 Brian Trummer
Brian Trummer Dietrich Haubenberger2
Dietrich Haubenberger2 Craig Blackstone
Craig Blackstone
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 21 December 2018
Sec. Movement Disorders
Volume 9 - 2018 | https://doi.org/10.3389/fneur.2018.01017
This article is part of the Research Topic Hereditary Spastic Paraplegias: Current Knowledge and Future Perspective View all 6 articles
Hereditary spastic paraplegias (HSPs) are a large group of genetically-diverse neurologic disorders characterized clinically by a common feature of lower extremity spasticity and gait difficulties. Current therapies are predominantly symptomatic, and even then usually provide inadequate relief of symptoms. Going forward, HSP therapeutics development requires a systematic analysis of quantifiable measures and tools to assess treatment response. This review summarizes promising therapeutic targets, assessment measures, and previous clinical trials for the HSPs. Oxidative stress, signaling pathways, microtubule dynamics, and gene rescue/replacement have been proposed as potential treatment targets or modalities. Quantitative evaluation of pre-clinical rodent HSP models emphasize rotarod performance, foot base angle, grip strength, stride length, beam walking, critical speed, and body weight. Clinical measures of HSP in humans include 10-m gait velocity, the Spastic Paraplegia Rating Scale (SPRS), Ashworth Spasticity Scale, Fugl-Meyer Scale, timed up-and-go, and the Gillette Functional Assessment Questionnaire. We conducted a broad search for past clinical trials in HSPs and identified trials that investigated pharmacological agents including atorvastatin, gabapentin, L-threonine, botulinum toxin, dalfampridine, methylphenidate, and baclofen. We provide recommendations for future HSP treatment directions based on these prior research experiences as well as regulatory insight.
Hereditary spastic paraplegias (HSPs) arise from mutations in a large number of different genes, encompassing autosomal dominant, autosomal recessive, X-linked, and mitochondrial inheritances; de novo mutations have also been described. Together, these conditions coalesce around a common phenotype comprising a progressive spastic gait disturbance, with or without additional clinical features. HSPs occur in ~1.8 per 100,000 people on average globally, but this prevalence can vary significantly across different populations (1). Pathologically, spasticity in the lower extremities arises from length-dependent degeneration and/or abnormal development of corticospinal axons, which can extend to 1 m in length (2).
Most HSPs have been systematically categorized using the prefix SPG followed by a number—with each number indicating a different genetic locus—in order of identification (SPG1-80, plus others). While these genes encode different proteins, the gene products tend to distribute into a relatively small number of cellular localizations and functions, comprising defects in myelination, mitochondrial function, organelle distribution and morphology, axon pathfinding, axon transport, bone morphogenetic protein signaling, and lipid metabolism. The three most common autosomal dominant forms—SPG4, SPG3A, and SPG31—account for about half of all cases and result from mutations in proteins that bind one another and shape the tubular endoplasmic reticulum (ER). The most common autosomal recessive forms—SPG11 and SPG15—are due to loss-of-function mutations in large proteins that bind one another and function in endolysosomal trafficking and autophagic pathways (3–11).
Previously published HSP therapeutic studies were searched for in PubMed using the terms “hereditary spastic paraplegia” and “therapeutic,” which also helped to identify HSP clinical trials. Further identification of HSP clinical trials was conducted through PubMed, utilizing the search terms “hereditary spastic paraplegia” and “hereditary spastic paraparesis” with an article-type filter “clinical trial.” Within PubMed, we also utilized the search term “hereditary spastic paraplegia phase.” In clinicaltrials.gov, we searched for “hereditary spastic paraplegia.” Studies employing interventional therapies that were specifically examined in the HSP population (as assessed by author BT) were also selected for review. Clinical assessment tools are assembled from these prior trials later in this review.
To optimize HSP clinical trial design in the future, it is sensible to consider already published preclinical treatment strategies. Oxidative stress is one potential therapeutic target that has been explored for SPG4, the most common form of HSP. Indeed, zebrafish treated with 2′,7′-dichlorofluorescein diacetate (DCF-DA), used to measure oxidative stress, have increased fluorescence when treated with a morpholino that depletes the SPG4 protein spastin (3). FDA-approved drugs that inhibit oxidative stress and ER stress—such as guanabenz, methylene blue, and N-acetyl-cysteine—have been tested in various SPG4 animal models (C. elegans, Drosophila, and zebrafish), with some success in improving movement (3). Mitochondrial fission has been also targeted, and inhibitors of the mitochondrial fission GTPase DRP1, specifically mdivi-1, improve neurite outgrowth in induced pluripotent stem cells derived from SPG15 and SPG48 patients (4).
A third target for SPG4 is microtubule dynamics more generally, with both microtubule destabilizing and stabilizing agents being investigated (5). This target seems particularly relevant for SPG4, since spastin functions as a microtubule-severing ATPase. Olfactory neurosphere-derived cells from SPG4 patients show altered levels of acetylated α-tubulin, a marker of stabilized microtubules; tubulin-binding drugs (0.5 nM paclitaxel, 0.5 nM vinblastine, 2 nM epothilone D, and 10 μM noscapine) restore acetylated α-tubulin levels in SPG4 patient-derived cells (6). One group has been developing a robotic method to assay plate wells for the identification of drugs that impact fast transport of mitochondria along microtubules, and they have found that nocodazole accomplishes this task by disrupting microtubules (7). In a Drosophilia model for SPG4 cold temperature, which destabilizes microtubules, rescues phenotypes in spastin mutant flies, when chilled during development as well as in adulthood (8).
A fourth mechanism under preclinical study for a variety of HSPs where loss-of-function or haploinsufficiency are postulated is gene rescue. For SPG4, lentiviral expression of M1 or M87 isoforms of spastin (generated via the use of different translational start sites) rescued pathogenic defects in SPG4 neurons, reducing neuronal swelling and increasing length of axons (9). In a knock out mouse model of SPG7, adeno-associated virus-mediated intramuscular delivery of the Spg7 gene product paraplegin improved performance as assessed by rotarod (10). An alternative approach to SPG4 spastin rescue involves knocking down miRNAs that negatively regulate spastin expression, such as MiR-96 and miR-182 (11). Increasing levels of transcription factors such as SOX11 and NRF1 that positively regulate spastin has also been proposed, particularly for NRF1, as elephants with long corticospinal tracts have lost the SOX11 site, which has been replaced by four putative NRF1 binding sites (11).
Additionally, for some autosomal recessive forms of HSP such as SPG11, SPG15, and SPG48, which are characterized by dysfunction in autophagy and endolysosomal pathways, compounds that induce autophagy have been suggested as treatment, such as carbamazepine, rapamycin, among others (12). SPG5, which results from an accumulation of 27-hydroxycholesterol (27-OHC), has been evaluated for responses to cholesterol-lowering drugs (13–15).
A variety of animal models for different HSPs, as well as protocols to test physical function in these animals, have been developed. Morpholinos against 14 HSP human genes in zebrafish impact motor neurons and impair locomotion (16). Rodent models have also been developed, along with ways to assess physical function.
One popular measure for rodent models is rotarod performance. Spg7−/− mice were placed on a rotating rod with starting speed of 4 rpm, achieving a final speed of 40 rpm in 5 min, with 3–4 trials a day; animals were permitted on the rod for a maximum of 600 s (17). Spg20−/− mice at 4–7 months of age were assessed on a rotarod treadmill 3.2 cm in diameter and monitored in three independent trials separated by 15 min for recovery, increasing from 4 to 40 rpm for a maximum of 300 s (18).
A second measure developed to assess mouse HSP models is the foot base angle. Reep1−/− knockout mice had the change in foot-base angle over time measured (19). In Spg15 knockout mice at 8 months of age, there was no difference in body weight or gait abnormality in the knockout mice, but at 12 months knockout mice had a progressive gait disorder quantified by discernable foot base angle changes; by 16 months foot-base angle was reduced to 50° as compared to 75° in wild-type mice (20).
A third measure to assess HSP mouse models is grip strength. In Spg20−/− mice, grip strength was measured using a Bioseb meter assessing the maximum force exerted by hind limbs (18).
A fourth measure is beam walking. In a Spg21 knockout mouse model, male mice from 2 to 12 months were placed on a beam 80 cm long and 1 cm wide; time to walk across the elevated beam was recorded along with the number of foot slips (counted with a tally counter) (21). An alternative measure for beam walking is the number of times a mouse falls off a beam, as used in a Spg15 knockout mouse model (20).
A fifth measure is the determination of critical speed. Critical speed is measured by running mice on a treadmill with a shock grid delivering 0.2 mA, placed 10 cm from the rear of the cell, to provide a stimulus to make the animals run. There are four runs leading to exhaustion, and a single trial performed each day over 4 days with mice running 18–41 m/min, limited to 45 min or exhaustion as defined by a total number of 50 shocks. Distance (m) is plotted on the y-axis and time(s) on x-axis, and the slope is the critical speed (22). In 4, 12, and 22-month old SPG4 mice, a statistically significant 35% decrease in critical speed was described in mutant mice from 15 to 24 months age, compared to a 17% decrease in control mice (23).
A clinical rating scale that has been developed specifically for HSPs is the clinical Spastic Paraplegia Rating Scale (SPRS), which comprises 13 items to assess the level of spasticity and shows high internal consistency (24). Changes in SPRS (24, 25) were used as a secondary outcome in a clinical trial investigating the efficacy of botulinum toxin type-A for HSP (26). A subset of this SPRS scale has been used to generate a “spastic subscore,” which is the sum of point values for spasticity of hip adductor muscles, weakness of hip abduction, spasticity of knee flexion and weakness of foot dorsiflexion (27). Some trials have used a 10-m maximum or comfortable gait velocity as a primary outcome measure. Clinicians measured the change in 10-m maximum gait velocity (28, 29) 8 weeks after botulinum toxin type-A injections, taking the average of three trials (26). The Ashworth spasticity scale (30) has been commonly used in clinical trials of HSP. One group has used the walking component of the Gillette Functional Assessment Questionnaire (31) in a baclofen pump trial (32). Also mentioned in single trials are: the Fugl-Meyer scale, which assesses motor function, some sensation, balance and joint function (33); timed up-and-go testing, which tests time to get up from an arm chair, walk 3 m, turn, walk back and sit down (34); multiple sclerosis (MS) impairment scale, which includes a neurological exam and limited neuropsychological tests (35); the Medical Research Council (MRC) scale; brief pain inventory; and fatigue scales. A simple 4 stage rating scale has also been proposed: (i) mild symptoms walking without an aid; (ii) walking without aid but unable to run; (iii) walking with aid; and (iv) wheelchair dependent (36). This 4-stage rating scale was found to predict SPRS scores with p < 0.0001 and was inversely related with SF-36 scale at −0.248 with p = 0.032 (37).
Genetic testing has dramatically advanced, and testing patients with physical findings suspicious for HSP is increasingly available at reasonable cost. Currently, >50 genes can be readily tested using comprehensive, commercial HSP panels. A number of exploratory laboratory measures can be pursued to further knowledge of specific variants of HSP. For instance, SPG5 patients with mutations in the CYP7B1 enzyme have a buildup of toxic cholesterol products. Measuring 25-OHC and 27-OHC, as well as their ratio to cholesterol, is 100% sensitive and specific for SPG5 as compared to normal controls (14).
Preliminary work has emphasized miRNAs, specifically miR-140 and miR-691 for SPG31 (38) as well as miR-638 (host gene DNM2) (39). One group has described an antibody against amino acid residues 244-326 of MUDENG (mu-2-related death-inducing gene, MuD) that may play a role in endosomal protein trafficking, as a biomarker for HSP (40). Another group studying SPG10 obtained skin biopsy samples from the distal leg, reporting a patient with decreased and fragmented staining with anti-synaptophysin, and on electronic microscopy, decreased number of pre-synaptic vesicles (41).
Imaging modalities are specific to certain SPGs and not generalizable to all HSPs. One group found that 3 patients with SPG5 had diffuse white matter hyperintensities in the centrum semiovale and corona radiata, while sparing the corpus callosum (42). Additionally, many SPG11 and SPG15 patients have a thin corpus callosum and “ears of the lynx” white matter changes on brain MRI (43). In a study of 3 patients with SPG5, PET scans using 18F-fluoro-deoxyglucose showed cerebellar hypometabolism in one of the patients, predominantly affecting the vermis (42). SPG11 patients with paraparesis had decreased paracentral and thalamic metabolism (43). Utilization of proton magnetic resonance spectroscopy has found that in SPG4, the choline/creatine (Cho/Cr) ratio in the motor cortex was significantly lower than in controls (p = 0.047), possibly indicating reduced membrane turnover or else cell loss (44).
In SPG54 due to mutation in DDHD2, a pathologic spectral lipid peak at 1.3 ppm was identified. The DDHD2 gene product normally hydrolyzes phosphatidic acid and has activity toward other phospholipids including phosphatidylethanolamine, acting typically at the ER-Golgi intermediate compartment (45). Finally, in patients with complicated SPG7, optical coherence tomography (OCT) has been useful in finding retinal nerve fiber layer thinning, likely due to mitochondrial defects (46). All SPG7 patients had pathologic OCT, but only 40% had decreased visual acuity and 50% had optic disc pallor, making OCT useful for detecting subclinical optic neuropathy in SPG7 patients (47).
HSP patients with an increased score on the Ashworth spasticity scale have a shorter cortical silent period relative to normal controls (48). This is a measure of supraspinal or intracortical inhibitory pathways, and not degeneration in the corticospinal tract axons (48). Other measures that were significantly different between HSP and controls were tibialis anterior motor threshold, total motor conduction time (TMCT), central motor conduction time (CMCT), and motor-evoked potential (MEP) amplitude; however, these did not correlate with the Ashworth spasticity scale (48). One study found 37% of HSP patients had prolonged CMCT to lower extremities, and CMCT to the legs correlated with total SPRS score (r = 0.176; p < 0.028) and spastic subscore (r = 0.241, p < 0.005); pathologic CMCT to legs correlated with disease duration (r = 0.231; p < 0.009) (27). SPG4 CMCTs were normal in both arms (5.1 ± 1.5 ms) and legs (14.1 ± 3.9 ms), while non-SPG4 HSP patients' CMCTs were significantly longer in arms (6.9 ± 2.6 ms) and legs (18.2 ± 7.3 ms). Across subgroups of SPG4 patients, CMCT to legs in those with missense mutations were shorter (10.5 ± 1.3 ms) than in those with SPG4 due to premature stop codons, exon deletions, or splice site mutations (13.9 ± 3.7 ms) (27).
A number of clinical trials of pharmacological agents have been tested in HSPs, as outlined in Table 1 and described below.
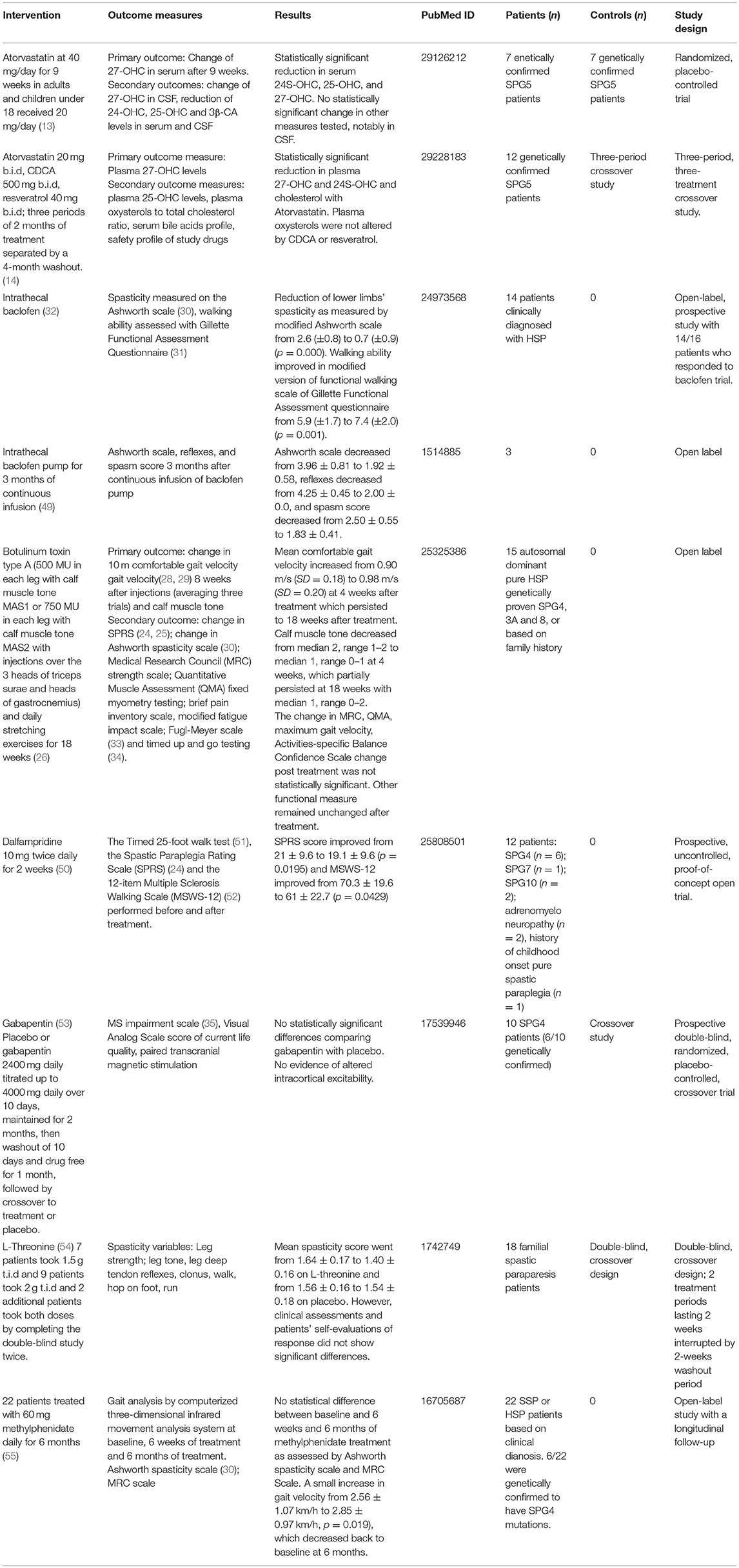
Table 1. Completed clinical trials for HSPs.
This study targeted a specific sub-type of HSP, SPG5, which is a rare autosomal recessive HSP due to mutation in oxysterol-7α-hydroxylase protein CYP7B1, which degrades side chain oxidized cholesterols. It was hypothesized that reducing cholesterol levels with atorvastatin would reduce toxic side-chain oxidized cholesterols, particularly 27-OHC, and while serum levels were lowered, CSF levels were not. There was no clinical benefit noted in the short time period of treatment (9 weeks).
In this study of SPG5, the primary outcome measure was plasma 27-OHC levels and secondary outcome measures included plasma 25-OHC levels, plasma oxysterols to total cholesterol ratio, a serum bile acids profile, and the safety profile of study drugs. The trial was designed such that a total of 12 SPG5 patients were treated for three periods of 2 months with each agent, separated by a 4-month washout. There was a statistically-significant reduction in plasma 27-OHC, 24S-OHC and cholesterol levels with atorvastatin. However, plasma oxysterols were not altered by CDCA or resveratrol.
Patients were given either normal saline or 50 μg of baclofen intrathecally, and those who had an average drop of two points in muscle tone and reflexes score were offered implantation of a baclofen pump and then monitored after 3 months of therapy. Measures of response of three patients after 3 months of therapy were: the Ashworth scale (0–5), the spasm score (0–4 with 0 no spasms, 1 mild spasms by stimulation, 2 infrequent spasms less than once per hour, 3 spasms more than once per hour, and 4 spasms occurring more than ten times an hour), and reflex score (0–5). They found that with a baclofen pump for 3 months, the Ashworth score decreased from 3.96 ± 0.81 to 1.92 ± 0.58, reflexes decreased from 4.25 ± 0.45 to 2.00 ± 0.0, and the spasm score decreased from 2.50 ± 0.55 to 1.83 ± 0.41.
In this study, 14 HSP patients had baclofen pumps placed finding a reduction of lower limb spasticity as measured using a modified Ashworth scale from 2.6 ± 0.8 to 0.7 ± 0.9 (p = 0.000) and that patients' walking ability improved as assessed in a modified version of functional walking scale of the Gillette Functional Assessment questionnaire from 5.9 ± 1.7 to 7.4 ± 2.0 (p = 0.001).
A clinical trial tested botulinum toxin type-A [500 mouse LD50 units (MU) in each leg with calf muscle tone MAS1 or 750 MU in each leg with calf muscle tone MAS2, with injections over the 3 heads of triceps surae and heads of gastrocnemius] and daily stretching exercises for 18 weeks in HSP patients (26). The primary outcome measure was a change in baseline of 10-m comfortable gait velocity (28, 29) measured at 4 weeks (peak effect time) and 18 weeks (residual effects of botulinum toxin type A) after injections, with an average of three trials used as final measure at each time point. Secondary outcome measures included change from baseline in SPRS (24, 25), change in baseline in Ashworth spasticity scale (30) of adductors and triceps surae, change from baseline in muscle strength, change from baseline in visual analogic scale of pain, brief pain inventory scale, and modified fatigue impact scale. The authors also addressed the Fugl-Meyer scale (33) and timed up-and-go testing (34). Interestingly, it was comfortable gait velocity that increased post-botulinum toxin type A and stretching, not maximum gait velocity. Besides tone, other measures did not statistically differ post-treatment.
In this prospective, uncontrolled, open label trial, 12 patients with different forms of HSP were treated with dalfampridine 10 mg twice daily for 2 weeks. While there was no control group, the total SPRS score improved from 21 ± 9.6 to 19.1 ± 9.6 (p = 0.0195), and the MSWS-12 improved from 70.3 ± 19.6 to 61 ± 22.7 (p = 0.0429). Given the lack of a control group, the authors noted that a placebo effect could not be ruled out.
In this prospective double-blind, randomized placebo-controlled crossover trial, patients were given placebo or gabapentin 2,400 mg daily titrated up to 4,000 mg daily over 10 days, maintained for 2 months; next, a washout of 10 days and drug-free period for 1 month were followed by crossover to treatment or placebo. Of note, 2/10 patients had gabapentin levels below 20 mmol on testing, indicating possible non-compliance with therapy. Patients were assessed using the MS Impairment Scale (35), Visual Analog Scale score of current life quality, and paired transcranial magnetic stimulation. Overall, no significant differences were noted between gabapentin treatment and placebo arms.
One early clinical trial tested L-threonine in 18 patients with familial spastic paraparesis in a double-blind crossover protocol for 2 weeks, at doses of 4.5 or 6.0 g/day. The rationale was to increase the inhibitory glycinergic tone of spinal cord interneurons with L-threonine, since glycine has limited blood-brain barrier penetration. While the treatment increased plasma and CSF levels of L-threonine with statistical significance, glycine levels in blood and CSF were not. While clonus and deep tendon reflexes improved on L-threonine, overall clinical assessments and patients' self-evaluations showed no differences between threonine and placebo treatment.
In this open-label study with a longitudinal follow-up, 22 patients were treated with 60 mg methylphenidate daily for 6 months. While 6 of 22 patients were genetically confirmed to harbor SPG4 mutations, the remaining 16 patients had a clinical diagnosis of HSP or a sporadic form (SSP). A small increase in gait velocity from 2.56 ± 1.07 to 2.85 ± 0.97 km/h (p = 0.019) reverted to baseline at 6 months; this could be attributed to possible placebo effect. One significant limitation in this study was the absence of a placebo group. Additional assessment measures showed no statistical difference between baseline and 6 weeks and 6 months of methylphenidate treatment as assessed by Ashworth spasticity scale and Medical Research Council Scale, cadence (steps/min), and stride length.
In a family with SPG8, an affected mother and daughter were started on L-DOPA (Co-Careldopa 25/100 mg); the mother reported responses in spasms and sensory symptoms in feet (which included burning), and the daughter experienced improvement in spasticity (56). A case study of SPG11 also reported some response of parkinsonism to levodopa (57).
One group bypassed the corticospinal tract in treatment using a startle response. They tested a startling acoustic stimulus (SAS) in 12 HSP patients (8 SPG4, 1 SPG8, and 3 unknown) as well as 12 healthy controls; voluntary ankle dorsiflexion reaction time onset latency was 146 ± 23 ms in HSP patients compared with 127 ± 15 ms in controls without a SAS, but administration of a SAS resulted in HSP patients having onset latency of 89 ± 20 ms compared to controls 91 ± 12 ms. The authors hypothesized that SAS released a subcortically-stored motor program relayed through the reticulospinal tract that improved response similar to normal controls (58). Additionally, 10 weeks of hydrotherapy has been tried in 9 HSP patients, with improvement in baseline velocity from 0.85 ± 0.22 to 0.94 ± 0.27 m/s (59). A clinical trial testing 6 weeks of robotic gait training in 13 uncomplicated HSP patients showed improvement in balance, walking speed, and endurance both after completing the treatment and at 2 months follow up (60).
A clear conclusion that can be garnered from clinical trials completed in HSPs is that, apart from cholesterol modifying therapy in SPG5 reported in 2017 and 2018 (13, 14), molecularly-targeted therapies have been noticeably absent. Other clinical trials have targeted clinical manifestations of HSPs, specifically spasticity. This may be due to an earlier focus on the symptomatic treatment of spasticity, as molecular and genetic understanding of HSP was limited. More recently, clinical trials targeting the molecular pathways of HSP have become more practical. Interestingly, clinical trial designs directed toward treating the symptom of spasticity have not extended to evaluating other common symptoms such as urinary incontinence.
Clinical trial design also has evolved more generally, and this is particularly important in rare diseases such as the HSPs with limited patient numbers. Many of the clinical trials presented here are open-label, unblinded studies; this raises the specter of placebo effect and overall interpretability of the findings. Better trial designs have been increasingly utilized, including double-blinded and cross-over studies. Utilizing the same patients in different arms of a study by cross-over, separated by drug washout, can facilitate clinical trial design for rare diseases.
Careful attention must be paid to whether physiological effects of a drug might persist beyond the washout period. Duration of therapy is also a notable challenge in clinical trials of HSP. While 2 months of CDCA treatment did not yield significant results (14), a case study of 5 years of CDCA treatment showed a marked reduction in 27-OHC levels in a SPG5 patient (61). Assessment of patient compliance by testing serum or urine for drug levels also is important in clinical design. In the clinical trial of gabapentin, serum levels were found to be low in 2/10 patients, raising questions of compliance (53). Given a starting dose of 2,400 mg daily titrated up to 4,000 mg daily over 10 days, it is conceivable that the side effect profile of gabapentin could have impacted patient compliance, particularly when initiated at a relatively high dose. Notably, there are several instances of differences between serum and CSF levels of diagnostic markers, specifically in the L-threonine (54) and atorvastatin trials (13). Care should be taken in attempts to extrapolate plasma biomarkers for HSP, as CSF levels could differ. Indeed, it is possible to therapeutically impact a biomarker without influencing the underlying disease process, and clinical assessment measures are critical in trials.
The future for innovative clinical trial design in the HSPs is encouraging, since we are learning progressively more about the underlying molecular mechanisms of disease. This knowledge has helped to provide molecular targets, biomarkers, animal assessment measures and human clinical measures to assess the therapeutic response for future clinical trials. While this review identifies multiple assessment measures relied upon to quantify response, a key focus on selecting measures that demonstrate effects on how one feels, functions, or survives would likely be more favorably received at the FDA.
The Orphan Drug Act of 1983 defines rare diseases as those affecting <200,000 people in the United States (62). Since HSPs occur in ~1.8 per 100,000 people (1), and given a population of about 325.7 million in the US, this translates to nearly 6,000 patients, rendering HSPs a rare disease, but one with sufficient numbers to perform meaningful trials. The individual genetic forms, of course, are rarer still. Information from natural history studies that evaluate exploratory biomarkers can help to design an efficient drug development pathway. Natural history biomarkers can also provide an understanding of subpopulations as well as help select outcome measures that are more specific or sensitive to changes.
The FDA encourages natural history studies to include a spectrum of disease severity and phenotypes over a significant duration. Prior to first-in-human studies, the FDA requires toxicology from in vitro experiments, animal studies, or both; for toxicology profiles, healthy animals are preferred over animal models of disease. Study endpoints should be optimized for validity, reliability, feasibility, resistance to bias, ability to detect change, relationship to meaningful symptoms or function, and clinical interpretability (63).
Biomarkers may be diagnostic (categorizes disease), prognostic (risk of disease / progression), predictive (response to treatment), or pharmacodynamic (biological response to intervention) (64). The FDA has provided guidance regarding biomarker use for drug development (64, 65), and biomarkers can be used to help in subject selection for clinical trials (65) in certain situations (e.g., enrichment or prognostic biomarkers). Given the large number of genetic causes of HSP, genotyping subjects prior to clinical trials will likely be important. A biomarker can also help assess disease state (65). Preliminary work has shown that CMCT is a prognostic biomarker (27); however, the question of whether CMCT could serve as a pharmacodynamic biomarker [as CMCT does in vitamin B12 deficiency (66)] remains unanswered. A search for additional biomarkers that may have higher specificity and sensitivity is underway. Preliminary work is studying miRNAs (38, 39), measures of oxidative stress (3), and levels of acetylated α-tubulin (6), among others. While p-values are important, sensitivity and specificity are also critical in biomarker development. Biomarkers can help assess mechanism of action and the mechanism of therapeutic effect (65). Biomarkers can also inform dose optimization, particularly in animal models, to determine no observed effect level (NOEL) and no observed adverse effect level (NOAEL) (65). Animal study measures discussed in this review could be helpful in generating these values, with potential extrapolation to human trials. A biomarker can also help monitor a drug's response, particularly safety and efficacy, in attempts to maximize drug efficacy and minimize adverse reactions (65).
In this review, we have set out to provide a roadmap for future clinical trials for the HSPs. Promising therapeutic targets include oxidative stress, microtubule dynamics, genetic rescue strategies, and for more specific subsets of HSPs, autophagy/endolysosomal function and cholesterol metabolism. We have reviewed animal models available to test potential agents on as well as animal assessment measures available to evaluate effect. Blinded experiments on animals will be critical for determining which therapeutics should be advanced to human trials. We have described a number of human clinical assessment tools available to evaluate the physical effects of HSPs and emphasize that the FDA looks for a positive effect on how one feels, functions, or survives as a clinical endpoint. With increasing knowledge of the genetic and cellular basis of HSPs, there will be more opportunities for clinical trial development. Biomarkers, animal models and assessment measures, electrophysiology, and clinical assessment measures continue to be refined, expanding our knowledge of the natural history of HSP. We are hopeful that application of these insights and clinical trial designs will usher in novel clinical trials in this rare disease population.
BT performed research and wrote the manuscript. DH and CB edited the manuscript for important intellectual content.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This work was supported by the Intramural Research Program of the National Institute of Neurological Disorders and Stroke, National Institutes of Health.
1. Ruano L, Melo C, Silva MC, Coutinho P. The global epidemiology of hereditary ataxia and spastic paraplegia: a systematic review of prevalence studies. Neuroepidemiology (2014) 42:174–83. doi: 10.1159/000358801
2. Harding AE. Hereditary “pure” spastic paraplegia: a clinical and genetic study of 22 families. J Neurol Neurosurg Psychiatry (1981) 44:871–83. doi: 10.1136/jnnp.44.10.871
3. Julien C, Lissouba A, Madabattula S, Fardghassemi Y, Rosenfelt C, Androschuk A, et al. Conserved pharmacological rescue of hereditary spastic paraplegia-related phenotypes across model organisms. Hum Mol Genet. (2016) 25:1088–99. doi: 10.1093/hmg/ddv632
4. Denton K, Mou Y, Xu C-C, Shah D, Chang J, Blackstone C, et al. Impaired mitochondrial dynamics underlie axonal defects in hereditary spastic paraplegias. Hum Mol Genet. (2018) 27:2517–30. doi: 10.1093/hmg/ddy156
5. Zempel H, Mandelkow EM. Tau missorting and spastin-induced microtubule disruption in neurodegeneration: Alzheimer disease and hereditary spastic paraplegia. Mol Neurodegener. (2015) 10:68. doi: 10.1186/s13024-015-0064-1
6. Fan Y, Wali G, Sutharsan R, Bellette B, Crane DI, Sue CM, et al. Low dose tubulin-binding drugs rescue peroxisome trafficking deficit in patient-derived stem cells in Hereditary Spastic Paraplegia. Biol Open (2014) 3:494–502. doi: 10.1242/bio.20147641
7. Miller KE, Liu XA, Puthanveettil SV. Automated measurement of fast mitochondrial transport in neurons. Front Cell Neurosci. (2015) 9:435. doi: 10.3389/fncel.2015.00435
8. Baxter SL, Allard DE, Crowl C, Sherwood NT. Cold temperature improves mobility and survival in Drosophila models of autosomal-dominant hereditary spastic paraplegia (AD-HSP). Dis Models Mech. (2014) 7:1005–12. doi: 10.1242/dmm.013987
9. Havlicek S, Kohl Z, Mishra HK, Prots I, Eberhardt E, Denguir N, et al. Gene dosage-dependent rescue of HSP neurite defects in SPG4 patients' neurons. Hum. Mol. Genet. (2014) 23:2527–41. doi: 10.1093/hmg/ddt644
10. Pirozzi M, Quattrini A, Andolfi G, Dina G, Malaguti MC, Auricchio A, et al. Intramuscular viral delivery of paraplegin rescues peripheral axonopathy in a model of hereditary spastic paraplegia. J Clin Invest. (2006) 116:202–8. doi: 10.1172/JCI26210
11. Henson BJ, Zhu W, Hardaway K, Wetzel JL, Stefan M, Albers KM, et al. Transcriptional and post-transcriptional regulation of SPAST, the gene most frequently mutated in hereditary spastic paraplegia. PLoS ONE (2012) 7:e36505. doi: 10.1371/journal.pone.0036505
12. Ebrahimi-Fakhari D, Saffari A, Wahlster L, Lu J, Byrne S, Hoffmann GF, et al. Congenital disorders of autophagy: an emerging novel class of inborn errors of neuro-metabolism. Brain (2016) 139:317–37. doi: 10.1093/brain/awv371
13. Schöls L, Rattay TW, Martus P, Meisner C, Baets J, Fischer I, et al. Hereditary spastic paraplegia type 5: natural history, biomarkers and a randomized controlled trial. Brain (2017) 140:3112–27. doi: 10.1093/brain/awx273
14. Marelli C, Lamari F, Rainteau D, Lafourcade A, Banneau G, Humbert L, et al. Plasma oxysterols: biomarkers for diagnosis and treatment in spastic paraplegia type 5. Brain (2018) 141:72–84. doi: 10.1093/brain/awx297
15. Mignarri A, Malandrini A, Del Puppo M, Magni A, Monti L, Ginanneschi F, et al. Treatment of SPG5 with cholesterol-lowering drugs. J Neurol. (2015) 262:2783–5. doi: 10.1007/s00415-015-7971-5
16. Patten SA, Armstrong GA, Lissouba A, Kabashi E, Parker JA, Drapeau P. Fishing for causes and cures of motor neuron disorders. Dis Model Mech. (2014) 7:799–809. doi: 10.1242/dmm.015719
17. Ferreirinha F, Quattrini A, Pirozzi M, Valsecchi V, Dina G, Broccoli V, et al. Axonal degeneration in paraplegin-deficient mice is associated with abnormal mitochondria and impairment of axonal transport. J Clin Invest. (2004) 113:231–42. doi: 10.1172/JCI200420138
18. Renvoisé B, Stadler J, Singh R, Bakowska JC, Blackstone C. Spg20−/− mice reveal multimodal functions for Troyer syndrome protein spartin in lipid droplet maintenance, cytokinesis and BMP signaling. Hum Mol Genet. (2012) 21:3604–18. doi: 10.1093/hmg/dds191
19. Beetz C, Koch N, Khundadze M, Zimmer G, Nietzsche S, Hertel N, et al. A spastic paraplegia mouse model reveals REEP1-dependent ER shaping. J Clin Invest. (2013) 123:4273–82. doi: 10.1172/JCI65665
20. Khundadze M, Kollmann K, Koch N, Biskup C, Nietzsche S, Zimmer G, et al. A hereditary spastic paraplegia mouse model supports a role of ZFYVE26/SPASTIZIN for the endolysosomal system. PLoS Genet. (2013) 9:e1003988. doi: 10.1371/journal.pgen.1003988
21. Soderblom C, Stadler J, Jupille H, Blackstone C, Shupliakov O, Hanna MC. Targeted disruption of the Mast syndrome gene SPG21 in mice impairs hind limb function and alters axon branching in cultured cortical neurons. Neurogenetics (2010) 11:369–78. doi: 10.1007/s10048-010-0252-7
22. Billat VL, Mouisel E, Roblot N, Melki J. Inter- and intrastrain variation in mouse critical running speed. J Appl Physiol. (2005) 98:1258–63. doi: 10.1152/japplphysiol.00991.2004
23. Tarrade A, Fassier C, Courageot S, Charvin D, Vitte J, Peris L, et al. A mutation of spastin is responsible for swellings and impairment of transport in a region of axon characterized by changes in microtubule composition. Hum Mol Genet. (2006) 15:3544–58. doi: 10.1093/hmg/ddl431
24. Schüle R, Holland-Letz T, Klimpe S, Kassubek J, Klopstock T, Mall V, et al. The Spastic Paraplegia Rating Scale (SPRS): a reliable and valid measure of disease severity. Neurology (2006) 67:430–4. doi: 10.1212/01.wnl.0000228242.53336.90
25. Adry RARC, Lins CC, Kruschewsky RA, Castro Filho BG. Comparison between the spastic paraplegia rating scale, Kurtzke scale, and Osame scale in the tropical spastic paraparesis/myelopathy associated with HTLV. Rev Soc Bras Med Trop. (2012) 45:309–12. doi: 10.1590/S0037-86822012000300006
26. de Niet M, de Bot ST, van de Warrenburg BP, Weerdesteyn V, Geurts AC. Functional effects of botulinum toxin type-A treatment and subsequent stretching of spastic calf muscles: a study in patients with hereditary spastic paraplegia. J Rehabil Med. (2015) 47:147–53. doi: 10.2340/16501977-1909
27. Karle KN, Schüle R, Klebe S, Otto S, Frischholz C, Liepelt-Scarfone I, et al. Electrophysiological characterisation of motor and sensory tracts in patients with hereditary spastic paraplegia (HSP). Orphanet J Rare Dis. (2013) 8:158. doi: 10.1186/1750-1172-8-158
28. Rossier P, Wade DT. Validity and reliability comparison of 4 mobility measures in patients presenting with neurologic impairment. Arch Phys Med Rahabil. (2001)82:9–13. doi: 10.1053/apmr.2001.9396
29. Collen FM, Wade DT, Bradshaw CM. Mobility after stroke: reliability of measures of impairment and disability. Int Disabil Stud. (1990) 12:6–9. doi: 10.3109/03790799009166594
30. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. (1987) 67:206–7. doi: 10.1093/ptj/67.2.206
31. Novacheck TF, Stout JL, Tervo R. Reliability and validity of the Gillette Functional Assessment Questionnaire as an outcome measure in children with walking disabilities. J Pediatr Orthop. (2000) 20:75–81. doi: 10.1097/01241398-200001000-00017
32. Margetis K, Korfias S, Boutos N, Gatzonis S, Themistocleous M, Siatouni A, et al. Intrathecal baclofen therapy for the symptomatic treatment of hereditary spastic paraplegia. Clin Neurol Neurosurg. (2014) 123:142–5. doi: 10.1016/j.clineuro.2014.05.024
33. Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand J Rehabil Med. (1975) 7:13–31.
34. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. (1991) 39:142–8. doi: 10.1111/j.1532-5415.1991.tb01616.x
35. Ravnborg M, Grønbech-Jensen M, Jønsson A. The MS impairment scale: a pragmatic approach to the assessment of impairment in patients with multiple sclerosis. Mult Scler. (1997) 3:31–42. doi: 10.1177/135245859700300104
36. Erichsen AK, Koht J, Stray-Pedersen A, Abdelnoor M, Tallaksen CME. Prevalence of hereditary ataxia and spastic paraplegia in southeast Norway: a population-based study. Brain (2009) 132:1577–88. doi: 10.1093/brain/awp056
37. Orsucci D, Petrucci L, Ienco EC, Chico L, Simi P, Fogli A, et al. Hereditary spastic paraparesis in adults: a clinical and genetic perspective from Tuscany. Clin Neurol Neurosurg. (2014) 120:14–9. doi: 10.1016/j.clineuro.2014.02.002
38. Beetz C, Schüle R, Deconinck T, Tran-Viet K-N, Zhu H, Kremer BPH, et al. REEP1 mutation spectrum and genotype/phenotype correlation in hereditary spastic paraplegia type 31. Brain (2008) 131:1078–86. doi: 10.1093/brain/awn026
39. Vrabec K, Boštjančič E, Koritnik B, Leonardis L, Dolenc Grošelj L, Zidar J, et al. Differential expression of several miRNAs and the host genes AATK and DNM2 in leukocytes of sporadic ALS patients. Front Mol Neurosci. (2018) 11:106. doi: 10.3389/fnmol.2018.00106
40. Wagley Y, Choi J-H, Wickramanayake DD, Choi G-Y, Kim C-K, Kim T-H, et al. A monoclonal antibody against human MUDENG protein. Monoclon Antib Immunodiagn Immunother. (2013) 32:277–82. doi: 10.1089/mab.2013.0015
41. Collongues N, Depienne C, Boehm N, Echaniz-Laguna A, Samama B, Dürr A, et al. Novel SPG10 mutation associated with dysautonomia, spinal cord atrophy, and skin biopsy abnormality. Eur J Neurol. (2013) 20:398–401. doi: 10.1111/j.1468-1331.2012.03803.x
42. Criscuolo C, Filla A, Coppola G, Rinaldi C, Carbone R, Pinto S, et al. Two novel CYP7B1 mutations in Italian families with SPG5: a clinical and genetic study. J Neurol. (2009) 256:1252–7. doi: 10.1007/s00415-009-5109-3
43. Samaranch L, Riverol M, Masdeu JC, Lorenzo E, Vidal-Taboada JM, Irigoyen J, et al. SPG11 compound mutations in spastic paraparesis with thin corpus callosum. Neurology (2008) 71:332–6. doi: 10.1212/01.wnl.0000319646.23052.d1
44. Erichsen AK, Server A, Landrø NI, Sandvik L, Tallaksen CME. Proton magnetic resonance spectroscopy and cognition in patients with spastin mutations. J Neurol Sci. (2009) 277:124–9. doi: 10.1016/j.jns.2008.10.030
45. Schuurs-Hoeijmakers JH, Geraghty MT, Kamsteeg EJ, Ben-Salem S, de Bot ST, Nijhof B, et al. Mutations in DDHD2, encoding an intracellular phospholipase A1, cause a recessive form of complex hereditary spastic paraplegia. Am J Hum Genet. (2012) 91:1073–81. doi: 10.1016/j.ajhg.2012.10.017
46. Kersten HM, Roxburgh RH, Danesh-Meyer HV. Ophthalmic manifestations of inherited neurodegenerative disorders. Nat Rev Neurol. (2014) 10:349–62. doi: 10.1038/nrneurol.2014.79
47. Klebe S, Depienne C, Gerber S, Challe G, Anheim M, Charles P, et al. Spastic paraplegia gene 7 in patients with spasticity and/or optic neuropathy. Brain (2012) 135:2980–93. doi: 10.1093/brain/aws240
48. Sartucci F, Tovani S, Murri L, Sagliocco L. Motor and somatosensory evoked potentials in Autosomal Dominant Hereditary Spastic Paraparesis (ADHSP) linked to chromosome 2p, SPG4. Brain Res Bull. (2007) 74:243–9. doi: 10.1016/j.brainresbull.2007.06.018
49. Meythaler JM, Steers WD, Tuel SM, Cross LL, Sesco DC, Haworth CS. Intrathecal baclofen in hereditary spastic paraparesis. Arch Phys Med Rehabil. (1992) 73:794–7.
50. Bereau M, Anheim M, Chanson JB, Tio G, Echaniz-Laguna A, Depienne C, et al. Dalfampridine in hereditary spastic paraplegia: a prospective, open study. J Neurol. (2015) 262:1285–8. doi: 10.1007/s00415-015-7707-6
51. Cohen JA, Cutter GR, Fischer JS, Goodman AD, Heidenreich FR, Jak AJ, et al. Use of the multiple sclerosis functional composite as an outcome measure in a phase 3 clinical trial. Arch Neurol. (2001) 58:961–7. doi: 10.1001/archneur.58.6.961
52. Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ. Measuring the impact of MS on walking ability: the 12-Item MS Walking Scale (MSWS-12). Neurology (2003) 60:31–6. doi: 10.1212/WNL.60.1.31
53. Scheuer KH, Svenstrup K, Jennum P, Rogvi-Hansen B, Werdelin L, Fenger K, et al. Double-blind crossover trial of gabapentin in SPG4-linked hereditary spastic paraplegia. Eur J Neurol. (2007) 14:663–6. doi: 10.1111/j.1468-1331.2007.01812.x
54. Growdon JH, Nader TM, Schoenfeld J, Wurtman RJ. L-threonine in the treatment of spasticity. Clin Neuropharmacol. (1991) 14:403–12.
55. Klebe S, Deuschl G, Stolze H. Methylphenidate fails to improve gait and muscle tone in patients with sporadic and hereditary spastic paraplegia. Mov Disord. (2006) 21:1468–71. doi: 10.1002/mds.20973
56. Bettencourt C, Morris HR, Singleton AB, Hardy J, Houlden H. Exome sequencing expands the mutational spectrum of SPG8 in a family with spasticity responsive to L-DOPA treatment. J Neurol. (2013) 260:2414–6. doi: 10.1007/s00415-013-7044-6
57. Guidubaldi A, Piano C, Santorelli FM, Silvestri G, Petracca M, Tessa A, et al. Novel mutations in SPG11 cause hereditary spastic paraplegia associated with early-onset levodopa-responsive Parkinsonism. Mov Disord. (2011) 26:553–6. doi: 10.1002/mds.23552
58. Nonnekes J, Oude Nijhuis LB, de Niet M, de Bot ST, Pasman JW, van de Warrenburg BP, et al. StartReact restores reaction time in HSP: evidence for subcortical release of a motor program. J Neurosci. (2014) 34:275–81. doi: 10.1523/JNEUROSCI.2948-13.2014
59. Zhang Y, Roxburgh R, Huang L, Parsons J, Davies TC. The effect of hydrotherapy treatment on gait characteristics of hereditary spastic paraparesis patients. Gait Posture (2014) 39:1074–9. doi: 10.1016/j.gaitpost.2014.01.010
60. Bertolucci F, Di Martino S, Orsucci D, Ienco EC, Siciliano G, Rossi B, et al. Robotic gait training improves motor skills and quality of life in hereditary spastic paraplegia. NeuroRehabilitation. (2015) 36:93–9. doi: 10.3233/NRE-141196
61. Dai D, Mills PB, Footitt E, Gissen P, McClean P, Stahlschmidt J, et al. Liver disease in infancy caused by oxysterol 7 α-hydroxylase deficiency: successful treatment with chenodeoxycholic acid. J Inherit Metab Dis. (2014) 37:851–61. doi: 10.1007/s10545-014-9695-6
63. U.S. Department of Health and Human Services FDA, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluation and Research (CBER). Rare Diseases: Common Issues in Drug Development Guidance for Industry Draft Guidance (2015).
64. U.S Department of Health and Human Services FDA, Center for Drug Evaluation and Research. Guidance for Industry and FDA Staff Qualification Process for Drug Development Tools (2014).
65. U.S Department of Health and Human Services FDA, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluation and Research (CBER). Guidance for Industry E16 Biomarkers Related to Drug or Biotechnology Product Development: Context, Structure, and Format of Qualification Submissions (2011).
Keywords: rating scales, spasticity, therapeutics, neurogenetics, neuromuscular
Citation: Trummer B, Haubenberger D and Blackstone C (2018) Clinical Trial Designs and Measures in Hereditary Spastic Paraplegias. Front. Neurol. 9:1017. doi: 10.3389/fneur.2018.01017
Received: 31 July 2018; Accepted: 12 November 2018;
Published: 21 December 2018.
Edited by:
Antonio Orlacchio, Fondazione Santa Lucia (IRCCS), ItalyReviewed by:
Ryosuke Miyamoto, Tokushima University, JapanCopyright © 2018 Trummer, Haubenberger and Blackstone. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Craig Blackstone, YmxhY2tzdGNAbmluZHMubmloLmdvdg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.