
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol., 26 April 2019
Sec. Stroke
Volume 10 - 2019 | https://doi.org/10.3389/fneur.2019.00433
 Shaonan Liu1,2,3,4†
Shaonan Liu1,2,3,4† Claire Shuiqing Zhang5†Yiyi Cai1,2,3,4,5Xinfeng Guo1,2,3,4Anthony Lin Zhang5Charlie Changli Xue1,3,4,5*
Claire Shuiqing Zhang5†Yiyi Cai1,2,3,4,5Xinfeng Guo1,2,3,4Anthony Lin Zhang5Charlie Changli Xue1,3,4,5* Chuanjian Lu1,3,4,5*
Chuanjian Lu1,3,4,5*Background: Shoulder-hand syndrome (SHS) is prevalent in hemiplegic patients after stroke. Potential benefits of acupuncture were shown in recent clinical trials. This systematic review aimed to comprehensively evaluate the safety and efficacy of acupuncture for SHS in stroke patients.
Methods: Five English databases (PubMed, Embase, CINAHL, CENTRAL, and AMED) and four Chinese databases (CBM, CNKI, CQVIP, and Wanfang) were searched from their inceptions to January 2019. Randomized, controlled trials that evaluated the add-on effects of acupuncture to rehabilitation for post-stroke SHS were identified.
Results: Thirty-eight studies involving 3,184 participants fulfilled the eligible criteria and were included in the review. The overall meta-analysis showed that acupuncture combined with rehabilitation significantly improved motor function (upper-limb Fugl-Meyer Assessment (FMA): 34 studies, mean difference (MD) 8.01, 95% confidence interval (CI) [6.69,9.33]), and reduced pain (visual analog scale (VAS): 25 studies, MD −1.59, 95%CI [−1.86,−1.32]). It also improved activities of daily living (ADL) when compared with rehabilitation alone (ADL: 11 studies, MD 9.99, 95%CI [5.91,14.06]). However, the certainty of evidence of all these outcomes was assessed as “low.” Subgroup analyses of acupuncture stimulation types and treatment duration all showed significant add-on effects comparing with rehabilitation alone. The safety of acupuncture was unclear because there is a lack of detailed reporting of adverse events in most of the included studies.
Conclusions: Acupuncture therapy seems effective for motor function, pain relief and activities of daily living in stroke patients with mild SHS, when it is used in combination with rehabilitation. The low certainty of evidence downgrades our confidence in making recommendations to clinical practice.
Shoulder-hand syndrome (SHS) is a common condition among people who have had a stroke, with its reported prevalence ranging from 12% to 49% (1, 2). The main symptoms of SHS include pain, hyperalgesia, joint swelling and limitations in range of motion (ROM) (3). Post-stroke SHS is also named type I complex regional pain syndrome (CRPS) or reflex sympathetic dystrophy (4). The key to effectively treating SHS is believed to be an expert multidisciplinary team that provides individualized therapy (5). There is a wide range of treatment options available to help manage post-stroke SHS, including physical therapy, medications, regional anesthesia techniques and neuromodulation. However, there is insufficient evidence to support their efficacy (5).
Acupuncture, one of the most popular traditional Chinese medicine therapies, has been widely used in the clinical management of stroke (6). Several systematic reviews have assessed its efficacy for improving stroke rehabilitation using outcomes in motor function recovery and disability, but results are inconsistent (7–11). Three reviews published before 2010 showed acupuncture did not improve motor function or dependency outcomes after rehabilitation (8, 9, 11). However, two more recently published reviews suggested acupuncture might aid rehabilitation in several areas, including motor function recovery and pain relief (7, 10).
Three systematic reviews specifically evaluating acupuncture for post-stroke SHS have been published (12–14). Two of these were published before 2013 (12, 13), so they don't include recently published clinical evidence. Moreover, one review including three studies did not perform quantitative synthesis due to clinical heterogeneity (13). The third review (14) does not evaluate the effectiveness of electro-acupuncture, and only two of its included studies evaluated the effectiveness of acupuncture combined with routine care. Considering electro-acupuncture is commonly used in the clinical management of stroke complications, the implication of the review results (14) for clinical practice is limited. Therefore, we conducted this systematic review looking at the most recent evidence of acupuncture (including electro-acupuncture) as an additional therapy in the clinical management of post-stroke SHS.
This systematic review included randomized controlled trials (RCT) or quasi-RCTs that were published in English or Chinese and evaluated acupuncture's effects as an additional therapy for post-stroke SHS. Quasi-RCTs were evaluated using the same methods applied to RCTs.
We registered its protocol with the PROSPERO international prospective register of systematic reviews (CRD 42016050446).
We limited participants to people who were diagnosed with post-stroke SHS. The stroke (ischemic or hemorrhagic) diagnosis needed to be confirmed by computer tomography or magnetic resonance imaging. The SHS or CRPS type I diagnosis was based on clinical symptoms, including pain, motor disturbances and skin changes (3).
We included RCTs or quasi-RCTs that evaluated the effects of manual or electro-acupuncture combined with routine care or rehabilitation as the experimental intervention in this review. Studies that assessed auricular acupuncture or other types of recently developed acupuncture forms, such as floating acupuncture, were excluded from this review.
The rehabilitation therapy used in RCTs or quasi-RCTs could be a combination of physiotherapy and occupational therapy, such as active ROM, passive ROM, mirror visual feedback, Bobath therapy, alternating heat and cold baths, and massage. The comparator was the same as the rehabilitation therapy used in the intervention group, but without acupuncture. Studies that used placebo or sham acupuncture and the same rehabilitation therapy in the control group were also eligible for inclusion.
RCTs or quasi-RCTs that reported validated SHS outcome measures as below were considered for inclusion in this review.
Primary outcome measures: (1) motor function: Fugl-Meyer Assessment (FMA) upper limb; (2) pain assessment using visual analog scale (VAS) or numerical rating scale (NRS).
Secondary outcome measures: (1) Barthel Index (BI) or Modified Barthel Index (MBI), which is assessed for self-care and activities of daily living; (2) ROM; and (3) adverse events.
We searched nine databases, five in English, and four in Chinese languages, from their inceptions to January 2019. They are: PubMed, Embase, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Controlled Trials (CENTRAL), the Allied and Complementary Medicine Database (AMED), China BioMedical Literature (CBM), China National Knowledge Infrastructure (CNKI), Chonqing VIP (CQVIP), and Wanfang. We also searched clinical trial registration agencies, including the Chinese Clinical Trial Registry and National Institutes of Health Register (Clinical Trials.gov), and hand-searched references lists of included studies and relative systematic reviews. The search terms and search strategy we used are presented in Appendix S1.
Two researchers (SL, YC) independently screened the titles, abstracts and full text of studies to assess eligibility. Any uncertainty was resolved through discussion with CZ. SL and YC developed a standardized data extraction file using Epidata software 3.1 (The EpiData Association, Odense, Denmark, 2003–2008). They also extracted data independently and cross-checked it for accuracy. Extracted data included: author, publication year, diagnostic criteria, duration of disease, sample size, participants' age, details of interventions and all clinical outcomes.
Two researchers (SL, YC) used the Cochrane risk of bias tool to assess the methodological quality of the included studies. They assessed seven items: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, selective reporting, and other sources of bias. The studies were judged as having a “low,” “high,” or “unclear” risk of bias. SL and YC resolved any difference in their assessment of a study by discussing it with a third researcher (CZ).
The Grading of Recommendations Assessment, Development and Evaluation Approach (GRADE) was used to evaluate the certainty of evidence. Five items involving risk of bias, inconsistency, imprecision, indirectness and publication bias were investigated for the clinical important outcomes.
The included studies calculated acupuncture's safety and efficacy when combined with rehabilitation to treat SHS, compared to rehabilitation alone. Data analyses were performed in a random-effects model using the RevMan software (version 5.3). Dichotomous data was reported as relative risk (RR) with corresponding 95% confidence intervals (CI). For continuous data, the mean difference (MD) with 95% CI was calculated.
The following subgroup analyses were planned: (1) subgroups of manual or electro-acupuncture; (2) subgroups of treatment duration ≤4 or >4 weeks. Since an inappropriate randomization sequence generation was associated with biased intervention effects (15), we conducted a sensitivity analysis to check the robustness of the results by only including the RCTs that were assessed as “low” risk of bias for this item.
We identified 36 eligible studies (16–51) by searching Chinese and English databases up to March 2017. An updated search, including studies from 2017 to January 2019, located another two studies that met the inclusion criteria (52, 53). As a result, 38 RCTs involving 3,184 participants were included in this review (Figure 1).
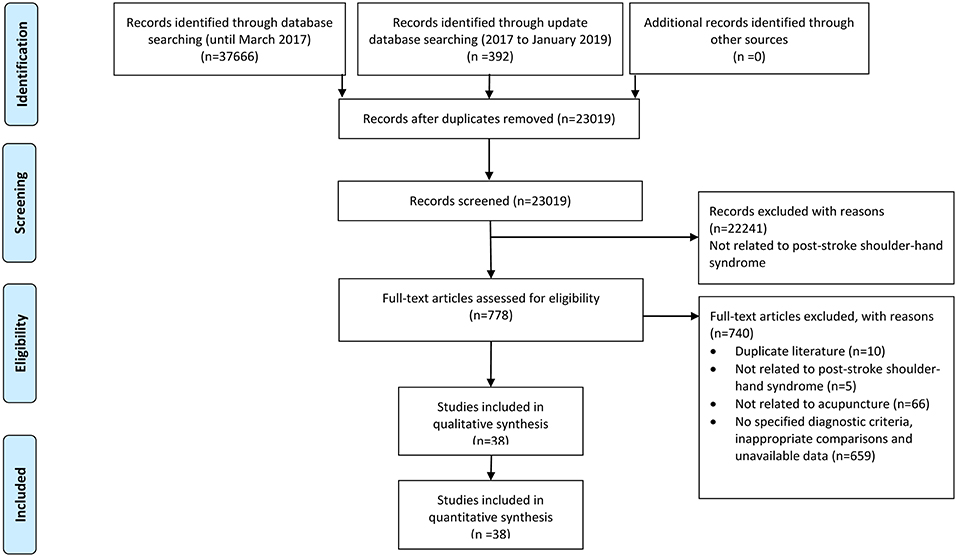
Figure 1. PRISMA flow chart.
As reported by the included studies, SHS occurred after ischemic stroke in four studies (40, 42, 44, 45), and after hemorrhagic or ischemic stroke in 23 studies. The remaining 11 studies (17–19, 23, 28, 30, 31, 41, 46, 47, 50) did not include information about the type of stroke. The duration of stroke ranged from 10 days (46) to 19 months (17). The severity of SHS was reported by 27 studies and divided into acute-hyperaemic (stage I), dystrophic-ischaemic (stage II) and atrophic (stage III) according to clinical symptoms (54). Twenty studies recruited participants at stage I with mild symptoms of <3 months of SHS. The remaining seven studies included participants with stage II or III.
All of the eligible trials compared body acupuncture plus routine rehabilitation with routine rehabilitation alone. Of all, 12 studies also applied electrical stimulation with acupuncture (16–18, 20, 21, 32, 34, 36–39, 46). The most commonly used acupuncture points were LI15 Jianyu, LI11 Quchi, TE5 Waiguan, LI4 Hegu, TE14 Jianliao, LI10 Shousanli, HT1 Jiquan, PC6 Neiguan, and SI9 Jianzhen. Routine rehabilitation included active ROM, passive ROM, mirror visual feedback, Bobath therapy, alternating heat and cold baths, and massage. Treatment duration ranged from 2 to 8 weeks. None of the included studies involved a follow-up phase to investigate acupuncture's long-term effects.
Thirty-four studies used FMA to evaluate acupuncture's effects on upper limb motor function. Pain severity was assessed with VAS in 26 studies. None of the included studies reported NRS. For secondary outcomes, 11 studies reported BI or MBI, six studies reported ROM, and five studies reported adverse events (Table 1).
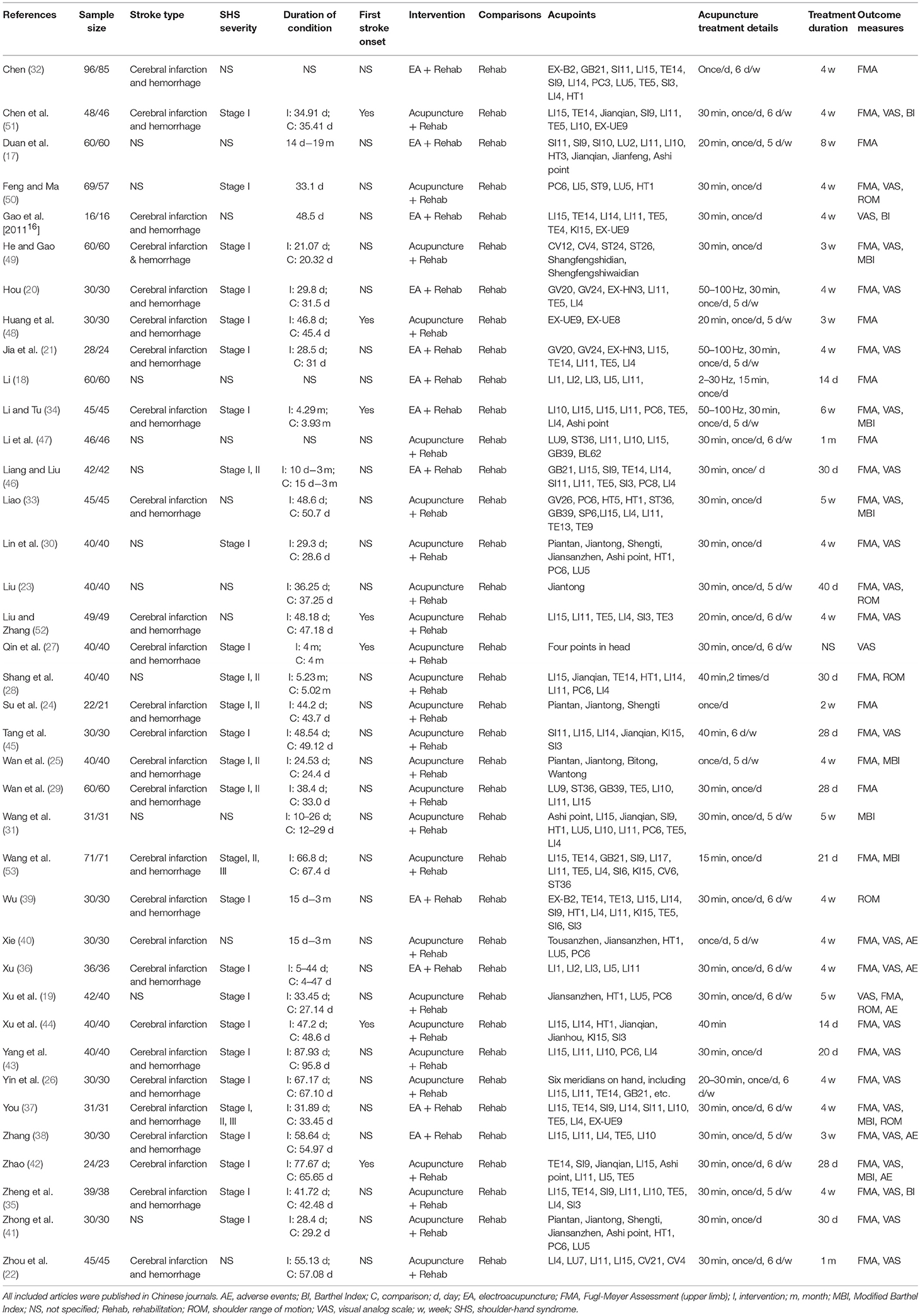
Table 1. Basic characteristics.
Seventeen studies (45%) were assessed as “low” risk of bias for sequence generation, and the remaining studies were assessed as “unclear” risk due to a lack of information. Only one study (38) used opaque envelopes to conceal the allocation procedure, so it was assessed as “low” risk of bias for this item. Blinding of participants and acupuncturists was not performed in any study. Blinding of outcome assessors was assessed as “unclear” risk of bias for all studies due to a lack of information. We also assessed selective outcome reporting as “unclear” risk of bias for all studies, because none of the studies had published their protocols. For incomplete outcome data, we assessed all studies as “low” risk of bias because there was no missing outcome data. Eleven studies (18, 19, 24–27, 29, 32, 43, 48, 52) reported the funding source and showed balanced baseline data, so we assessed the relative other bias as “low” risk. Details are summarized in Figure 2 and Figure S1.
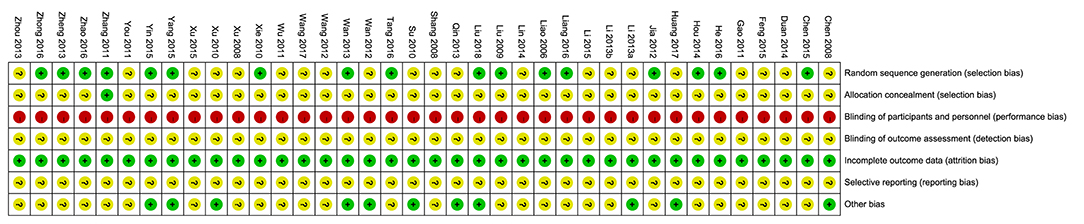
Figure 2. Risk of bias of each study.
Thirty-four studies reported data on upper limb FMA scores when acupuncture was combined with rehabilitation compared to rehabilitation alone. Meta-analysis of 29 studies showed the combination therapy had a significant superior effect (MD: 8.01, 95% CI [6.69, 9.33]; I2 = 78%). We did not include the remaining five studies (17, 18, 32, 33, 48) in our analysis due to their inappropriate data reporting: three studies (18, 33, 48) only reported scores of certain items without the total score, one study (32) reported FMA as categorical data, and one study (17) did not report FMA data for the control group.
Compared with routine rehabilitation alone, acupuncture combined with routine rehabilitation showed superior effects on VAS scores in 25 studies (MD: −1.59, 95% CI [−1.86, −1.32]; I2 = 87%). We excluded one study (27) in the meta-analysis because its data was reported with median and interquartile ranges.
Eleven studies reported acupuncture's effects on ADL performance, as measured by the Barthel Index (BI) or Modified Barthel Index (MBI). Meta-analysis showed that acupuncture combined with routine rehabilitation enhanced ADL performance more than rehabilitation alone did (MD: 9.99, 95% CI [5.91, 14.06]; I2 = 86%).
Acupuncture combined with routine rehabilitation improved shoulder abduction by an average of 11.94 degrees (three studies (19, 23, 37): 95% CI [9.44, 14.45]; I2 = 0%), shoulder internal rotation by 18.72 degrees (one study (37): 95% CI [9.63, 27.81]), and shoulder external rotation by 15.73 degrees (one study (37): 95% CI [6.82, 24.64]), when compared with rehabilitation alone.
Subgroup analysis was conducted to examine whether adding electrical stimulation to manual acupuncture will affect primary outcomes. Manual and electro-acupuncture combined with routine rehabilitation improved FMA and pain VAS outcomes more than rehabilitation alone did (Figures 3, 4). The effect of electro-acupuncture (MD 9.08, 95% CI [6.81, 11.35]) seems greater in magnitude than manual acupuncture (MD 7.80, 95% CI [6.30, 9.30]) for improving upper limb motor function, however, there was not any direct analysis to compare electro-acupuncture with manual acupuncture in this research.
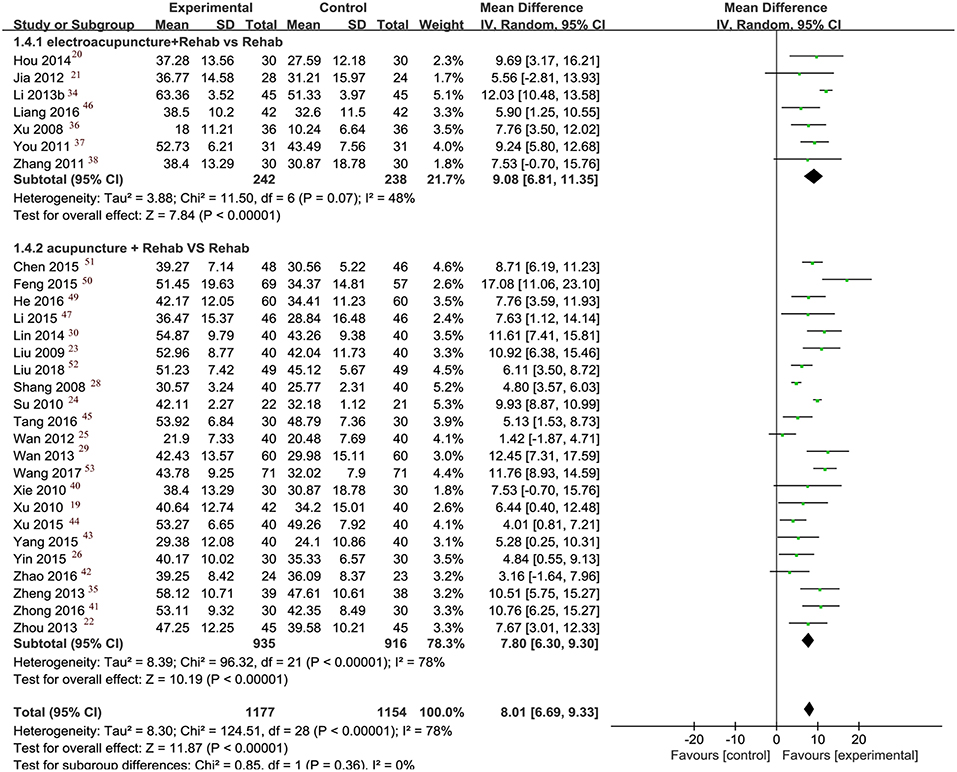
Figure 3. Forest plot of FMA.
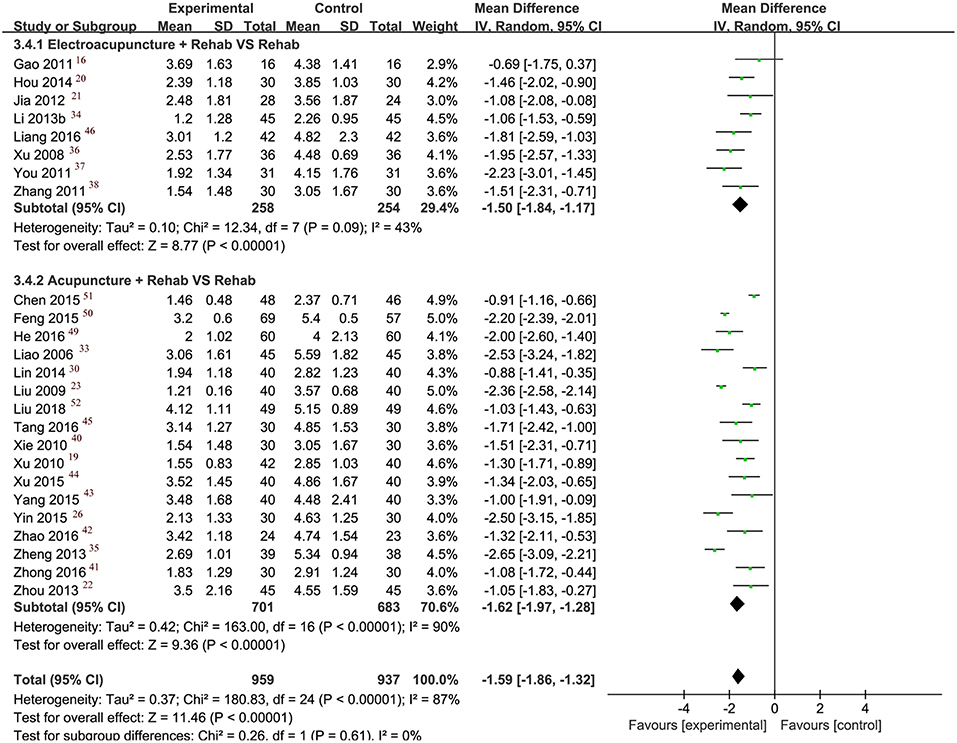
Figure 4. Forest plot of VAS.
Further subgroup analyses in the manual or electro-acupuncture group looked at the impact of treatment duration on outcomes. We found that treatment duration (≤4 weeks or >4 weeks) did not significantly change the outcome. However, the number of studies included in each subgroup was relatively small (Table 2).
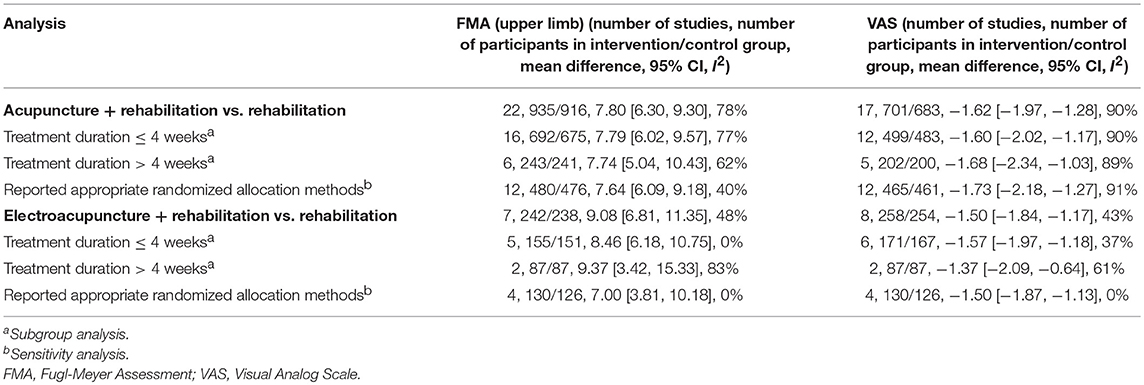
Table 2. Subgroup analysis and sensitivity analysis.
Sensitivity analysis was performed by only including studies that reported appropriate randomization sequence generation methods. The results were similar to that of the overall pool, with lower heterogeneity. The results also showed that acupuncture combined with routine rehabilitation produces better outcomes for FMA and VAS than rehabilitation alone (Table 2).
Publication bias was evaluated based on FMA and VAS, which were reported in 29 and 25 studies, respectively. Egger's test demonstrated there was no significant publication bias (FMA: t = −0.39, P = 0.702; VAS: t = 1.50, P = 0.147).
Thirty-three studies did not mention adverse events. Four studies reported that no adverse event occurred during the trials (19, 36, 40, 42). One RCT (38) described that three participants in the intervention group and two in the control group reported bruising after treatment. These events were considered to be mild and did not require any medical management. The study did not explore the causality of these adverse events (38).
The evidence of all these outcomes was assessed as “low” certainty. The certainty of evidence was downgraded mainly due to the limitations in study design and inconsistency of results. The summary of finding table was presented in Table 3.
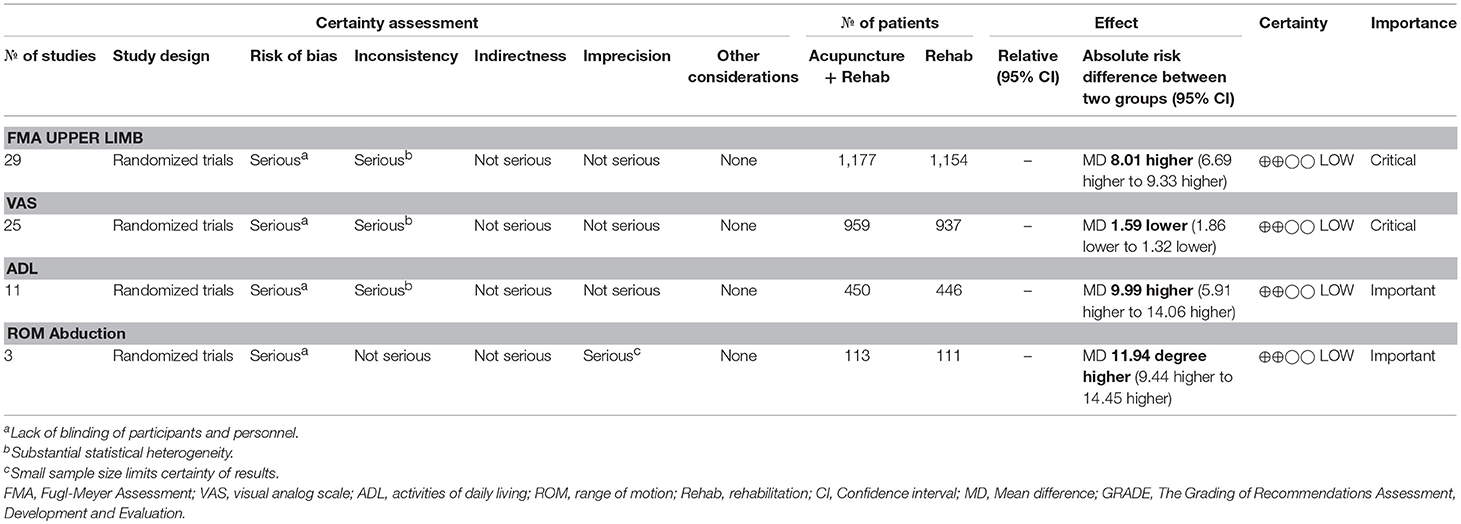
Table 3. Certainty of evidence (GRADE).
In this review, we identified 38 RCTs that evaluated the effects of adding acupuncture to routine rehabilitation to treat post-stroke SHS. Results showed that the combination of acupuncture and routine rehabilitation was superior to rehabilitation alone for improving motor function and ADL, and reducing pain. Manual and electro-acupuncture were both beneficial in the subgroup analysis. Further analysis of treatment duration did not indicate that treatment outcomes change with a long course of treatment (e.g., more than 4 weeks). The safety of acupuncture should be further validated, because most of the included studies did not mention adverse events. In addition, the overall “low” GRADE assessment results made our certainty in recommending this therapy to clinical practice as “low.”
Manual and electro-acupuncture combined with routine rehabilitation improved FMA more than rehabilitation alone did. Moreover, the results reached the minimal clinical important difference (MCID) suggested by Page et al. (55) and Chen et al. (56) (5.2 and 4.58, respectively). Our results, based on 29 RCTs, confirmed the results of one previous systematic review (12) that evaluated FMA in six RCTs. Another previously published review (14) showed no benefit of acupuncture, however, the review only included two manual acupuncture RCTs in its meta-analysis. In contrast, our review included more studies with a larger sample size. It should also be noted that recent studies have sought to improve their methodology quality, with half of the included studies reporting appropriate randomization sequence generation. These will provide a greater certainty of the evidence of acupuncture's effect on motor function.
In terms of pain VAS, our review showed acupuncture combined with routine rehabilitation was much more effective than rehabilitation alone at reducing pain. These results are consistent with a recent systematic review of acupuncture for post-stroke shoulder pain (57). Furthermore, our review showed that manual and electro-acupuncture both help to relieve pain when used in combination with routine rehabilitation. This could reinforce the evidence for acupuncture in reducing pain associated with post-stroke SHS (Table 2).
The mechanism of how acupuncture relieves pain has been extensively studied. Electro-acupuncture alleviates sensory and affective inflammatory pain by acting through bioactive chemicals, including opioids, serotonin, and norepinephrine; glutamate receptors and transporters; cytokines; and signal molecules (58–63). With regard to how acupuncture helps to improve motor function, experimental studies indicate it may work by enhancing the gamma-aminobutyric acid receptor expression or promoting angiogenesis (64, 65). Currently, there is no consensus on the mechanism of acupuncture for SHS or CRPS, so further research is needed to investigate how acupuncture influences sympathetic/somatic nervous system dysfunction.
Our systematic review has several strengths. First, we explored the effects of acupuncture for a specific complication (SHS) after stroke, rather than general motor function. Acupuncture points around the shoulder were the most frequently points used in treatment for SHS, which is consistent with two previous reviews (57, 66). These results may provide more focused evidence to improve clinical practice and health outcomes. Second, this systematic review was based on a comprehensive and up-to-date search of literature, with reliable evidence generated from analyses with large sample sizes. Third, subgroup analyses were conducted according to the type of acupuncture stimulation. Both electro-acupuncture and manual acupuncture were effective when they were used as add-on therapies. Fourth, validated outcome measures were selected to assess acupuncture's efficacy, which will also strengthen the reliability of our results.
However, some limitations of this review should be considered before its results can be translated to clinical practice. First, none of the studies used sham or placebo acupuncture in the control treatment. This means that the placebo effects of adding an intervention cannot be ruled out. In particular, Chinese populations usually have high expectations for acupuncture and this may have inflated treatment outcomes for the combined therapy. Second, the treatment duration and number of treatment sessions in the included studies varied greatly. Although we conducted a subgroup analysis based on treatment duration, the optimal duration, and number of treatment sessions are still unclear. Third, the included studies did not give enough information about the acupuncture parameters, such as depth of needle insertion and the acupuncturists' backgrounds. This may affect the clinical implications of this research. Fourth, few studies reported adverse events, making it difficult for us to provide a conclusion about acupuncture's safe use in the management of post-stroke SHS. Moreover, none of the studies performed a long-term follow-up investigation of acupuncture, so it's unclear if acupuncture has a sustained effect on post-stroke SHS. Future clinical studies should include a sham/placebo control, a follow-up phase, and an in-depth data collection of adverse events.
All of the studies included in this review were conducted on mainland China. Further studies should be done around the world to involve more ethnically and culturally diverse populations. The methodological quality of future clinical trials should also be improved. In particular, double-blinding should be used where possible to avoid RCT performance bias. While it's difficult to have genuine double-blinding in acupuncture trials because acupuncturists have to be aware of the participants' group allocation to treat them, participants can be blinded by using well-designed placebo acupuncture devices and sham acupuncture (67, 68). Outcome assessors can also be blinded. Finally, reports from future RCTs should follow the Consolidated Standards of Reporting Trials (CONSORT) statement and STRICTA checklists (69, 70).
This systematic review shows that adding acupuncture to routine rehabilitation can improve clinical outcomes (pain and motor function) for people with mild post-stroke SHS. However, the evidence was assessed as “low” by GRADE due to the methodological limitations and heterogeneity of included studies, which made our certainty in recommending acupuncture for this condition in clinical practice as “low.” Well-designed placebo-controlled RCTs with a long treatment duration and follow up, as well as standardized reporting, are needed to support acupuncture's safe and effective use in the management of post-stroke SHS.
SL and CZ designed this study. SL, CZ, and YC performed data extraction and statistical analysis. SL, CZ, YC, XG, AZ, CX, and CL revised and approved the final manuscript.
The project is supported by a grant from the China–Australia International Research Centre for Chinese Medicine, funded by the Guangdong Provincial Academy of Chinese Medical Sciences and Guangdong Provincial Hospital of Chinese Medicine, Guangdong, China, and RMIT University, Australia. It is also partially supported by a grant from the International Science & Technology Cooperation Project of the Ministry of Science and Technology of China (Project Grant no. 2012DFA31760), the State Administration of Traditional Chinese Medicine, China (Project Grant no. 1601500000027(11)) and the State Administration of Traditional Chinese Medicine, China (Project Grant no. GJZX2016019).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank clinical rehabilitation experts, Dr. Chen hongxia and Dr. Pan ruihuan for their comments on this manuscript. They also acknowledge Dr. Lai jiaqi and Dr. Zuo jinhong for their assistance with extracting the data.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2019.00433/full#supplementary-material
Figure S1. The summary of risk of bias graph.
Appendix S1. Search strategy.
1. Kocabas H, Levendoglu F, Ozerbil OM, Yuruten B. Complex regional pain syndrome in stroke patients. Int J Rehabil Res. (2007) 30:33–8. doi: 10.1097/MRR.0b013e3280146f57
2. Petchkrua W, Weiss DJ, Patel RR. Reassessment of the incidence of complex regional pain syndrome type 1 following stroke. Neurorehabil Neural Repair. (2000) 14:59–63. doi: 10.1177/154596830001400107
3. Pertoldi S, Di Benedetto P. Shoulder-hand syndrome after stroke. A complex regional pain syndrome. Eura Medicophys. (2005) 41:283–92.
4. Swati M, Teasull R, Foley N. Evidence-Based Review of Stroke Rehabilitation–Hemiplegic Shoulder Pain. Available online at: www.ebrsr.com (accessed April 10, 2018).
5. Forouzanfar T, Koke AJ, van Kleef M, Weber WE. Treatment of complex regional pain syndrome type I. Eur J Pain. (2002) 6:105–22. doi: 10.1053/eujp.2001.0304
6. Hu HH, Chung C, Liu TJ, Chen RC, Chen CH, Chou P, et al. A randomized controlled trial on the treatment for acute partial ischemic stroke with acupuncture. Neuroepidemiology. (1993) 12:106–13. doi: 10.1159/000110308
7. Wu P, Mills E, Moher D, Seely D. Acupuncture in poststroke rehabilitation: a systematic review and meta-analysis of randomized trials. Stroke. (2010) 41:e171–9. doi: 10.1161/STROKEAHA.109.573576
8. Park J, Hopwood V, White AR, Ernst E. Effectiveness of acupuncture for stroke: a systematic review. J Neurol. (2001) 248:558–63. doi: 10.1007/s004150170132
9. Sze FK, Wong E, Or KK, Lau J, Woo J. Does acupuncture improve motor recovery after stroke? A meta-analysis of randomized controlled trials. Stroke. (2002) 33:2604–19. doi: 10.1161/01.STR.0000035908.74261.C9
10. Yang A, Wu HM, Tang JL, Xu L, Yang M, Liu GJ. Acupuncture for stroke rehabilitation. Cochrane Database Syst Rev. (2016) 8:CD004131. doi: 10.1002/14651858.CD004131.pub3
11. Zhang SH, Liu M, Asplund K, Li L. Acupuncture for acute stroke. Cochrane Database Syst Rev. (2005) 2:CD003317. doi: 10.1002/14651858.CD003317.pub2
12. Xu Y, Li W, Liu J, Ma L. Acupuncture versus rehabilitation therapy for shoulder hand syndrome: a systematic review and meta-analysis [Article in Chinese]. Lishizhen Med Mater Med Res. (2013) 24:1794–8. doi: 10.3969/j.issn.1008-0805.2013.07.114
13. Lu Y, Fu L, Mu J, Xu H, Qi Y. Acupuncture for post stroke shoulder hand syndrome: a systematic review [Article in Chinese]. Chinese J Evid-based Med. (2009) 9:976–8. doi: 10.3969/j.issn.1672-2531.2009.09.010
14. Liu K, Han X, Pan X, Xiong J. Acupuncture in the treatment of poststroke shoulder hand syndrome: a systematic review [Article in Chinese]. Chinese J Rehabil Med. (2015) 30:1041–5. doi: 10.3969/j.issn.1001-1242.2015.10.014
15. Savovic J, Jones HE, Altman DG, Harris RJ, Juni P, Pildal J, et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Ann Intern Med. (2012) 157:429–38. doi: 10.7326/0003-4819-157-6-201209180-00537
16. Gao P, Li Y, Wang Z, Jiang M, Luo Y. Effect of electro-acupuncture combined with rehabilitation for the treatment of shoulder hand syndrome [Article in Chinese]. Chin Manipul Rehabilit Med. (2011) 2:49–50.
17. Duan Y, Liu F, Zhang Y. Effect of electro-acpuncture combined with rehabilitation training on shoulder hand syndrome [Article in Chinese]. Jilin J Trad Chin Med. (2014) 34:190–1. doi: 10.13463/j.cnki.jlzyy.2014.02.031
18. Li M. Clinical research of electro-acupuncture on Large intestine meridian five acupoint for the treatment of poststroke should-hand syndrome [Article in Chinese]. Jilin J Trad Chin Med. (2013) 33:191–2. doi: 10.3969/j.issn.1003-5699.2013.02.041
19. Xu S, Zhuang L, Jia C, Xu D, Pan C. Clinical observation of Jin's Three-needle manipulation combined with rehabilitation therapy for treatment of post-stroke shoulder-hand syndrome [Article in Chinese]. J Guangzhou University Trad Chin Med. (2010) 27:19–22. doi: 10.13359/j.cnki.gzxbtcm.2010.01.009
20. Hou Z. Effect of acupuncture combined with rehabilitation on stage I of shoulder-hand syndrome after stroke [Article in Chinese]. J Clin Med in Prac. (2014) 18:58–59, 66.
21. Jia C, Ni G, Tan H, Zhang X. Clinical effect of acupuncture combined with rehabilitation on stage I of shoulder-hand syndrome after stroke [Article in Chinese]. J Changchun University Trad Chin Med. (2012) 28:711–2. doi: 10.13463/j.cnki.cczyy.2012.04.084
22. Zhou F, Zeng K, Lu Y. Clincial effect of Taichi acupuncture combined with rehabilitation for the treatment of poststroke shoulder-hand syndrome [Article in Chinese]. Modern Diagn Treatment. (2013) 24:1004–6. doi: 10.3969/j.issn.1001-8174.2013.05.027
23. Liu Y. Clinical research of treating shoulder-hand syndrome by contralateral acupuncture on shoulder pain point combining with rehabilitation training [Article in Chinese]. Gansu Med J. (2009) 28:176–8. doi: 10.15975/j.cnki.gsyy.2009.03.002
24. Su J, Pan C, Wan X. The balancing acupuncture combined with rehabilitation for the treatment of shoulder-hand syndrome after stroke [Article in Chinese]. Chin J Rehab. (2010) 25:188–9. doi: 10.3870/zgkf.2010.03.010
25. Wan X, Su J, Ye Z, Luo R, Zeng Y. Effects of balancing acupuncture combined with rehabilitation in treatment of shoulder-hand syndrome after stroke [Article in Chinese]. Int Med Health Guid News. (2012) 18:3534–7. doi: 10.3760/cma.j.issn.1007-1245.2012.24.002
26. Yin J, Zhou G, Zhou G, Fan H. Therapeutic observation of acupuncture at the interiorly-exteriorly related meridians plus rehabilitation training for poststroke shoulder-hand syndrome [Article in Chinese]. Shanghai J Acupunct Moxibust. (2015) 34:7–10. doi: 10.13460/j.issn.1005-0957.2015.01.0007
27. Qin H, Shi J, Zhang Y, Ma D, Gao Q. Observations on the efficacy of scalp point-to-point acupuncture plus rehabilitation training in treating poststroke shoulder-hand syndrome [Article in Chinese]. Shanghai J Acupunct Moxibust. (2013) 32:167–169. doi: 10.3969/j.issn.1005-0957.2013.03.167
28. Shang Y, Ma C, Cai Y, Wang D, Kong L. Clinical study on acupuncture combined with rehabilitation therapy for treatment of poststroke shoudler-hand syndrome [Article in Chinese]. Chinese J Acupunct Moxibust. (2008) 28:331–3. doi: 10.13703/j.0255-2930.2008.05.017
29. Wan W, Wang T, Cheng S, Zhao Y, Zhang W, Wu Q, et al. Poststroke shoulder-hand syndrome treated with acupuncture and rehabilitation: a randomized controlled trial [Article in Chinese]. Chinese J Acupunct Moxibust. (2013) 33:970–4. doi: 10.13703/j.0255-2930.2013.11.026
30. Lin H, Ye G, Liao H, Lin F, Liang B. Acupuncture combined with rehabilitation training in the treatment of shoulder-hand syndrome after stroke [Article in Chinese]. World Chin Med. (2014) 9:84–85, 88. doi: 10.3969/j.issn.1673-7202.2014.01.030
31. Wang X, Gao C, Ma S. Clinica study on acupuncture combined with rehabilitation training in treatment of shoulder-hand syndrome after stroke [Article in Chinese]. J Clin Exp Med. (2012) 11:942–3. doi: 10.3969/j.issn.1671-4695.2012.12.018
32. Chen M. Clinical observation on the resluts of treatment of shoulder-hand syndrome due to cerebral stroke with acupuncture [Article in Chinese]. China Trop Med. (2008) 8:1781, 1717. doi: 10.3969/j.issn.1009-9727.2008.10.061
33. Liao H. Clinical observation on the efficacy of occupational therapy plus acupuncture for treating reflex sympathetic dystrophy [Article in Chinese]. Shanghai J Acupunct Moxibust. (2006) 25:9–10. doi: 10.3969/j.issn.1005-0957.2006.03.004
34. Li F, Tu M. Effect of electroacupuncture combined with occupational therapy on stage I of shoulder-hand syndrome after stroke [Article in Chinese]. China J Pharmaceut Econom. (2013) :370–1.
35. Zheng S, Wu Y, Chang J, Cui S, Xu M, Lian J, et al. Clinical effect of acupuncture on shoulder-hand syndrome after stroke [Article in Chinese]. Chinese J Rehabil Med. (2013) 28:40–1. doi: 10.3870/zgkf.2013.01.015
36. Xu Z. Clinical Observation of Electro-Acupuncture on Large Intestine Meridian Five Acupoint for the Treatment of Poststroke Should-Hand Syndrome [Dissertation]. Changchun, Changchun University of Chinese Medicine (2008).
37. You Y. A Clinical Study of Electroacupuncture Combined with Rehabilitation Training in the Treatment of Shoulder-Hand Syndrome of Poststroke [Dissertation]. Jinan, Shandong University of Chinese Medicine (2011).
38. Zhang X. Clinical Research of Acupuncture Combined With Rehabilitation Training for the Treatment of Shoulder-Hand Syndrome after Stroke [Dissertation]. Guangzhou, Guangzhou University of Chinese Medicine (2011).
39. Wu Z. Investigate the Clincial Effect of the Neck Clip Ridge and Through Thorn Acupuncture Methods on Treating the Shoulder-Hand Syndrome [Dissertation]. Harbin, Heilongjiang University of Chinese Medicine (2011).
40. Xie Q. A Clinical Study of Acupuncture Combined with Rehabilitation Training in the Treatment of Shoulder-Hand Syndrome after Stroke [Dissertation]. Guangzhou, Guangzhou University of Chinese Medicine (2010).
41. Zhong C, Ni D, Lin W, Chen F. Clinical observation of acupuncture combined with rehabilitation training for the treatment of poststroke shoulder-hand syndrome [Article in Chinese]. Hainan Med J. (2016) 27:1687–8. doi: 10.3969/j.issn.1003-6350.2016.10.048
42. Zhao J. Clinical Effect of Acupuncture Combined with TDP Lamp Irradiation for the Treatment of Shoulder-Hand Syndrome After Stroke [Dissertation]. Shenyang, Liaoning University of Traditional Chinese Medicine (2016).
43. Yang D, He X, Cai W, Yang X, Yang M. Clinical effect of floating acupuncture combined with rehabilitation for the treatment of shoulder-hand syndrome after stroke [Article in Chinese]. Lishizhen Med Mater Med Res. (2015) 26:139–1341.
44. Xu F, Li H, Zhang Q. Acupuncture combined with rehabilitation for the treatment of poststroke shoulder-hand syndrome: a randomised controlled trial [Article in Chinese]. Chin J Trauma Disability Med. (2015) 3:141–2. doi: 10.13214/j.cnki.cjotadm.2015.16.107
45. Tang D, Wu W, Sun X. Acupuncture combined with rehabilitation for the treatment of poststroke shoulder-hand syndrome: a randomised controlled trial [Article in Chinese]. J Clin Acupunct Moxibust. (2016) 32:26–9.
46. Liang N, Liu X. Clinical observation of electroacupuncture combined with rehabilitation training for the treatment of poststroke shoudler-hand syndrome [Article in Chinese]. Guide China Med. (2016) 14:200–1. doi: 10.15912/j.cnki.gocm.2016.25.163
47. Li Z, Gu J, Hu M. Clinical observation of acupuncture for the treatment of 46 case of shoudler-hand syndrome after stroke [Article in Chinese]. Chin J Ethnomed Ethnoph. (2015) 24:78–9.
48. Huang C, Fan W, Yu A, Cui X, Wu J. Penetration acupuncture at Baxie(EX-UE 9) combinded with rehabilitation for swelling hand of poststroke shoudler-hand syndrome [Article in Chinese]. Chinese J Acupunct Moxibust. (2017) 37:121–124. doi: 10.13703/j.0255-2930.2017.02.004
49. He S, Gao S. Evaluation of abdominal acupuncture and rehabilitation treatment for shoudler-hand syndrome. (period I) after stroke [Article in Chinese]. J Clin Acupunct Moxibust. (2016) 32:11–13.
50. Feng Y, Ma S. Acupuncture combined with infrared acupoint irradiation and rehabilitation treatment of 126 cases of clinical observation on shoulder-hand syndrome after stroke [Article in Chinese]. Laser J. (2015) 36:195–7. doi: 10.14016/j.cnki.jgzz.2015.04.195
51. Chen Y, Huang T, Liu K. Clinical research of using acupuncture and rehabilitation training in the treatment of poststroke shoudler-hand syndrome stage I [Article in Chinese]. Sichuan J Trad Chin Med. (2015) 23:150–2.
52. Liu Y, Zhang H. Effect of acupuncture combined with rehabilitation training on patients with acute shoulder-hand syndrome after stroke [Article in Chinese]. J Hun Univers Chin Med. (2018) 38:546–9. doi: 10.3969/j.issn.1674-070X.2018.05.015
53. Wang X, Gao Y, Gao S. Effect of acupuncture combined with rehabilitation training on PRI, FMA and MBI in patients with shoulder-hand syndrome after stroke [Article in Chinese]. Global Trad Chin Med. (2017) 10:361–3. doi: 10.3969/j.issn.1674-1749.2017.03.033
54. Schwartzman RJ, McLellan TL. Reflex sympathetic dystrophy. A review. Arch Neurol. (1987) 44:555–61. doi: 10.1001/archneur.1987.00520170081028
55. Page SJ, Fulk GD, Boyne P. Clinically important differences for the upper-extremity Fugl-Meyer Scale in people with minimal to moderate impairment due to chronic stroke. Phys Ther. (2012) 92:791–8. doi: 10.2522/ptj.20110009
56. Chen R, Wu J, Shen X. A research on the minimal clinically important differences of Chinese version of the Fugl-Meyer motor scale [Article in Chinese]. Acta Univers Med Anhui. (2015) 50:519–22. doi: 10.19405/j.cnki.issn1000-1492.2015.04.025
57. Lee JA, Park SW, Hwang PW, Lim SM, Kook S, Choi KI, et al. Acupuncture for shoulder pain after stroke: a systematic review. J Altern Complement Med. (2012) 18:818–23. doi: 10.1089/acm.2011.0457
58. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. (2014) 120:482–503. doi: 10.1097/ALN.0000000000000101
59. Zhang GG, Yu C, Lee W, Lao L, Ren K, Berman BM. Involvement of peripheral opioid mechanisms in electroacupuncture analgesia. Explore. (2005) 1:365–71. doi: 10.1016/j.explore.2005.06.006
60. Li A, Zhang RX, Wang Y, Zhang H, Ren K, Berman BM, et al. Corticosterone mediates electroacupuncture-produced anti-edema in a rat model of inflammation. BMC Complement Altern Med. (2007) 7:27. doi: 10.1186/1472-6882-7-27
61. Lee JH, Jang KJ, Lee YT, Choi YH, Choi BT. Electroacupuncture inhibits inflammatory edema and hyperalgesia through regulation of cyclooxygenase synthesis in both peripheral and central nociceptive sites. Am J Chin Med. (2006) 34:981–8. doi: 10.1142/S0192415X06004454
62. Sekido R, Ishimaru K, Sakita M. Corticotropin-releasing factor and interleukin-1beta are involved in the electroacupuncture-induced analgesic effect on inflammatory pain elicited by carrageenan. Am J Chin Med. (2004) 32:269–79. doi: 10.1142/S0192415X04001928
63. Goldman N, Chen M, Fujita T, Xu Q, Peng W, Liu W, et al. Adenosine A1 receptors mediate local anti-nociceptive effects of acupuncture. Nat Neurosci. (2010) 13:883–8. doi: 10.1038/nn.2562
64. Xu Q, Yang JW, Cao Y, Zhang LW, Zeng XH, Li F, et al. Acupuncture improves locomotor function by enhancing GABA receptor expression in transient focal cerebral ischemia rats. Neurosci Lett. (2015) 588:88–94. doi: 10.1016/j.neulet.2014.12.057
65. Du Y, Shi L, Li J, Xiong J, Li B, Fan X. Angiogenesis and improved cerebral blood flow in the ischemic boundary area were detected after electroacupuncture treatment to rats with ischemic stroke. Neuro Res. (2011) 33:101–7. doi: 10.1179/016164110X12714125204317
66. Lin Y, Li Z, Fu J, Liu X. The systematic evaluation of acupuncture combined with rehabilitation training for the treatment of poststroke shoudler pain [Article in Chinese]. J Nurses Train. (2015) 30:1004–9. doi: 10.16821/j.cnki.hsjx.2015.11.011
67. Zhang CS, Tan HY, Zhang GS, Zhang AL, Xue CC, Xie YM. Placebo devices as effective control methods in acupuncture clinical trials: a systematic review. PLoS ONE. (2015) 10:e0140825. doi: 10.1371/journal.pone.0140825
68. Moroz A, Freed B, Tiedemann L, Bang H, Howell M, Park JJ. Blinding measured: a systematic review of randomized controlled trials of acupuncture. Evid Based Complement Alternat Med. (2013) 2013:708251. doi: 10.1155/2013/708251
69. Moher D, Hopewell S, Schulz KF, Montori V, Gotzsche PC, Devereaux PJ, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c869. doi: 10.1136/bmj.c869
Keywords: acupuncture, stroke, shoulder-hand syndrome, rehabilitation, systematic review
Citation: Liu S, Zhang CS, Cai Y, Guo X, Zhang AL, Xue CC and Lu C (2019) Acupuncture for Post-stroke Shoulder-Hand Syndrome: A Systematic Review and Meta-Analysis. Front. Neurol. 10:433. doi: 10.3389/fneur.2019.00433
Received: 10 December 2018; Accepted: 09 April 2019;
Published: 26 April 2019.
Edited by:
Valerie Moyra Pomeroy, University of East Anglia, United KingdomReviewed by:
Fang Zeng, Chengdu University of Traditional Chinese Medicine, ChinaCopyright © 2019 Liu, Zhang, Cai, Guo, Zhang, Xue and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Charlie Changli Xue, Y2hhcmxpZS54dWVAcm1pdC5lZHUuYXU=
Chuanjian Lu, bHVjaHVhbmppYW44ODhAdmlwLnNpbmEuY29t
†These authors have contributed equally to this work and are co-first-authors
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.