 Heikki Kiiski1*†
Heikki Kiiski1*† Ville Jalkanen1†
Ville Jalkanen1† Marika Ala-Peijari1Mari Hämäläinen2Eeva Moilanen2
Marika Ala-Peijari1Mari Hämäläinen2Eeva Moilanen2 Jukka Peltola3
Jukka Peltola3 Jyrki Tenhunen1,4
Jyrki Tenhunen1,4
- 1Critical Care Medicine Research Group, Department of Intensive Care, Tampere University Hospital, Tampere, Finland
- 2The Immunopharmacology Research Group, Faculty of Medicine and Life Sciences, University of Tampere, Tampere University Hospital, Tampere, Finland
- 3Department of Neurology, University of Tampere, Tampere University Hospital, Tampere, Finland
- 4Department of Surgical Sciences, Division of Anesthesiology and Intensive Care, Uppsala University, Uppsala, Sweden
Object: Aneurysmal subarachnoid hemorrhage (aSAH) is a common cause of death or long-term disability. Despite advances in neurocritical care, there is still only a very limited ability to monitor the development of secondary brain injury or to predict neurological outcome after aSAH. Soluble urokinase-type plasminogen activator receptor (suPAR) has shown potential as a prognostic and as an inflammatory biomarker in a wide range of critical illnesses since it displays an association with overall immune system activation. This is the first time that suPAR has been evaluated as a prognostic biomarker in aSAH.
Methods: In this prospective population-based study, plasma suPAR levels were measured in aSAH patients (n = 47) for up to 5 days. suPAR was measured at 0, 12, and 24 h after patient admission to the intensive care unit (ICU) and daily thereafter until he/she was transferred from the ICU. The patients’ neurological outcome was evaluated with the modified Rankin Scale (mRS) at 6 months after aSAH.
Results: suPAR levels (n = 47) during the first 24 h after aSAH were comparable in groups with a favorable (mRS 0–2) or an unfavorable (mRS 3–6) outcome. suPAR levels during the first 24 h were not associated with the findings in the primary brain CT, with acute hydrocephalus, or with antimicrobial medication use during 5-days’ follow-up. suPAR levels were associated with generally accepted inflammatory biomarkers (C-reactive protein, leukocyte count).
Conclusion: Plasma suPAR level was not associated with either neurological outcome or selected clinical conditions. While suPAR is a promising biomarker for prognostication in several conditions requiring intensive care, it did not reveal any value as a prognostic biomarker after aSAH.
Introduction
Urokinase plasminogen activator receptor (uPAR) (CD87) is present on various immunologically active cells, and its expression becomes elevated by inflammatory conditions and ischemic diseases (1, 2). The soluble form [soluble urokinase-type plasminogen activator receptor (suPAR)] in serum or plasma has emerged as an inflammatory biomarker capable of reflecting overall immune system activation (3, 4).
Previously, it has been shown that uPAR expression is induced in cerebral ischemia (5) and traumatic brain injury (6). Moreover, it has been claimed that uPAR may further augment cerebral injury (7). The induction of uPAR expression on the cell surface is believed to increase the levels of the soluble form of uPAR (8). Previously, suPAR has been shown to have predictive value in acutely, critically ill patients (9–13), including those who have suffered brain trauma (14). However, as far as we are aware, suPAR concentrations have not been evaluated as a prognostic biomarker in patients with subarachnoid hemorrhage.
Aneurysmal subarachnoid hemorrhage (aSAH) is a devastating disease causing long-term disability and up to 50% mortality (15). A significant proportion of the patients are young and previously healthy in comparison to individuals suffering other types of strokes (16). The main causes for poor prognosis are early brain injury and delayed cerebral ischemia (DCI), which cause permanent neurological deficits (17–19). The prediction of outcome is difficult and unsatisfactory as the secondary injury process in aSAH is multifactorial and incompletely understood (17, 20).
It is well established that inflammation plays a major role in vasospasm and subsequent DCI after aSAH (21, 22). A plethora of biomarkers have been studied in aSAH and DCI, e.g., neuron and astrocyte-specific markers (e.g., NSE, s100b, and UCHL-1), inflammatory biomarkers (e.g., IL-6, HMGB-1), and molecular adhesion and extracellular matrix markers (e.g., MMP-9) (16, 23–25). However, none of these putative biomarkers has so far proved to be useful in clinical decision-making. As ischemic events and inflammation are one characteristic feature of aSAH, it seemed reasonable to speculate that circulating plasma suPAR concentrations would increase during the acute stage after aSAH. Therefore, we hypothesized that either the plasma suPAR concentration or alternatively its changes over time could be useful in predicting the neurological outcome following aSAH.
Materials and Methods
The clinical data and blood samples from this patient cohort have been used in a previously published study (25). Following registration in Clinical Trials (NCT02026596, https://clinicaltrials.gov) and approval by the institutional ethics committee, we conducted a prospective, observational, single-center clinical study in Tampere University Hospital (Tampere, Finland) intensive care unit (ICU). The study population consisted of 61 consecutive adult aSAH patients admitted to our tertiary referral center during a 10-month period in 2013. Written informed consent was obtained from each of the patients or from their next of kin. All patients were treated according to standard in-house guidelines, which included intravenous nimodipine to prevent vasospasm and routine laboratory samples. In the final analyses, we chose to exclude those 14 patients with an unknown time of onset of symptoms or in whom the suPAR concentration was not measured during the first 24 h after the onset of symptoms. By including only those 47 patients with a known onset of clinical ictus and suPAR measurement during the first 24 h after the onset of symptoms, we eliminated the possibility that changes in suPAR concentrations would be attributable to different delays to hospital admission after aSAH.
The plasma suPAR concentration was measured at 0, 12, and 24 h after the admission and every 24 h for up to 5 days or until the patient was transferred from the ICU. World Federation of Neurological Surgeons Grading Scale, Fisher grade, and 6-month modified Rankin Scale (mRS) were used to evaluate the severity of aSAH and neurological recovery as previously described (25). The incidence of acute hydrocephalus was defined as the need for ventriculostomy on a clinical basis during the first 24 h after aSAH. Infection was defined as the need for antimicrobial medication during intensive care follow-up period.
As a part of our in-house guideline, an arterial cannula was routinely inserted. Blood samples for suPAR were collected into EDTA-containing tubes from the arterial cannula and the samples were immediately centrifuged for 10 min at 2,000 g at room temperature. After centrifugation, the plasma was collected and frozen at −70°C. After thawing, plasma suPAR levels were measured with a commercially available enzyme-linked immunosorbent assay kit according to the manufacturer’s instructions (suPARnostic®, ViroGates, Birkeroed, Denmark). The detection limit and inter-assay coefficient of variation were 0.45 ng/ml and 3.2%, respectively.
Before the statistical analysis, the suPAR measurements were divided into consecutive 24 h intervals, starting from the onset of symptoms. If suPAR was measured more than once per interval, the mean concentration was used. In a subgroup of 22 patients who had up to 5-days’ follow-up, we also checked whether the patient had been treated for DCI. Initiation of this treatment was based on clinical evaluation. Statistical analyses were performed with R (version 3.3.2 for Mac Os X). Fisher’s exact test was used with the categorical variables. Due to the non-normal distribution of measured biomarkers, Mann–Whitney U-test was used for between-group comparisons. Correlations were evaluated with Spearman’s correlation test. Linear regression was used in the time interval analyses.
Results
The basic characteristics of the study cohort and the subset of patients with 5-day follow-up have been previously reported (25). The time course of plasma suPAR concentrations in the two groups according to neurological outcome are depicted in Figure 1.
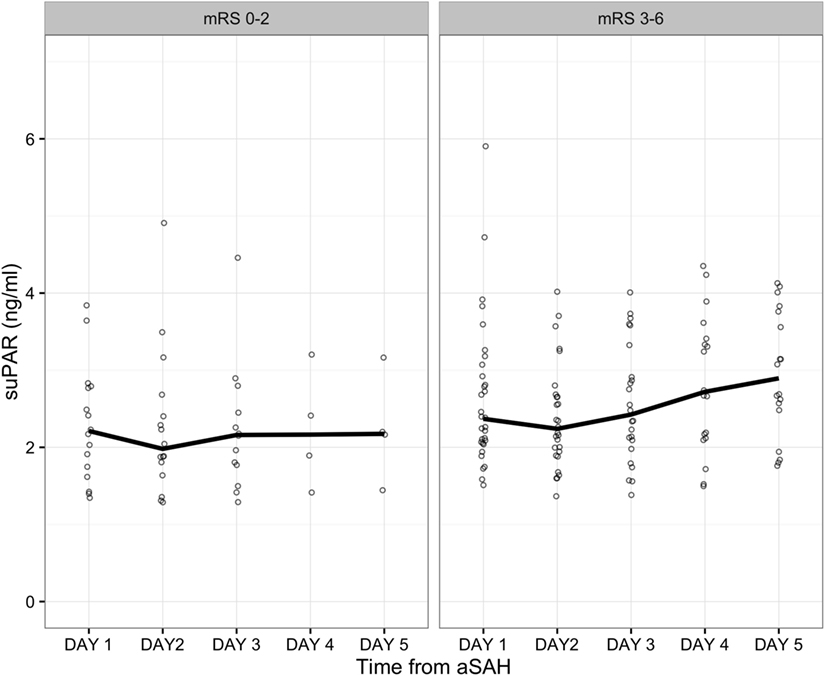
Figure 1. Soluble urokinase-type plasminogen activator receptor (suPAR) levels in all patients and at all time intervals. Values are grouped according to whether the patients had a favorable or an unfavorable neurological outcome. Dots represent individual patient values. The line represents group median.
Plasma suPAR concentrations during the first 24 h after aSAH were comparable in the groups with a favorable (mRS 0–2) and an unfavorable (mRS 3–6) outcome (Figure 2A). Similarly, no differences were detected in the suPAR levels between those patients presenting with severe (WFNS 4–5) vs. non-severe (WFNS 1–3) findings in terms of their clinical status on admission (Table 1). Furthermore, the plasma suPAR concentration during the first 24 h was not associated with the findings from the primary brain CT (Fisher grade) with acute hydrocephalus or with antimicrobial medication during the 5-days’ follow-up (Table 1). Age over 70 years was a strong predictor of an unfavorable neurological outcome, i.e., only one patient over 70 years experienced a neurologically favorable outcome (p = 0.037, Table 2).
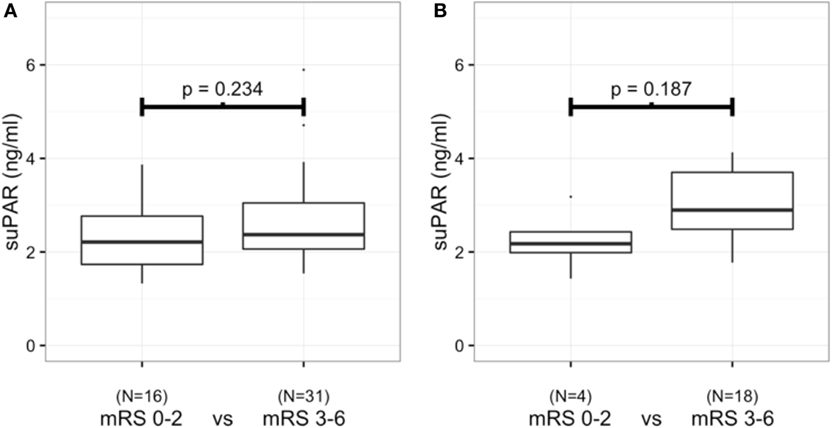
Figure 2. Soluble urokinase-type plasminogen activator receptor (suPAR) levels during the first 24 h after aneurysmal subarachnoid hemorrhage between patients (n = 47) with a favorable or an unfavorable neurological outcome (A). suPAR levels at the end of 5-day follow-up between patients (n = 22) with a favorable or an unfavorable neurological outcome (B).
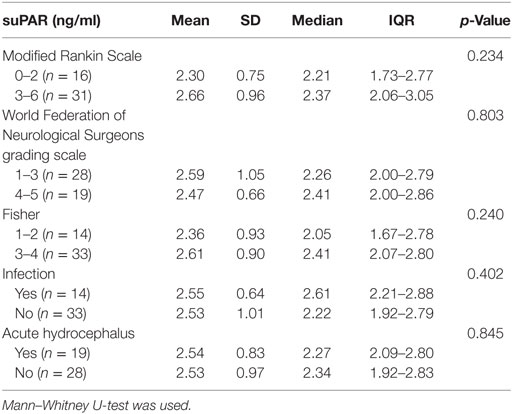
Table 1. Soluble urokinase-type plasminogen activator receptor (suPAR) concentrations (n = 47) within 24 h from aneurysmal subarachnoid hemorrhage and the association with selected clinical conditions.
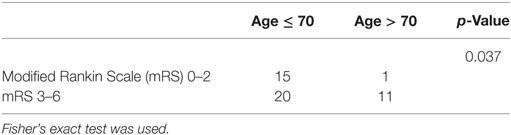
Table 2. The relationship between neurological outcome and age.
suPAR was measured daily up to 5 days after the admission unless the patient died or was transferred from the ICU. In the 22 patients in whom we had suPAR concentrations measured up to 5 days, four patients achieved a favorable neurological outcome (mRS 0–2). The linear regression did not detect any statistically significant elevation of suPAR levels during the 5-days’ follow-up in patients with either a favorable (mRS 0–2) or an unfavorable (mRS 3–6) neurological outcome (Figure 3). In addition, at day five, plasma suPAR concentrations were comparable in the two groups (Figure 2B).
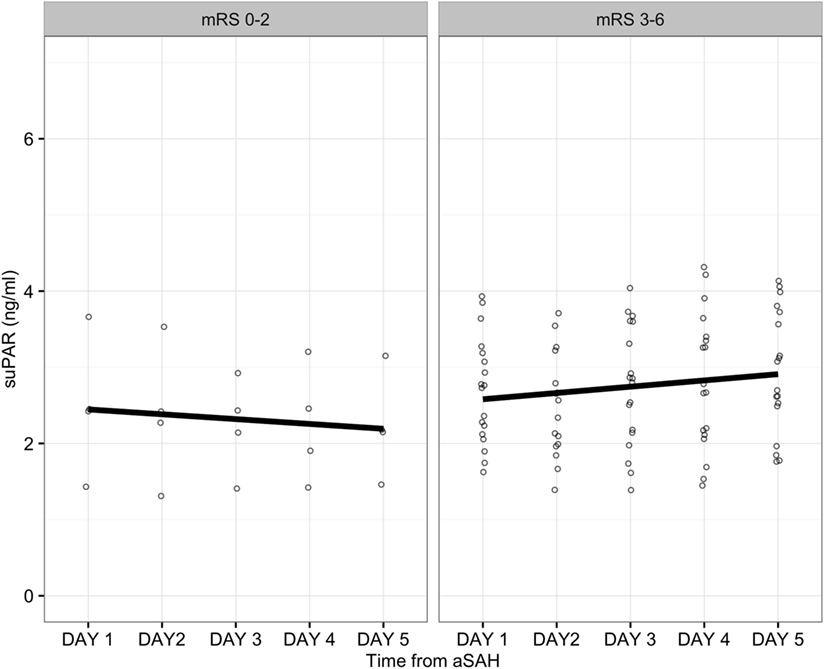
Figure 3. Soluble urokinase-type plasminogen activator receptor (suPAR) levels for patients with a follow-up of up to 5 days (n = 22). Dots represent individual patient values. Regression line is calculated with linear regression. Values are grouped according to favorable (p = 0.584) or non-favorable (p = 0.158) neurological outcome.
Delayed cerebral ischemia treatment was initiated in 16/22 patients during the hospital stay in the subgroup in which we had at least a 5-day ICU follow-up. Neither DCI treatment nor infection or acute hydrocephalus was associated with plasma suPAR concentrations (Table 3).
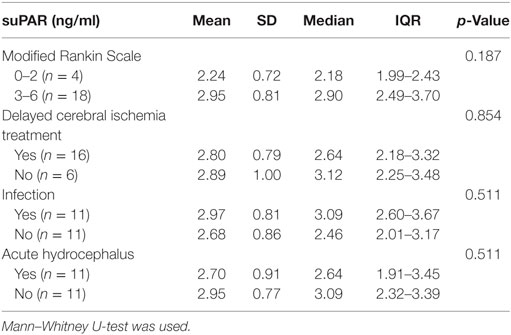
Table 3. Soluble urokinase-type plasminogen activator receptor (suPAR) levels on day five from aneurysmal subarachnoid hemorrhage patients (n = 22) in whom there was 5-days’ intensive care unit follow-up data and their association with selected clinical conditions.
The peak plasma suPAR concentration during the 5 days of follow-up was positively correlated with peak levels of C-reactive protein (CRP) (p = 0.039) and leukocyte numbers (p = 0.006). The plasma suPAR concentration was positively correlated with the leukocyte count during the first 24 h (p = 0.049). In contrast, suPAR levels were not associated with age (Table 4).
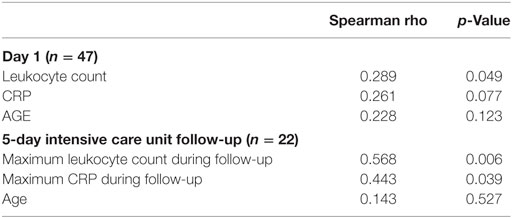
Table 4. Soluble urokinase-type plasminogen activator receptor and its association with leukocyte count, C-reactive protein (CRP), and age.
Discussion
The present study aimed to evaluate the potential prognostic value of plasma suPAR concentrations after an aSAH. In contrast to our working hypothesis, plasma suPAR did not show any association with neurological outcome, survival, acute hydrocephalus, clinical infection, or DCI in our patient cohort.
The inflammatory reaction and increase of systemic inflammatory mediators in aSAH is well documented (22, 26). Even though substantial evidence is accumulating in the literature highlighting the significant role of neuroinflammation in the outcome of aSAH, it is still unclear which, if any, inflammatory biomarkers can be used to guide clinical decision-making. The apparent biphasic nature of the inflammatory response after aSAH makes this challenge even more demanding. Neuroinflammation seems to have properties, which can be considered in some cases as protective, but in others, as deleterious, e.g., depending on the magnitude of the response, time-point after the ictus when activation of the inflammatory response occurs, and the type of cells recruited in the response (27). Hence, it is not surprising that there is inconsistency regarding the prognostic value of many inflammatory biomarkers such as IL-6 and HMGB1 after aSAH (19, 25, 28, 29). Nevertheless, although no biomarker has been identified, these studies have increased our understanding of the inflammatory process in aSAH and, in fact, also novel inflammatory biomarkers are claimed to have some prognostic potential, e.g., toll-like receptor 4 (30).
suPAR is considered as an inflammatory biomarker and mediator, a proposal that is well supported in the literature. Previously, increased serum or plasma suPAR levels have been postulated as a prognostic factor for poor outcome in critically ill patients with an inflammatory condition (31). The plasma suPAR concentrations in our aSAH cohort were low compared to septic and non-septic ICU patients with organ dysfunction (32). Nosocomial infections, organ dysfunction, and SIRS are frequent after aSAH (33, 34). Although the value of suPAR has been verified in infections and organ dysfunction (13, 32, 35), we did not detect high levels of suPAR, even later in the course of intensive care. One possible confounding factor distinguishing aSAH from other acute neurological conditions is that all of our patients received nimodipine to prevent DCI. Nimodipine has been shown to decrease plasminogen activator inhibitor 1 (PAI-1) activity (36). As PAI-1 is the major inhibitor of urokinase plasminogen activator (uPA), plasminogen activity and fibrinolysis may increase as a consequence of decreased PAI-1 activity. UPA can cleave the GPI-anchor on cell surface, but since a correct ratio of uPA is required for cleavage, it is possible that excess uPA due to nimodipine may inhibit the cleavage of suPAR from the cell surface (4, 8). suPAR also displays uPA dose dependence for binding to vitronectin (37), which may alter suPAR levels. Furthermore, previous reports have described suPAR-fragment release from activated neutrophils (38) and inhibition of neutrophil activation by two calcium antagonists, felodipine, and nimodipine (39), thereby supporting the concept that nimodipine may indeed be the factor modifying the suPAR response in our patient cohort. This speculative hypothesis and thus the potential direct effect of nimodipine on plasma suPAR concentrations could not be further tested/evaluated in our patient cohort. Moreover, as nimodipine is considered as part of current best practice, it would be unethical to establish a control group not receiving nimodipine after aSAH. Any further experiments to test this hypothesis will need to be conducted as preclinical/animal studies.
Overall, the suPAR response, i.e., the increase in the plasma concentrations of suPAR observed in this study, was rather modest in comparison with that observed in other critically ill patients, even though there was biochemically logical correlation between suPAR levels and generally accepted inflammatory biomarkers (CRP, leukocyte count). The correlation, however, was weak in comparison to previously reported results (35, 40) possibly indicating that there are numerous factors influencing inflammatory biomarkers and mediators in aSAH. In addition, although higher age was associated with poor outcome per se, in our patient cohort, we observed no correlation between age and plasma suPAR levels. This finding contradicts the results of several previous studies (10, 13, 41, 42). Finally, the low incidence (29.8%) of nosocomial infections in our patient cohort may partially explain the observed low plasma suPAR levels.
Even though serum suPAR levels have been shown to be elevated in ischemic stroke (43) and in cerebrospinal fluid (CSF) following disruption of the blood–brain barrier (44), no marked elevation of plasma suPAR was found in patients either diagnosed with DCI or acute hydrocephalus. Further analyses will be necessary to clarify potential importance of suPAR release to CSF in patients with DCI and acute hydrocephalus. In order to reveal the actual role of suPAR as a biomarker or mediator in aSAH, it would be worthwhile evaluating the potential value of suPAR levels in CSF in diagnosing ventriculitis related to ventriculostomy catheter.
Our study has some limitations. First, we had some patients that were lost to follow-up. In other words, we were not able to obtain samples late in the course of the acute illness as patients had either died or been transferred to some other health-care facility. These patients represent two extremes, i.e., either the best or the worst outcome, and this may have altered the results of our analysis. Second, our sample size was limited. In particular, only four patients with a favorable neurological outcome remained in the final analyses on day 5. However, some of our patients experienced mild whereas others had very severe presentations of aSAH. We followed suPAR levels during the whole ICU stay and suPAR levels were constantly low with no high peaks being observed. This suggests that aSAH does not induce high suPAR levels in plasma or they are depressed by some aspect of the treatment, for example, administration of the calcium antagonist. Third, our study is a single-center study. Although our unit is a tertiary referral hospital with a high patient influx, single-center bias is possible. Despite their relatively low numbers, it is of interest that those patients with a good neurological outcome had remarkably low plasma suPAR levels with a very small SD (Figure 2B). Our previous studies have suggested that while high suPAR levels may be prognostic for poor outcome, in contrast, a low plasma suPAR concentration is predictive of a good outcome (11, 45). In the present study, the number of patients is limited, but the same phenomenon may apply to aSAH.
Conclusion
This study reports the first population-based prospective, observational results evaluating plasma suPAR concentrations in aSAH. Plasma suPAR levels were not associated with neurological outcome or selected clinical conditions. While suPAR is a promising biomarker in several conditions requiring intensive care, based on this study, it does not seem to be useful as a prognostic biomarker in patients with aSAH.
Ethics Statement
The study was approved by the Ethics Committee of Pirkanmaa Hospital District. Written informed consent was obtained from each of the patients or from the next of kin.
Author Contributions
HK contributed to study conception, neurological outcome evaluations, statistical analyses, and drafted of the manuscript. VJ contributed to patient recruitment, statistical analyses, and drafted the manuscript. MA-P contributed to patient recruitment, evaluation of the initial clinical severity, evaluation of the initial computed tomography findings, and drafted the manuscript. MH contributed to the laboratory analysis of suPAR and drafted the manuscript. EM contributed to the laboratory analysis of suPAR and drafted the manuscript. JP contributed to neurological outcome evaluations, and drafted the manuscript. JT contributed to study conception, statistical analyses, and drafted the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The study was financially supported by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital.
References
1. Fuhrman B. The urokinase system in the pathogenesis of atherosclerosis. Atherosclerosis (2012) 222:8–14. doi:10.1016/j.atherosclerosis.2011.10.044
2. Smith HW, Marshall CJ. Regulation of cell signalling by uPAR. Nat Rev Mol Cell Biol (2010) 11:23–36. doi:10.1038/nrm2821
3. Backes Y, van der Sluijs KF, Tuip de Boer AM, Hofstra JJ, Vlaar AP, Determann RM, et al. Soluble urokinase-type plasminogen activator receptor levels in patients with burn injuries and inhalation trauma requiring mechanical ventilation: an observational cohort study. Crit Care (2011) 15:R270. doi:10.1186/cc10550
4. Thunø M, Macho B, Eugen-Olsen J. suPAR: the molecular crystal ball. Dis Markers (2009) 27:157–72. doi:10.3233/DMA-2009-0657
5. Persson M, Östling G, Smith G, Hamrefors V, Melander O, Hedblad B, et al. Soluble urokinase plasminogen activator receptor: a risk factor for carotid plaque, stroke, and coronary artery disease. Stroke (2014) 45:18–23. doi:10.1161/STROKEAHA.113.003305
6. Beschorner R, Schluesener HJ, Nguyen TD, Magdolen V, Luther T, Pedal I, et al. Lesion-associated accumulation of uPAR/CD87- expressing infiltrating granulocytes, activated microglial cells/macrophages and upregulation by endothelial cells following TBI and FCI in humans. Neuropathol Appl Neurobiol (2000) 26:522–7. doi:10.1046/j.0305-1846.2000.287.x
7. Nagai N, Okada K, Kawao N, Ishida C, Ueshima S, Collen D, et al. Urokinase-type plasminogen activator receptor (uPAR) augments brain damage in a murine model of ischemic stroke. Neurosci Lett (2008) 432:46–9. doi:10.1016/j.neulet.2007.12.004
8. Høyer-Hansen G, Ploug M, Behrendt N, Rønne E, Danø K. Cell-surface acceleration of urokinase-catalyzed receptor cleavage. Eur J Biochem (1997) 243:21–6. doi:10.1111/j.1432-1033.1997.0021a.x
9. Donadello K, Scolletta S, Taccone FS, Covajes C, Santonocito C, Cortes DO, et al. Soluble urokinase-type plasminogen activator receptor as a prognostic biomarker in critically ill patients. J Crit Care (2014) 29:144–9. doi:10.1016/j.jcrc.2013.08.005
10. Haupt TH, Petersen J, Ellekilde G, Klausen HH, Thorball CW, Eugen-Olsen J, et al. Plasma suPAR levels are associated with mortality, admission time, and Charlson Comorbidity Index in the acutely admitted medical patient: a prospective observational study. Crit Care (2012) 16:R130. doi:10.1186/cc11434
11. Jalkanen V, Yang R, Linko R, Huhtala H, Okkonen M, Varpula T, et al. suPAR and PAI-1 in critically ill, mechanically ventilated patients. Intensive Care Med (2013) 39:489–96. doi:10.1007/s00134-012-2730-x
12. Zimmermann HW, Koch A, Seidler S, Trautwein C, Tacke F. Circulating soluble urokinase plasminogen activator is elevated in patients with chronic liver disease, discriminates stage and aetiology of cirrhosis and predicts prognosis. Liver Int (2012) 32:500–9. doi:10.1111/j.1478-3231.2011.02665.x
13. Huttunen R, Syrjänen J, Vuento R, Hurme M, Huhtala H, Laine J, et al. Plasma level of soluble urokinase-type plasminogen activator receptor as a predictor of disease severity and case fatality in patients with bacteraemia: a prospective cohort study. J Intern Med (2011) 270:32–40. doi:10.1111/j.1365-2796.2011.02363.x
14. Yu L, Wu X, Wang H, Long D, Yang J, Zhang Y. Diagnostic and prognostic significance of suPAR in traumatic brain injury. Neurol India (2014) 62:498–502. doi:10.4103/0028-3886.144439
15. Zacharia BE, Hickman ZL, Grobelny BT, DeRosa P, Kotchetkov I, Ducruet AF, et al. Epidemiology of aneurysmal subarachnoid hemorrhage. Neurosurg Clin N Am (2010) 21:221–33. doi:10.1016/j.nec.2009.10.002
16. Carpenter KL, Czosnyka M, Jalloh I, Newcombe VF, Helmy A, Shannon RJ, et al. Systemic, local, and imaging biomarkers of brain injury: more needed, and better use of those already established. Front Neurol (2015) 6:26. doi:10.3389/fneur.2015.00026
17. Budohoski KP, Guilfoyle M, Helmy A, Huuskonen T, Czosnyka M, Kirollos R, et al. The pathophysiology and treatment of delayed cerebral ischaemia following subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry (2014) 85:1343–53. doi:10.1136/jnnp-2014-307711
18. Rowland MJ, Hadjipavlou G, Kelly M, Westbrook J, Pattinson KT. Delayed cerebral ischaemia after subarachnoid haemorrhage: looking beyond vasospasm. Br J Anaesth (2012) 109:315–29. doi:10.1093/bja/aes264
19. Sarrafzadeh AS, Vajkoczy P, Bijlenga P, Schaller K. Monitoring in neurointensive care – the challenge to detect delayed cerebral ischemia in high-grade aneurysmal SAH. Front Neurol (2014) 5:134. doi:10.3389/fneur.2014.00134
20. Macdonald RL, Pluta RM, Zhang JH. Cerebral vasospasm after subarachnoid hemorrhage: the emerging revolution. Nat Clin Pract Neurol (2007) 3:256–63. doi:10.1038/ncpneuro0490
21. Dumont AS, Dumont RJ, Chow MM, Lin CL, Calisaneller T, Ley KF, et al. Cerebral vasospasm after subarachnoid hemorrhage: putative role of inflammation. Neurosurgery (2003) 53:123–35. doi:10.1227/01.NEU.0000068863.37133.9E
22. Miller BA, Turan N, Chau M, Pradilla G. Inflammation, vasospasm, and brain injury after subarachnoid hemorrhage. Biomed Res Int (2014) 2014:384342. doi:10.1155/2014/384342
23. Chou SH, Robertson CS; Participants in the International Multi-disciplinary Consensus Conference on the Multimodality Monitoring. Monitoring biomarkers of cellular injury and death in acute brain injury. Neurocrit Care (2014) 21(Suppl 2):S187–214. doi:10.1007/s12028-014-0039-z
24. Hong CM, Tosun C, Kurland DB, Gerzanich V, Schreibman D, Simard JM. Biomarkers as outcome predictors in subarachnoid hemorrhage – a systematic review. Biomarkers (2014) 19:95–108. doi:10.3109/1354750X.2014.881418
25. Kiiski H, Tenhunen J, Ala-Peijari M, Huhtala H, Hämäläinen M, Långsjö J, et al. Increased plasma UCH-L1 after aneurysmal subarachnoid hemorrhage is associated with unfavorable neurological outcome. J Neurol Sci (2016) 361:144–9. doi:10.1016/j.jns.2015.12.046
26. Kiiski H, Långsjö J, Tenhunen J, Peltola J. Time-courses of plasma IL-6 and HMGB-1 reflect initial severity of clinical presentation but do not predict poor neurologic outcome following subarachnoid hemorrhage. eNeurologicalSci (2016) 6:55–62. doi:10.1016/j.ensci.2016.11.010
27. Lucke-Wold BP, Logsdon AF, Manoranjan B, Turner RC, McConnell E, Vates GE, et al. Aneurysmal subarachnoid hemorrhage and neuroinflammation: a comprehensive review. Int J Mol Sci (2016) 17:497. doi:10.3390/ijms17040497
28. Höllig A, Remmel D, Stoffel-Wagner B, Schubert GA, Coburn M, Clusmann H. Association of early inflammatory parameters after subarachnoid hemorrhage with functional outcome: a prospective cohort study. Clin Neurol Neurosurg (2015) 138:177–83. doi:10.1016/j.clineuro.2015.08.030
29. Zhu XD, Chen JS, Zhou F, Liu QC, Chen G, Zhang JM. Relationship between plasma high mobility group box-1 protein levels and clinical outcomes of aneurysmal subarachnoid hemorrhage. J Neuroinflammation (2012) 9:194. doi:10.1186/1742-2094-9-194
30. Ma C, Zhou W, Yan Z, Qu M, Bu X. Toll-like receptor 4 (TLR4) is correlated with delayed cerebral ischemia (DCI) and poor prognosis in aneurysmal subarachnoid hemorrhage. J Neurol Sci (2015) 359:67–71. doi:10.1016/j.jns.2015.10.018
31. Backes Y, van der Sluijs KF, Mackie DP, Tacke F, Koch A, Tenhunen JJ, et al. Usefulness of suPAR as a biological marker in patients with systemic inflammation or infection: a systematic review. Intensive Care Med (2012) 38:1418–28. doi:10.1007/s00134-012-2613-1
32. Donadello K, Scolletta S, Covajes C, Vincent JL. suPAR as a prognostic biomarker in sepsis. BMC Med (2012) 10:2. doi:10.1186/1741-7015-10-2
33. Laban KG, Rinkel GJ, Vergouwen MD. Nosocomial infections after aneurysmal subarachnoid hemorrhage: time course and causative pathogens. Int J Stroke (2015) 10:763–6. doi:10.1111/ijs.12494
34. Stevens RD, Nyquist PA. The systemic implications of aneurysmal subarachnoid hemorrhage. J Neurol Sci (2007) 261:143–56. doi:10.1016/j.jns.2007.04.047
35. Koch A, Voigt S, Kruschinski C, Sanson E, Dückers H, Horn A, et al. Circulating soluble urokinase plasminogen activator receptor is stably elevated during the first week of treatment in the intensive care unit and predicts mortality in critically ill patients. Crit Care (2011) 15:R63. doi:10.1186/cc10037
36. Roos Y, Levi M, Carroll TA, Beenen LFM, Vermeulen M. Nimodipine increases fibrinolytic activity in patients with aneurysmal subarachnoid hemorrhage. Stroke (2001) 32:1860–2. doi:10.1161/01.STR.32.8.1860
37. Sidenius N, Andolfo A, Fesce R, Blasi F. Urokinase regulates vitronectin binding by controlling urokinase receptor oligomerization. J Biol Chem (2002) 277:27982–90. doi:10.1074/jbc.M111736200
38. Pliyev BK. Activated human neutrophils rapidly release the chemotactically active D2D3 form of the urokinase-type plasminogen activator receptor (uPAR/CD87). Mol Cell Biochem (2009) 321:111–22. doi:10.1007/s11010-008-9925-z
39. Haga Y, Dumitrescu A, Zhang Y, Stain-Malmgren R, Sjöquist PO. Effects of calcium blockers on the cytosolic calcium, H2O2 production and elastase release in human neutrophils. Pharmacol Toxicol (1996) 79:312–7. doi:10.1111/j.1600-0773.1996.tb00015.x
40. Galliera E, Drago L, Marazzi MG, Romanò C, Vassena C, Corsi Romanelli MM. Soluble urokinase-type plasminogen activator receptor (suPAR) as new biomarker of the prosthetic joint infection: correlation with inflammatory cytokines. Clin Chim Acta (2015) 441:23–8. doi:10.1016/j.cca.2014.11.029
41. Eugen-Olsen J, Andersen O, Linneberg A, Ladelund S, Hansen TW, Langkilde A, et al. Circulating soluble urokinase plasminogen activator receptor predicts cancer, cardiovascular disease, diabetes and mortality in the general population. J Intern Med (2010) 268:296–308. doi:10.1111/j.1365-2796.2010.02252.x
42. Persson M, Engström G, Björkbacka H, Hedblad B. Soluble urokinase plasminogen activator receptor in plasma is associated with incidence of CVD. Results from the Malmö Diet and Cancer Study. Atherosclerosis (2012) 220:502–5. doi:10.1016/j.atherosclerosis.2011.10.039
43. Olson FJ, Thurison T, Ryndel M, Hoyer-Hansen G, Fagerberg B. Soluble urokinase-type plasminogen activator receptor forms in plasma as markers of atherosclerotic plaque vulnerability. Clin Biochem (2010) 43:124–30. doi:10.1016/j.clinbiochem.2009.09.028
44. Garcia-Monco JC, Coleman JC, Benach JL. Soluble urokinase receptor (uPAR, CD 87) is present in serum and cerebrospinal fluid in patients with neurologic diseases. J Neuroimmunol (2002) 129:216–23. doi:10.1016/S0165-5728(02)00186-8
45. Jalkanen V, Vaahersalo J, Pettilä V, Kurola J, Varpula T, Tiainen M, et al. The predictive value of soluble urokinase plasminogen activator receptor (suPAR) regarding 90-day mortality and 12-month neurological outcome in critically ill patients after out-of-hospital cardiac arrest. Data from the prospective FINNRESUSCI study. Resuscitation (2014) 85:1562–7. doi:10.1016/j.resuscitation.2014.08.017
Keywords: aneurysmal subarachnoid hemorrhage, biomarkers, neurological outcome, secondary brain injury, soluble urokinase-type plasminogen activator receptor, neuroinflammation
Citation: Kiiski H, Jalkanen V, Ala-Peijari M, Hämäläinen M, Moilanen E, Peltola J and Tenhunen J (2017) Plasma Soluble Urokinase-Type Plasminogen Activator Receptor Is Not Associated with Neurological Outcome in Patients with Aneurysmal Subarachnoid Hemorrhage. Front. Neurol. 8:144. doi: 10.3389/fneur.2017.00144
Received: 15 February 2017; Accepted: 30 March 2017;
Published: 18 April 2017
Edited by:
J. Marc Simard, University of Maryland Baltimore, USAReviewed by:
Anke Höllig, Uniklinik RWTH Aachen, GermanyCaron Hong, University of Maryland Medical Center, USA
Copyright: © 2017 Kiiski, Jalkanen, Ala-Peijari, Hämäläinen, Moilanen, Peltola and Tenhunen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Heikki Kiiski, aGVpa2tpLmtpaXNraUBmaW1uZXQuZmk=
†These authors have contributed equally to this work.