
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 07 June 2018
Sec. Movement Disorders
Volume 9 - 2018 | https://doi.org/10.3389/fneur.2018.00435
This article is part of the Research Topic Movement Disorders and Sleep – Underlying Mechanisms, Clinical Aspects and Treatment View all 12 articles
 Carmen Rodríguez-Blázquez1*
Carmen Rodríguez-Blázquez1* Maria João Forjaz2
Maria João Forjaz2 Monica M. Kurtis3
Monica M. Kurtis3 Roberta Balestrino4
Roberta Balestrino4 Pablo Martinez-Martin1
Pablo Martinez-Martin1Introduction: In recent years, a wide variety of rating scales and questionnaires for movement disorders have been developed and published, making reviews on their contents, and attributes convenient for the potential users. Sleep disorders are frequently present in movement disorders, and some movement disorders are accompanied by specific sleep difficulties.
Aim: The aim of this study is to perform a narrative review of the most frequently used rating scales for movement disorders with sleep problems, with special attention to those recommended by the International Parkinson and Movement Disorders Society.
Methods: Online databases (PubMed, SCOPUS, Web of Science, Google Scholar), related references from papers and websites and personal files were searched for information on comprehensive or global rating scales which assessed sleep disturbances in the following movement disorders: akathisia, chorea, dystonia, essential tremor, myoclonus, multiple system atrophy, Parkinson's disease, progressive supranuclear palsy, and tics and Tourette syndrome. For each rating scale, its objective and characteristics, as well as a summary of its psychometric properties and recommendations of use are described.
Results: From 22 rating scales identified for the selected movement disorders, only 5 included specific questions on sleep problems. Movement Disorders Society-Unified Parkinson's Disease Rating scale (MDS-UPDRS), Non-Motor Symptoms Scale and Questionnaire (NMSS and NMSQuest), Scales for Outcomes in Parkinson's Disease (SCOPA)-Autonomic and Progressive Supranuclear Palsy Rating Scale (PSPRS) were the only rating scales that included items for assessing sleep disturbances.
Conclusions: Despite sleep problems are frequent in movement disorders, very few of the rating scales addresses these specific symptoms. This may contribute to an infra diagnosis and mistreatment of the sleep problems in patients with movement disorders.
A wide variety of rating scales and questionnaires for the wide range of movement disorders that can affect patients have been developed and are currently available for clinical practice and research. These instruments may be classified as “rater-based,” which are applied by a health professional or trained person, and “patient-based,” which are directly completed by patients themselves. Rater-based scales (clinician-reported outcomes measures) are used to evaluate observable signs of the disorder (e.g., tremor, rigidity, instability, myoclonus, tics) by means of clinical examination, and other non-observable aspects through interview with the patient and/or caregiver. Patient-based instruments (patient-reported outcomes measures) allow the assessment of non-observable, subjective features, and perceptions (e.g., pain, fatigue, sensations, feelings, hallucinations, health state) (1). Some effects caused by the health disorder (e.g., disability, symptoms) can be appraised by both methods.
Their simplicity of use, as well as the amount and quality of information the rating scales provide, justify why rating scales and questionnaires are widely used in clinical and research settings.
Sleep disorders are frequently present in movement disorders, as they can share pathophysiological mechanisms and damage to brain structures (2). Insomnia and sleep fragmentation are common in Parkinson's disease (PD), multiple system atrophy (MSA), progressive supranuclear palsy (PSP) (3), and different choreic disorders. REM-sleep behavior disorder appears associated to α-synucleinopathies, such as PD, Lewy body dementia, and MSA, and can be an early marker of the disease (4). Impaired sleep architecture is frequent in Tourette syndrome (5). PD and essential tremor (ET) are often associated with restless legs and nocturnal periodic limb movements (6, 7). The relevance of sleep problems in movement disorders has been acknowledged in the recent years and specific rating scales for assessing sleep have been developed and validated. However, these scales are only available for PD, and specific symptoms are not sufficiently addressed (8). Simultaneously, global rating scales for the assessment of specific movement disorders have been developed, such as the Unified Huntington's Disease Rating Scale (UHDRS), Unified Dystonia Rating Scale (UDRS), or the Unified Multiple System Atrophy Rating Scale (UMSARS), with the aim of providing a comprehensive appraisal of the clinical manifestations (motor and non-motor symptoms) of these disorders.
The aim of this study is to perform a narrative review of most frequently used rating scales for those movement disorders that comprise sleep dysfunction among their primary manifestations or sleep problems secondary to the movement disorder, with special attention to the scales recommended by the International Parkinson and Movement Disorders Society (IPMDS) Task Force (9).
Authors made a list of the movement disorders that can course with sleep symptoms that included akathisia, chore, dystonia, essential tremor, multiple system atrophy, myoclonus, Parkinson's Disease, progressive supranuclear palsy, and tics and Tourette syndrome. The literature search, carried out using PubMed, Web of Science and Scopus, included these terms plus “sleep” and “rating scales.” In addition, the reviews published by IPMDS on these movement disorders (9) and related references from papers and personal files were examined. The IPMDS Task force classifies a scale as “recommended” if it has been used in PD, shows adequate psychometric properties, and has been used by investigators other than the original developers; as “suggested” if it has been used in PD and fulfills only one other criterion; and as “listed” if it has been used in PD but does not meet the other criteria.
The main rating scales for Parkinson's disease (PD), such as the Movement Disorders Society–Unified Parkinson's Disease Rating Scale (MDS-UPDRS) and the Non-Motor Symptoms Scale (NMSS), are also included. Table 1 lists the scales incorporated to this review. Specific instruments assessing sleep disorders in movement disorders, such as the Parkinson's Disease Sleep Scale (PDSS) and the Scales for Outcomes in PD (SCOPA)-Sleep, are reviewed in another article in this issue (8). For each rating scale, its objective, characteristics, psychometric properties, and recommendations of use are described.
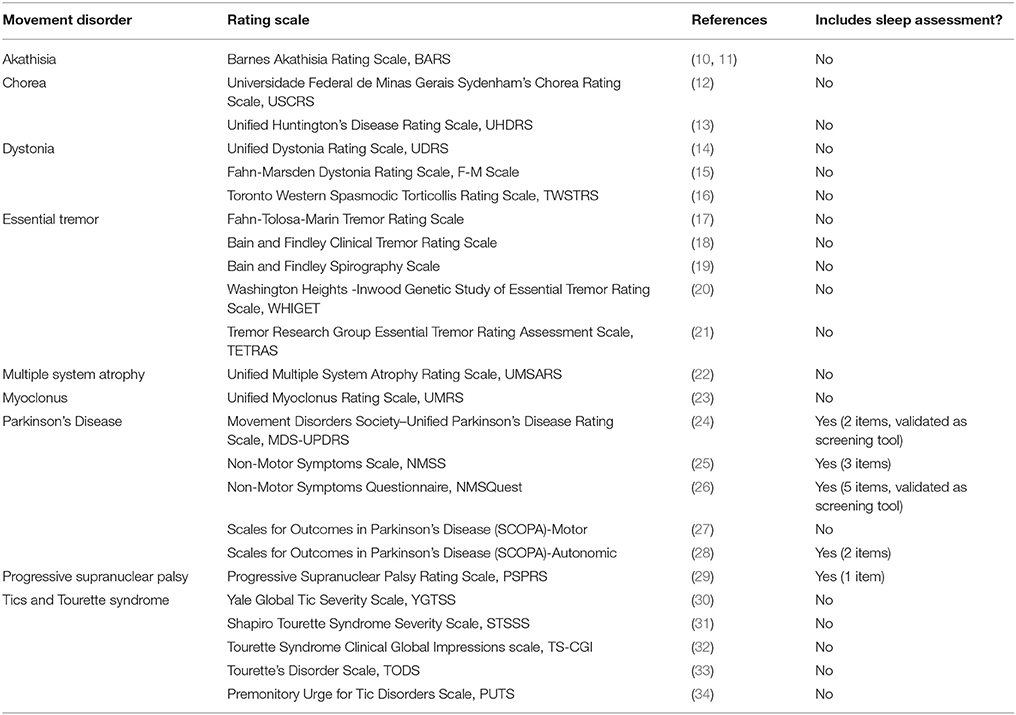
Table 1. Rating scales for movement disorders with sleep disturbances included in this review.
Akathisia has been associated to nocturnal periodic limb movements and increased number of awakenings (35). However, the main rating scale for akathisia, the Barnes Akathisia Rating Scale (BARS) does not include sleep assessment (10). The BARS is a 4-item scale for rating the presence and severity of the drug-induced akathisia. It shows adequate reliability, validity, and responsiveness (11).
Results of an online survey of juvenile Huntington's disease (HD) suggests that disrupted sleep is the most prevalent common, unrecognized symptom (87%), followed by periodic limb movements, tics, and pain (36, 37). HD gene carriers complain about sleep problems, both in terms of sleep quality as well as excessive daytime sleepiness (38, 39). Sleep complaints seem to be associated with neuropathology and neuropsychiatric symptoms in HD (40). However, ratings scales for chorea or HD do not assess sleep difficulties.
The Universidade Federal de Minas Gerais Sydenham's Chorea Rating Scale (USCRS) assesses signs and symptoms of children and adults with Sydenham's Chorea and related disorders (12). It is formed by 27 items organized into three sections (behavior, activities of daily living, and motor assessment). Items are scored on a 0–4 rating scale, with higher values indicating higher severity of disability or signs. Although the scale presented a two-factor structure (motor function and ADL; behavioral) (12), a total sum score is used in most studies (41–44). Published in 2005 (12), the scale is rater-based and it is owned by the IPMDS. It has shown adequate inter-rater reliability and internal consistency (12), as well as discriminative validity by disease stage (44). The USCRS has been used in Brazil (12, 43, 44), Italy (42), and Israel (41).
The UHDRS was developed by the Huntington Study Group as a research tool, and it has been used as an outcome measure in clinical trials (13). It is formed by the following components: motor, with 15 items (45); cognitive (formed by Verbal Fluency Test; Symbol Digit Modalities Test; Stroop Interference Test), behavioral (10 items) and functional (5 items) assessments, independence scale (1 item, from 10, totally dependent, to 100, totally independent), and total functional capacity (TFC, 25 items). Internal consistency is high and the UHDRS shows satisfactory inter-rater reliability and sensitivity to change. Although it was published as annex of an article (13), it is actually owned by the Huntington Study Group and permission for use is required.
A IPMDS task force rated the UHDRS behavioral section (UHDRS-b) as a “suggested” scale for assessing severity of and screening for behavioral symptoms in patients with HD (46). The UHDRS also has a version for advanced patients (UHDRS-FAP), with satisfactory internal consistency and inter-rater reliability (47).
There is a growing interest on non-motor symptoms of dystonia patients, including sleep problems (48). Sleep impairment may be a primary effect of dystonia or secondary effects of pain and medications (49). Different types of dystonia may be associated to specific sleep disorders: poor sleep quality has been described in blepharospasm, cervical dystonia patients report more daytime sleepiness than controls (50), and impaired sleep efficiency and decreased rapid eye movement (REM) sleep has been reported in blepharospasm and oromandibular dystonia (51).
On the basis of their psychometric properties and clinical and research application, a review commissioned by the IPMDS qualified five disease-specific scales as “recommended,” and two scales as “listed” for laryngeal dystonia (52). None of them assesses sleep disorders.
The UDRS (14), a rating scale for generalized dystonia, was “suggested” for use in dystonia and did not reach a “recommended” rating due to insufficient psychometric studies about responsiveness (52). The clinician assesses 14 body locations, rated for both duration (0–4 score, including half-scores) and severity (0–4 scale) of dystonia. The total score is the sum of the duration and severity ratings. Internal consistency is high, and the scale shows good inter-rater reliability and convergent validity with other dystonia rating scales (14). The UDRS is owned by the IPMDS and license for use is needed.
The Fahn-Marsden Dystonia Rating Scale (F-M Scale), a predecessor of the UDRS, was initially developed to assess primary torsion dystonia in 9 body parts (15). It has two factors, one for severity (each body part is rated from 0, no dystonia, to 4, severe dystonia) and the other for the precipitation or provoking factor (from 0, no dystonia, to 4, dystonia at rest). The scores for eyes, mouth, and neck are multiplied by 0.5 when calculating the total score, which is then obtained by summing the product of the severity, provoking, and weighting factors. The F-M Scale also includes a disability scale based on the patient's report that evaluates the impact of dystonia on seven activities of daily living. The walking item is rated on a 7-point scale and the rest of the disability items on a 0–4 point scale. The F-M scale has shown good internal consistency, inter-rater agreement, and convergent validity with other dystonia rating scales (14), as well as adequate responsiveness (52). Despite criticisms of the low contribution of some body parts to the overall score, this scale is “recommended” to assess the severity of the dystonia (52) and has been used for evaluating dystonia in many conditions and clinical trials.
The Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) (16) is a “recommended” rating scale that was designed to assess a specific condition, cervical dystonia, in clinical trials (52). It is formed by three subscales assessing motor severity (11 items), disability (6 items), and pain (3 items). The first subscale is rated by the clinician whereas the other two are patient-rated. The scoring system is not uniform and a videotape for training is available for the severity section. This scale, available in English, has been frequently used in clinical trials. Its psychometric properties are satisfactory and well-documented, including internal consistency, inter-rater agreement for the severity subscale, internal, and convergent validity, as well as responsiveness. The TWSTRS has been criticized for its complexity for clinical practice (52). Excessive daytime sleepiness in cervical dystonia was not associated with TWSTRS scores (50).
Besides motor features, essential tremor also includes non-motor symptoms such as sleep problems (53–55), which have a negative effect on quality of life (56). Excessive daytime sleepiness, shorter sleep duration (57), and restless legs complaints are more frequent in essential tremor patients than in healthy controls (8).
Despite increasing evidence of sleep problems in essential tremor, none of the currently available rating scales to assess tremor include items about sleep. The IPMDS Task Force recommends several rating scales for evaluating tremor severity.
The Fahn-Tolosa-Marin Tremor Rating Scale provides a comprehensive assessment of tremor, rated by the clinician and the patient (17). It is formed by 3 parts: tremor in 9 body parts and orthostatic tremor; action tremor in 3 tasks; and patient-reported functional disability. In addition, both clinical and patient rate a global assessment item. Items are rated on a 0–4 point scale. The scale presents good intra and inter-rater reliability (18), but there is a lack of data on other psychometric parameters (58). It has been used in many clinical trials.
The Bain and Findley Clinical Tremor Rating Scale assesses tremor severity (59) and impact on activities of daily living. For each body part (head, voice, and limbs), the clinician rates the severity of several tremor components: rest, postural, and kinetic/intention tremor. The initial 0–10 response scale was simplified to a 5-point scale with intermediate values. Inter-rater reliability was satisfactory as a whole, especially for upper limb postural and head tremor, but not for voice tremor (59). The severity scale shows good convergent validity with other tremor measures, and it was sensitive to change in clinical trials (58). With a scoring system based on subjective impression, the Bain and Findley Clinical Tremor Rating Scale is easy to apply in a diversity of conditions and circumstances, including bedside.
In the Bain and Findley Spirography Scale, action tremor is assessed through Archimedes spirals. Rating are on a 0–10 scale, and rating examples are provided (59, 19). Its reliability is good provided that raters are trained (58). This scale has been criticized for its high floor and ceiling effects; however, it shows adequate face and construct validity (58).
The Washington Heights -Inwood Genetic Study of Essential Tremor (WHIGET) Rating Scale is aimed at assessing the severity of essential tremor during the performance of several tasks (20). The clinician rates the following tremor parameters: intensity, amplitude, oscillation prevalence, and persistency of rest, kinetic and postural tremor. There are 26 items rated on a 0–3 scale. A revised version rates kinetic tremor from 0 to 4 (60). A training videotape is available (60). Test-retest and inter-rater reliability are satisfactory, as well as convergent validity with other measures of tremor (61). Some studies support the scale's sensitivity to change (62, 63). The WHIGET limits assessment to upper extremity tremor.
The Tremor Research Group Essential Tremor Rating Assessment Scale (TETRAS) is formed by two subscales (21). The performance subscale, with 9 items, rates action tremor in head, face, voice, limbs, and trunk. The activities of daily living section if formed by 12 items. Both sections use a 0–4 point scale, but performance items admit half-point scores. This short, easy to apply scale has appropriate reliability, validity, and sensitivity to change for the performance section (64–66). More psychometric studies are needed for the activities of daily living subscale.
MSA affects sleep in several ways: sleep-disordered breathing (67), sleep fragmentation, REM sleep behavior disorder, insomnia, and excessive daytime sleepiness (68). In addition, sleep study (polysomnography) are included in a list of useful tools for differential diagnosis of MSA (69). Despite this, specific rating scales for this movement disorder do not include items for assessment of sleep disturbances.
The most used scale for MSA is the UMSARS developed by the European MSA Study Group (22). It comprises four parts: Part I, historical (functional status), with 12 items; Part II, motor examination, with 14 items; Part III, autonomic examination, with items assessing blood pressure, heart rate and orthostatic symptoms; and Part IV, global disability scale. In Parts I and II, scores range from 0 to 4, and in Part IV, the scale ranges from 1 (completely independent) to 5 (totally independent). The UMSARS psychometric properties are adequate, showing high internal consistency in Parts I and II, satisfactory inter and intra-rater reliability and sensitivity to change over time (22, 70). The UMSARS can distinguish between different subtypes (parkinsonism- vs cerebellar ataxia-predominant) of MSA (71) and has been used as reference in the validation of other scales for MSA (72). It is owned and licensed by the IPMDS. A comparative review of the longitudinal performance of the UMSARS and other scales for MSA can be found in Matsushima et al. (73).
Clinical presentations of myoclonus are divided into physiological, essential, epileptic, and symptomatic (74). While physiological myoclonus can occur as jerks during sleep or sleep transitions in healthy individuals, other myoclonic sleep disorders (e.g., propriospinal myoclonus) can be identified (75) and some types of myoclonic epilepsy, characterized by abnormal sleep electroencephalogram and an activation of the paroxysms during non-REM sleep and on waking up (76).
The main tool for assessing myoclonus is the Unified Myoclonus Rating Scale (UMRS) (23). It assesses the severity and characteristics of the disorder and the associated disability. The UMRS has 73 items, grouped into five sections: patient's questionnaire (12 items, scored from 1 to 5); myoclonus at rest (8 items for frequency and amplitude, scored from 0 to 4); stimulus sensitivity (17 items, dichotomous); myoclonus with action (10 items, scored for frequency and amplitude on a 5-point scale); and functional tests (5 items, scored from 0 to 4). It also includes a global disability scale, scored from 0 (normal) to 4 (severe), and two items assessing presence (yes/no) and severity (from 0 to 3) of negative myoclonus. Components for evaluation of myoclonus-related sleep disorders are not included in this scale. The UMRS has satisfactory internal consistency and inter-rater reliability (23, 77) and is responsive to changes due to treatment (78).
Sleep disorders are common in PD: they can affect up to 60–90% of PD patients, with increasing prevalence as the disease progresses (7). Insomnia and sleep fragmentation, excessive daytime sleepiness, restless legs and REM-sleep behavior disorder are frequently present in PD (79). Some specific rating scales for sleep disorders in PD are currently available, but they are the object of another article in this issue. Sleep problems are included in the main multi-domain, comprehensive rating scales for PD, the MDS-Unified Parkinson's Disease Rating Scale (MDS-UPDRS) (24), and the Non-Motor Symptoms Scale (NMSS) (25).
The MDS-UPDRS is the revised version of the widely used UPDRS (80). It has four sections: Part I, non-motor experiences of daily living; Part II, motor experiences of daily living; Part III, motor examination; and Part IV, motor complications. In Part I, with 6 rater-based items and 7 self-assessed items, two questions rating nighttime sleep problems and daytime sleepiness can be used as screening tool for sleep disturbances (81). All items are scored from 0 (normal) to 4 (severe). The MDS-UPDRS has good psychometric properties and is responsive to changes due to treatment (82, 83). The minimal clinically important difference of the Part III has been calculated (84).
The NMSS, which is administered by interview, was designed to assess the burden (frequency and severity) of non-motor symptoms (NMS). It is composed of 30 items, grouped in nine domains: cardiovascular (2 items), sleep/fatigue (4 items), mood/cognition (6 items), perceptual problems/hallucinations (3 items), attention/memory (3 items), gastrointestinal tract (3 items), urinary (3 items), sexual function (2 items), and miscellaneous (4 items). In the domain sleep/fatigue, there are three questions to rate daytime sleepiness, problems falling or staying asleep and restless legs syndrome, while in the urinary domain, one item assesses nocturia. All items are scored 0–3 for severity and 1–4 for frequency. The total item score is obtained by multiplication of both aspects and domain and scale score by sum of the respective items scores. The scale, validated, and available in several languages, has good psychometric properties, including responsiveness (85–87).
An instrument related with the NMSS is the Non-Motor Symptoms Questionnaire (NMSQuest) (26), which was developed as a self-assessment of non-motor symptoms. It is composed by 30 yes/no questions, of which six address sleep disturbances: nocturia, daytime sleepiness, insomnia, vivid dreams, acting out while dreaming, and restless legs. These items have been validated and resulted useful as a screening tool for sleep difficulties in PD patients (88). The NMSQuest has good feasibility, acceptability and validity, resulting suitable for patients to flag symptoms that may be undeclared and remain untreated (89). A NMSQuest-based grading system for NMS burden has also been published (90).
Another recommended rating scale (91) is the Scales for Outcomes in Parkinson's Disease (SCOPA)-Motor (27) for assessing motor functioning and disability in PD. It is composed by 21 items, scored from 0 (normal) to 3 (severe), and grouped into three sections: motor examination (10 items), activities of daily living (7 items), and motor complications (4 items). It does not include sleep problems. Satisfactory internal consistency, inter-rater and test-retest reliability and construct validity have been reported (92). It is also responsive to changes over time (93) and can predict an increase in PD-related costs (94).
The SCOPA-Autonomic (28), the first validated rating scale specifically designed for assessing autonomic symptoms in PD, includes two items on symptoms that can cause sleep disturbances: nicturia and excessive sweating during the night. This scale, composed by 25 items grouped in 6 domains (cardiovascular, gastrointestinal, urinary, thermoregulatory, pupillomotor, and sexual), meets criteria for “recommended” (95, 96).
A wide set of other rating scales for assessing specific symptoms and manifestations of PD are recommended by the IPMDS (9), but they are out of the scope of this review.
Insomnia and impaired sleep architecture are the most common sleep abnormalities in PSP, and are more frequently described in PSP than in other atypical parkinsonisms (4). In particular, PSP patients can show a shorter total sleep time, a lower sleep efficiency and a lower percentage of REM sleep than controls (97).
The Progressive Supranuclear Palsy Rating Scale (PSPRS) (29) is the IPMDS Task Force recommended rating scale for assessing symptoms and associated disability of the PSP (98). It has 28 items, scored on a 3- or 5-point scale, and grouped into six dimensions: history (with an item on sleep difficulty), mental, bulbar, supranuclear ocular motor, and limb and gait/mildline examinations. The item named “Sleep difficulty” focused on insomnia and rated from 0 to 4 is included in the “History/Daily activities” section. The total scale score ranges from 0 to 100. The scale shows good inter-rater reliability and satisfactory predictive validity in relation to survival. The minimal clinically important worsening has been established in 5.7 points (99).
Tics and TS can be associated with sleep disturbances such as insomnia and abnormal behaviors during sleep (100). Specific sleep architecture abnormalities, such as shorter REM latency and increased percentage of REM sleep, have also been reported in patients with TS (6). However, none of the IPMDS-recommended scales for tics and TS assesses sleep problems.
Five rating scales have been recommended for the IPMDS Task Force for assessment of tics and Tourette syndrome (101). The most widely used rating scale for motor and phonic tics is the Yale Global Tic Severity Scale (YGTSS) (30). It is a complex, rater-based tool, composed by items rating number, frequency, intensity, complexity, and interference of symptoms in a scoring scale from 0 (none/absent) to 5 (severe/always). The YGTSS yields total motor and phonic scores, an overall impairment rating and a global severity score. Its psychometric properties are satisfactory and thresholds of score changes due to clinical treatment are available (102, 103).
The Shapiro Tourette Syndrome Severity Scale (STSSS) (31) rates intensity of symptoms and interference with functioning, and it is reliable, valid, brief, and easy to administer. The Tourette Syndrome Clinical Global Impressions scale (TS-CGI) (32), also a brief scale, scores the overall adverse impact of tics. These two scales are less comprehensive than the YGTSS, as they do not include some aspects such as frequency, complexity, and distribution of tics. The Tourette's Disorder Scale (TODS) (33) rates overall tics severity but also assess comorbid behavioral symptoms: inattention, hyperactivity, obsessions, compulsions, aggression, and emotional symptoms. It shows excellent internal consistency and excellent inter-rater agreement and convergent and divergent validity (104).
Finally, the Premonitory Urge for Tic Disorders Scale (PUTS), the only specific scale for tic-related premonitory urges, presented satisfactory psychometric properties only for patients older than 10 years (34).
Several conditions, toxic agents, and metabolic dysfunctions can produce effects on brain structures and functional circuits in such a way that movement disorders and sleep disorders are manifested simultaneously. On the other hand, some movement disorders are associated with disturbed physiological sleep patterns, adding to the distress, and quality of life deterioration these patients suffer. Correct management of both types of disorders is mandatory and thus requires close evaluation and monitoring. However, as frequently occurs in the realm of movement disorders, the existence of non-motor symptoms and, specifically, sleep disturbances may remain undeclared (89) and underdiagnosed, missing the opportunity of appropriate treatment to improve the patient's health state.
Objective methods, based on wearable devices and technological developments, can be used for the appraisal of severity of movement disorders, sleep disturbances, and both types of conditions simultaneously when they are present in combination. Objective methods are also used for the diagnosis of several sleep disorders according to sleep disorder diagnostic criteria (periodic limb movement, obstructive sleep apneas, etc.), and particularly when the sleep dysfunction is due to several different causes as in atypical Parkinsonism or HD.
Polysomnography is very useful for this objective, but due to the complexity and costs of the sleep laboratories, this resource can be applied usually to a limited proportion of patients (105). Inertial sensors for capturing and recording movement during sleep are increasingly used and this is a rapidly growing field because progress in technology continuously offers easier to manage and portable devices that provide great amounts of information. The great advantage of these objective methods is that they furnish genuine measures providing real numbers based on physical phenomena.
The main disadvantages of rating scales are the influence of subjectivity in score assignment and the ordinal level of measurement (representing an ordered classification rather than real numerical values) adopted for the huge majority of them. Nonetheless, rating scales have the advantage of low cost, simplicity of application without need of special circumstances and settings, long time frame evaluation, and the multitude of facets they can assess. These characteristics have favored the wide use of these instruments in clinical daily practice and research.
Many of the rating scales described in this review are focused on the specific abnormal movement they evaluate and, therefore, do not include other elements for sleep assessment. However, the fact that several comprehensive scales that were designed to gather those components representing the most relevant aspects of the corresponding disorder, do not include sleep evaluations even when sleep disorders are frequently present in such condition, is striking. In general, it seems that the field of motor disorders has difficulty recognizing the presence of non-motor manifestations as disturbances causing important health problems to patients. The existence of similar non-motor symptoms in the general population (e.g., insomnia), although usually with lower prevalence and severity, may explain why these symptoms remained hidden to the attention of clinicians interested in movement disorders. In turn, the lack of systematic screening of these non-motor problems, has possibly led to the infradiagnosis and treatment of these disorders.
The present review offers a rapid and pragmatic vision of the properties of the most used rating scales in those movement disorders with related sleep disorders and reflects how most scales do not cover the simultaneous evaluation of sleep disturbances. The inclusion of instruments for screening and appraisal of sleep disorders in the assessment of patients with, for example, essential tremor or chronic tics, and the development of new rating scales including items and domains for evaluation of sleep disorders in movement disorders will help to recognize the magnitude of the problem this combination represents.
CR-B and MF conception and design of the study and wrote the first draft of the manuscript. MK, RB, and PM-M revised the work critically for important intellectual content. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Hobart JC, Cano SJ, Zajicek JP, Thompson AJ. Rating scales as outcome measures for clinical trials in neurology: problems, solutions, and recommendations. Lancet Neurol. (2007) 6:1094–105. doi: 10.1016/S1474-4422(07)70290-9
2. Giannoccaro MP, Antelmi E, Plazzi G. Sleep and movement disorders. Curr Opin Neurol. (2013) 26:428–34. doi: 10.1097/WCO.0b013e3283632cef
3. Abbott SM, Videnovic A. Sleep disorders in atypical Parkinsonism. Mov Disord Clin Pract. (2014) 1:89–96. doi: 10.1002/mdc3.12025
4. Iranzo A, Molinuevo JL, Santamaría J, Serradell M, Martí MJ, Valldeoriola F, et al. Rapid-eye-movement sleep behaviour disorder as an early marker for a neurodegenerative disorder: a descriptive study. Lancet Neurol. (2006) 5:572–7. doi: 10.1016/S1474-4422(06)70476-8
5. Martino D, Ganos C, Pringsheim TM. Tourette syndrome and chronic tic disorders: the clinical spectrum beyond tics. Int Rev Neurobiol. (2017) 134:1461–90. doi: 10.1016/bs.irn.2017.05.006
6. Zoccolella S, Savarese M, Lamberti P, Manni R, Pacchetti C, Logroscino G. Sleep disorders and the natural history of Parkinson's disease: the contribution of epidemiological studies. Sleep Med Rev. (2011) 15:41–50. doi: 10.1016/j.smrv.2010.02.004
7. Wu Y, Wang X, Wang C, Sun Q, Song N, Zhou Y, et al. Prevalence and clinical features of non-motor symptoms of essential tremor in Shanghai rural area. Parkinsonism Relat Disord. (2016) 22:15–20. doi: 10.1016/j.parkreldis.2015.10.617
8. Kurtis MM, Balestrino R, Rodriguez-Blazquez C, Forjaz MJ, Martinez-Martin P. A review of scales to evaluate sleep disturbances in movement disorders. Front Neurol. (2018) 9:369. doi: 10.3389/fneur.2018.00369
9. Movement Disorders Society. MDS Rating Scales [Internet]. Available online at: http://www.movementdisorders.org/MDS/Education/Rating-Scales.htm (Cited November 10, 2017).
11. Barnes TRE. The barnes akathisia rating scale–revisited. J Psychopharmacol. (2003) 17:365–70. doi: 10.1177/0269881103174013
12. Teixeira AL, Maia DP, Cardoso F. UFMG Sydenham's chorea rating scale (USCRS): reliability and consistency. Mov Disord. (2005) 20:585–91. doi: 10.1002/mds.20377
13. Unified Huntington's disease rating scale: reliability and consistency. Mov Disord. (1996) 11:136–42. doi: 10.1002/mds.870110204
14. Comella CL, Leurgans S, Wuu J, Stebbins GT, Chmura T, Dystonia study group. rating scales for dystonia: a multicenter assessment. Mov Disord. (2003) 18:303–12. doi: 10.1002/mds.10377
15. Burke RE, Fahn S, Marsden CD, Bressman SB, Moskowitz C, Friedman J. Validity and reliability of a rating scale for the primary torsion dystonias. Neurology (1985) 35:73–7.
16. Consky E, Lang A. Clinical assessments of patients with cervical dystonia. In: Jankovic J, Hallett M, editors. Therapy with Botulinum Toxin. New York, NY: Marcel Dekker (1994). p. 221–37.
17. Fahn S, Tolosa E, Marín C. Clinical rating scale for tremor. In: Jankovic J, Tolosa E, editors. Parkinson's Disease and Movement Disorders. Baltimore, MD: Williams and Wilkins (1993). p. 271–80.
18. Stacy MA, Elble RJ, Ondo WG, Wu S-C, Hulihan J, TRS study group. Assessment of interrater and intrarater reliability of the Fahn-Tolosa-Marin Tremor Rating Scale in essential tremor. Mov Disord. (2007) 22:833–8. doi: 10.1002/mds.21412
19. Bain PG, Findley LJ. Assessing Tremor Severity: A Clinical Handbook. London: Gordon-Smith (1993).
20. Louis ED, Ottman R, Ford B, Pullman S, Martinez M, Fahn S, et al. The Washington heights-inwood genetic study of essential tremor: methodologic issues in essential-tremor research. Neuroepidemiology (1997) 16:124–33.
21. Elble R, Comella C, Fahn S, Hallett M, Jankovic J, Juncos JL, et al. Reliability of a new scale for essential tremor. Mov Disord. (2012) 27:1567–9. doi: 10.1002/mds.25162
22. Wenning GK, Tison F, Seppi K, Sampaio C, Diem A, Yekhlef F, et al. Development and validation of the Unified Multiple System Atrophy Rating Scale (UMSARS). Mov Disord. (2004) 19:1391–402. doi: 10.1002/mds.20255
23. Frucht SJ, Leurgans SE, Hallett M, Fahn S. The unified myoclonus rating scale. Adv Neurol. (2002) 89:361–76.
24. Goetz CG, Fahn S, Martinez-Martin P, Poewe W, Sampaio C, Stebbins GT, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS): process, format, and clinimetric testing plan. Mov Disord. (2007) 22:41–7. doi: 10.1002/mds.21198
25. Chaudhuri KR, Martinez-Martin P, Brown RG, Sethi K, Stocchi F, Odin P, et al. The metric properties of a novel non-motor symptoms scale for Parkinson's disease: results from an international pilot study. Mov Disord. (2007) 22:1901–11. doi: 10.1002/mds.21596
26. Chaudhuri KR, Martinez-Martin P, Schapira AHV, Stocchi F, Sethi K, Odin P, et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson's disease: the NMSQuest study. Mov Disord. (2006) 21:916–23. doi: 10.1002/mds.20844
27. Marinus J, Visser M, Stiggelbout AM, Rabey JM, Martínez-Martín P, Bonuccelli U, et al. A short scale for the assessment of motor impairments and disabilities in Parkinson's disease: the SPES/SCOPA. J Neurol Neurosurg Psychiatry (2004) 75:388–95. doi: 10.1136/jnnp.2003.017509
28. Visser M, Marinus J, Stiggelbout AM, Van Hilten JJ. Assessment of autonomic dysfunction in Parkinson's disease: the SCOPA-AUT. Mov Disord. (2004) 19:1306–12. doi: 10.1002/mds.20153
29. Golbe LI, Ohman-Strickland PA. A clinical rating scale for progressive supranuclear palsy. Brain (2007) 130:1552–65. doi: 10.1093/brain/awm032
30. Leckman JF, Riddle MA, Hardin MT, Ort SI, Swartz KL, Stevenson J, et al. The yale global tic severity scale: initial testing of a clinician-rated scale of tic severity. J Am Acad Child Adolesc Psychiatry. (1989) 28:566–73.
31. Shapiro AK, Shapiro E. Controlled study of pimozide vs. placebo in Tourette's syndrome. J Am Acad Child Psychiatry (1984) 23:161–73.
32. Leckman JF, Towbin KE, Ort SI, Cohen DJ. Clinical assessment of tic disorders severity. In: Cohen DJ, Bruun RD, Leckman JF, editors. Tourette's Syndrome and Tic Disorders: Clinical Understanding and Treatment. New York, NY: John Wiley & Sons (1988).
33. Shytle RD, Silver AA, Sheehan KH, Wilkinson BJ, Newman M, Sanberg PR, et al. The Tourette's Disorder Scale (TODS): development, reliability, and validity. Assessment (2003) 10:273–87. doi: 10.1177/1073191103255497
34. Woods DW, Piacentini J, Himle MB, Chang S. Premonitory Urge for Tics Scale (PUTS): initial psychometric results and examination of the premonitory urge phenomenon in youths with Tic disorders. J Dev Behav Pediatr. (2005) 26:397–403.
35. Walters AS, Hening W, Rubinstein M, Chokroverty S. A clinical and polysomnographic comparison of neuroleptic-induced akathisia and the idiopathic restless legs syndrome. Sleep (1991) 14:339–45.
36. Moser AD, Epping E, Espe-Pfeifer P, Martin E, Zhorne L, Mathews K, et al. A survey-based study identifies common but unrecognized symptoms in a large series of juvenile Huntington's disease. Neurodegener Dis Manag. (2017) 7:307–15. doi: 10.2217/nmt-2017-0019
37. Piano C, Losurdo A, Della Marca G, Solito M, Calandra-Buonaura G, Provini F, et al. Polysomnographic findings and clinical correlates in huntington disease: a cross-sectional cohort study. Sleep (2015) 38:1489–95. doi: 10.5665/sleep.4996
38. Maskevich S, Jumabhoy R, Dao PDM, Stout JC, Drummond SPA. Pilot validation of ambulatory activity monitors for sleep measurement in Huntington's disease gene carriers. J Huntingt Dis. (2017) 6:249–53. doi: 10.3233/JHD-170251
39. Bellosta Diago E, Pérez Pérez J, Santos Lasaosa S, Viloria Alebesque A, Martínez Horta S, Kulisevsky J, et al. Circadian rhythm and autonomic dysfunction in presymptomatic and early Huntington's disease. Parkinsonism Relat Disord. (2017) 44:95–100. doi: 10.1016/j.parkreldis.2017.09.013
40. Baker CR, Domínguez D JF, Stout JC, Gabery S, Churchyard A, Chua P, et al. Subjective sleep problems in Huntington's disease: a pilot investigation of the relationship to brain structure, neurocognitive, and neuropsychiatric function. J Neurol Sci. (2016) 364:148–53. doi: 10.1016/j.jns.2016.03.021
41. Ben-Pazi H, Stoner JA, Cunningham MW. Dopamine receptor autoantibodies correlate with symptoms in Sydenham's chorea. PLoS ONE (2013) 8:e73516. doi: 10.1371/journal.pone.0073516
42. Fusco C, Ucchino V, Frattini D, Pisani F, Della Giustina E. Acute and chronic corticosteroid treatment of ten patients with paralytic form of Sydenham's chorea. Eur J Paediatr Neurol. (2012) 16:373–8. doi: 10.1016/j.ejpn.2011.12.005
43. Barreto LB, Maciel ROH, Maia DP, Teixeira AL, Cardoso F. Parkinsonian signs and symptoms in adults with a history of Sydenham's chorea. Parkinsonism Relat Disord. (2012) 18:595–7. doi: 10.1016/j.parkreldis.2011.11.002
44. Teixeira AL, Maia DP, Cardoso F. The initial testing and the discrimination property of the UFMG Sydenham's Chorea Rating Scale (USCRS). Arq Neuropsiquiatr. (2005) 63:825–7. doi: 10.1590/S0004-282X2005000500019
45. Siesling S, Zwinderman AH, van Vugt JP, Kieburtz K, Roos RA. A shortened version of the motor section of the Unified Huntington's disease rating scale. Mov Disord. (1997) 12:229–34. doi: 10.1002/mds.870120214
46. Mestre TA, van Duijn E, Davis AM, Bachoud-Lévi A-C, Busse M, Anderson KE, et al. Rating scales for behavioral symptoms in Huntington's disease: critique and recommendations. Mov Disord. (2016) 31:1466–78. doi: 10.1002/mds.26675
47. Youssov K, Dolbeau G, Maison P, Boissé M-F, Cleret De Langavant L, Roos R, et al. Unified Huntington's disease rating scale for advanced patients: validation and follow-up study. Mov Disord. (2013) 28:1717–23. doi: 10.1002/mds.25654
48. Torres JAKL, Rosales RL. Nonmotor symptoms in dystonia. Int Rev Neurobiol. (2017) 134:1335–71. doi: 10.1016/bs.irn.2017.05.003
49. Kuyper DJ, Parra V, Aerts S, Okun MS, Kluger BM. The non-motor manifestations of dystonia: a systematic review. Mov Disord. (2011) 26:1206–17. doi: 10.1002/mds.23709
50. Trotti LM, Esper CD, Feustel PJ, Bliwise DL, Factor SA. Excessive daytime sleepiness in cervical dystonia. Parkinsonism Relat Disord. (2009) 15:784–6. doi: 10.1016/j.parkreldis.2009.04.007
51. Sforza E, Montagna P, Defazio G, Lugaresi E. Sleep and cranial dystonia. Electroencephalogr Clin Neurophysiol. (1991) 79:166–9.
52. Albanese A, Sorbo FD, Comella C, Jinnah HA, Mink JW, Post B, et al. Dystonia rating scales: critique and recommendations. Mov Disord. (2013) 28:874–83. doi: 10.1002/mds.25579
53. Rohl B, Collins K, Morgan S, Cosentino S, Huey ED, Louis ED. Daytime sleepiness and nighttime sleep quality across the full spectrum of cognitive presentations in essential tremor. J Neurol Sci. (2016) 371:24–31. doi: 10.1016/j.jns.2016.10.006
54. Chunling W, Zheng X. Review on clinical update of essential tremor. Neurol Sci. (2016) 37:495–502. doi: 10.1007/s10072-015-2380-1
55. Louis ED. Non-motor symptoms in essential tremor: a review of the current data and state of the field. Parkinsonism Relat Disord. (2016) 22:S115–118. doi: 10.1016/j.parkreldis.2015.08.034
56. Sengul Y, Sengul HS, Yucekaya SK, Yucel S, Bakim B, Pazarci NK, et al. Cognitive functions, fatigue, depression, anxiety, and sleep disturbances: assessment of nonmotor features in young patients with essential tremor. Acta Neurol Belg. (2015) 115:281–7. doi: 10.1007/s13760-014-0396-6
57. Lenka A, Benito-León J, Louis ED. Is there a Premotor Phase of Essential Tremor? Tremor Other Hyperkinetic Mov. (2017) 7:498. doi: 10.7916/D80S01VK
58. Elble R, Bain P, Forjaz MJ, Haubenberger D, Testa C, Goetz CG, et al. Task force report: scales for screening and evaluating tremor: critique and recommendations. Mov Disord. (2013) 28:1793–800. doi: 10.1002/mds.25648
59. Bain PG, Findley LJ, Atchison P, Behari M, Vidailhet M, Gresty M, et al. Assessing tremor severity. J Neurol Neurosurg Psychiatry (1993) 56:868–73.
60. Louis ED, Barnes L, Wendt KJ, Ford B, Sangiorgio M, Tabbal S, et al. A teaching videotape for the assessment of essential tremor. Mov Disord. (2001) 16:89–93.
61. Louis ED, Ford B, Bismuth B. Reliability between two observers using a protocol for diagnosing essential tremor. Mov Disord. (1998) 13:287–93.
62. Louis ED, Agnew A, Gillman A, Gerbin M, Viner AS. Estimating annual rate of decline: prospective, longitudinal data on arm tremor severity in two groups of essential tremor cases. J Neurol Neurosurg Psychiatry (2011) 82:761–5. doi: 10.1136/jnnp.2010.229740
63. Frucht SJ, Bordelon Y, Houghton WH, Reardan D. A pilot tolerability and efficacy trial of sodium oxybate in ethanol-responsive movement disorders. Mov Disord. (2005) 20:1330–7. doi: 10.1002/mds.20605
64. Voller B, Lines E, McCrossin G, Artiles A, Tinaz S, Lungu C, et al. Alcohol challenge and sensitivity to change of the essential tremor rating assessment scale. Mov Disord. (2014) 29:555–8. doi: 10.1002/mds.25667
65. Chang WS, Chung JC, Kim JP, Chang JW. Simultaneous thalamic and posterior subthalamic electrode insertion with single deep brain stimulation electrode for essential tremor. Neuromodulation Technol Neural Interface (2013) 16:236–43. doi: 10.1111/j.1525-1403.2012.00503.x
66. Mostile G, Fekete R, Giuffrida JP, Yaltho T, Davidson A, Nicoletti A, et al. Amplitude fluctuations in essential tremor. Parkinsonism Relat Disord. (2012) 18:859–63. doi: 10.1016/j.parkreldis.2012.04.019
67. Ohshima Y, Nakayama H, Matsuyama N, Hokari S, Sakagami T, Sato T, et al. Natural course and potential prognostic factors for sleep-disordered breathing in multiple system atrophy. Sleep Med. (2017) 34:13–7. doi: 10.1016/j.sleep.2017.01.020
68. Videnovic A. Management of sleep disorders in Parkinson's disease and multiple system atrophy. Mov Disord. (2017) 32:659–68. doi: 10.1002/mds.26918
69. Palma J-A, Norcliffe-Kaufmann L, Kaufmann H. Diagnosis of multiple system atrophy. Auton Neurosci Basic Clin. (2017). 211:15–25. doi: 10.1016/j.autneu.2017.10.007
70. Krismer F, Seppi K, Tison F, Sampaio C, Zangerl A, Peralta C, et al. The unified multiple system atrophy rating scale: intrarater reliability. Mov Disord. (2012) 27:1683–5. doi: 10.1002/mds.25181
71. Guo XY, Cao B, Lei F, Huang L, Chen K, Song W, et al. Clinical and polysomnographic features of patients with multiple system atrophy in Southwest China. Sleep Breath (2013) 17:1301–7. doi: 10.1007/s11325-013-0839-y
72. Matsushima M, Yabe I, Takahashi I, Hirotani M, Kano T, Horiuchi K, et al. Validity and reliability of a pilot scale for assessment of multiple system atrophy symptoms. Cereb Ataxias (2017) 4:11. doi: 10.1186/s40673-017-0067-5
73. Matsushima M, Yabe I, Oba K, Sakushima K, Mito Y, Takei A, et al. Comparison of Different symptom assessment scales for multiple system atrophy. Cerebellum (2016) 15:190–200. doi: 10.1007/s12311-015-0686-4
74. Caviness JN, Brown P. Myoclonus: current concepts and recent advances. Lancet Neurol. (2004) 3:598–607. doi: 10.1016/S1474-4422(04)00880-4
75. Montagna P, Provini F, Vetrugno R. Propriospinal myoclonus at sleep onset. Neurophysiol Clin. (2006) 36(5–6):351–5. doi: 10.1016/j.neucli.2006.12.004
76. Salas Puig J, Tuñón A, Vidal JA, Mateos V, Guisasola LM, Lahoz CH. [Janz's juvenile myoclonic epilepsy: a little-known frequent syndrome. A study of 85 patients]. Med Clin. (1994) 103:684–9.
77. van Zijl JC, Beudel M, Elting J-WJ, de Jong BM, van der Naalt J, van den Bergh WM, et al. The inter-rater variability of clinical assessment in post-anoxic myoclonus. Tremor Other Hyperkinetic Mov. (2017) 7:470. doi: 10.7916/D81R6XBV
78. Hainque E, Vidailhet M, Cozic N, Charbonnier-Beaupel F, Thobois S, Tranchant C, et al. A randomized, controlled, double-blind, crossover trial of zonisamide in myoclonus-dystonia. Neurology (2016) 86:1729–35. doi: 10.1212/WNL.0000000000002631
79. Schrempf W, Brandt MD, Storch A, Reichmann H. Sleep disorders in Parkinson's disease. J Park Dis. (2014) 4:211–21. doi: 10.3233/JPD-130301
80. Fahn S, Elton R, UPDRS program members. Unified Parkinson's disease rating scale. In: Fahn S, Marsden C, Goldstein M, Calne D, editors. Recent Developments in Parkinson's Disease. Florham Park, NJ: Macmillan Healthcare Information (1987), p. 153–163.
81. Horváth K, Aschermann Z, Acs P, Bosnyák E, Deli G, Pál E, et al. Is the MDS-UPDRS a good screening tool for detecting sleep problems and daytime sleepiness in Parkinson's disease? Park Dis. (2014) 2014:806169. doi: 10.1155/2014/806169
82. Poewe W, Hauser RA, Lang A, ADAGIO Investigators. Effects of rasagiline on the progression of nonmotor scores of the MDS-UPDRS. Mov Disord. (2015) 30:589–92. doi: 10.1002/mds.26124
83. Jafari N, Pahwa R, Nazzaro JM, Arnold PM, Lyons KE. MDS-UPDRS to assess non-motor symptoms after STN DBS for Parkinson's disease. Int J Neurosci. (2016) 126:25–9. doi: 10.3109/00207454.2015.1065257
84. Horváth K, Aschermann Z, Ács P, Deli G, Janszky J, Komoly S, et al. Minimal clinically important difference on the Motor Examination part of MDS-UPDRS. Parkinsonism Relat Disord. (2015) 21:1421–6. doi: 10.1016/j.parkreldis.2015
85. Martinez-Martin P, Rodriguez-Blazquez C, Abe K, Bhattacharyya KB, Bloem BR, Carod-Artal FJ, et al. International study on the psychometric attributes of the non-motor symptoms scale in Parkinson disease. Neurology (2009) 73:1584–91. doi: 10.1212/WNL.0b013e3181c0d416
86. Chaudhuri KR, Martinez-Martin P, Antonini A, Brown RG, Friedman JH, Onofrj M, et al. Rotigotine and specific non-motor symptoms of Parkinson's disease: post hoc analysis of RECOVER. Parkinsonism Relat Disord. (2013) 19:660–5. doi: 10.1016/j.parkreldis.2013.02.018
87. Martinez-Martin P, Reddy P, Katzenschlager R, Antonini A, Todorova A, Odin P, et al. EuroInf: a multicenter comparative observational study of apomorphine and levodopa infusion in Parkinson's disease. Mov Disord. (2015) 30:510–6. doi: 10.1002/mds.26067
88. Perez Lloret S, Rossi M, Cardinali DP, Merello M. Validation of the sleep related items of the Non-motor Symptoms Questionnaire for Parkinson's disease (NMSQuest). Parkinsonism Relat Disord. (2008) 14:641–5. doi: 10.1016/j.parkreldis.2008.01.004
89. Chaudhuri KR, Prieto-Jurcynska C, Naidu Y, Mitra T, Frades-Payo B, Tluk S, et al. The nondeclaration of nonmotor symptoms of Parkinson's disease to health care professionals: an international study using the nonmotor symptoms questionnaire. Mov Disord. (2010) 25:704–9. doi: 10.1002/mds.22868
90. Chaudhuri KR, Sauerbier A, Rojo JM, Sethi K, Schapira AHV, Brown RG, et al. The burden of non-motor symptoms in Parkinson's disease using a self-completed non-motor questionnaire: a simple grading system. Parkinsonism Relat Disord. (2015) 21:287–91. doi: 10.1016/j.parkreldis.2014.12.031
91. Shulman LM, Armstrong M, Ellis T, Gruber-Baldini A, Horak F, Nieuwboer A, et al. Disability rating scales in Parkinson's disease: critique and recommendations. Mov Disord. (2016) 31:1455–65. doi: 10.1002/mds.26649
92. Martínez-Martín P, Benito-León J, Burguera JA, Castro A, Linazasoro G, Martínez-Castrillo JC, et al. The SCOPA-Motor Scale for assessment of Parkinson's disease is a consistent and valid measure. J Clin Epidemiol. (2005) 58:674–9. doi: 10.1016/j.jclinepi.2004.09.014
93. Marinus J, van der Heeden JF, van Hilten JJ. Calculating clinical progression rates in Parkinson's disease: methods matter. Parkinsonism Relat Disord. (2014) 20:1263–7. doi: 10.1016/j.parkreldis.2014.08.009
94. Martinez-Martín P, Rodriguez-Blazquez C, Paz S, Forjaz MJ, Frades-Payo B, Cubo E, et al. Parkinson symptoms and health related quality of life as predictors of costs: a longitudinal observational study with linear mixed model analysis. PLoS ONE (2015) 10:e0145310. doi: 10.1371/journal.pone.0145310
95. Evatt ML, Chaudhuri KR, Chou KL, Cubo E, Hinson V, Kompoliti K, et al. Dysautonomia rating scales in Parkinson's disease: sialorrhea, dysphagia, and constipation–critique and recommendations by movement disorders task force on rating scales for Parkinson's disease. Mov Disord. (2009) 24:635–46. doi: 10.1002/mds.22260
96. Pavy-Le Traon A, Amarenco G, Duerr S, Kaufmann H, Lahrmann H, Shaftman SR, et al. The Movement Disorders task force review of dysautonomia rating scales in Parkinson's disease with regard to symptoms of orthostatic hypotension. Mov Disord. (2011) 26:1985–992. doi: 10.1002/mds.23742
97. Montplaisir J, Petit D, Décary A, Masson H, Bédard MA, Panisset M, et al. Sleep and quantitative EEG in patients with progressive supranuclear palsy. Neurology (1997) 49:999–1003.
98. Hall DA, Forjaz MJ, Golbe LI, Litvan I, Payan CAM, Goetz CG, et al. Scales to assess clinical features of progressive supranuclear palsy: MDS task force report. Mov Disord Clin Pract. (2015) 2:127–34. doi: 10.1002/mdc3.12130
99. Hewer S, Varley S, Boxer AL, Paul E, Williams DR. AL-108-231 Investigators. Minimal clinically important worsening on the progressive supranuclear Palsy Rating Scale. Mov Disord. (2016) 31:1574–7. doi: 10.1002/mds.26694
100. Ghosh D, Rajan PV, Das D, Datta P, Rothner AD, Erenberg G. Sleep disorders in children with Tourette syndrome. Pediatr Neurol. (2014) 51:31–5. doi: 10.1016/j.pediatrneurol.2014.03.017
101. Martino D, Pringsheim TM, Cavanna AE, Colosimo C, Hartmann A, Leckman JF, et al. Systematic review of severity scales and screening instruments for tics: critique and recommendations. Mov Disord. (2017) 32:467–73. doi: 10.1002/mds.26891
102. Storch EA, De Nadai AS, Lewin AB, McGuire JF, Jones AM, Mutch PJ, et al. Defining treatment response in pediatric tic disorders: a signal detection analysis of the Yale global tic severity scale. J Child Adolesc Psychopharmacol. (2011) 21:621–7. doi: 10.1089/cap.2010.0149
103. Jeon S, Walkup JT, Woods DW, Peterson A, Piacentini J, Wilhelm S, et al. Detecting a clinically meaningful change in tic severity in Tourette syndrome: a comparison of three methods. Contemp Clin Trials (2013) 36:414–20. doi: 10.1016/j.cct.2013.08.012
104. Storch EA, Merlo LJ, Lehmkuhl H, Grabill KM, Geffken GR, Goodman WK, et al. Further psychometric examination of the Tourette's Disorder Scales. Child Psychiatry Hum Dev. (2007) 38:89–98. doi: 10.1007/s10578-006-0043-4
Keywords: movement disorders, sleep disorders, rating scales, Parkinson's disease, progressive supranuclear palsy
Citation: Rodríguez-Blázquez C, Forjaz MJ, Kurtis MM, Balestrino R and Martinez-Martin P (2018) Rating Scales for Movement Disorders With Sleep Disturbances: A Narrative Review. Front. Neurol. 9:435. doi: 10.3389/fneur.2018.00435
Received: 29 January 2018; Accepted: 23 May 2018;
Published: 07 June 2018.
Edited by:
Huifang Shang, Sichuan University, ChinaReviewed by:
Giovanna Calandra-Buonaura, Università degli Studi di Bologna, ItalyCopyright © 2018 Rodríguez-Blázquez, Forjaz, Kurtis, Balestrino and Martinez-Martin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carmen Rodríguez-Blázquez, Y3JvZGJAaXNjaWlpLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.