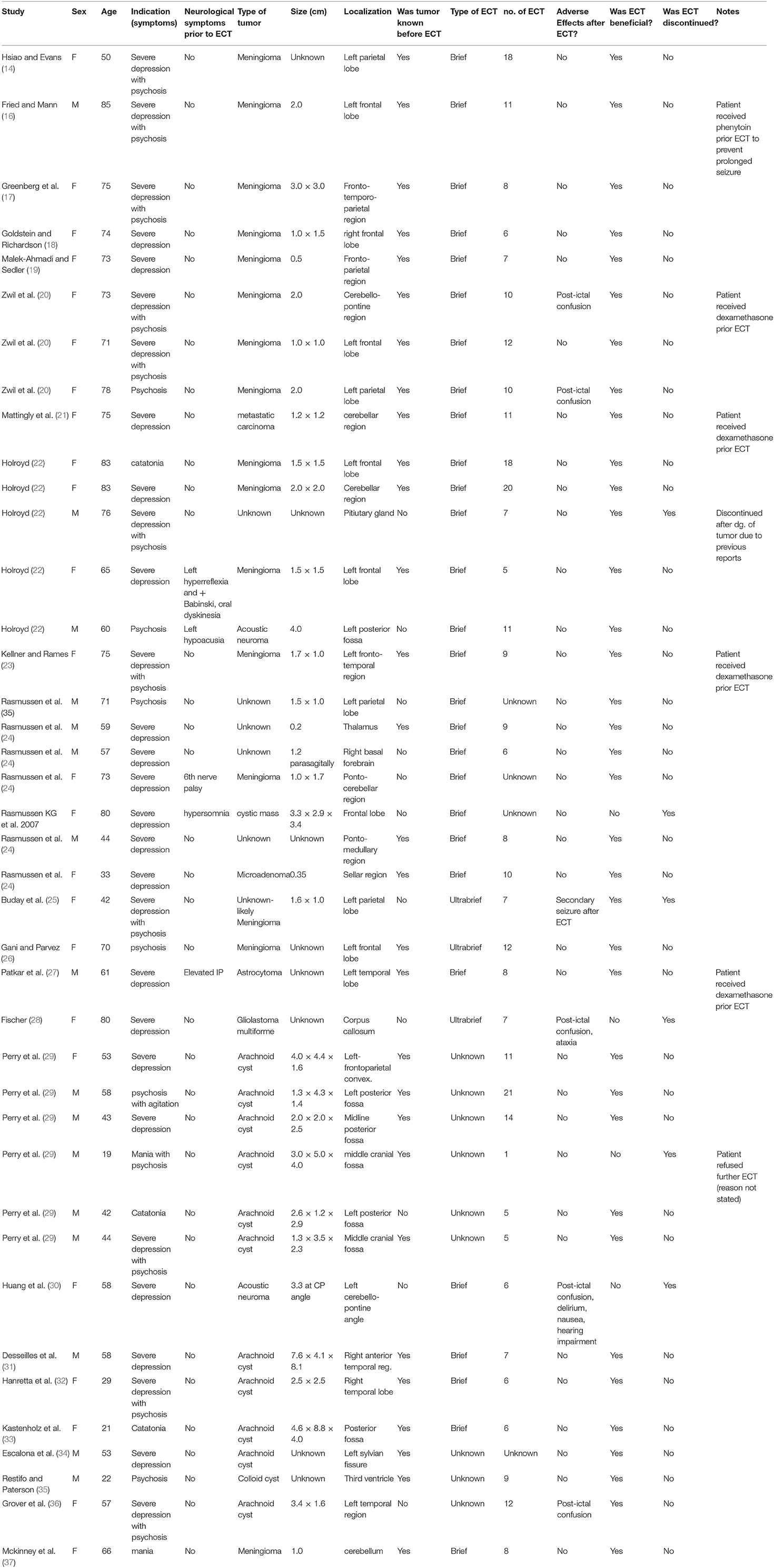
Table 2. ECT in patients with a brain tumor 1984–2020.
Outcome data were determined by scoring several questions:
• Were there any neurological symptoms present before ECT?
• Was the presence of the tumor known before ECT?
• What was the type of ECT used—pulse width, electrode placement, dosage, titration strategy?
• Were there any AEs present after ECT, especially neurological and lateralizing symptoms?
• Was ECT discontinued due to the presence of any AEs?
• What was the indication for ECT?
• Was the application of ECT beneficial for the patients according to the authors of the respective case report?
• How many sessions of ECT were applied?
• Were any precautionary measures undertaken if the presence of the brain tumor was known before ECT application?
Despite the large variation in quality and quantity of the information provided, we were also able to sort patients by their biological sex, age, type, localization, and size of the tumor.
The main bias of our review is the fact that the topic of ECT and brain tumor is likely underreported in general. The same weakness was pointed out by Maltbie et al. (1) in their original study from 1980. It is very likely that a substantial amount of patients with an undiagnosed brain tumor undergo this treatment without any observable side effects and are therefore not reported in scientific literature. On the other hand, it is possible that AEs after ECT treatment in this subgroup of patients are also underreported, as the newer case reports after 1980 consist largely of patients with clinically insignificant tumors. More advanced investigations, such as the analysis of registry-based data [health maintenance organization (HMO)/insurance claims, government regulation data] could provide a more clear and complex view of this topic.
Another weakness is the varied quality of the presented case reports. In particular, the authors generally did not specify as to how exactly the AEs were monitored after ECT (nor to what extent the patients were neurologically examined prior to ECT). It is therefore possible that these patients did manifest discreet symptoms that were not noticed and only the more obvious AEs were reported.
Starting from the first case report by Hsiao and Evans (14) in 1984 up to our own in 2019, we reviewed a total of 40 patients, which represents a comparable size-sample to the one analyzed by Maltbie et al. (1) between the years 1945 and 1980 (total of 35). In contrast with the previous review, the presence of a brain tumor was known before ECT in 29 patients (72.5%). Brief pulse width ECT was administered to 28 patients, ultrabrief pulse width to three, and in nine patients, we were unable to trace the pulse width.
The most common indication for ECT in this group of patients was severe depression (18 patients−45%) and psychosis, usually associated with a severe mood disorder (18 patients−45%). Three patients were indicated for ECT due to symptoms of catatonia and one patient for mania.
The most common type of tumor was a meningioma, which was present in 16 patients (40%), with arachnoid cysts coming in second place with 11 patients (27.5%).
Six patients (15% of the sample) manifested AEs after ECT. Out of this group, four patients developed postictal confusion; one patient manifested a set of several unusual, but reversible, symptoms (secondary myoclonic seizure with lateralization unresponsive to intravenous diazepam application, ping-pong gaze, and Todd's paralysis); and one patient was observed to develop a 3-day-long delirium with hearing impairment. All reported AEs were reversible.
ECT was discontinued in six patients (15%)—the first described by Holroyd (22) in 1993, where the treatment was stopped immediately after a random CT scan revealed a tumor in the pituitary area. Ironically, the patient did not show any AEs during ECT administration, and at the time, it was stopped only due to the previous series of negative case reports on the topic. The second cessation of ECT was in the case of an 80-year-old woman due to terminal-stage cancer (24). In another two cases, the ECT was canceled due to lack of effect and refusal to continue with the procedure from the side of the patient (28, 29). Huang et al. (30) described a patient who developed severe AEs after ECT including nausea, hearing loss, and a 3-day delirium—the patient was later diagnosed with acoustic neuroma, and ECT was discontinued. And finally, in our department, we halted ECT in a female patient who manifested a secondary seizure and was subsequently found to have an intracranial tumor in the left parietal lobe (25).
Five patients (12.5%) had neurological symptomatology prior to the administration (including one report of a patient with an elevated intracranial pressure), but none of them manifested any AEs following ECT administration. Five patients were premedicated with dexamethasone to prevent acute edema or phenytoin to prevent secondary seizures.
According to the authors of the respective case reports, ECT was beneficial for 36 patients (90%). ECT was ineffective in three cases and discontinued in one patient after he refused to undergo further treatment (the reason behind this decision was not stated).
Only one patient (27) was reported to have had elevated intracranial pressure prior to the procedure, and he underwent ECT without any AEs.
In this group of patients, we were able to determine the exact number of ECT sessions in 36 patients. The average number of sessions per patient was 9.47.
No patient was reported to have died as a result of ECT application in this sample. The average age of patients in this group was 59.72 years.
There seems to be a clear difference between the two similarly sized groups from 1945 to 1980 and 1984 to 2019. However, our results must also be seen as biased—the topic of ECT and brain tumor is likely in general underreported; in the majority (72.5%) of these new case reports, the presence of the brain tumor was known prior to ECT application which had allowed undertaking specialized precautions (23) (dexamethasone or phenytoin administration) in a substantial number of patients (12.5%), and last but not least, 40% of these reports constitute patients with benign meningiomas or clinically insignificant tumors, which is in contrast to the group of patients reported on by Maltbie et al. (1), where this group represents only seven patients (20%). It should be noted that the latter review consisted of a substantial amount of patients with more aggressive and clinically more significant tumors, such as gliomas (Table 1). We also point out a difference between patients with neurological symptoms manifesting prior to ECT administration-−12.5% of patients in the new group and 45.7% in the Maltbie et al. (1) sample.
Despite this bias, the case reports between 1984 and 2019 demonstrate that ECT can be applied safely in certain patients with an intracranial mass. The average number of ECT sessions was 9.47 in this group compared to 4.57 in the older group. Six patients manifested AEs after the treatment—out of these, only two patients discontinued treatment due to their presence. All AEs in the 1984–2019 sample were reversible, and the majority constituted of patients who were confused after the procedure—an AE not that rare even in patients undergoing ECT without a brain tumor.
We know that seizure activity increases blood pressure and cerebral blood flow, which can lead to an increased edema around the tumor and subsequently to an increase in intracranial pressure and eventually manifestation of neurological signs. This mechanism was first proposed by Carter (38) in 1977 and considered to be the likely cause of the more prominent AEs in this review reported by Huang et al. (30) and Buday et al. (25).
Dexamethasone was used in a substantial amount of patients (12.5%) to reduce the risk of this pathophysiological mechanism in the newer set of case reports. Phenytoin was administered to one patient to prevent a prolonged seizure. None of these individuals manifested AEs; it is therefore possible that the administration of these substrates prior to ECT may reduce the risk of an acute edema and prolonged seizure, respectively.
In their review, Maltbie et al. (1) suggested that more invasive and aggressive tumors might result in a higher incidence of AEs during ECT. The majority of patients in the newer case reports had benign, small, and clinically insignificant tumors, which seem to support the conclusion that this type of lesion poses a minimal risk increase in regard to ECT application. However, as several new case reports mention in this review, some patients with a brain tumor (especially a previously undiagnosed lesion) can manifest reversible, but unusual and concerning, AEs. Currently, neuroimaging is not mandatory before initiating ECT—it was reported several times that the yield of organic pathology if performed in all patients before undergoing ECT is very low (34, 39, 40). We suggest that any new neurological symptoms manifesting during and after ECT (such as a significant lateralization of the seizure, Todd's paralysis, aphasia, eye-movement disorders, secondary seizures, etc.) should prompt a complex neurological investigation and neuroimaging to exclude the presence of an intracranial mass (which might, depending on its localization, play a role in the psychopathology due to which ECT was indicated in the first place), another organic disease of the central nervous system, or even an acute problem, such as intracranial bleeding.
We must also consider that technological advancement and modern titration strategies that seek to individualize the dosage in each patient might also be one of the reasons why there are less and far more benign and reversible reported AEs (41). Unfortunately, in most cases between 1945 and 1980, it was not possible to track the type of devices, titration strategy, and dosage levels used during ECT. Based on the review of case reports emerging since 1984, it seems that the application of ECT is safer than it was originally presumed by Maltbie et al. (1) in 1980, and this method can be applied safely on a case-by-case basis.
We have reviewed a total of 33 articles of 75 individual patients who underwent ECT in the presence of a brain tumor over the last 80 years. Mounting case reports from 1984 show that this method can be safely administered in patients with benign, small, and otherwise clinically insignificant tumors. The application of ECT in this type of patients should be considered in a case-by-case basis after interdisciplinary consultation with a neurologist and neurosurgeon with a risk/benefit assessment. ECT practitioners should be vigilant of any AEs (especially neurological) manifesting during and after the procedure. The occurrence of such abnormal symptoms should prompt an immediate neurological investigation and proper imaging studies to exclude any underlying organic pathology. Certain precautionary measures, such as dexamethasone or phenytoin application before ECT, could lead to a further minimalization of AEs.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
This work was supported by MH CZ-DRO VFN64165, Q27/LF1.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Maltbie AA, Wingfield MS, Volow MR, Weiner RD, Sullivan JL, Cavenar JO. Electroconvulsive therapy in the presence of brain tumor. J Nerv Ment Dis. (1980) 168:400–5. doi: 10.1097/00005053-198007000-00002
2. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
3. Karliner W. ECT for patients with CNS disease. Psychosomatics. (1978) 19:781–3. doi: 10.1016/S0033-3182(78)70896-0
5. Dressler DM, Folk J. The treatment of depression with ECT in the presence of brain tumor. Am J Psychiatry. (1975) 132:1320–1. doi: 10.1176/ajp.132.12.1320
6. Shapiro MF, Goldberg HH. Electroconvulsive therapy in patients with structural disease of the central nervous system. Am J Med Sci. (1957) 233:186–95. doi: 10.1097/00000441-195702000-00011
7. Gassel MM. Deterioration after ECT in patients with intracranial meningioma. Arch Gen Psychiatry. (1960) 3:504–6. doi: 10.1001/archpsyc.1960.01710050054005
8. Gralnick AA. A fatality incident to electroshock treatment. J Nerv Ment Dis. (1945) 102:483–95. doi: 10.1097/00005053-194511000-00008
9. Cole G. The masking of organic brain disease by a schizophrenia-like illness. S Afr Med J. (1973) 47:731–3.
11. Malamud N. Psychiatric disorders with intracranial tumors of the limbic system. Arch Neurol. (1967) 13:113–23. doi: 10.1001/archneur.1967.00470260003001
13. Kalinowski LB, Kippins H. Pharmacological, Convulsive and Other Somatic Treatments in Psychiatry. New York, NY: Grune and Stratton (1969).
14. Hsiao JK, Evans DL. ECT in a depressed patient after craniotomy. Am J Psychiatry. (1984) 141:442–4. doi: 10.1176/ajp.141.3.442
15. Waggoner RW, Bagchi BK. Initial masking of organic brain changes by psychic symptoms. Am Psychiat J. (1953) 110:904–10. doi: 10.1176/ajp.110.12.904
16. Fried D, Mann JJ. Electroconvulsive treatment of patient with a known intracranial tumor. Biol Psychiatry. (1988) 23:176–80. doi: 10.1016/0006-3223(88)90088-1
17. Greenberg LB, Mofson R, Fink M. Prospective ECT in a delusional depressed patient with a frontal meningioma. Br J Psychiatry. (1988) 153:105–7. doi: 10.1192/bjp.153.1.105
18. Goldstein MZ, Richardson C. Meningioma with depression. Psychosomatics. (1988) 29:349–51. doi: 10.1016/S0033-3182(88)72377-4
19. Malek-Ahmadi P, Sedler RR. Electroconvulsive therapy and asymptomatic meningioma. Convuls Ther. (1990) 5:168–70.
20. Zwil AS, Bowring MA, Price TR, Goetz KL, Greenbarg JB, Kane-Wanger G. Prospective electroconvulsive therapy in the presence of intracranial tumor. Convuls Ther. (1990) 6:299–307.
21. Mattingly G, Figiel GS, Jarvis MR, Zorumski CF. Prospective uses of ECT in the presence of intracranial tumors (letter). J Neuropsychiatry Clin Neurosci. (1991) 3:459–63. doi: 10.1176/jnp.3.4.459
22. Holroyd S. Electroconvulsive therapy in elderly patients with intracranial tumor: A case series. Int J Geriat Psychiatry. (1993) 8:953–6. doi: 10.1002/gps.930081110
23. Kellner CH, Rames L. Dexamethasone pretreatment for ECT in a patient with meningioma. Clin Gerontol. (1990) 10:67–72. doi: 10.1300/J018v10n02_06
24. Rasmussen KG, Perry CL, Sutor B, Moore KM. ECT in patients with intracranial masses. J Neuropsychiatry Clin Neurosci. (2007) 19:191–3. doi: 10.1176/jnp.2007.19.2.191
25. Buday J, Albrecht J, Mareš T, Fabián V, Buday J, Raboch J, et al. Unusual set of adverse effects during right-unilateral ultrabrief electroconvulsive therapy led to the discovery of a brain tumor: a case report. J ECT. (2020) 36:69–71. doi: 10.1097/YCT.0000000000000618
26. Gani M, Parvez F. ECT in a patient with a meningioma and Takotsubo cardiomyopathy. Prog Neurol Psychiatry. (2016) 20:15–8. doi: 10.1002/pnp.450
27. Patkar AA, Hill KP, Weinstein SP, Schwartz SL. ECT in the presence of brain tumor and increased intracranial pressure: evaluation and reduction of risk. J ECT. (2000) 16:189–97. doi: 10.1097/00124509-200006000-00011
28. Fischer CE. Experience of electroconvulsive therapy in a case of glioblastoma multiforme. Psychiatry Clin Neurosci. (2004) 58:671. doi: 10.1111/j.1440-1819.2004.01320.x
29. Perry CL, Lindell EP, Rasmussen KG. ECT in patients with arachnoid cysts. J ECT. (2007) 23:36–7. doi: 10.1097/01.yct.0000264340.27072.e3
30. Huang WL, Hsieh MH, Liao SC. Acoustic neuroma identified after electroconvulsive therapy in a patient with recurrent major depression undifferentiated somatoform disorder. J ECT. (2010) 26:330–1. doi: 10.1097/YCT.0b013e3181cadc1f
31. Desseilles M, Thiry JC, Monville JF, Ansseau M, Makhinson M. Electroconvulsive therapy for depression in a patient with an intracranial arachnoid cyst. J ECT. (2009) 5:64–6. doi: 10.1097/YCT.0b013e3181729268
32. Hanretta AT, Akra I, Malek-Ahmadi P. Electroconvulsive therapy arachnoid cysts. J ECT. (2007) 23:126–7. doi: 10.1097/yct.0b013e318042b642
33. Kastenholz KJ, Rosenthal LJ, Dinwiddie SH. Electroconvulsive therapy in a patient with catatonia an intracranial arachnoid cyst. J ECT. (2014) 30:e53–4. doi: 10.1097/YCT.0000000000000182
34. Escalona PR, Coffey CE, Maus-Feldman J. Electroconvulsive therapy in a depressed patient with an intracranial arachnoid cyst: a brain magnetic resonance imaging study. Convuls Ther. (1991) 7:133–8.
35. Restifo S, Paterson R. Brief case report: uneventful electroconvulsive therapy in a patient with psychosis and coincidental colloid cyst of the third ventricle. Aust N Z J Psychiatry. (1999) 33:603.
36. Grover S, Aneja J, Singh A, Singla N. Use of electroconvulsive therapy in the presence of Arachnoid cyst: a case report review of existing literature. J ECT. (2013) 29:e38–9. doi: 10.1097/YCT.0b013e31828b3546
37. McKinney PA, Beale MD, Kellner CH. Electroconvulsive therapy in a patient with a cerebellar meningioma. J ECT. (1998) 14:49–52. doi: 10.1097/00124509-199803000-00008
38. Carter C. Neurological considerations with ECT. Convuls Ther Bull Tardive Dyskinesia Notes. (1977) 2:16–9.
39. Figiel GS, Coffey CE, Djang WT, Hoffman G, Doraiswamy PM. Brain magnetic resonance imaging findings in ECT-induced delirium. J Neuropsychiatr Clin Neurosci. (1990) 253–8. doi: 10.1176/jnp.2.1.53
40. Figiel GS, Coffey CE, Weiner RD. Brain magnetic resonance imaging in elderly depressed patients receiving electroconvulsive therapy. Convuls Ther. (1989) 5:26–34.
Keywords: ECT, brain tumor, abnormal recovery, ECT safety, ECT and cancer
Citation: Buday J, Albrecht J, Mareš T, Podgorná G, Horáčková K, Kališová L, Raboch J and Anders M (2020) Brain Tumors and Electroconvulsive Therapy: A Literature Overview of the Last 80 Years. Front. Neurol. 11:723. doi: 10.3389/fneur.2020.00723
Received: 22 April 2020; Accepted: 15 June 2020;
Published: 31 July 2020.
Edited by:
Jose Ramon Pineda, University of the Basque Country, SpainReviewed by:
Shih-Cheng Liao, National Taiwan University Hospital, TaiwanCopyright © 2020 Buday, Albrecht, Mareš, Podgorná, Horáčková, Kališová, Raboch and Anders. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jozef Buday, am96ZWYuYnVkYXlAdmZuLmN6
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.