
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Neurol. , 11 March 2019
Sec. Stroke
Volume 10 - 2019 | https://doi.org/10.3389/fneur.2019.00206
This article is part of the Research Topic Tandem Extracranial-Intracranial Lesions in Acute Ischemic Stroke View all 7 articles
 François Zhu1
François Zhu1 Serge Bracard1,2René Anxionnat1,2Anne-Laure Derelle1Romain Tonnelet1Liang Liao1Gioia Mione3Lisa Humbertjean3Jean-Christophe Lacour3Gabriela Hossu2Mohammad Anadani4
Serge Bracard1,2René Anxionnat1,2Anne-Laure Derelle1Romain Tonnelet1Liang Liao1Gioia Mione3Lisa Humbertjean3Jean-Christophe Lacour3Gabriela Hossu2Mohammad Anadani4 Sébastien Richard3,5
Sébastien Richard3,5 Benjamin Gory1,2*
Benjamin Gory1,2*Introduction: Endovascular therapy has been shown to be an effective and safe treatment for tandem occlusion. The endovascular therapeutic strategies for tandem occlusions strokes have not been adequately evaluated and the best approach is still controversial. The TITAN (Thrombectomy in TANdem occlusions) registry was a result of a collaborative effort to identify the best therapeutic approach for acute ischemic stroke due to tandem lesion. In this review, we aim to summarize the main findings of the TITAN study and discuss the challenges of treatment for tandem occlusion in the era of endovascular thrombectomy.
Methods: A review of the data from the multicenter international observational and non-randomized TITAN registry was performed. The TITAN registry included acute ischemic stroke patients with tandem lesions (proximal intracranial occlusion and cervical carotid artery occlusion or stenosis>90%) who were treated with thrombectomy with or without carotid artery stenting.
Results: Prior intravenous thrombolysis and emergent cervical carotid stenting were associated with higher reperfusion (mTICI 2b-3 and mTICI 3) rates at the end of the intervention. Poor outcome did not occur more frequently after stenting than after conservative treatment of the cervical carotid lesion. Emergent carotid stenting with antithrombotic agents and intracranial thrombectomy yielded higher reperfusion rate and good outcome (90 day mRS 0–2) compared to other strategies (carotid artery stenting and thrombectomy without antithrombotic, angioplasty and thrombectomy, or thrombectomy alone). Pretreatment intravenous thrombolysis was not associated with increased risk of hemorrhagic complications. Likewise, periprocedural unfractionated heparin did not modify the efficacy and safety results. Etiology of carotid artery lesion (atherosclerosis vs. dissection) did not emerge as predictor of outcome or recanalization.
Conclusion: Emergent stenting of the cervical carotid lesion with antithrombotic agents in conjunction to thrombectomy appears to be the best treatment strategy for acute ischemic strokes with tandem lesions. These findings will be further investigated in the ongoing randomized controlled TITAN trial.
Tandem occlusions, defined as proximal anterior circulation intracranial occlusion and an ipsilateral cervical internal carotid artery (ICA) high-grade stenosis or occlusion, account for about 10–15% of acute ischemic strokes due to large-vessel occlusions (LVO). Data on the outcome of endovascular treatment of tandem occlusion is scarce (1), and tandem occlusion was among the exclusion criteria of most of the endovascular randomized trials (2, 3). Treatment effect of mechanical thrombectomy (MT) in patients with tandem occlusions was comparable to isolated intracranial occlusion in the HERMES meta-analysis (3); however, the optimal revascularization strategy of the extracranial lesion was not reported and many patients with non-severe stenosis (<70–80%) were included, especially in the MR CLEAN trial (4). Emergent carotid artery stenting in conjunction with intracranial MT is one of the therapeutic approaches for tandem occlusions. However, the safety of this approach is uncertain mainly due to the need for peri-procedural antithrombotic agents, which could increase the risk of hemorrhagic complications. In this review, we aimed to summarize the results of the TITAN study, focusing on the efficacy and safety of emergent carotid artery stenting in conjunction with mechanical thrombectomy approach, and to compare our results to the recent literature.
The TITAN (Thrombectomy In TANdem lesions) international collaboration pooled individual data of non-randomized thrombectomy databases from 18 comprehensive stroke centers for all consecutive anterior circulation tandem patients who underwent emergent thrombectomy between January 2012 and September 2016. Patients were included if they presented with acute ischemic stroke due to anterior circulation tandem occlusion and were treated with modern endovascular devices such as second-generation stent retriever and/or contact aspiration. Tandem lesion was defined as a proximal intracranial occlusion (distal ICA, and/or M1 and/or M2 segment of the middle cerebral artery) and an extracranial ICA lesion (complete occlusion or stenosis ≥90% North American Symptomatic Carotid Endarterectomy Trial).
Treatment of the extracranial ICA lesion was left at the discretion of the operators. Four therapeutic strategies for the cervical steno-occlusive lesion were possible: (1) acute stenting with antithrombotic agents, (2) acute stenting without antithrombotic agents, (3) acute balloon angioplasty without stenting, and (4) no treatment. Intravenous thrombolysis was administered for eligible patients according to the international guidelines. Intravenous sedation and general anesthesia were permitted.
All patients included had a computed tomography or magnetic resonance imaging at 24 h after treatment onset to assess for hemorrhagic complications. The local ethics committees approved the use of patient data for the retrospective analysis and waived the need for patient consent. All data were retrospectively collected and scored by one neuro-interventionist in each center.
All studies primary outcome was the good outcome defined as a 90 day modified Rankin Scale (mRS) 0–2. Secondary outcomes included successful reperfusion defined as modified Thrombolysis In Cerebral Infarction (mTICI) score 2b-3 (5), complete reperfusion (mTICI 3), all-cause mortality at 90 day, any procedural related complications, any intracranial hemorrhage (ICH), and symptomatic ICH. Cerebral hemorrhages were classified as hemorrhagic infarction (HI) or parenchymal hematoma (PH) according to the European Cooperative Acute Stroke Study II criteria (6). Symptomatic ICH (sICH) was defined as any parenchymal hematoma, subarachnoid hemorrhage, or intraventricular hemorrhage associated with worsening of the National Institutes of Health Stroke Scale (NIHSS) score by 4 points or more.
Among the 295 included patients, the etiology of the cervical ICA lesion was atherosclerosis in 230 (78%) patients and dissection in 65 (22%) patients (7). Interestingly, the etiology of the cervical ICA lesion (atherosclerosis vs. dissection) did not impact the final reperfusion rates or clinical outcomes (7). This finding suggests that the etiology of the extracranial disease should not influence the treatment strategy.
Papanagiotou et al. compared four therapeutic strategies of the cervical steno-occlusive lesion (8). Treatment of the cervical ICA lesion in conjunction with intracranial mechanical thrombectomy led to a higher rate of successful reperfusion compared to thrombectomy without ICA treatment (79.4 vs. 60.2%; OR = 2.04; 95% CI = 1.18–3.51; P = 0.011), with or without prior thrombolysis. Although was not statistically significant, the rate of good outcome (90 day mRS 0-2) was higher in patients who received cervical ICA treatment with intracranial mechanical thrombectomy compared to those who received mechanical thrombectomy alone without ICA lesion treatment (53.4 vs. 41.0%; OR = 1.42; 95%CI = 0.83–2.41; P = 0.20) (8). In addition, there was no significant difference in the rate of 90 day mortality (11.4 vs. 17.1%; OR = 0.56; 95%CI = 0.29–1.09; P = 0.086), or sICH (4.6 vs. 4.6%; OR = 1.23; 95%CI = 0.40–3.72; P = 0.72) between the two groups after pre-specified adjustments (8).
A significantly higher rate of successful reperfusion in the carotid stenting and antiplatelet group compared to the thrombectomy alone group was observed (83.1 vs. 60.2%; OR = 2.66; 95% CI = 1.38–5.10; P = 0.003) (Table 1) (8). Likewise, complete reperfusion rate was higher in the former group (41.2 vs. 23.2%; OR = 1.91; 95% CI = 1.08–3.40; P = 0.026). In addition, carotid stenting with antithrombotic appeared superior to stenting without antithrombotic and balloon angioplasty groups, although these differences were not statistically significant (8).
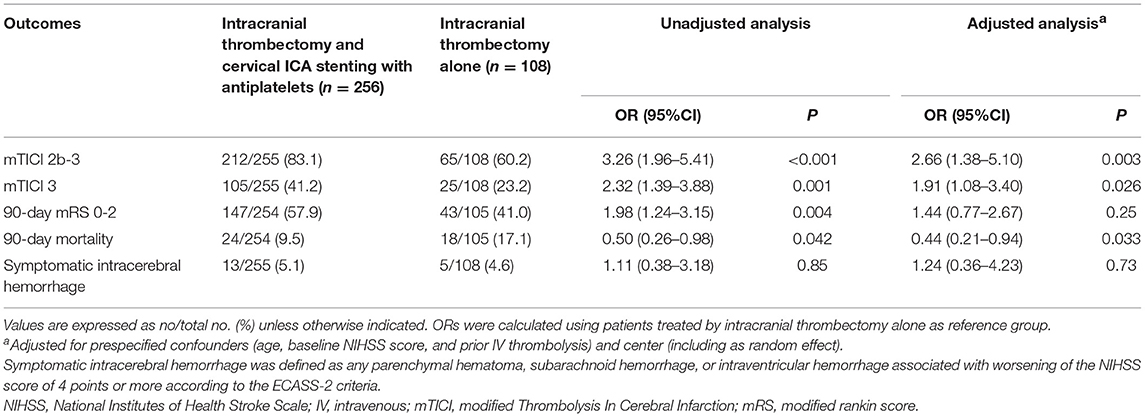
Table 1. Efficacy and safety outcomes between patients treated by intracranial thrombectomy alone vs. those treated by intracranial thrombectomy and cervical carotid artery stenting with antiplatelets [from Papanagiotou et al. (8)].
Similar results were found for clinical outcomes at 90 days with a higher rate of good outcome in the setting of ICA stenting with antithrombotic agents compared to thrombectomy alone (57.9 vs. 41.0%; unadjusted OR = 1.98; 95% CI = 1.24–3.15; P = 0.004) (8). However, this difference became non-significant after adjusting for pre-specified confounders (OR = 1.44; 95% CI = 0.77–2.67; P = 0.25) (Table 1). In addition, good outcome was achieved more in the stenting with antithrombotic group than the stenting without antithrombotic, and balloon angioplasty groups; however, the difference did not reach statistical significance which likely related to a small sample size in the latter groups (8).
In case of acute stenting, mortality within 90 days was significantly lower (9.5 vs. 17.1%; OR = 0.50; 95% CI = 0.26–0.98; P = 0.033) compared to intracranial thrombectomy alone (8). Predictors of 90 day mortality in the TITAN cohort were age (OR = 1.05; 95% CI = 1.02–1.08; P = 0.001), current smoker (OR = 1.05; 95% CI = 1.02–1.08; P = 0.001), NIHSS scores (OR = 1.14; 95%CI = 1.07–1.22; P < 0.001), ASPECTS scores (OR = 0.75; 95% CI = 0.62–0.89; P = 0.001), and prior thrombolysis (OR = 0.48; 95% CI = 0.25–0.90; P = 0.022) (8).
Of the 267 patients with available data on hemorrhagic transformation, there were 66% (24.7%) of HI (31 HI1 and 35 HI2) and 38 (14.2%) of PH (24 PH1 and 14 PH2) (9). Intracranial and extracranial ICA occlusions, diabetes mellitus, no prior use of IVT were predictors of hemorrhagic transformation (9). Interestingly, no impact of thrombolysis on different outcomes was observed in our study. Administering one or even two antiplatelet drugs was associated with a lower risk of sICH (Figure 1A) (9).
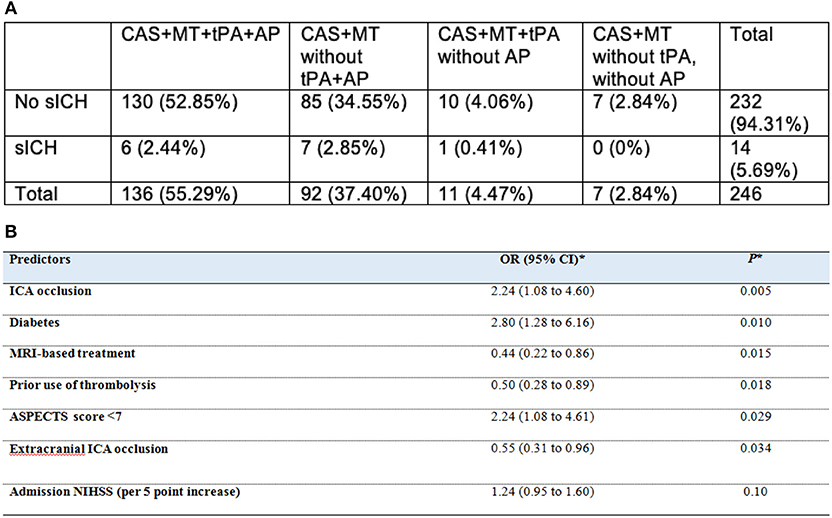
Figure 1. (A) sICH prevalence according to the endovascular and pharmacological strategy. CAS, Carotid Acute Stenting; MT, Mechanical Thrombectomy; tPA, IV thrombolysis; AP, Periprocedural use of antiplatelet. (B) Multivariable regression analysis of predictors of any hemorrhagic transformation (from Zhu et al. (9)). *Calculated after handling missing data by multiple imputations using a backward-stepwise logistic model including all univariate predictors at P < 0.20. ASPECTS, Alberta Stroke Program Early CT Score; CI, confidence interval; ICA, internal carotid artery; IV, intravenous; MRI, magnetic resonance imaging; NIHSS, National Institutes of Health Stroke Scale; OR, odds ratio.
In TITAN, periprocedural heparin use during endovascular therapy of patients with tandem occlusion was not associated with a better clinical outcome or a higher risk of intracerebral hemorrhagic complications (Zhu et al., submitted). Acute ICA stenting and antiplatelet administration were not predictors of HI and PH within 24 h in TITAN registry (Figure 1B) (9).
We found an association between intravenous thrombolysis (IVT) and successful reperfusion when we included all patients in the TITIAN registry regardless of the ICA treatment strategy (OR, 1.47; 95% CI, 1.01–2.12) (10). Interestingly, when only patients treated with carotid artery stenting included, we did not find association between IVT and functional outcome or more importantly safety outcomes (11).
Among the patients from the TITAN cohort, order of treatment of intracranial occlusion or cervical occlusion led to a similar rate of successful reperfusion (12). As expected, treating the intracranial occlusion first was associated with faster time from puncture to reperfusion; however, the order of treatment was not associated with clinical outcomes (12).
The main result of the TITAN collaboration is that mechanical thrombectomy and emergent carotid stenting with antiplatelet therapy seems to be the most effective therapeutic approach for tandem lesions in acute ischemic stroke, even in patients who received prior intravenous thrombolysis. A similar association between acute stenting and successful reperfusion in stroke patients with tandem lesion treated with thrombectomy was reported by Sadeh-Gonik et al. in a meta-analysis including a total of 590 patients pooled from 13 case series (13).
The rate of hemorrhagic complications after tandem occlusion endovascular treatment seems similar to the rate of hemorrhagic complications after isolated intracranial MT. In the aforementioned meta-analysis, the reported rates of all hemorrhage and sICH were 24 and 8%, respectively (13), whereas the rate of HI was 23% and the rate of PH was 13% in THRACE (THRombectomie des Artères CErebrales) trial (2). Similar safety outcomes for acute ICA stenting were found by Behme et al. in a German multicenter study (14). Our results parallel those from STRATIS (Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke) registry, which included 147 patients with tandem occlusions, treated with Solitaire device with or without carotid artery stenting (15).
Despite the encouraging results of the abovementioned studies demonstrating high successful reperfusion rate and good outcome with carotid artery stenting, the need of antithrombotic agents in the acute phase makes it a less appealing approach prompting some experts to recommend alternative approaches such as MT alone or angioplasty without acute stenting (16). Two retrospective studies demonstrated a high successful reperfusion rate and good outcome with angioplasty or MT alone (17–19); however, these studies suffered a small sample size. With angioplasty or MT alone approach, antithrombotic agents are often not required; therefore, the risk of hemorrhagic transformation is of lesser concern. As a result of inconsistent literature and lack of consensus, the best strategy remains unknown highlighting the need for randomized controlled trial. These precautionary approaches obviate the theoretical hemorrhagic risks due to the antiplatelets administration. Otherwise, these analyses did not take into account cervical occlusion as treatment of extracranial disease, which appears to be effective to prevent early embolic recurrence (20) and better reperfusion rates. Then, should we consider acute carotid stenting as the best strategy? And if yes, is “the best is the enemy of the good”? Actually no deleterious effect of carotid stenting has been already proved (19). To date, as Blassiau et al. said, choice of strategy “may vary between institution and physicians and adapts as a result of personal experience” (17), though the absence of consensus. This debate highlights the need of a randomized controlled trial for tandem lesions population.
Bridging with intravenous thrombolysis prior to thrombectomy remains the standard of care in eligible patients (21). Bridging approach was repeatedly shown to be superior to MT alone (22, 23). TITAN results are in line with previous studies and showed that intravenous thrombolysis prior to endovascular therapy is safe and may be helpful in patients with tandem occlusions.
We learnt from the cardiology literature that antiplatelet therapy is essential in case of stenting to prevent in-stent thrombosis. In case of acute stroke, the decision on best antithrombotic treatment is more complex, mainly due to the risk of hemorrhagic complications. Despite the extensive literature addressing the best long-term antiplatelet therapy (24), the best antiplatelet therapy in the acute phase following endovascular therapy is unknown; especially in case of carotid artery stenting. A recent systematic review found possible increased risk of sICH with periprocedural use of antiplatelets with neutral effect on the functional outcome (25).
In the TITAN study, we did not find an increased risk of hemorrhage with periprocedural antithrombotic use; on the contrary, patients who were treated with carotid stenting and antithrombotic agents performed better than those who did not receive periprocedural antithrombotic agents.
Heparin is commonly used in endovascular therapy and was found to be associated with good outcome in a post-hoc analysis of TREVO-2 trial (26). We did not find a significant association between periprocedural heparin use and clinical or safety outcomes. Heparin use theoretically reduces the risk of re-occlusion and distal emboli during endovascular therapy (27); unfortunately, the data regarding re-occlusion or distal emboli was not available in the TITAN registry, which may explain the lack of benefit of heparin in our registry. The ongoing randomized controlled trial MR CLEAN MED (Multicenter Randomized Clinical trial of Endovascular treatment for Acute ischemic stroke in the Netherlands investigating the effect of periprocedural MEDication) (28) will further evaluate the risks and benefit of periprocedural antithrombotic with aim to identify the best periprocedural medications.
Concerning the order to treat, treating the cervical lesion first “neck-first” provides accessibility to the distal occlusion, whereas treating the intracranial occlusion first “head-first” has advantage of faster reperfusion, but theoretically increase the risk of distal emboli. Studies comparing the two approaches provided conflicting results. Meta-analysis found no difference between the two approaches (19); on the contrary, a retrospective analysis of 171 tandem stroke patients found that patients who were treated with “head-first” approach performed better than those treated with “neck-first” approach (29).
Despite the large sample size and multi-center design, the TITIAN registry suffered from multiple limitations. First, the observational and non-randomized design has known methodological shortcomings. Second, there was no core-lab assessment of brain imagings, which may have introduced bias to our results. Third, despite handling the missing data with multiple imputations, the risk of bias is still a concern. Finally, treatment strategy was left to the interventionist discretion, and drug dosages and administration times were unknown, which likely subject to selection bias.
Emergent stenting of the cervical carotid artery steno-occlusion lesion with periprocedural antithrombotic agents and intracranial mechanical thrombectomy was associated with favorable clinical and radiological outcomes. No safety concerns were reported in the TITAN collaboration, especially concerning hemorrhagic transformation risks. However, due to several discordances in the literature, further randomized controlled trials are warranted, as the on-going French multicenter prospective randomized TITAN trial.
FZ and BG substantial contribution to the conception and design of the work, drafting the work, final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. SB, RA, A-LD, RT, LL, GM, LH, J-CL, GH, MA, and SR substantial contributions to the interpretation of data for the work, revising the work critically for important intellectual content, final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Sivan-Hoffmann R, Gory B, Armoiry X, Goyal M, Riva R, Labeyrie PE, et al. Stent-Retriever thrombectomy for acute anterior ischemic stroke with tandem occlusion: a systematic review and meta-analysis. Eur Radiol. (2017) 27:247–54. doi: 10.1007/s00330-016-4338-y
2. Bracard S, Ducrocq X, Mas JL, Soudant M, Oppenheim C, Moulin T, et al. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): a randomised controlled trial. Lancet Neurol. (2016) 15:1138–47. doi: 10.1016/S1474-4422(16)30177-6
3. Goyal M, Menon BK, van Zwam WH, Dippel DWJ, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet Lond Engl. (2016) 387:1723–31. doi: 10.1016/S0140-6736(16)00163-X
4. Berkhemer OA, Fransen PSS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. (2015) 372:11–20. doi: 10.1056/NEJMoa1411587
5. Zaidat OO, Yoo AJ, Khatri P, Tomsick TA, Kummer R von, Saver JL, et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement. Stroke. (2013) 44:2650–63. doi: 10.1161/STROKEAHA.113.001972
6. Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet Lond Engl. (1998) 352:1245–51. doi: 10.1016/S0140-6736(98)08020-9
7. Gory B, Piotin M, Haussen DC, Steglich-Arnholm H, Holtmannspötter M, Labreuche J, et al. Thrombectomy in acute stroke with tandem occlusions from dissection versus atherosclerotic cause. Stroke. (2017) 48:3145–8. doi: 10.1161/STROKEAHA.117.018264
8. Papanagiotou P, Haussen DC, Turjman F, Labreuche J, Piotin M, Kastrup A, et al. Carotid stenting with antithrombotic agents and intracranial thrombectomy leads to the highest recanalization rate in patients with acute stroke with tandem lesions. JACC Cardiovasc Interv. (2018) 11:1290–9. doi: 10.1016/j.jcin.2018.05.036
9. Zhu F, Labreuche J, Haussen DC, Piotin M, Steglich-Arnholm H, Taschner C, et al. Hemorrhagic transformation after thrombectomy for tandem occlusions. Stroke. (2018) 50:516–9. doi: 10.1161/STROKEAHA.118.023689
10. Gory B, Haussen DC, Piotin M, Steglich-Arnholm H, Holtmannspötter M, Labreuche J, et al. Impact of intravenous thrombolysis and emergent carotid stenting on reperfusion and clinical outcomes in patients with acute stroke with tandem lesion treated with thrombectomy: a collaborative pooled analysis. Eur J Neurol. (2018) 25:1115–20. doi: 10.1111/ene.13633
11. Anadani M, Spiotta A, Alawieh A, Turjman F, Piotin M, Haussen DC, et al. Emergent carotid stenting plus thrombectomy after thrombolysis in tandem strokes: analysis of the TITAN registry. Stroke. (Accepted).
12. Haussen DC, Turjman F, Piotin M, Labreuche J, Steglich-Arnholm H, Holtmannspötter M, et al. Head or neck first? Speed and rates of reperfusion in thrombectomy for tandem large vessel occlusion strokes. Interv Neurol. (2019) 8:92–100. doi: 10.1159/000496292
13. Sadeh-Gonik U, Tau N, Friehmann T, Bracard S, Anxionnat R, Derelle A-L, et al. Thrombectomy outcomes for acute stroke patients with anterior circulation tandem lesions: a clinical registry and an update of a systematic review with meta-analysis. Eur J Neurol. (2018) 25:693–700. doi: 10.1111/ene.13577
14. Behme D, Mpotsaris A, Zeyen P, Psychogios MN, Kowoll A, Maurer CJ, et al. Emergency stenting of the extracranial internal carotid artery in combination with anterior circulation thrombectomy in acute ischemic stroke: a retrospective multicenter study. Am J Neuroradiol. (2015) 36:2340–5. doi: 10.3174/ajnr.A4459
15. Jadhav AP, Zaidat OO, Liebeskind DS, Yavagal DR, Haussen DC, Hellinger FR, et al. Emergent management of tandem lesions in acute ischemic stroke. Stroke. (2018) 50:428–33. doi: 10.1161/STROKEAHA.118.021893
16. Behme D, Molina CA, Selim MH, Ribo M. Emergent carotid stenting after thrombectomy in patients with tandem lesions. Stroke. (2017) 48:1126–8. doi: 10.1161/STROKEAHA.117.016182
17. Blassiau A, Gawlitza M, Manceau P-F, Bakchine S, Serre I, Soize S, et al. Mechanical thrombectomy for tandem occlusions of the internal carotid artery—results of a conservative approach for the extracranial lesion. Front Neurol. (2018) 9:928. doi: 10.3389/fneur.2018.00928
18. Akpinar CK, Gürkaş E, Aytac E. Carotid angioplasty-assisted mechanical thrombectomy without urgent stenting may be a better option in acute tandem occlusions. Interv Neuroradiol J Peritherapeutic Neuroradiol Surg Proced Relat Neurosci. (2017) 23:405–11. doi: 10.1177/1591019917701113
19. Wilson MP, Murad MH, Krings T, Pereira VM, O'Kelly C, Rempel J, et al. Management of tandem occlusions in acute ischemic stroke - intracranial versus extracranial first and extracranial stenting versus angioplasty alone: a systematic review and meta-analysis. J Neurointerv Surg. (2018) 10:721–8. doi: 10.1136/neurintsurg-2017-013707
20. Labeyrie M-A, Ducroux C, Civelli V, Reiner P, Cognat E, Aymard A, et al. Endovascular management of extracranial occlusions at the hyperacute phase of stroke with tandem occlusions. J Neuroradiol. (2017) 45:196–201. doi: 10.1016/j.neurad.2017.10.003
21. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the american heart association/american stroke association. Stroke. (2018) 49:e46–110. doi: 10.1161/STR.0000000000000158
22. Gariel F, Lapergue B, Bourcier R, Berge J, Barreau X, Mazighi M, et al. Mechanical thrombectomy outcomes with or without intravenous thrombolysis. Stroke. (2018) 49:2383–90. doi: 10.1161/STROKEAHA.118.021500
23. Mistry EA, Mistry AM, Nakawah MO, Chitale RV, James RF, Volpi JJ, et al. Mechanical thrombectomy outcomes with and without intravenous thrombolysis in stroke patients: a meta-analysis. Stroke. (2017) 48:2450–6. doi: 10.1161/STROKEAHA.117.017320
24. Verdoia M, Schaffer A, Barbieri L, Montalescot G, Collet JP, Colombo A, et al. Optimal duration of dual antiplatelet therapy after DES implantation: a meta-analysis of 11 randomized trials. Angiology. (2016) 67:224–38. doi: 10.1177/0003319715586500
25. van de Graaf RA, Chalos V, Del Zoppo GJ, van der Lugt A, Dippel DWJ, Roozenbeek B. Periprocedural antithrombotic treatment during acute mechanical thrombectomy for ischemic stroke: a systematic review. Front Neurol. (2018) 9:238. doi: 10.3389/fneur.2018.00238
26. Winningham MJ, Haussen DC, Nogueira RG, Liebeskind DS, Smith WS, Lutsep HL, et al. Periprocedural heparin use in acute ischemic stroke endovascular therapy: the TREVO 2 trial. J Neurointerventional Surg. (2018) 10:611–614. doi: 10.1136/neurintsurg-2017-013441
27. Nahab F, Kass-Hout T, Shaltoni HM. Periprocedural antithrombotic strategies in acute ischemic stroke interventional therapy. Neurology. (2012) 79(13 Suppl. 1):S174–81. doi: 10.1212/WNL.0b013e31826959af
28. European Union Clinical Trials Register. Identifier: 2017-001466-21, Multicenter Randomized CLinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands. The Effect of Periprocedural MEDication: Heparin, Antiplatelet Agents, Both or Neither. Available online at: https://www.clinicaltrialsregister.eu/ctr-search/trial/2017-001466-21/NL London: European Union Clinical Trials Register.
Keywords: tandem occlusion, stroke, carotid stenting, endovascular treatment, thrombectomy, emergent stenting in tandem occlusion
Citation: Zhu F, Bracard S, Anxionnat R, Derelle A-L, Tonnelet R, Liao L, Mione G, Humbertjean L, Lacour J-C, Hossu G, Anadani M, Richard S and Gory B (2019) Impact of Emergent Cervical Carotid Stenting in Tandem Occlusion Strokes Treated by Thrombectomy: A Review of the TITAN Collaboration. Front. Neurol. 10:206. doi: 10.3389/fneur.2019.00206
Received: 24 September 2018; Accepted: 18 February 2019;
Published: 11 March 2019.
Edited by:
Johannes Kaesmacher, Technische Universität München, GermanyReviewed by:
Muhib Khan, Michigan State University, United StatesCopyright © 2019 Zhu, Bracard, Anxionnat, Derelle, Tonnelet, Liao, Mione, Humbertjean, Lacour, Hossu, Anadani, Richard and Gory. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Benjamin Gory, Yi5nb3J5QGNocnUtbmFuY3kuZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.