 Annabelle Vaughan
Annabelle Vaughan Danielle Gardner1
Danielle Gardner1- 1Speech Pathology Service, Gold Coast University Hospital, Gold Coast, QLD, Australia
- 2School of Health and Rehabilitation Sciences, University of Queensland, Brisbane, QLD, Australia
- 3School of Allied Health Sciences, Griffith University, Gold Coast, QLD, Australia
- 4Speech Science, The University of Auckland, Auckland, New Zealand
- 5School of Health Sciences, Discipline of Physiotherapy, The University of Sydney, Camperdown, NSW, Australia
Background: Facial palsy is a frequent and debilitating sequela of stroke and brain injury, causing functional and aesthetic deficits as well as significant adverse effects on quality of life and well-being. Current literature reports many cases of acquired facial palsy that do not recover spontaneously, and more information is needed regarding the efficacy of physical therapies used in this population.
Methods: A systematic search of eight electronic databases was performed from database inception to December 2018. Gray literature searches were then performed to identify additional articles. Studies were included if they addressed physical rehabilitation interventions for adults with acquired facial palsy. Reasons for exclusion were documented. Independent data extraction, quality assessment, and risk of bias assessment followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Results: Following abstract screening, a total of 13 full-text articles were identified for independent screening by two reviewers. This included four randomized control trials, two non-randomized control trials, one cohort study, and six prospective case series studies. Twelve out of the 13 included studies reported on facial palsy as a sequela of stroke. A total of 539 participants received intervention for facial palsy across the 13 included studies. Therapy design, length and frequency of intervention varied across the studies, and a wide range of outcome measures were used. Improvement on various outcome measures was reported across all 13 studies. The quality of the evidence was low overall, and most studies were found to have high risk of bias.
Conclusions: All the studies in this review report improvement of facial movement or function following application of various methods of physical rehabilitation for facial palsy. Methodological limitations and heterogeneity of design affect the strength of the evidence and prevent reliable comparison between intervention methods. Strong evidence supporting physical rehabilitation was not found; well-designed rigorous research is required.
Introduction
The facial nerve (CNVII) plays a critical role in multiple complex functions of human life including mastication, speech, and successful social communication through expression of mood and emotion (1–4). Central facial palsy (CFP) results from damage to the central segment of this nerve (facial nucleus in the pons, motor cortex, or connections between the two) (5) and manifests typically as a unilateral impairment of movement opposite to the side of the injury, with predominance in the lower face (6). In contrast, peripheral facial palsy (PFP) results from injury or damage to extratemporal segments of the facial nerve (7), for example in idiopathic “Bell's” palsy, surgery such as mastoidectomy, or inflammation such as herpes zoster (Ramsay Hunt syndrome) (8).
CFP is a frequent initial symptom in patients after stroke and other neurological injury. A study conducted by Cattaneo and Pavesi (9) found that 60% of patients with first-time ischemic cortical stroke (MCA and ACA territories) presented with CFP. Other studies of stroke populations have reported a prevalence of approximately 45% (6). It is evident from multiple searches of libraries and online evidence repositories during clinical management of CFP that most of the available literature relates to rehabilitation of peripheral facial palsy (PFP), and there is very little evidence available to guide therapists working with people suffering from CFP. Whilst systematic reviews have evaluated physical rehabilitation and other management for PFP (10–12), the different etiopathogenesis of CFP suggests that rehabilitation approaches should be specifically modified for this group (13).
Spontaneous recovery of CFP has been reported in two-thirds of people at 6 months post-stroke, with approximately one-third of patients after stroke continue to present with persisting facial palsy after 6 months (14). More recently, differing opinions are emerging in the literature regarding rates of spontaneous resolution of CFP (including associated functional and QOL deficits), with some authors noting that in the absence of rehabilitation, symptoms seem unlikely to improve (15). In their study, Volk et al. (6) reported that a high percentage of patients continued to present with CFP 3 weeks post-onset, and over 60% of these patients were discharged from sub-acute rehabilitation with deficits persisting for more than 41 days post-stroke. As the available literature suggests that CFP can persist past the initial acute phase of stroke and not resolve spontaneously, people with CFP may benefit from access to a specific rehabilitation program aimed at maximizing recovery of facial movement and function (6, 13, 16).
Facial palsy can be distressing and debilitating for those affected, causing both functional and aesthetic deficits (16). Functional deficits may be characterized by facial asymmetry and weakness of the lower half of the face, drooping of the corner of the mouth, dribbling from the corner of the mouth at rest or during oral intake, reduced masticatory force and efficiency, asymmetrical smile and dysarthria (slurring or reduced clarity of speech) (15). It is well-recognized in the literature that in addition to functional deficits, facial palsy has a negative effect on quality of life (QOL) and emotional well-being (7, 17–21). In their 2016 study comparing QOL between individuals with pure CFP post stroke vs. pure dysarthria, Chang et al. (21) found that the CFP group had significantly worse scores on QOL and depression scales. Interestingly, it has been found that the presence of facial palsy alone regardless of its severity has a detrimental effect on the psychological well-being of those who experience it (19).
Rationale
Currently, there is minimal evidence available to guide clinical decision-making in the rehabilitation of CFP (22, 23) and very little information available regarding the effectiveness of popular intervention techniques (21, 23). As mentioned above, CFP may not resolve spontaneously and the negative impacts of CFP on people who experience this disorder can be wide-ranging. Rehabilitation may maximize functional recovery and improve the quality of life and psychological well-being of people with CFP (6, 13, 16) however there is currently no comprehensive or systematic review of the literature specific to this disorder to inform therapy planning and provision. This has significant implications for patient management, as it is still not clear to health professionals whether physical rehabilitation techniques work, or which technique is most effective.
Objective
The purpose of this review is to identify and examine the available literature specifically relating to physical rehabilitation of CFP. This review aims to (1) identify the types of physical rehabilitation methods used in remediation of CFP, (2) review the effectiveness of various methods of physical rehabilitation, and (3) review the methodological quality of the studies retrieved. The findings will be pertinent to clinicians working with patients with CFP as this is the only review that the authors are aware of that systematically evaluates the evidence base for rehabilitation of this disorder.
Research Question
What is the effectiveness of physical rehabilitation for acquired central facial palsy in adults?
Methods
Study Design and Search Strategy
This review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The review protocol is registered on PROSPERO (CRD42018115303). A systematic search strategy was devised in conjunction with a senior librarian, using the core concepts of facial paralysis, central nervous system disease, and physical rehabilitation. The Medical Subject Headings (MeSH) database was used to obtain terms that were related to these concepts to ensure a comprehensive search of the literature was performed. The search strategy was designed and performed using Medline (Ovid) terminology (see Appendix 1). No limitations were used for year published, language, or publication type. The search strategy was then translated for searching the following databases: Embase (Elsevier), CINAHL (Ebsco), Cochrane Central Register of Controlled Trials, Proquest Dissertations and Theses Global, PEDro, Speechbite, and Web of Science (Clarivate).
Gray literature searches included searches of WHO ICTRP (3) and ANZCTR (0) using the terms central facial pa*, with no completed studies (3 currently registered trials) retrieved. ClinicalTrials.gov was searched using the heading facial palsy with 18 completed studies retrieved, however all retrieved studies either pertained to peripheral facial palsy or did not have results available and were therefore not included in this review. Clinical practice guidelines and best practice statements were searched for relevant literature/references, including Clinical Guidelines for Stroke Management 2017 (24), United Kingdom National Clinical Guideline for Stroke (25), and American Speech and Hearing Association Evidence Maps (https://www.asha.org/MapLanding.aspx?id=8589947062).
Further hand-searching of library and clinical databases were conducted. Specialists from facial therapy services in Australia and internationally were asked to provide any relevant literature which informs their current clinical practice. The reference lists of articles eligible for inclusion following full text screening were searched, and any titles that appeared to fit the criteria set were retrieved.
Participants, Interventions, Comparators
The inclusion and exclusion criteria for the review are presented in Table 1.
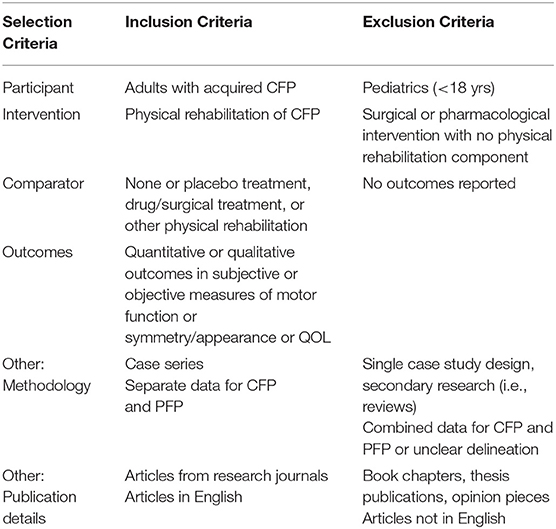
Table 1. Selection criteria.
Systematic Review Protocol
The systematic search strategy is presented in Figure 1. A senior health service librarian performed database searching. Articles retrieved in the database searches were deduplicated using the Bond University CREB SRA deduplicating tool (http://crebp-sra.com) and then further screened to remove other duplicates. Abstracts of all articles remaining following deduplication were then collated into an Endnote library, which was then uploaded to Covidence (Veritas Health Innovation Ltd, Melbourne, Australia) for blind review by two independent reviewers (AV and DG). Titles and abstracts were screened against the predetermined inclusion/exclusion criteria and subsequently added to full text screening lists. Articles included by both independent reviewers and articles that were marked as “maybe” by one or both reviewers were considered eligible for further review. Full texts of eligible studies were then retrieved and independently assessed for inclusion/exclusion. Any conflicts that arose during eligibility assessment were resolved by (a) discussion between reviewers, or where agreement could not be reached, by (b) discussion with the review team and relevant experts in the field.
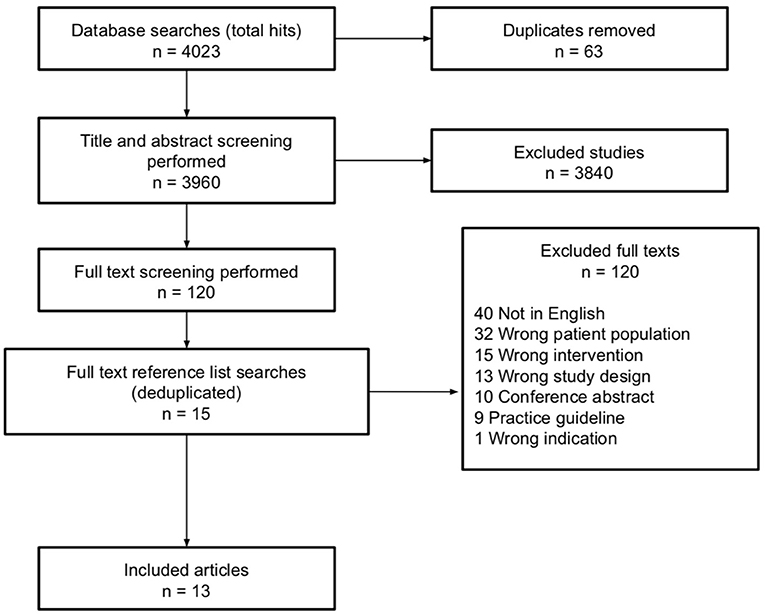
Figure 1. Preferred reporting items systematic reviews and meta-analyses (PRISMA) flow diagram detailing search strategy and selection criteria.
Data Extraction
For all included articles, a range of variables including study population/participant details, selection criteria, methodology, interventions (therapy approach, intensity, follow-up) and outcomes were extracted and are presented in a descriptive summary in Table 2. These variables were identified as most relevant to our clinical question. Data extraction was performed initially by the second author (DG), and then amended and expanded where necessary by the first author (AV) using Google Sheets (Google, CA, USA). Due to heterogeneity in the included studies a meta-analysis was not able to be performed.
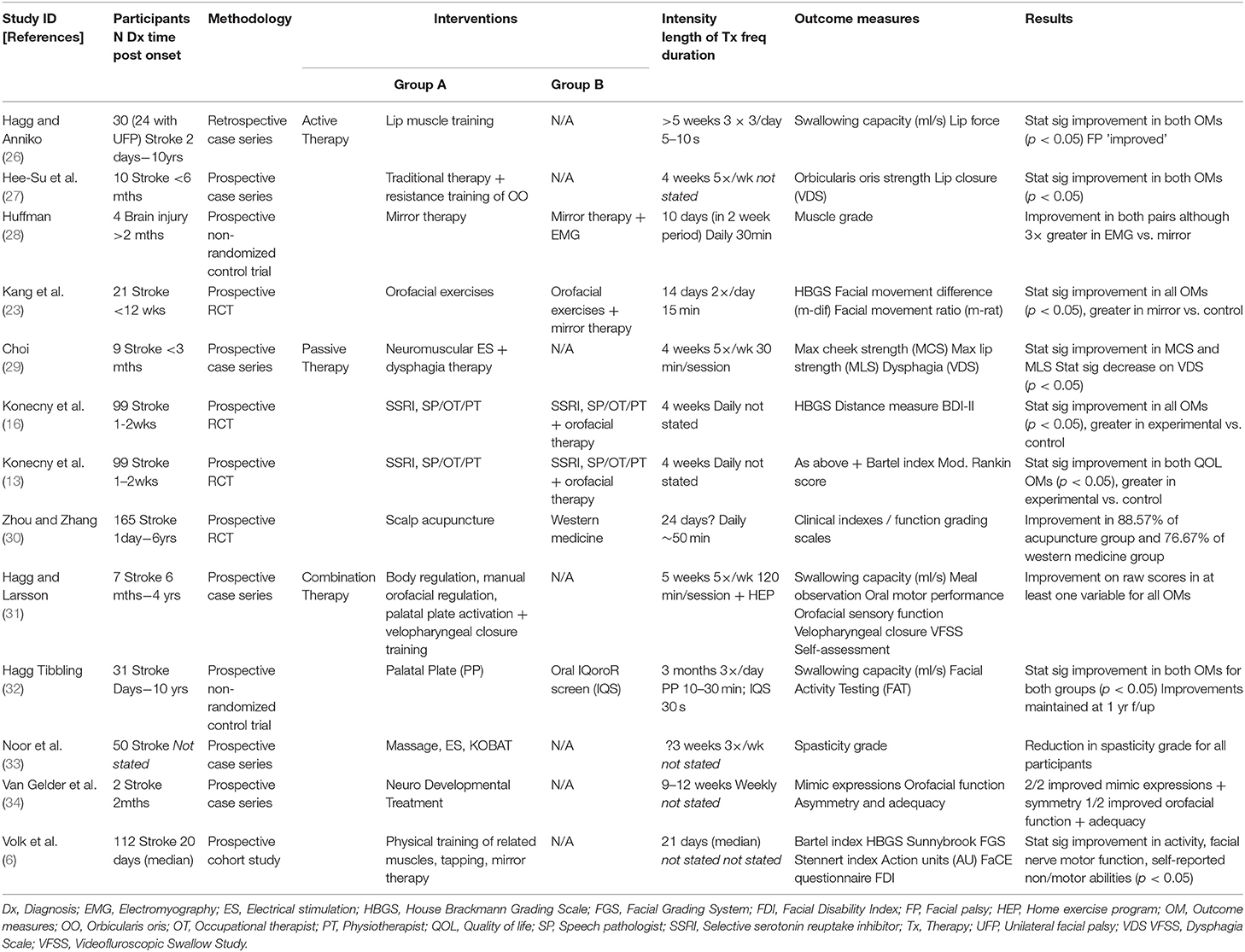
Table 2. Extracted data.
Quality Assessment
Risk of bias was assessed using tools appropriate to the study methodology determined during the data extraction process: case series reports were assessed using the JBI Critical Appraisal Checklist for Case Series (35), cohort studies were assessed using the JBI Critical Appraisal Checklist for Cohort Studies (35), and control trials were assessed using the Physiotherapy Evidence Database—Psychbite scale (PEDro-P) (36). No mixed-method studies were identified during the search, therefore the tools used to assess risk of bias were altered from the original PROSPERO protocol to be more appropriate to the various study designs retrieved (control trials, case series, cohort study). Risk of bias analyses were performed independently by two reviewers (AV and RW) and discrepancies were discussed by the two authors until consensus was achieved.
Data Analysis
Meta-analysis of the results was not indicated due to the clinical diversity of the studies retrieved, as recommended by the Cochrane Handbook for Systematic Reviews of Interventions (37). Each of the studies retrieved described differing experimental designs, treatment protocols, and methods of outcome measurement, and there was inadequate reporting of data and statistics necessary for appropriate and meaningful meta-analysis. Types of physical rehabilitation used in CFP have been broadly grouped as having used either an active approach (recipients actively move their own muscles or structures to perform exercises or volitional muscle movements), passive approach (movement is facilitated by external force, person or device e.g., massage/stretching, acupuncture, electrical stimulation), or a combination of the two. The effectiveness of physical rehabilitation has been determined by the examination of the reported results in those studies that provided sufficient data and is discussed in the context of the various grouped approaches. Rating of the overall quality of the evidence has been performed by applying relevant sections of the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) approach to individual studies (38).
Results
Study Selection
The results from database searching and selection processes are shown in Figure 1.
Study Characteristics
Six case series (total no. of subjects = 108) one cohort study (total no. of subjects = 112), and six control trials (total no. of subjects = 133) were identified. Methodological details are outlined in Table 2. Of the four RCTs, two appeared to use identical participant populations and outcome data and are subsequently discussed as one study in parts of this review (n = 99 (13, 16). All the included studies used a pre-test post-test design.
Participant Demographics
Participant demographics for all included studies are reported in Table 2. Twelve out of the 13 included studies reported on facial palsy as a sequela of stroke, and one study reported facial palsy secondary to acquired brain injury. A total of 539 participants received intervention for facial palsy in the 13 studies included in this review (age range 48–88 yr old). There was a large range in time post-onset of facial palsy from acute (e.g., “days”) to chronic (e.g., 6–10 years) stages of recovery.
Types of Physical Rehabilitation for Facial Palsy
There was a high degree of heterogeneity in physical rehabilitation methods described for adults with CFP. Seven studies reported interventions aimed at remediation of facial palsy as their primary objective (6, 26–29, 31, 33), and six reported targeting lip function or movement in the context of post-stroke dysphagia therapy (13, 16, 23, 30, 32, 34). Four studies reported on active intervention methods for remediation of oromotor function or facial palsy (23, 26–28); two used muscle strengthening exercises alone (26, 27) and the other two used biofeedback (via mirror or device) while performing orofacial exercises (23, 28). Four studies reported on passive intervention techniques such as massage, stretching or electrical stimulation for the remediation of facial muscle strength or facial palsy (13, 16, 29, 30). Acupuncture is classified in this review as passive rehabilitation; one study (30) reported on the use of scalp acupuncture compared to a group that received “western medicine.” Five studies combined active and passive approaches in the rehabilitation of CFP (6, 31–34); therapy varied across these studies but all included elements of active exercise, massage, stretching or passive manipulation, or application of various devices (Table 2).
Dosage
Length and frequency of therapy varied across the studies, with participants receiving multiple therapy sessions per week for between 10 days and 9 weeks. Details relating to intensity of therapy (length, frequency, and duration of intervention) are presented in Table 2.
Outcome Measures
A wide range of outcome measures for muscle strength and facial movements were used including measures of muscle strength, facial movement, and symmetry; details are outlined in Table 2. No validated outcome measurement tools were used. The majority of studies did not provide detailed descriptions of grading scales; only three studies (6, 13, 16, 23) used well-known outcome measures specific to facial palsy. Facial palsy was often measured in conjunction with other deficits of speech, swallowing, emotional and psychological well-being.
Effectiveness of Physical Rehabilitation of Facial Palsy
Four RCTs and nine observational studies reported improvements in various measures of facial palsy or facial motor function, which are outlined below in the context of the rehabilitation approach used (active, passive or combination). Eight of the 13 studies included comments about the statistical significance of the results (p-values), however none performed calculations of effect size, and therefore none of the studies provided sufficient data to assess imprecision or inconsistency as outlined in the GRADE approach. There were also insufficient data reported to facilitate judgement of indirectness; the nine observational studies do not undertake comparison with an alternative therapy or control group, and none of the RCTs provided calculations of risk ratio or effect size that would enable meaningful direct comparison.
Active Therapy
Four studies reported on active therapy methods; one RCT (23), one nRCT (28), and two case series' (26, 27). All four studies reported improvements in treatment variables measured. Kang et al. (23) reported improvement in HBGS scores and functional measures (facial movement ratios) in both the control group and the experimental group (both groups performed the exercise protocol with the experimental group receiving mirror feedback as the experimental condition). Huffman (28) also reported improvement in all subjects on an unvalidated ‘muscle grade' rating scale mentioned but not detailed by the authors; as well as improvements three times greater for the subjects receiving EMG feedback compared to mirror feedback. Both the case series' implemented protocols of lip strengthening using instrument-based exercise. Hee-su et al. (27) reported improvements in orbicularis oris muscle strength and lip closure function during swallowing; no outcomes specific to facial palsy (e.g., measures of movement or symmetry) were used. Hagg and Anniko (26) also reported improvement in raw scores of lip force from baseline measures taken using a Lip Force Meter instrument however did not specifically report on outcomes for facial palsy.
Passive Therapy
Four studies reported on passive therapy methods, including a case series study (29) and three RCTs (13, 16, 30); two RCTs are discussed together (13, 16) for reasons mentioned previously. All four reported improvements in relevant measures. Choi (29) reported changes in facial muscle strength compared to baseline measures however did not explicitly report outcomes for facial palsy. Zhou and Zhang (30) reported a larger change in all outcome measures (including a facial movement grading scale not described in the study) for the group receiving acupuncture compared to those receiving “western medicine.” There was no detail provided regarding the method for administration of this grading scale. Konecny et al. (13, 16) reported improvements in formal facial nerve assessment measures (HBGS) as well as in a variety of other functional and quality-of-life scales.
Combination Therapy
Five studies reported on therapy protocols that combined passive and active methods (e.g., massage/manipulation with active exercise regime). These included three case series' (31, 33, 34), one non-randomized control trial (32) and one cohort study (6). One case series (33) reported improvements in spasticity of facial muscles; this was demonstrated by reporting the number of participants per scoring level (grade I–V) pre and post treatment on an unnamed grading tool. There were no individual assessment outcomes reported and there was an absence of statistical analysis of the data. One (31) reported improvements in raw scores of orofacial motility on an informal four-point scale as well as improvement in mean severity score of oral motor performance. The authors provided raw pre and post assessment data for each participant as rated by multiple assessors; there was an absence of further analysis of this data and overall outcomes were focused on dysphagia rather than facial palsy. The case series reported by Volk (6) reported improvements in three well-known tools to assess facial palsy [HBGS (39), Sunnybrook Grading Scale (40), and Stennert Index (41)], two validated quality of life instruments [FaCE Questionnaire (42) and FDI (43)], and a system of automated facial movement analysis described in the study.
Maintenance of Therapeutic Effects
Eleven of the 13 included studies did not report any follow up assessment, and therefore no evaluation of the maintenance of therapeutic effects was available. One study (32) reported maintenance of improved facial activity at follow-up assessment at least 1 year post treatment in both groups. Van Gelder et al. (34) reported on follow-up assessment 9 weeks post treatment in only one of the two participants. Their results showed a decline in function between completion of treatment and re-assessment, which the authors interpreted as showing treatment effects were not maintained.
Methodological Quality and Risk of Bias
A summary of the consensus ratings for methodological assessment is shown using modified harvest plots, which have been used previously in systematic reviews to present data that is not able to be graphed using traditional methods (44, 45). These modified harvest plots were created by grouping similar criteria together for each appraisal tool, as detailed in Table 3. As in previous studies where modified harvest plots have been used, methodological quality is represented by bar height (45). “Unclear” consensus ratings have been scored as zero when calculating scores for each criterion on the JBI tools.
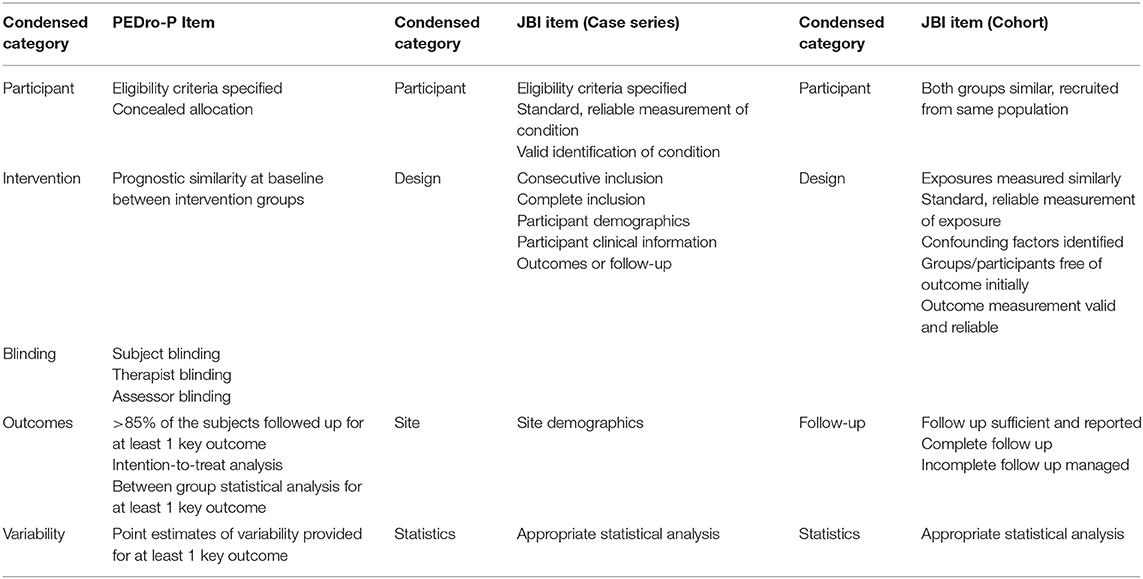
Table 3. PEDro-P and JBI ratings.
Control Trials
Across the control trials, scores on the PEDRO-P ranged from 3 to 9 with an average of 5.5 out of 11 (see Figure 2). Of the RCTs, 2 of the 4 specified eligibility criteria for inclusion in the study, and while the majority allocated subjects randomly to interventions only one concealed this allocation. Blinding was an area of significant risk across the RCTs, with 1 of 4 studies blinding subjects and assessors and no blinding of therapists in any study. The nRCTs showed similar shortcomings in allocation and blinding items. The intervention groups were similar at baseline regarding the most important prognostic indicators in >90% of the studies. Outcome measurement was an area of strength for all the control studies; 100% obtained measures of at least one key outcome from >85% of subjects and demonstrated that all subjects for whom outcome measures were available received the treatment or control condition. Overall the quality of the control trials is low due to the significant limitations present in the majority of studies.
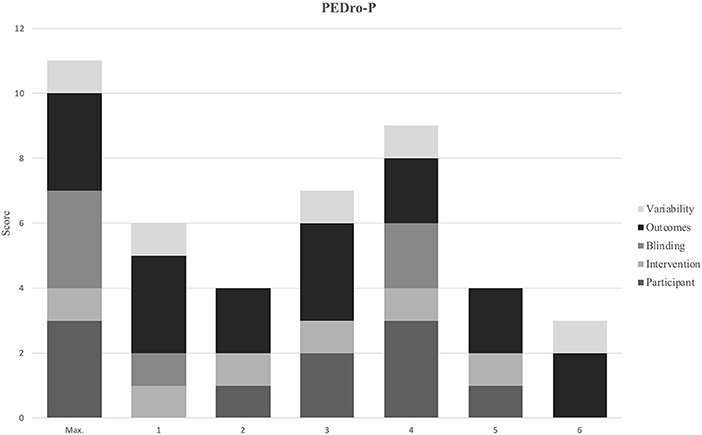
Figure 2. Study identification number: 1. (32) 2. (28) 3. (23) 4. (16) 5. (13) 6. (30) Max. indicates the highest possible score that an article could receive in each category.
Case Series and Cohort Study
Scores on the JBI tool for case series evaluation ranged from 2 to 7 with an average of 3.8 out of 10 (see Figure 3). Four (27, 29, 33, 34) of the six case studies were judged to be at high risk of bias; 2 of the 6 of studies failed to outline clear criteria, only 30% used valid methods for identification of the condition, >80% did not report consecutive recruitment of subjects and failed to clearly report clinical information of the participants. Two case studies were judged to have an unclear risk of bias (26, 31); strengths of both these studies were found in reliable condition measurement and clear reporting of participant demographics. Limitations of the case series' judged as “unclear risk of bias” were varied—in one (31) it was not clear if the study included consecutive and complete inclusion and methods of statistical analysis were ambiguous; in the other (26) criteria were not clearly defined and it was not possible to determine if valid methods for identification of the condition were used.
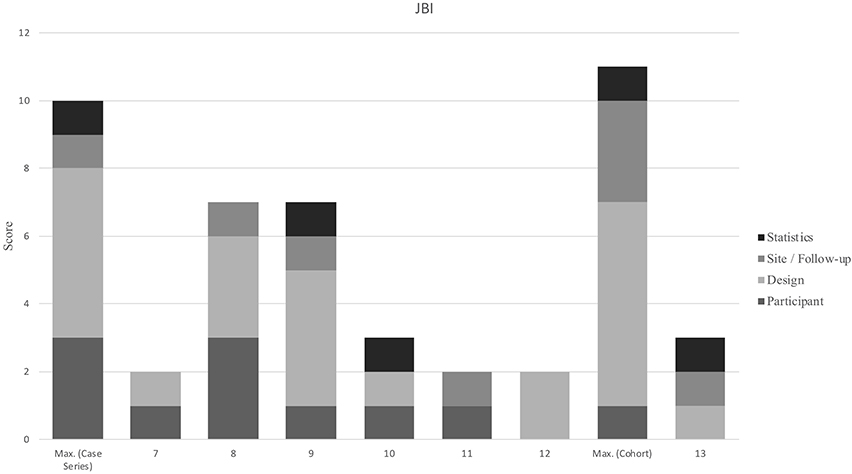
Figure 3. Study identification number: 7. (29) 8. (28) 9. (26) 10. (27) 11. (33) 12. (34) 13. (6) Max. indicates the highest possible score that an article could receive in each category.
Discussion
This review has shown that despite trends demonstrating improvement in CFP following various types of physical rehabilitation, there is a lack of high-quality evidence currently available to inform clinical practice. Many questions remain for clinicians planning and providing therapy for this population. Literature is emerging which recognizes CFP as an impairment in its own right (separate to its impact on speech or swallowing function), and therapies specifically targeting this disorder are being investigated with increasing frequency. All the studies in this review report improvement on various parameters of facial movement or function and, although lacking in rigor, indicate potential benefit from using physical rehabilitation approaches.
Effectiveness of Therapy
Improvement in facial muscle strength or movement was reported across all 13 studies, and positive changes in other outcome measures such as swallow function and quality of life were also shown (where measured). Only one study provided data for maintained effects of therapy at >1 year post intervention (32), and while this study had comparative strengths in methodology, its lack of overall rigor reduced the strength of the data. All 13 studies reported statistically significant improvements from baseline measures, however none performed calculations of optimal sample size or treatment effect measures. It is therefore unclear if the improvements reported can be attributed to the physical therapy provided or if other variables influenced the outcomes. Overall, the studies included in this review provide insufficient evidence to draw strong conclusions regarding the effectiveness of physical rehabilitation for CFP.
Comparison of the effectiveness of differing therapy approaches remains unclear following this review. Of the four studies that were found to be the most methodologically sound (as per risk of bias assessments), two provided active therapy (one involved strengthening exercises only) (23, 26), one provided passive therapy (16), and one described a combination of these two approaches (32). Active and passive approaches were explored by only a small number of methodologically weak RCTs, and there were no RCT designs that investigated a combination of approaches. As well as insufficient reporting of treatment effect size or precision, there was a large amount of variation in all aspects of the design of the studies—each study described different participant variables (e.g., time post onset), dosage and treatment duration. These factors restrict any meaningful comparison being made between outcomes, which leads to a lack of support for one method of rehabilitation over another.
This review highlights the need for further well-designed and rigorous research to examine the efficacy of physical rehabilitation of CFP. The trend of improvement across various outcome measures reported in all studies provides some indication that physical therapy may be of benefit, however overall there were significant limitations that impact on confident application of these findings to current clinical practice. These include a lack of comprehensive reporting and analysis of data in all studies, and methodological limitations (e.g., lack of RCT designs, lack of concealed allocation, minimal use of blinding, and lack of follow-up assessment). The majority of studies also failed to use standardized, reliable outcome measurements, which creates questions about the validity of findings and makes any comparison of outcomes difficult. Future studies should aim for more rigor in their design, for example by using RCTs to minimize risk of bias and strengthen the validity of findings and including follow-up assessment to measure maintenance of therapeutic effect.
Assessment
A major challenge for evaluation of methods of physical rehabilitation of CFP is the heterogeneity of assessment tools (and subsequently outcome measures) described. Only four of the 13 included studies utilized any standardized method of assessing facial palsy (6, 13, 16, 23, 32) and only three of these used widely-accepted quantitative outcome measures (6, 13, 16, 23). The remainder of the studies described a variety of informal clinical measures of muscle strength or facial movement and function. As such, comparison of findings between the studies in an effort to establish which methods were more effective is not able to be reliably performed.
Clinical Implications
Positive trends in favor of physical rehabilitation were found. All the studies retrieved by this review process do appear to show improvements in facial palsy with rehabilitation, which lends support to the rationale for continuation of therapy provision as well as ongoing research. The strength of the evidence is low overall, which should be considered when planning intervention for this population.
Future Directions
Future studies should aim to use objective and standardized assessment tools. Objective assessment of facial palsy is notoriously difficult (42, 46). Due to the lack of published, validated assessment tools available specific to CFP, further validation of tools designed for broader use (including peripheral types of facial palsy) may be indicated. Literature specific to PFP recommends use of the Sunnybrook Facial Grading System (40), and the House-Brackmann Grading Scale (39), and these tools have been used with some effectiveness to measure CFP in studies by Volk et al. (6), Kang et al. (23), and Konecny et al. (13, 16). There are limitations in both tools including subjective ordinal grading systems with limited items (47, 48). The Electronic Facial Paralysis Assessment (eFACE) was developed to provide clinicians with a tool that “has greater sensitivity and objectivity when assessing incomplete paralysis and post-interventional improvement…in cases of both acute peripheral nerve palsy and recovery” (49). This tool has been found to have high test-retest reliability (50), have high validity and reliability (49), and had positive feedback from a panel of international facial nerve experts (51). The tool needs further validation in a CFP population. In addition to measuring facial function, the inclusion of reliable outcome measures that evaluate the emotional and psychological impact of CFP would enable a broader assessment of the holistic impacts of rehabilitation. Two examples of validated patient-graded tools that are referenced in current CFP literature are the Facial Clinometric Evaluation (FaCE Scale) (42) and the Facial Disability Index (FDI) (43). Studies of CFP should include use of one of these tools, as non-motor impacts of facial palsy have been shown to be as important as motor function to people with this impairment (52).
It would be beneficial to have a comprehensive picture of current clinical practice to incorporate into future studies. Clinical physiotherapists and speech pathologists provide rehabilitation for CFP for using principles derived from peripheral nerve damage literature due to the lack of studies specific to CFP, despite these therapies also having low quality supporting evidence (12) and varying significantly in mechanism of impairment. A comprehensive survey of current practice would enable “expert opinion” to be integrated into the development of a gold standard of evidence-based physical rehabilitation, along with stronger evidence from well-designed clinical trials.
Exercise-based physical rehabilitation for facial palsy must be performed in a controlled and precise manner, and repeated sufficient times to induce long-term synaptic change (53). These exercises are often performed using some method of biofeedback (e.g., mirror); primarily relying on the visual system to obtain accurate proprioceptive information about position of facial muscles during slow, controlled movements that focus on symmetry (54). Without some form of external proprioceptive feedback, it is extremely difficult for patients to precisely and effectively judge and monitor the movements of facial structures (54). Exercise protocols can therefore be difficult for people to perform accurately if they have concomitant visual-perceptual, cognitive or behavioral changes secondary to stroke. Well-designed research which evaluates the effectiveness of interventions which are accessible to a wider clinical population would be of great benefit to people suffering from central facial palsy whose other impairments prevent them from engaging in strict exercise-based protocols. Regardless of the intervention strategy employed, clear and detailed reporting should be ensured to enable replicable therapeutic protocols.
Further investigation of physical rehabilitation methods for CFP is required to determine effective types and approaches for therapy and to guide clinical decision-making. There is a gap in services currently available for people wishing to access therapy for CFP and is not possible to base a strong case for clinical input on the current literature, even though trends have been identified that indicate potential benefit of physical rehabilitation.
Limitations
Although every effort was made to ensure database and other searches were comprehensive it is possible that some records were not retrieved via the search methods. Due to the difficulties and cost associated with obtaining verified and reliable document translation, this review was unable to include articles where the full text was not available in English. This may have resulted in some studies being missed; the authors are aware of at least one non-English study (14) which may have contributed toward this review. Our systematic review also had limitations relating to methodological quality and available data in the existing literature; only four RCTs were retrieved, which were of low quality, and the observational studies all lacked sufficient data to draw strong conclusions or perform calculation of treatment effect size. It is recognized that in many areas of health care, some interventions are supported by evidence from RCTs and others are not (55). It is also acknowledged in medical research literature that decision-making is often necessary even when there is imperfect evidence (56). As clinicians who provide assessment and therapy to patients with central facial palsy, we included the smaller observational studies due to a lack of larger or more well-designed trials—as per Balshem et al. “in the absence of high-quality evidence, clinicians must look to lower quality evidence to guide their decisions” (57). While we are aware that the limitations in methodology affect the reliability of these studies, and thus also affect the strength of recommendations that can be drawn from their findings, the reality is that there are not enough large well-designed RCTs available to rely solely on this level of evidence for clinical decision-making and intervention.
Conclusions
The studies in this review report improvement of facial movement or function following application of various methods of physical rehabilitation for CFP. Methodological limitations and heterogeneity of design affect the strength of the evidence and prevent reliable comparison between intervention methods. Strong conclusions regarding the effectiveness of intervention cannot be drawn using the studies identified by this review as good quality, robust evidence supporting physical rehabilitation of central facial palsy was not found.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Author Contributions
AV and DG conceived the idea for this review. AV, DG, RW, AM, and SC formulated the question for review and designed the search strategy. AV and DG performed the abstract screening, full text review, and extracted data from included studies. AV and RW performed the risk of bias assessments. AV analyzed and interpreted the data and drafted the manuscript. AC and AM provided overall supervision of the project and final approval of the version to be published. All authors provided critical feedback and helped shape the research, analysis, and manuscript.
Funding
This study was undertaken with support from a Gold Coast Health Allied Health Clinical Backfill for Research grant, which provided AV and DG with four weeks of funded offline time. Assistance with funding open-access publication was granted via the Gold Coast Health Study, Education and Research Trust.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The review team thanks Sarah Thorning for her valuable assistance with database searching and deduplication of search results. We also thank the Speech Pathology and Audiology Service (Allied Health Services|Gold Coast Health).
References
1. Takezawa K, Townsend G, Ghabriel M. The facial nerve: anatomy and associated disorders for oral health professionals. Odontology. (2018) 106:103–16. doi: 10.1007/s10266-017-0330-5
2. Perry ES, Potter NL, Rambo KD, Short R. Effects of strength training on neuromuscular facial rehabilitation. Dev Neurorehabil. (2011) 14:164–70. doi: 10.3109/17518423.2011.566595
3. Owusu JA, Boahene KD. Management of long-standing flaccid facial palsy: midface/smile: locoregional muscle transfer. Otolaryngol Clin North Am. (2018) 51:1119–28. doi: 10.1016/j.otc.2018.07.008
4. Krippl M, Karim AA, Brechmann A. Neuronal correlates of voluntary facial movements. Front Hum Neurosci. (2015) 9:598. doi: 10.3389/fnhum.2015.00598
5. Adour KK. Current concepts in neurology: diagnosis and management of facial paralysis. N Eng J Med. (1982) 307:348–51. doi: 10.1056/NEJM198208053070605
6. Volk G, Steinerstauch A, Lorenz A, Modersohn L, Mothes O, Denzler J, et al. Facial motor and non-motor disabilities in patients with central facial paresis: a prospective cohort study. J Neurol. (2019) 266:46–56. doi: 10.1007/s00415-018-9099-x
7. Wax MK. Facial Paralysis: A Comprehensive Rehabilitative Approach. San Diego, CA: ProQuest, Plural Publishing Inc. (2015).
8. Roob G, Fazekas F, Hartung HP. Peripheral facial palsy: etiology. diagnosis and treatment. Eur Neurol. (1999) 41:3–9. doi: 10.1159/000007990
9. Cattaneo L, Pavesi G. The facial motor system. Neurosci Biobehav Rev. (2014) 38:135–59. doi: 10.1016/j.neubiorev.2013.11.002
10. Pereira LM, Obara K, Dias JM, Menacho MO, Lavado EL, Cardoso JR. Facial exercise therapy for facial palsy: systematic review and meta-analysis. Clin Rehabil. (2011) 25:649–58. doi: 10.1177/0269215510395634
11. Cardoso JR, Teixeira EC, Moreira MD, Fávero FM, Fontes SV, Bulle De Oliveira AS. Effects of exercises on Bell's Palsy: systematic review of randomized controlled trials. Otol Neurotol. (2008) 29:557–60. doi: 10.1097/MAO.0b013e31816c7bf1
12. Teixeira L, Soares B, Vieira VP, Prado G. Physical therapy for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. (2008) D006283. doi: 10.1002/14651858.CD006283.pub2
13. Konecny P, Elfmark M, Horak S, Pastucha D, Krobot A, Urbanek K, et al. Central facial paresis and its impact on mimicry, psyche and quality of life in patients after stroke. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. (2014) 158:133–7. doi: 10.5507/bp.2013.014
14. Svensson BH, Christiansen LS, Jepsen E. [Treatment of central facial nerve paralysis with electromyography biofeedback and taping of cheek. A controlled clinical trial]. Ugeskrift Laeger. (1992) 154:3593–6.
15. Schimmel M, Ono T, Lam OL, Muller F. Oro-facial impairment in stroke patients. J Oral Rehabil. (2017) 44:313–26. doi: 10.1111/joor.12486
16. Konecny P, Elfmark M, Urbanek K. Facial paresis after stroke and its impact on patients' facial movement and mental status. J Rehabil Med. (2011) 43:73–5. doi: 10.2340/16501977-0645
17. Ho AL, Scott AM, Klassen AF, Cano SJ, Pusic AL, Van Laeken N. Measuring quality of life and patient satisfaction in facial paralysis patients: a systematic review of patient-reported outcome measures. Plast Reconstr Surg. (2012) 130:91–9. doi: 10.1097/PRS.0b013e318254b08d
18. Ishii LE, Nellis JC, Boahene KD, Byrne P, Ishii M. The importance and psychology of facial expression. Otolaryngol Clin North Am. (2018) 51:1011–17. doi: 10.1016/j.otc.2018.07.001
19. Walker DT, Hallam MJ, Ni Mhurchadha S, McCabe P, Nduka C. The psychosocial impact of facial palsy: our experience in one hundred and twenty six patients. Clin Otolaryngol. (2012) 37:474–7. doi: 10.1111/coa.12026
20. Dai R, Lam OL, Lo EC, Li LS, Wen Y, McGrath C. Orofacial functional impairments among patients following stroke: a systematic review. Oral Dis. (2015) 21:836–49. doi: 10.1111/odi.12274
21. Chang WH, Sohn MK, Lee J, Kim DY, Lee SG, Shin YI, et al. Impact of central facial palsy and dysarthria on quality of life in patients with stroke: the KOSCO study. Neurorehabilitation. (2016) 39:253–9. doi: 10.3233/NRE-161355
22. Morgan Stuart JR, Byrne JP. The importance of facial expression and the management of facial nerve injury. Neurosurg Q. (2004) 14:239–48. doi: 10.1097/00013414-200412000-00009
23. Kang JA, Chun MH, Choi SJ, Chang MC, Yi YG. Effects of mirror therapy using a tablet PC on central facial paresis in stroke patients. Ann Rehabil Med Arm. (2017) 41:724. doi: 10.5535/arm.2017.41.4.724
24. Stroke Foundation. Clinical Guidelines for Stroke Management. Melbourne, VIC: Stroke Foundation (2019).
25. Rudd AG, Bowen A, Young G, James MA. National Clinical Guideline for Stroke, 5th ed. (2016) London: Clinical Medicine. (2017).
26. Hagg M, Anniko M. Lip muscle training in stroke patients with dysphagia. Acta Otolaryngol. (2008) 128:1027–33. doi: 10.1080/00016480701813814
27. Hee-Su P, Park JY, Kwon YH, Choi Hee SU, Kim Hee J. Effect of orbicularis oris muscle training on muscle strength and lip closure function in patients with stroke and swallowing disorder. J Phys Ther Sci. (2018) 30:1355–6. doi: 10.1589/jpts.30.1355
28. Huffman AL. Biofeedback treatment of orofacial dysfunction: a preliminary study. Am J Occup Ther. (1978) 32:149–54.
29. Choi JB. Effect of neuromuscular electrical stimulation on facial muscle strength and oral function in stroke patients with facial palsy. J Phys Ther Sci. (2016) 28:2541–3. doi: 10.1589/jpts.28.2541
30. Zhou J, Zhang F. A research on scalp acupuncture for cerebral infarction. J Tradition Chin Med. (1997) 17:194–7.
31. Hägg M, Larsson B. Effects of motor and sensory stimulation in stroke patients with long-lasting dysphagia. Dysphagia. (2004) 19:219–30. doi: 10.1007/s00455-004-0016-3
32. Hagg M, Tibbling L. Effect of oral IQoro R and palatal plate training in post-stroke, four-quadrant facial dysfunction and dysphagia: a comparison study. Acta Otolaryngol. (2015) 135:962–8. doi: 10.3109/00016489.2015.1042043
33. Noor R, Ghazanaffar M, Neelam H, Bashir MS. Role of physiotherapy in rehabilitation of facial muscles in facial palsy due to hemorrhagic stroke. Rawal Med J. (2014) 39:389–91.
34. Van Gelder RS, Philippart SMM, Hopkins B. Treatment of facial paralysis of CNS-origin: initial studies. Int J Psychol. (1990) 25:213–28. doi: 10.1080/00207599008247858
35. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. Joanna Briggs Institute Reviewer's Manual. The Joanna Briggs Institute (2017). Available online at: https://reviewersmanual.joannabriggs.org/
36. Tate R, Perdices M, McDonald S, Togher L, Moseley A, Winders K, et al. Development of a database of rehabilitation therapies for the psychological consequences of acquired brain impairment. Neuropsychol Rehabil. (2004) 14:517–34. doi: 10.1080/09602010343000182
37. Higgins JPT. Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed. Hoboken, NJ: Wiley-Blackwell, Cochrane Collaboration (2019).
38. Meader N, King K, Llewellyn A, Norman G, Brown J, Rodgers M. A checklist designed to aid consistency and reproducibility of GRADE assessments: development and pilot validation. Syst Rev. (2014) 3:82. doi: 10.1186/2046-4053-3-82
39. House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. (1985) 93:146–7. doi: 10.1177/019459988509300202
40. Ross BR, Fradet G, Nedzelski JM. Development of a sensitive clinical facial grading system. Otolaryngol Head Neck Surg. (1994) 114:380–6.
41. Stennert E, Limberg CH, Frentrup KP. An index for paresis and defective healing–an easily applied method for objectively determining therapeutic results in facial paresis (author's transl). HNO. (1977) 25:238–45.
42. Kahn JB, Gliklich RE, Boyev KP, Stewart MG, Metson RB, McKenna MJ. Validation of a patient-graded instrument for facial nerve paralysis: the FaCE scale. Laryngoscope. (2001) 111:387–98. doi: 10.1097/00005537-200103000-00005
43. Vanswearingen JM, Brach JS. The Facial Disability Index: reliability and validity of a disability assessment instrument for disorders of the facial neuromuscular system. Phys Ther. (1996) 76:1288–98. doi: 10.1093/ptj/76.12.1288
44. Crowther M, Avenell A, Maclennan G, Mowatt G. A further use for the Harvest plot: a novel method for the presentation of data synthesis. Res Synth Methods. (2011) 2:79–83. doi: 10.1002/jrsm.37
45. Finch E, Copley A, Cornwell P, Kelly C. Systematic review of behavioral interventions targeting social communication difficulties after traumatic brain injury. Arch Phys Med Rehabil. (2016) 97:1352–65. doi: 10.1016/j.apmr.2015.11.005
46. Banks AC, Bhama KP, Park RJ, Hadlock AC, Hadlock AT. Clinician-graded electronic facial paralysis assessment: the eFACPlastic. Reconstruct Surg. (2015) 136:223e−30e. doi: 10.1097/PRS.0000000000001447
47. Coulson SE, Croxson GR, Adams RD, O'Dwyer NJ. Reliability of the “Sydney,” “Sunnybrook,” and “House Brackmann” facial grading systems to assess voluntary movement and synkinesis after facial nerve paralysis. Otolaryngol Head Neck Surg. (2005) 132:543–9. doi: 10.1016/j.otohns.2005.01.027
48. Kang ST, Vrabec TJ, Giddings JN, Terris JD. Facial nerve grading systems (1985–2002): beyond the House-Brackmann scale. Otol Neurotol. (2002) 23:767–71. doi: 10.1097/00129492-200209000-00026
49. Chong HLS, Eviston JT, Low TH, Hasmat ES, Coulson RS, Clark RJ. Validation of the clinician-graded electronic facial paralysis assessment. Plastic Reconstruct Surg. (2017) 140:159–67. doi: 10.1097/PRS.0000000000003447
50. Banks CA, Jowett N, Hadlock TA. Test-retest reliability and agreement between In-Person and Video assessment of facial mimetic function using the eFACE facial grading system. JAMA Facial Plastic Surg. (2017) 19:206–11. doi: 10.1001/jamafacial.2016.1620
51. Banks CA, Jowett N, Azizzadeh B, Beurskens C, Bhama P, Borschel G, et al. Worldwide testing of the eFACE facial nerve clinician-graded scale. Plastic Reconstruct Surg. (2017) 139:491e. doi: 10.1097/PRS.0000000000002954
52. Volk GF, Granitzka T, Kreysa H, Klingner CM, Guntinas-Lichius O. Initial severity of motor and non-motor disabilities in patients with facial palsy: an assessment using patient-reported outcome measures. Eur Arch Otorhinolaryngol. (2017) 274:45. doi: 10.1007/s00405-016-4018-1
53. Dorion J. Facial neuromuscular retraining. Perspect Swallow Swallow Disord. (2005) 14:18–23. doi: 10.1044/sasd14.2.18
54. Lindsay RW, Robinson M, Hadlock TA. Comprehensive facial rehabilitation improves function in people with facial paralysis: a 5-year experience at the Massachusetts Eye and Ear Infirmary. Phys Ther. (2010) 90:391–7. doi: 10.2522/ptj.20090176
55. Schünemann HJ, Higgins JPT, Vist GE, Glasziou P, Akl EA, Skoetz N, et al. Chapter 14: Completing ‘Summary of findings' tables and grading the certainty of the evidence. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions version 6.0. Cochrane (2019). Available online at: www.training.cochrane.org/handbook
56. O'Neil M, Berkman N, Hartling L, Chang S, Anderson J, Motu'Apuaka M, et al. Observational evidence and strength of evidence domains: case examples. Syst Rev. (2014) 3:35. doi: 10.1186/2046-4053-3-35
57. Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. rating the quality of evidence. J Clin Epidemiol. (2011) 64:401–6. doi: 10.1016/j.jclinepi.2010.07.015
Appendix
Search Strategy (Example)
Database: Ovid MEDLINE(R) ALL <1946 to December 31, 2018>
— — — — — — — — — — — — — — — — — — — –
1. exp Facial Paralysis/ (11721)
2. ((facial or orofacial or oro-facial) adj3 (paralys* or paresis or droop* or palsy or asymmetr* or impair*)).tw. (14536)
3. ((facial or orofacial or oro-facial) adj3 (express* or nerve* or muscle* or move* or reanimat*)).tw. (26746)
4. or/1-3 (38981)
5. exp Physical Therapy Modalities/ (140199)
6. (exercis* or therap* or physiotherap* or rehabilit* or retrain* or train* or treat* or manag* or intervention*).tw. (7745138)
7. (mime* or miming or mirror* or tap* or massag* or stretch* or acupunctur* or needling* or biofeedback or neuromuscular* or kinesio* or cryo*).tw. (382977)
8. (electric* adj2 stimul*).tw. (62989)
9. (e-stim* or electromyograph* or semg).tw. (39537)
10. or/5-9 (8084566)
11. 4 and 10 (15595)
12. exp Central Nervous System Diseases/ (1342443)
13. (central nervous system adj2 (diseas* or injur* or infect*)).tw. (9406)
14. upper motor neuron.tw. (1424)
15. stroke*.tw. (218936)
16. brain injur*.tw. (57635)
17. tbi.tw. (21035)
18. (central adj3 (facial.tw. adj2 (paralys* or paresis or palsy or palsies))).tw. (144)
19. or/12-18 (1463675)
20. 11 and 19 (1970).
Keywords: central facial palsy, rehabilitation, exercise, systematic review, therapy
Citation: Vaughan A, Gardner D, Miles A, Copley A, Wenke R and Coulson S (2020) A Systematic Review of Physical Rehabilitation of Facial Palsy. Front. Neurol. 11:222. doi: 10.3389/fneur.2020.00222
Received: 27 September 2019; Accepted: 10 March 2020;
Published: 31 March 2020.
Edited by:
Limor Avivi-Arber, University of Toronto, CanadaReviewed by:
Meg E. Morris, La Trobe University, AustraliaOrlando Guntinas-Lichius, University Hospital Jena, Germany
Adriaan Grobbelaar, University College London, United Kingdom
Copyright © 2020 Vaughan, Gardner, Miles, Copley, Wenke and Coulson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Annabelle Vaughan, YW5uYWJlbGxlLnZhdWdoYW5AaGVhbHRoLnFsZC5nb3YuYXU=