
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol. , 04 June 2018
Sec. Neuro-Otology
Volume 9 - 2018 | https://doi.org/10.3389/fneur.2018.00352
This article is part of the Research Topic Bilateral Vestibulopathy - Current Knowledge and Future Directions to Improve its Diagnosis and Treatment View all 20 articles
 Florence Lucieer1*
Florence Lucieer1* Stijn Duijn2
Stijn Duijn2 Vincent Van Rompaey3
Vincent Van Rompaey3 Angelica Pérez Fornos4
Angelica Pérez Fornos4 Nils Guinand4
Nils Guinand4 Jean Philippe Guyot4
Jean Philippe Guyot4 Herman Kingma1,5
Herman Kingma1,5 Raymond van de Berg1,5
Raymond van de Berg1,5
Objective: To systematically review the symptoms reported by patients with bilateral vestibulopathy (BV) in clinical studies and case reports. This would serve as the first step in establishing a validated patient-reported outcome measures (PROM) for BV.
Methods: A search on symptoms reported by patients with BV was performed in PubMed, and all publications covering these symptoms were included. Exclusion criteria comprised reviews and insufficient details about the frequency of occurrence of symptoms.
Results: 1,442 articles were retrieved. 88 studies were included (41 clinical studies, 47 case reports). In consensus, 68 descriptions of symptoms were classified into 6 common and generic symptoms. Frequency of symptoms in clinical studies and case reports were reviewed, respectively; imbalance (91 and 86%), chronic dizziness (58 and 62%), oscillopsia (50 and 70%), and recurrent vertigo (33 and 67%). BV could be accompanied by hearing loss (33 and 43%) and tinnitus (15 and 36%). 15 clinical studies and 10 case reports reported symptoms beyond vestibular and hearing deficits such as limited social activities, depression, concentration, and memory impairment and reduced quality of life in general.
Conclusion: The literature on BV symptomatology mainly focuses on classic symptoms such as imbalance and oscillopsia, while only few report additional symptoms such as cognitive memory impairment and performing dual tasks. In fact, none of the reviewed clinical studies and case reports provided a comprehensive overview of BV symptoms. To develop a validated PROM, qualitative research using semi-structured and unstructured interviews is needed to explore the full spectrum of BV symptoms.
Bilateral vestibulopathy (BV) is a heterogeneous chronic condition in which the vestibular function is bilaterally absent or reduced (1). BV can be due to a dysfunction of the vestibular organs, nerves, and/or the brain (1, 2). In 2017, consensus was reached by the Classification Committee of the Bárány Society about the diagnostic criteria of BV (3). Symptoms for diagnosis include unsteadiness when walking or standing, movement-induced blurred vision/oscillopsia during walking or quick head movements, or worsening of unsteadiness on uneven ground and/or darkness (1, 3, 4). However, clinical experience and current literature point to a wider variety of symptoms (5). For example, many patients report a negative impact on physical and social functioning, and compromised cognitive abilities (6–8).
At this moment, questionnaires like the dizziness handicap inventory (DHI) exist to quantify the dizziness symptoms. However, these questionnaires are not specific for vestibular loss (9). Therefore, the objective of this study was to systematically evaluate the nature and frequency of BV symptoms reported in clinical studies and case reports. This would serve as the first step in establishing validated patient-reported outcome measures (PROM) specifically for patients with BV (10). This is a tool to measure patient perceptions of their own functional status and well-being (11).
A systematic literature search was performed according to the PRISMA statement in the bibliographical database PubMed based on the following keywords: Bilateral[All Fields] AND ((Vestibular[All Fields] AND (Hypofunction[All Fields] OR Failure[All Fields] OR Loss[All Fields])) OR Vestibulopathy[All Fields]) (12). At the beginning, a full search was performed followed by entering some additional restrictions. The outcomes of this selection were first screened by title and then also by abstract. The last selection included a complete reading of the articles found. The selections and full article analysis was performed by the first two authors (Florence Lucieer and Stijn Duijn).
A requirement in the basic search was that all articles were written in English. All publications reporting on symptoms of patients with BV were considered, including all types of BV (central, peripheral, or mixed etiology).
Articles were excluded in case of animal studies, if they did not report on BV, if they did not report on symptoms of patients with BV, if no or insufficient details on the frequency of symptoms were available, and in case of systematic reviews, comments, errata, or books.
Exclusion criteria were the same as for title screening. In case an abstract was not available, the full article was screened to search for any of the exclusion criteria.
In case the full article was not available, the article was excluded. Whenever the inclusion or exclusion criterion of an article included only “unsteadiness” or “oscillopsia,” or “unsteadiness and oscillopsia,” the article was excluded, so few reported symptoms could lead to a bias of interpretation of the frequency of the symptoms.
Title selection, abstract selection, full read through selection, and the analysis of the included articles were performed by the first and second author (Florence Lucieer and Stijn Duijn). The list of articles found in the PubMed search was exported to EndNote X8 for Windows and Mac (Clarivate Analytics, Philadelphia). This Endnote library was then used to perform the title, abstract, and full article selection by the two researchers separately. After the title and abstract screening the articles of both researchers were combined and duplicates were removed. After full article selection, articles were combined. Discrepancies between the two authors were discussed and a consensus was reached about selecting the articles for data analysis. A Cohen’s kappa of the full article selection was calculated to evaluate the interrater reliability (13).
The nature and frequency of symptoms and the total number of patients were extracted by the first two authors and compiled using Microsoft Excel. If only percentages were reported, the authors were contacted to get the exact number of patients. The method of symptom collection in the articles was collected to assess risk of bias of the studies. Clinical studies and case reports were analyzed separately.
The primary outcome measure of this systematic review was a detailed overview regarding nature and frequency of symptoms of BV as reported in clinical studies and case reports. Three authors (Florence Lucieer, Stijn Duijn, and Raymond van de Berg) reviewed the list of descriptions. In consensus, these descriptions were categorized into common symptoms. The frequency of these common symptoms was calculated.
The search was conducted in the bibliographical database PubMed on October 25, 2017. The initial search resulted in 1,442 publications. For a schematic overview of the search strategy, see Figure 1. A high level of interrater reliability was reached on the full article selection with a Cohen’s kappa of 0.98. Finally, 1,385 unique patients from 41 clinical studies and 86 patients from 47 case reports were included (2, 5, 14–99). The characteristics of these articles can be found in Tables A1 and A2 in Supplementary Material.
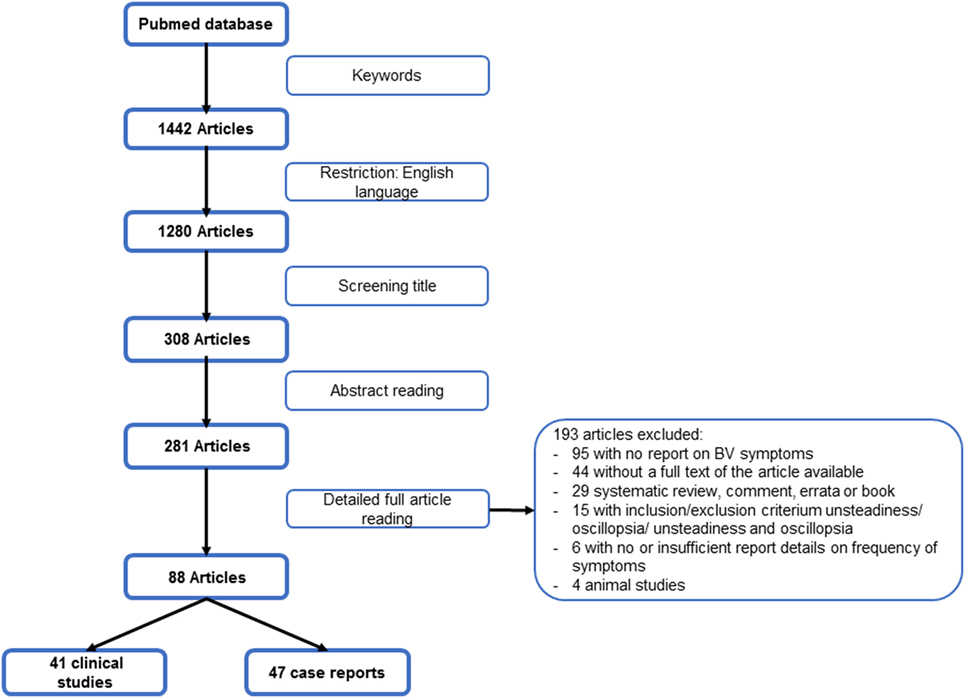
Figure 1. Flowchart search strategy.
Twenty-two of the clinical studies were European, 12 North-American, 4 Asian, 3 Australian, and 1 South-American, dated between 1984 and 2017. Twenty-one case reports were European, 13 North-American, 11 Asian, 1 Australian, and 1 South-American, originated from 1985 until 2017.
Sixty-eight descriptions of BV symptoms were retrieved. In consensus, these descriptions were classified into six universal symptoms: imbalance (including worsening in darkness or on uneven grounds), chronic dizziness, oscillopsia, recurrent vertigo, hearing loss, and tinnitus. Data from these six universal symptom classes can be found in Table A3 in Supplementary Material.
Symptoms found in clinical studies are presented in Table 1. Two times, two publications were merged in the results because of reporting duplicate data (24, 74, 97, 98). Imbalance was the most frequent symptom (91.4%). Fifteen clinical studies reported additional symptoms, for example, socio-economic impacts, depression, cognitive impairment, and increased risk of falling (5, 16, 27, 32, 43, 45, 54, 60, 63, 75, 76, 81–83, 90).
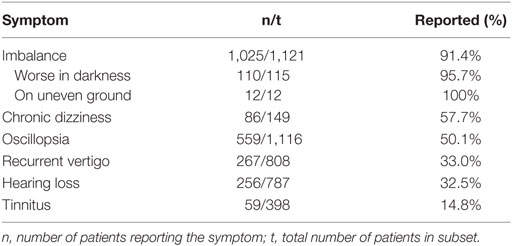
Table 1. Nature and frequency of most common symptoms reported by patients with bilateral vestibulopathy in clinical studies.
Symptoms found in case studies are presented in Table 2. Imbalance was the major symptom (86.1%). Ten case reports reported additional symptoms like sleep disturbances, unable to perform daily chores, and appearing to be depressed (18, 28, 30, 62, 67, 68, 70, 89, 91, 94). For a complete overview of additional symptoms in clinical studies and case reports, see Table 3.
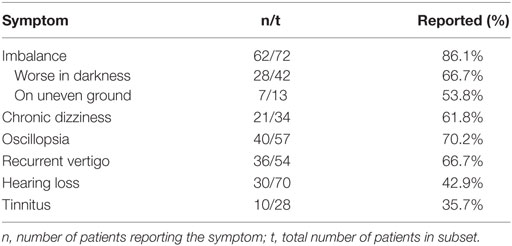
Table 2. Nature and frequency of most common symptoms reported by patients with bilateral vestibulopathy in case reports.
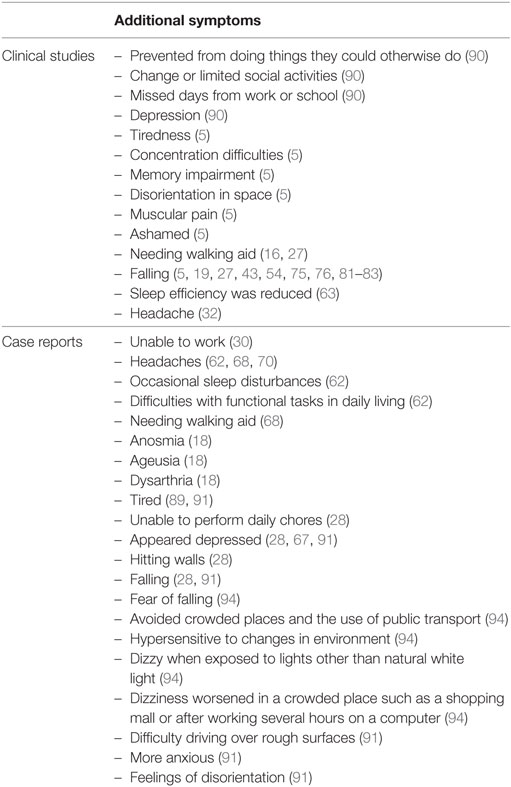
Table 3. Additional symptoms in bilateral vestibulopathy reported in articles.
After a structural review until October 2017, 41 clinical studies and 47 case reports were reviewed to determine the nature and frequency of symptoms experienced by patients with BV. No study was identified that created an inventory of patient-reported outcomes. Almost all patients suffered from imbalance, chronic dizziness, and oscillopsia, next to other inner ear problems like hearing loss and tinnitus. The high rate of imbalance and oscillopsia comply with the recent diagnostic criteria for BV (3). However, additional symptoms were rarely mentioned.
Hearing loss and tinnitus most likely shared the same etiology as BV or resulted from aging, rather than from vestibular dysfunction. A typical example for this is aminoglycoside toxicity is a well-known cause of sensorineural hearing loss and vestibular dysfunction (2, 97, 100). In addition, the average patient with BV in the literature was 60–62 years old and the prevalence of hearing loss in the United States is 25.1 and 42.7% for the age groups 55–64 and 65–84, respectively (101). The same conclusion could be drawn for recurrent vertigo. Vertigo is most likely an expression of the shared etiology, but is not the result of BV since an absent or reduced vestibular function is most likely not the cause of attacks of vertigo (2, 4).
Only 15 clinical studies and 10 case reports reported additional symptoms. The existence of these symptoms is supported by other literature that suggested that patients with BV could also suffer from cognitive deficits (7, 8), autonomic (102–104) and psychological symptoms (6, 105, 106), tiredness (6), visually induced dizziness (7, 107, 108), and impaired quality of life (6, 90, 106). Unfortunately, these symptoms could not reliably be quantified since they were not often mentioned in clinical studies and case reports. At this moment, it is uncertain why these symptoms were reported so infrequently. It could be hypothesized that these symptoms did have a low occurrence, that they were not part of routine history taking, or that patients were not aware of the link between their vestibular deficit and these types of symptoms (4). Therefore, structured patient interviews with open-ended questions should be conducted in which patients with BV are specifically asked to describe all of their symptoms and thereby evaluate in which words they describe their own symptoms, to determine the nature and frequency of all symptoms related to BV. This is necessary to develop PROM for BV (10).
At this moment, vestibular specific PROM exist like the DHI (109) and the vestibular disorders activities of daily living scale (VADL) (110). The DHI evaluates different aspects of vestibular complaints (function, physical, and emotional) and the VADL assesses the independency in activities of daily living. However, both questionnaires only focus on balance and do not assess the classic BV symptoms like oscillopsia, recurrent vertigo, hearing loss, and tinnitus. Therefore, there is also a need for PROM for BV specifically.
Several limitations of this systematic review were identified. Almost all articles gathered data differently and many of them were of retrospective nature. It was uncertain whether all publications used an open interview and whether all symptoms were explicitly mentioned or not. In addition, it was not possible to determine whether symptoms were mentioned but denied, or not even mentioned at all. Moreover, patients can describe the same complaint (e.g., dizziness and vertigo) differently. As a result, the same complaints could be categorized into different universal symptoms (4, 111). In addition, different articles used various diagnostic criteria for BV, resulting in a heterogeneous patient population, which made direct comparison of the patient population between articles difficult. Furthermore, it is known that BV is often misdiagnosed and missed (4, 90). This implies that even the percentages mentioned in literature do not reflect the real prevalence of the symptoms. Finally, only three clinical studies and one case report measured quality of life (e.g., DHI and HADS), therefore, outcomes could not be pooled for analysis (27, 30, 41, 42).
In this review, clinical studies and case reports provided complimentary information. Clinical studies were better in quantifying the established symptoms and case reports were better in giving an overview of the array of symptoms.
In the future, a qualitative research model would be of added value. This would allow getting a clear overview of all symptoms patients with BV experience, including additional symptoms.
Current literature on BV symptomatology mainly focuses on classic symptoms such as imbalance and oscillopsia, while only a few report additional symptoms such as cognitive memory impairment and dual tasking. In fact, none of the reviewed clinical studies and case reports provided a comprehensive overview of BV symptoms. To develop validated PROM, a qualitative research using semi-structured and unstructured interviews is needed to explore the full spectrum of BV symptoms.
All authors contributed extensively to the work presented in this paper. FL and SD conducted the analysis and wrote the manuscript. RB supervised the writing and edited the manuscript. HK supervised the writing and reviewed the manuscript. VR, AF, NG, and JP reviewed the manuscript.
The first author was supported through funding of MedEl. The remaining coauthors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer DS and handling Editor declared their shared affiliation.
The Supplementary Material for this article can be found online at https://www.frontiersin.org/articles/10.3389/fneur.2018.00352/full#supplementary-material.
1. Hain TC, Cherchi M, Yacovino DA. Bilateral vestibular loss. Semin Neurol (2013) 33(3):195–203. doi:10.1055/s-0033-1354597
2. Lucieer F, Vonk P, Guinand N, Stokroos R, Kingma H, van de Berg R. Bilateral vestibular hypofunction: insights in etiologies, clinical subtypes, and diagnostics. Front Neurol (2016) 7:26. doi:10.3389/fneur.2016.00026
3. Strupp M, Kim JS, Murofushi T, Straumann D, Jen JC, Rosengren SM, et al. Bilateral vestibulopathy: diagnostic criteria consensus document of the classification committee of the Barany Society. J Vestib Res (2017) 27(4):177–89. doi:10.3233/VES-170619
4. van de Berg R, van Tilburg M, Kingma H. Bilateral vestibular hypofunction: challenges in establishing the diagnosis in adults. ORL J Otorhinolaryngol Relat Spec (2015) 77(4):197–218. doi:10.1159/000433549
5. Miffon M, Guyot JP. Difficulties faced by patients suffering from total bilateral vestibular loss. ORL J Otorhinolaryngol Relat Spec (2015) 77(4):241–7. doi:10.1159/000433553
6. Guinand N, Boselie F, Guyot JP, Kingma H. Quality of life of patients with bilateral vestibulopathy. Ann Otol Rhinol Laryngol (2012) 121(7):471–7. doi:10.1177/000348941212100708
7. Hanes DA, McCollum G. Cognitive-vestibular interactions: a review of patient difficulties and possible mechanisms. J Vestib Res (2006) 16(3):75–91.
8. McCall AA, Yates BJ. Compensation following bilateral vestibular damage. Front Neurol (2011) 2:88. doi:10.3389/fneur.2011.00088
9. Gofrit SG, Mayler Y, Eliashar R, Bdolah-Abram T, Ilan O, Gross M. The association between vestibular physical examination, vertigo questionnaires, and the electronystagmography in patients with vestibular symptoms. Ann Otol Rhinol Laryngol (2017) 126(4):315–21. doi:10.1177/0003489417691298
10. Rothrock NE, Kaiser KA, Cella D. Developing a valid patient-reported outcome measure. Clin Pharmacol Ther (2011) 90(5):737–42. doi:10.1038/clpt.2011.195
11. Dawson J, Doll H, Fitzpatrick R, Jenkinson C, Carr AJ. The routine use of patient reported outcome measures in healthcare settings. BMJ (2010) 340:c186. doi:10.1136/bmj.c186
12. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg (2010) 8(5):336–41. doi:10.1016/j.ijsu.2010.02.007
13. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb) (2012) 22(3):276–82. doi:10.11613/BM.2012.031
14. Acierno MD, Trobe JD, Shepard NT, Cornblath WT, Disher MJ. Two types of oscillopsia in a patient with idiopathic vestibulopathy. J Neuroophthalmol (1997) 17(2):92–4.
15. Agrup C, Keir G, Thompson EJ, Bronstein AM. Systemic autoantibodies against discrete inner ear compartments in bilateral vestibular loss. Neurology (2005) 65(1):167. doi:10.1212/01.wnl.0000167609.12890.da
16. Ahmed RM, Hannigan IP, MacDougall HG, Chan RC, Halmagyi GM. Gentamicin ototoxicity: a 23-year selected case series of 103 patients. Med J Aust (2012) 196(11):701–4. doi:10.5694/mja11.10850
17. Albernaz PL, Cusin FS. The video head impulse test in a case of suspected bilateral loss of vestibular function. Int Arch Otorhinolaryngol (2016) 20(1):84–6. doi:10.1055/s-0034-1395999
18. Aran Yoo BS, Kattah JC. Superficial siderosis syndrome with progressive hearing loss and bilateral vestibular failure, 51 years after a neurosurgical procedure: diagnostic value of combined MRI and video head impulse test. J Neurol (2017) 264(2):391–3. doi:10.1007/s00415-016-8358-y
19. Baloh RW, Enrietto J, Jacobson KM, Lin A. Age-related changes in vestibular function: a longitudinal study. Ann N Y Acad Sci (2001) 942:210–9. doi:10.1111/j.1749-6632.2001.tb03747.x
20. Baloh RW, Honrubia V, Yee RD, Hess K. Changes in the human vestibulo-ocular reflex after loss of peripheral sensitivity. Ann Neurol (1984) 16(2):222–8. doi:10.1002/ana.410160209
21. Baloh RW, Jacobson K, Fife T. Familial vestibulopathy: a new dominantly inherited syndrome. Neurology (1994) 44(1):20–5. doi:10.1212/WNL.44.1.20
22. Baloh RW, Jacobson K, Honrubia V. Idiopathic bilateral vestibulopathy. Neurology (1989) 39(2 Pt 1):272–5. doi:10.1212/WNL.39.2.272
23. Baxter M, Agrawal Y. Vestibular dysfunction in Turner syndrome: a case report. Otol Neurotol (2014) 35(2):294–6. doi:10.1097/MAO.0b013e31829e16df
24. Brandt T, Schautzer F, Hamilton DA, Bruning R, Markowitsch HJ, Kalla R, et al. Vestibular loss causes hippocampal atrophy and impaired spatial memory in humans. Brain (2005) 128(Pt 11):2732–41. doi:10.1093/brain/awh617
25. Brantberg K, Lofqvist L. Preserved vestibular evoked myogenic potentials (VEMP) in some patients with walking-induced oscillopsia due to bilateral vestibulopathy. J Vestib Res (2007) 17(1):33–8.
26. Bringoux L, Schmerber S, Nougier V, Dumas G, Barraud PA, Raphel C. Perception of slow pitch and roll body tilts in bilateral labyrinthine-defective subjects. Neuropsychologia (2002) 40(4):367–72. doi:10.1016/S0028-3932(01)00103-8
27. Brown KE, Whitney SL, Wrisley DM, Furman JM. Physical therapy outcomes for persons with bilateral vestibular loss. Laryngoscope (2001) 111(10):1812–7. doi:10.1097/00005537-200110000-00027
28. Calder JH, Jacobson GP. Acquired bilateral peripheral vestibular system impairment: rehabilitative options and potential outcomes. J Am Acad Audiol (2000) 11(9):514–21.
29. Castellucci A, Piras G, Brandolini C, Modugno GC, Ferri GG. Waldenstrom’s macroglobulinemia presenting with bilateral vestibular loss: a case report. Braz J Otorhinolaryngol (2015) 81(5):571–5. doi:10.1016/j.bjorl.2015.03.010
30. Chen PY, Hsieh WL, Wei SH, Kao CL. Interactive wiimote gaze stabilization exercise training system for patients with vestibular hypofunction. J Neuroeng Rehabil (2012) 9:77. doi:10.1186/1743-0003-9-77
31. Choi SY, Kee HJ, Park JH, Kim HJ, Kim JS. Combined peripheral and central vestibulopathy. J Vestib Res (2014) 24(5–6):443–51. doi:10.3233/VES-140524
32. Choi SY, Kim HJ, Kim JS. Chasing dizzy chimera: diagnosis of combined peripheral and central vestibulopathy. J Neurol Sci (2016) 371:69–78. doi:10.1016/j.jns.2016.09.063
33. Constantinescu L, Schneider D, Claussen C. Vestibular evoked potentials in two patients with bilateral vestibular loss. Int Tinnitus J (1996) 2:45–57.
34. de Waele C, Shen Q, Magnani C, Curthoys IS. A novel saccadic strategy revealed by suppression head impulse testing of patients with bilateral vestibular loss. Front Neurol (2017) 8:419. doi:10.3389/fneur.2017.00419
35. Deroualle D, Toupet M, van Nechel C, Duquesne U, Hautefort C, Lopez C. Anchoring the self to the body in bilateral vestibular failure. PLoS One (2017) 12(1):e0170488. doi:10.1371/journal.pone.0170488
36. Durrant JD, Furman JM. Long-latency rotational evoked potentials in subjects with and without bilateral vestibular loss. Electroencephalogr Clin Neurophysiol (1988) 71(4):251–6. doi:10.1016/0168-5597(88)90024-X
37. Finn S, Dietzek M, Karvouniari P, Klingner CM, Neumann R, Guntinas-Lichius O, et al. Bilateral vestibulopathy with positive Tullio phenomenon. Laryngoscope (2017) 128(5):1223–5. doi:10.1002/lary.26690
38. Fujimoto C, Iwasaki S, Matsuzaki M, Murofushi T. Lesion site in idiopathic bilateral vestibulopathy: a galvanic vestibular-evoked myogenic potential study. Acta Otolaryngol (2005) 125(4):430–2. doi:10.1080/00016480410024668
39. Fujimoto C, Murofushi T, Chihara Y, Suzuki M, Yamasoba T, Iwasaki S. Novel subtype of idiopathic bilateral vestibulopathy: bilateral absence of vestibular evoked myogenic potentials in the presence of normal caloric responses. J Neurol (2009) 256(9):1488–92. doi:10.1007/s00415-009-5147-x
40. Fujimoto C, Murofushi T, Sugasawa K, Chihara Y, Ushio M, Yamasoba T, et al. Bilateral vestibulopathy with dissociated deficits in the superior and inferior vestibular systems. Ann Otol Rhinol Laryngol (2012) 121(6):383–8. doi:10.1177/000348941212100604
41. Ghulyan-Bedikian V, Paolino M, Paolino F. Short-term retention effect of rehabilitation using head position-based electrotactile feedback to the tongue: influence of vestibular loss and old-age. Gait Posture (2013) 38(4):777–83. doi:10.1016/j.gaitpost.2013.03.018
42. Gill-Body KM, Beninato M, Krebs DE. Relationship among balance impairments, functional performance, and disability in people with peripheral vestibular hypofunction. Phys Ther (2000) 80(8):748–58.
43. Gillespie MB, Minor LB. Prognosis in bilateral vestibular hypofunction. Laryngoscope (1999) 109(1):35–41. doi:10.1097/00005537-199901000-00008
44. Grunfeld EA, Morland AB, Bronstein AM, Gresty MA. Adaptation to oscillopsia: a psychophysical and questionnaire investigation. Brain (2000) 123(Pt 2):277–90. doi:10.1093/brain/123.2.277
45. Herdman SJ, Blatt P, Schubert MC, Tusa RJ. Falls in patients with vestibular deficits. Am J Otol (2000) 21(6):847–51.
46. Hertel S, Schwaninger M, Helmchen C. Combined toxicity of penicillin and aspirin therapy may elicit bilateral vestibulopathy. Clin Neurol Neurosurg (2013) 115(7):1114–6. doi:10.1016/j.clineuro.2012.08.033
47. Hirvonen TP, Aalto H. Recovery of bilateral vestibular loss in Cogan’s syndrome – a case report. Otol Neurotol (2013) 34(9):1736–8. doi:10.1097/MAO.0b013e3182953154
48. Honrubia V, Marco J, Andrews J, Minser K, Yee RD, Baloh RW. Vestibulo-ocular reflexes in peripheral labyrinthine lesions: III. Bilateral dysfunction. Am J Otolaryngol (1985) 6(5):342–52. doi:10.1016/S0196-0709(85)80011-9
49. Hughes GB, Kinney SE, Hamid MA, Barna BP, Calabrese LH. Autoimmune vestibular dysfunction: preliminary report. Laryngoscope (1985) 95(8):893–7. doi:10.1288/00005537-198508000-00001
50. Ishiyama G, Ishiyama A, Kerber K, Baloh RW. Gentamicin ototoxicity: clinical features and the effect on the human vestibulo-ocular reflex. Acta Otolaryngol (2006) 126(10):1057–61. doi:10.1080/00016480600606673
51. Jahn K, Arbusow V, Zingler VC, Strupp M, Kretzschmar HA, Brandt T. Bilateral vestibular failure as an early sign in Creutzfeldt-Jakob disease. Ann N Y Acad Sci (2009) 1164:390–3. doi:10.1111/j.1749-6632.2008.03741.x
52. Jandl NM, Sprenger A, Wojak JF, Gottlich M, Munte TF, Kramer UM, et al. Dissociable cerebellar activity during spatial navigation and visual memory in bilateral vestibular failure. Neuroscience (2015) 305:257–67. doi:10.1016/j.neuroscience.2015.07.089
53. Jansen NL, Feuerecker R, Becker-Bense S, Zwergal A, Wulff M, Xiong G, et al. Assessment of cerebral dopamine D 2/3 formula-receptors in patients with bilateral vestibular failure. J Vestib Res (2014) 24(5–6):403–13. doi:10.3233/VES-140526
54. Janssen M, Stokroos R, Aarts J, van Lummel R, Kingma H. Salient and placebo vibrotactile feedback are equally effective in reducing sway in bilateral vestibular loss patients. Gait Posture (2010) 31(2):213–7. doi:10.1016/j.gaitpost.2009.10.008
55. Jung I, Choi SY, Kim HJ, Kim JS. Delayed vestibulopathy after heat exposure. J Neurol (2017) 264(1):49–53. doi:10.1007/s00415-016-8322-x
56. Kagoya R, Iwasaki S, Chihara Y, Ushio M, Tsuji S, Murofushi T, et al. Cephalic tetanus presenting as acute vertigo with bilateral vestibulopathy. Acta Otolaryngol (2011) 131(3):334–6. doi:10.3109/00016489.2010.526144
57. Kang KW, Lee C, Kim SH, Cho HH, Lee SH. Bilateral vestibulopathy documented by video head impulse tests in superficial siderosis. Otol Neurotol (2015) 36(10):1683–6. doi:10.1097/MAO.0000000000000865
58. Kapoula Z, Gaertner C, Yang Q, Denise P, Toupet M. Vergence and standing balance in subjects with idiopathic bilateral loss of vestibular function. PLoS One (2013) 8(6):e66652. doi:10.1371/journal.pone.0066652
59. Kim S, Oh YM, Koo JW, Kim JS. Bilateral vestibulopathy: clinical characteristics and diagnostic criteria. Otol Neurotol (2011) 32(5):812–7. doi:10.1097/MAO.0b013e31821a3b7d
60. Lekhel H, Popov K, Bronstein A, Gresty M. Postural responses to vibration of neck muscles in patients with uni- and bilateral vestibular loss. Gait Posture (1998) 7(3):228–36. doi:10.1016/S0966-6362(98)00012-5
61. Lempert T, Gianna CC, Gresty MA, Bronstein AM. Effect of otolith dysfunction. Impairment of visual acuity during linear head motion in labyrinthine defective subjects. Brain (1997) 120(Pt 6):1005–13. doi:10.1093/brain/120.6.1005
62. MacDougall HG, Moore ST, Black RA, Jolly N, Curthoys IS. On-road assessment of driving performance in bilateral vestibular-deficient patients. Ann N Y Acad Sci (2009) 1164:413–8. doi:10.1111/j.1749-6632.2008.03733.x
63. Martin T, Moussay S, Bulla I, Bulla J, Toupet M, Etard O, et al. Exploration of circadian rhythms in patients with bilateral vestibular loss. PLoS One (2016) 11(6):e0155067. doi:10.1371/journal.pone.0155067
64. Matsuzaki M, Murofushi T. Vestibular evoked myogenic potentials in patients with idiopathic bilateral vestibulopathy. Report of three cases. ORL J Otorhinolaryngol Relat Spec (2001) 63(6):349–52. doi:10.1159/000055772
65. Minor LB. Gentamicin-induced bilateral vestibular hypofunction. JAMA (1998) 279(7):541–4. doi:10.1001/jama.279.7.541
66. Moon M, Chang SO, Kim MB. Diverse clinical and laboratory manifestations of bilateral vestibulopathy. Laryngoscope (2017) 127(1):E42–9. doi:10.1002/lary.25946
67. Nuti D, Passero S, Di Girolamo S. Bilateral vestibular loss in vertebrobasilar dolichoectasia. J Vestib Res (1996) 6(2):85–91. doi:10.1016/0957-4271(95)02010-1
68. Pollak L, Milo R, Kossych V, Rabey MJ, Shapira E. Bilateral vestibular failure as a unique presenting sign in carcinomatous meningitis: case report. J Neurol Neurosurg Psychiatry (2001) 70(5):704–5. doi:10.1136/jnnp.70.5.704
69. Rinne T, Bronstein AM, Rudge P, Gresty MA, Luxon LM. Bilateral loss of vestibular function: clinical findings in 53 patients. J Neurol (1998) 245(6–7):314–21. doi:10.1007/s004150050225
70. Robinson BS, Cook JL, Richburg CM, Price SE. Use of an electrotactile vestibular substitution system to facilitate balance and gait of an individual with gentamicin-induced bilateral vestibular hypofunction and bilateral transtibial amputation. J Neurol Phys Ther (2009) 33(3):150–9. doi:10.1097/NPT.0b013e3181a79373
71. Ruehl RM, Guerkov R. Amiodarone-induced gait unsteadiness is revealed to be bilateral vestibulopathy. Eur J Neurol (2017) 24(2):e7–8. doi:10.1111/ene.13203
72. Rust H, Peters N, Allum JHJ, Wagner B, Honegger F, Baumann T. VEMPs in a patient with cerebellar ataxia, neuropathy and vestibular areflexia (CANVAS). J Neurol Sci (2017) 378:9–11. doi:10.1016/j.jns.2017.04.029
73. Sargent EW, Goebel JA, Hanson JM, Beck DL. Idiopathic bilateral vestibular loss. Otolaryngol Head Neck Surg (1997) 116(2):157–62. doi:10.1016/S0194-5998(97)70318-8
74. Schautzer F, Hamilton D, Kalla R, Strupp M, Brandt T. Spatial memory deficits in patients with chronic bilateral vestibular failure. Ann N Y Acad Sci (2003) 1004:316–24. doi:10.1196/annals.1303.029
75. Schlick C, Schniepp R, Loidl V, Wuehr M, Hesselbarth K, Jahn K. Falls and fear of falling in vertigo and balance disorders: a controlled cross-sectional study. J Vestib Res (2016) 25(5–6):241–51. doi:10.3233/VES-150564
76. Schniepp R, Schlick C, Schenkel F, Pradhan C, Jahn K, Brandt T, et al. Clinical and neurophysiological risk factors for falls in patients with bilateral vestibulopathy. J Neurol (2017) 264(2):277–83. doi:10.1007/s00415-016-8342-6
77. Schuler O, Strupp M, Arbusow V, Brandt T. A case of possible autoimmune bilateral vestibulopathy treated with steroids. J Neurol Neurosurg Psychiatry (2003) 74(6):825. doi:10.1136/jnnp.74.6.825
78. Smith JH, Stovall KC, Coons S, Fife TD. Bilateral vestibular hypofunction in neurosarcoidosis: a case report. Ear Nose Throat J (2011) 90(1):E1–3.
79. Spiegel R, Kalla R, Classen J, Bardins S, Anciaes da Silva F, Farahmand P, et al. Aminopyridine treatment in a patient with bilateral vestibular failure and cryptogenic downbeat nystagmus. J Neuroophthalmol (2012) 32(2):190. doi:10.1097/WNO.0b013e31824f397f
80. Strupp M, Jahn K, Brandt T. Another adverse effect of aspirin: bilateral vestibulopathy. J Neurol Neurosurg Psychiatry (2003) 74(5):691. doi:10.1136/jnnp.74.5.691
81. Suarez H, Sotta G, San Roman C, Arocena S, Ferreira E, Geisinger D, et al. Postural response characterization in elderly patients with bilateral vestibular hypofunction. Acta Otolaryngol (2013) 133(4):361–7. doi:10.3109/00016489.2012.739731
82. Swanenburg J, Zurbrugg A, Straumann D, Hegemann SCA, Palla A, de Bruin ED. A pilot study investigating the association between chronic bilateral vestibulopathy and components of a clinical functional assessment tool. Physiother Theory Pract (2017) 33(6):454–61. doi:10.1080/09593985.2017.1323362
83. Szmulewicz DJ, Waterston JA, Halmagyi GM, Mossman S, Chancellor AM, McLean CA, et al. Sensory neuropathy as part of the cerebellar ataxia neuropathy vestibular areflexia syndrome. Neurology (2011) 76(22):1903–10. doi:10.1212/WNL.0b013e31821d746e
84. Tang L, Schubert M, Marlowe A, Weinreich H. Bilateral hearing and vestibular loss in a patient with untreated chronic myeloid leukemia. JAMA Otolaryngol Head Neck Surg (2017) 143(7):736–7. doi:10.1001/jamaoto.2017.0283
85. Tuo KS, Cheng YY, Kao CL. Vestibular rehabilitation in a patient with whiplash-associated disorders. J Chin Med Assoc (2006) 69(12):591–5. doi:10.1016/S1726-4901(09)70336-3
86. van de Berg R, Guinand N, Guyot JP, Kingma H, Stokroos RJ. The modified ampullar approach for vestibular implant surgery: feasibility and its first application in a human with a long-term vestibular loss. Front Neurol (2012) 3:18. doi:10.3389/fneur.2012.00018
87. van Kerckhoven G, Mert A, De Ru JA. Treatment of vertigo and postural instability using visual illusions. J Laryngol Otol (2014) 128(11):1005–7. doi:10.1017/S0022215114002254
88. van Leeuwen RB, Smits BW, Rodenburg RJ, van Engelen BG. Bilateral vestibulopathy aggravates balance and gait disturbances in sensory ataxic neuropathy, dysarthria, and ophthalmoparesis: a case report. J Clin Neuromuscul Dis (2016) 18(1):34–6. doi:10.1097/CND.0000000000000126
89. van Leeuwen RB, van Kooten B, de Cock AF. Bilateral vestibular hypofunction and Lyme disease: a causal link? Acta Neurol Belg (2017) 117(1):367–8. doi:10.1007/s13760-016-0658-6
90. Ward BK, Agrawal Y, Hoffman HJ, Carey JP, Della Santina CC. Prevalence and impact of bilateral vestibular hypofunction: results from the 2008 US National Health Interview Survey. JAMA Otolaryngol Head Neck Surg (2013) 139(8):803–10. doi:10.1001/jamaoto.2013.3913
91. Wenzel A, Ward BK, Schubert MC, Kheradmand A, Zee DS, Mantokoudis G, et al. Patients with vestibular loss, Tullio phenomenon, and pressure-induced nystagmus: vestibular atelectasis? Otol Neurotol (2014) 35(5):866–72. doi:10.1097/MAO.0000000000000366
92. Wester JL, Ishiyama A, Ishiyama G. Recurrent vestibular migraine vertigo attacks associated with the development of profound bilateral vestibulopathy: a case series. Otol Neurotol (2017) 38(8):1145–8. doi:10.1097/MAO.0000000000001486
93. Wiest G, Demer JL, Tian J, Crane BT, Baloh RW. Vestibular function in severe bilateral vestibulopathy. J Neurol Neurosurg Psychiatry (2001) 71(1):53–7. doi:10.1136/jnnp.71.1.53
94. Wong RS, Abdul Kadir SY. An unusual case of bilateral vestibulopathy, chronic subjective dizziness and spondyloarthropathy. Gen Hosp Psychiatry (2015) 37(4):372.e3–4. doi:10.1016/j.genhosppsych.2015.03.011
95. Yetiser S. Bilateral cochleovestibulopathy due to internal auditory canal metastasis in a patient with stomach cancer. J Int Adv Otol (2016) 12(3):353–5. doi:10.5152/iao.2016.2762
96. Yukawa K, Hagiwara A, Ogawa Y, Nishiyama N, Shimizu S, Kawaguchi S, et al. Bilateral progressive hearing loss and vestibular dysfunction with inner ear antibodies. Auris Nasus Larynx (2010) 37(2):223–8. doi:10.1016/j.anl.2009.06.005
97. Zingler VC, Cnyrim C, Jahn K, Weintz E, Fernbacher J, Frenzel C, et al. Causative factors and epidemiology of bilateral vestibulopathy in 255 patients. Ann Neurol (2007) 61(6):524–32. doi:10.1002/ana.21105
98. Zingler VC, Weintz E, Jahn K, Huppert D, Cnyrim C, Brandt T, et al. Causative factors, epidemiology, and follow-up of bilateral vestibulopathy. Ann N Y Acad Sci (2009) 1164:505–8. doi:10.1111/j.1749-6632.2009.03765.x
99. Zingler VC, Weintz E, Jahn K, Mike A, Huppert D, Rettinger N, et al. Follow-up of vestibular function in bilateral vestibulopathy. J Neurol Neurosurg Psychiatry (2008) 79(3):284–8. doi:10.1136/jnnp.2007.122952
100. Rybak LP, Whitworth CA. Ototoxicity: therapeutic opportunities. Drug Discov Today (2005) 10(19):1313–21. doi:10.1016/S1359-6446(05)03552-X
101. Cruickshanks KJ, Tweed TS, Wiley TL, Klein BE, Klein R, Chappell R, et al. The 5-year incidence and progression of hearing loss: the epidemiology of hearing loss study. Arch Otolaryngol Head Neck Surg (2003) 129(10):1041–6. doi:10.1001/archotol.129.10.1041
102. Balaban CD. Projections from the parabrachial nucleus to the vestibular nuclei: potential substrates for autonomic and limbic influences on vestibular responses. Brain Res (2004) 996(1):126–37. doi:10.1016/j.brainres.2003.10.026
103. Highstein SM, Holstein GR. The anatomical and physiological framework for vestibular prostheses. Anat Rec (Hoboken) (2012) 295(11):2000–9. doi:10.1002/ar.22582
104. Holstein GR, Friedrich VL Jr, Kang T, Kukielka E, Martinelli GP. Direct projections from the caudal vestibular nuclei to the ventrolateral medulla in the rat. Neuroscience (2011) 175:104–17. doi:10.1016/j.neuroscience.2010.12.011
105. Grill E, Strupp M, Muller M, Jahn K. Health services utilization of patients with vertigo in primary care: a retrospective cohort study. J Neurol (2014) 261(8):1492–8. doi:10.1007/s00415-014-7367-y
106. Sun DQ, Ward BK, Semenov YR, Carey JP, Della Santina CC. Bilateral vestibular deficiency: quality of life and economic implications. JAMA Otolaryngol Head Neck Surg (2014) 140(6):527–34. doi:10.1001/jamaoto.2014.490
107. Cutfield NJ, Scott G, Waldman AD, Sharp DJ, Bronstein AM. Visual and proprioceptive interaction in patients with bilateral vestibular loss. Neuroimage Clin (2014) 4:274–82. doi:10.1016/j.nicl.2013.12.013
108. Guerraz M, Yardley L, Bertholon P, Pollak L, Rudge P, Gresty MA, et al. Visual vertigo: symptom assessment, spatial orientation and postural control. Brain (2001) 124(Pt 8):1646–56. doi:10.1093/brain/124.8.1646
109. Jacobson GP, Newman CW. The development of the dizziness handicap inventory. Arch Otolaryngol Head Neck Surg (1990) 116(4):424–7. doi:10.1001/archotol.1990.01870040046011
110. Cohen HS, Kimball KT. Development of the vestibular disorders activities of daily living scale. Arch Otolaryngol Head Neck Surg (2000) 126(7):881–7. doi:10.1001/archotol.126.7.881
Keywords: bilateral vestibulopathy, symptoms, dizziness, vertigo, imbalance, oscillopsia, bilateral vestibular hypofunction, patient-reported outcome measures
Citation: Lucieer F, Duijn S, Van Rompaey V, Pérez Fornos A, Guinand N, Guyot JP, Kingma H and van de Berg R (2018) Full Spectrum of Reported Symptoms of Bilateral Vestibulopathy Needs Further Investigation—A Systematic Review. Front. Neurol. 9:352. doi: 10.3389/fneur.2018.00352
Received: 31 January 2018; Accepted: 01 May 2018;
Published: 04 June 2018
Edited by:
Bryan Kevin Ward, Johns Hopkins University, United StatesReviewed by:
Christopher Schutt, Michigan Ear Institute, United StatesCopyright: © 2018 Lucieer, Duijn, Van Rompaey, Pérez Fornos, Guinand, Guyot, Kingma and van de Berg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Florence Lucieer, Zi5sdWNpZWVyQG11bWMubmw=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.